combined therapy vasodilator and beta-adrenergic...
TRANSCRIPT
Combined Therapy with Vasodilator Drugsand Beta-Adrenergic Blockade
in Hypertension
A Comparative Study of Minoxidil and Hydralazine
By THOMAS B. GOTTLIEB, M.D., FRED H. KATZ, M.D.,
AND CHARLES A. CHIDSEY III, M.D.
SUMMARYThe hypotensive efficacies of two vasodilators, hydralazine and minoxidil, were as-
sessed as these drugs were used individually in combination with beta-adrenergicblockade and diuretics in 11 hypertensive patients in whom elevated blood pressurehad not been adequately controlled previously by other antihypertensive therapy.
Control supine blood pressure fell from 191/128 mm Hg on propranolol and hydro-chlorothiazide to 169/108 mm Hg on hydralazine, with a significantly greater reduc-tion to 142/92 mm Hg on minoxidil. Although sodium retention and tachycardia werecontrolled by the use of concomitant diuretics and beta-blockade, an increment in eachof these drugs was occasionally required to prevent these complications. Renal func-tion was changed little with the decrease in blood pressure. Plasma renin increasedfrom a standing control of 14.5 mgg/ml/hr to 35.9 and 31.1 m,gg/ml/hr, respectively,on hydralazine and minoxidil. These data suggest the role of vasodilators used incombination with beta-blockers and diuretics and indicate the greater therapeuticefficacy of minoxidil.
Additional Indexing Words:Antihypertensive therapy Propranolol Renin Aldosterone
T HE USE OF drugs which lower bloodpressure by direct dilation of the arterial
bed appears to be a logical approach to thetreatment of systemic hypertension. Such vaso-dilator drugs will reverse the elevated periph-eral vascular resistance characteristics of hy-pertension without producing the side effectsso frequently encountered with drugs that in-terfere with total adrenergic function.' In a
From the Department of Medicine, University ofColorado Medical Center, Denver, Colorado.
Supported by grants from the National Heart andLung Institute (HE-05722 and HE-09932) and fromthe Population Council, New York, New York.
Address for reprints: Dr. Charles A. Chidsey III,Division of Clinical Pharmacology, University of Colo-rado Medical Center, 4200 East Ninth Avenue, Den-ver, Colorado 80220.
Received August 6, 1971; revision accepted forpublication October 21, 1971.
Circuation, Volume XLV, March 1972
previous study minoxidil, a new vasodilator,was shown to lower blood pressure effectivelyin hypertensive patients and to have a signifi-cantly greater effect when combined withbeta-adrenergic blockade with propranolol.2Beta-blockade itself has recently received con-siderable attention in the treatment of hyper-tension.3 4 However, the magnitude of theantihypertensive response with beta-blockadealone has been variable, with some investi-gators reporting effective control of hyperten-sion using propranolol,5 while others havefound minimal reductions using either pro-pranolol6 or newer beta-blocking drugs, alpre-nolol7 and practolol.8 In addition, propranololhas been found not to lower vascular resis-tance, and the observed hypotensive responseappears to be the consequence of a reductionin cardiac output.6
571
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

GOTTLIEB ET AL.
It would seem preferable to control bloodpressure in hypertension by lowering vascularresistance with direct-acting vasodilators andto use beta-adrenergic blockade secondarily toprevent reflex stimulation of the heart, thusmaintaining an unchanged cardiac output. Infact, this approach has been demonstrated us-ing minoxidil combined with propranolol.`
In the present report we have extended ourprevious observations with minoxidil2 to com-pare its therapeutic power or efficacy directlywith that of hydralazine, the standard vaso-dilator available for treatment of hypertension.In this study we have examined the relativeantihypertensive efficacy of minoxidil and hy-dralazine in a group of hypertensive patientswho were difficult to manage with convention-al antihypertensive therapy. These two vaso-dilators were used sequentially in the samepatients together with beta-blockade and di-uretic therapy to inhibit both the reflexly in-duced tachycardia and the sodium retentionthat are known to accompany the effect ofvasodilators in hypertension.9 Thus, we wereable to compare the efficacy of minoxidil withthat of hydralazine in the control of severehypertension.
MethodsEleven patients were studied ranging from 29
to 55 years of age; seven were males and fourwere females; two were Negroes. Essential hyper-tension was present in 10 patients and unilateralrenal artery disease complicated by azotemia waspresent in one (K L A). Severe hypertension waspresent in spite of the administration of a varietyof major antihypertensive drugs together withdiuretics in all but one patient (table 1). The solepatient (D A V) not on therapy was unable totolerate alpha-methyldopa or hydrochlorothiazidebecause of previous drug reactions and would notaccept guanethidine. Side effects of those anti-hypertensive drugs being used when the patientswere considered for the study occurred in sevenof the patients. The extent of therapy before in-clusion into the study reflected the patients' tol-erance to the drugs. In several instances majordrugs had been discontinued earlier because ofintolerable side effects or lack of response to thesedrugs.
Retinopathy was present in all, varying fromgrade II to grade IV. Cardiac evaluation revealedeither electrocardiographic evidence of left ven-tricular hypertrophy or radiographic evidence of
left ventricular dilation or both. Three patients hadmild to moderate symptoms of hypertensive en-cephalopathy and one had had a previous sub-arachnoid hemorrhage. In all but one patient(H U R) renal function was depressed and serumcreatinine levels ranged from 1.4 to 7.5 mg/100 ml.A complete description of the experimental na-
ture of the study and of the drugs to be used waspresented to all the patients and written consentwas obtained. Antihypertensive therapy, with theexception of hydrochlorothiazide, was then dis-continued for 1 to 3 weeks in seven patients;in four other patients (B R I, P U L, K A U, andM A C) the patients' clinical status would notjustify stopping these drugs during this prestudyperiod and the patients were admitted to the studywithout such a preliminary drug-free period.The patients were hospitalized in the Clinical
Research Center of the University of ColoradoMedical Center for study. Throughout the studyall were placed on a sodium intake that was con-stant in each patient but varied among the pa-tients from 50 to 160 mEq/day, the level of sodi-um intake being determined by individual dietaryhistories. Daily weights were obtained and bloodpressures and heart rates were measured four timesdaily with the patients in the supine and erectpositions. Twenty-four hour urine collections wereobtained for analysis of creatinine and sodi-um output together with 3-day stool collec-tions for sodium output which provided the datafor sodium balance studies.
Serial laboratory determinations were monitoredduring a control, hydralazine, and minoxidil pe-riod, including chest film, electrocardiogram, lupuserythematosis (LE) preparation, and serum cre-atinine, lactate dehydrogenase (LDH), creatinephosphokinase (CPK), serum glutamic oxaloacetictransaminase (SGOT), and antinuclear factor. Inaddition, renal function was measured by clear-ance techniques using continuous infusion of para-aminohippurate (PAHl) and inulin contained in0.9% NaCl at a rate of 1 ml/min.10 The urineswere collected with spontaneous voiding during awater diuresis. Plasma renin activity and aldoste-rone concentration were determined during thethree study periods by radioimmunoassay;t1 12bloods were drawn after 8 hours with the pa-tients in the supine fasting state and after 2hours in the erect position. The data were analyzedby standard statistical methods using Student's t-test for paired data and linear regression analysis.
In eight patients the study was begun with acontrol period of 4 to 6 days during whichthese patients received diuretics and propranolol,with the latter administered every 6 hours. Inthe remaining three patients, a drug-free controlperiod was not present before vasodilator drugs
C'rculation, Volume XLV. March 1972
572
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

VASODILATOR DRUGS IN HYPERTENSION 573
ct
ct
ct
P4
CZ,
ct
ct cn
ct
Z;
ct
ct
P4Ct
P4
7
pu
P4
ctP4
T-r~
,:~
w-C
W
c
C)z
z
z 0U Z
a)
z
W
c
a)
:t
E11c3
xll
¢S ¢
rr -ZI"i-l ,i-- -.-, 4
--- ' '> ...--!. .: ::. 4
W1 4 z .2 -5 .. J .
S-W h-W W-W S-4.-S S-4
c :.. .. ..1-1 -e. > -.!. >
... si .-",
+.PZ
:>t_
QCc
c-
-11-f--a)9.
m bim ...CD
.. Ec E00-
dq
dq1- c
c,
X
---
t-
a) D
XL CZ
nf
c3
c
C.
4-_-R
:: e,, ,: _,;~4
C MUt NDsc_0
_ a _
Circulation, VolumeXL,Mrh17
C-
c
C.
-j c::+- 2
m n *^. 'tnt O c- O c CO c m - O m C- OO cl-O cc Cn o~ o csic cl] c cq ~
1-4
CS
--j
.i"
a)Z1
"j .'- d -d 0>-. .. -51 .>. z
..,. .!i.-J- ... .zxSwS z = ¢ r 3 <~~'h
a 2 >~~~c..1
-c -0
cq .:) z.!. t
.4
P..
-0
t-- .
1. c. r--,1-1.I" .c
_ -0_ U
C
ct _
-r.; =; Jc
= c 3-C1,~ -4~c
.-_ r 1
_ #C XC ct
_ 4 ; ., _
,_
't t
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

GOTTLIEB ET AL.
t-b , j .c . 0] c . S -ZC X - 0 0]-l 1 -0]
-_ -_ _ _--- 1 01
"!t CZ _ _Z ^S X t- _1-'C -_-: r
-_ - -_^ _
_E ^ - -;1 X -- 1S e
0- X 1 - ---:- ,^
c,l 7~ __~7 = X - - --- )`X X XL _- X t- t- X X
X -z 01 crX X 0,1 - X X ct- 1- t- X X t- X I- Cc t- X
1 YIrIL _01 -I IL ^c X X -- -- X 1- X Xc X0110 IIxL
IR-A -- X -- "!^' cc1)]I- t_ X t- 1- t- 1- 1- X
] 'I 011,X IX
--C-_ ^ 1CI_X ^ LO 01 01- 0: X XL X c,
U -" X
co _IL00IL IL 1 IL -01100101
CS-0 1 10
_0 IL C1 t^I IL _1
U- 10 C- U01_Z1 1-
rs 10101_ 0]d10
_I _ _
-..-1;0_ C C01
IL_ 0-
doU- Co 001 X 0_1 ,_ 01_
IL X0000
cc 1,1 O ^ t-- --W X Zt\\- \C0I~1 L IL 011~
-4
XIL 10_IL 1 U- 0101_
In-=---4^X5 "!,W : \!~7-: O C.
01 0~̂1 CO :01C~L^."~401f7C0~10-0-1 -9 10 _0
01 0,11001~ \~C ll
'' }--Q
01 01_1 01 _0
XI
X U-
C10-~
c=
01-
Ll^:Cd X -_
_ _W -4 IL -
00 -4_
10XI)X DC'XN C7S i _1 :,n -4 O - CS d
I _ _" --_. -- 1_4
,- 0 A'
_0 CO1-4 -4
x GC
:RcO
11 11
z z
Circulat
574
I'-
-1
VT.i
_0._
SE
W
.00.:tao2
-0
*._
It
._
G0
._e
. _
.-c3
ron, Voum
&..
0D
C0
0>
0:
P0
0
0
0
.0 .. ... -. .. . . .. > 111 US.-1.1 U -cC$ . S-. C) -.i, .. -. -. .Q .-.
-.pm. cc X .4 .m p-.' P. .4 _^4 .C- h-. ..
XLV, March 1972
Il!+ *-`
---
_.-
,'.1,
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

VASODILATOR DRUGS IN HYPERTENSION
were started and the control values representedthose obtained during an initial hospital treatmentperiod on the general medical service prior totransfer to the Clinical Research Ward. These pa-tients (B R I, K A U, and M A C) were all onalpha-methyldopa and hydrochlorothiazide and,in addition, one (K A U) was on guanethidine aswell. In these patients the therapy period was be-gun by adding propranolol and hydralazine simul-taneously, continuing hydrochlorothiazide, anddiscontinuing alpha-methyldopa and guanethidine.
Minoxidil and hydralazine were generally givenevery 6 hours, although those patients who weretreated with less than 20 mg of minoxidil dailyreceived the drug less frequently. In one patient(S C H) minoxidil was given prior to hydralazine;following its discontinuance blood pressure re-mained at the reduced level for at least 9 days, atwhich time the study was discontinued and thepatient discharged. Therefore, in the subsequent10 patients hydralazine was administered first for5 to 10 days followed by minoxidil for 7 to 14days, completing the study. One patient (B R I)was readmitted later while on chronic minoxidiltreatment specifically for study of the time of onsetand duration of the hypotensive activity ofminoxidil.
Results
The therapeutic response to minoxidil wasgreater than that to hydralazine in these hyper-tensive patients (table 2). Hydralazine con-sistently lowered the blood pressure when thepatient was in the recumbent position from anaverage control level of 191/128 to 169/108(P <0.01). This hypotensive response wasachieved without any orthostatic symptomsand no postural decline in diastolic blood pres-sure was observed. A moderate decline in sys-tolic blood pressure was observed in nine pa-tients, but this was present in both the controland hydralazine periods. Substitution of min-oxidil resulted in a markedly improved anti-hypertensive effect, with the average bloodpressure declining from 169/108 on hydral-azine to 142/92 in the group of 10 patients inwhom it was possible to compare the minox-idil response directly to that of hydralazine(P < 0.02). Again, there was an orthostatic de-cline in systolic blood pressure, but here it wasof smaller magnitude than in the other pe-riods of observation.
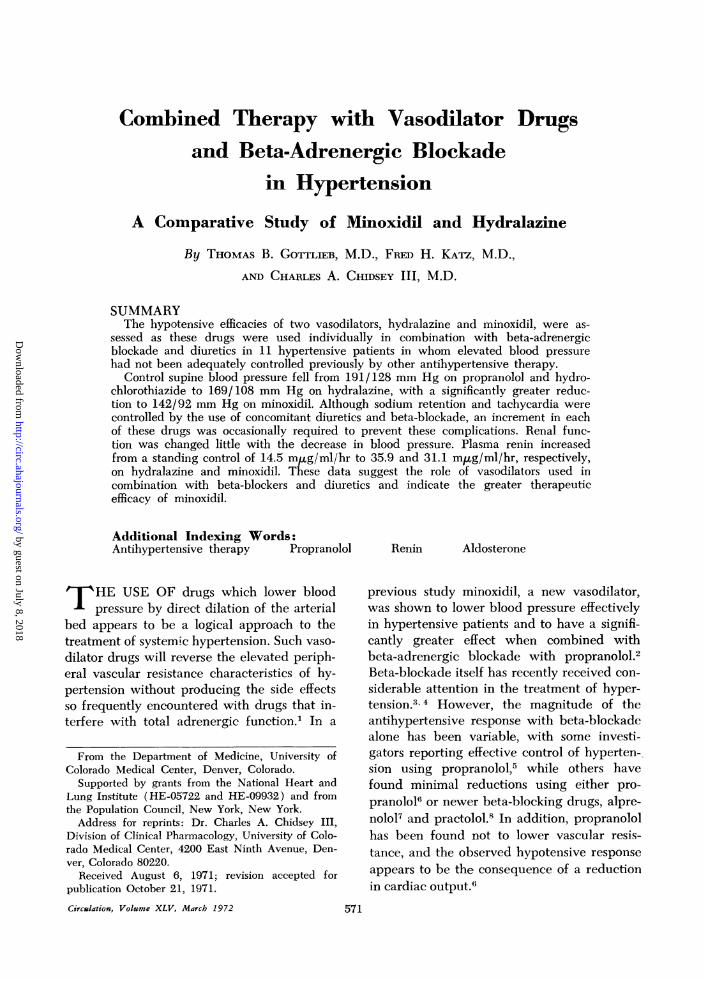
The hospital course of one patient (BAL)particularly emphasizes the therapeutic effi-cacy of vasodilators when used in combinationwith beta-adrenergic blockade (fig. 1). Thispatient was difficult to control in clinic becauseshe could not tolerate alpha-methyldopa be-cause of its central nervous system side effects,and guanethidine produced severe posturalhypotension in the absence of significant re-duction of supine blood pressure. She devel-oped symptoms of hypertensive encephalop-athy on hydrochlorothiazide therapy in theclinic and was admitted to the Clinical Re-search Center because of these symptoms.Initial therapy with alpha-methyldopa wasunsatisfactory because of recurrence of som-nolence and symptomatic postural hypoten-sion. Consequently, alpha-methyldopa wasstopped and propranolol was begun, followedsequentially by hydralazine and then minox-idil. Although some control of blood pressurewas effected by hydralazine (600 mg/day),it was only when minoxidil was substitutedthat adequate blood pressure control wasachieved. With supine blood pressures in the140/88 mm Hg range, systolic postural hypo-tension was observed, but this was not sympto-matic, nor was there any decline in diastolicpressure on standing. The systolic hypotensionthat was observed on standing may have beendue to a relatively inadequate blood volume,the consequence of excessive diuretics, in thepresence of minoxidil-induced dilation of thevascular bed.The complications of any vasodilator used
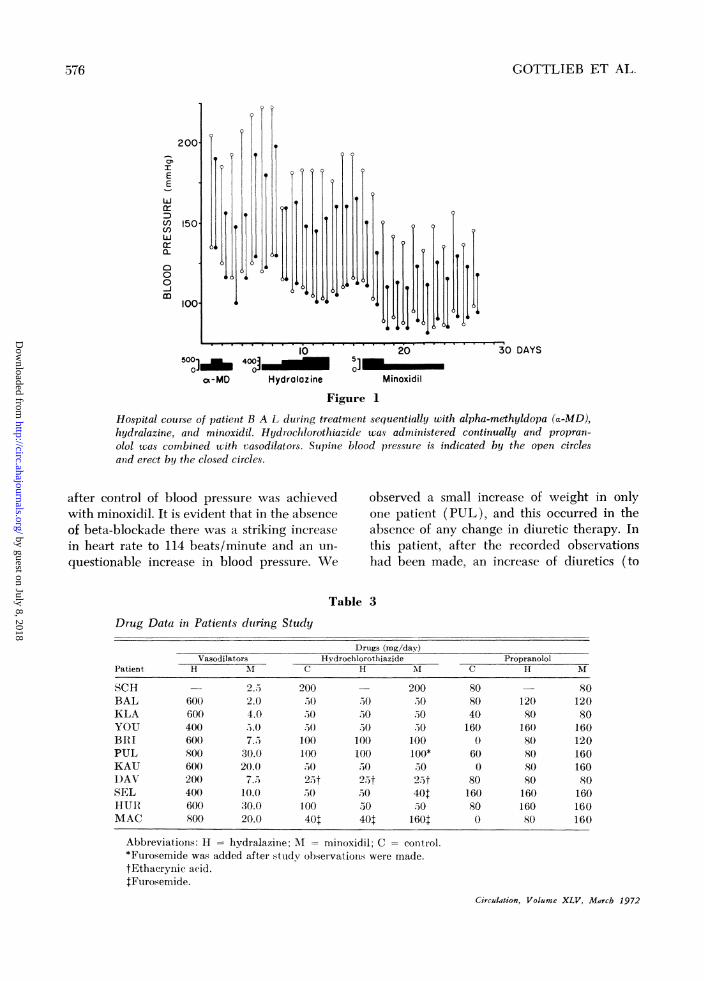
in the hypertensive patient, such as tachycar-dia, sodium retention, and weight gain, werenot observed in this group of patients. Al-though tachycardia vas not encountered dur-ing the hypotensive response with hydralazineand minoxidil, increased adrenergic blockadewas required during minoxidil in four patientsto maintain heart rate at the control level(table 3). It was of some interest to determinehow long propranolol would be required toblock the reflex adrenergic stimulation of car-diac function associated with vasodilation anda reduced blood pressure. In one patient (fig.2), propranolol was discontinued for 2 days
Circulation, Volume XLV, March 1972
575
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from
GOTTLIEB ET AL.
200
crE
E
W
150UnllJJ
c0
0
0
m100.
3- _ . . . . 2 . . . 1
10 20500]_ 40j0 5]
ox-MD Hydralazine Minoxidil
i0 DAYS
Figure 1
Hospital courXse of patient B A L during treatment sequentially with alpha-methyldopa (a-MD),hydralazine, and minoxidil. Hydrochlorothiazide was adninlistered continually and propran-olol wias combined with vasodilators. Supine blood pressure is indicated by the open circlesand erect by the closed circles.
after control of blood pressure was achievedwith minoxidil. It is evident that in the absenceof beta-blockade there was a striking increasein heart rate to 114 beats/minute and an un-
questionable increase in blood pressure. We
observed a small increase of weight in onlyone patient (PUL), and this occurred in theabsence of any change in diuretic therapy. Inthis patient, after the recorded observationshad been made, an increase of diuretics (to
Table 3
Drug Data in Patients duering Study
Drtugs (mg/day)Vasodilators Hydrochlorothiazide Propranolol
Patient H MI C H M C H M
SCH 2.5 200 200 80 80BAL 600 2.0 ;50 50 o080 120 120KLA 600 4.0 .50 50 150 40 o0 80YOU 400 5. 5( 30() 50 160 160 160BRIi 600 7.5 100 100 100 0 80 120PUL 800 30.0 100 100 100* 60 80 160KAU 600 20.0 50 50 570 0 80 160DAV 200 7.5 2,t 25t 25t 8( 80 80SEL 400 10.0 50 50 40t 160 160 160HUR 600 30.0 100 30 50 80 160 160MAC 800 20.0 40t 40$ 160t 0 80 160
Abbreviations: H hydralazirne; :1 = minoxidil; C control.*Ftlrosemide was added after studv observations were made.tEthacrynic acid.tFurosemide.
Circulation, Volume XLV, Marcb 1972
. 1 .
/D
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from
VASODILATOR DRUGS IN HYPERTENSION
200.c,.I
EE
WX
U) 150.UnWerLL
000m
100
I-E 100.
W80
U)
CLj ^
[E] MINOXIDIL I
6'0 7 0,7 0, 2 '4' 6, 8' 10`12 DAYS
IPROPRANOLOL8 80
S 100 IHCTZ 100
Figure 2Blood pressure and heart rate data are summarizedfrom one patient (P U L) during the control period(C), the hydralazine period (H), and the minoxidil pe-
riod. The effect of withdrawing propranolol (arrows)is shown by the increase in blood pressure and heartrate. HCTZ = hydrochlorothiazide.
40 mg/day of furosemide) effected a returnto her control weight. Similar increases in di-uretics were required in only two other patients(SEL and MAC) during the study period,specifically in order to maintain weight at thecontrol level (table 3). The sodium balancedata provided no evidence of sodium accumu-
lation.Renal function was variable in the patients
studied, ranging from normal values to levelsof frank azotemia (table 4). The glomerularfiltration rate was largely unchanged duringthe hypotensive response to either hydralazineor minoxidil. The effective renal plasma flowwas slightly increased during both hydralazineCirculation, Volume XLV, March 1972
and minoxidil, but the average increase in thegroup as a whole was insignificant during eachtreatment period. Although sodium retentionwas not observed on either vasodilator withthe dietary sodium loads that were used, di-minished sodium excretion was observed tran-siently in six of seven patients during minoxidilwith the acutely increased sodium load (150,Eq/min) used during the renal clearancestudies.
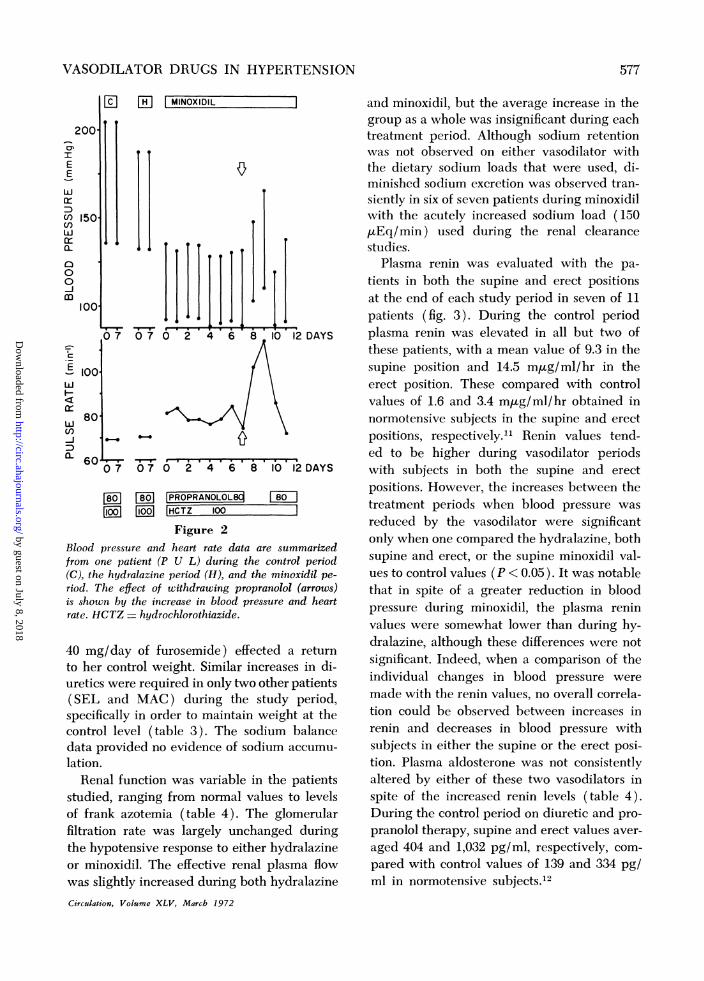
Plasma renin was evaluated with the pa-tients in both the supine and erect positionsat the end of each study period in seven of 11patients (fig. 3). During the control periodplasma renin was elevated in all but two ofthese patients, with a mean value of 9.3 in thesupine position and 14.5 mgg/ml/hr in theerect position. These compared with controlvalues of 1.6 and 3.4 m,ug/ml/hr obtained innormotensive subjects in the supine and erectpositions, respectively.'1 Renin values tend-ed to be higher during vasodilator periodswith subjects in both the supine and erectpositions. However, the increases between thetreatment periods when blood pressure wasreduced by the vasodilator were significantonly when one compared the hydralazine, bothsupine and erect, or the supine minoxidil val-ues to control values (P < 0.05). It was notablethat in spite of a greater reduction in bloodpressure during minoxidil, the plasma reninvalues were somewhat lower than during hy-dralazine, although these differences were notsignificant. Indeed, when a comparison of theindividual changes in blood pressure weremade with the renin values, no overall correla-tion could be observed between increases inrenin and decreases in blood pressure withsubjects in either the supine or the erect posi-tion. Plasma aldosterone was not consistentlyaltered by either of these two vasodilators inspite of the increased renin levels (table 4).During the control period on diuretic and pro-pranolol therapy, supine and erect values aver-aged 404 and 1,032 pg/ml, respectively, com-pared with control values of 139 and 334 pg/ml in normotensive subjects.12
577
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

Cl 02 CO Cl -(0 .o(0 CO . Cl k.C
Cl
.iz.;
.-4 - - L' .4
. Cl .CO02 t- (0Cl02. Cl - 02 IC-
02 (0 . (002CO 02 .O - Cl
Cl (0CO
CO . 020202020202 Cl
CO CO z 02Cl -
(0(0 .02 Cl(0(0
Cl Cl IC.LO
02 . 02 (0 . 02C . - CO 02 CO- CO
CO (0(002- 02
02 . Cl02.-CZIC- - (0- (0(0 -
(0IC-ci .,IC-02Cl 02.
(0 N.ClIC..
- . - Cl -- --CO
--02.02
(0.- Cl
.- - - Cl
COCIO
- - Cl -
(0 C- c.02 Cl '0 02 .- Cl CO CO L.
(0 CO 02 0202 IC- 02 Cl- - CO Cl IC-
(0 ..10o -02 .O CO- Cl CO Cl
- IC- CO 02 Cl ClCO CO IC- 2. .'
Cl CO . . Cl .CO .C c. 02 . 02
02 Cl . LO 02 (0CO . CO Y
GOTTLIEB ET AL.
14l
Ld
Cl:t t
cmc2
Cl-zr S
C Cl
5c
CO _
~~~~ (12~~~~~~~~1
n £
O dCO.
_S1
+-+
Circuation Volum XV
v X 2
- L? S
n 0
rrlClO
C:C
n (1(1
~~ClCln~~~~~ (12(1
a) d 2tt * I-+
C_clainVoueXV3Mrh17
578
CE
0
CM
P.0
I o~
CO..
I-~
X2 s
Iz f °
CO CO CO:
- - Cl -
C x
t-l LO C.lceXn̂ -
02b_C_ s
- 0
02 OCl ~
cOCl1t I-)0
Xl -
II!!.4).0C9
E..4 CO
0
C
C3
k-̂
F(.2
0
r.2E"t;
CIZ
-4-1r. ... 'i -. .) * .. .:) .. ..
-, U.2 b...4` U .C. b... 0 .:) -. -. P4 -,!.CdP.. m pp A >-. pp P.' .. "-, m nj.-,
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

VASODILATOR DRUGS IN HYPERTENSION
S ECONTROL
S E S EHYDRALAZINE
Figure 3MINOXIDIL
Plasma renin activity (mgig/ml/hr) as measured withpatients in both supine (S) and erect (E) positions inall three study periods. The mean and individual valuesare given.
Symptomatic improvement was noted inthose three patients who had significant symp-
tomatology in the control period (BAL,BRI, and PUL). These patients all had evi-dence of mild to moderate encephalopathy,and these findings cleared completely whenblood pressures were established within thetherapeutic range. Although some improve-ment of symptoms was observed with thehypotensive effect of hydralazine, it was onlywith the administration of minoxidil that com-
plete resolution of the patients' symptoms was
achieved. Untoward symptoms were minimalin both the hydralazine and minoxidil periods,and these were confined to transient angina inthree patients (KLA, KAU, and MAC)during the initiation of minoxidil therapy. Thissymptom was controlled by adjustment of theminoxidil dosage so that more gradual reduc-tion in blood pressure was accomplished or
by increasing the propranolol dosage. The an-
gina occurred without changes in serial electro-cardiograms or in serum enzymes.
Clinical studies of potential chemical toxicityof hydralazine, as used in these high doses,and of minoxidil were carried out. No altera-tion in serum enzymes, antinuclear factor, or
LE preparations was observed. Also, the ECGand chest films were unchanged during thetwo treatment periods.
Discussion
There is a rational physiologic basis in an
approach to the therapy of hypertension basedCirculation, Volume XLV, March 1972
on peripheral vascular dilators used in com-
bination with beta-adrenergic blocking drugs,with the latter being used to attenuate thereflex adrenergic activity stimulated by vaso-
dilation.2 Minoxidil has been shown to lowerarterial blood pressure in experimental animalsby a direct action on vascular smooth muscleand to exhibit no interference with autonomicfunction (W. A. Freyburger: Unpublished ob-servations). Furthermore, recent animal stud-ies have shown the drug to be specifically re-
tained in arterial tissue, which supports thecontention that this may be its locus of action.13The results of our present observations of the
use of minoxidil in hypertensive patients whoare relatively refractory to conventional anti-hypertensive therapy establish this approach as
an effective means of lowering blood pressure
and confirm earlier preliminary observationsfrom this laboratory that minoxidil can reduceblood pressure when used in combination withpropranolol.2 In the present study we haveshown, by direct comparison in the same group
of patients, that minoxidil is in fact more ef-fective as an antihypertensive drug than ishydralazine. Not only were much smalleramounts of drug required to achieve bloodpressure control in these patients, indicatinggreater pharmacologic potency, but in addi-tion minoxidil exhibited clearly greater efficacyor power. Thus, in four patients the hypoten-sive response to hydralazine was inadequatein spite of extremely large doses, whereas sub-stitution of minoxidil resulted in a substantiallygreater hypotensive effect. In only one patient(BRI) was the blood pressure response inminoxidil less than adequate, and in this pa-
tient the maximum hypotensive effect was notpursued because of a history of cerebral vas-
cular disease in this patient. Furthermore, ineight patients on chronic therapy of up to 10months we have recently encountered no evi-dence of tachyphylaxis to minoxidil. It mustbe emphasized that the doses of hydralazinewere clearly excessive and were of a magnitudethat could not be justified on any but a short-term basis because of the possibility of devel-opment of a lupus erythematosis-like syn-
drome.14 This problem, although considered
100
- 80'
-f 60-zzm 40
tn4 200C
579
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

GOTTLIEB ET AL.
as a potential complication of minoxidil in our
earlier report,' has not been found to be ofsubstance in these present observations, andantinuclear factor and LE preparations havebeen consistently negative.Although the rationale for the use of beta-
adrenergic blocking drugs in conjunction vithvasodilators has been suggested in earlier re-
ports,2-4 the importance of these drugs requiresfurther definition. Vasodilators have long beenrecognized as being capable of producingsymptoms of myocardial ischemia,9 and thesedrugs have not customarily been employedwithout some form of generalized inhibition ofadrenergic function.15 The specificity of beta-blockade in inhibiting primarily the cardiaccomponent of adrenergic innervation makes itpossible to utilize powerful vasodilators inhypertension without the side effects attendanton generalized inhibition of adrenergic func-tion. Interference with the reflex stimulation ofcardiac activity may also be important indiminishing the subjective manifestations, suchas palpitations and headache, which have beennoted with two vasodilators, hydralazine9 andguancydine.'6A further property of beta-blockade that
should be emphasized is its capacity to effecta greater hypotensive response than thatachieved with a vasodilator drug used alone.2This effect is accomplished by preventing or
attenuating the augmentation of cardiac out-put, thereby lowering blood pressure withoutany further alteration of vascular resistance.Propranolol used in this manner appears to bebetter justified than when used alone in thehypertensive patient, since vascular resistanceremains elevated under these latter eircum-stances.6 Combined therapy with propranololand minoxidil requires judicious adjustment ofthe levels of beta-blockade while achieving a
maximal hypotensive effect with minoxidil.Thus, it was necessary in the present studyoccasionally to increase the amount of propran-
olol or to adjust the amount of minoxidil toavoid excessive cardiac activity with the oc-
casional transient appearance of angina.The diuretics are drugs of equal importance
for use in combination with minoxidil or, in
fact, with any vasodilator. Sodium retentionhas been observed clinically with a variety ofvasodilators, and it has been suggested thatthe renal tubular basis of this response ismediated by enhanced sodium reabsorption inthe proximal convoluted tubule.17 We haveshown that small amounts of hydrochlorothi-azide are adequate to prevent sodium reten-tion under most circumstances. In threepatients with varying degrees of renal insuffi-ciency it was necessary to increase the diuretictherapy to include furosemide during maximalblood pressure reduction with minoxidil. So-dium excretion during the renal clearancestudies under the stimulus of a sodium load of150 gEq/min was in fact reduced in all pa-tients. However, with the exception of thethree patients mentioned above, sodium bal-ance was maintained on the individual dietarysodium intakes, suggesting preservation of thecapacity to handle sodium under normal cir-cumstances but a defective potential for dis-posing of large acute sodium loads. The use ofdiuretics in this study may have been re-sponsible for the fact that approximately equiv-alent hypotensive responses were achievedwith smaller amounts of minoxidil than wereemployed in our earlier study.2 Furthermore,we observed some moderate postural systolichypotension in the present study, whereas thiswas not appreciated earlier with minoxidil.This may have been the result of diuretic ther-apy which induced a hypovolemia, relative tothe dilated vascular bed. It should be empha-sized that such hypovolemia may be especiallyundesirable in the presence of inadequaterenal function and in these circumstancesmight be unnecessary with the use of minox-idil, which has such marked pharmacologicpower. Perhaps these patients would have hada similar therapeutic response with smalleramounts of diuretics and larger amounts ofminoxidil.
There were no other side effects except thoseof increased cardiac activity and sodium re-tention during the short-term evaluation ofminoxidil. Headache and palpitations specifi-cally were not encountered. The laboratory
Circulation, Volume XLV, March 1972
580
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

VASODILATOR DRUGS IN HYPERTENSION
tests that were monitored revealed no altera-tion of- renal or hepatic function. However,moderate hypertrichosis has been observed infive of eight patients on chronic treatment formore than 2 months. The mechanism of thisside effect has not been identified. This com-plication has also been seen with diazoxide.18
Observations on plasma renin were generallyconsistent with that response which could beanticipated with the use of vasodilators.19 Plas-ma renin tended to be higher during bloodpressure reduction with both vasodilators, al-though, despite the greater therapeutic re-sponse to minoxidil, plasma renin was no great-er during that period than during hydralazine.Individual patient responses were not exactlycompatible with existing concepts of renin se-cretion.20 Thus, changes in plasma renin couldnot be correlated with individual hypotensiveresponses or with decreases of sodium output.One important pharmacologic factor in therenin response of this group of patients may bethat of propranolol. This drug has been sug-gested to interfere with renin release,21 andthis factor may have played a role in the pres-ent observations.The lack of increase of aldosterone levels as
the renin values increased was an unexpectedfinding in view of the well-established relation-ship between plasma renin activity and bothaldosterone secretion and excretion rates.22These findings are consistent with our previousmeasurements of aldosterone excretion, whichdemonstrated that aldosterone excretion wasunchanged in patients treated with minoxidilwhen they received propranolol concurrently.2However, the explanation of the failure ofaldosterone secretion to increase (as indicatedby the -plasma aldosterone concentration) inthe face of significant increases in plasma reninis not readily apparent. It is interesting to spec-ulate that propranolol may not only interferewith renin release21 but may alter the effect ofthe renin stimulus on the secretion of aldoste-rone either by inhibition of angiotensin I con-version or by a direct effect on the adrenalcortical response to angiotensin II.As a final point, we have considered how
minoxidil, which clearly is effective in severe
Circulation, Volume XLV, March 1972
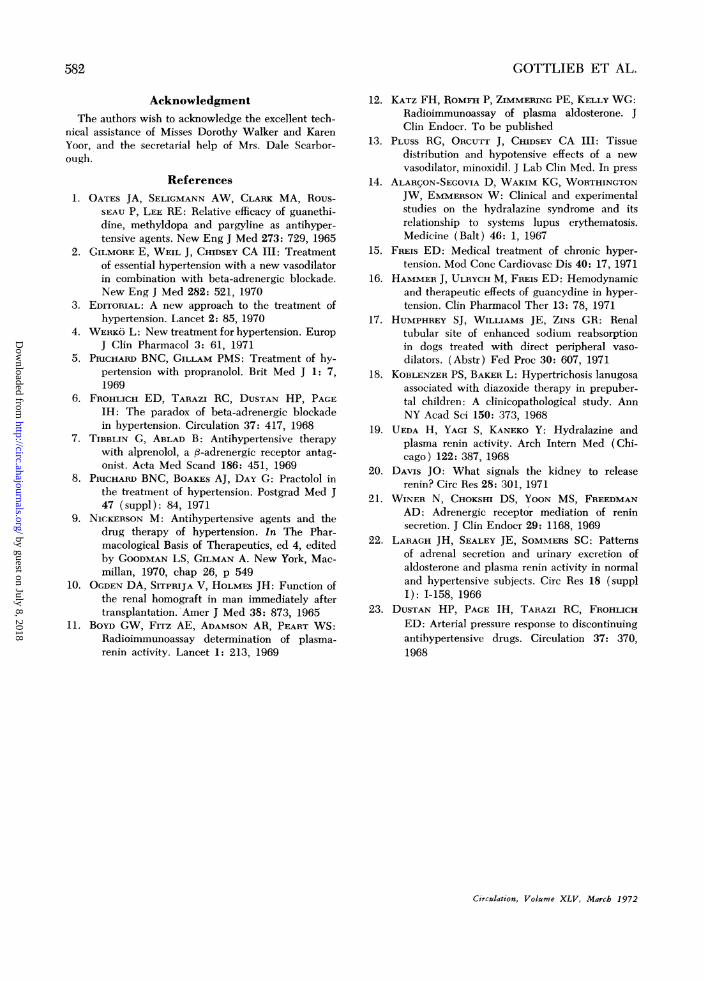
hypertension, may be used clinically. We havemade preliminary observations regarding dura-tion and onset of action of the drug when usedorally. The hypotensive effect was found topersist for several days after the drug was dis-continued (fig. 4). After reinstitution of ther-apy with a single oral dose of the drug, theonset of hypotensive action was rapid, occur-ring within a few hours. Although the rate atwhich controlled blood pressure values willreturn to a hypertensive level when therapy isstopped may be extremely variable, more se-verely hypertensive patients generally tend torevert more rapidly to their pretreatmentlevels.23 However, no data directly comparingthe duration of action of minoxidil with that ofother vasodilators are available at this time.If the suggestion of the prolonged action whichwe have derived from our clinical observationscan be substantiated, minoxidil would providean important advantage in therapy of hyper-tension, since patients might be treated witha single daily dose.
200'
IEE
W 150
Cl)(nC)Wa-
0 1000
iM 20mg/d
|PROPRANOLOLFUROSEMIDE
0 2 4 6 8
DAYS
4.M 20mg
160 mg/d80 mg/d
6 4 A 2 16 2HOURS
Figure 4
Blood pressure data on a patient (B R I) followingdiscontinuance of minoxidil (M) and after readminis-tration of a single oral dose (arrow).
S81
m
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from
GOTTLIEB ET AL.
AcknowledgmentThe authors wish to acknowledge the excellent tech-
nical assistance of Misses Dorothy Walker and KarenYoor, and the secretarial help of Mrs. Dale Scarbor-ough.
References1. OATES JA, SELIGMANN AW, CLARK MA, Rous-
SEAU P, LEE RE: Relative efficacy of guanethi-dine, methyldopa and pargyline as antihyper-tensive agents. New Eng J Med 273: 729, 1965
2. GILMORE E, WEIL J, CHIDSEY CA III: Treatmentof essential hypertension with a new vasodilatorin combination with beta-adrenergic blockade.New Eng J Med 282: 521, 1970
3. EDITORIAL: A new approach to the treatment ofhypertension. Lancet 2: 85, 1970
4. WERKO L: New treatment for hypertension. EuropJ Clin Pharmacol 3: 61, 1971
5. PRICHARD BNC, GILLAM PMS: Treatment of hy-pertension with propranolol. Brit Med J 1: 7,1969
6. FROHLICH ED, TARAZI RC, DUSTAN HP, PAGEIH: The paradox of beta-adrenergic blockadein hypertension. Circulation 37: 417, 1968
7. TIBBLIN G, ABLAD B: Antihypertensive therapywith alprenolol, a f3-adrenergic receptor antag-onist. Acta Med Scand 186: 451, 1969
8. PRICHARD BNC, BOAKES AJ, DAY G: Practolol inthe treatment of hypertension. Postgrad Med J47 (suppl): 84, 1971
9. NICKEIRSON M: Antihypertensive agents and thedrug therapy of hypertension. In The Phar-macological Basis of Therapeutics, ed 4, editedby GOODMAN LS, GILMAN A. New York, Mac-millan, 1970, chap 26, p 549
10. OGDEN DA, SITPRIJA V, HOLMES JH: Function ofthe renal homograft in man immediately aftertransplantation. Amer J Med 38: 873, 1965
11. BOYD GW, FITz AE, ADAMSON AR, PEART WS:Radioimmunoassay determination of plasma-renin activity. Lancet 1: 213, 1969
12. KATZ FH, ROMFH P, ZIMMERING PE, KELLY WG:Radioimmunoassay of plasma aldosterone. JClin Endocr. To be published
13. PLUss RG, ORCUTT J, CHIDSEY CA III: Tissuedistribution and hypotensive effects of a newvasodilator, minoxidil. J Lab Clin Med. In press
14. ALARCON-SEGOVIA D, WAKIM KG, WORTHINGTONJW, EMMERSON W: Clinical and experimentalstudies on the hydralazine syndrome and itsrelationship to systems lupus erythematosis.Medicine (Balt) 46: 1, 1967
15. FREIs ED: Medical treatment of chronic hyper-tension. Mod Conc Cardiovasc Dis 40: 17, 1971
16. HAMMER J, ULRYCH M, FREIs ED: Hemodynamicand therapeutic effects of guancydine in hyper-tension. Clin Pharmacol Ther 13: 78, 1971
17. HUMPHREY SJ, WILLIAMS JE, ZINs GR: Renaltubular site of enhanced sodium reabsorptionin dogs treated with direct peripheral vaso-dilators. (Abstr) Fed Proc 30: 607, 1971
18. KOBLENZER PS, BAKER L: Hypertrichosis lanugosaassociated with diazoxide therapy in prepuber-tal children: A clinicopathological study. AnnNY Acad Sci 150: 373, 1968
19. UEDA H, YAGI S, KANEKO Y: Hydralazine andplasma renin activity. Arch Intern Med (Chi-cago) 122: 387, 1968
20. DAVIS JO: What signals the kidney to releaserenin? Circ Res 28: 301, 1971
21. WINER N, CHOKSHI DS, YOON MS, FREEDMANAD: Adrenergic receptor mediation of reninsecretion. J Clin Endocr 29: 1168, 1969
22. LARAGH JH, SEALEY JE, SOMMERS SC: Patternsof adrenal secretion and urinary excretion ofaldosterone and plasma renin activity in normaland hypertensive subjects. Circ Res 18 (supplI): 1-158, 1966
23. DUSTAN HP, PAGE IH, TARAZI RC, FROHLICHED: Arterial pressure response to discontinuingantihypertensive drugs. Circulation 37: 370,1968
Circulation, Volume XLV, March 1972
582
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

THOMAS B. GOTTLIEB, FRED H. KATZ and CHARLES A. CHIDSEY IIIHypertension: A Comparative Study of Minoxidil and Hydralazine
Combined Therapy with Vasodilator Drugs and Beta-Adrenergic Blockade in
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1972 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation
doi: 10.1161/01.CIR.45.3.5711972;45:571-582Circulation.
http://circ.ahajournals.org/content/45/3/571located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer
of the Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle columnClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from