beta adrenergic blockers
TRANSCRIPT

Beta adrenergic blockers
Moderator Dr. Ali AhmadResident Dr. Karun Kumar (JR – II)

Overview of presentation
• Location & effects of β receptors
• Classification & brief overview of β blockers
• Chemistry & Pharmacokinetics of β blockers
• Pharmacodynamics of β blockers
• Effects of β blockers on CVS, RS, Eye, Metabolic, etc.
• Clinical pharmacology of β blockers and rationale of use
• Synopsis of β blockers (Uses, A/E, C/I, Interactions)
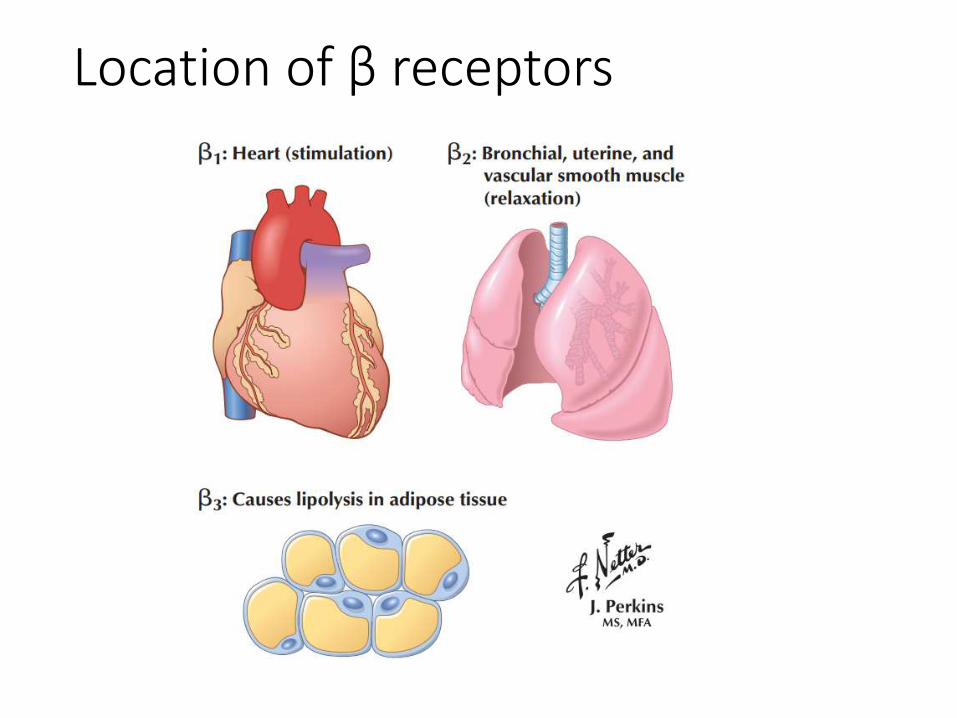
Location of β receptors


Introduction
• All β blockers used clinically are competitive
pharmacologic antagonists
• 1958 Dichloroisoprenaline (low potency &
partial agonist)
• 1963 Propranolol (blocks β1,β2 & weak activity
on β3). Also, an inverse agonist (↓ resting HR*)
*HR – Heart Rate

Classification
I. Nonselective (β1 and β2)
a. Without ISA* Propranolol, Sotalol, Timolol.
b. With ISA* Pindolol
c. Addnl. α blocking property Labetalol, Carvedilol
II. Cardioselective (β1) [safe in asthmatics]
Metoprolol, Atenolol, Acebutolol, Bisoprolol,
Esmolol, Betaxolol, Celiprolol, Nebivolol
*ISA - intrinsic sympathomimetic activity

Non-selective beta blockers
• Most imp. effects CVS & bronchial sm. Muscle
• Competitively block the effects of NE on β1 & β2
• Some exhibit ISA & memb. stabilizing (LA) activity
• Blockade of β1 receptors (Heart, Kidneys)
• Blockade of β2 receptors (Lungs, Liver)
• Also mask some of the early signs of hypoglycemia(e.g., tachycardia and sweating) in diabetic patients

Cardioselective β blockers (Rationale)
1. ↓ propensity to cause bronchoconstriction
2. Safer in diabetics
3. ↓ incidence of cold hands and feet
4. Less deleterious effect on blood lipid profile
5. Less liable to impair exercise capacity
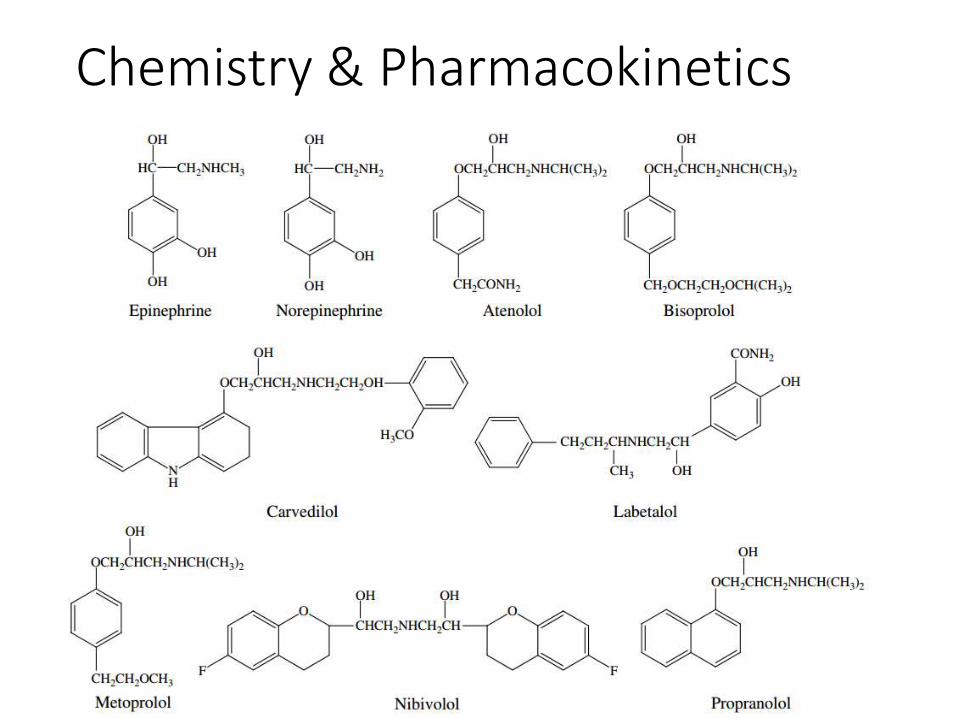
Chemistry & Pharmacokinetics

FPMBBB

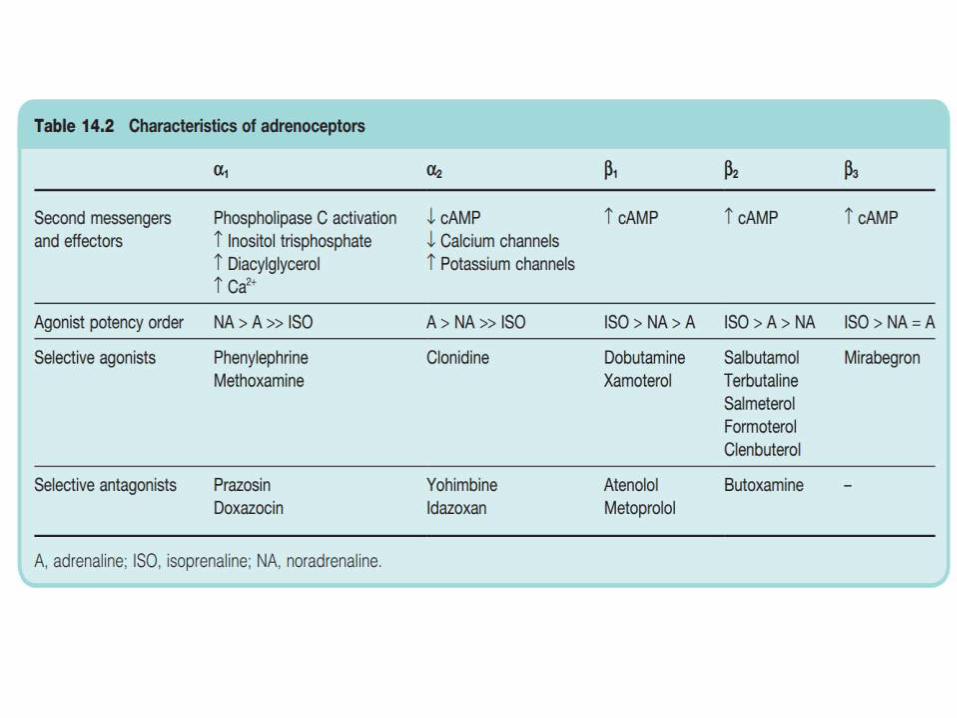
Pharmacodynamics

β1 β3β2

Effect on CVS
• Do not cause hypotension in healthy individuals
• Slowed AV conduction with ↑ PR interval β1 block in AVN
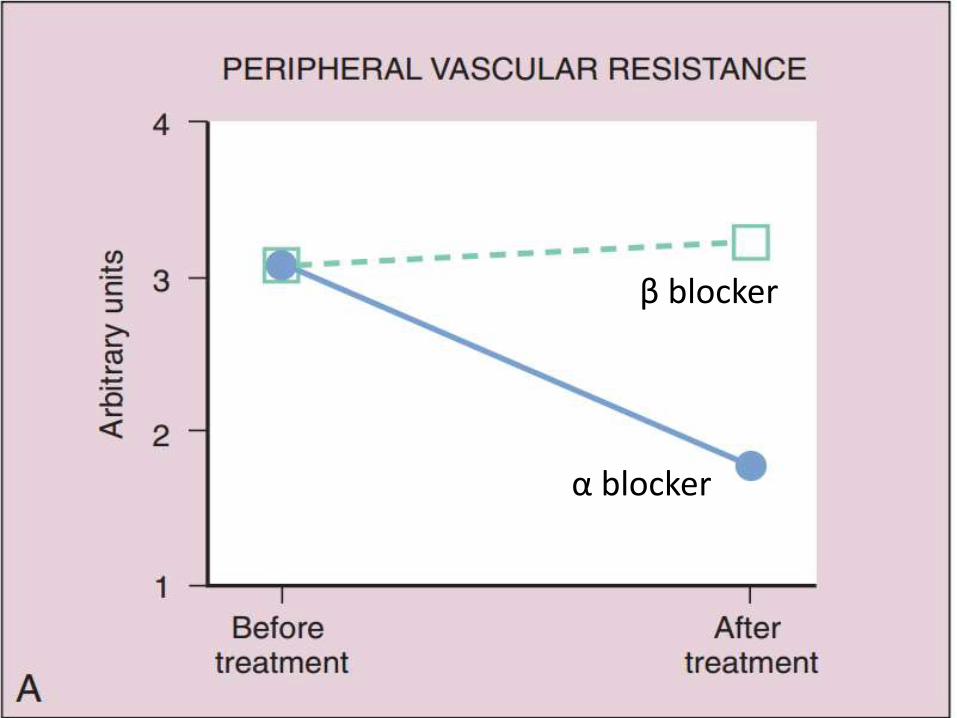
• In vascular system, β2 blockade ↑ SVR (α1)
• Nonselective and β1-block Inhibit renin
• Acute effects ↑ peripheral resistance
• Chronic drug admin. ↓ peripheral resistance
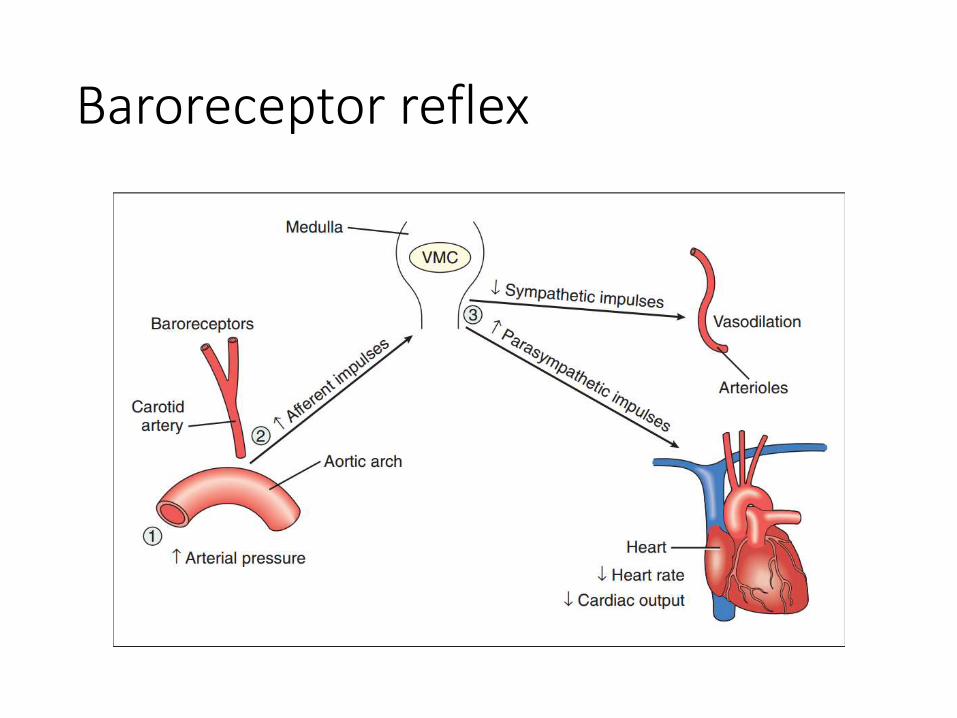
Baroreceptor reflex


Effect in an anaesthetized dog

Effect on respiratory tract
• Blockade of β2 rec. in bronchial smooth muscle ↑ airway resistance (asthma)
• Patients with chronic obstructive pulmonary disease (COPD) tolerate these drugs quite well & benefits outweigh the risks (Albouaini et al., 2007)
• Patients with COPD discharged with β-blockers after an MI had a lower all-cause mortality compared to patients not prescribed β-blockers (Andell et al., 2015) [JAHA, 2015]

Other effects
• Eye ↓ i.o.p. (glaucoma)
• Metabolic & Endocrine - inhibit SNS stimulation of lipolysis ↑ VLDL & ↓ HDL
• Sotalol Nonselective β-receptor antagonist that lacks LA action but has marked class III antiarrhythmic effects, reflecting K channel blockade

Clinical Pharmacology of β blockers
1. Hypertension
2. Ischemic heart disease (Angina, MI)
3. Cardiac arrhythmias
4. Heart failure
5. Glaucoma
6. Hyperthyroidism
7. Neurologic disease (Migraine, tremors, “stage fright”)
8. Miscellaneous (BOV)

Hypertension

β blocker
α blocker

β blocker
α blocker

α blocker
β blocker



• Atenolol Less lipophilic (fewer CNS s/e)
• Labetalol chr. HTN & HTN emergencies. Because of its α-adrenoceptor–blocking activity, it can cause orthostatic hypotension.
• Esmolol (i.v.) HTN in surgical patients & in persons with HTN emergencies
• Carvedilol Antioxidant properties that can protect the vascular wall from free radicals that damage blood vessels and thereby contribute to the progression of cardiovascular disease.
• Nebivolol (3rd gen.) selective β1-blocker with antioxidant properties; ↑ endothelial NO rel. (vasodilating effect)

Management of Hypertension
• Lifestyle Modifications exercise,wt. loss, mod. of alcohol intake & diet low in Na & adeq. K Ca Mg. Fruits & vegetables & low sat. & total fat.
• Selection of Drug Therapy
• Stage I HTN A+B (<55) ; C + D (>55)
• Stage II HTN 1 out of A/B + 1 out of C/D
• Step 3 A/B + C + D
• Step 4 (Resistant HTN) A + B + C + D

Ischemic heart disease

Rationale for use
• Typical angina pectoris and acute MI but NOT in vasospastic angina/acute anginal attacks.
• In typical angina Prevent exercise-induced tachycardia & ↓ MOD (myocardial O2 demand)
• Also prevent reflex tachycardia induced by either organic nitrates or DHPs CCBs
• Post-MI ↓ risk of recurrence & improve survival
• MI Metoprolol (i.v.) during the early phase of treatment, followed by oral maintenance therapy
• C/I HF late stage (-ve inotropic effect)

• Abrupt withdrawal of BB should not be done (ppt. angina attack & acute MI due to sudden ↑ sympathetic tone of heart; upregul. Of beta rec. (tapered over 2-3 days)]
• ↑ EDV & ↑ ejection time (↑ MOD) blunts beneficial effects of BB if used as a single drug therapy for angina

Additional use
• β-blockers protect the heart against the damage caused by ischemia and free radicals that may be formed during reperfusion of the coronary arteries when fibrinolytic drugs are used.

• Prophylaxis β-blocker/long-acting NO3/CCB
• β-blockers ↓ risk of MI & improve survival in SA
• UA Aspirin + β-blockers for patients with unstable
• VA CCB
• Angina & asthma CCB (relax bronch. sm. Musc.)
• angina & diabetes CCB/β1 blocker/3rd gen
• HF long-acting nitrate (angina prophylaxis)

β blocker + long-acting NO3 because:
(a) Tachycardia due to nitrate is blocked by β blocker.
(b) The tendency of β blocker to cause ventricular dilatation is counteracted by nitrate.
(c) The tendency of β blocker to reduce total coronary flow is opposed by nitrate.
Heart failure
• Exc. SNS Cardiac remodeling by :-
1. Tachycardia (β1 receptors) ↑ MOD
2. RAAS
3. Chr. Stim. of cardiac β rec. myocytehypertrophy & apoptosis Cardiac dilatation & ventricular wall thinning
4. ↑ cardiac cytokines (TNF α & Ils) induce myocyte hypertrophy and apoptosis Fibrosis & ventricular wall stiffness.
• β bl. ↓ exc. Sympath. Stimul. of heart (Mild to severe HF caused by LV systolic dysfunction)

Rationale in Heart failure (early)
1. Inhibition of the sympathetic stimulation of myocardium and cardiac remodelling
2. Suppression of the RAAS activation by decreasing the release of renin from renal juxtaglomerular cells
3. attenuation of oxidative stress and inflammation in myocardium.

• Carvedilol β1,β2, α1 (vd); antioxidant, antiinflmmatory and antiapoptotic (multiple-action neuroendocrine antagonist).
• Given in symptomatic HF without hypotension, pulmonary congestion, or AV block.
• A/E Bradycardia, worsening heart failure, and dizziness or light headedness (vd & ↓ BP)
• Started on low doses & then gradually ↑ (beneficial effects have a delayed onset of action & a/e occur immediately)
• Also, can lead to ↑ symptoms for 4 to 10 weeks before any improvement is noted


Arrhythmias
• The Class II antiarrhythmics are β-adrenoceptorantagonists (β-blockers) such as esmolol, metoprolol, and propranolol.
• Prevent & treat SVA* & ↓ ventricular ectopic depol. and sudden death in patients with MI
• Antiarrhythmic effects Inhibit sympathetic activation of cardiac automaticity and conduction (↓ HR, ↓ AVN conduction velocity & ↑ AVN refractory period)
SVA Supraventricular arrhythmias

• Esmolol Acute SVT/HTN during or immediately after surgery
• Metoprolol & Propranolol SVA & VA

Synopsis of β blockers
• Uses, A/E, C/I and drug interactions of non-selective β blockers (Propranolol prototype)
• Uses of partial agonists & other non-selective agents
• Uses of cardioselective β blockers
• Uses of 3rd generation β blockers
• Dosage forms & strengths of commonly used βblockers

Uses of Propranolol (THAPPAD)
1. Thyrotoxicosis & Tremors
2. HTN, HOCM, HF (Compensated)
3. Angina & Acute MI
4. Prophylaxis of migraine
5. Phaeochromocytoma (α blockers)
6. Anxiety & Arrhythmias
7. Dissecting aortic aneurysm
8. Digitalis toxicity

A/E of Propranolol (BBC Loses Viewers in Rochedale)
• Bradycardia
• Bronchoconstriction
• Claudication
• Lipids (LDL & TG ↑; HDL ↓)
• Vivid dreams & nightmares
• Negative ionotropic action
• Reduced sensitivity to hypoglycemia
• Tiredness & ↓ exercise capacity
• Cold hands and feet, worsening of PVD

Contraindications of Propranolol
• Don’t Prescribe Him Propranolol
1. Diabetes mellitus
2. Pulmonary diseases (Asthma, COPD)
3. Heart block, bradycardia
4. Prinzmetal’s angina
5. Peripheral vascular disease


Interactions
1. Additive depression of SAN & AV conduction with digitalis and verapamil cardiac arrest
2. Propranolol delays recovery from hypoglycaemia due to insulin and oral anti diabetics.
3. Phenylephrine, ephedrine in cold remedies ↑ BP
4. Indomethacin & other NSAIDs Attenuate anti-HTN action of β blockers.
5. Ppnl retards lidocaine metabolism
6. ↑ bioavailability of chlorpromazine by ↓ FPM

Partial agonistic (ISA) action
• Exhibited by Pindolol, Carteolol, Celiprolol and acebutolol
• Benefits are :-
1. Preferred in those prone to severe bradycardia (elderly patients; sick sinus) or with low cardiac reserve
2. Withdrawal less likely to exacerbate HTN/angina
3. Plasma lipid profile is not/less worsened.

Uses of other beta blockers
1. Pindolol HTN
2. Nadolol HTN, angina & prevent migraine, BOV
3. Timolol HTN, acute MI, glaucoma & prevent migraine
4. Levobunolol Glaucoma
5. Carteolol Glaucoma


Uses of cardioselective β blockers
• Acebutolol HTN and cardiac arrhythmias
• Atenolol HTN, angina & acute MI
• Esmolol HTN & acute SVT during surgery
• Metoprolol HTN, angina & acute MI
• Bisoprolol HTN
• Betaxolol HTN & POAG

α- and β-adrenoceptor antag.
• Carvedilol (β1,β2,α1) & has antioxidant activity:-
1. Inhibition of lipid peroxidation in myocardial membranes
2. Anti-oxidant (scavenging of free radicals)
3. Inhibition of neutrophil release of O2
4. Antiapoptotic properties (prevent myocyte death and reduce infarct size in persons with myocardial ischemia and Systolic HF)
• Carvedilol is also known as “third-generation β-blocker and neurohumoral antagonist,” (HTN, AMI, HF)

Baroreceptor reflex

• Labetalol (β1,β2,α1 blocker) HTN emergencies (i.v.)
• Nebivolol is a novel β1-selective antagonist
1. Promotes vasodilation via NO release from endothelial cells
2. Activates cardiac β3‐adrenergic receptors (protective mechanism against heart failure and myocardial ischemia–reperfusion injury)

Dosage forms & strengths• Atenolol (Tenormin): Oral, 25, 50, and 100mg tablets
• Bisoprolol (Zebeta): Oral, 5 and 10mg tablets
• Carvedilol (Coreg): Oral, 3.125, 6.25, 12.5, and 25mg tablets
• esmolol (Brevibloc): Intravenous, 10ml (10mg/ml) vials
• labetalol (Normodyne, Trandate): Oral, 100, 200, and 300mg tablets; 5 mg/ml in 20 and 40 ml vials
• metoprolol (lopressor, Toprol): Oral, 50 and 100mg tablets (metoprolol tartrate); 25, 50, 100, and 200mg extended‐release tablets (metoprolol succinate)
• Nebivolol (Bystolic): Oral, 2.5, 5, 10, and 20mg tablets
• Propranolol (Inderal): Oral, 10, 20, 40, 60, and 80mg tablets; 60, 80, 120, and 160 mg capsules (extended release); intravenous, 1mg/ml in 1 ml vials

Thank you
Old man (Mr . Propranolol) needs to change his glasses !!, he can read the large β Letters but he cant get a clear vision of their numbers Business man (Mr. Atenolol) Very hardworking. He focuses all the time on his One and only target ( β1 selective )Mr. carvidilol is young but he is far from the Flying Betas so he cant recognize their types ( Non selective). Also, Mr. Carvidilol likes to blow red cylindrical Gum .. this reminds you of something ? Blood vessels