clavicle fracture
DESCRIPTION
fraktur klavkulaTRANSCRIPT
Clavicle Fracture
INTRODUCTION
In children the clavicle fractures easily, but it almost invariably unites rapidly and without complications.
In adults this can be a much more troublesome injury.

EPIDEMIOLOGY
• In adults clavicle fractures 2.6–4 per cent. • Midshaft fractures 69–82 per cent, • Lateral fractures 21–28 per cent• Medial fractures 2–3 per cent

Anatomy• The clavicle is S-shaped• The first bone to ossify 5 week of gestation• It is widest at its medial end and thins laterally• The medial one-third protects:
– Brachial plexus– Subclavian and axillary vessels– Superior lung
• Ligament– Coracoclavicular – Trapezoid – Conoid– acromioclavicular

Mechanism of injury
• A fall on the shoulder• The outstretched hand – the outer fragment is pulled down by the weight
of the arm– the inner half is held up by the sternomastoid
muscle.

Clinical features• The arm is clasped to the chest to prevent
movement.• A subcutaneous lump may be obvious and
occasionally a sharp fragment threatens the skin
• A careful neurovascular examination to assess the integrity of neural and vascular elements
Imaging
• Radiographic analysis requires at least an anteroposterior view
• Another view with a 30 degree cephalic tilt.• CT scanning with three-dimensional
reconstructions to determine accurately the degree of shortening or for diagnosing a sternoclavicular fracture-dislocation
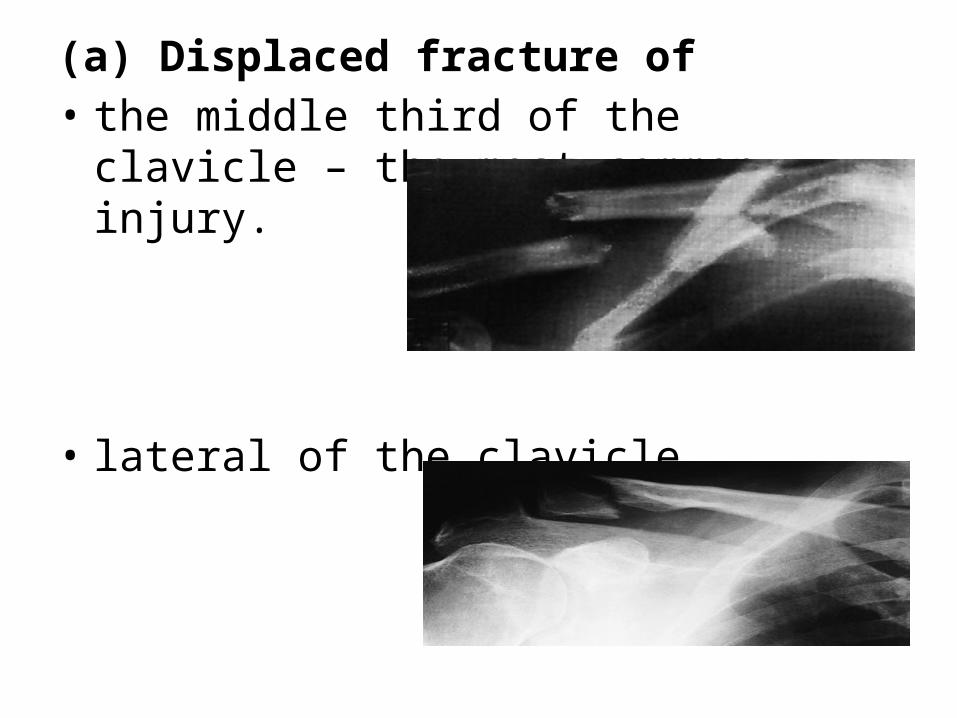
(a) Displaced fracture of• the middle third of the clavicle – the most
common injury.
• lateral of the clavicle
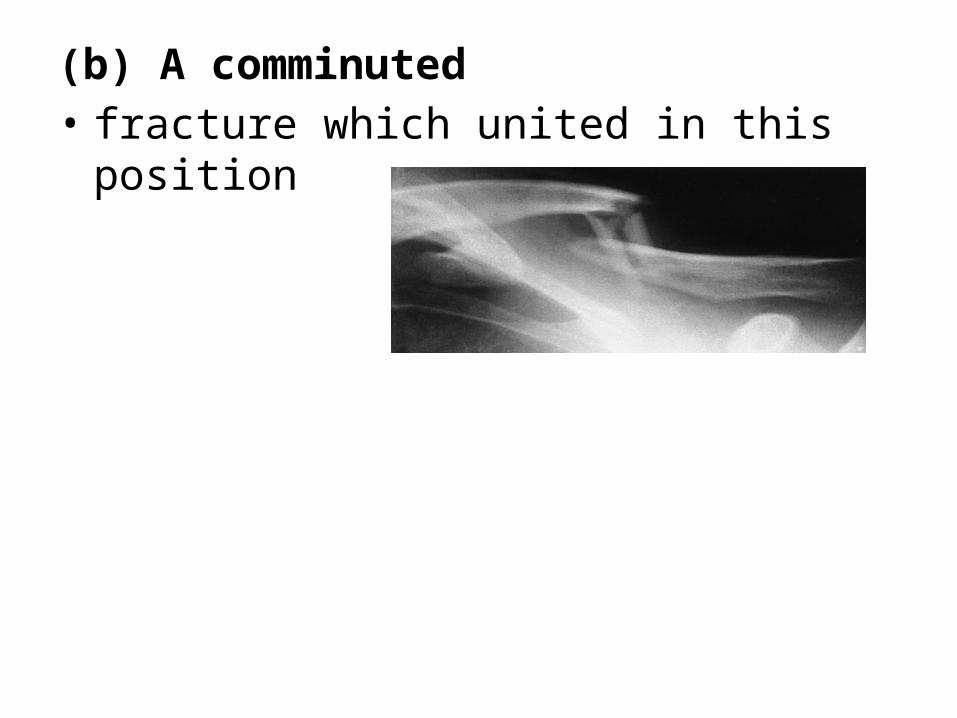
(b) A comminuted• fracture which united in this position

Classification
Classified on the basis of their location: • Group I (middle third fractures)• Group II (lateral third fractures)
(a) coracoclavicular ligaments intact(b) coracoclavicular ligaments are torn or detached
from the medial segment (c) factures which are intra-articular
• Group III (medial third fractures).

TREATMENT
• That undisplaced fractures Treated by non- operativel management: – applying a simple sling for comfort (1–3 weeks)– the traditional figure-of-eight bandage– the patient is then encouraged to mobilize the
limb as pain allows
MIDDLE THIRD FRACTURES
MIDDLE THIRD FRACTURES
• That displaced fractures by simple splintage:– shortening of more than 2 cm– risk of symptomatic mal-union– mainly pain – lack of power during shoulder movements– increased incidence of non-union.
Operative treatment:– acute clavicular fractures associated with severe
displacement.

LATERAL THIRD FRACTURES
non-operative management• Most lateral clavicle fractures are minimally
displaced and extra-articular• the coracoclavicular ligaments are intact
operative management– Displaced lateral third fractures are associated
with disruption of the coracoclavicular ligaments

Operative treatment
• Initial • K-wires• Suture and graft techniques• The newer locking plates.
Complication
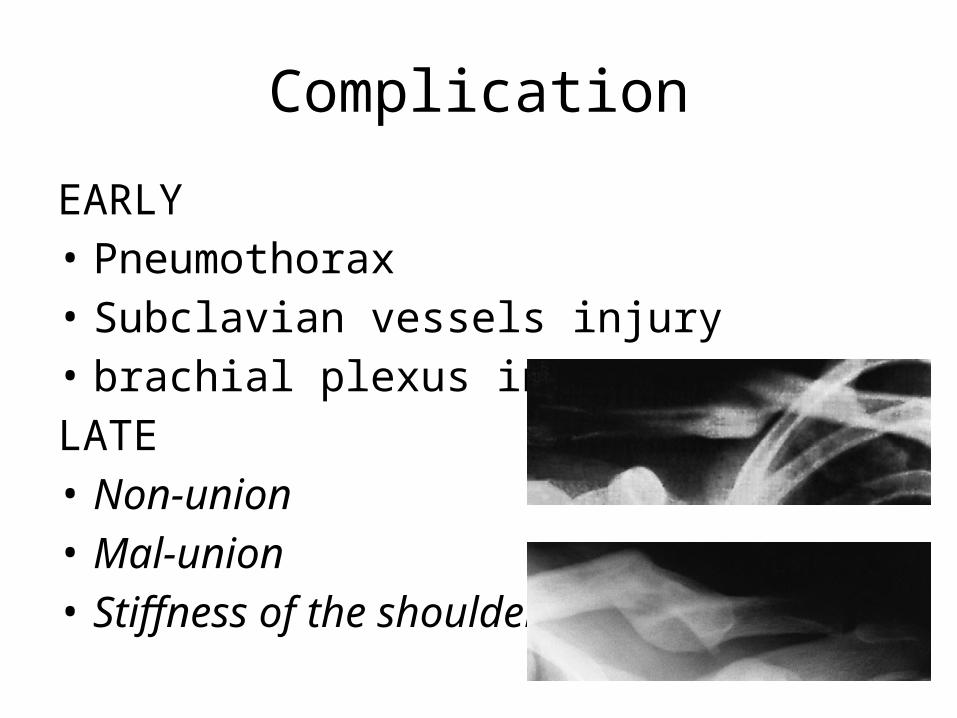
EARLY• Pneumothorax• Subclavian vessels injury • brachial plexus injuriesLATE• Non-union• Mal-union• Stiffness of the shoulder
Reference
• Koval, Kenneth J, Zuckerman Joseph D, Clavicle Fracture, Upper extremity fracture and dislocation,Handbook of fracture, Lippincot Williams & Wilkins, New York, 2006.
• Solomon, Louis, Fracture and joint injuries, Injury of the Shoulder, upper arm and elbow, Apley,s system of orthopaedics and fractures, Hodder Arnold, UK, 2010.