case - steven johnson's
TRANSCRIPT

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 1/72
Introduction
In 1922, Stevens and Johnson first described 2 patients, boys aged 7 and 8 years, with “an extraordinary,
generalized eruption with continued fever, inflamed buccal mucosa, and severe purulent conjunctivitis.” Both cases
were misdiagnosed by primary care physicians as hemorrhagic measles. Erythema multiforme (EM), originally
described by von Hebra in 1866, was part of the differential diagnosis in both cases, but it was excluded because of
the “character of skin lesions, the lack of subjective symptoms, the prolonged high fever, and the terminal heavy
crusting.” In spite of leukopenia in both cases, Stevens and Johnson in their initial report suspected an infectious
disease of unknown etiology as the cause.
In 1950, Thomas divided EM into 2 categories, as follows: erythema multiforme minor (von Hebra) and
erythema multiforme major (EMM; also known as Stevens-Johnson syndrome, or SJS). Since 1983, the eponym of
Stevens-Johnson syndrome had been used as a synonym for EMM.
Stevens-Johnson Syndrome is a rare disorder characterized by inflammation of the mucous membranes of
the mouth, throat, anogenital region, intestinal tract and membrane lining the eyelids (conjunctiva). Affected
individuals may have abnormalities (lesions) of the skin and mucous membranes that are purplish or red in color.
The abnormalities may be flat (macules) or small and raised (papules). In some cases, the lesions may develop
raised fluid-filled centers (bullae or blisters). Affected individuals may also have blisters and/or bleeding in the
mucous membranes of the lips, eyes, mouth, nasal passage, and genitals. In addition, abnormalities of the eyes
may develop as a result of the lesions caused by Stevens-Johnson Syndrome (ocular sequelae). Such abnormalities
may include infection of the delicate membrane of the eye and eyelids (conjunctiva) and inflammation associated
with an abnormal discharge from the conjunctiva (purulent conjunctivitis).

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 2/72
Some researchers believe that Stevens-Johnson Syndrome is a severe form of Erythema Multiforme, an
inflammatory disorder of the skin and mucous membranes (mucocutaneous) that is triggered by an allergic
reaction. Other researchers believe that Stevens-Johnson Syndrome is an independent syndrome. It is uncertain
exactly what causes the allergic reaction, but researchers think it may be triggered by an allergic reaction tocertain drugs such as antibiotics, including sulfonamides, tetracyclines, amoxicillin, and ampicillin. In some cases,
nonsteroidal anti-inflammatory medications and anticonvulsants, such as Tegretol and phenobarbitals, have also
been implicated. In some cases, it is also possible that the disorder may be triggered by an infection. 50% of the
cases are idiopathic..
Causes: Various etiologic factors (eg, infection, vaccination, drugs, systemic diseases, physical agents,
food) have been implicated as causes of SJS. Drugs most commonly are blamed. Recent reports linked SJS to the
use of drugs, rather than to other etiologic factors. Antibiotics are the most common cause of SJS, followed byanalgesics, cough and cold medication, nonsteroidal anti-inflammatory drug (NSAID), psycho-epileptics, and
antigout drugs. Other drugs also can be involved in the pathogenesis of SJS. Individuals with antigens human
leukocyte antigen Bw44 (HLA-Bw44), a part of human leukocyte antigen B12 (HLA-B12), and human leukocyte
antigen DQB1*0601 (HLA-DQB1*0601) appear to be more susceptible to developing SJS.
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 3/72
ObjectivesPatient Centered Objectives
To realize the significance of health in their lives
To obtain enlightenment on how to maintain health and prevent complications through health
edification
To put the knowledge that he has acquired into practice
To enthusiastically partake in medical care procedures and nursing interventions that would hasten
the healing process and expedite their recuperation
To manifest indications of positive changes in their current health situation
Nurse Centered Objectives
To establish rapport and rehabilitative affinity with the patient
To discern various health issues and problems of the patient who is the center of this study
To accustom ourselves with the definition, etiology, occurrence, diagnostics and management of
stevens-johnson’s disease
To master all the appropriate nursing interventions befitting stevens-johnson’s disease
To utilize the theoretical learning that we have acquired into actual setting particularly in this disease
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 4/72
Anatomy and Physiology of the IntegumentarySystem
The skin is the largest organ in the body: 12-15% of body weight, with a surface area of 1-2 meters.Skin is continuous with, but structurally distinct from mucous membranes that line the mouth, anus,urethra, and vagina. Two distinct layers occur in the skin: the dermis and epidermis. The basic cell type of the epidermis is the keratinocyte, which contain keratin, a fibrous protein. Basal cells are the innermostlayer of the epidermis. Melanocytes produce the pigment melanin, and are also in the inner layer of theepidermis. The dermis is a connective tissue layer under the epidermis, and contains nerve endings,sensory receptors, capillaries, and elastic fibers.
The integumentary system has multiple roles in homeostasis, including protection, temperatureregulation, sensory reception, biochemical synthesis, and absorption. All body systems work in aninterconnected manner to maintain the internal conditions essential to the function of the body.
Follicles and GlandsHair follicles are lined with cells that synthesize the proteins that form hair. A sebaceous gland (thatsecretes the oily coating of the hair shaft), capillary bed, nerve ending, and small muscle are associatedwith each hair follicle. If the sebaceous glands becomes plugged and infected, it becomes a skin blemish(or pimple). The sweat glands open to the surface through the skin pores. Eccrine glands are a type of sweat gland linked to the sympathetic nervous system; they occur all over the body. Apocrine glands are
the other type of sweat gland, and are larger and occur in the armpits and groin areas; these produce asolution that bacteria act upon to produce "body odor".
Hair and NailsHair, scales, feathers, claws, horns, and nails are animal structures derived from skin. The hair shaftextends above the skin surface, the hair root extends from the surface to the base or hair bulb. Geneticscontrols several features of hair: baldness, color, texture.Nails consist of highly keratinized, modified epidermal cells. The nail arises from the nail bed, which isthickened to form a lunula (or little moon). Cells forming the nail bed are linked together to form the nail.

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 5/72
Skin and HomeostasisSkin functions in homeostasis include protection, regulation of body temperature, sensory reception,water balance, synthesis of vitamins and hormones, and absorption of materials. The skin's primaryfunctions are to serve as a barrier to the entry of microbes and viruses, and to prevent water and
extracellular fluid loss. Acidic secretions from skin glands also retard the growth of fungi. Melanocytesform a second barrier: protection from the damaging effects of ultraviolet radiation. When a microbepenetrates the skin (or when the skin is breached by a cut) the inflammatory response occurs.Heat and cold receptors are located in the skin. When the body temperature rises, the hypothalamus sends a nerve signal to the sweat-producing skin glands, causing them to release about 1-2 liters of waterper hour, cooling the body. The hypothalamus also causes dilation of the blood vessels of the skin,allowing more blood to flow into those areas, causing heat to be convected away from the skin surface.When body temperature falls, the sweat glands constrict and sweat production decreases. If the bodytemperature continues to fall, the body will engage in thermiogenesis, or heat generation, by raising thebody's metabolic rate and by shivering.
Water loss occurs in the skin by two routes.
1. evaporation2. sweating
In hot weather up to 4 liters per hour can be lost by these mechanisms. Skin damaged by burns is lesseffective at preventing fluid loss, often resulting in a possibly life threatening problem if not treated.
Skin and Sensory ReceptionSensory receptors in the skin include those for pain, pressure (touch), and temperature. Deeper within
the skin are Meissner's corpuscles, which are especially common in the tips of the fingers and lips, andare very sensitive to touch. Pacinian corpuscles respond to pressure. Temperature receptors: more coldones than hot ones.
Skin and SynthesisSkin cells synthesize melanin and carotenes, which give the skin its color. The skin also assists in thesynthesis of vitamin D. Children lacking sufficient vitamin D develop bone abnormalities known as rickets.
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 6/72
Skin Is Selectively Permeable The skin is selectively soluble to fat-soluble substances such as vitamins A, D, E, and K, as well as steroid hormones such as estrogen. These substances enter the bloodstream through the capillary networks in
the skin. Patches have been used to deliver a number of therapeutic drugs in this manner. These includeestrogen, scopolamine (motion sickness), nitroglycerin (heart problems), and nicotine (for those trying toquit smoking).
Thick Skin The epidermis of thick skin follows the contours of the dermal ridges, producing the epidermal ridgesof the fingerprint. The dermal ridges penetrate into the epidermis as true papillae, and are separated byepithelial downgrowths called interpapillary pegs Five layers of cells or cell products are found in theepidermis: (1) stratum germinativum, columnar basal stem cells; (2) stratum spinosum, polyhedralcells with "spiny" projections: (3) stratum granulosum, diamond shaped cells containing keratohyalin
granules; (4) stratum lucidum, a clear, homogenous line composed of eleidin, a keratohyalintransformation product (not always seen); and (5) stratum corneum, the keratin filled squames
Dermis The dermis is composed of two layers: (1) the papillary dermis closest to the epithelium, is composedof less dense connective tissue and is vascularized with capillary networks penetrating the papillae and(2) the underlying reticular dermis composed of avascular, dense irregular connective tissue
Subcutaneous LayerBeneath the dermis, a layer composed of adipose and loose/dense connective tissues make of the
subcutaneous layer. Numerous structures are found in this layer. The secretory portion of the eccrinesweat glands are found here, with their ducts penetrating the dermis to enter the epidermis through theinterpapillary pegs Also, sensory structures (pacinian corpuscles), nerve bundles, blood vessels, and thebases of hair follicles are found in the subcutaneous layer.
Thin Skin The epidermis differs from that of thick skin in having thinner stratum spinosum, granulosum, andcorneum, and lacks the stratum lucidum . The dermis is not arranged in ridges, but does project into the

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 7/72
epidermis as true papillae. However, no epidermal ridges are produced The pigment of the skin isproduced by melanocytes, which take up residence in the basal layer (stratum germinativum) andproduce melanin or pigment granules .
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 8/72
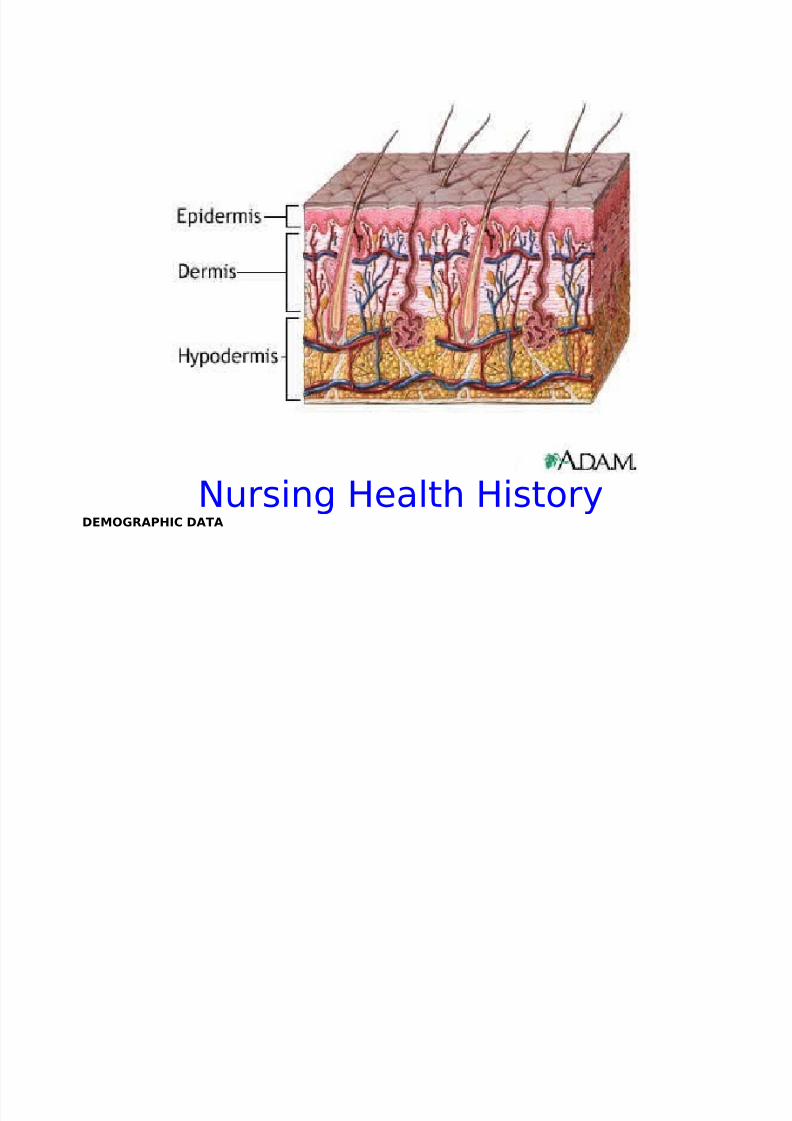
Nursing Health HistoryDEMOGRAPHIC DATA
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 9/72
Name: Bienvinido de LeonAge: 65 years oldBirthday: July 14, 1938Address: Blk. 1, San Jose, TarlacStatus: Married
Religion: Roman CatholicDOA: November 27, 2004 @ 8:49 amAttending Physician: Dr. Martinez
ADMITTING DIAGNOSIS: Psoriasis
REASON FOR SEEKING HEALTH CARE: Drowsiness, Chest Pain
HISTORY OF SEEKING HEALTH CARE
• On November 4, 2004, patient noted appearance of macules and lesions first on the extremities
then after a few days, it spread all over the body.• The rashes became very itchy.
• After few more days, patient’s skin became very scaly and the rashes turned brownish.• At about 7:30 in the morning of November 27, 2004, the patient complained of chest pain. Later on,
patient’s relatives noted difficulty of breathing with drowsiness. The condition persisted for 30 minutes. Hesought consultation at CLDH OPD, hence, was admitted.
PERCEPTION OF HEALTH STATUSRates himself as ( 2 )- Able to cope up with ADL’s
On a scale of 1 ( illness ) to ( 5 ) healthy• " Pakiramdam ko, para akong kandilang nauupos.”
• “Habang tumatagal kasi, pahina ako ng pahina.”
PREVIOUS ILLNESS, HOSPITALIZATION AND SURGERY • The patient has hypertension.
• He was not admitted to a hospital before. This was his first time.
• He had not undergone any major or minor surgery.

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 10/72
CLIENT-FAMILY MEDICAL HISTORY • The patient claimed that both his maternal and paternal side has hypertensive and cardiac disorders.
• He does not know any relative suffering from the disease same as his.
IMMUNIZATIONS and COMMUNICABLE DISEASES• The patient had his basic immunizations but not remember when and what kind.
• He had chickenpox, measles, mumps and pneumonia during his childhood and teenage years.
ALLERGIES• The client has no drug, food, or environmental allergies.
CURRENT MEDICATIONS
• Ulcepraz 40 mg. IVP OD
• Nootropil 1 gm. IVP every 8 hours
• Iselpin 1 gram 1 tab every 6 hours
• Laxoberal 1 tbsp. HS
• Imdur 60 mg. 1 tab OD
• Flagyl 500 mg. IV Infusion every 8 hours
• Moriamin Forte 1 tab TID
DEVELOPMENTAL LEVEL
Erik EriksonIntegrity vs. Despair
• He had viewed his life as meaningful and fulfilling.
• He had gone through a lot of hardships but through it all, he is happy that she was able tosurpass all of them.
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 11/72
•
Sigmund FreudAccording to Freud’s early theory, all behaviors are motivated by a desire to satisfy biological
needs and release of tension. Freud believed that gratification behavior is expressed primarily throughdifferent body zone (oral, anal, genital) at certain ages during the course of personality development. “ The goal of development is maximizing need gratification minimizing punishment and guilt usingdefenses to control anxiety. Freud’s theory stated unresolved gratification at a certain stage leads to afixation of development at that stage.
Genital Stage (15 years to adulthood)
• He has reached sexual maturity.
• He has developed an intimate relationship to his partner, who is also his sexual partner.
• He has a successful marriage and a happy family.
Jean PiagetFormal Operations (11+ years )
• The client is able to see relationships of objects, events and situations.
• He can reason in the abstract.
• He logically solves problems.
• Thinks scientifically and solves complex problems.
Lawrence KohlbergKohlberg’s model states that the person’s ability to make moral judgments in a behave and a
morally correct manner develops over a period of time. Kohlberg identified three levels of morality: apreconventional level, based on obedience or punishment; a conventional level when reasoning beginsto focus or more abstract principles of right or wrong rather than established moral truths
Level III: Postconventional
• He understands that it is wrong to violate others' rights.
• He follows laws and orders of the society.
• He respects the dignity of human beings as individuals.
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 12/72
• He has developed morality and ethics.
• His judgements are based on principles of justice.
• He lives by the saying that "Do to others as you would have them do to you."
Harry Stack Sullivan
Theorized that relationships with others influence how one’s personality develops. Approval anddisapproval from significant others influence the formation of one’s personality. To form satisfyingrelationships with others, an individual must complete six stages of development.
Late Adoloscence Has established an intimate and long lasting relationship with someone of the opposite sex.
Havighurst Theorized that there are 6 developmental stages of life, each with essential task to be achieved.
Mastery of task in one developmental stage is essential for mastery of tasks in subsequent stages.When a task in one stage is mastered, it is learned for life.
Stage of Late Maturity
• Adapted with his physiological changes and alterations in health status
• The client had adjusted to retirement.
• Has established satisfactory living arrangements
• ·
PSYCHOSOCIAL HISTORY The client’s usual source of stress includes several factors such as his job/ occupation and his
illness. However, he stated that he could easily cope up with these stresses as long as there are those
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 13/72
people who are close to him who are always there to support him. Specifically, these people compriseof his family especially his , wife, and his children. Best of all, he said that his family is a God fearingfamily.
VALUES and BELIEFS The client claimed that he believes in hilots , albularyos , tawas and pag-aatang ( offering of food sacrifices) mainly because of his social status and their background as a typical Filipino. He also saidthat he also resort to traditional/ herbal medicines (eg. Guava leaves) as their primary treatment.
As a Roman Catholic, he does not eat meat during Holy Week. He gives credence to God.
NUTRITION The client claimed that he has a good eating habit not until he became ill. He eats typical Filipino
food comprising mainly of vegetables, meat and rice. He eats more meat than fish and vegetables. Hesays he puts MSG in almost all their viands.
He drinks plenty of water, at least 7 glasses per day.
SLEEP PATTERN The client usually sleeps at around 8-9:00 in the evening and wakes up at around 5 in the
morning. When he became ill, he almost sleeps the entire day because of severe weakness.
RECREATION and HOBBIES The client usually spends his leisure time (free day) breeding chickens and training them for
“sabong”.
LIFE STYLE The client reported that he used to smoke around 10-15 sticks a day. He likewise stated that heis an occasional drinker.
ECONOMIC and SOCIO-CULTURAL DATAOur client is an elementary undergraduate of San JoseElementary School.He is a Kapampangan in ethnic affiliation.He belongs to the economic status letter B.
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 14/72
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 15/72
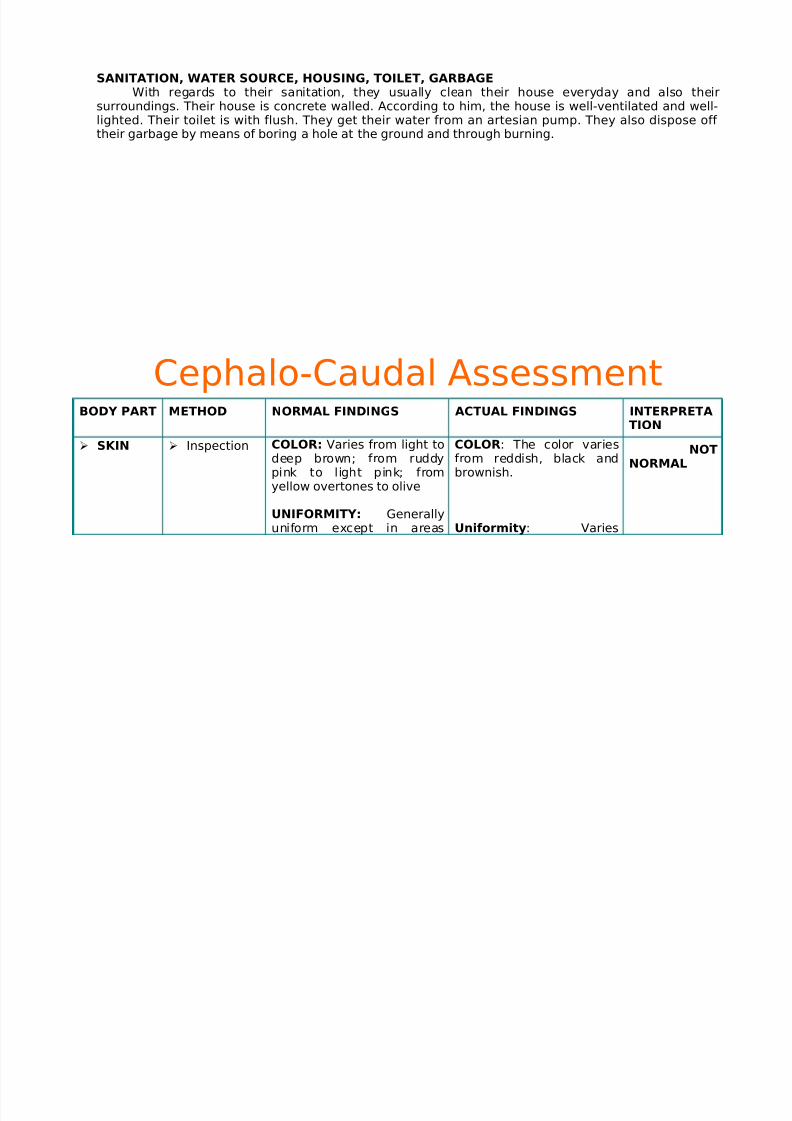
InspectionandPalpation
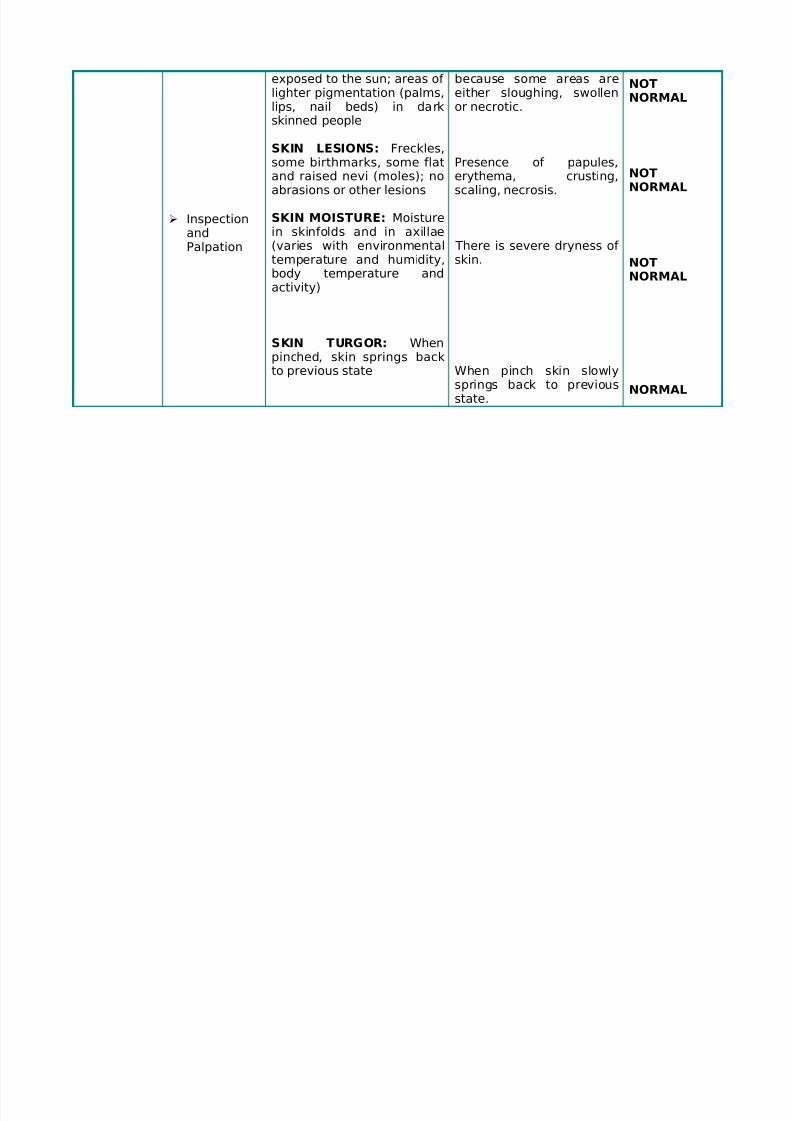
exposed to the sun; areas of lighter pigmentation (palms,lips, nail beds) in darkskinned people
SKIN LESIONS: Freckles,some birthmarks, some flatand raised nevi (moles); noabrasions or other lesions
SKIN MOISTURE: Moisturein skinfolds and in axillae(varies with environmentaltemperature and humidity,
body temperature andactivity)
SKIN TURGOR: Whenpinched, skin springs backto previous state
because some areas areeither sloughing, swollenor necrotic.
Presence of papules,erythema, crusting,scaling, necrosis.
There is severe dryness of skin.
When pinch skin slowlysprings back to previousstate.
NOTNORMAL
NOTNORMAL
NOT
NORMAL
NORMAL
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 16/72
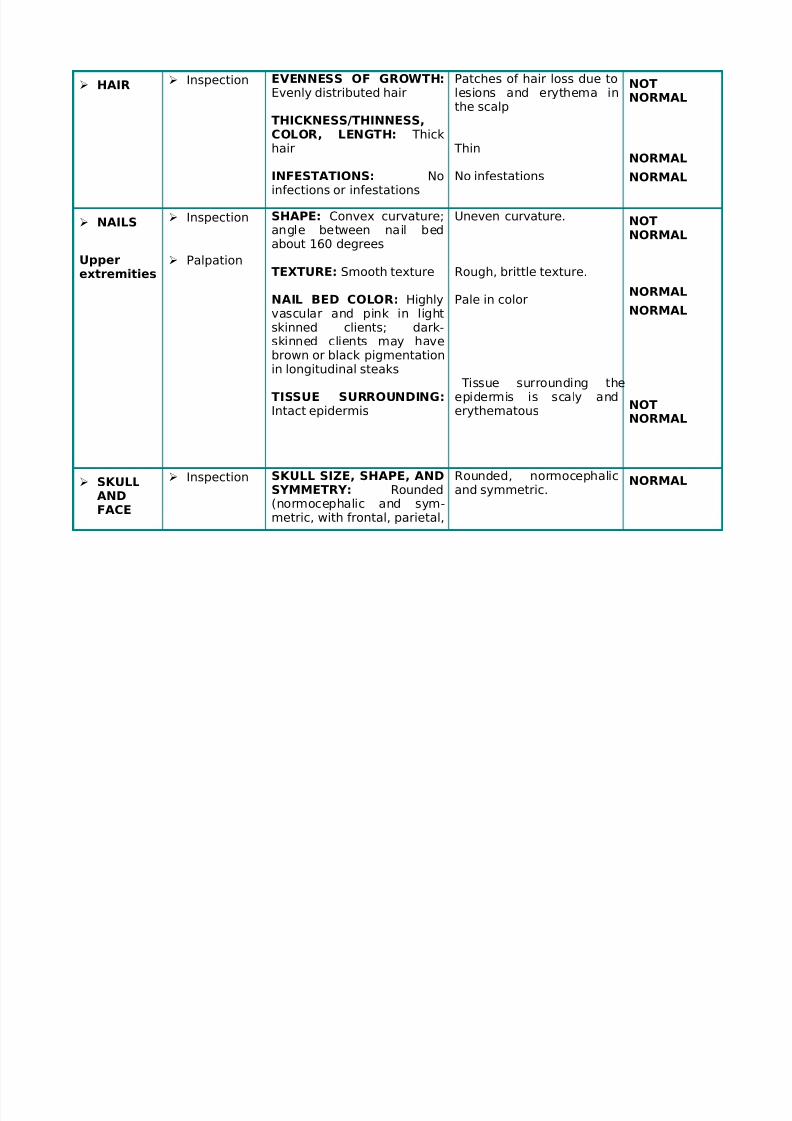
HAIR Inspection EVENNESS OF GROWTH:Evenly distributed hair
THICKNESS/THINNESS,
COLOR, LENGTH: Thickhair
INFESTATIONS: Noinfections or infestations
Patches of hair loss due tolesions and erythema inthe scalp
Thin
No infestations
NOTNORMAL
NORMAL
NORMAL
NAILS
Upper
extremities
Inspection
Palpation
SHAPE: Convex curvature;angle between nail bedabout 160 degrees
TEXTURE: Smooth texture
NAIL BED COLOR: Highlyvascular and pink in lightskinned clients; dark-skinned clients may havebrown or black pigmentationin longitudinal steaks
TISSUE SURROUNDING:
Intact epidermis
Uneven curvature.
Rough, brittle texture.
Pale in color
Tissue surrounding theepidermis is scaly and
erythematous
NOTNORMAL
NORMAL
NORMAL
NOT
NORMAL
SKULLANDFACE
Inspection SKULL SIZE, SHAPE, ANDSYMMETRY: Rounded(normocephalic and sym-metric, with frontal, parietal,
Rounded, normocephalicand symmetric.
NORMAL
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 17/72
Palpation
Inspection
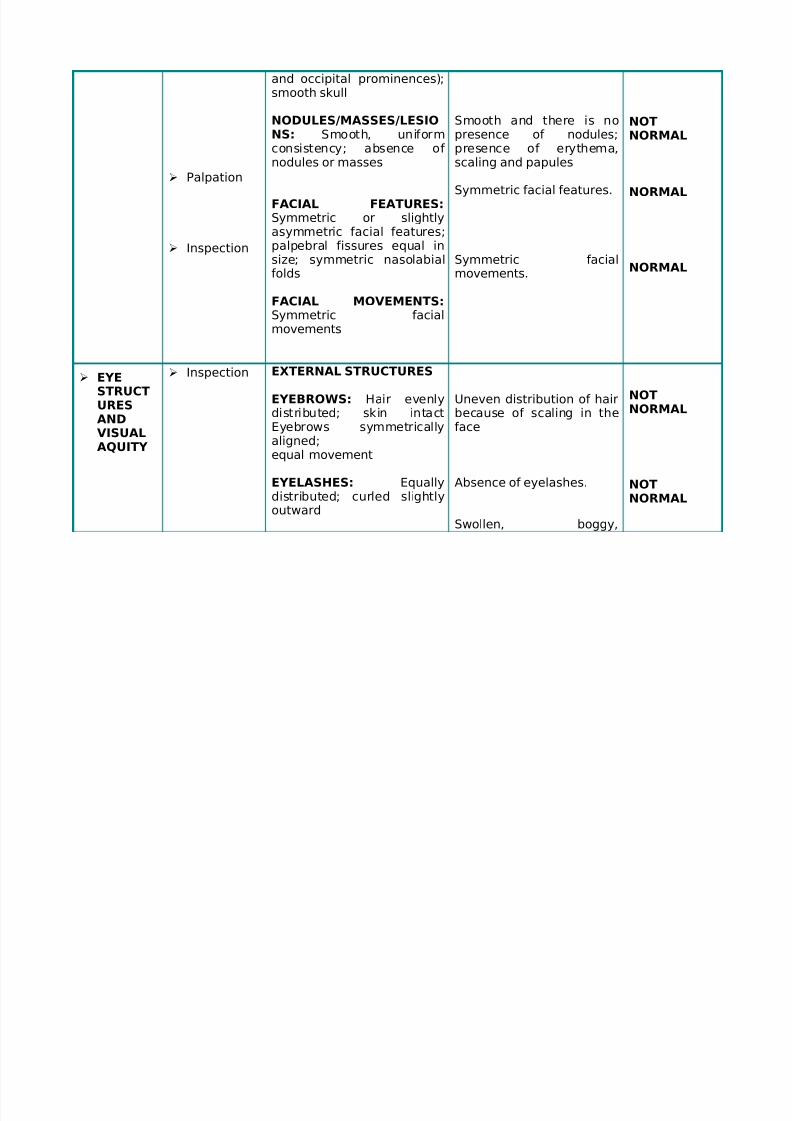
and occipital prominences);smooth skull
NODULES/MASSES/LESIO
NS: Smooth, uniformconsistency; absence of nodules or masses
FACIAL FEATURES:Symmetric or slightlyasymmetric facial features;palpebral fissures equal insize; symmetric nasolabial
folds
FACIAL MOVEMENTS:Symmetric facialmovements
Smooth and there is no
presence of nodules;presence of erythema,scaling and papules
Symmetric facial features.
Symmetric facial
movements.
NOT
NORMAL
NORMAL
NORMAL
EYESTRUCTURES
ANDVISUALAQUITY
Inspection EXTERNAL STRUCTURES
EYEBROWS: Hair evenly
distributed; skin intactEyebrows symmetricallyaligned;equal movement
EYELASHES: Equallydistributed; curled slightlyoutward
Uneven distribution of hair
because of scaling in theface
Absence of eyelashes.
Swollen, boggy,
NOTNORMAL
NOTNORMAL
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 18/72
Inspection
andPalpation
Inspection
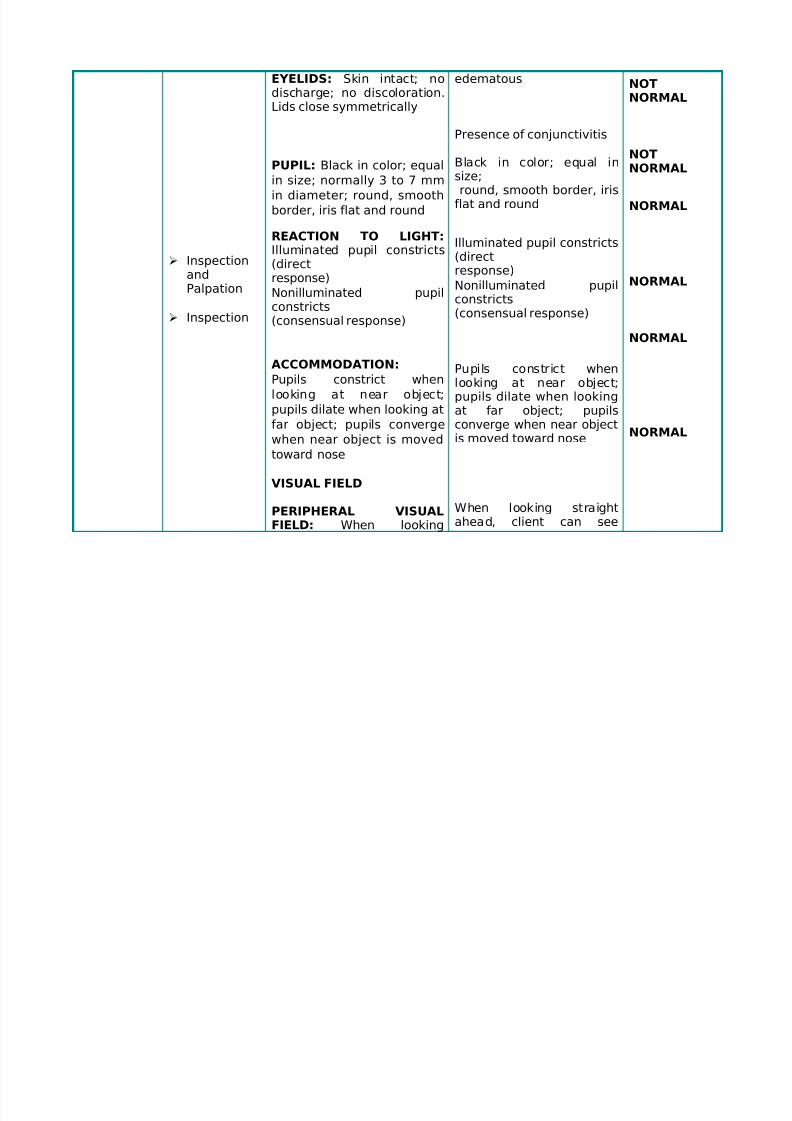
EYELIDS: Skin intact; nodischarge; no discoloration.Lids close symmetrically
PUPIL: Black in color; equal
in size; normally 3 to 7 mm
in diameter; round, smooth
border, iris flat and round
REACTION TO LIGHT:Illuminated pupil constricts(direct
response)Nonilluminated pupilconstricts(consensual response)
ACCOMMODATION:
Pupils constrict when
looking at near object;
pupils dilate when looking at
far object; pupils converge
when near object is moved
toward nose
VISUAL FIELD
PERIPHERAL VISUALFIELD: When looking
edematous
Presence of conjunctivitis
Black in color; equal insize;round, smooth border, iris
flat and round
Illuminated pupil constricts(directresponse)
Nonilluminated pupilconstricts(consensual response)
Pupils constrict whenlooking at near object;pupils dilate when looking
at far object; pupilsconverge when near objectis moved toward nose
When looking straightahead, client can see
NOTNORMAL
NOTNORMAL
NORMAL
NORMAL
NORMAL
NORMAL
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 19/72
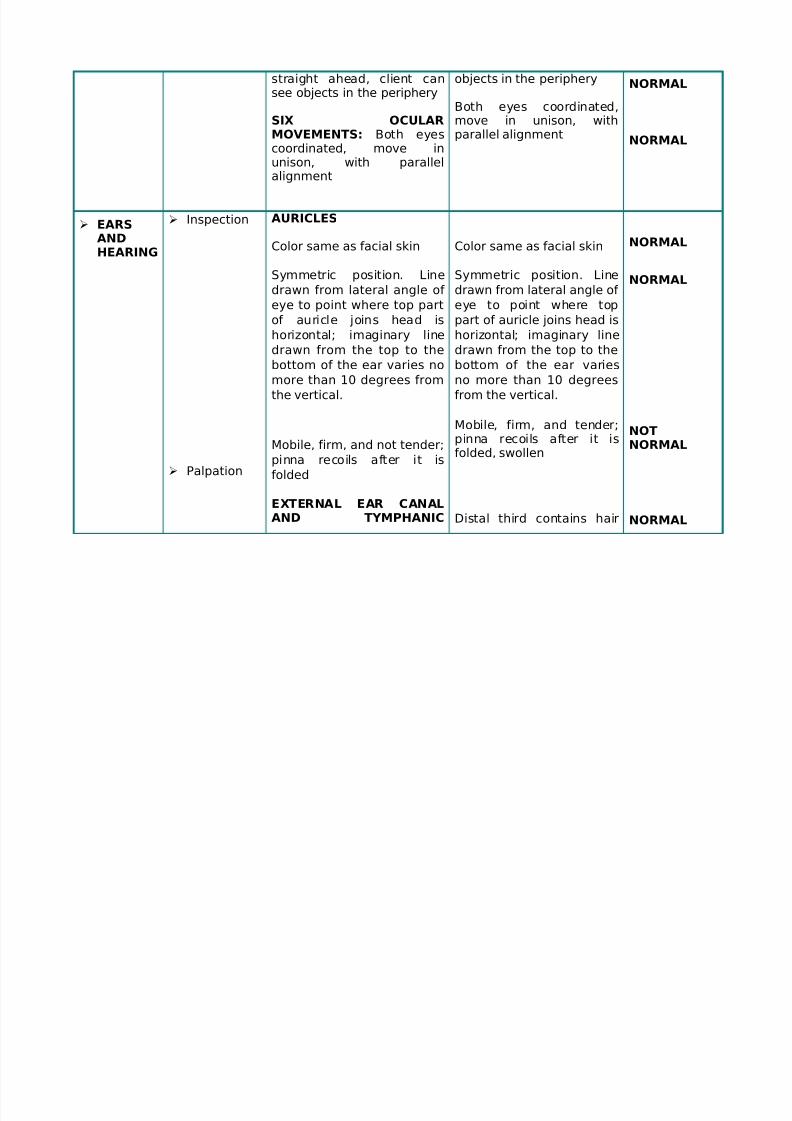
straight ahead, client cansee objects in the periphery
SIX OCULAR
MOVEMENTS: Both eyescoordinated, move inunison, with parallelalignment
objects in the periphery
Both eyes coordinated,move in unison, with
parallel alignment
NORMAL
NORMAL
EARSANDHEARING
Inspection
Palpation
AURICLES
Color same as facial skin
Symmetric position. Linedrawn from lateral angle of
eye to point where top part
of auricle joins head is
horizontal; imaginary line
drawn from the top to the
bottom of the ear varies no
more than 10 degrees from
the vertical.
Mobile, firm, and not tender;
pinna recoils after it is
folded
EXTERNAL EAR CANALAND TYMPHANIC
Color same as facial skin
Symmetric position. Linedrawn from lateral angle of
eye to point where top
part of auricle joins head is
horizontal; imaginary line
drawn from the top to the
bottom of the ear varies
no more than 10 degrees
from the vertical.
Mobile, firm, and tender;pinna recoils after it isfolded, swollen
Distal third contains hair
NORMAL
NORMAL
NOTNORMAL
NORMAL
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 20/72
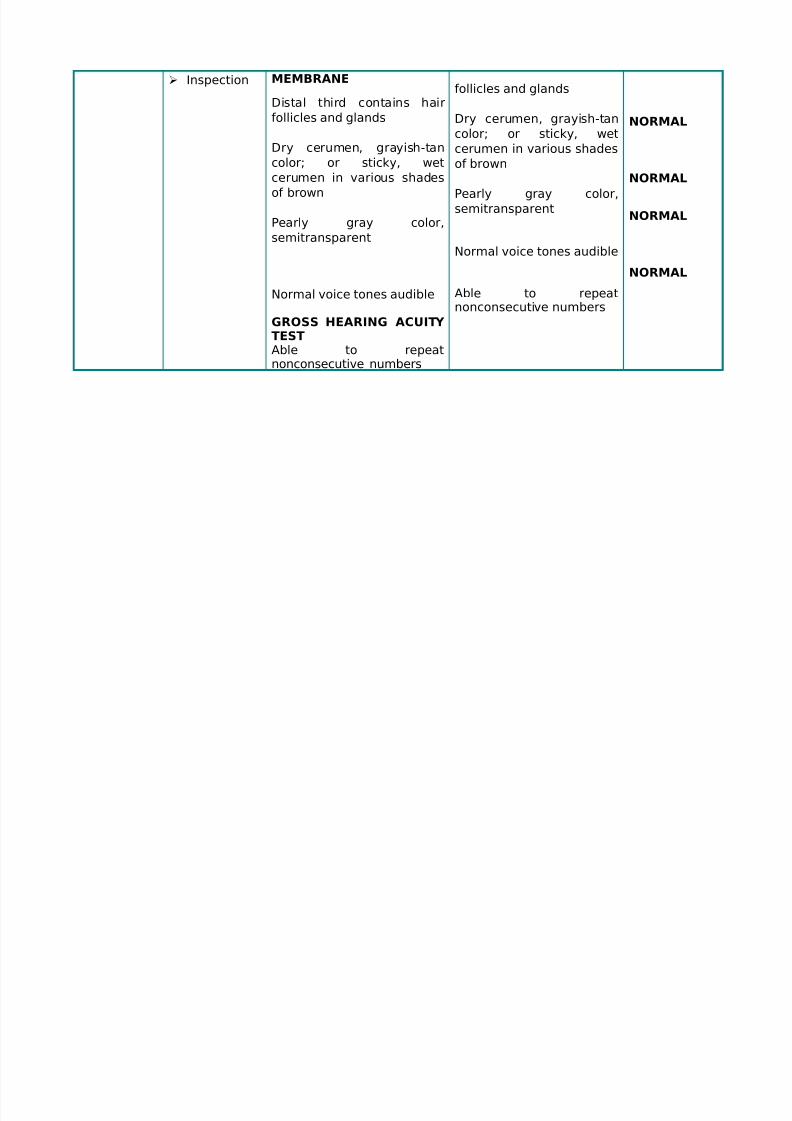
Inspection MEMBRANE
Distal third contains hair
follicles and glands
Dry cerumen, grayish-tan
color; or sticky, wet
cerumen in various shades
of brown
Pearly gray color,
semitransparent
Normal voice tones audible
GROSS HEARING ACUITY TESTAble to repeatnonconsecutive numbers
follicles and glands
Dry cerumen, grayish-tan
color; or sticky, wet
cerumen in various shades
of brown
Pearly gray color,
semitransparent
Normal voice tones audible
Able to repeatnonconsecutive numbers
NORMAL
NORMAL
NORMAL
NORMAL
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 21/72
NOSEANDSINUSES
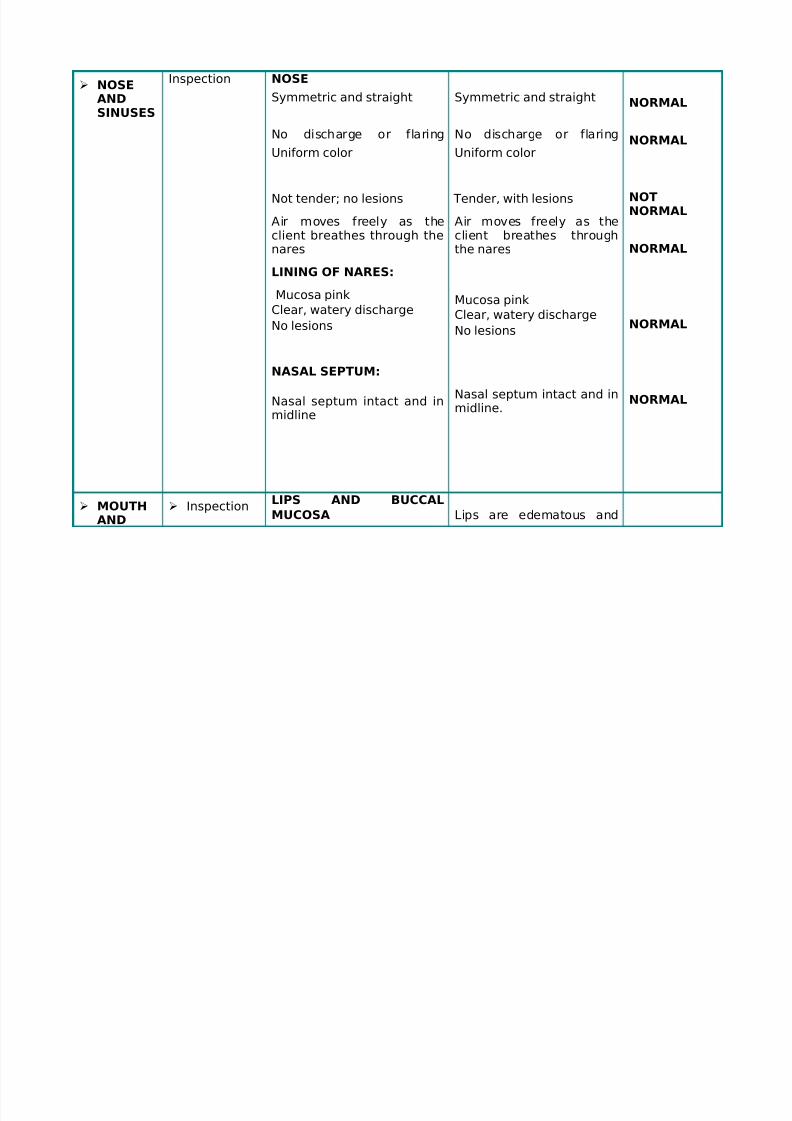
Inspection NOSE
Symmetric and straight
No discharge or flaring
Uniform color
Not tender; no lesions
Air moves freely as theclient breathes through thenares
LINING OF NARES:
Mucosa pink
Clear, watery discharge
No lesions
NASAL SEPTUM:
Nasal septum intact and in
midline
Symmetric and straight
No discharge or flaring
Uniform color
Tender, with lesions
Air moves freely as theclient breathes throughthe nares
Mucosa pink
Clear, watery discharge
No lesions
Nasal septum intact and inmidline.
NORMAL
NORMAL
NOTNORMAL
NORMAL
NORMAL
NORMAL
MOUTHAND
InspectionLIPS AND BUCCAL
MUCOSA Lips are edematous and

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 22/72
OROPHARYNX
InspectionandPalpation
Uniform pink color (darker,
eg, bluish hue, in
Mediterranean groups and
dark-skinned clients)
Soft, moist, smooth textureSymmetry of contour. Ability
to purse lips
INNER LIPS AND BUCCAL
MUCOSA
Uniform pink color (freckled
brown pigmentation in dark-
skinned clients)
TEETH AND GUMS
32 adult teeth
Smooth, white, shiny toothenamel
Pink gums (bluish or darkpatches in dark-skinnedclients) Moist, firm textureto gums
TONGUE/FLOOR OFMOUTH
swollen; unable to purse
lips
Reddish, swollen
Teeth appear to becomplete.
Smooth , and presence of tarry black regionsspecifically at the molarand pre molar region.
Gums have blackishdiscoloration specially atthe upper region of theoral cavity.
Not normal
Not NORMAL
NORMAL
NOTNORMAL
NOTNORMAL
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 23/72
Inspection
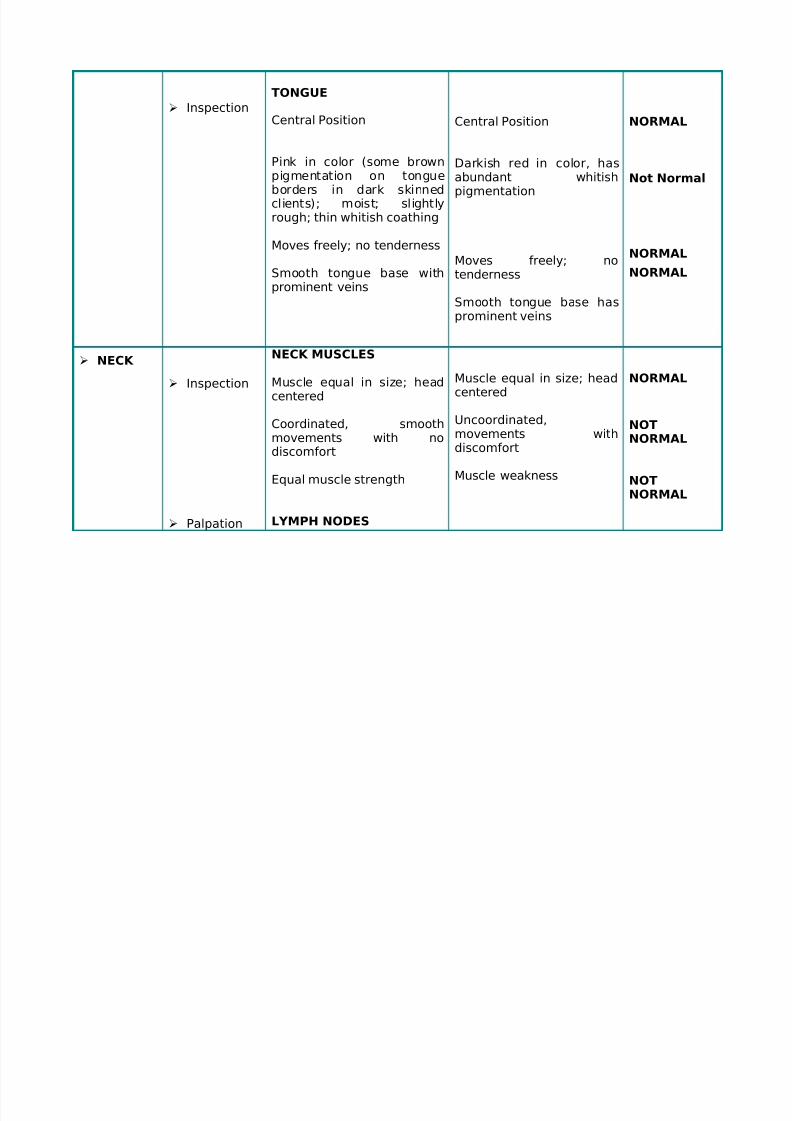
TONGUE
Central Position
Pink in color (some brownpigmentation on tongueborders in dark skinnedclients); moist; slightlyrough; thin whitish coathing
Moves freely; no tenderness
Smooth tongue base withprominent veins
Central Position
Darkish red in color, hasabundant whitishpigmentation
Moves freely; no
tenderness
Smooth tongue base hasprominent veins
NORMAL
Not Normal
NORMAL
NORMAL
NECK
Inspection
Palpation
NECK MUSCLES
Muscle equal in size; headcentered
Coordinated, smoothmovements with nodiscomfort
Equal muscle strength
LYMPH NODES
Muscle equal in size; headcentered
Uncoordinated,movements withdiscomfort
Muscle weakness
NORMAL
NOTNORMAL
NOTNORMAL
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 24/72
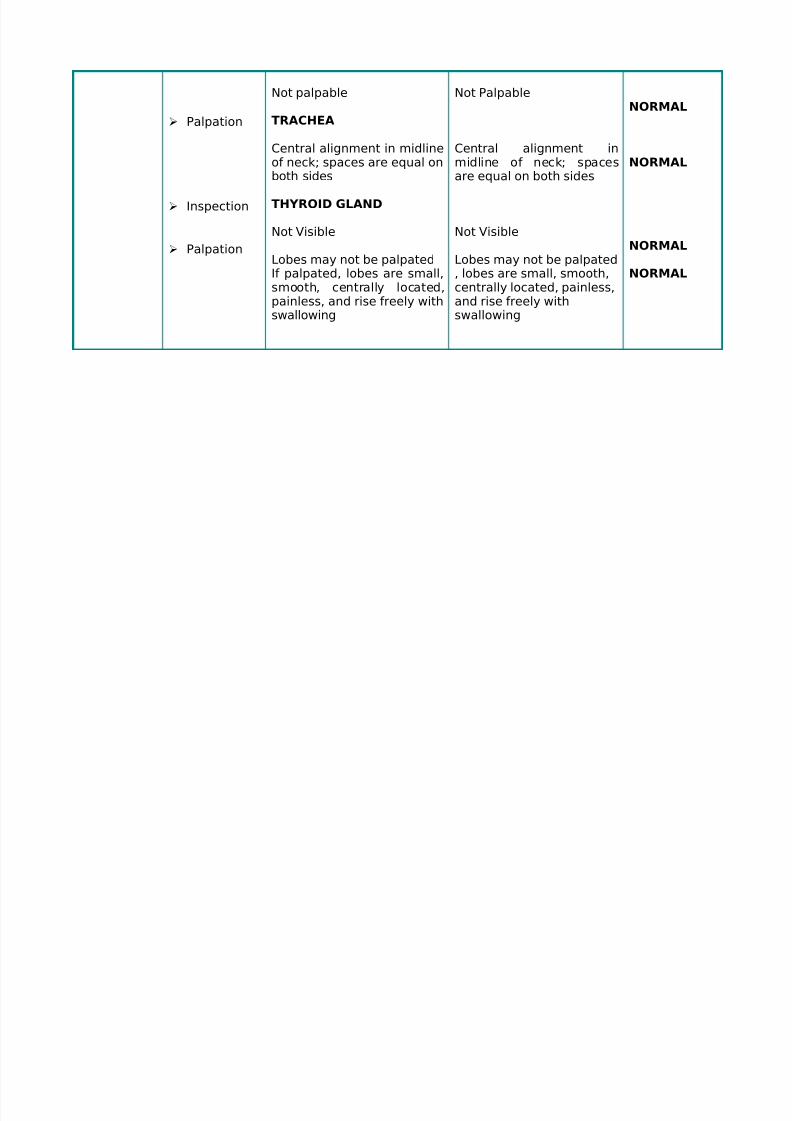
Palpation
Inspection
Palpation
Not palpable
TRACHEA
Central alignment in midlineof neck; spaces are equal onboth sides
THYROID GLAND
Not Visible
Lobes may not be palpated
If palpated, lobes are small,smooth, centrally located,painless, and rise freely withswallowing
Not Palpable
Central alignment inmidline of neck; spacesare equal on both sides
Not Visible
Lobes may not be palpated
, lobes are small, smooth,centrally located, painless,and rise freely withswallowing
NORMAL
NORMAL
NORMAL
NORMAL
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 25/72
THORAXANDLUNGS
Inspection
Palpation
Palpation
Percussion
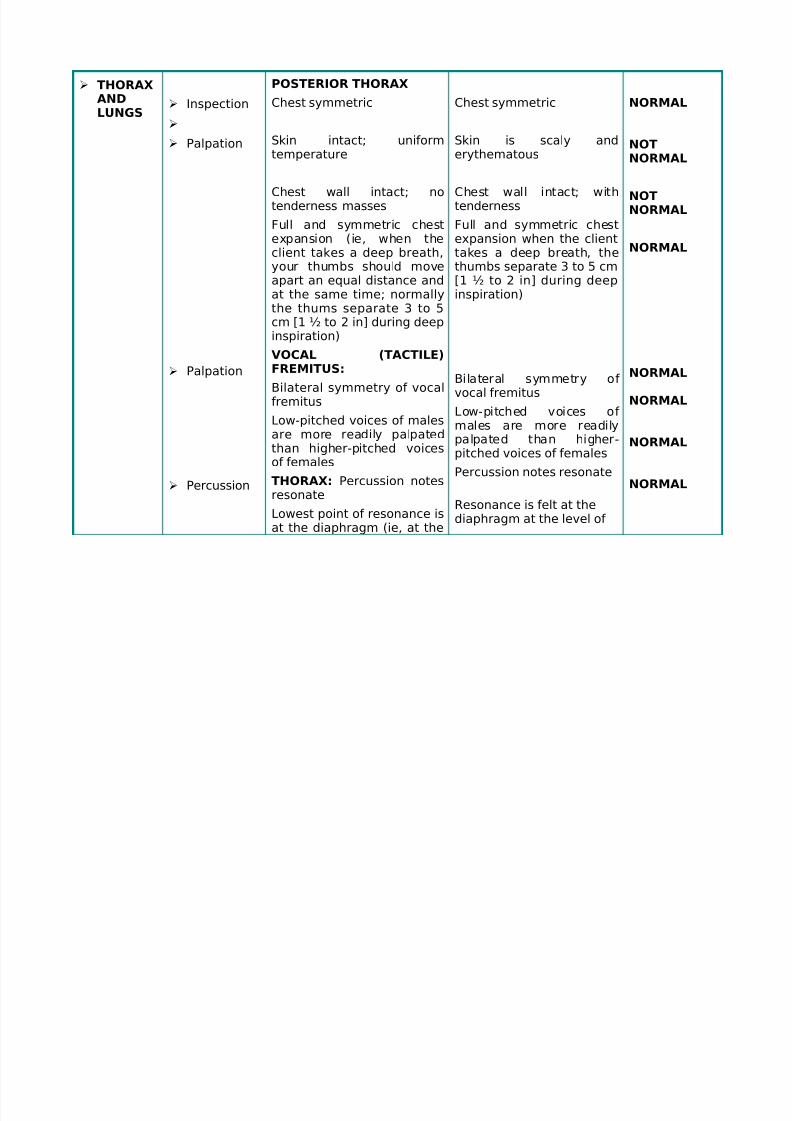
POSTERIOR THORAX
Chest symmetric
Skin intact; uniformtemperature
Chest wall intact; notenderness masses
Full and symmetric chestexpansion (ie, when theclient takes a deep breath,your thumbs should move
apart an equal distance andat the same time; normallythe thums separate 3 to 5cm [1 ½ to 2 in] during deepinspiration)
VOCAL (TACTILE)FREMITUS:
Bilateral symmetry of vocalfremitus
Low-pitched voices of malesare more readily palpatedthan higher-pitched voicesof females
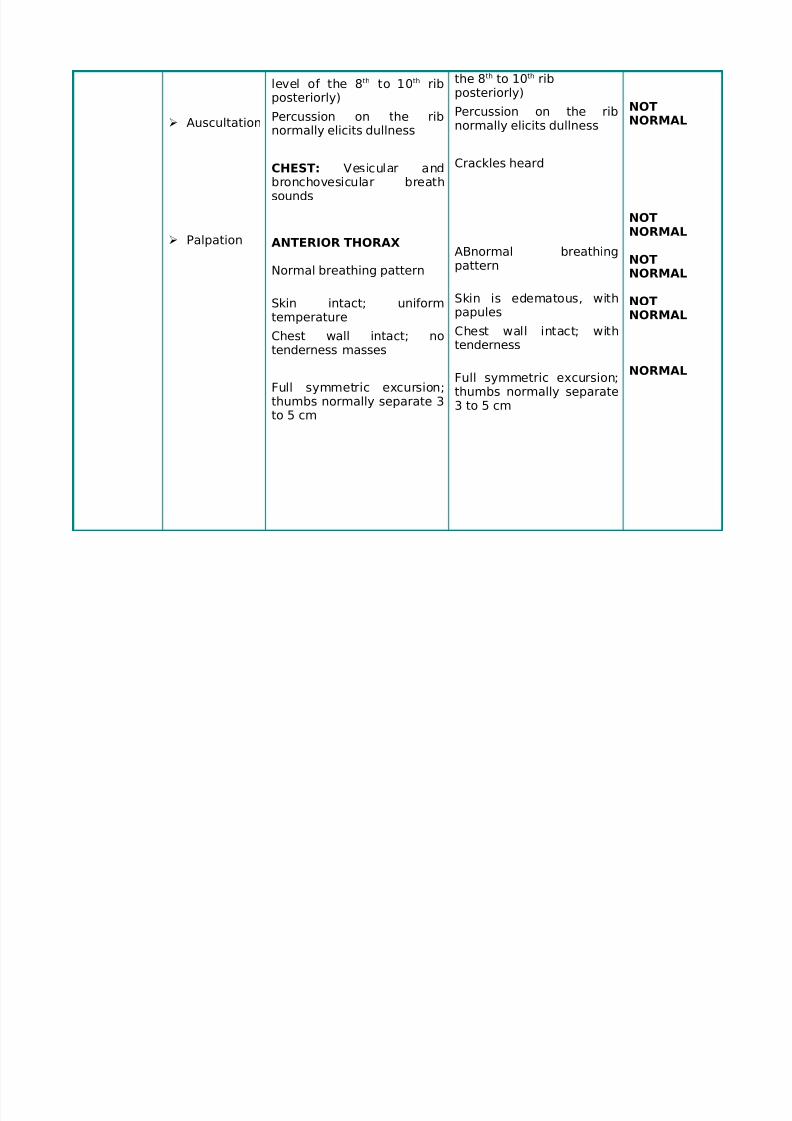
THORAX: Percussion notesresonate
Lowest point of resonance isat the diaphragm (ie, at the
Chest symmetric
Skin is scaly anderythematous
Chest wall intact; withtenderness
Full and symmetric chestexpansion when the clienttakes a deep breath, thethumbs separate 3 to 5 cm
[1 ½ to 2 in] during deepinspiration)
Bilateral symmetry of vocal fremitus
Low-pitched voices of males are more readilypalpated than higher-pitched voices of females
Percussion notes resonate
Resonance is felt at thediaphragm at the level of
NORMAL
NOTNORMAL
NOTNORMAL
NORMAL
NORMAL
NORMAL
NORMAL
NORMAL
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 26/72

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 27/72
ABDOMEN
Inspection There should be no lesions,nodules. It should be clear.
Skin is scaly and someparts are swollen andreddish
NOTNORMAL
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 28/72
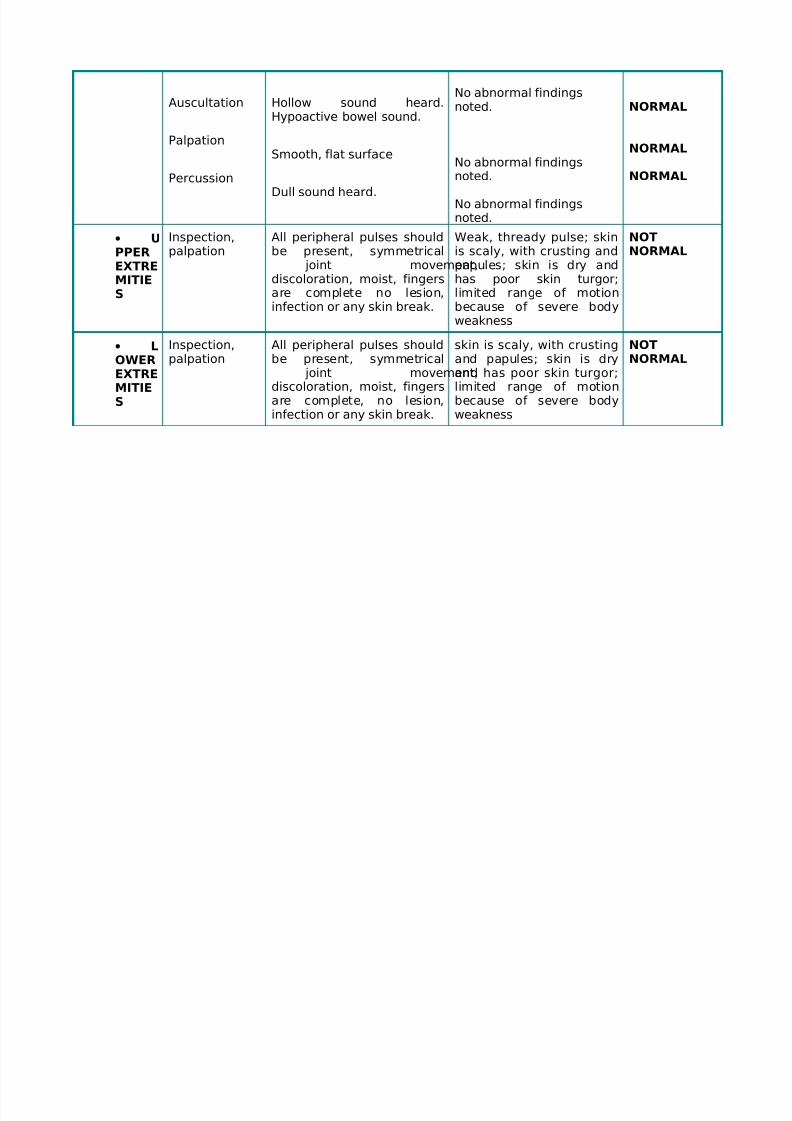
Auscultation
Palpation
Percussion
Hollow sound heard.Hypoactive bowel sound.
Smooth, flat surface
Dull sound heard.
No abnormal findingsnoted.
No abnormal findingsnoted.
No abnormal findingsnoted.
NORMAL
NORMAL
NORMAL
• UPPEREXTRE
MITIES
Inspection,palpation
All peripheral pulses shouldbe present, symmetrical
joint movement,
discoloration, moist, fingersare complete no lesion,infection or any skin break.
Weak, thready pulse; skinis scaly, with crusting andpapules; skin is dry and
has poor skin turgor;limited range of motionbecause of severe bodyweakness
NOTNORMAL
• LOWEREXTREMITIES
Inspection,palpation
All peripheral pulses shouldbe present, symmetrical
joint movement,discoloration, moist, fingersare complete, no lesion,
infection or any skin break.
skin is scaly, with crustingand papules; skin is dryand has poor skin turgor;limited range of motionbecause of severe body
weakness
NOTNORMAL
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 29/72
Review of Systems
PERIPHERAL PERFUSION
Patient is pale looking and appears weak.
The nails of upper and lower extremities are also pale in color; exhibits poor capillary refill
His blood study shows a low number of RBC, Hemoglobin and hematocrit
RESPIRATORY SYSTEM
Crackles auscultated.
Patient’s RR is 20 cpm.
Non-productive cough noted Difficulty of breathing noted
CARDIOVASCULAR SYSTEM
Patient’s BP is 140/80 mmHg & CR is 80 bpm.
His maternal and paternal side had a history of Hypertensive diseases and as well as havingheart diseases
GASTROINTESTINAL
The patient has no episodes of diarrhea.
Hypoactive bowel sounds
Constipation
Presence of erythema, rashes, scaling in the abdomen

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 30/72
MUSCULOSKELETAL
Has difficulty of moving because of weakness
The patient is unable to sustain ADLs and needs assistance and support
He also claimed that he has no muscle spasm or loss of sensation from his bony to muscularprominence
NEUROLOGIC
The patient in general felt weakness and felt a sense of uselessness
Exhibits no difficulty of hearing
Has slurred speech because of the inability of the lips to close
Reflexes are poor
GENITOURINARY
Exhibits normal micturation/voiding pattern.
Bowel movement was noted at the descending colon with characteristics of normal activity
No dysuria nor hematuria noted.
There is no pain reported during micturation and defacation
PERSONP• 65 year old male, married
• smoker (10-15 sticks a day)

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 31/72
• alcohol drinker
• lives with his familyPast History:- No surgeries- No hospitalizations
-History of chickenpox, mumps and measles (childhood years)
• Practicing, Devout Roman Catholic
• Expressed some concern over the prognosis of his disease whether he could still recover or not
E• Voiding with no difficulty
• Clear and yellow urine
• Voids in the bed using a bedpan
• Defecates with difficulty because he still has to exert effort
• No laxatives used at home
• Normoactive bowel sounds
• No distention or tenderness on palpation
R• No sleep aids used at home
• ROM limited on both upper and lower extremities
• Performs ADL's with difficulty due to severe weakness
S• RBC, Hgb and Hct lower than the normal range• Albumin lower than normal range
• Stool exam positive for occult blood
• With lesions, skin breaks and scaling on the entire body
• Normal liver, gallbladder, pancreas, spleen, kidneys as shown in the ultrasound
• Chest X-ray done: Impression: PTB Moderately advanced
O
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 32/72
• Crackles auscultated
• RR: 18 Breaths per minute
• With non productive cough
N• Soft diet because of swollen buccal mucosa
• States hospital food is "not bad at all"
• States that he is not "picky" with regards to foods
• Prefers to eat vegetables, meat and lots of rice
• Height: 5 feet 7 in.
• Weight: approx. 80 kg.
• Swollen lips and buccal mucosa
• Without dentures
• Redness in the gums
IDEAL Diagnostic and Laboratory Examinations Lab Studies:
• No laboratory studies (other than biopsy) exist that can aid the physician in establishing thediagnosis.
•
A complete blood count (CBC) may reveal a normal white blood cell (WBC) count or a nonspecificleukocytosis. A severely elevated WBC count indicates the possibility of a superimposed bacterialinfection.
• Determine renal function and evaluate urine for blood.
• Electrolytes and other chemistries may be needed to help manage related problems.
• Cultures of blood, urine, and wounds are indicated when an infection is clinically suspected.

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 33/72
Imaging Studies:
• Chest radiography may indicate the existence of a pneumonitis when clinically suspected. Otherwise,routine plain films are not indicated.
Other Tests:
• Skin biopsy is the definitive diagnostic study but is not an emergency department (ED) procedure.
o Skin biopsy demonstrates that the bullae are subepidermal.
o Epidermal cell necrosis may be noted.
o Perivascular areas are infiltrated with lymphocytes
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 34/72
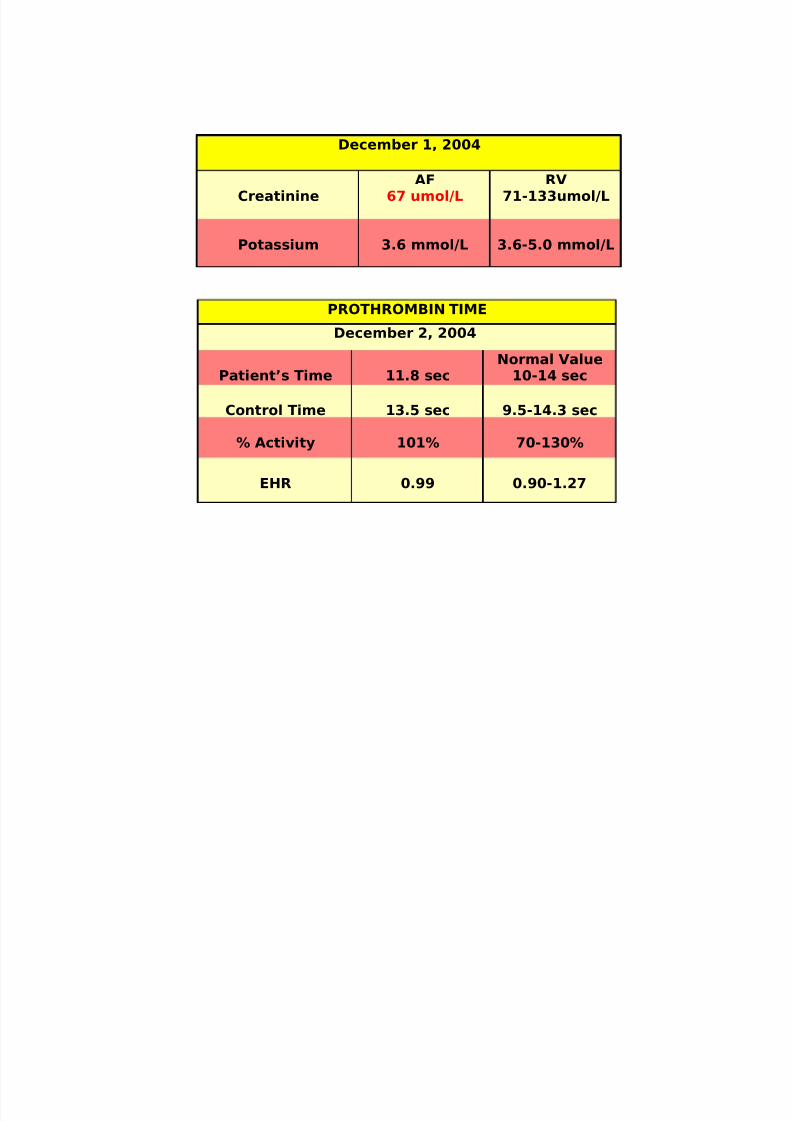
December 1, 2004
CreatinineAF
67 umol/LRV
71-133umol/L
Potassium 3.6 mmol/L 3.6-5.0 mmol/L
PROTHROMBIN TIME
December 2, 2004
Patient’s Time 11.8 secNormal Value
10-14 sec
Control Time 13.5 sec 9.5-14.3 sec
% Activity 101% 70-130%
EHR 0.99 0.90-1.27
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 35/72
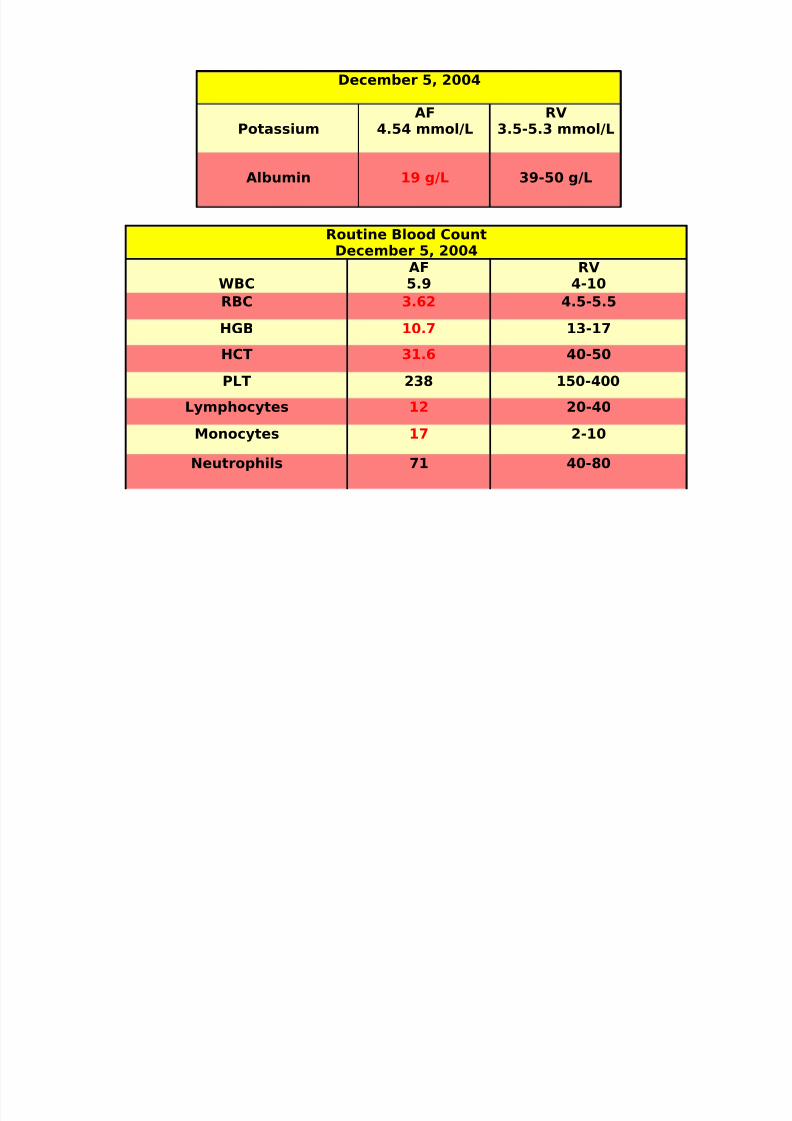
December 5, 2004
PotassiumAF
4.54 mmol/LRV
3.5-5.3 mmol/L
Albumin 19 g/L 39-50 g/L
Routine Blood CountDecember 5, 2004
WBC
AF
5.9
RV
4-10RBC 3.62 4.5-5.5
HGB 10.7 13-17
HCT 31.6 40-50
PLT 238 150-400
Lymphocytes 12 20-40
Monocytes 17 2-10
Neutrophils 71 40-80
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 36/72
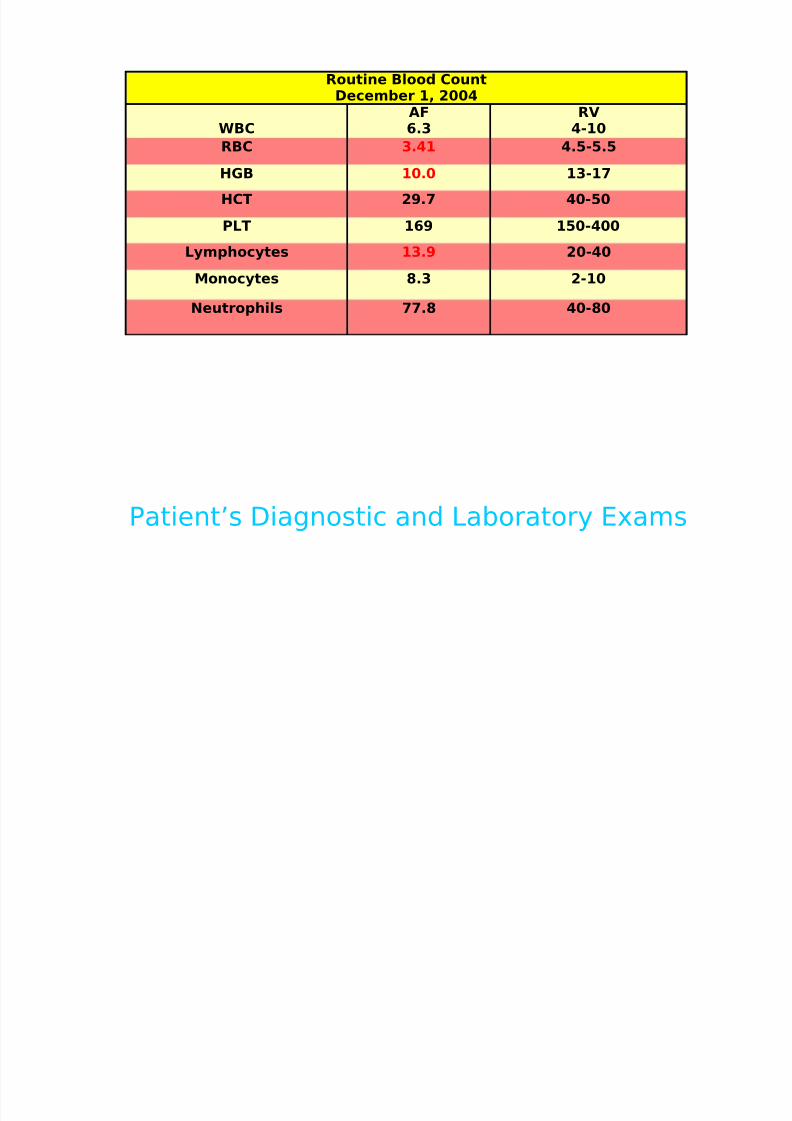
Routine Blood CountDecember 1, 2004
WBCAF6.3
RV4-10
RBC 3.41 4.5-5.5
HGB 10.0 13-17
HCT 29.7 40-50
PLT 169 150-400
Lymphocytes 13.9 20-40
Monocytes 8.3 2-10
Neutrophils 77.8 40-80
Patient’s Diagnostic and Laboratory Exams
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 37/72
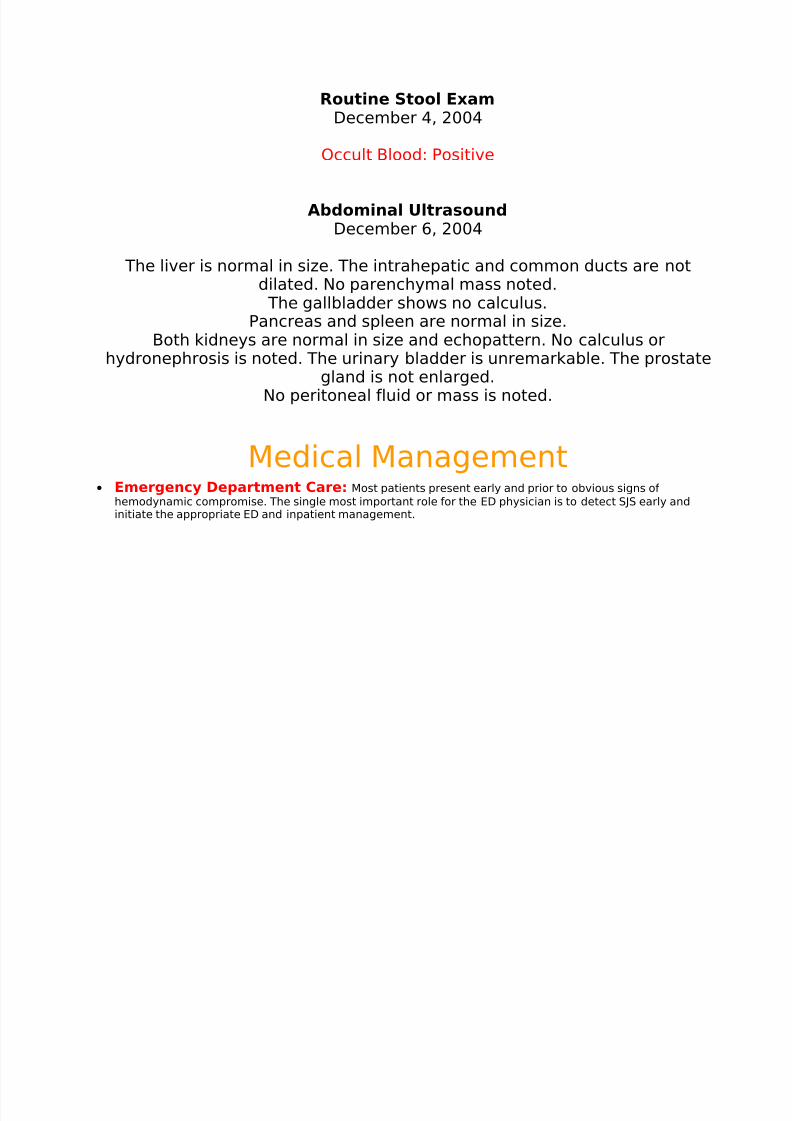
Routine Stool ExamDecember 4, 2004
Occult Blood: Positive
Abdominal UltrasoundDecember 6, 2004
The liver is normal in size. The intrahepatic and common ducts are not
dilated. No parenchymal mass noted. The gallbladder shows no calculus.
Pancreas and spleen are normal in size.Both kidneys are normal in size and echopattern. No calculus or
hydronephrosis is noted. The urinary bladder is unremarkable. The prostategland is not enlarged.
No peritoneal fluid or mass is noted.
Medical Management• Emergency Department Care: Most patients present early and prior to obvious signs of
hemodynamic compromise. The single most important role for the ED physician is to detect SJS early andinitiate the appropriate ED and inpatient management.

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 38/72
• Care in the ED must be directed to fluid replacement and electrolyte correction.
• Skin lesions are treated as burns.
• Patients with SJS should then be treated with special attention to airway and hemodynamic stability, fluid
status, wound/burn care, and pain control.
• Treatment of SJS is primarily supportive and symptomatic. Some have advocated cyclophosphamide,plasmapheresis, hemodialysis and immunoglobulin, but none of those should be considered standard atthis time.
o Manage oral lesions with mouthwashes.
o Topical anesthetics are useful in reducing pain and allowing the patient to take in fluids.
o
Areas of denuded skin must be covered with compresses of saline or Burow solution.
• Underlying diseases and secondary infections must be identified and treated. Offending drugs must bestopped.
• The use of systemic steroids is controversial. Some authors believe that they are contraindicated. Treatment with systemic steroids has been associated with an increased prevalence of complications.
• Address tetanus prophylaxis.
• Supportive systemic therapy: Management of patients with SJS usually is provided in ICUs or
burn centers. No specific treatment for SJS exists; therefore, most patients are treated symptomatically. Inprincipal, the symptomatic treatment of patients with SJS does not differ from the treatment for patientswith extensive burns.
o Fluid management is provided by macromolecules and saline solutions during the first 24 hours.

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 39/72
o After the second day of hospitalization, oral intake of fluids provided by nasogastric tube often isbegun, so that intravenous fluids can be tapered progressively and discontinued, usually in 2weeks.
o Massive parenteral nutrition is necessary as soon as possible to replace the protein loss and to
promote healing of cutaneous lesions.
o Intravenous insulin therapy may be required because of impaired glycoregulation.o Patients with SJS are at a high risk of infection. Sterile handling and/or reverse-isolation nursing
techniques are essential to decrease the risk of nosocomial infection.o Cultures of blood, catheters, gastric tubes, and urinary tubes must be performed regularly.o Because of the association between SJS and sulfonamides, avoid the use of silver sulfadiazine,
commonly used in burn units; instead, use another antiseptic, such as 0.5% silver nitrate or 0.05%chlorhexidine, to paint and bathe the affected skin areas.
o Prophylactic systemic antibiotics are not recommended.o The diagnosis of sepsis is difficult. Carefully consider the decision to administer systemic
antibiotics. The first signs of infection are an increase in the number of bacteria cultured from theskin, a sudden drop in fever, and deterioration of the patient's condition, indicating the need forantibiotic therapy. The choice of antibiotic usually is based on the bacteria present on the skin.Because of impaired pharmacokinetics, similar to that present in burn patients, the administrationof high doses may be required to reach therapeutic levels. Monitoring the serum levels is necessaryto adjust the dosage.
o Environmental temperature raised to 30-32°C reduces caloric loss through the skin. Fluidized airbeds are recommended if a large portion of the skin on the patient's backside is involved. Heatshields and infrared lamps are used to help reduce heat loss.
o Anticoagulation with heparin for the duration of hospitalization is recommended. Antacids reduce
the incidence of gastric bleeding.o Pulmonary care includes aerosols, bronchial aspiration, and physical therapy. Tranquilizers are usedto the extent limited by respiratory status.
o Several skin care approaches have been described. Extensive debridement of nonviable epidermis,followed by immediate cover with biologic dressings, such as porcine cutaneous xenografts,cryopreserved cutaneous allografts, and amnion- or collagen-based skin substitutes, are among therecommended treatments. Leaving the involved epidermis that has not yet peeled off in place andusing biologic dressings only on raw dermis also has been recommended. Skin allotransplantationreduces pain, minimizes fluid loss, improves heat control, and prevents bacterial infection.Hyperbaric oxygen also can improve healing.
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 40/72
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 41/72
• Treatment of chronic ocular manifestations
o In the case of mild chronic superficial keratopathy, long-term lubrication may be sufficient. Inaddition to lubrication, some patients may require a cosmetically acceptable long-term lateraltarsorrhaphy. The visual rehabilitation in patients with severe ocular involvement resulting in
profound dry eye syndrome with posterior lid margin keratinization, limbal stem cell deficiency,persistent epithelial defects with subsequent corneal neovascularization, and frank corneal opacitywith surface conjunctivalization and keratinization, is difficult and often frustrating for both thepatient and the physician. A close, usually long-term, relationship between the patient and thephysician needs to be established to achieve the best possible result.
o Removal of keratinized plaques from posterior lid margins, along with mucous membrane grafting,is usually the first step and one of the most important determining factors for future success of corneal surgeries. Preferably, a skilled oculoplastic surgeon with specific experience on patientswith SJS should perform this procedure.
• Subsequently, limbal stem cell transplantation with superficial keratectomy removing conjunctivalized orkeratinized ocular surface can follow. Patients with persistent corneal opacity require lamellar orpenetrating keratoplasty in the next step. To preserve corneal clarity after the visual reconstruction, along-term use of gas permeable scleral contact lenses may be necessary to protect the ocular surface.Long-term management frequently involves treatment of trichitic lashes and/or eyelid margin repair fordistichiasis or entropion. If the ocular surface repeatedly fails to heal upon multiple surgical interventions,keratoprosthesis may be considered as the procedure of last resort.
Clinical Manifestations• Ocular symptoms
o Red eye
o Tearing
o Dry eye
o Pain
o Blepharospasm
o Itching
o Grittiness
o Heavy eyelid
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 42/72
o Foreign bodysensation
o Decreased vision
o Burn sensation
o Photophobia
o Diplopia
Physical:
• External examination
o Conjunctival hyperemia (ie, red eye)
o Entropion
o Skin lesions
o Nasal lesions
o Mouth lesions
o Discharge (ie, catarrhal, mucous, membranous
• Typically, the disease process begins with a nonspecific upper respiratory tract infection.
o This usually is part of a 1- to 14-day prodrome during which fever, sore throat, chills, headache, andmalaise may be present.
o Vomiting and diarrhea are occasionally noted as part of the prodrome.
• Mucocutaneous lesions develop abruptly. Clusters of outbreaks last from 2-4 weeks. The lesions aretypically nonpruritic.
• A history of fever or localized worsening should suggest a superimposed infection; however, fever hasbeen reported to occur in up to 85% of cases.

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 43/72
• Involvement of oral and/or mucous membranes may be severe enough that patients may not be able toeat or drink.
• Patients with genitourinary involvement may complain of dysuria or an inability to void.
• A history of a previous outbreak of SJS or of erythema multiforme may be elicited. Recurrences may occurif the responsible agent is not eliminated or if the patient is reexposed.
• Typical symptoms are as follows:
o Cough productive of a thick purulent sputum
o Headache
o Malaise
o Arthralgia
• The rash can begin as macules that develop into papules, vesicles, bullae, urticarial plaques, or confluenterythema.
o The center of these lesions may be vesicular, purpuric, or necrotic.
o The typical lesion has the appearance of a target. The target is considered pathognomonic.
o Lesions may become bullous and later rupture, leaving denuded skin. The skin becomes susceptibleto secondary infection.
o Urticarial lesions typically are not pruritic.
o Infection may be responsible for the scarring associated with morbidity.
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 44/72
o Although lesions may occur anywhere, the palms, soles, dorsum of hands, and extensor surfacesare most commonly affected.
o The rash may be confined to any one area of the body, most often the trunk.
o Mucosal involvement may include erythema, edema, sloughing, blistering, ulceration, and necrosis.
• The following signs may be noted on examination:
o Fever
o Orthostasis
o Tachycardia
o
Hypotension
o Altered level of consciousness
o Epistaxis
o Conjunctivitis
o Corneal ulcerations
o
Erosive vulvovaginitis or balanitis
o Seizures, coma
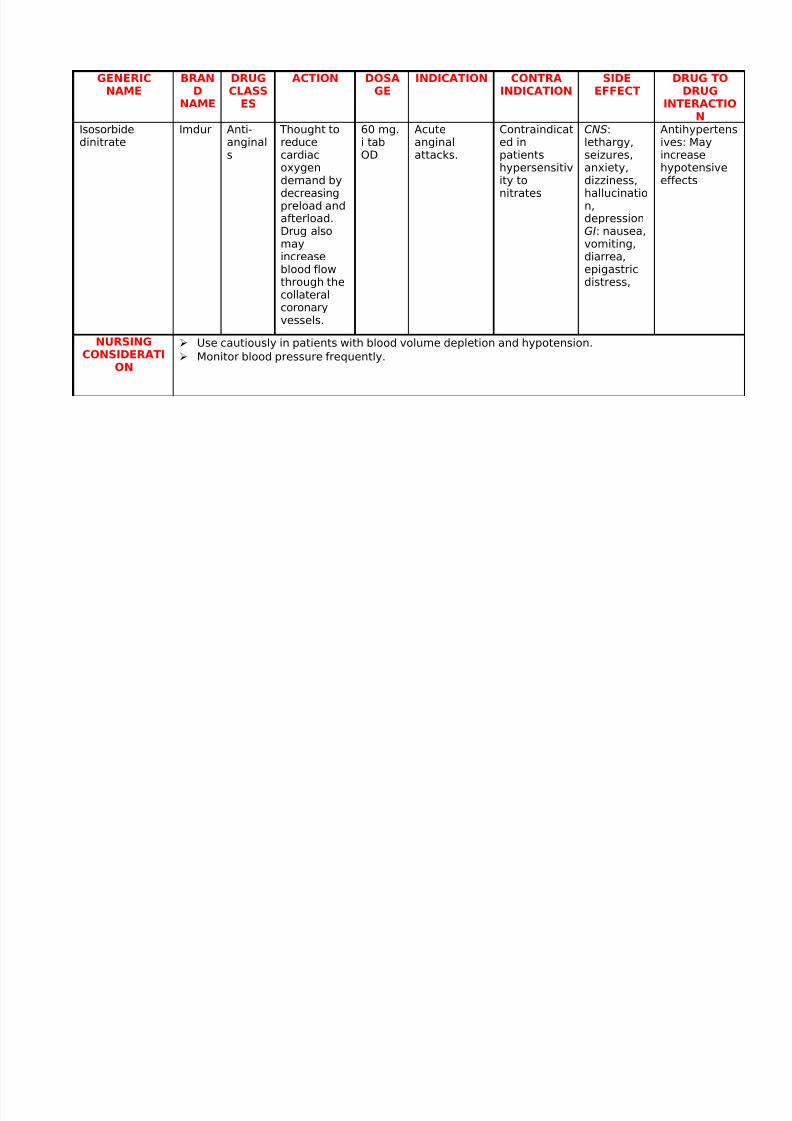
Drug StudyGENERICNAME BRAND
NAME
DRUGCLASSES
ACTION DOSAGE INDICATION CONTRAINDICATION SIDEEFFECT DRUG TODRUGINTERACTIO
N
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 45/72
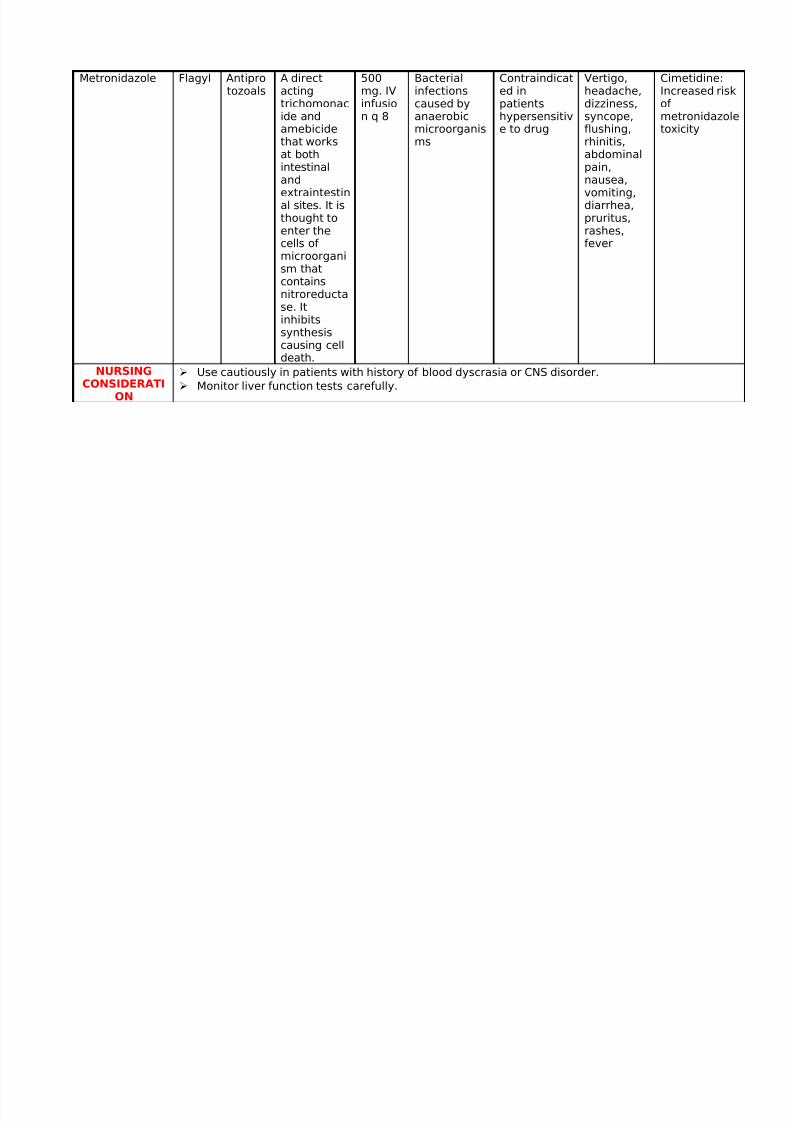
Metronidazole Flagyl Antiprotozoals
A directactingtrichomonacide andamebicide
that worksat bothintestinalandextraintestinal sites. It isthought toenter thecells of microorganism that
containsnitroreductase. Itinhibitssynthesiscausing celldeath.
500mg. IVinfusion q 8
Bacterialinfectionscaused byanaerobicmicroorganis
ms
Contraindicated inpatientshypersensitive to drug
Vertigo,headache,dizziness,syncope,flushing,
rhinitis,abdominalpain,nausea,vomiting,diarrhea,pruritus,rashes,fever
Cimetidine:Increased riskof metronidazoletoxicity
NURSINGCONSIDERATI
ON
Use cautiously in patients with history of blood dyscrasia or CNS disorder.
Monitor liver function tests carefully.
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 46/72
GENERICNAME
BRAND
NAME
DRUGCLASS
ES
ACTION DOSAGE
INDICATION CONTRAINDICATION
SIDEEFFECT
DRUG TODRUG
INTERACTION
Isosorbide
dinitrate
Imdur Anti-
anginals
Thought to
reducecardiacoxygendemand bydecreasingpreload andafterload.Drug alsomayincreaseblood flow
through thecollateralcoronaryvessels.
60 mg.
i tabOD
Acute
anginalattacks.
Contraindicat
ed inpatientshypersensitivity tonitrates
CNS:
lethargy,seizures,anxiety,dizziness,hallucination,depressionGI: nausea,vomiting,diarrea,epigastric
distress,
Antihypertens
ives: Mayincreasehypotensiveeffects
NURSINGCONSIDERATI
ON
Use cautiously in patients with blood volume depletion and hypotension.
Monitor blood pressure frequently.

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 47/72
GENERICNAME
BRAND
NAME
DRUGCLASS
ES
ACTION DOSAGE
INDICATION CONTRAINDICATION
SIDEEFFECT
DRUG TODRUG
INTERACTION
Sodium
picosulfate
Laxobe
ral
Laxativ
es
Stimulant
laxative thatincreasesperistalsis.
1 tbsp
@ HS
Acute
constipation
Contraindicat
ed in pts withulcerativebowellesions, fecalimpaction,intestinalobstruction.
nausea,
vomitinganddiarrhea,loss of normalbowelfunction,electrolyteimbalance
NURSING
CONSIDERATION
Determine whether patient has adequate fluid intake, exercise, diet.
Avoid exposing product to heat or light.
Drug is for short-term use.

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 48/72
GENERICNAME
BRANDNAME
DRUGCLASS
ES
ACTION DOSAGE
INDICATION CONTRAINDICATION
SIDEEFFECT
DRUG TODRUG
INTERACTIONSucralfate Iselpin Antiulc
erdrugs
Protectssurface of ulcer byforming abarrier.
1 tabq6
Short termtreatment forduodenalulcers
No knowncontraindications
dizziness,sleepiness,headache,vertigo,nausea,vomiting,dry mouth,flatulence
Antacids: Maydecreasebinding of drug togastroduodenal mucosa,impairingeffectiveness.
NURSINGCONSIDERA
TION
Use cautiously in pts with chronic renal failure.
Monitor for severe constipation.
GENERICNAME
BRAND
DRUGCLASS
ACTION DOSAGE
INDICATION
CONTRAINDICATION
SIDEEFFECT
DRUG TODRUG
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 49/72
NAME INTERACTION
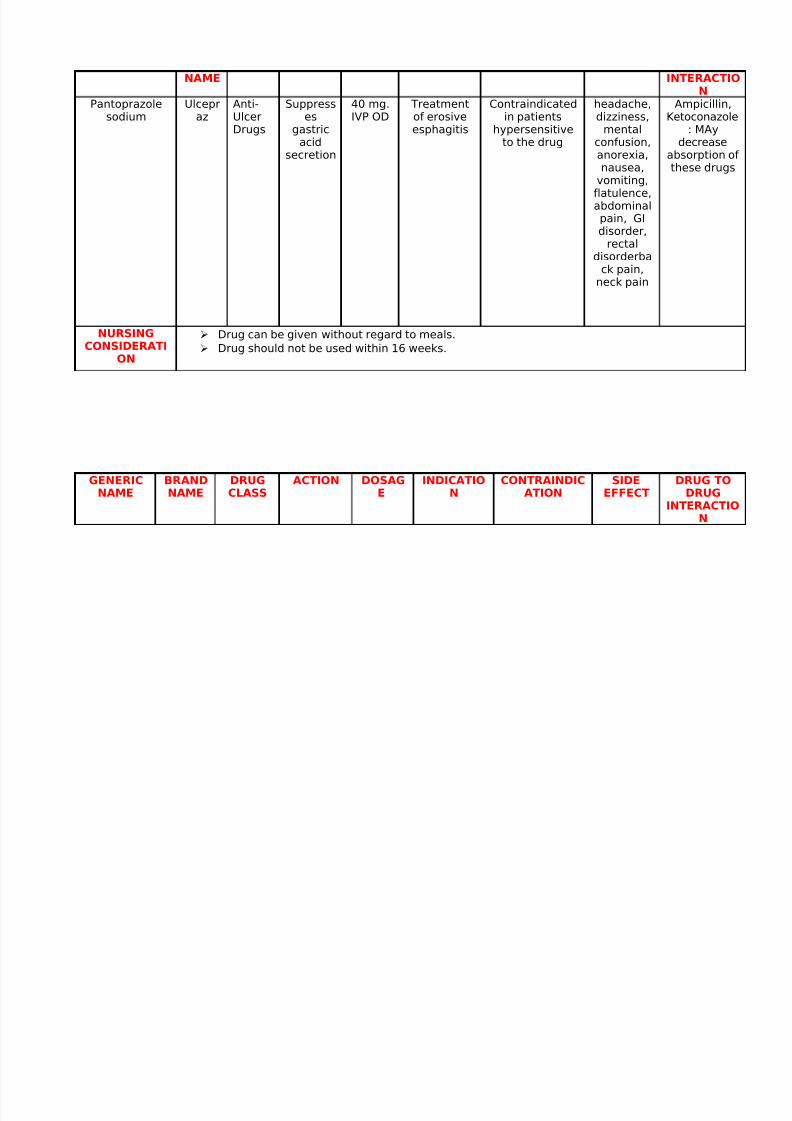
Pantoprazolesodium
Ulcepraz
Anti-UlcerDrugs
Suppresses
gastric
acidsecretion
40 mg.IVP OD
Treatmentof erosiveesphagitis
Contraindicatedin patients
hypersensitive
to the drug
headache,dizziness,
mental
confusion,anorexia,nausea,
vomiting,flatulence,abdominalpain, GIdisorder,
rectaldisorderba
ck pain,
neck pain
Ampicillin,Ketoconazole
: MAy
decreaseabsorption of these drugs
NURSINGCONSIDERATI
ON
Drug can be given without regard to meals.
Drug should not be used within 16 weeks.
GENERICNAME
BRANDNAME
DRUGCLASS
ACTION DOSAGE
INDICATION
CONTRAINDICATION
SIDEEFFECT
DRUG TODRUG
INTERACTION
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 50/72
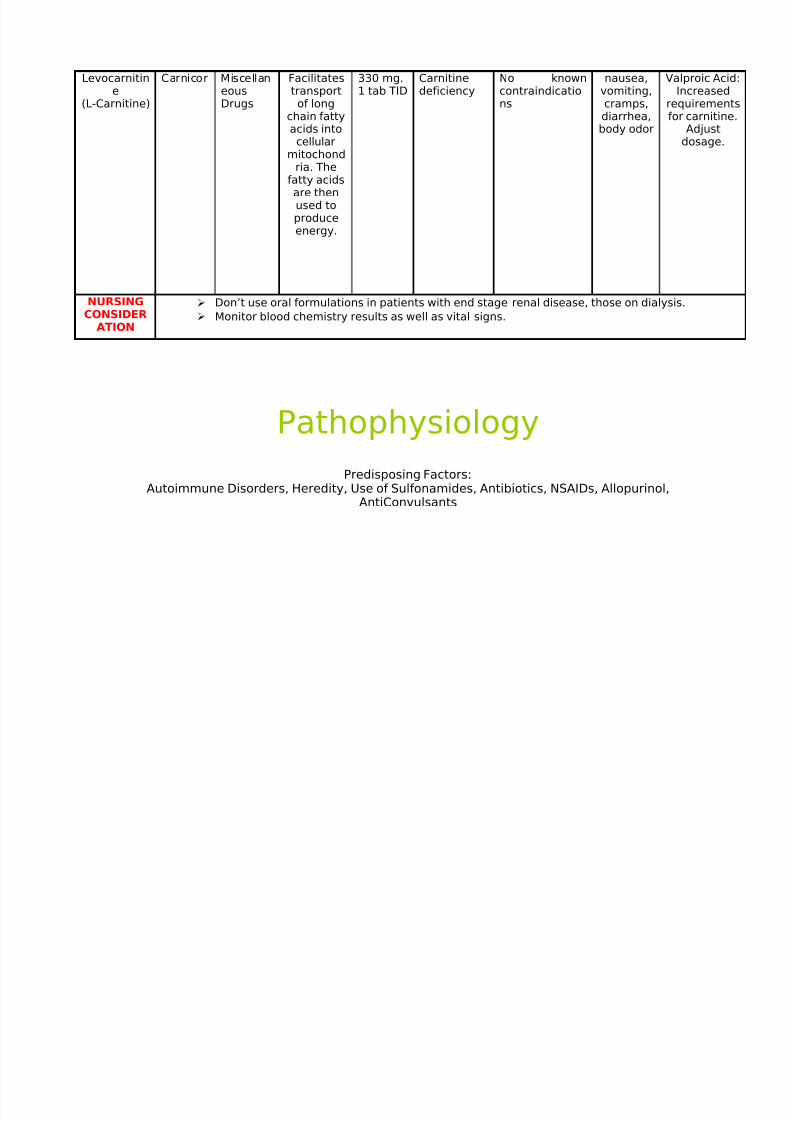
Levocarnitine
(L-Carnitine)
Carnicor MiscellaneousDrugs
Facilitatestransportof long
chain fattyacids into
cellularmitochondria. The
fatty acidsare thenused toproduceenergy.
330 mg.1 tab TID
Carnitinedeficiency
No knowncontraindications
nausea,vomiting,cramps,diarrhea,body odor
Valproic Acid:Increased
requirementsfor carnitine.
Adjust
dosage.
NURSINGCONSIDER
ATION
Don’t use oral formulations in patients with end stage renal disease, those on dialysis.
Monitor blood chemistry results as well as vital signs.
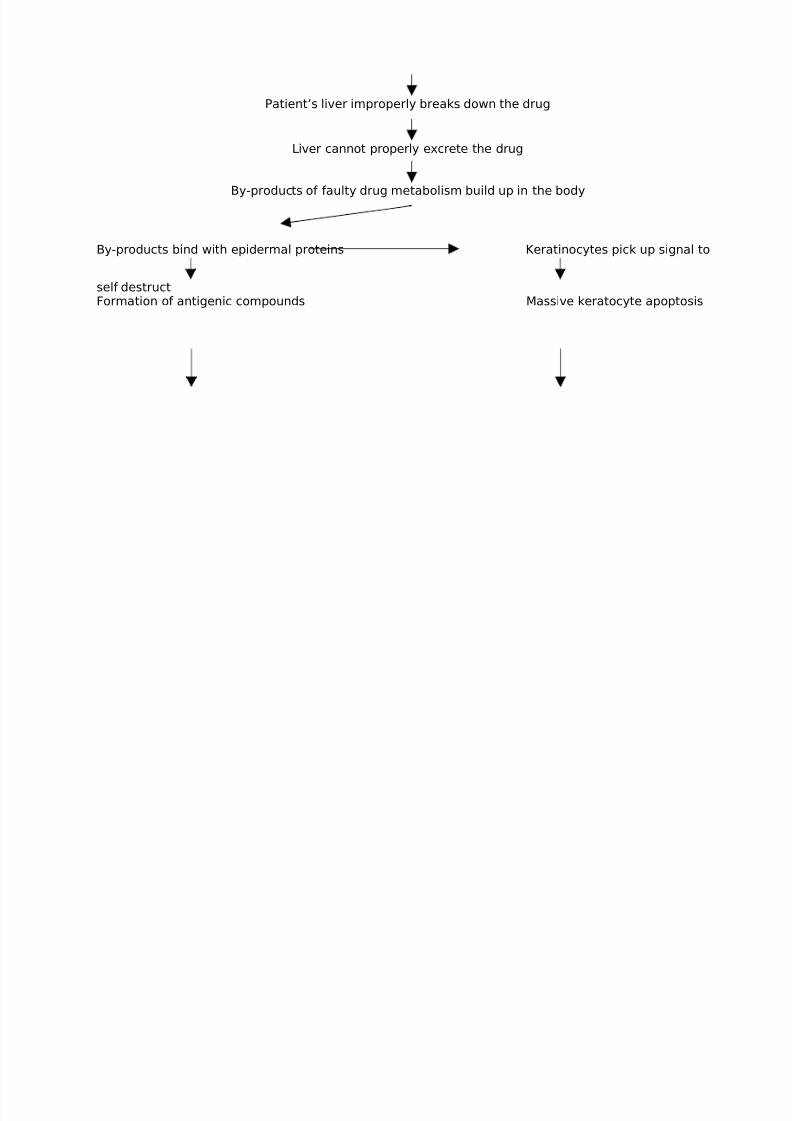
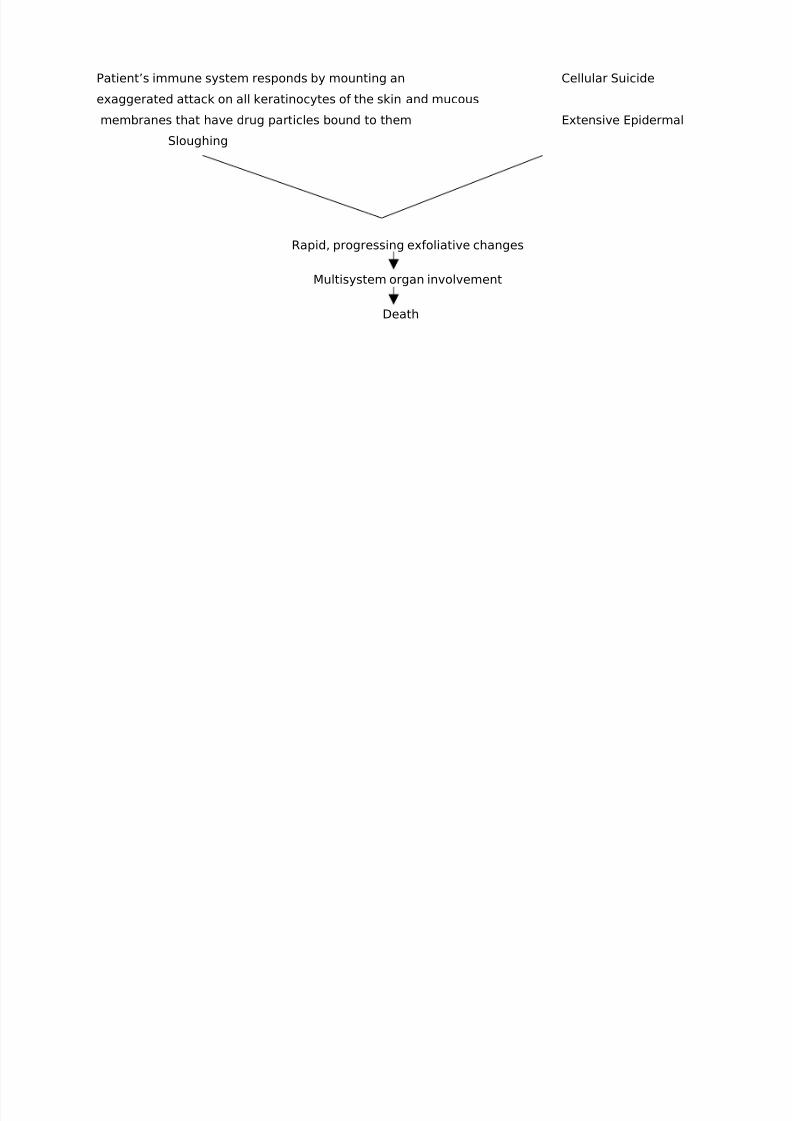
PathophysiologyPredisposing Factors:
Autoimmune Disorders, Heredity, Use of Sulfonamides, Antibiotics, NSAIDs, Allopurinol,AntiConvulsants
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 51/72
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 52/72
Patient’s immune system responds by mounting an Cellular Suicide
exaggerated attack on all keratinocytes of the skin and mucous
membranes that have drug particles bound to them Extensive Epidermal
Sloughing
Rapid, progressing exfoliative changes
Multisystem organ involvement
Death

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 53/72
Evaluation
SJS is definitely a nightmare, but there is hope. With adverse drug reactions being
the 4th leading cause of death in North America, it behooves each person to think
carefully before taking something. If a blood relative has had an allergic reaction to a
drug in the past, even a mild one, consider yourself at risk and avoid the drug.
"I was shocked to find out after my reaction that my father and brother both had
developed skin rashes when they took sulfa drugs for short periods in their lives," Callejo
said. "If only I'd known." It makes more sense, however, to seek drug-free alternatives
for one's ailments if and when they arise.
Nevertheless, knowledge is power and the group felt that more education about
drug reactions and SJS are all that we need. Farrell said forcefully, "It is so tragic. You're
warned not to give aspirin to children. How can you not tell people about a life-
threatening reaction to a drug . . . any drug?"

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 54/72
CUES NURSING
DIAGNOSIS
SCI.EXPLANATIO
N
GOAL INTERVENTION RATIONALE EVALUATION

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 55/72
S;" Masakitangbuongkatawan
ko dahilsa mgasugat ko."PasinScale: 4/5O:- gener
alizedweakness
-withscaling,erythema,lesionsandnecrosis intheentire
body- with
lesionsinmouth,buccalmucosa
Acutepain R/Tinflammation,swelling,
lesions of the entirebody
The ptexperiencesunpleasantsensation dueto stimulation
of painreceptors. This happenswhen painsubstancewere releaseand transmitit in the brainvia the spinalcord and onceit has been
sent canperceived asPAIN.
After 1hour of nursingintervention,
patient's painwill belessened.
Encourage reportsof pain, notinglocation, duration,and quality of pain.
-Maintainimmobilization of affected part.
-Explainprocedures beforebeginning them.
-Provide alternatecomfort measuressuch as massage,backrub, andposition changes.
-Encourage use of stressmanagementtechniques such as
progressiverelaxation, deepbreathingexercises.
-Identifydivertionalactivitiesappropriate for
Influences choice of/monitorseffectiveness of interventions.
-Relieves pain andprevent bonedisplacement/extension of tissue injury.
-Allows patient toprepare mentally foractivity as well as toparticipate incontrolling level of
discomfort.
-Improves generalcirculation; reducesareas of localpressure and musclefatigue.
-Refocuses attention,promotes sense of control, and may
enhance copingabilities in themanagement of pain.
-Prevents boredom,reduces tension, andcan increase musclestrength; mayenhance self-esteem
GOAL:MET The patient'spaindecreasedfrom 4/5 to
2/5.

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 56/72
- withswollenconjunctiva
-
withreddish,swollengums
- V/S:BP-140/80 CR-85 RR-
18 T-37.2
patient age,physical abilities,and personalpreferences.
Administeranalgesics asprescribed.
and coping abilities.
-This provides relief of pain.
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 57/72
CUES NURSINGDIAGNOSI
S
SCI.EXPLANATIO
N
GOAL INTERVENTION RATIONALE EVALUATION
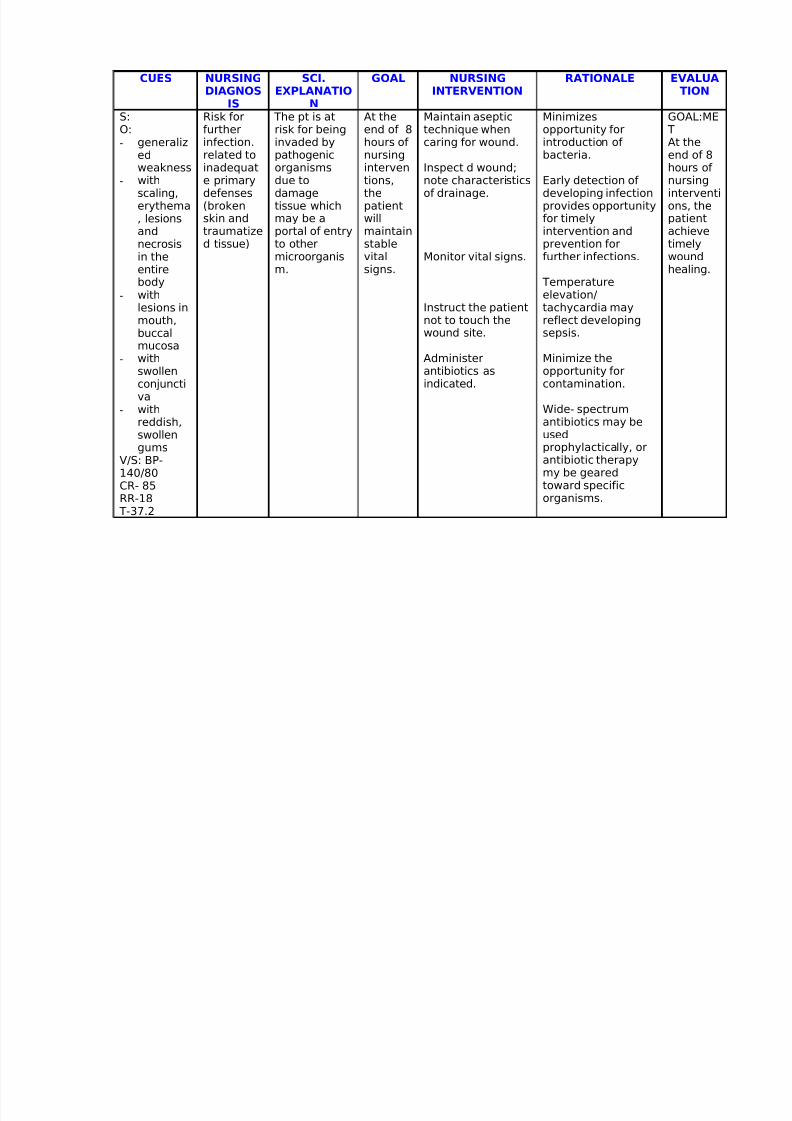
S:
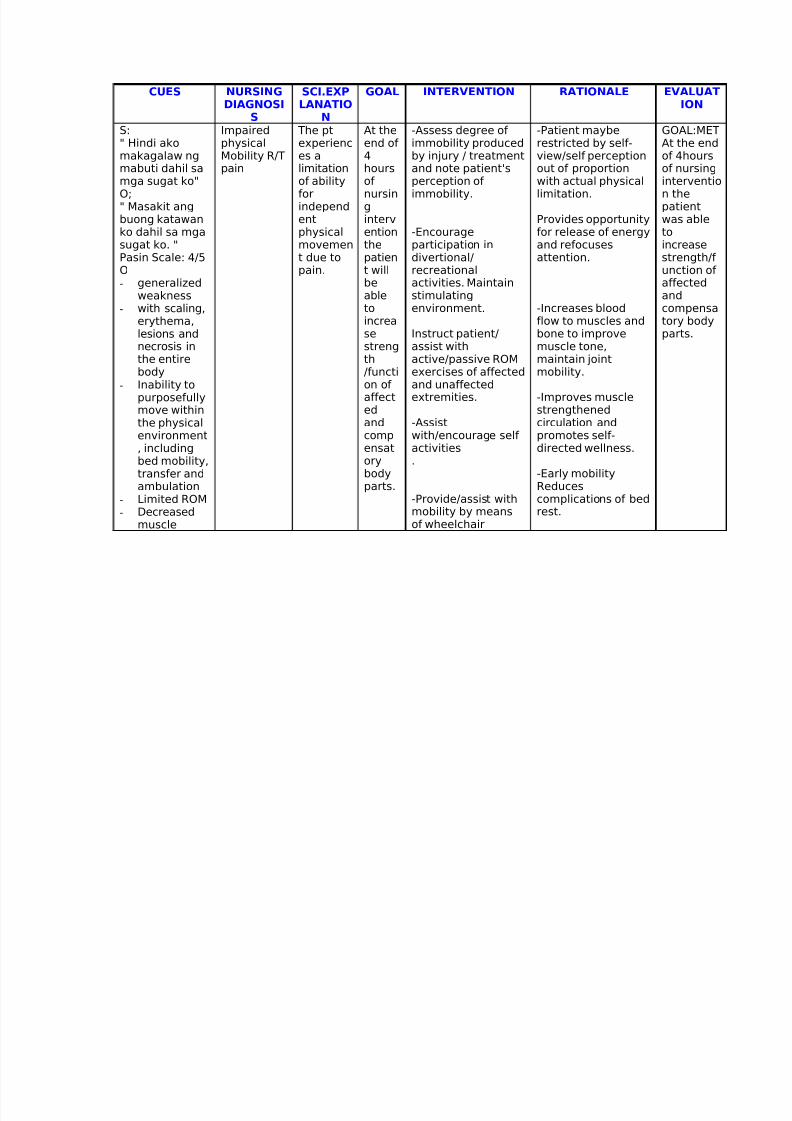
" Hindi akomakagalaw ngmabuti dahil samga sugat ko"O;" Masakit angbuong katawanko dahil sa mgasugat ko. "Pasin Scale: 4/5O
-generalizedweakness
- with scaling,erythema,lesions andnecrosis inthe entirebody
- Inability topurposefullymove within
the physicalenvironment, includingbed mobility,transfer andambulation
- Limited ROM- Decreased
muscle
Impaired
physicalMobility R/Tpain
The pt
experiences alimitationof abilityforindependentphysicalmovement due topain.
At the
end of 4hoursof nursinginterventionthepatient will
beabletoincreasestrength/function of affected
andcompensatorybodyparts.
-Assess degree of
immobility producedby injury / treatmentand note patient'sperception of immobility.
-Encourageparticipation indivertional/recreational
activities. Maintainstimulatingenvironment.
Instruct patient/assist withactive/passive ROMexercises of affectedand unaffectedextremities.
-Assistwith/encourage self activities.
-Provide/assist withmobility by meansof wheelchair
-Patient maybe
restricted by self-view/self perceptionout of proportionwith actual physicallimitation.
Provides opportunityfor release of energyand refocusesattention.
-Increases bloodflow to muscles andbone to improvemuscle tone,maintain jointmobility.
-Improves musclestrengthened
circulation andpromotes self-directed wellness.
-Early mobilityReducescomplications of bedrest.
GOAL:MET
At the endof 4hoursof nursingintervention thepatientwas abletoincreasestrength/f unction of
affectedandcompensatory bodyparts.

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 58/72
strength- Imposed
restrictionsof movement
crutches.
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 59/72
CUES NURSINGDIAGNOS
IS
SCI.EXPLANATIO
N
GOAL NURSINGINTERVENTION
RATIONALE EVALUATION
S:O:-
generalizedweakness
- withscaling,erythema, lesionsandnecrosisin theentire
body- with
lesions inmouth,buccalmucosa
- withswollenconjunctiva
- with
reddish,swollengums
V/S: BP-140/80CR- 85RR-18 T-37.2
Risk forfurther
infection.related toinadequate primarydefenses(brokenskin andtraumatized tissue)
The pt is atrisk for being
invaded bypathogenicorganismsdue todamagetissue whichmay be aportal of entryto othermicroorganism.
At theend of 8
hours of nursinginterventions,thepatientwillmaintainstablevitalsigns.
Maintain aseptictechnique when
caring for wound.
Inspect d wound;note characteristicsof drainage.
Monitor vital signs.
Instruct the patientnot to touch thewound site.
Administerantibiotics asindicated.
Minimizesopportunity for
introduction of bacteria.
Early detection of developing infectionprovides opportunityfor timelyintervention andprevention forfurther infections.
Temperatureelevation/tachycardia mayreflect developingsepsis.
Minimize theopportunity forcontamination.
Wide- spectrum
antibiotics may beusedprophylactically, orantibiotic therapymy be gearedtoward specificorganisms.
GOAL:ME T
At theend of 8hours of nursinginterventions, thepatientachievetimelywoundhealing.

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 60/72
CUES NURSINGDIAGNOSIS
SCIENTIFICEXPLANATIO
N
GOAL NURSINGINTERVENTION
RATIONALE OUTCOME
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 61/72
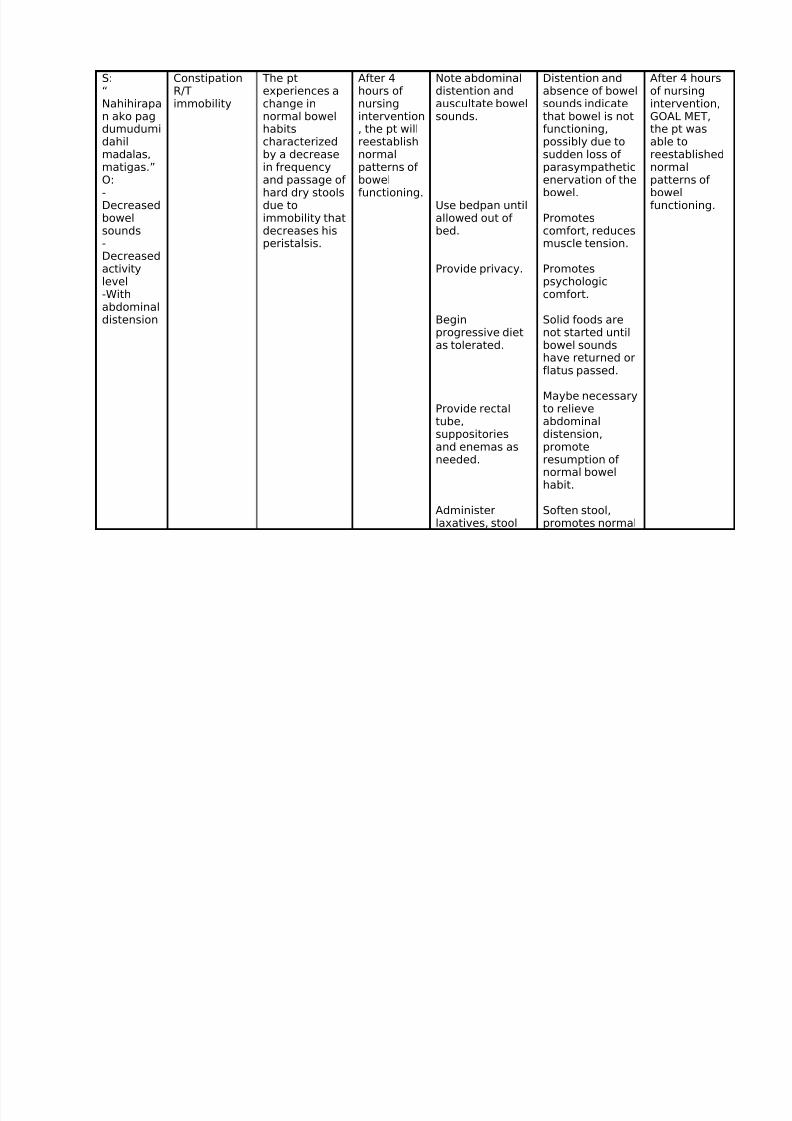
S:“Nahihirapan ako pagdumudumidahilmadalas,matigas.”O:-Decreasedbowelsounds-Decreasedactivity
level-Withabdominaldistension
ConstipationR/Timmobility
The ptexperiences achange innormal bowelhabitscharacterizedby a decreasein frequencyand passage of hard dry stoolsdue toimmobility thatdecreases hisperistalsis.
After 4hours of nursingintervention, the pt willreestablishnormalpatterns of bowelfunctioning.
Note abdominaldistention andauscultate bowelsounds.
Use bedpan untilallowed out of bed.
Provide privacy.
Beginprogressive dietas tolerated.
Provide rectal
tube,suppositoriesand enemas asneeded.
Administerlaxatives, stool
Distention andabsence of bowelsounds indicatethat bowel is notfunctioning,possibly due tosudden loss of parasympatheticenervation of thebowel.
Promotescomfort, reducesmuscle tension.
Promotes
psychologiccomfort.
Solid foods arenot started untilbowel soundshave returned orflatus passed.
Maybe necessaryto relieve
abdominaldistension,promoteresumption of normal bowelhabit.
Soften stool,promotes normal
After 4 hoursof nursingintervention,GOAL MET,the pt wasable toreestablishednormalpatterns of bowelfunctioning.
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 62/72
softeners, asindicated.
bowel habits anddecreasesstraining.
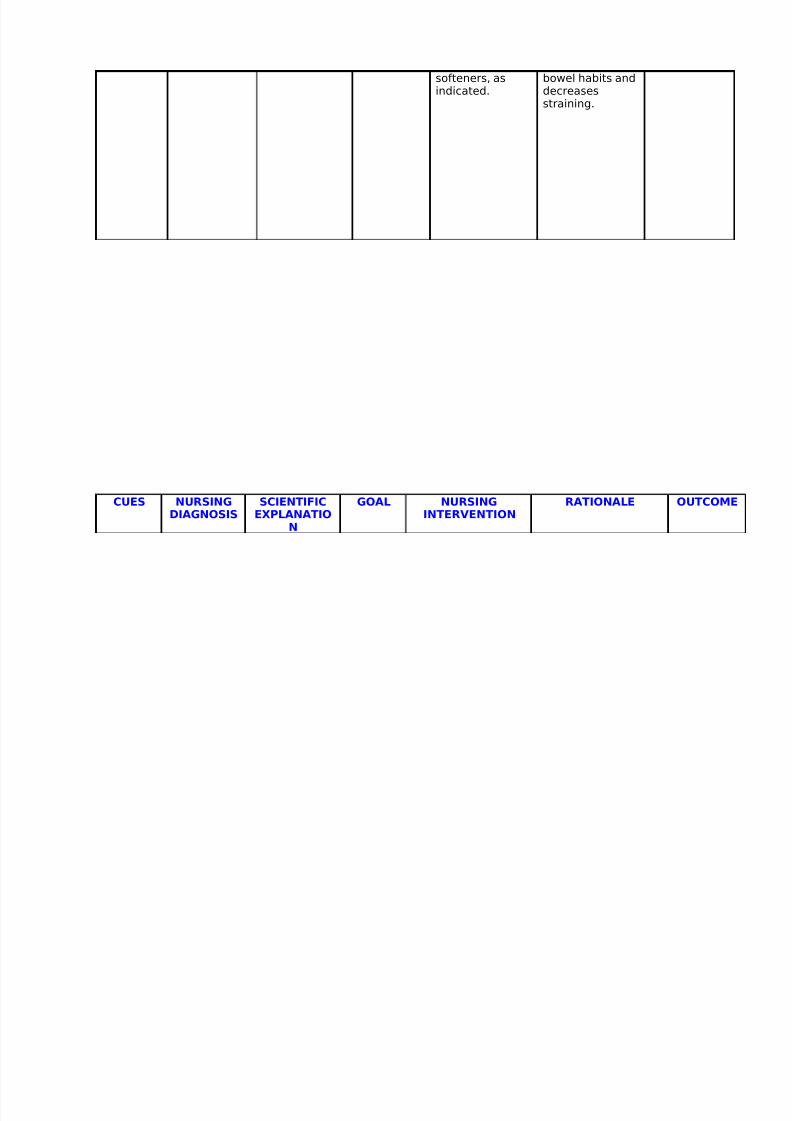
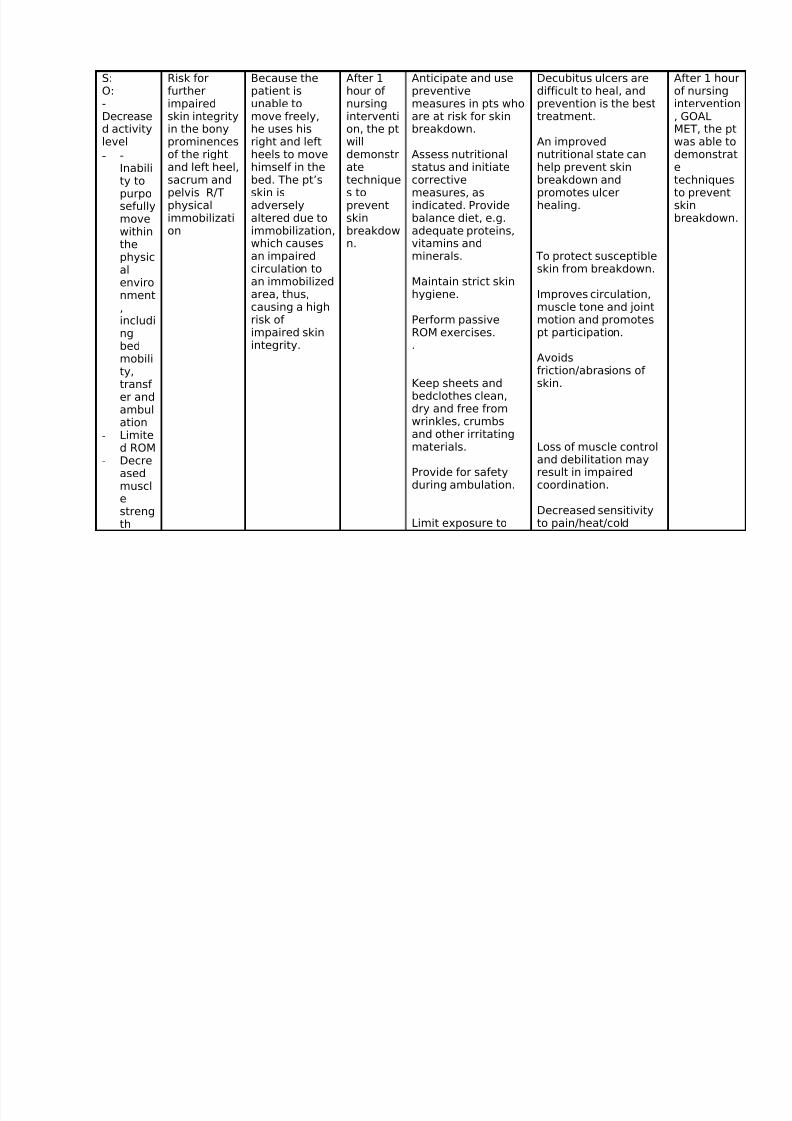
CUES NURSINGDIAGNOSIS
SCIENTIFICEXPLANATIO
N
GOAL NURSINGINTERVENTION
RATIONALE OUTCOME
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 63/72
S:O:-Decreased activitylevel
- -Inability topurposefullymovewithinthephysical
environment,includingbedmobility,transf er andambul
ation- Limite
d ROM- Decre
asedmusclestrength
Risk forfurtherimpairedskin integrityin the bonyprominencesof the rightand left heel,sacrum andpelvis R/Tphysicalimmobilization
Because thepatient isunable tomove freely,he uses hisright and leftheels to movehimself in thebed. The pt’sskin isadverselyaltered due toimmobilization,which causesan impairedcirculation to
an immobilizedarea, thus,causing a highrisk of impaired skinintegrity.
After 1hour of nursingintervention, the ptwilldemonstratetechniques topreventskinbreakdown.
Anticipate and usepreventivemeasures in pts whoare at risk for skinbreakdown.
Assess nutritionalstatus and initiatecorrectivemeasures, asindicated. Providebalance diet, e.g.adequate proteins,vitamins andminerals.
Maintain strict skinhygiene.
Perform passiveROM exercises..
Keep sheets andbedclothes clean,dry and free from
wrinkles, crumbsand other irritatingmaterials.
Provide for safetyduring ambulation.
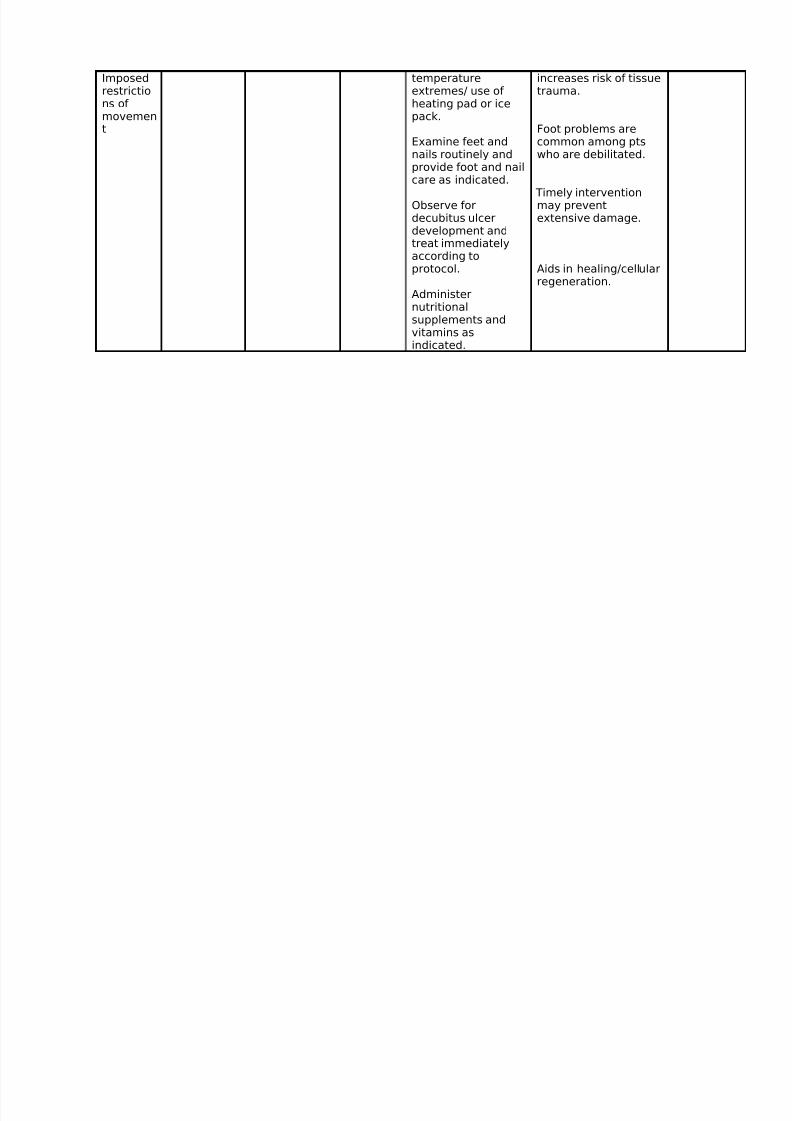
Limit exposure to
Decubitus ulcers aredifficult to heal, andprevention is the besttreatment.
An improvednutritional state canhelp prevent skinbreakdown andpromotes ulcerhealing.
To protect susceptibleskin from breakdown.
Improves circulation,muscle tone and jointmotion and promotespt participation.
Avoidsfriction/abrasions of skin.
Loss of muscle controland debilitation mayresult in impairedcoordination.
Decreased sensitivityto pain/heat/cold
After 1 hourof nursingintervention, GOALMET, the ptwas able todemonstratetechniquesto preventskinbreakdown.
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 64/72
Imposedrestrictions of movement
temperatureextremes/ use of heating pad or icepack.
Examine feet andnails routinely andprovide foot and nailcare as indicated.
Observe fordecubitus ulcerdevelopment andtreat immediatelyaccording toprotocol.
Administernutritionalsupplements andvitamins asindicated.
increases risk of tissuetrauma.
Foot problems arecommon among ptswho are debilitated.
Timely interventionmay preventextensive damage.
Aids in healing/cellular
regeneration.
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 65/72
Discharge PlanMedications
Instructed client to religiously take medications prescribed by the physician.
Exercise
Advised to perform activities according to tolerance for relaxation and endurance. (as prescribed)
Relaxation and deep breathing exercises especially in the morning.
Gentle increasing exercise is helpful, prevents excessive fatigue and conserves energy for healing.
Treatment
Instructed patient to treat wounds properly, as prescribed by the physician.
Advised to do aseptic technique when cleaning the wound.
Health Teachings
Provide patient a thorough explanation of the disease process, treatment regimen and follow-up.
Teach the importance of follow-up care, healthy diet and adequate rest.
Encourage alternating rest period and activity.
Advise SO to provide comfort measures and divers ional activities such as music, television. Thesepromote relaxation and helps refocus attention.
Teach client to avoid stress.
Discuss need for safe environment (removing scattered drugs) at home and use of assistive devices
because of impaired mobility. Maintain nutritional status and promote overall health by encouraging good oral intake.
Instruct the patient to finish all prescribed medications, especially antibiotics.
OPD/ Follow-Up

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 66/72
Advise patient to come back after 1 week of discharge for follow-up check-up at the OPD. This will provideongoing monitoring of progression and resolution of disease process.
Diet
Adequate hydration and nutrition to promote wellness and health.
Maintain a balanced diet to improve body’s ability to heal itself.
Advise patient to increase intake of foods rich in vitamin C like fruits and vegetables for collagenformation that promotes tissue regeneration and healing of wound.
Instructed patient to eat foods rich in protein such as eggs, meat and fish to facilitate tissue formation.
Complications and Prognosis

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 67/72
Complications:
• Ophthalmologic - Corneal ulceration, anterior uveitis, panophthalmitis, blindness
• Gastroenterologic - Esophageal strictures
• Genitourinary - Renal tubular necrosis, renal failure, penile scarring, vaginal stenosis
• Pulmonary - Tracheobronchial shedding with resultant respiratory failure
• Cutaneous - Scarring and cosmetic deformity, recurrences of infection through slow-healing ulcerations
Prognosis:
• Individual lesions typically should heal within 1-2 weeks, unless secondary infectionoccurs. The majority of patients recover without sequelae.
• Development of serious sequelae, such as respiratory failure, renal failure, and blindness,determines prognosis in those affected.
• Up to 15% of all patients with SJS die as a result of the condition.

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 68/72
Nursing Care Plans• Acute pain R/T inflammation, swelling, lesions of the entire body
• Constipation R/T immobility
• Impaired physical Mobility R/T pain
• Risk for further impaired skin integrity in the bony prominences of the right and left
heel, sacrum and pelvis R/T physical immobilization
• Risk for further infection. related to inadequate primary defenses (broken skin and
traumatized tissue)

8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 69/72
STEVENS- JOHNSON
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 70/72
SYNDROME
GROUP II BSN 4 -A
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 71/72
Lea Marie Salazar
Rey Raniaga
Loredel Melegrito
Shiela Tomas
Mayleen Mutuc
Kristine Padlan
Melissa Matusalem
Giovanni Tebia
Jennelyn Pascual
Michelle Sidoro
Jennilyn Dampil
Aleda Pineda
Michael Tan
Raymond Lorenzo
Hermel Joseph Paras
A Case Study
8/3/2019 Case - Steven Johnson's
http://slidepdf.com/reader/full/case-steven-johnsons 72/72
Submitted To
Ms. Odette Tanedo, R.N.December 9, 2004