cardio vascular risk reduction in diabetes mellitus
TRANSCRIPT

Cardio vascular risk reduction in Diabetes mellitus
Dr S.VenkatesanCardiologist Madras medical collegeChennai TAN-CSI Thiruvanandhapuram10-9- 2017
www.drsvenkatesan.com

www.drsvenkatesan.com

•DM pathology in CVD•Risk quantification•Risk reduction •Conventional DM management •CVOT focussed strategies•What we have achieved ?•Introspection & Future
www.drsvenkatesan.com

CAD pathology In Diabetes
www.drsvenkatesan.com

www.drsvenkatesan.com

www.drsvenkatesan.com

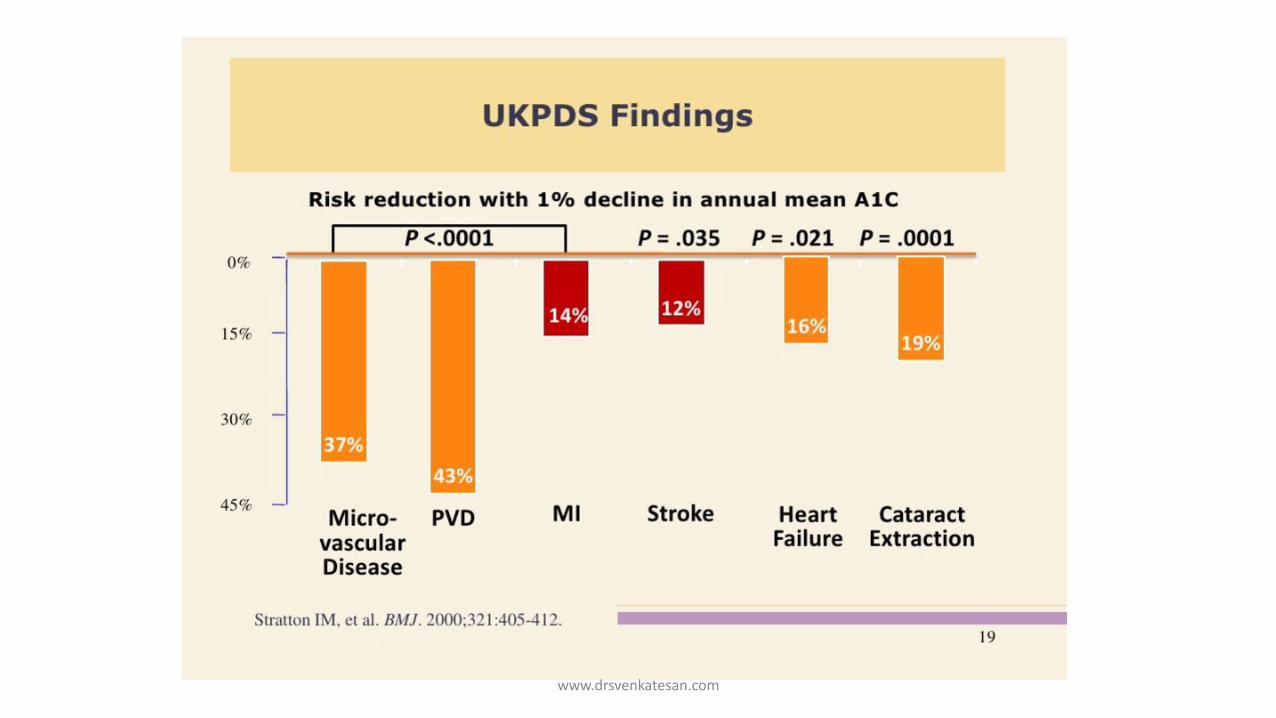
Higher HbA1c predicts higher CV risk
Meta-analysis: Increase of 1% of HbA1C is concomitant with-
17% increase in CVD 15% increase in CHD
29% increase in PAD 11% increase in Stroke
Zhang Y et al. 2012. PLoS ONE 7(8): e42551
Stroke
www.drsvenkatesan.com

Macro
Micro RetinalNephroNeuro
CardiacCerebralPeripheral
www.drsvenkatesan.com

Brownlee’s Unifying hypothesis
www.drsvenkatesan.com

Type 1
DM
Type 2
DM
Blurring margins between two types
www.drsvenkatesan.com

www.drsvenkatesan.com

Diffuse macro vascular disease
www.drsvenkatesan.com

Diabetes and heart failure
Is it macro or macro vascular complication ?
Microalbuminuria is strongly correlated with diabetic risk of cardiac failure
www.drsvenkatesan.com

How risky is DM in CVD ?
www.drsvenkatesan.com

www.drsvenkatesan.com

www.drsvenkatesan.com

www.drsvenkatesan.com

2013 ACC/AHA down graded it as Just another risk factor in 2013
Some controversies risk assessment
DM is CHD equivalent IN 2001 by ATP 3 (Alarmist reaction meant 100% )
www.drsvenkatesan.com

Risk reduction how good it is ?
www.drsvenkatesan.com
www.drsvenkatesan.com

Impact of Intensive vs Conventional Glycemic-Lowering Strategies on Risk of CV Outcomes Is Unclear
StudyDiabetes Duration (mean)
Antihyperglycemic Medicationa
Follow-up(median)
HbA1c: Baseline, Between-arm
Difference
Microvascular
CVDMortalit
y
UKPDS1
Newly diagnosed
SU/insulin or metformina vs dietary
restriction
10 years7.1% (all
patients)b, –0.9%c
↓ ↔ ↔UKPDSLong-term
follow-up2
10 years post
intervention
No difference in HbA1c between
treatment armsd↓ ↓ ↓
ADVANCE3 8 years
Intensive glucose control including gliclazide vs standard treatment
5 years7.5% (both
arms)b, –0.8%d
↓ ↔ ↔ACCORD4,
5 10 yearsMultiple drugs in both
arms3.4 years
8.1% (both arms)e, –1.1%c
↓ ↔ ↑
VADT6 11.5 yearsMultiple drugs in both
arms5.6 years
9.4% (both arms)b, –1.5%d
↔ ↔ ↔
aObese patients; bMean baseline HbA1c; cMedian between-arm difference; dMean between-arm difference; eMedian baseline HbA1c.
CV = cardiovascular; UKPDS = United Kingdom Prospective Diabetes Study (UKPDS); ADVANCE = Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation; ACCORD = Action to Control Cardiovascular Risk in Diabetes; VADT = Veterans Affairs Diabetes Trial.
1. UKPDS Group. Lancet. 1998;352:837–853. 2. Holman RR et al. N Engl J Med. 2008;359:1577–1589. 3. ADVANCE Collaborative Group et al. N Engl J Med. 2008;358:2560–2572. 4. Gerstein HC et al. N Engl J Med. 2008;358:2545–2559. 5. Ismail-Beigi F et al. Lancet. 2010;376:419–430. 6. Duckworth W et al. N Engl J Med. 2009;360:129–139.
Lowering HbA1c may prevent macrovascular disease if started early, but the effects may not be apparent for a very long time
www.drsvenkatesan.com

Conventional drugs : Big let down ? :
Except Metformin, ? GlimiperideGlitazone was good but risky ?
www.drsvenkatesan.com

• Difficult • Incomplete • Not uniform • Prone with risk
Challenges in Diabetic CVD risk reduction
www.drsvenkatesan.com

Search for new strategies . . .
www.drsvenkatesan.com

Back to basics
www.drsvenkatesan.com

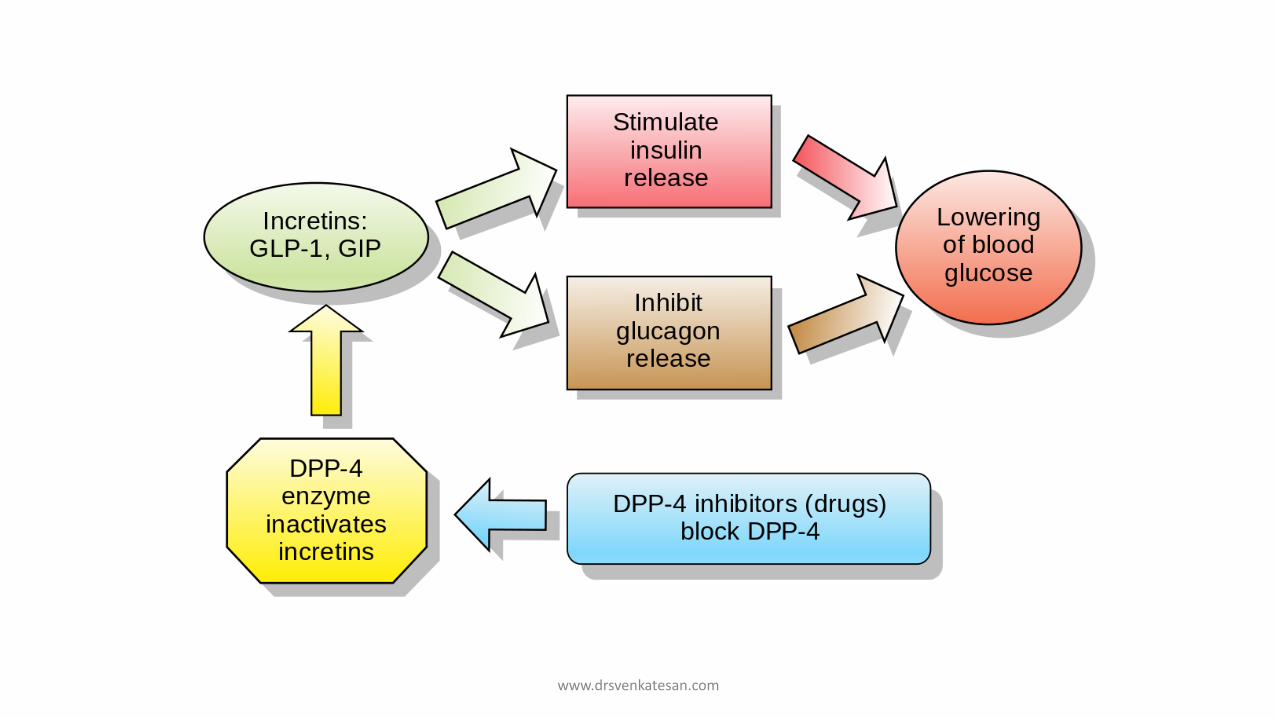
We realised its essentially Islet cell mismatch between Alpha and beta and a literal fight between Insulin and the counter hormone Glucagon
www.drsvenkatesan.com

www.drsvenkatesan.com
www.drsvenkatesan.com

www.drsvenkatesan.com

DPP-4 inhibitorsSitagliptin, Saxagliptin,Alogliptin, linagliptin
EXAMINE [Examination of Cardiovascular Outcomes with Alogliptin versus Standard of Care] trial),2 saxagliptin (in the SAVOR-TIMI 53 [SaxagliptinAssessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus–Thrombolysis in Myocardial Infarction 53] trial),3 and sitagliptin (in TECOS [Trial Evaluating Cardiovascular Outcomes
www.drsvenkatesan.com

Vildagliptin does not have an ongoing CV outcomes trial
Linagliptin CARMELINA (N=8,300)4
Pre-existing CVD + albuminuria or impaired renal function
Risk Factors Stable CAD-CVD-PAD Post ACS patients
Sitagliptin TECOS (N=~14,000)3
Pre-existing CVD
Alogliptin EXAMINE (N=5,380)1
ACS within 15–90 days
Saxagliptin SAVOR-TIMI (N=16,492)2
Pre-existing CVD or multiple risk factors for CVD
CV = cardiovascular; DPP-4 = dipeptidyl peptidase-4; CAD = coronary artery disease; CVD = cardiovascular disease; PAD = peripheral artery disease; ACS = acute coronary syndrome; ACS = acute coronary syndrome; EXAMINE = Examination of Cardiovascular Outcomes: Alogliptin vs Standard of Care in Patients With Type 2 Diabetes Mellitus and Acute Coronary Syndrome; SAVOR-TIMI = Saxagliptin Assessment of Vascular Outcomes Recorded in Patients With Diabetes Mellitus Trial-Thrombolysis in Myocardial Infarction; TECOS = Trial Evaluating Cardiovascular Outcomes With Sitagliptin; CARMELINA = Cardiovascular and Renal Microvascular Outcome Study With Linagliptin in Patients With Type 2 Diabetes Mellitus at High Vascular Risk.
1. White W et al. N Engl J Med. 2013;369:1327–1335. 2. Scirica BM et al. N Engl J Med. 2013;369:1317–1326. 3. Green JB et al. Am Heart J 2013;166:983–989.e7. 4. CARMELINA: Cardiovascular and renal microvascular outcome study with linagliptin in patients with type 2 diabetes mellitus at high vascular risk. ClinicalTrials.gov web site. http://clinicaltrials.gov/ct2/show/ NCT01703298. Accessed September 12, 2014.
Baseline Risk of Patient Populations Enrolled in CV Outcome Trials of DPP-4 Inhibitors
www.drsvenkatesan.com

DPPI summary
Powerful Insulin sensitising action
Good anti hyperglycemic effect
Still, not good enough to for meaningfullCVD protection
www.drsvenkatesan.com

LEADERS study www.drsvenkatesan.com

GLP
Lir
www.drsvenkatesan.com

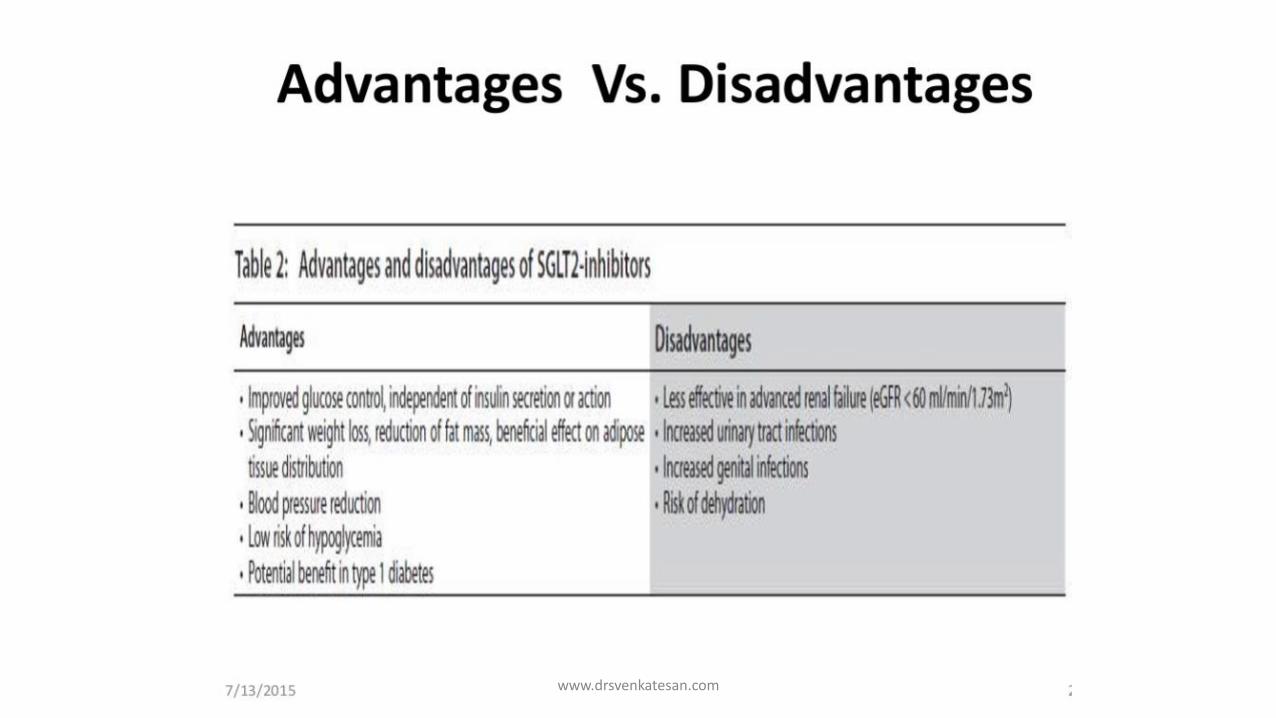
Moving away from pancreas . . .
www.drsvenkatesan.com

www.drsvenkatesan.com

SGLT2 are not new molecules !
www.drsvenkatesan.com

www.drsvenkatesan.com

www.drsvenkatesan.com

www.drsvenkatesan.com

EMPA-REG Outcome CANVASDECLARE
CVOT trials on SGL2 Inhibitors
www.drsvenkatesan.com
www.drsvenkatesan.com

EmpagliflozinType 2 diabetes
57 % DM > 10 years
99 % Had CAD
Reduced the composite outcome of MI, stroke, and cardiovascular death by 14% cardiovascular death by 38%
FDA recently added a new indication for empagliflozin, to reduce the risk of cardiovascular death in adults with type 2 diabetes and cardiovascular disease.
www.drsvenkatesan.com

www.drsvenkatesan.com

Ketogenic drug www.drsvenkatesan.com
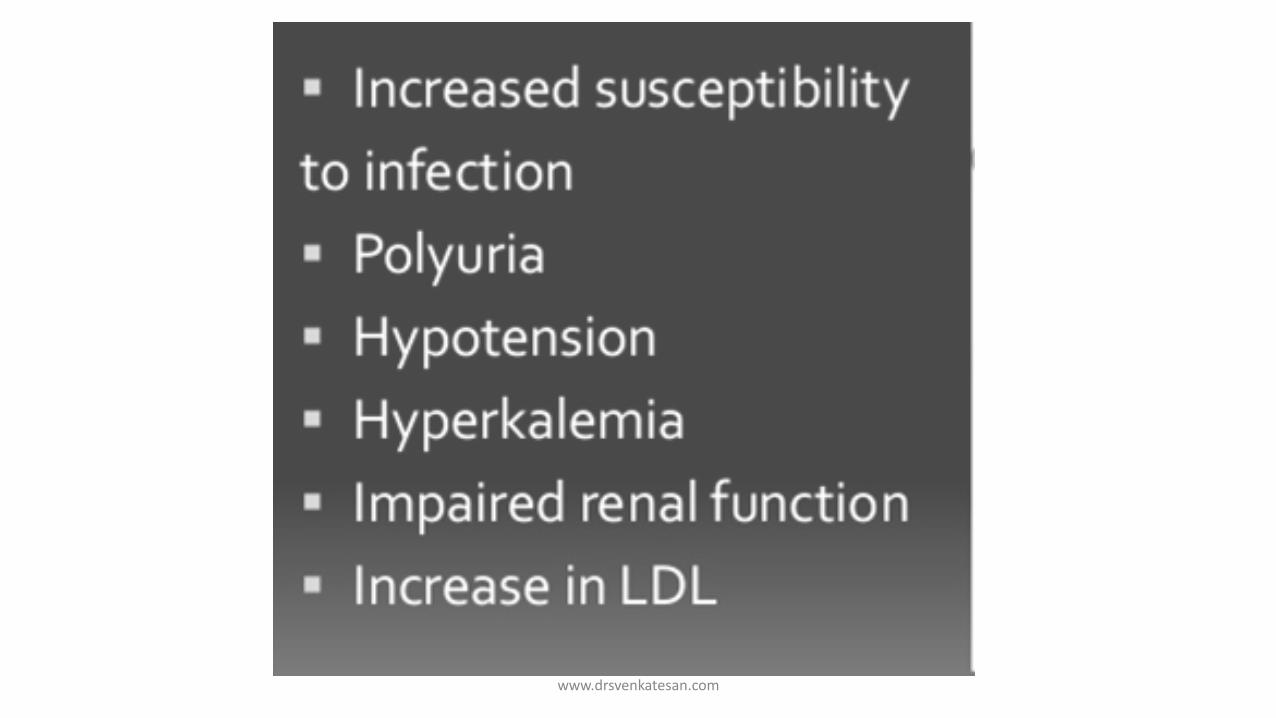
www.drsvenkatesan.com

www.drsvenkatesan.com

Troublesome in few www.drsvenkatesan.com

DM practice changing break through ?
www.drsvenkatesan.com
www.drsvenkatesan.com
Insulin & CVOT
Has no direct mortality benefit
Still ,will remain the key
For rapid control
In difficult profiled patients
www.drsvenkatesan.com

Future of Empaglifloxin
Usefulness in Heart failure will tested –EMPEROR Study
www.drsvenkatesan.com

www.drsvenkatesan.com

DM management in specific situations
Hypertension Obesity DyslipidemiaPregnancy ACS
www.drsvenkatesan.com

LDL
BP
HBA1C
Statin
Aspirin
ACEI/ARB
Multiple targets
www.drsvenkatesan.com

How to treat hypertension in DM ?
ACCORD, ADVANCE, SPRINT, AND HOT
Less than 140 mm hg is suffice
Beta blockers : Still safe in documented CAD !
www.drsvenkatesan.com

Caution with aggressive management
ICU setting
ACS
Hyperglycemia is stress induced Physiological response
www.drsvenkatesan.com

NICE-SUGARNormoglycemia in Intensive Care Evaluation Survival Using Glucose Algorithm Regulation
6104 patients ; 1/3 (surgical) and 2/3( medical) Only 20% had known diabetes
Intensive-Rx Group
Conventional Group
Subjects received IV insulin
97% 69%
Mean BG achieved 115 mg/dL. 144 mg/dL.
Mortality rate at 90 days
27.5% 14% higher mortality rate OR
1.14 (85% CI, 0.4 to 4.8)
24.9%
Severe hypoglycemia 6.8% 0.5%
(P<0.001) (BG ≤40 mg/dL) www.drsvenkatesan.com
Concluding analysis Introspection !
www.drsvenkatesan.com

Diabetes is not simple elevated blood sugar ,Rather hyperglycemiais one of the markers of diabetes
www.drsvenkatesan.com
Diabetes is not simply excess sugar in the body
www.drsvenkatesan.com

Are we fighting a wrong target ?
Why we struggle to arrest progressive vascular disease ?
Why risk reduction is not absolute ?
www.drsvenkatesan.com

Regulatory bodies & knowledge(Data ?) creators
www.drsvenkatesan.com

Watch for safety warnings
www.drsvenkatesan.com

Current CVOT landscape
Aleglitazar, a dual agonist of peroxisome proliferator–activated receptors was the first OAD which failed to qualify
Approximately 150,000 are being or have been followed in CVOTs
Mannucci E. et al. Diabetes Care. 2016 Aug;39 Suppl 2:S196-204
www.drsvenkatesan.com

Luckily ,common sense rediscovered as breaking news science !
INTERHEART study reveals Activity and diet can reduce risk of CVD and DM tremendously
Drugs vs Diet & Excercise
www.drsvenkatesan.com

Benefits for 10 % weight loss
www.drsvenkatesan.com

Diabetes is a metabolic disease . . .
www.drsvenkatesan.com

A diabetic diet simply means eating the healthiest foods in moderate amounts and sticking to regular mealtimes.
Non weight gaining or preferably weight loosing diet .
Fat vs cardbohydrate controversy not likely to end !(PURE study 2017)
www.drsvenkatesan.com

Key messages
DM increases CVD risk many fold
Controlling DM do bring CVD risk down, but never to the basal levels.
Old generation OHA Metforminremains corner stone
New generation drugs are promising.But, caution is required www.drsvenkatesan.com

Patient
Cardiologist
Physician
Diabetologist
Industry
Who shall take care ?
www.drsvenkatesan.com

Thank you www.drsvenkatesan.com