biology i-biological macromolecules a-carbohydrate files/biology/macromolecules,...
TRANSCRIPT
I-Biological Macromolecules
A-Carbohydrate
Continued Education Program
Biology
Presented by:Dr. Shaimaa Nasr Amin
Lecturer of Medical Physiology
2
•Organic compounds:are Compounds
that contain CARBON .
•Macromolecules are large organic
molecules.
Macromolecule
A large oraganic molecule, such as a polymer
or protein, consisting of many smaller
structural units linked together.
MACROMOLECULES OF LIFE
• Found in all living things
• Building blocks of all cells
• Made up of the atoms: Carbon, oxygen, hydrogen, Nitrogen, Phosphorus, and Sulfur
• There are 4
1. Carbohydrates C, H, & O
2. Lipids C, H, & O
3. Proteins C, H, O, N, & S
4. Nucleic Acids C, H, O, N, & P
All biological macro-molecule are made
up of a small number of elements:
Carbon, Hydrogen, Oxygen, Nitrogen,
Phosphorus and Sulfur
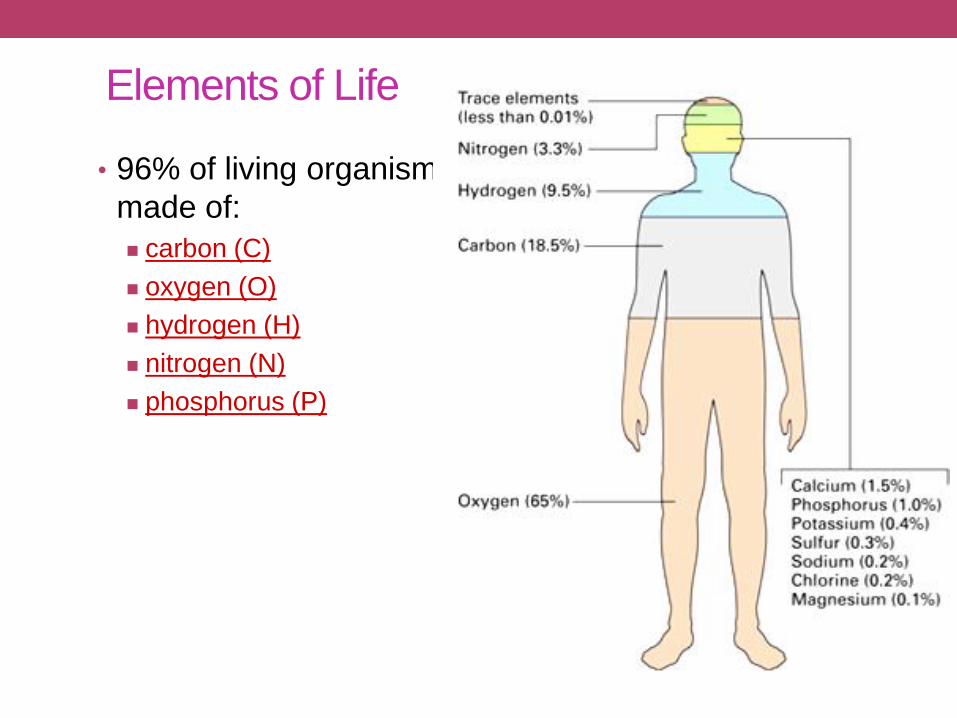
• 96% of living organisms is
made of:
carbon (C)
oxygen (O)
hydrogen (H)
nitrogen (N)
phosphorus (P)
Elements of Life

Molecules of Life• Put C, H, O, P, and N together in different
ways to build living organisms
• What are bodies made of?
• carbohydrates
• sugars & starches
• proteins
• fats (lipids)
• nucleic acids
• DNA, RNA

• Water
• 65% of your body is H2O
• water is inorganic
• doesn’t contain carbon
• Rest of you is made of carbon molecules
• organic molecules
• carbohydrates
• proteins
• fats
• nucleic acids
Don’t forget water
I. Polymers
• What is a polymer?
• Poly = many; mer = part. A polymer is a large molecule
consisting of many smaller sub-units bonded together.
• What is a monomer?
• A monomer is a sub-unit of a polymer.
A. Making and Breaking Polymers
• How are covalent linkages between monomers formed in the creation of organic polymers?
• Condensation or dehydration synthesis reactions.
• Monomers are covalently linked to one another through
the removal of water.
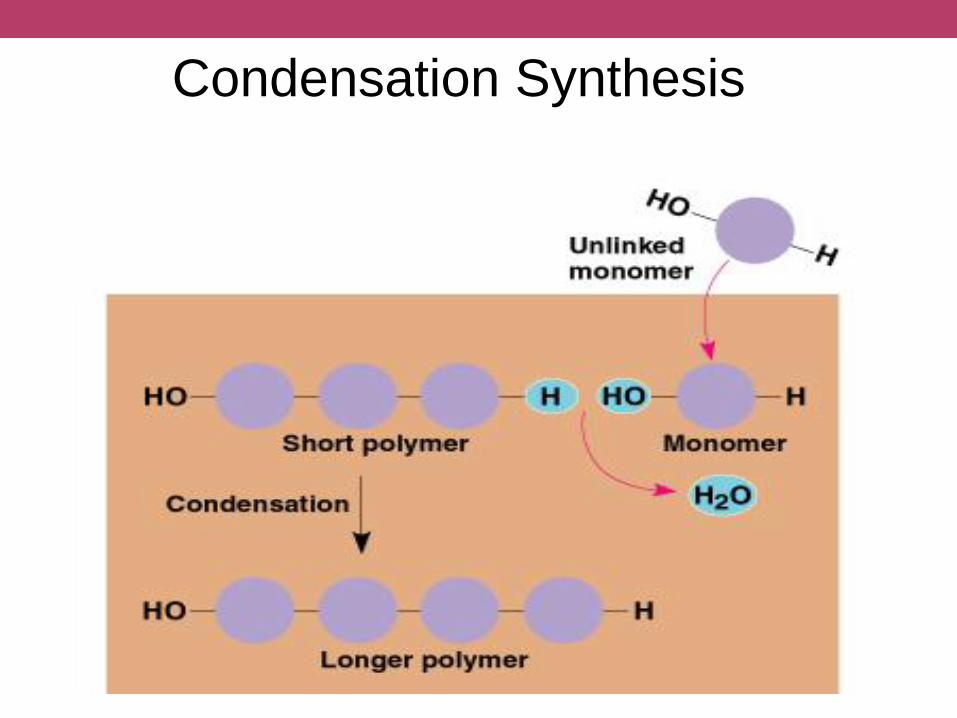
Condensation Synthesis
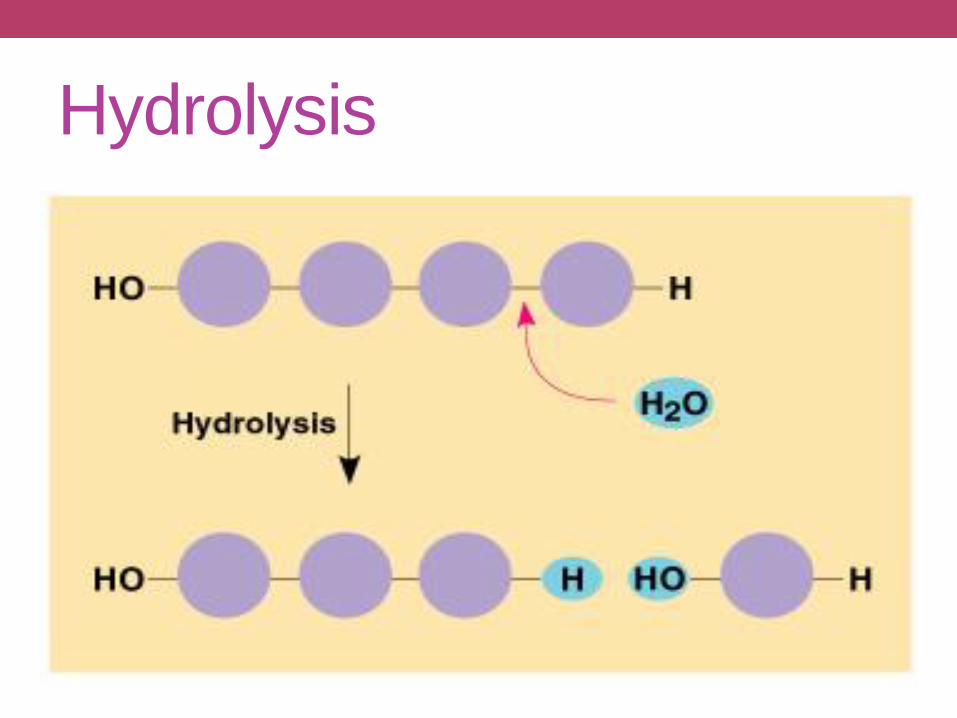
Hydrolysis
• What is a hydrolysis reaction?
• Polymers are broken down into monomers.
• Hydro = water; lysis = loosening/
• Water is added and the lysis of the polymer occurs.
Hydrolysis
II. Classes of Organic Molecules:
• What are the four classes of organic molecules?
• Carbohydrates
• Lipids
• Proteins
• Nucleic Acids
A-CARBOHYDRATE
A. Carbohydrates• Sugars
• Carbo = carbon, hydrate = water; carbohydrates have
the molecular formula (CH2O)n
• Functions:
• Store energy in chemical bonds
• Glucose is the most common monosaccharide
• Glucose is produced by photosynthetic autotrophs
• Carbohydrates are placed in to one of three catagories,
depending on the number of monosaccharide units, or
residues, they contain.
• Monosaccharides, contain a single monosaccharide residue.
• Oligosaccharides, contain 2 to 10 monosaccharide residues.
• These include the disaccharides, which contain 2 monosaccharide
residues.
• Polysaccharides, which contain more than 10 monosaccharide
residues.
• These can contain thousands of monosaccharide residues.
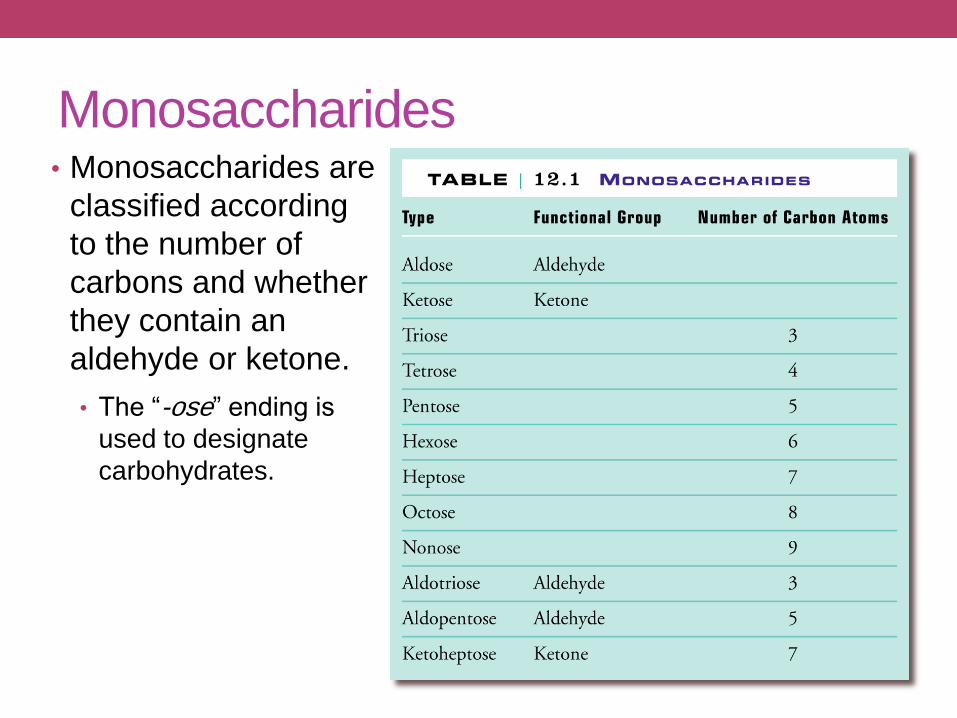
Monosaccharides• Monosaccharides are
classified according
to the number of
carbons and whether
they contain an
aldehyde or ketone.
• The “-ose” ending is
used to designate
carbohydrates.
Monosaccharides
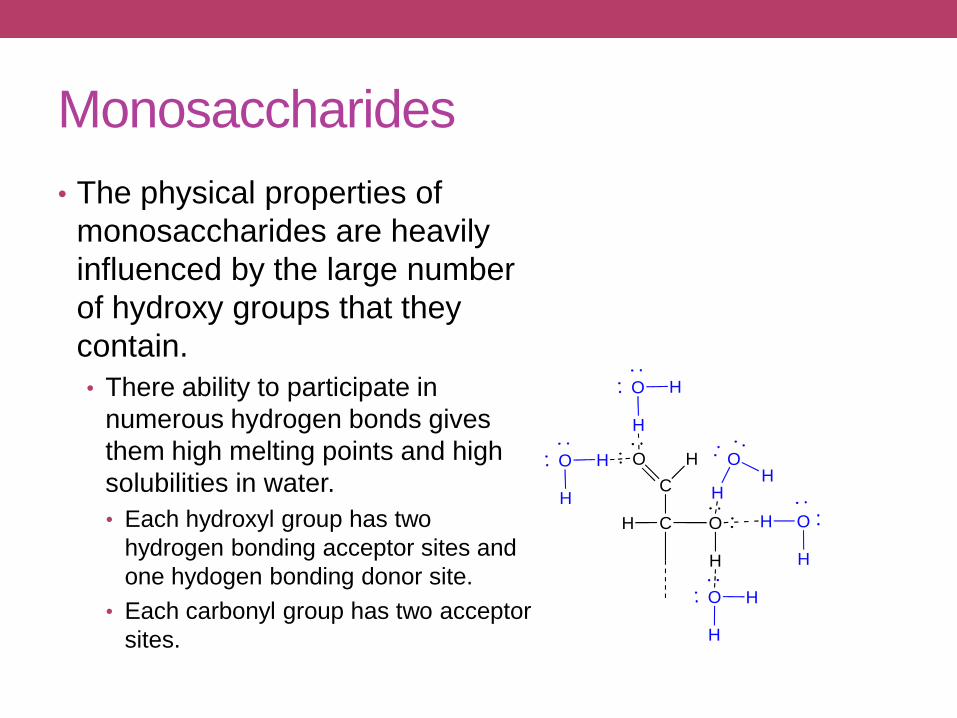
• The physical properties of
monosaccharides are heavily
influenced by the large number
of hydroxy groups that they
contain.
• There ability to participate in
numerous hydrogen bonds gives
them high melting points and high
solubilities in water.
• Each hydroxyl group has two
hydrogen bonding acceptor sites and
one hydogen bonding donor site.
• Each carbonyl group has two acceptor
sites.
C
C
O H
O
H
H
H
O H
H O
H
H
OH
H
O H
H
O H
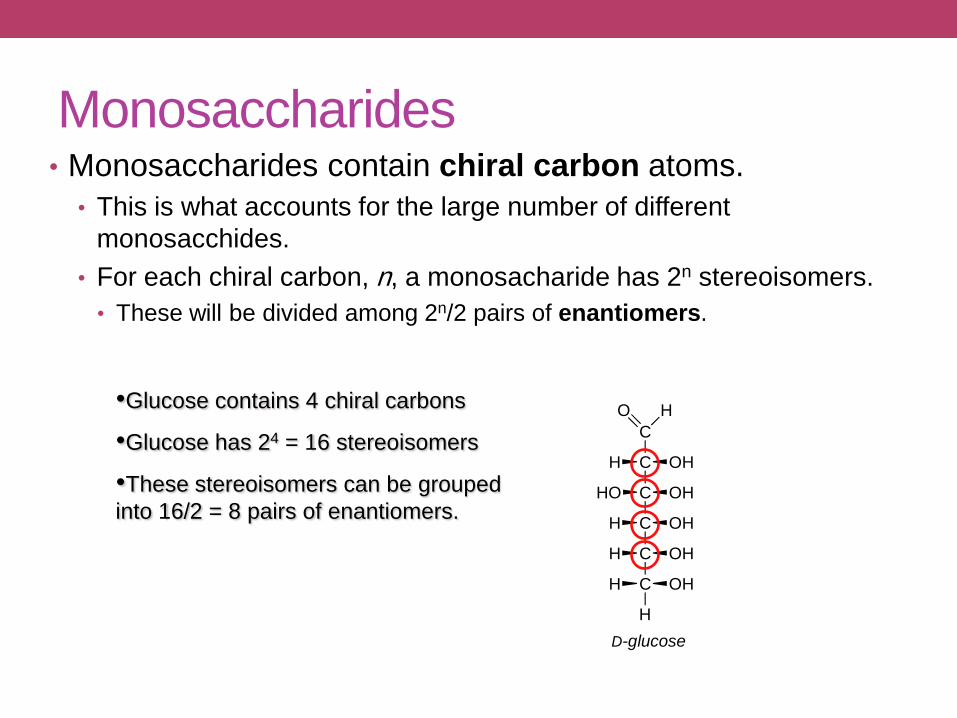
Monosaccharides• Monosaccharides contain chiral carbon atoms.
• This is what accounts for the large number of different
monosacchides.
• For each chiral carbon, n, a monosacharide has 2n stereoisomers.
• These will be divided among 2n/2 pairs of enantiomers.
•Glucose contains 4 chiral carbons
•Glucose has 24 = 16 stereoisomers
•These stereoisomers can be grouped
into 16/2 = 8 pairs of enantiomers.
O
C
H
C
C
C
C
C
H
H
HO
H
H
H OH
OH
OH
OH
OH
D-glucose
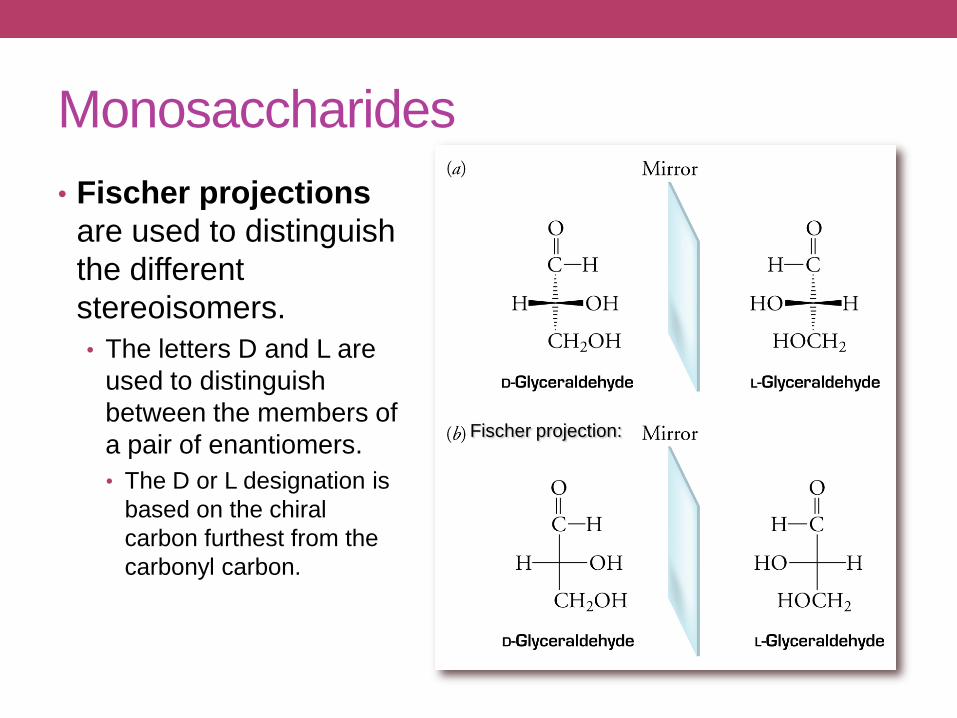
Monosaccharides
• Fischer projections
are used to distinguish
the different
stereoisomers.
• The letters D and L are
used to distinguish
between the members of
a pair of enantiomers.
• The D or L designation is
based on the chiral
carbon furthest from the
carbonyl carbon.
Fischer projection:
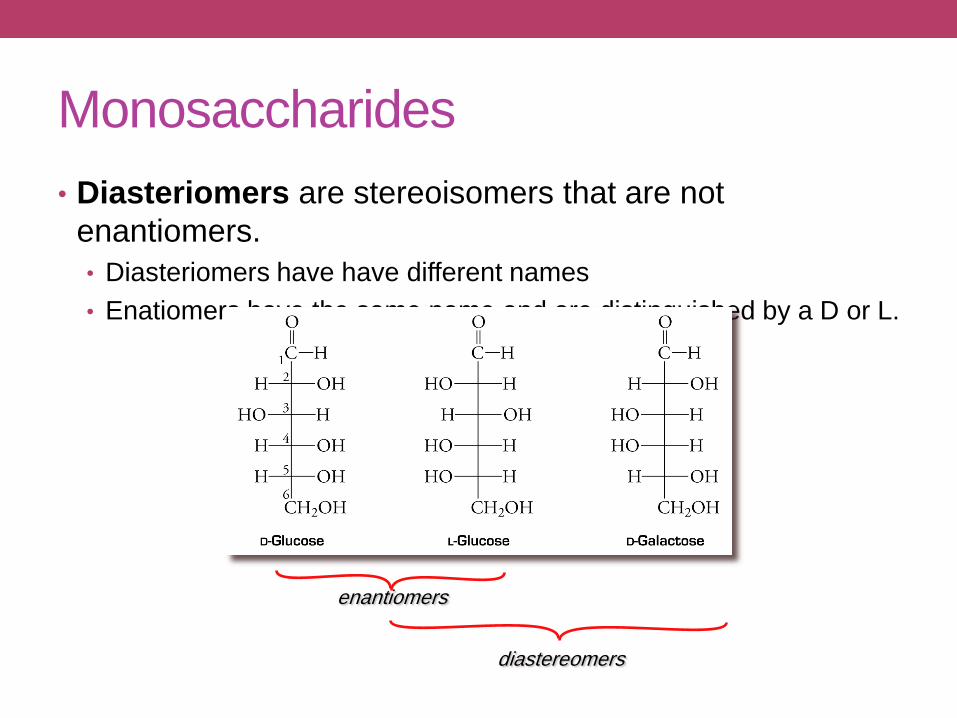
Monosaccharides
• Diasteriomers are stereoisomers that are not
enantiomers.
• Diasteriomers have have different names
• Enatiomers have the same name and are distinguished by a D or L.
enantiomers
diastereomers

Monosaccharides
• Important monosaccharides.
• pentose and hexoses are the most abundant
• Pentoses
• D-ribose and D-2-deoxyribose are found in DNA, RNA and
nucleotides such as FADH2 and NADH

Monosaccharides
• Important monosaccharides.
• pentose and hexoses are the most
abundant
• Hexoses
• D-glucose (dextrose or blood surgar) -
major metabolite and strorage form of
chemical energy.
• D-galactose - combines with glucose to
produce lactose (milk sugar)
• D-fructose (fruit sugar) - major metabolite
and sweetest tasting natural sugar.
• fructose is a ketose
25
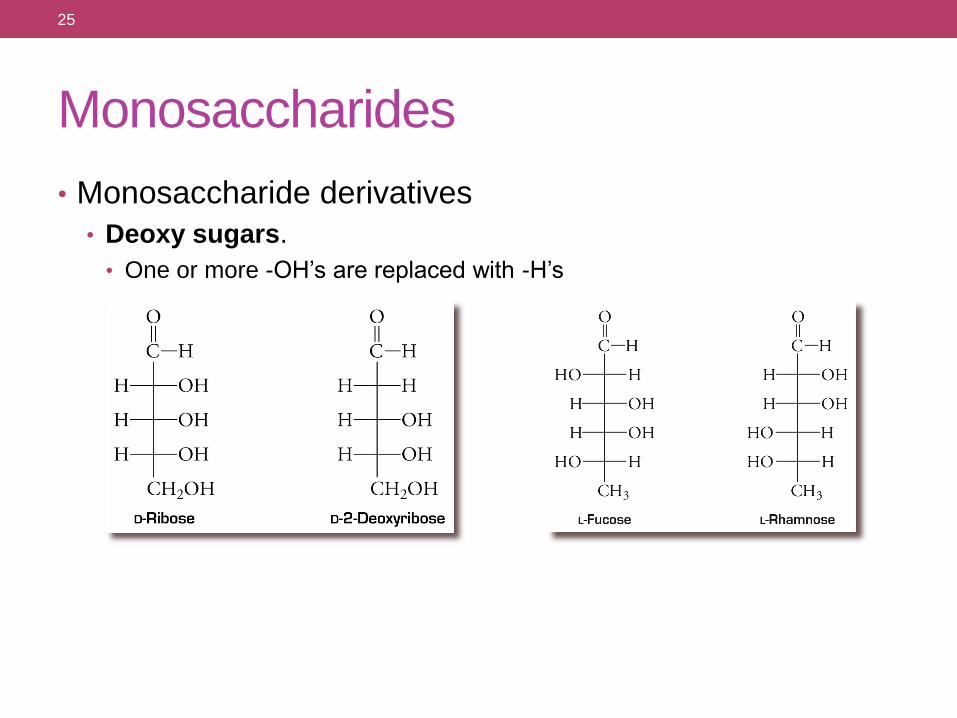
Monosaccharides
• Monosaccharide derivatives
• Deoxy sugars.
• One or more -OH’s are replaced with -H’s
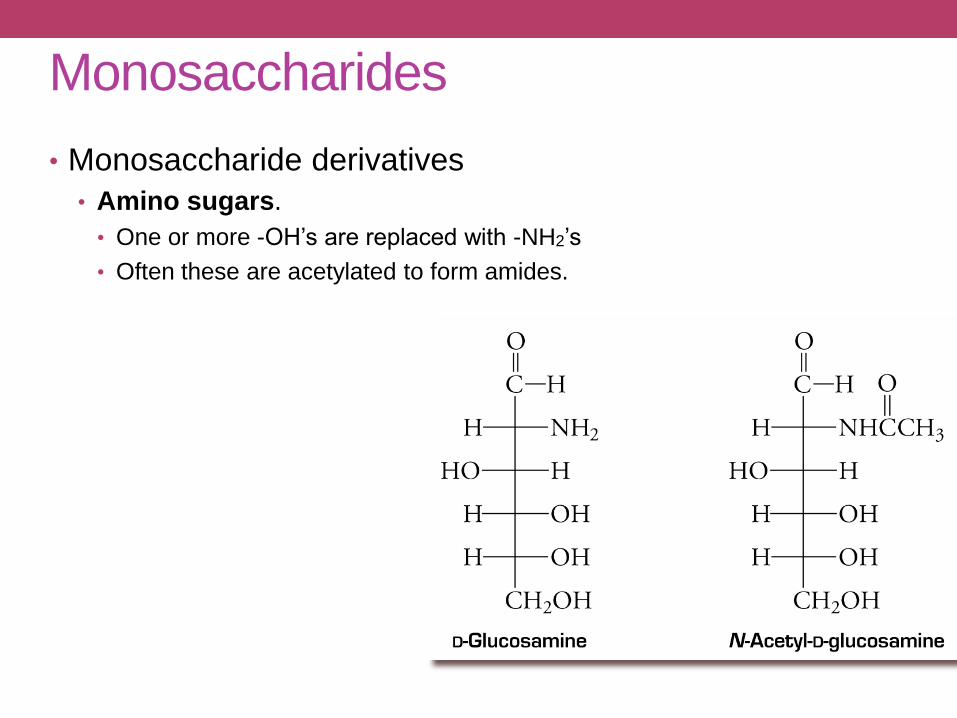
Monosaccharides
• Monosaccharide derivatives
• Amino sugars.
• One or more -OH’s are replaced with -NH2’s
• Often these are acetylated to form amides.
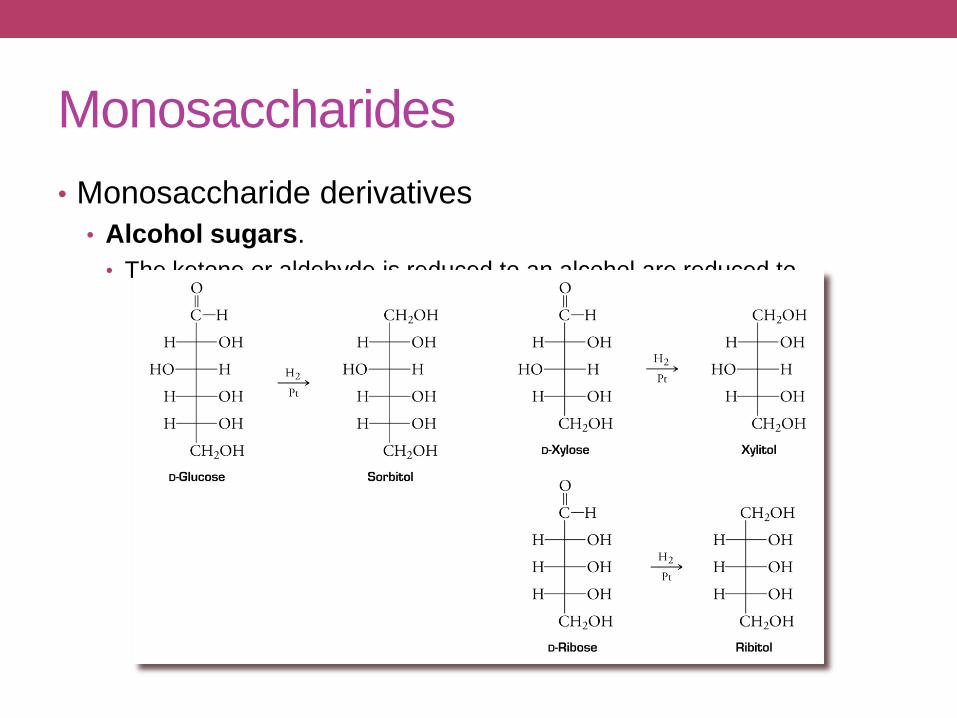
Monosaccharides
• Monosaccharide derivatives
• Alcohol sugars.
• The ketone or aldehyde is reduced to an alcohol are reduced to

Monosaccharides
• Monosaccharide derivatives
• Carboxylic acid sugars.
• The ketone, aldehyde, or primary alcohol is oxidized to a carboxylic acid.
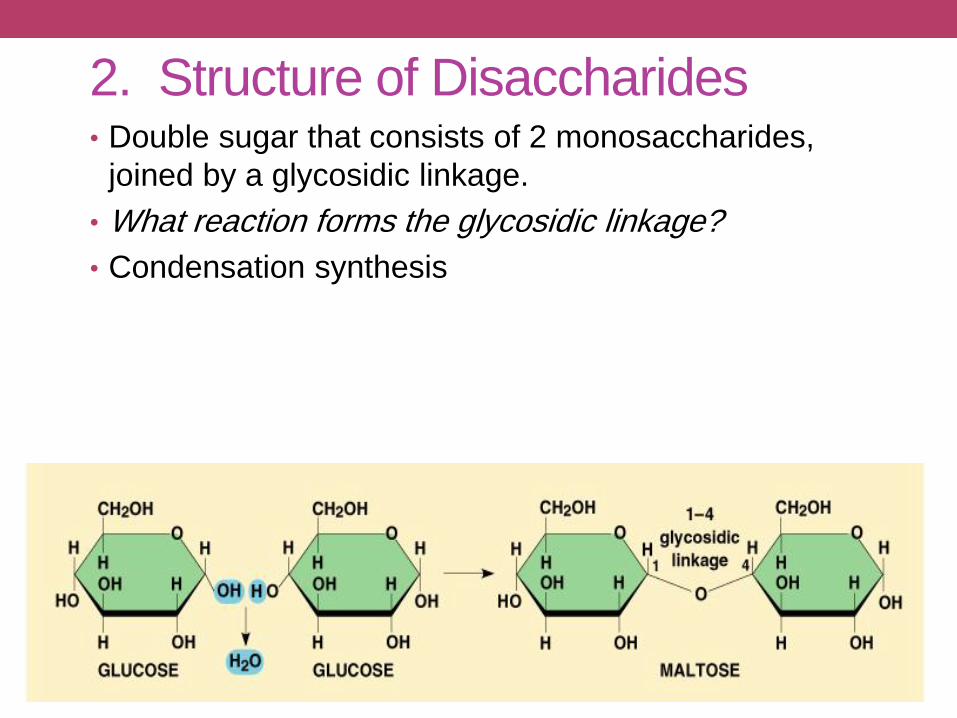
2. Structure of Disaccharides• Double sugar that consists of 2 monosaccharides,
joined by a glycosidic linkage.
• What reaction forms the glycosidic linkage?
• Condensation synthesis
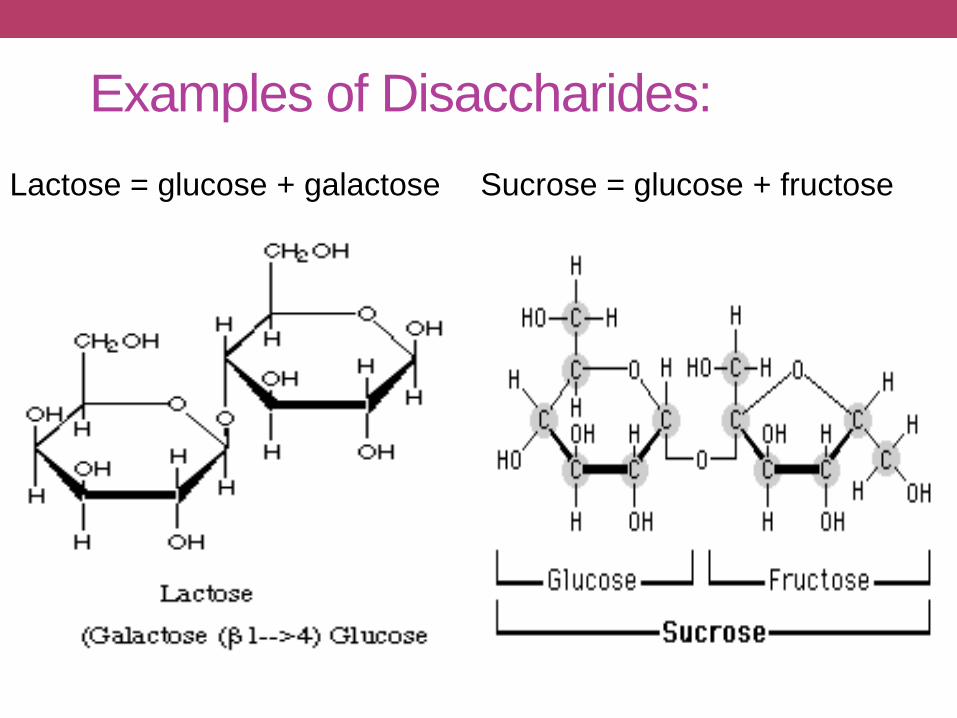
Examples of Disaccharides:
Lactose = glucose + galactose Sucrose = glucose + fructose
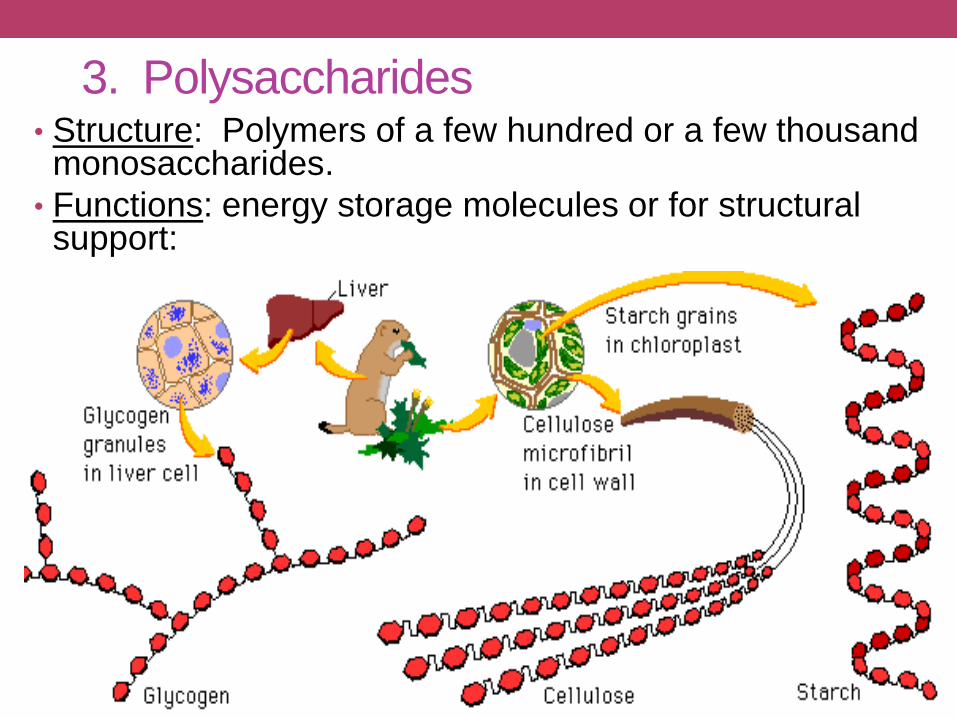
3. Polysaccharides• Structure: Polymers of a few hundred or a few thousand monosaccharides.
• Functions: energy storage molecules or for structural support:
• Starch is a plant storage from of energy, easily
hydrolyzed to glucose units
• Cellulose is a fiber-like structureal material - tough and
insoluble - used in plant cell walls
• Glycogen is a highly branched chain used by animals to
store energy in muscles and the liver.
• Chitin is a polysaccharide used as a structural material
in arthropod exoskeleton and fungal cell walls.

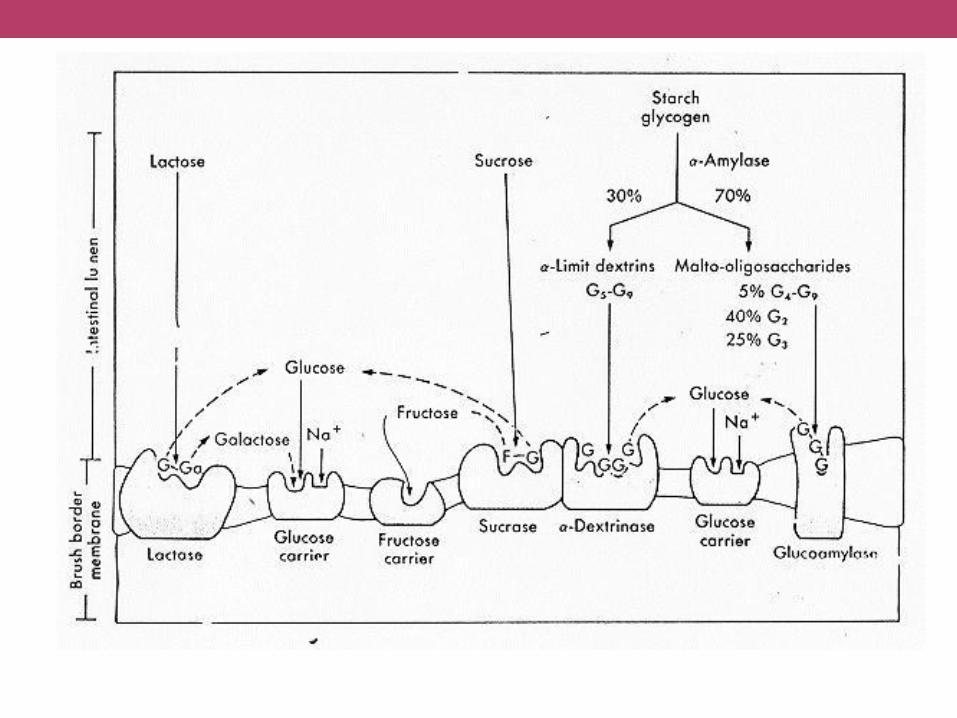
CARBOHYDRATE DIGESTION
AND ABSORPTION
Carbohydrate Digestion
• break down into glucose• body is able to absorb and use
• large starch molecules• extensive breakdown
• disaccharides• broken once
• monosaccharides• don’t need to be broken down
• begins in mouth
• chewing releases saliva
• enzyme amylase hydrolyzes starch to polysaccharides and maltose
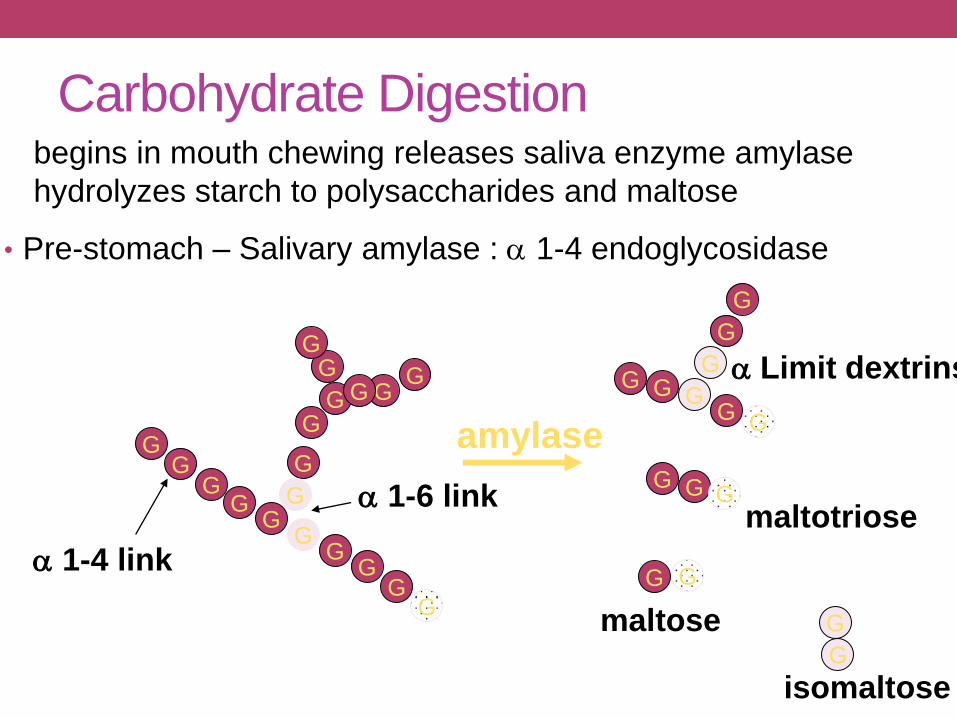
• Pre-stomach – Salivary amylase : a 1-4 endoglycosidase
GG
GG
G
GG
Ga 1-4 linkG
G
G
G a 1-6 link
G
GG
GGG G G G
G
G
G
G G
G
maltose
G
G
G
isomaltose
amylase
maltotriose
G
G
G
G
a Limit dextrins
Carbohydrate Digestionbegins in mouth chewing releases saliva enzyme amylase
hydrolyzes starch to polysaccharides and maltose
Stomach
• Not much carbohydrate digestion
• Acid and pepsin to unfold proteins
• Ruminants have forestomachs with extensive
microbial populations to breakdown and
anaerobically ferment feed
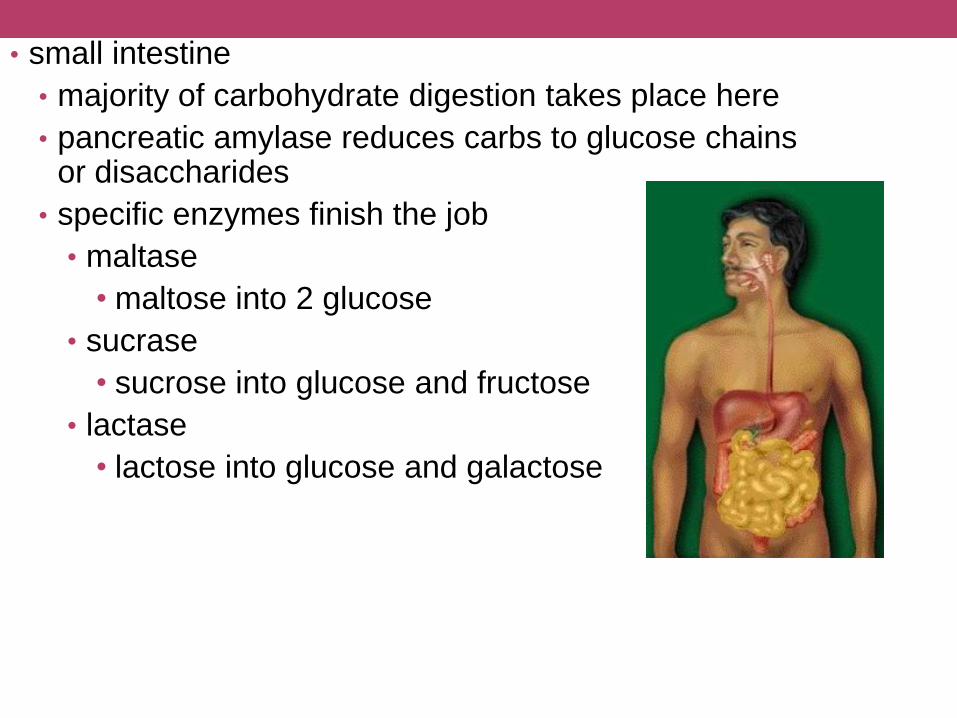
• small intestine
• majority of carbohydrate digestion takes place here
• pancreatic amylase reduces carbs to glucose chains or disaccharides
• specific enzymes finish the job
• maltase
• maltose into 2 glucose
• sucrase
• sucrose into glucose and fructose
• lactase
• lactose into glucose and galactose
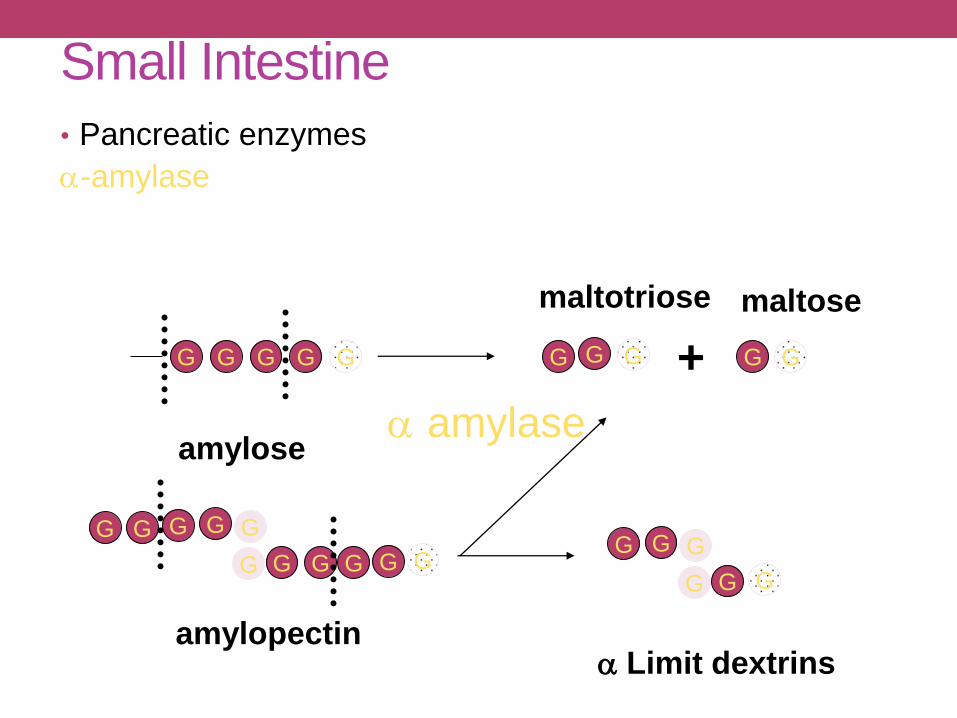
Small Intestine
• Pancreatic enzymes
a-amylase
G G GG G
G
G G G
G G GG
GG G
amylose
amylopectin
G G G G G
a amylase
+
G
G G
G G
maltotriose maltose
a Limit dextrins
G
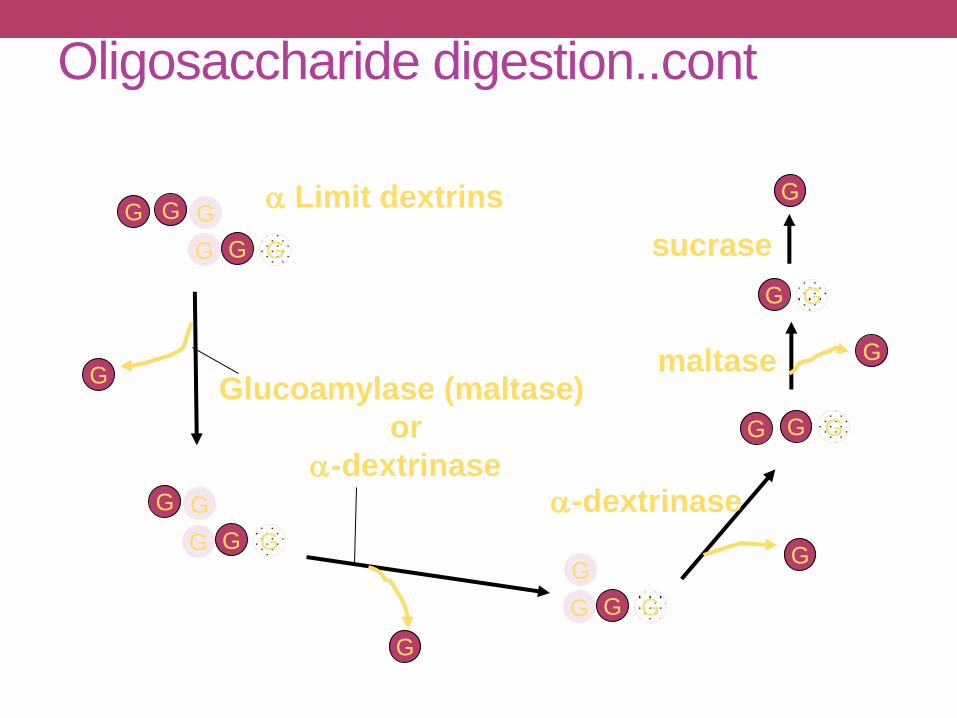
Oligosaccharide digestion..cont
G
G G
G G
G
G
G
G G
G
G
Glucoamylase (maltase)
or
a-dextrinase
G G
G
G
G
a-dextrinase
G GG
G
G G
Gmaltase
sucrase
a Limit dextrins G
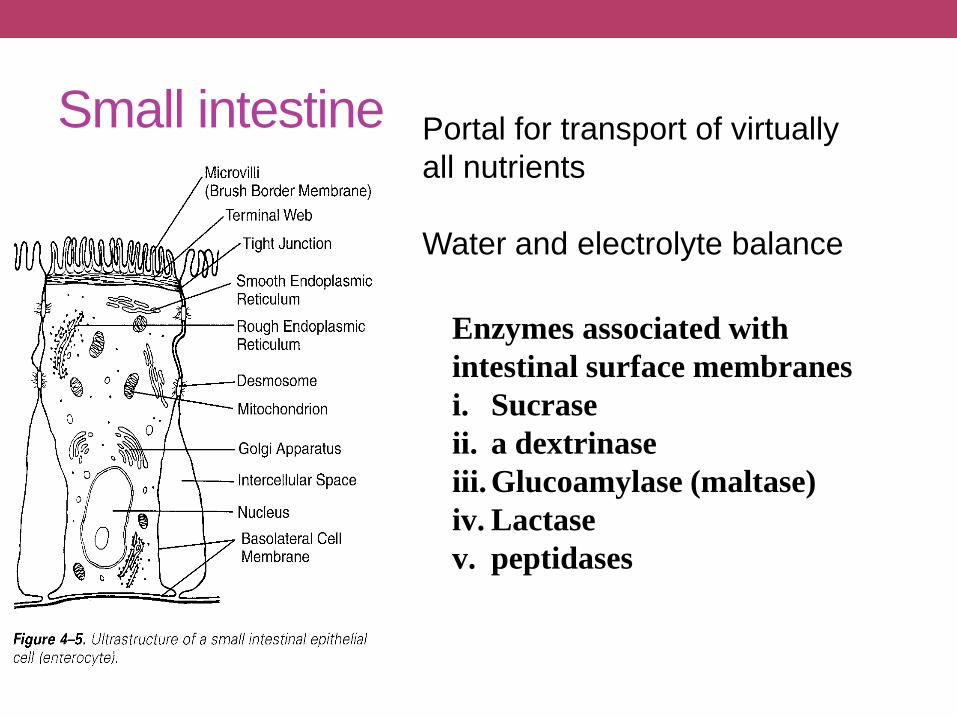
Small intestine Portal for transport of virtually
all nutrients
Water and electrolyte balance
Enzymes associated with
intestinal surface membranes
i. Sucrase
ii. a dextrinase
iii. Glucoamylase (maltase)
iv. Lactase
v. peptidases

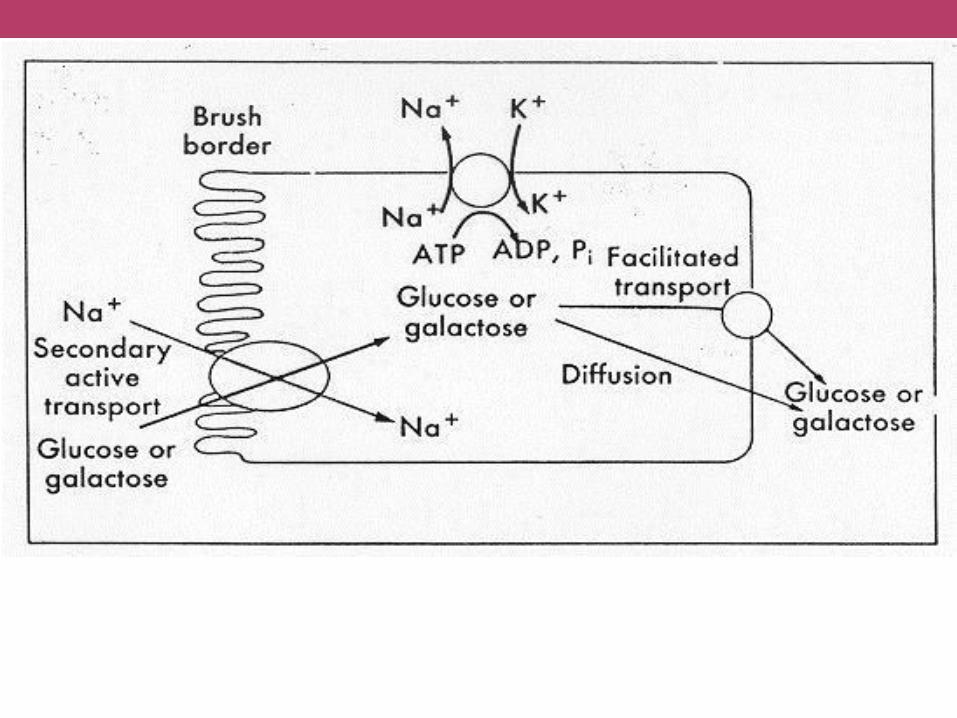
Carbohydrate absorption
apical basolateral


• large intestine
• 1-4 hours for sugars and starches to be digested
• only fibers remain
• attract water, which softens stool
• bacteria ferment some fibers
• water, gas, short-chain fatty acids (used for energy)

Carbohydrate Absorption
• glucose can be absorbed in the mouth
• majority absorbed in small intestine
• active transport
• glucose and galactic
• facilitated diffusion
• fructose
• smaller rise in blood glucose
Lactose Intolerance• more lactose is consumed than can be digested
• lactose molecules attract water
• cause floating, abdominal discomfort, diarrhea
• intestinal bacteria feed on undigested lactose
• produce acid and gas

Lactose Intolerance
• age, damage, medication, diarrhea, malnutrition
• management requires dietary change
• 6 grams (1/2 cup) usually tolerable
• take in gradually
• hard cheeses & cottage cheese
• enzyme drops or tablets
• lactose free diet is extremely difficult to accomplish
CARBOHYDRATE
METABOLISM
Carbohydrate Metabolism• 1/3 of body’s glycogen is stored in liver
• released as glucose to bloodstream
1. eat – intake glucose
2. liver condenses extra glucose to glycogen
3. blood glucose falls
4. liver hydrolyzes glycogen to glucose
Glycogen is bulky, so we store only so much: short term energy supply
Fat is the long term energy supply.
Glucose for Energy
• enzymes break apart glucose – yielding energy
• inadequate supply of carbohydrates• ketone bodies (fat fragments) are an alternate energy source
during starvation
• excess ketones can lead to ketosis: imbalance of acids in body
• minimum of 50 – 100 grams of carbs/day are needed to avoid ketosis
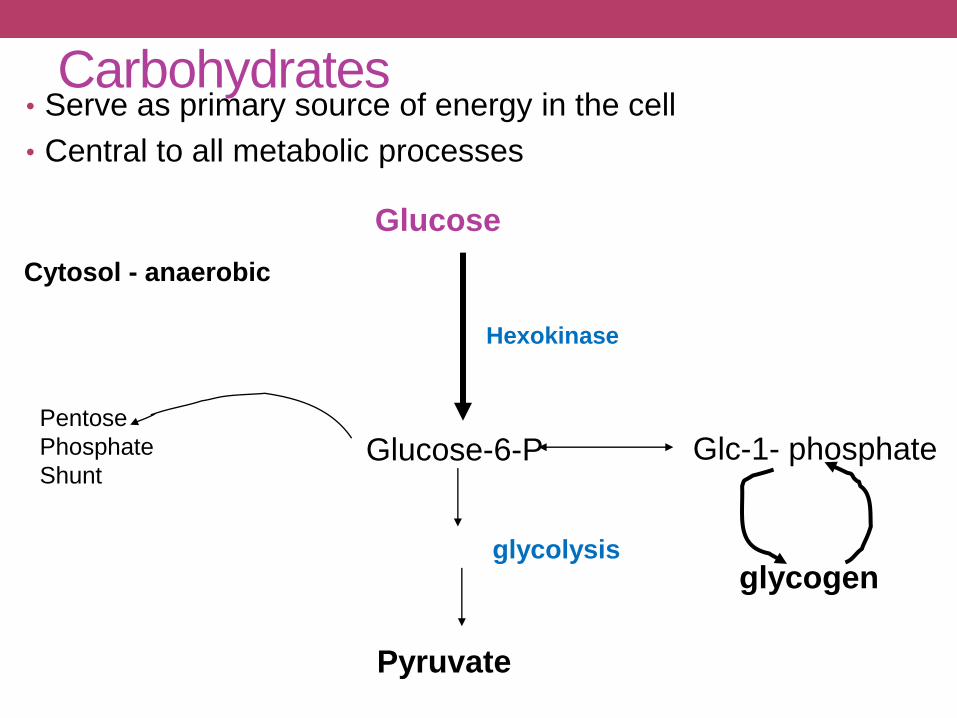
Glucose
Glucose-6-P
Pyruvate
Hexokinase
Pentose
Phosphate
Shunt
glycolysis
Carbohydrates• Serve as primary source of energy in the cell
• Central to all metabolic processes
Glc-1- phosphate
glycogen
Cytosol - anaerobic

Pyruvatecytosol
Aceytl CoAmitochondria
(aerobic)
Krebs
cycleReducing
equivalents
Oxidative
Phosphorylation
(ATP)
AMINO
ACIDS
FATTY ACIDS
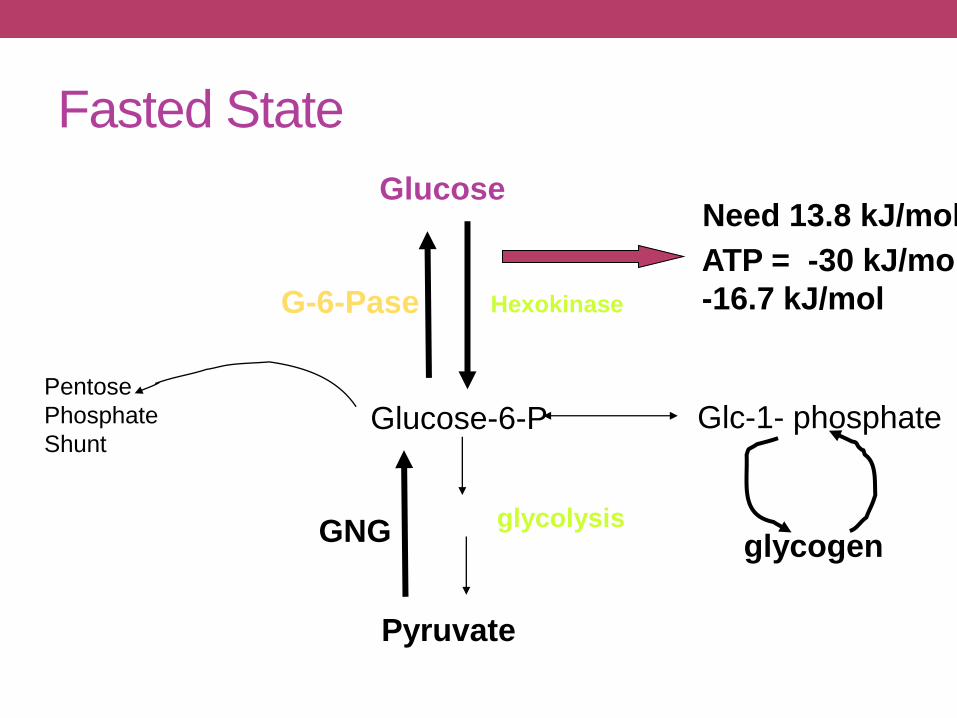
Fasted State
Glucose
Glucose-6-P
Pyruvate
Hexokinase
Pentose
Phosphate
Shunt
glycolysis
Glc-1- phosphate
glycogen
Need 13.8 kJ/mol
ATP = -30 kJ/mol
-16.7 kJ/mol
GNG
G-6-Pase
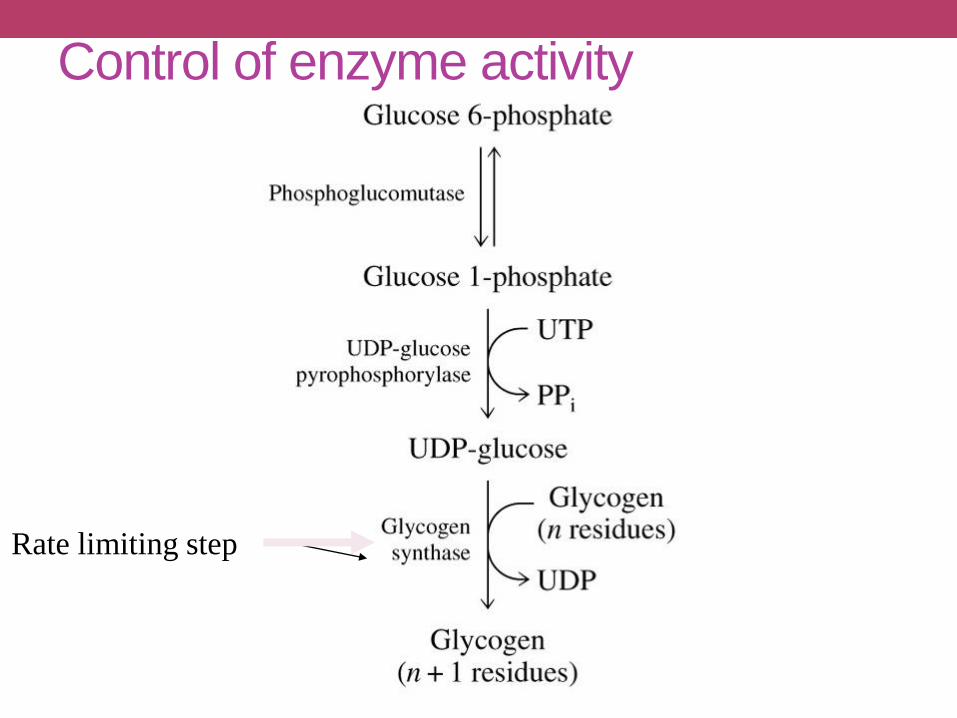
Control of enzyme activity
Rate limiting step
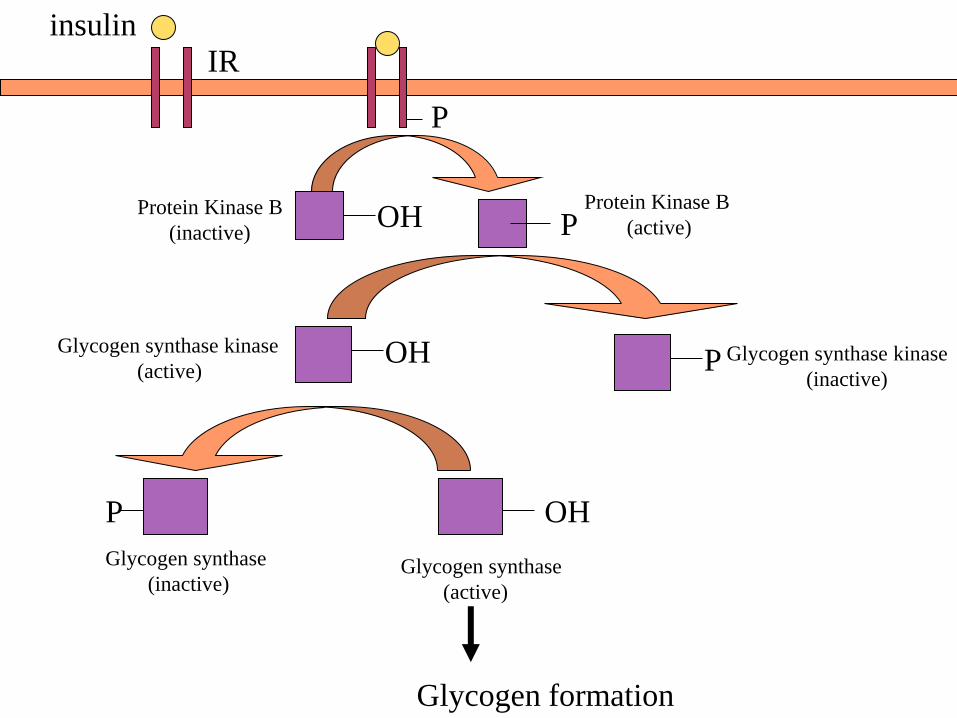
Glycogen synthase
(active)
OHP
Glycogen synthase
(inactive)
Glycogen formation
Glycogen synthase kinase
(active)OH
IRinsulin
P
PProtein Kinase B
(active)Protein Kinase B
(inactive)OH
P Glycogen synthase kinase
(inactive)
Carbohydrate Metabolism/ Utilization-
Tissue Specificity• Muscle – cardiac and skeletal
• Oxidize glucose/produce and store glycogen (fed)• Breakdown glycogen (fasted state)• Shift to other fuels in fasting state (fatty acids)
• Adipose and liver• Glucose acetyl CoA• Glucose to glycerol for triglyceride synthesis• Liver releases glucose for other tissues
• Nervous system• Always use glucose except during extreme fasts
• Reproductive tract/mammary• Glucose required by fetus• Lactose major milk carbohydrate
• Red blood cells• No mitochondria• Oxidize glucose to lactate• Lactate returned to liver for Gluconeogenesis

Glucose Homeostasis
• maintaining an even balance of glucose is controlled by
insulin and glucagon
• insulin
• moves glucose into the blood
• glucagon
• brings glucose out of storage
• maintaining balance
• balanced meals at regular intervals
• fiber and some fat slow the digestive process down
• glucose gets into the blood slow and steady
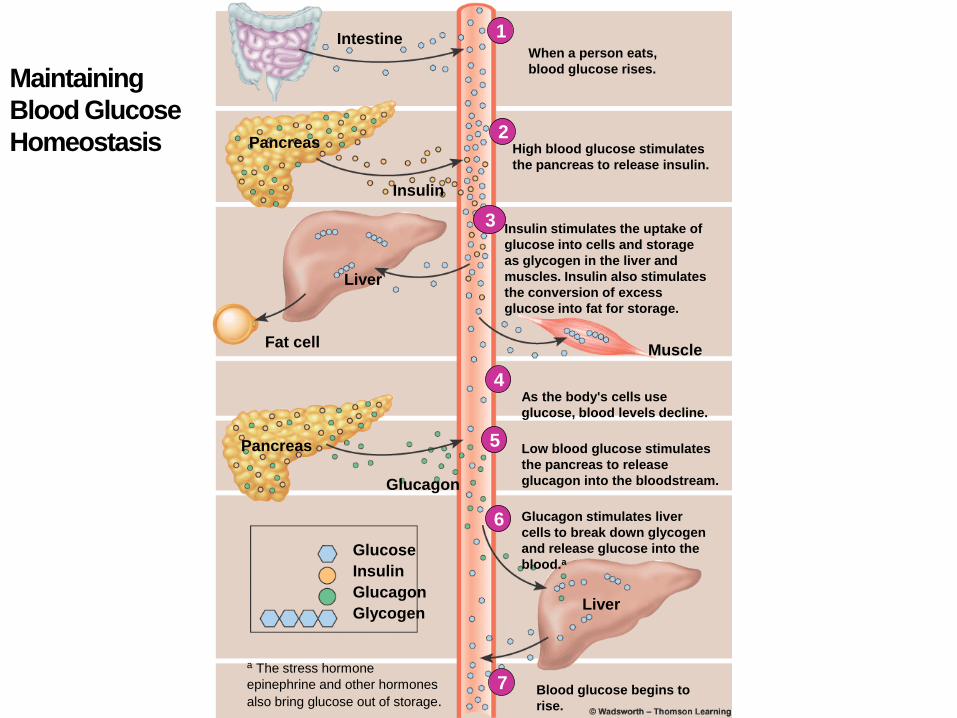
Maintaining
Blood Glucose
Homeostasis
IntestineWhen a person eats,
blood glucose rises.
1
2
Insulin stimulates the uptake of
glucose into cells and storage
as glycogen in the liver and
muscles. Insulin also stimulates
the conversion of excess
glucose into fat for storage.
3
4
5
6
7 Blood glucose begins to
rise.
a The stress hormone
epinephrine and other hormones
also bring glucose out of storage.
Glucose
Insulin
Glucagon
Glycogen
Glucagon stimulates liver
cells to break down glycogen
and release glucose into the
blood.a
Liver
Low blood glucose stimulates
the pancreas to release
glucagon into the bloodstream.
As the body's cells use
glucose, blood levels decline.
Glucagon
Pancreas
Fat cell
Liver
Muscle
High blood glucose stimulates
the pancreas to release insulin.
Pancreas
Insulin
Imbalance
• diabetes• after food intake, blood glucose rises and is not regulated because
insulin is inadequate
• hypoglycemia• blood glucose drops dramatically
• too much insulin, activity, inadequate food intake, illness
• diet adjustment includes fiber-rich carbs and protein
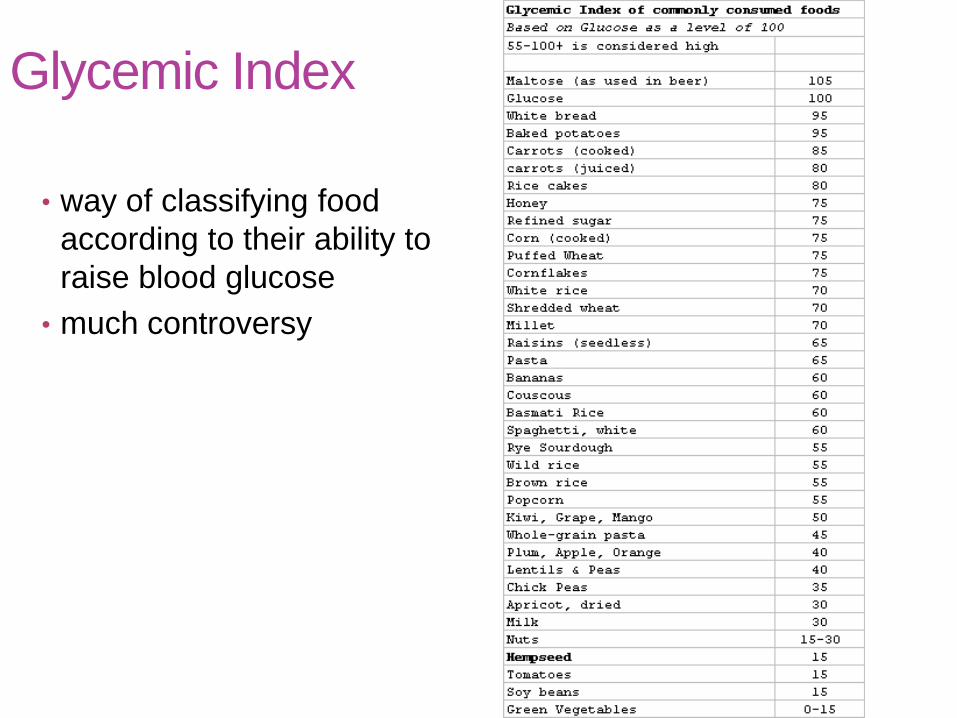
Glycemic Index
• way of classifying food
according to their ability to
raise blood glucose
• much controversy
Sugar
• ½ comes from natural sources, ½ from refined and
added
• sucrose, corn syrup, honey
• excess can lead to nutrient deficiencies and tooth
decay
• empty calories
• sugar and starch break down in the mouth
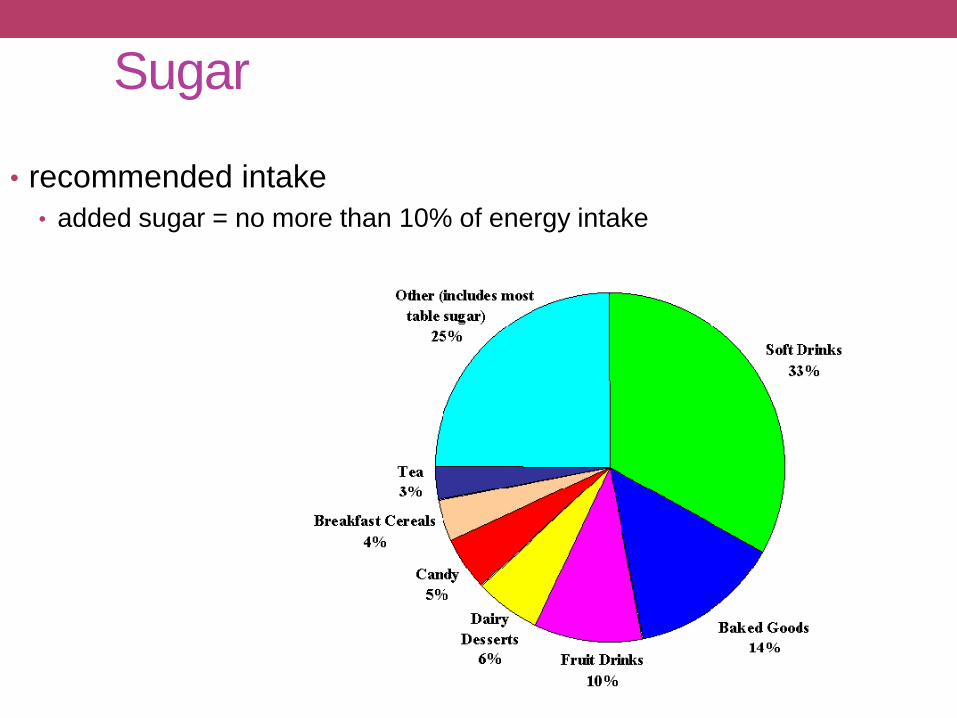
Sugar
• recommended intake
• added sugar = no more than 10% of energy intake

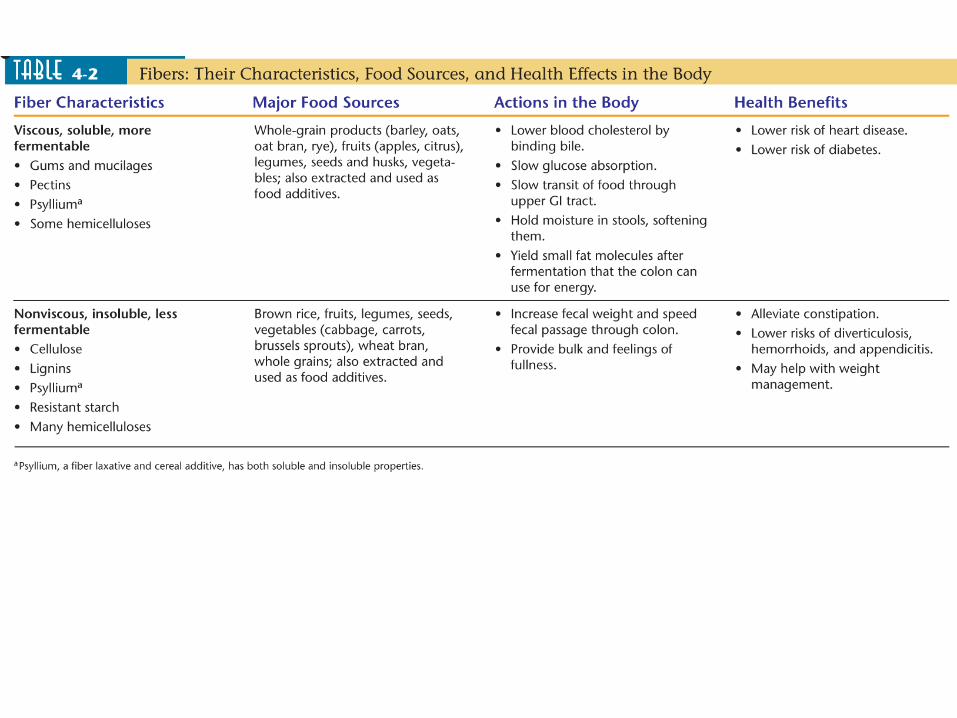
Starch and Fiber
• diet that includes starch, fiber and natural sugars
• whole grains, vegetables, legumes, fruits
• may protect against heart disease and stroke
• reduces the risk of type 2 diabetes
• enhances the health of the large intestine
• can promote weight loss
Starch and Fiber• starch intake
• 45-65%
• 225 – 325 grams (DV is 300 grams)
• 900-1300 kcal/2000 kcal
• RDA is 130 grams
• fiber intake
• Daily Value is 25 grams/2000 kcal

Artificial Sweeteners
• help keep sugar and energy intake down
• anything we eat has FDA approval
• saccharin
• aspartame
• acesulfame potassium
• sucralose
• neotame

Sugar Replacers
• sugar alcohols
• provide bulk and sweetness
• cookies, gum, candy, jelly
• do contain minimal kcal
• low glycemic response
• absorbed slowly
• do not cause dental caries
DISTURBANCE IN
CARBOHYDRATE METABOLISM
1. Disaccharidase deficiency syndrome
saccharase = enzyme which hydrolyses disaccharide
saccharose (to fructose and glucose)
laktase = enzyme which splits disaccharide lactose
(to glucose and galactose)
maltase = enzyme which splits disaccharide maltose
(to two molecule of glucose)
Pathomechanisms
a) Activity of disaccharidase is decreased decreased
hydrolysis of disaccharide decreased resorbtion of substrate
increased concentration of disaccharide in small intestine
lumen increased osmotic activity of the lumen fluid
diarrhea
b) Activity of disaccharidase is decreased increased
concentration of disaccharide in small intestine lumen
increased concentration of disaccharide in large intestine
disaccharide fermentation by bacteria increased
concentration of lactic acid and fatty acids
stimulation of intestine wall abdominal cramps,
bloating, diarrhea, acidic stools, explosive diarrhea
Lactase deficiency syndrome
Causes of lactase deficiency:
- genetic defect (primary)
- secondary to a wide variety of gastrointestinal diseases
that damage the mucosa of the small intestine (secondary)
Disaccharide lactose is the principal carbohydrate in milk.
- Many persons showing milk intolerance prove to be lactase –
deficient
- Primary lactase deficiency incidence is as high as 80 % to 90 % among African - Americans, Asians, and Bantus population
- Milk intolerance may not become clinically apparent until
adolescence
Causes of secondary lactase deficiency:
- nontropical (celiac disease)and tropical sprue,
- regional enteritis,
- viral and bacterial infections of the intestinal tract,
- giardiasis, cystic fibrosis, ulcerative colitis,
- kwashiorkor, coeliac disease
Symptoms and signs - are mentioned at previous page
Monosaccharides malabsorbtion
Small intestine ability to resorb glucose and galactose is
decreased
Cause: Specific transport system for galactose and glucose
absorbtion in cells of small intestine is insufficient
Results: Symptoms and signs similar to disaccharidase
deficiency syndrome
Glycogenosis (glycogen storage disease)
Autosomal recessive disease (inborn errors of metabolism,
emzymopathy)
There are defects in degradation of glycogen.
The disturbances result in storage of abnormal glycogen,
or storage of abnormal amount of glycogen in various organs of the body
Example: Hepatorenal glycogenosis (Morbus von Gierke)
Cause: Deficit of glucose-6-fosfatase in liver and kidney
Results: Hypoglycemia in fasting individuals,
hyperlipemia, ketonemia
There are 9 other types of glycogenosis
DIABETES MELLITUS
DM – complex chronic metabolic disorder leading to multiorgan complications
Main pathophysiological questions related to DM
Why and how the DM develops?
Why and how develop the complications of DM?
What are the mechanisms involved in manifestationof diabetic symptoms and signs
Regulation of the blood glucose level depends on liver:
1. extracting glucose from blood
2. synthesizing glycogen
3. performing glycogenolysis
4. performing gluconeogenesis
To a lesser extent peripheral tissues (muscle and adipocytes) use glucose
for their energy needs, thus contributing to maintinance of normal blood
glucose level
The livers uptake and output of glucose and the use of glucose by
peripheral tissues depend on the physiologic balance of several
hormones that:
1. lower blood glucose level - insulin
2. rise blood glucose level - glucagon, epinephrine, GH,
glucocorticoids...

DM is a chronic complex syndrome induced by absolute or relative
deficit of insuline which is characterized by metabolic disorders of
carbohydrates, lipids and proteins.
The metabolic disturbances are accompanied by loss of carbohydrate
tolerance, fasting hyperglycemia, ketoacidosis, decreased
lipogenesis, increased lipolysis, increased proteolysis and some
other metabolic disorders
Definition of DM

I. Diabetes mellitus - type 1: due to destruction of beta
cells of pancreatic islets
Consequence: absolute deficit of insulin
A. subtype: induced by autoimmunity processes
B. subtype: idiopathic mechanism
Types of DM
II.Diabetes mellitus -type 2: at the beginning-predominance
of insulin resistance and relative deficit of insulin(normo- or
hyper -insulinemia), later on - combination of impaired insulin
secretion and simultaneous insulin resistance (hypoinsulinemia,
insulin resistance)
IV. Gestational DM -
III. Other specific types of DM
DM due to genetic defects of beta cells of pancreas islets and due
to genetic defect of insulin function
DM due to diseases influencing exocrine functions of pancreas –
- secondary is damaged endocrine function, too.
DM due to endocrinopathies, drugs, chemicals, infections,
metabolic and genetic disturbances
glucose intolerance which onsets
for the first time during pregnancy
Main differences between “old” and “new” classification
of diabetes mellitus
In new classification of DM:
- terms IDDM and NIDDM are not used
- term DM due to malnutrition is not used
- terms - primary and secondary DM are not used
New terms were introduced into new classification of DM:
* impaired fasting plasma glucose(FPG)
* impaired glucose tolerance(IGT)
Why?
Normal fasting value of plasmatic glucose concentration:
6.1 mmol/l
● Normal value of PGTT – blood glucose concentration 2 hs
after beginning of test 7.8 mmol/l
New criteria for diagnose of DM
1st: classic symptoms and signs of DM are present (polyuria,
polydipsia, weight loss), and increased day-time blood glucose
concentration to 11.1 mmol/l and more
or
2nd: fasting glucose level is 7.0 mmol/l and more
or
3rd: 2 hours glucose level in PGTT is 11.1 mmol/l and more
For confirmation of diagnosis DM positivity each of the mentioned
parameters have to be confirmed next day by positivity any of
the mentioned parameter
Impaired fasting plasma glucose:
6.1 but 7.0 mmol/l
Impaired glucose tolerance (IGT):
Glucose tolerance test shows abnormal values but these
patients are asymptomatic and they do not meet the criteria
for diagnosis of DM.
IGT criteria:
- fasting plasma glucose level can be normal
- 2 hours after intake glucose is plasma glucose level higher
than normal (from 7.8mmol/l to 11.1mmol/l)
The individuals with IGT are recognized as being at higher risk than the
general population for the development of DM (about 1.5 - 4.0 % of patients
with IGT DM).
Syndrome X (metabolic X syndrome)
- frequently occurs in people suffering form visceral obesity
Characteristic features:
insuline resistance
compensatory hyperinsulinemia
visceral obesity
dyslipidemia ( LDL, TG, HDL)
systemic hypertension
Increased probability of DM-type2 development


Insuline Resistance (IR)
IR is one of the mechanisms involved in pathogenesis of IGT
and DM, especially in DM type 2
Causes of insuline resistance:
1. autoimmune reactions
- development of anti-insulin antibodies
- development of anti-insulin receptor antibodies
2. defects in the insulin receptor at the cell surface
a) defect in receptor processing
b) decrease in receptor number
3. defective signal transduction
(from the receptor to the plasma of cell)
4. postreceptor defect
5. increased concentration of anti-insulinic hormones
Etiopathogenesis of DM
Type 1 DM - characteristics
- it is most typical in individuals under 30 years of age (juvenile DM)
- 80 % - 90 % of beta cells in the islets of Langerhans are destroyed
Possible mechanisms of beta cells destruction:
a) by islet cell antibodies of the IgG class
b) by non-immune mechanism (idiopathic up to now)
Evidence suggest that type 1 DM is caused by a gradual process
of autoimmune destruction of beta cells in genetically susceptive
individuals
The result of beta cells destruction:
- almost no or absolute no functional insulin is produced
- glucagon is present in relative excess
- individuals are prone to ketoacidosis
- insulin resistance is rare
- patients are insulin dependent

Type 2 DM - characteristics
1. Primary disturbance:
- biological activity of insuline
2. Compensatory hyperinsulinemia
- due to concentration of blood glucose
3. Insulinoresistentia:
- ability of insuline to inhibit production of glucose in
liver glucose production
Type 2 DM -characteristics
- is rare in populations not affected by urban modernization
- adult onset (mostly after 40 years of age, slow, insidious
onset)
- results from the action of several abnormal genes ; - inherited
susceptibility, familial tendency stronger than for type 1 DM
- associated with long - duration obesity (mainly visceral)
- islet of Langerhans cells antibodies are rare
- increased insulin resistance
- nonspecific changes (damage) of islet cells
- usually not insulin dependent
- individuals are not ketosis prone (but they may form
keton bodies under stress)


Main symptomes and signs of DM and mechanisms of their onset
Hyperglycemia:
relative or absolute deficiency of insulin effect transport of
glucose to muscle and fat cells glycemia
insulin effect gluconeogenesis in liver blood level of
glucose
glycogenolysis (?)
Glycosuria: hyperglycemia (8-15 mmol/l) glycosuria
Polyuria: high blood level of glucose increased amount of glucose
filtered by the glomeruli of the kidney absorbtion capacity
of renal tubules for glucose is exceeded glycosuria results,
accompanied by large amounts of water lost in the urine
(osmotic effect of glucose)
Polydipsia : high blood level of glucose hyperosmolality of plasma water moves from cells to ECF (IVF) intracellular dehydratation
creation of thirst feeling (in hypothalamus)
intake of fluids
Polyphagia: depletion of cellular stores of carbohydrates, fats,
and proteins results in cellular starvation and a
corresponding increase in hunger
Weight loss : fluid loss in osmotic diuresis, loss of body tissue
as fats and proteins are used for energy creation
Fatigue : metabolic changes result in poor use of food
products lethargy and fatique
Complications of Diabetes Mellitus
A. Acute complications
• Hypoglycemia
• Ketoacidosis
• Hyperosmolar hyperglycemic nonketotic coma
B. Chronic complications
• Diabetic micro- and macrovascular changes
• Diabetic neuropathy
• Diabetic retinopathy
• Diabetic nephropathy
• Other complications

A. Acute complications
1. Hypoglycemia ( 3.3mmol/l of blood glucose) - results from:
a) exogenous causes - overdose of insuline plus inadequate
food intake, increased exercise - overdose of oral hypoglycemic agents- alcohol- other agents (e.g. salicylates)
b) endogenous causes - insulinoma (neoplasm of beta cells
of islet of Langerhans) - extrapancreatic neoplasm (hepatomas,tumor of GIT)
- inborn errors of metabolism (fructose intolerance)
Symptoms and signs of hypoglycemia are caused by epinephrine
release (sweating, shakiness, headache, palpitation) and by lack
of glucose in the brain (bizarre behaviour, dullness, coma).

Hypoglycemia unawareness (HU)
Cause: antihypoglycemic mechanisms are insufficient
Result: hypoglycemia develops without warning
symptoms and signs
Pathomechanism involved in HU development:
• Primary defect is localised to the CNS
- or loss of neurotransmiter production on
hypoglycemic stimulus
- reactivity of peripheral tissues counterregulatory
hormones
Consequences: Deep hypoglycemia hypoglycemic coma
death

2. Diabetic ketoacidosis - the most serious metabolic
complication of DM
– It develops when there is severe insulin insufficiency
– Insulin insufficiency triggers a complex metabolic reactions
which involve:
- decreased glucose utilisation hyperglycemia and glycosuria
- acceleration of gluconeogenesis hyperglycemia
- decreased lipogenesis and increased lipolysis increase
oxidation of free fatty acids production of ketone bodies
(aceto-acetate, hydroxy-butyrate, and acetone) hyperketonemia
metabolic acidosis coma
3. Hyperosmolar hyperglycemic nonketotic coma(HHNC)(hyperosmolar hyperglycemic syndrome)
a) - insulin is present to some degree it inhibits fat
breakdown lack of ketosis
b) - insulin is present to some degree its effectivity is
less than needed for effective glucose transport
hyperglycemia glycosuria and polyuria body fluids
depletion intracellular dehydration neurologic
disturbancies (stupor, coma)


B. Chronic complications
Today, long-term survival of patient suffering from DM is the
rule. As a result, the problems of neuropathy, microvascular
disease, and macrovascular disease have become important
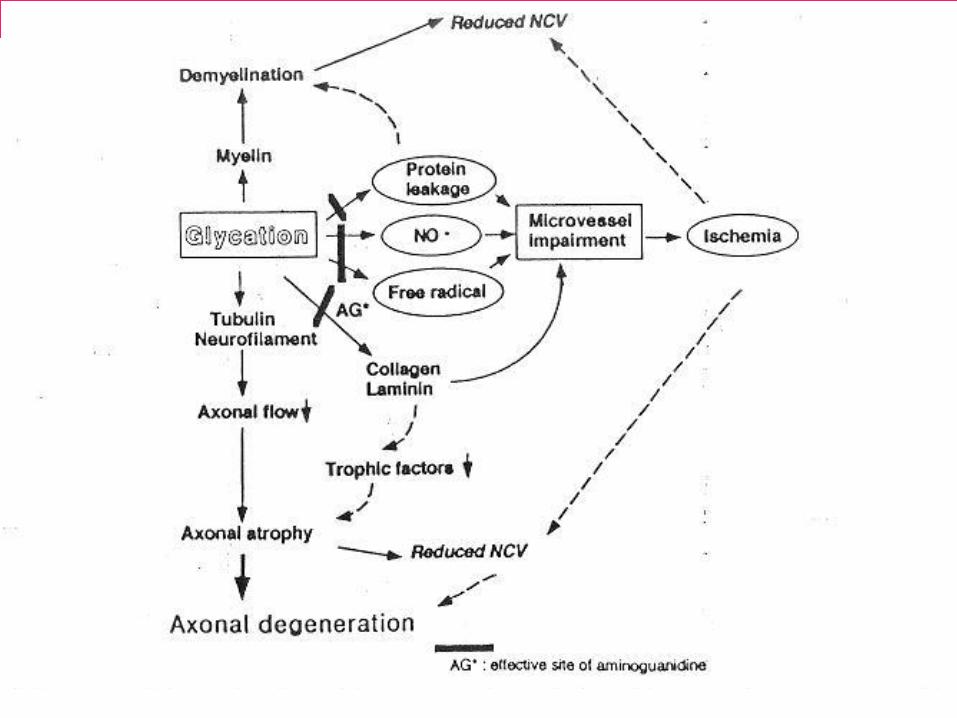
1. Diabetic neuropathies(DN) - probably the most common
complication in DM
Pathogenesis:
a) vascular damage of vasa nervorum
b) metabolic damage of nerve cels
c) non-enzymatic glycation of proteins
The very first morphologic and functional changes:
- axonal degeneration preferentially involved unmyelinated fibers
(in spinal cord, the posterior root ganglia, peripheral nerves)
Functional consequences:
- abnormalities in motor nerve function
(in advanced stages of DM)
- sensory nerve conduction is impaired
- autonomic neuropathy (diabetic diarrhea, orthostatic
hypotension....)
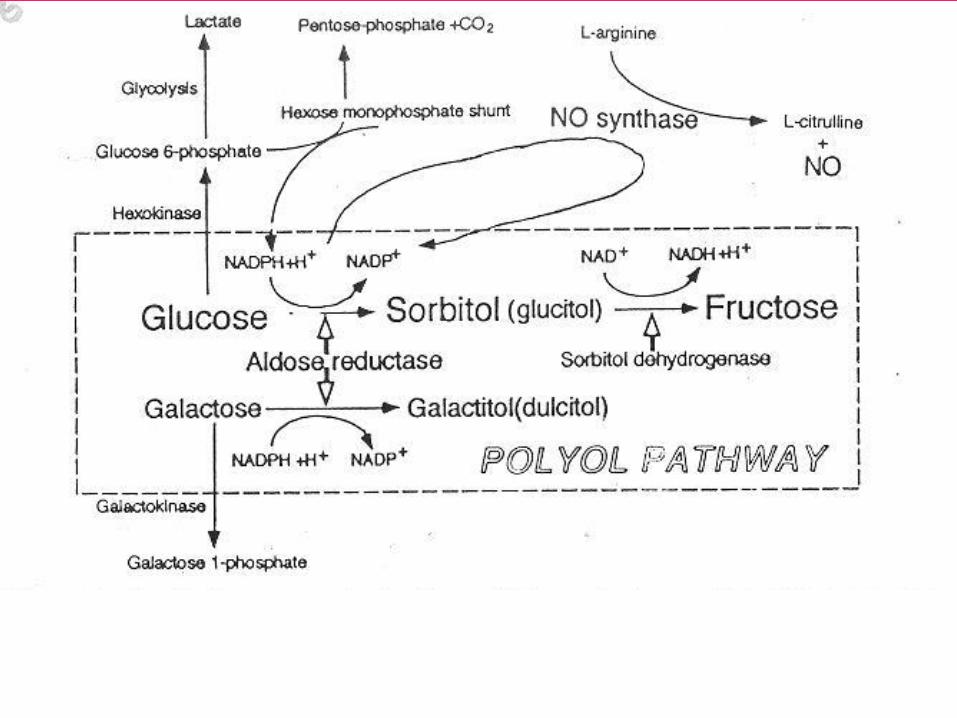
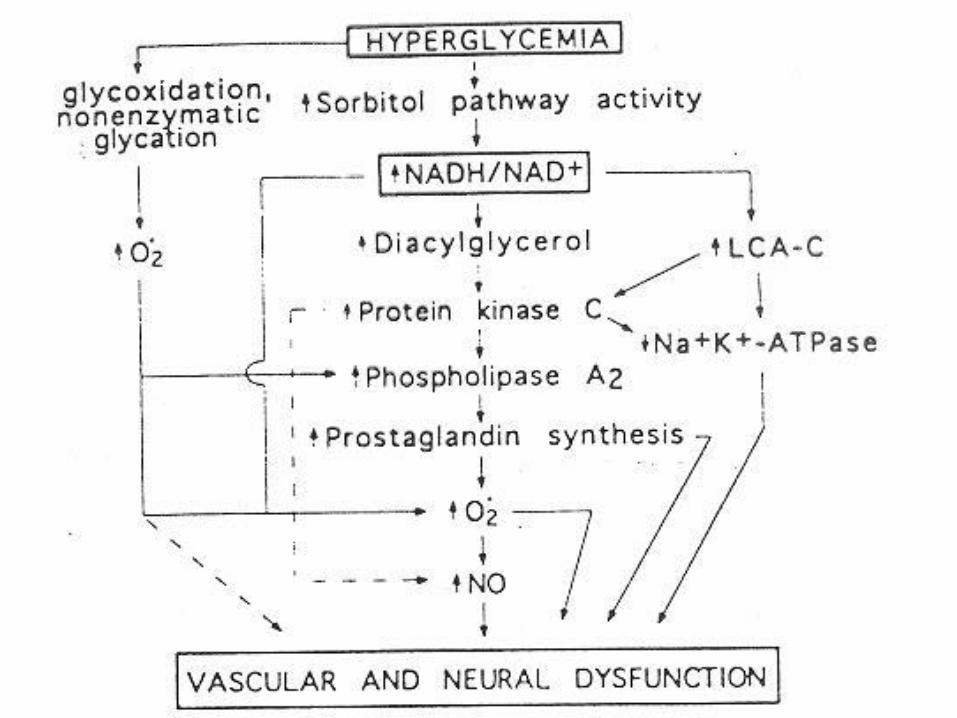
Possible mechanisms involved in development of DN
- blood supply to nerves is decreased because of microvascular damage
(vasa nervorum may be damaged)
- energy source for normal rest membrane potential maintain is
insufficient
- increased accumulation of sorbitol and fructose, decreased
concentration of myoinositol
- non-enzymatic glycation of proteins

Main functions of vascular endotelium
• regulates vascular tone and permeability
• regulates the balance between coagulation and fibrinolysis
• regulation of subendothelial matrix composition
• influences extravasation of leucocytes
• influences the proliferation of vascular smooth muscleand renal mesangial cells
To curry out these functions, the endothelium produces components of extracellular matrix and variety of regulatory mediators
2. Diabetic micro- and macroangiopathies
A) Microvascular disease - specific lesion of DM that affect capillaries
and arterioles of the retina, renal glomeruli, peripheral nerves, muscles
and skin
Characteristic lesion :
- thickening of the capillary basement membrane
- increased accumulation of glycoprotein in wall of small
arteries and capillaries
a)Retinopathy - it is the result of retinal ischemia caused by
microangiopathy
Pathomechanisms involved in retinopathy occurence:
- increased retinal capillary permeability, vein dilation
- microaneurism formation and hemorrhages
- narrowing of small arteries lumen
- neovascularisation and fibrous tissue formation within
the retina
- retinal scars formation blindness
