acute bacterial prostatitis -it is inflam. refluxed from bladder or ascend from urethra...
TRANSCRIPT

ACUTE BACTERIAL PROSTATITIS
• -it is inflam. Refluxed from bladder or ascend from urethra
• -PRESENTATION :fever,constit. Symp.,urolog. Symp.,PR avoided,catheter avoided.
• -Dx :GUE,micrscopic exam. & culture of prostatic expressate,E.coli is common.,U/S,TRU/S.
• Rx :empiric therapy against G-ve bacteria• indication of hospitalisation:• 1-sepsis• 2-immunecompromised• 3-acute retention• 4-significant medical comorbidities

CHRONIC BACTERIAL PROSTATITIS
• -INSIDOUS ONSET• -CAUSED BY PERSISTENCE OF PATHOGEN IN PROSTATIC
FLUID DESPITE OF ANTIBIOTIC.• -PRESENTATION:asymp.,dysuria,frequency,low
backpain,urgency,nocturia.,PR (normal,tendered,firm,stone)
• Ix :GUE,4 CUP TESTS,TRU/S• -Rx : antibiotic for 3-4 m.• alpha-blockers(reduce recurrence rate)• cure is difficult• suppressive therapy(not responding)• TUR-P(refractory condition)

GRANULOMATOUS PROSTATITIS
• bacterial,viral,fungal,BCG,systemic• -eisinophilic or non eiosinophilic• -fever,chills,obst/irrit. Symp.• -GUE,PR(hard),prostatic biopsy• -Rx : antibiotic • steroid• temperory emptying• TUR-P(if not responding)

PROSTATIC ABSCESS
• -inadequate Rx of acute prostatitis• -DM,pt. on dialysis,immuncompromised
undergoing cath. • -simillar to acute bact. Prostatitis• -PR(tendered ,swollen prostate)• -TRU/S &pelvic CT• -Rx :transrectal drainage under TRU/S or CT wth antib.
• if fail TUR drainage done

EPIDIDYMITIS
-caused by ascending infection from LUT.-in males <35 yr caused by STD.-in children & old age caused by uropathogens.

PRESENTATION
• -scrotal pain radiating to groin &flank.
• -scrotal swelling due to infl. Or hydrocele.
• -symp. Of ureth.,cystitis,prostatitis.• -O/E tendered red scrotal swelling.

epididymitis

investigations
• GUE : WBCS.• Urethral discharge C/S.• Doppler U/S &isotope scan.• U/S :epididymal enlargement
&hydrocele.• Radiological evaluation in children.
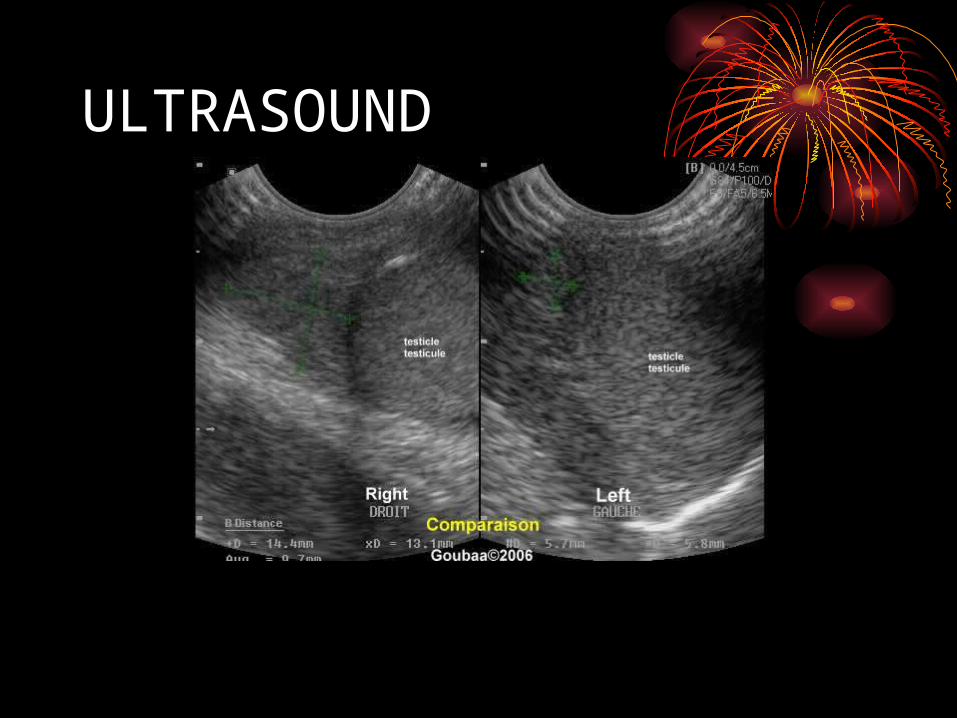
ULTRASOUND

DOPPLER U/S

Doppler u/s of torsed lt. testicle

TREATMENT
• -ORAL ANTIBIOTIC.• -SCROTAL ELEVATION, bed
rest,&use of NSAID.• -admission & IV drugs used.• -in STD treat partner.• -in chronic pain do
epididymectomy.

URETHRITIS
•-NGU Rx by erythromycin or doxycyclin with follow up of pt. for 7 days.
• -treatment of persistent or recurrent urethritis is by metronidazole & erythromycin to act against both T.vaginalis &genital mycoplasma.

UTI IN PREGNANCY• -anatomical changes :enlarged
uterus specially in 2nd &3rd trimesters.
• -physiological changes :increase GFR &increase progesteron.
• -30% of pt. with BU develop PN.• -INCIDENCE OF PN IN PREGNANT IS
1-4%.
UTI IN PREGNANCY
• -PN if untreated lead to prematurity &perinatal death.
• -evaluation at 1st &16th wk visit.• -asympt. BU :URINE CULTURE
>100.000cfu/cc.• -symp. BU :>1000cfu/cc• -drugs used in pregnancy.
UTI IN CHILDREN• -in 1st yr boys >girls affected.• -presentation :infant non specific.more
localisation in older children.• -diagnosis :urine C/S ,GUE,blood
tests(ESR,C-reactive prot.• -classification ;1st infection & recurrent
infection.• - recurrent infection :unresolved
BU ,b.persistence or reinfection.

UTI IN CHILDREN
• -E.coli is the most causative agent.• -host factors• -child is at greater risk of renal scarring
by UTI.• -incomplete immune & neurologic
system.• -delayed Dx due to non specific
presentation.

UTI IN CHILDREN
• -renal scarrings may lead to HT & even ESRD.• -TREATMENT :not severely ill child treated
orally.• Severly ill pt. treated by hospitalisation ,IV
drugs.• -prophylactic antibiotics &radiological
assessment is needed to prevent renal scarring.