xiv curso de puesta al día en tratamiento … · guías de manejo periquirúrgico de los fármacos...
TRANSCRIPT

XIV Curso de puesta al día en tratamiento antitrombótico
SETH Castelldefels, 10 – 11 marzo 2016
Controversias en terapia puente
José Ramón González Porras
Unidad de Trombosis-Hemostasia Servicio de Hematología
Hospital Universitario de Salamanca-IBSAL-USAL

Guías de manejo periquirúrgico de los fármacos antitrombóticos
• Manejo periquirúrgico de los antiagregantes plaquetarios (AAP)
– Información limitada (estudios observacionales y recomendaciones de expertos)
– Las diferentes situaciones durante la actividad quirurgica inducen a la variabilidad de la atención.
• Guías de práctica clínica disponibles
Darvish-Kazem S. CHEST 2013:144:1848-56

Manuscrito en elaboración
Evaluación de la adherencia a las guías de manejo periquirúrgico de los AAP y sus consecuencias clínicas
Comisión de Trombosis del Hospital Universitario de Salamanca
• Consenso multidisciplinar del manejo periquirúrgico de AAP en cirugía no cardiaca electiva
• Basado en la evidencia científica disponible
• Evaluación de resultados
• Adherencia terapéutica en AAP en el año 2011: 42.1% (n=109)
• Adherencia terapéutica en AAP en el año 2014: 52.4% (n=97)
• Comparativa con AVK
• Adherencia terapéutica en AVK en el año 2014: 74% (n = 207)
• Adherencia terapéutica en AAP en el año 2014: 52.4% (n=97)
• El incumplimiento terapéutico en AAP se relacionó con
• Mayor tasa de complicaciones hemorrágicas, OR 2.49 IC 95% (1.08-5.73)
• Mayor tasa de complicaciones trombóticas, OR 2.88 IC95% (0.98-8.52)
p < 0.05
p < 0.05

Caso no. 1 • Varón de 68 años con SFA hace 4 meses por NSTEMI • Ahora requiere cirugía de parótida (adenocarcinoma) • En tratamiento con AAS (100 mg/día) + CLOPIDOGREL (75 mg/día) • Otros factores de riesgo cardiovascular
• CABG hace 8 años • HTA • DM tipo2
PREGUNTA
1. Stop AAS y CLOPIDOGREL 5 días pre-op y comenzar ambos 1-2 días post-op
2. Stop AAS y CLOPIDOGREL 5 días pre-op y administrar terapia puente con HBPM o HNF
3. Continuar con AAS pre-/post-op y stop CLOPIDOGREL 5 días pre-op
4. Continuar AAS + CLOPIDOGREL pre-/post-op
5. Stop AAS y CLOPIDOGREL 5 días pre-op y administrar inhibidores GP IIa/IIIb

• ¿Cuándo se consideraría seguro realizar una cirugía no cardiaca electiva tras la implantación de stent coronario? ¿Y tras un ictus? • ¿Qué antiagregantes deben suspenderse o mantenerse durante un procedimiento invasivo? .
• ¿En qué situaciones es necesaria una terapia puente con anticoagulantes o antiagregantes en pacientes antiagregados programados para procedimientos invasivos? .
Preguntas de “Controversias en terapia puente”

• ¿Cuándo se consideraría seguro realizar una cirugía no cardiaca electiva tras la implantación de stent coronario? ¿Y tras un ictus? • ¿Qué antiagregantes deben suspenderse o mantenerse durante un procedimiento invasivo? .
• ¿En qué situaciones es necesaria una terapia puente con anticoagulantes o antiagregantes en pacientes antiagregados programados para procedimientos invasivos? .
Preguntas de “Controversias en terapia puente”

Caso no. 2 • Varón de 60 años con stent metálico en circunfleja por AI • Gran hernia inguinal • ¿Cuándo la cirugía de la hernia inguinal podría realizarse de manera “segura”?
RESPUESTA
1. 1 semana
2. 2 semanas
3. 6 semanas
Caso no. 2 • Varón de 60 años con stent metálico en circunfleja por AI • Gran hernia inguinal • ¿Cuándo la cirugía de la hernia inguinal podría realizarse de manera “segura”?
RESPUESTA
1. 1 semana
2. 2 semanas
3. 6 semanas
Khayr T. Cardiovas Revasc Med 2011;12: 99–104.
Contemporary approaches to perioperative management of coronary stents and to preoperative coronary revascularization: a survey of 374 interventional cardiologists • 98% C option

Coronary stent and surgery
1.- Moschovitis A. EuroIntervention. 2010;6:-189-94. 2.- Savonitto S. J Thromb Haemost. 2011;9:2133-42. 3.- Rossini R. Am J Cardiol. 2011;107:186-94. 4.- WijnsW. Eur Heart J. 2010;31:2501–55
• Every year more than one million PCI are performed in the USA and Europe1,2
• In more than 85% of cases a coronary stent is implanted3,
and pro- longed antiplatelet therapy is mandatory after stent implantation4
Dual antiplatelet therapy (DAT) for minimal 14 days after angioplasty
DAT for minimal 30 days for BMS
DAT for minimal 180 days for new-generation DES
DAT for minimal 360 days for myocardial revascularization for high-risk ACS
• The most common causes of discontinuation are surgery and bleeding events3
4-8% of patients undergo surgery within the first year after corronary stent
23% within five years

Predictors of coronary stent thrombosis
Nijmegen N, et al. J Am Coll Cardiol. 2009;53:-1399-409.

Tokushige A. Circ Cardiovasc Interv 2012; 5: 237-46
Bleeding within 30 days after surgical procedures, according to status of perioperative antiplatelet therapy

When Should Elective Noncardiac Surgery Be
Done in Patients With a Coronary Stent? Review
of Clinical Practice Guidelines
Darvish-Kazem S. Chest. 2013; 144: 1848-56
Type of stent Delaying time after stent implantation Guidelines
BMS At least 3 months 1
At least 6 weeks 4
At least 4 weeks 5
At least 2 weeks 1
DES At least 12 months 9
At least 6 months 2

Incidence and Outcome of Surgical Procedures
After BMS and DES Implantation
1.- Tokushige A. Circ Cardiovasc Interv 2012;5:237-46
• CREDO-Kyoto registry1 on 1878 patients undergoing noncardiac surgery < 2 y. after stent Overall MACE rate of 3.2% Similar rates between BMS (3.5%) and DES (2.9%).
• Ontario registry2 on 2725 patients undergoing surgery within 2 years of stent placement
2.- Wijeysundera DN. Circulation. 2012;126:1635-62

Hawn MT. JAMA. 2013;310:1462-72
Risk of MACEs Following Noncardiac Surgery in
Patients With Coronary Stents
Study Design
• A national, retrospective cohort study of 41.989 operations occurring in the 24 months after a
coronary stent implantation between 2000 and 2010.
Primary efficacy endpoint
• A composite 30-day MACE rate of all-cause mortality, myocardial infarction, and cardiac
revascularization.
Results
• 1980 MACE (4.7%; 95% CI, 4.5%-4.9%).
• Time between stent and surgery was associated with MACE
11.6%: <6 weeks
6.4%, 6 weeks to <6 months
4.2%, 6-12 months
3.5%, >12-24 months
p < 0.001

Hawn MT. JAMA. 2013;310:1462-72
Adjusted risk Odds Ratio of perioperative
MACE
Best-Fit Model of perioperative Major Adverse Cardiac Event
Partial Effects Analysis
OR (95% CI) P Value X2 - df Rank
Nonelective inpatient 4.77 (4.07-5.59) <.001 388.9 1
Myocardial infarction in past 6 mo 2.63 (2.32-2.98) <.001 230.0 2
Revised cardiac index ≥ 3 2.13 (1.85-2.44) <.001 119.6 3
Operation type
Digestive
Respiratory
2.30 (1.82-2.90)
2.80 (2.18-3.59)
<.001 86.1 4
Time between stent and surgery, wk <.001 45.0 5
Congestive heart failure in past 6 mo 1.45 (1.23-1.72) <.001 17.7 6
PCI in past 2 y ≥ 2 1.25 (0.95-1.65) <.001 13.8 7
Age at surgery ≥ 60y 1.20 (1.00-1.02) <.001 7.0 8
Stent type 0.91 (0.83-1.01) .08 2.1 12

Hawn MT. JAMA. 2013;310:1462-72
Adjusted risk Odds Ratio of MACE by stent type
2014 ACC/AHA Perioperative Guidelines
• Class I
• Elective noncardiac surgery should be delayed
• 14 D after balloon angioplasty
• 30 D after BMS implantation
• 365 D after DES implantation
• Class IIb
• Elective noncardiac surgery after DES implantation may be
considered after 180 D if risk of further delay > risk of stent
thrombosis
Fleisher LA. J AM Coll Cardiol. 2014;64:e77-137

Time Elapsed After Ischemic Stroke and Risk of
Adverse Cardiovascular Events and Mortality
Following Elective Noncardiac Surgery
• Danish nationwide cohort study (2005-2011)
• Including all patients undergoing elective noncardiac surgeries (n=481 183 surgeries).
• Prior stroke in 7137 patients
• Compared with patients with prior stroke, ORs for MACE were 4.03 (95% CI, 3.55-4.57)
Jørgensen MA. JAMA. 2014;312:269-277

Time Elapsed After Ischemic Stroke and Risk of
Adverse Cardiovascular Events and Mortality
Following Elective Noncardiac Surgery
Jørgensen MA. JAMA. 2014;312:269-277

•Conclusiones: ¿Cuándo se consideraría seguro realizar una
cirugía no cardiaca electiva tras la implantación de stent coronario? ¿Y tras un ictus?
• Idealmente 1 mes tras BMS (preferiblemente 3 meses)
• Idealmente 6 meses tras DES (preferiblemente 1 año)
• 9 meses tras ictus se considera “seguro” para la realización de
una cirugía no cardiaca electiva

• ¿Cuándo se consideraría seguro realizar una cirugía no cardiaca electiva tras la implantación de stent coronario? ¿Y tras un ictus? • ¿Qué antiagregantes deben suspenderse o mantenerse durante un procedimiento invasivo? .
• ¿En qué situaciones es necesaria una terapia puente con anticoagulantes o antiagregantes en pacientes antiagregados programados para procedimientos invasivos? .
Preguntas de “Controversias en terapia puente”

Caso no. 3 • Varón de 55 años con SFA en descendente anterior por AI • 13 meses después se descubre AAA de 7 cm •¿Qué opción recomendaría por ser la de menor riesgo “periquirúrgico”
RESPUESTA
1. Stop CLOPIDOGREL y AAS
2. Stop CLOPIDOGREL y mantener AAS
3. Continuar con CLOPIDOGREL y AAS

Caso no. 3 • Varón de 55 años con SFA en descendente anterior por AI • 13 meses después se descubre AAA de 7 cm •¿Qué opción recomendaría por ser la de menor riesgo periquirúrgico”
RESPUESTA
1. Stop CLOPIDOGREL y AAS
2. Stop CLOPIDOGREL y mantener AAS
3. Continuar con CLOPIDOGREL y AAS
A survey of 374 interventional cardiologists A) 11% B) 48% c) 41%
Khayr T. Cardiovas Revasc Med 2011;12: 99–104.

Caso no. 4 • Varón de 50 años con SFA en descendente anterior por STEMI • Rx tórax muestra una masa pulmonar lóbulo superior izquierdo • Sospechoso de malignidad requiere biopsia • Neumología y Radiología rechazan hacerlo con clopidogrel • ¿Qué opción recomendaría?
RESPUESTA
1. STOP AAS y CLOPIDOGREL durante 5 días
2. Continuar AAS, stop CLOPIDOGREL y administrar TIROFIBÁN
3. Continuar AAS y CLOPIDOGREL y encontrar un médico que le haga la biopsia

Caso no. 4 • Varón de 50 años con SFA en descendente anterior por STEMI • Rx tórax muestra una masa pulmonar lóbulo superior izquierdo • Sospechoso de malignidad requiere biopsia • Neumología y Radiología rechazan hacerlo con clopidogrel • ¿Qué opción recomendaría”
RESPUESTA
1. STOP AAS y CLOPIDOGREL durante 5 días
2. Continuar AAS, stop CLOPIDOGREL y administrar TIROFIBÁN
3. Continuar AAS y CLOPIDOGREL y encontrar un médico que le haga la biopsia
Survey of 374 interventional cardiologists A) 1% B) 50% c) 49%
Khayr T. Cardiovas Revasc Med 2011;12: 99–104.

Bleedign Risk of continuing aspirin on
non-cardiac surgery
• Large meta-analysis, including 41 studies in 49.590 patients
• To compare pre-precedural withdrawals vs bleeding risk of aspirin
• Results
Risk of bleeding complications with aspirin therapy was increased
by 50%
Aspirin did not lead to greater severity complications
Burger W. Int Med 2005;257:399-414

Risk of continuing aspirin on non-cardiac surgery
1.- Mantz J. Br J of Anaest 2011;107: 899–910. 2.- Oscarsson A. Br J of Anaest 2010;104:305–12.
• Two randomised controlled trials assessing a primary outcome of
bleeding and thrombotic risk of continuing aspirin
The first: no difference between aspirin or placebo had a composite
outcome of major thrombotic and bleeding events within 30 days of surgery1.
Another RCT found a significant reduction in major cardiovascular events on
aspirin (1.2% vs 9.0%, p = 0.02), but was underpowered to detect any
differences in bleeding rates

Devereaux PJ. N Engl J Med 2014;370:1494-503
Aspirin in Patients Undergoing
Noncardiac Surgery: POISE-2 trial
• Aspirin did not have a protective effect for MACE or death in patients either continuing aspirin or starting aspirin during the perioperative period
• To evaluate the effects of aspirin versus placebo in patients undergoing noncardiac surgery

Devereaux PJ. N Engl J Med 2014;370:1494-503
Aspirin in Patients Undergoing
Noncardiac Surgery: POISE-2 trial
• Aspirin use was associated with an increased risk of major bleeding
Safety outcomes Aspirin
(N=4998)
Placebo
(N=5012)
Hazard Ratio
(95% CI)
P-Value
Life-threatening bleeding 87 (1.7) 73 (1.5) 1.19 (0.88-1.63) 0.26
Major bleeding 230 (4.6) 188 (3.8) 1.23 (1.01-1.49) 0.04
Clinically important hypotension 2143 (42.9) 2096 (41.8) 1.03 (0.97-1.09) 0.37
Stroke 16 (0.3) 19 (0.4) 0.84 (0.43-1.64) 0.62
Congestive heart failure 44 (0.9) 38 (0.8) 1.16 (0.75-1.79) 0.50
Infection 488 (9.8) 495 (9.9) 0.99 (0.87-1.12) 0.86
Sepsis 243 (4.9) 258 (5.2) 0.94 (0.79-1.13) 0.52

Devereaux PJ. N Engl J Med 2014;370:1494-503
Aspirin in Patients Undergoing
Noncardiac Surgery: POISE-2 trial
LIMITATIONS
• Patients within 6 weeks of placement of a BMS or within 1 year of placement of a
DES were excluded from the trial
• The number of stented patients outside these time intervals was too small
• Only 23% of the study population had known prior CAD
• The population excluded patients undergoing carotid endarterectomy surgery
Continuation may still be reasonable in patients with high-risk CAD or
cerebrovascular disease, where the risks of potential increased
cardiovascular events outweigh the risks of increased bleeding.

Risk of continuing clopidogrel on
non-cardiac surgery
• There is very little information on the bleeding risk for clopidogrel
monotherapy in general surgery.
• Although this appears to be higher than for aspirin1-3, some expert
groups suggest continuing the agent in a similar manner to aspirin4.
• The bleeding risk on dual antiplatelet treatment is increased2-3 and
although neuraxial anaesthesia can be performed in patients on aspirin,
it is contra-indicated in patients on clopidogrel, prasugrel and ticagrelor5.
1.- Yusuf S. New Engl J Med. 2001;345: 494–502. 2.- Sørensen R. Lancet. 2009;374: 1967–74. 3.- Ernst A. Chest. 2006;129: 734–7. 4.- Korte W. Thromb Haemost. 2011;105:743–9. 5.- Makris M. Anaesthesia. 2013;68:966–72.

Rossini R. Thromb Haemost. 2015;113:272-82
Patients with perioperative discontinuation of
antiplatelet therapy experienced a significantly
higher incidence of MACE
Antiplatelet discontinuation
No antiplatelet discontinuation
• Multicentre, retrospective, observational study conducted in patients with coronary stent(s) undergoing cardiac or non-cardiac surgery (n = 666)

Rossini R. Thromb Haemost. 2015;113:272-82
Patients with perioperative discontinuation of
antiplatelet therapy experienced a significantly
higher incidence of MACE
In conclusion, antiplatelet discontinuation increases the 30-day risk MACE,
in patients with coronary stent undergoing non-cardiac surgery, while
not offering significant protection from BARC ≥ 2 bleeding

Which Antiplatelet Agents Should Be Stopped or
Continued Around the Time of Surgery?
Darvish-Kazem S. Chest 2013; 144: 1848-56
Recommendation Situation Guidelines
Continuing ASA Non cardiac surgery 11
Discontinuing both ASA
and clopidogrel
High bleeding risk (spinal, intracranial,
extraocular, urologic or major reconstructive
procedures)
1
Discontinuing clopidogrel High bleeding risk (spinal, intracranial,
extraocular, urologic or major reconstructive
procedures)
1
Changing clopi to ASA Increased bleeding risk 8

Aspirin in the recent perioperative period
guidelines: 2014 ACC/AHA and 2014 ESC/ESA
• 2014 ACC/AHA: In patients undergoing nonemergency/nonurgent
noncardiac surgery who have not had previous coronary stenting, it may be
reasonable to continue aspirin when the risk of potential increased cardiac
events outweighs the risk of increased bleeding (IIb)
• 2014 ESC/ESA: the use of low-dose aspirin in patients undergoing non-
cardiac surgery should be based on an individual decision which depends on the
perioperative bleeding risk, weighed against the risk of thrombotic
complications.

Dual anti-platelet therapy in the recent
perioperative period guidelines: 2014 ACC/AHA
and 2014 ESC/ESA
• 2014 ACC/AHA:
• In patients who have received coronary stents and must undergo surgical
procedures that mandate the discontinuation of P2Y12 inhibitor, it is
recommended that aspirin be continued if possible and the P2Y12 platelet
receptor-inhibitor be started as soon as possible after surgery (Ic)
• 2014 ESC/ESA:
• In patients treated with P2Y12 inhibitors, who need to undergo surgery,
postponing surgery for at least 5 days after cessation of ticagrelor and
clopidogrel—and for 7 days in the case of prasugrel—if clinically feasible,
should be considered unless the patient is at high risk of an ischaemic event.

Sierra P. Rev Esp Anestesiol Reanim 2011;158:243-50
Estratificación del riesgo hemorrágico /
trombótico

Sierra P. Rev Esp Anestesiol Reanim 2011; 158: 243-50
Guías SEDAR 2011

Protocol for preoperative antiplatelet therapy with DES
Vetter TR. BMC Anesthes. 2014;14:73

Thrombotic risk
Low risk Intermediate risk High risk
ASA: continue
P2Y12r inhib:
Discontinuate 5 days before*
Elective surgery: postpone
ASA: continuate
P2Y12r inhib: continuate
Elective surgery: postpone
ASA: continuate
P2Y12r inhib: continuate
ASA: continue
P2Y12r inhib:
Discontinuate 5 days before*
Elective surgery: postpone
ASA: continuate
P2Y12 r inhib:
Discontinuate 5 days before*
Elective surgery: postpone
ASA: continuate
P2Y12r inhib:
Discontinuate 5 days before*
Bridge therapy with GPIIb/IIIa inhib**
ASA: discontinue
P2Y12r inhib:
Discontinuate 5 days before*
Elective surgery: postpone
ASA: continuate
P2Y12r inhib:
Discontinuate 5 days before*
Elective surgery: postpone
ASA: continuate
P2Y12r inhib:
Discontinuate 5 days before*
Bridge therapy with GPIIb/IIIa inhib**
He
mo
rrag
he
ris
k
Low
In
term
ed
iate
H
igh
Development of the thrombotic versus
bleeding risk algorithm
* Prasugrel 7 days
** Consensual decision
Rossini R. Eurointerventions 2014; 10: 38-49

•Conclusiones: ¿Qué antiagregantes deben suspenderse o
mantenerse durante un procedimiento invasivo? .
• Debe valorarse de manera cautelosa y consensuada el balance entre el riesgo trombótico
implícito a la suspensión del fármaco y el riesgo hemorrágico inherente a su acción terapéutica
• En general, el AAS debería mantenerse para la mayoría de los procedimientos invasivos excepto
en pacientes con bajo riesgo trombótico pero sometidos a un procedimiento invasivo de alto-
moderado riesgo hemorrágico.
• Mantener clopidogrel en pacientes de alto riesgo trombótico sometidos a procedimientos
invasivos de no alto riesgo hemorrágico puede ser una opción prudente para reducir el riesgo de
complicaciones cardiovasculares.
• Si retiramos el clopidogrel debería mantenerse el AAS
• En pacientes con BMS o DES que requieran cirugía en los primeras 4-6 semanas tras la
implantacion del stent, debería mantenerse la doble terapia antitrombótica a menos que el
riesgo hemorrágico del procedimiento supere al beneficio en la prevención de la trombosis del
stent.

• ¿Cuándo se consideraría seguro realizar una cirugía no cardiaca electiva tras la implantación de stent coronario? ¿Y tras un ictus? • ¿Qué antiagregantes deben suspenderse o mantenerse durante un procedimiento invasivo? .
• ¿En qué situaciones es necesaria una terapia puente con anticoagulantes o antiagregantes en pacientes antiagregados programados para procedimientos invasivos? .
Preguntas de “Controversias en terapia puente”
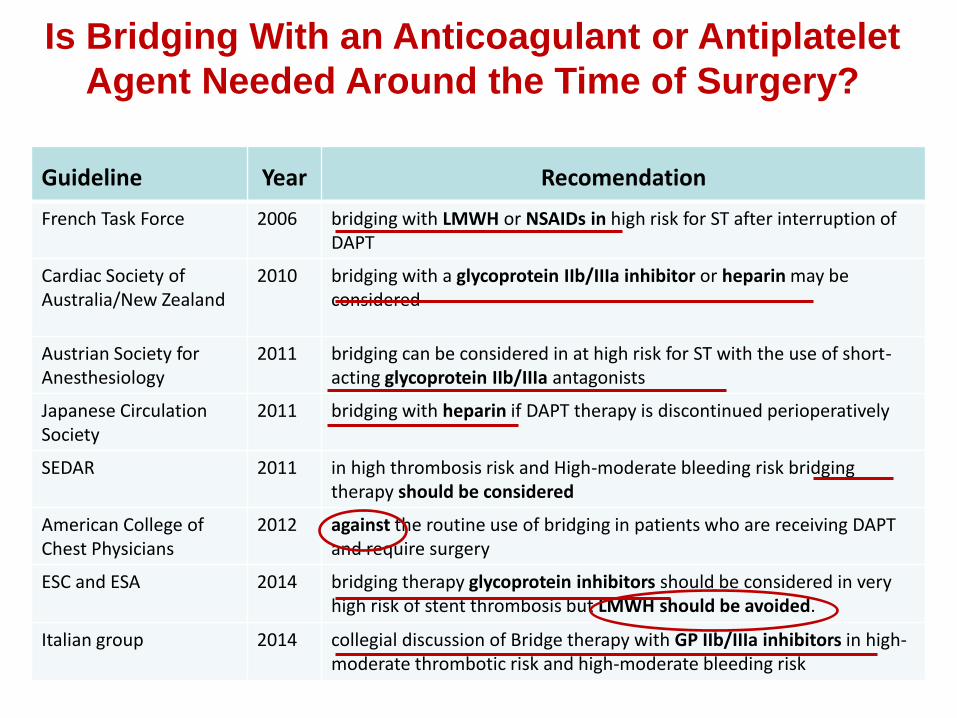
Is Bridging With an Anticoagulant or Antiplatelet
Agent Needed Around the Time of Surgery?
Guideline Year Recomendation
French Task Force 2006 bridging with LMWH or NSAIDs in high risk for ST after interruption of DAPT
Cardiac Society of Australia/New Zealand
2010 bridging with a glycoprotein IIb/IIIa inhibitor or heparin may be considered
Austrian Society for Anesthesiology
2011 bridging can be considered in at high risk for ST with the use of short-acting glycoprotein IIb/IIIa antagonists
Japanese Circulation Society
2011 bridging with heparin if DAPT therapy is discontinued perioperatively
SEDAR 2011 in high thrombosis risk and High-moderate bleeding risk bridging therapy should be considered
American College of Chest Physicians
2012 against the routine use of bridging in patients who are receiving DAPT and require surgery
ESC and ESA 2014 bridging therapy glycoprotein inhibitors should be considered in very high risk of stent thrombosis but LMWH should be avoided.
Italian group 2014 collegial discussion of Bridge therapy with GP IIb/IIIa inhibitors in high-moderate thrombotic risk and high-moderate bleeding risk

Parenteral inhibitors of GP IIb-IIIa and cangrelor
Abciximab
(ReoPro)
eptifibatide
(INTEGRILIN®)
tirofiban HCI
(Aggrastat)
Cangrelor
(Kengreal)
Pharma Fab portion of chimeric monoclonal antibody
Synthetic non-peptide
Cyclic heptapeptide
ATP analogue
Half-life 30 minutes 1.8 hours 2.5 hours 3 – 6 minutes
Renal Adj
No Yes Yes No
Dosage 0.25 mg/kg bolus followed by 0.125 mg/kg/min drip (max 10 mg/min) for 12-24 hours
0.4 mg/kg/min for 30 minutes followed by 0.1 mg/kg/min drip for 48-96 hours
180 mg/kg bolus (x2) followed by 2.0 mg/kg/min drip for 18-24 hours
infusion 0.75 μg/kg/min

I IIa IIb III
• GP IIb/IIIa Inhibitor in addition to ASA and
Heparin for patients in whom PCI is planned
• Eptifibatide or Tirofiban for high risk* patients
if medically managed
* High-risk: Age >75; prolonged, ongoing CP; hemodynamic instability
(CHF, new MR, ↓BP, ↑HR); rest CP w/ST ∆; VT; positive cardiac markers
Anti-Thrombotic Therapy: Platelet GP
IIb/IIIa Inhibitors

Bridge with intravenous antiplatelet therapy during temporary withdrawal of
oral agents for surgical procedures: a systematic review
• N = 420 with high-risk characteristics for stent thrombosis
• Eight case series and one randomised controlled trial
• Bridge therapy with anti-GP IIb/IIIa
DAT
Surgery
Clopidogrel Stop (- 5 d)
Anti-IIb/IIIa Start (- 4 d)
Anti-IIb/IIIa stop 4 h before
Anti-IIb/IIIa resume 2 h after
Resume oral administration Stop anti-IIb/IIIa
Resume Clopidogrel
Treat per Standard of Care
(CABG
rule-in) 0
100
200
300
400
-1 0 1 2 3 4 5-7
Elapsed Days
PR
U
CABG
Thru Hospital Discharge
Demonstrate that cangrelor infusion of maintains PRU< 240
Cangrelor/Placebo Infusion Dose Determined in Stage I :
0.75 µg/kg/min
Clopidogrel
or prasugrel
• Bridge therapy with cangrelor
Morici N. Intern Emerg Med 2014;9:225–35

• The technique was effective 96.2 % of the times
freedom from cardiac ischaemic adverse events
• The technique was safety 72.6% of the times
freedom from bleeding/transfusion events
was higher with cangrelor (88.7 %) than with other drugs
Efficacy and safety of Bridge with intravenous antiplatelet
therapy during temporary withdrawal of oral agents for
surgical procedures
Morici N. Intern Emerg Med 2014;9:225–35

Impact of bridging with perioperative LMWH
on cardiac and bleeding outcomes of stented
patients undergoing non-cardiac surgery
• Retrospective analysis
• Among 515 patients with coronary stent(s) on any antiplatelet therapy underwent
non-cardiac surgery, LMWH bridging was used in 251 (49 %).
• At 30 days, MACCE occurred:
LMWH group = 7.2 % vs non-LMWH = 1.1 % (p=0.001),
• At 30 days, BARC bleedings 2 occured:
LMWH group = 21.9 % vs non-LMWH = 11.7 % (p=0.002)
Capodanno D. Thromb Haemost. 2015;114:23–431

•Conclusiones: ¿En qué situaciones es necesaria una terapia
puente con anticoagulantes o antiagregantes en pacientes antiagregados programados para procedimientos invasivos?.
• La terapia puente en pacientes antiagregados programados para
procedimientos invasivos debe constituir una situación excepcional y siempre
consensuada (equipo multidisciplinar)
• Debe evitarse el uso de heparinas
• Los inhibidores del receptor de la GP IIb/IIIa pueden valorarse en pacientes
de muy alto riesgo trombótico en los que la doble terapia AAP debe
suspenderse por alto-moderado riesgo hemorrágico
• La mayor evidencia del uso de la terapia puente con AAP es con cangrelor en
pacientes con doble antiagregación en espera de cirugía cardiaca

Caso no. 1 • Varón de 68 años con SFA hace 4 meses por NSTEMI • Ahora requiere cirugía de parótida (adenocarcinoma) • En tratamiento con AAS (100 mg/día) + CLOPIDOGREL (75 mg/día) • Otros factores de riesgo cardiovascular
• CABG hace 8 años • HTA • DM tipo2
PREGUNTA
1. Stop AAS y CLOPIDOGREL 5 dias pre-op y comenzar ambos 1-2 días post-op
2. Stop AAS y CLOPIDOGREL 5 días pre-op y administrar terapia puente con HBPM o HNF
3. Continuar con AAS pre-/post-op y stop CLOPIDOGREL 5 días pre-op
4. Continuar AAS + CLOPIDOGREL pre-/post-op
5. Stop AAS y CLOPIDOGREL 5 días pre-op y administrar inhibidores GP IIa/IIIb

XIV Curso de puesta al día en tratamiento antitrombótico
SETH Castelldefels, 10 – 11 marzo 2016
Controversias en terapia puente
José Ramón González Porras
Unidad de Trombosis-Hemostasia Servicio de Hematología
Hospital Universitario de Salamanca-IBSAL-USAL