workshop i hdt mi ih emodynamic monitoring - rcpt.org lecture... · workshop i hdt mi ih emodynamic...
TRANSCRIPT
WorkshopWorkshopH d i M it i H d i M it i Hemodynamic Monitoring Hemodynamic Monitoring
พพ ออ นพนพ นครินทร ศันสนยทธนครินทร ศันสนยทธพพ..ออ. . นพนพ. . นครนทร ศนสนยุทธนครนทร ศนสนยุทธแผนกโรคหัวใจและหลอดเลือดแผนกโรคหัวใจและหลอดเลือด
โรงพยาบาลพระมงกฎเกลาโรงพยาบาลพระมงกฎเกลาโรงพยาบาลพระมงกุฎเกลาโรงพยาบาลพระมงกุฎเกลา๒๙ ๒๙ กรกฎาคม กรกฎาคม ๒๕๕๒๒๕๕๒
OutlineOutlineOutlineOutline
Central venous pressureCentral venous pressure : Internal Jugular: Internal JugularCentral venous pressureCentral venous pressure : Internal Jugular, : Internal Jugular, Subclavian, cutSubclavian, cut--downdownSwan Ganz or PA catheterSwan Ganz or PA catheter : RV PA and: RV PA andSwan Ganz or PA catheter Swan Ganz or PA catheter : RV, PA and : RV, PA and PCW pressure PCW pressure AA lili A t i l bl dA t i l bl dAA--line : line : Arterial blood pressureArterial blood pressure
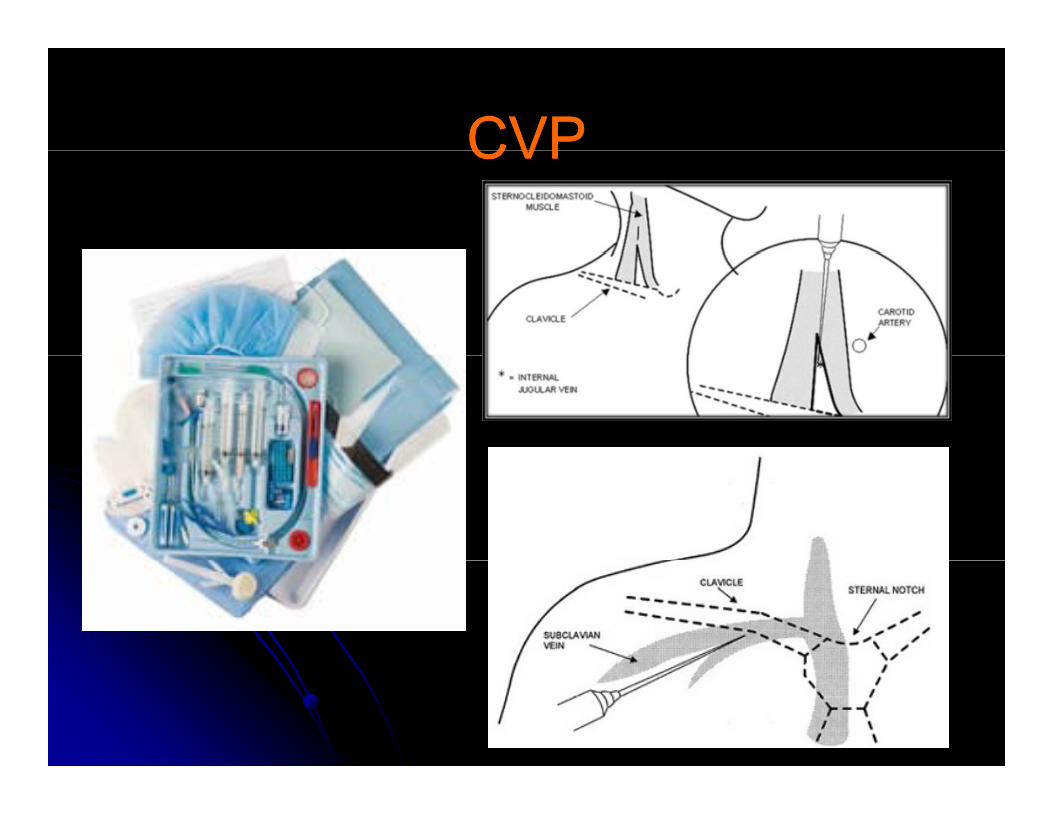
CVPCVPCVPCVP
Q:Q: CVP monitoringCVP monitoring มปีระโยชนในการมีประโยชนในการQ:Q: CVP monitoringCVP monitoring มประโยชนในการมประโยชนในการ..........
1)1) Assess volume statusAssess volume status1)1) Assess volume statusAssess volume status2)2) Diagnosis of cardiac arrhythmiaDiagnosis of cardiac arrhythmia
Di i f di b litDi i f di b lit3)3) Diagnosis of cardiac abnormalityDiagnosis of cardiac abnormality4)4) Number Number 1 1 and and 3 3 are correctare correct5)5) All All 11,,2 2 and and 3 3 are correctare correct
CVPCVPCVPCVP
Use of Central lineUse of Central lineUse of Central lineUse of Central lineAssess intravascular volume statusAssess intravascular volume statusDiagnosis of cardiac abnormalitiesDiagnosis of cardiac abnormalitiesDiagnosis of cardiac abnormalitiesDiagnosis of cardiac abnormalitiesDiagnosis of arrhythmiaDiagnosis of arrhythmia
Others: other catheters, frequent blood Others: other catheters, frequent blood sampling drug or IV administrationsampling drug or IV administrationsampling, drug or IV administrationsampling, drug or IV administration
CVPCVPCVPCVP
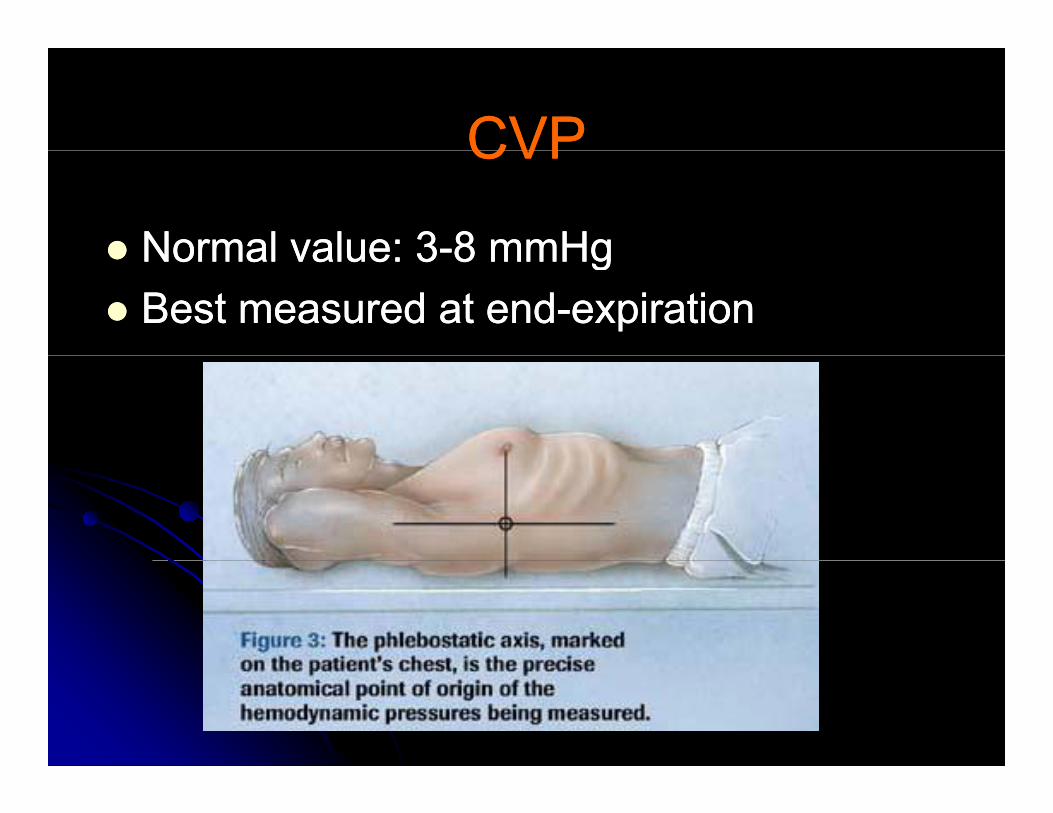
Normal value:Normal value: 33--88 mmHgmmHgNormal value: Normal value: 33 8 8 mmHgmmHgBest measured at endBest measured at end--expirationexpiration
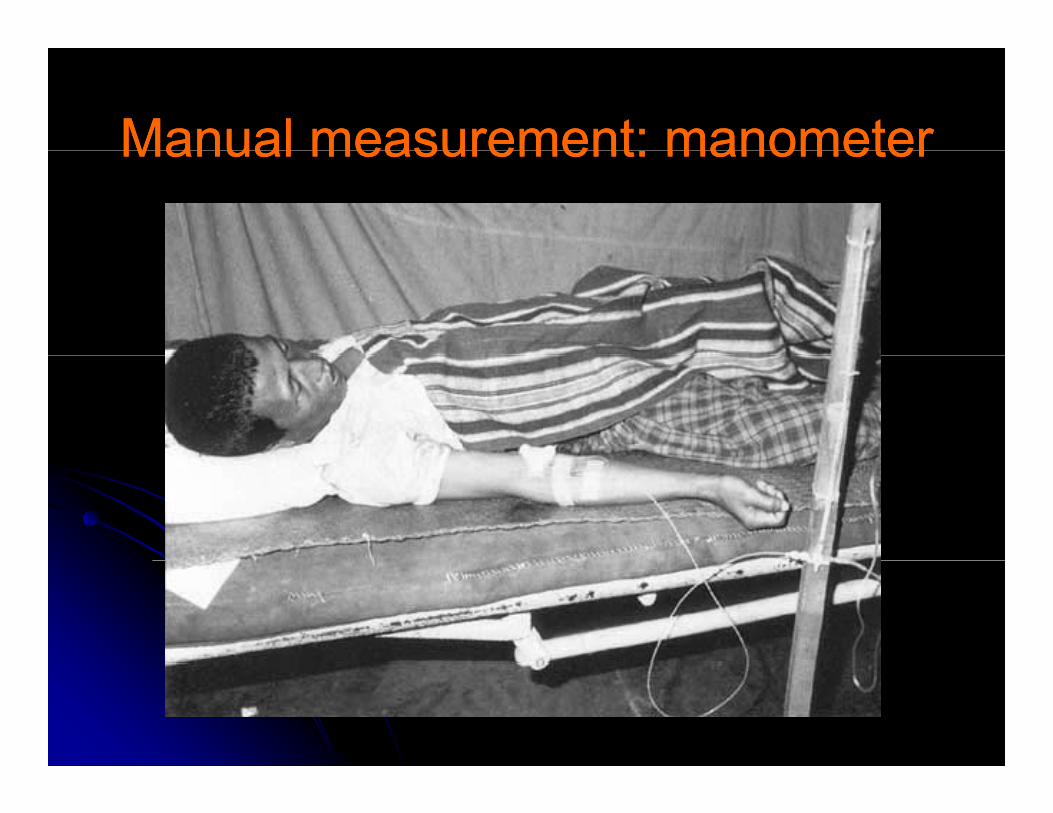
Manual measurement: manometerManual measurement: manometerManual measurement: manometerManual measurement: manometer
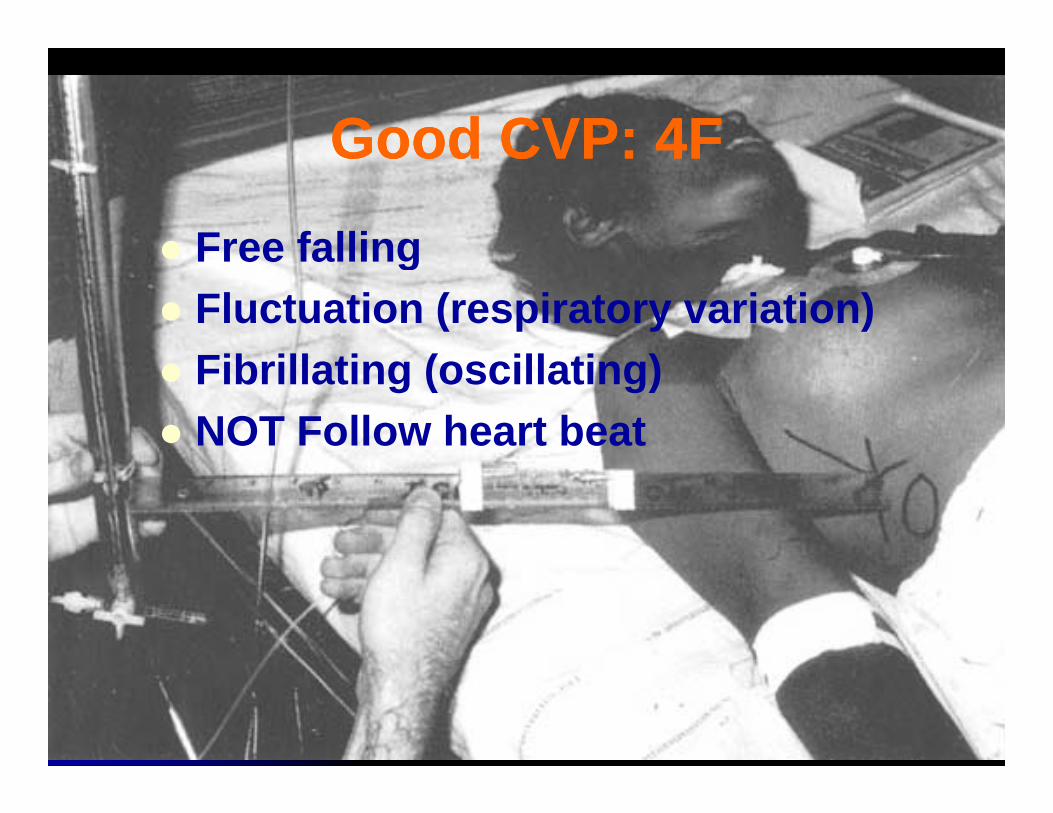
Good CVP:Good CVP: 44FFGood CVP: Good CVP: 44FF
Free fallingFree fallingFluctuation (respiratory variation)Fib ill ti ( ill ti )Fibrillating (oscillating)NOT Follow heart beat
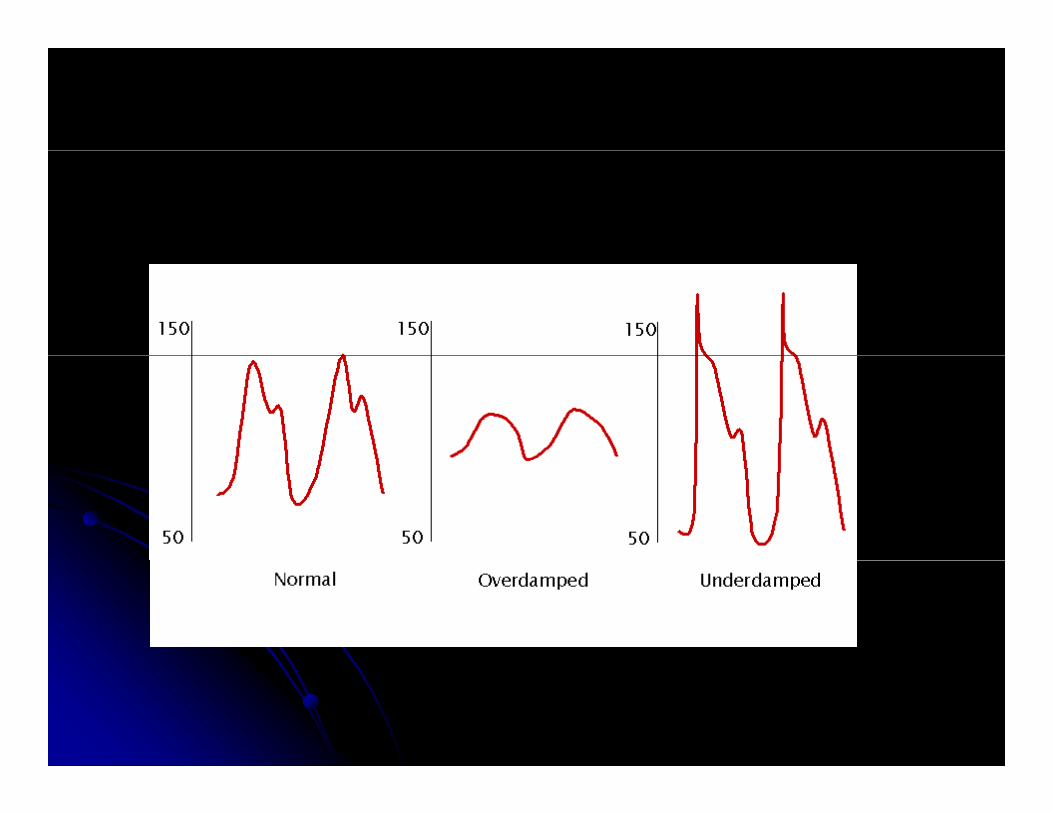
Transducer systemTransducer systemTransducer systemTransducer system
Hemodynamic interpretationHemodynamic interpretationHemodynamic interpretationHemodynamic interpretation
LevelLevelLevelLevel
WaveformWaveformWaveformWaveform
EKGEKG
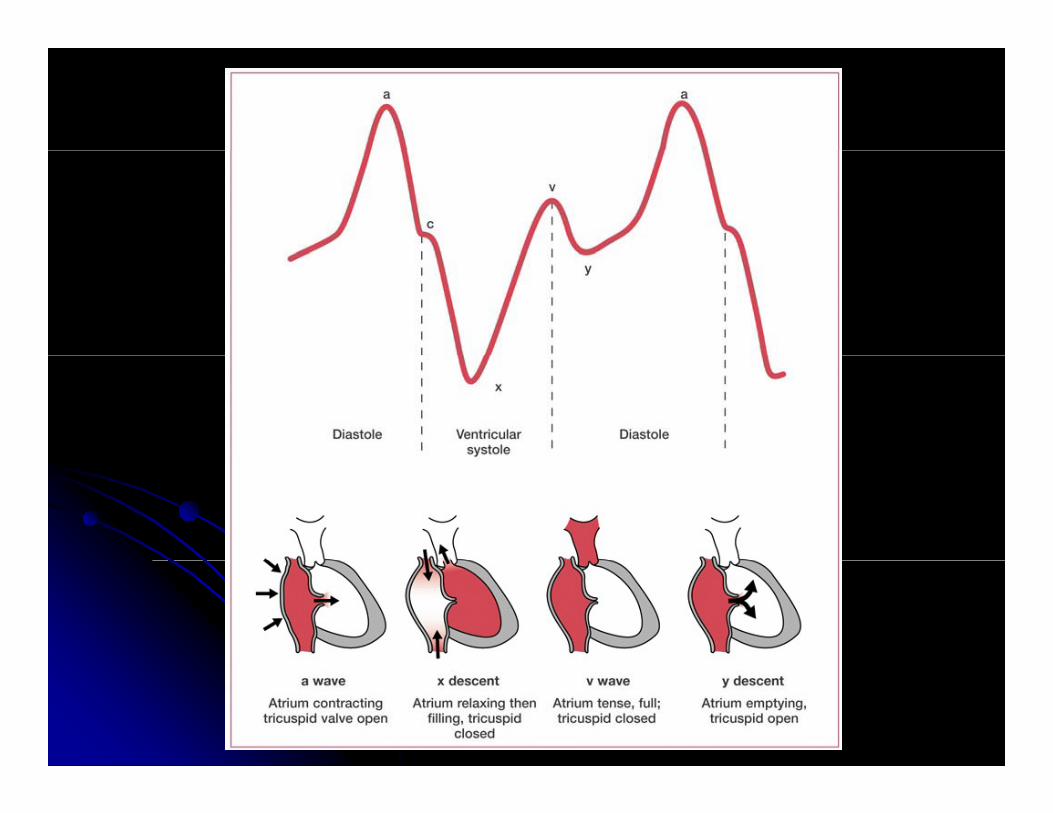
The a wave:The a wave: RightRight aatrial contrtrial contraactionctionThe a wave: The a wave: Right Right aatrial contrtrial contraactionctionThe c wave: The c wave: TriTriccuspid valve uspid valve cclosurelosure
tid ltid lccarotid pulsearotid pulseThe x descent:The x descent: Right atrial relaRight atrial relaxxationationThe v wave:The v wave: Right atrial fillingRight atrial filling
RightRight vventricular contractentricular contractnnRight Right vventricular contractentricular contractThe y descent:The y descent: Right atrial emptRight atrial emptyyinging
Use EKG to identify waveformUse EKG to identify waveformUse EKG to identify waveformUse EKG to identify waveform8080--100100msec for EKG and waveform delaymsec for EKG and waveform delay
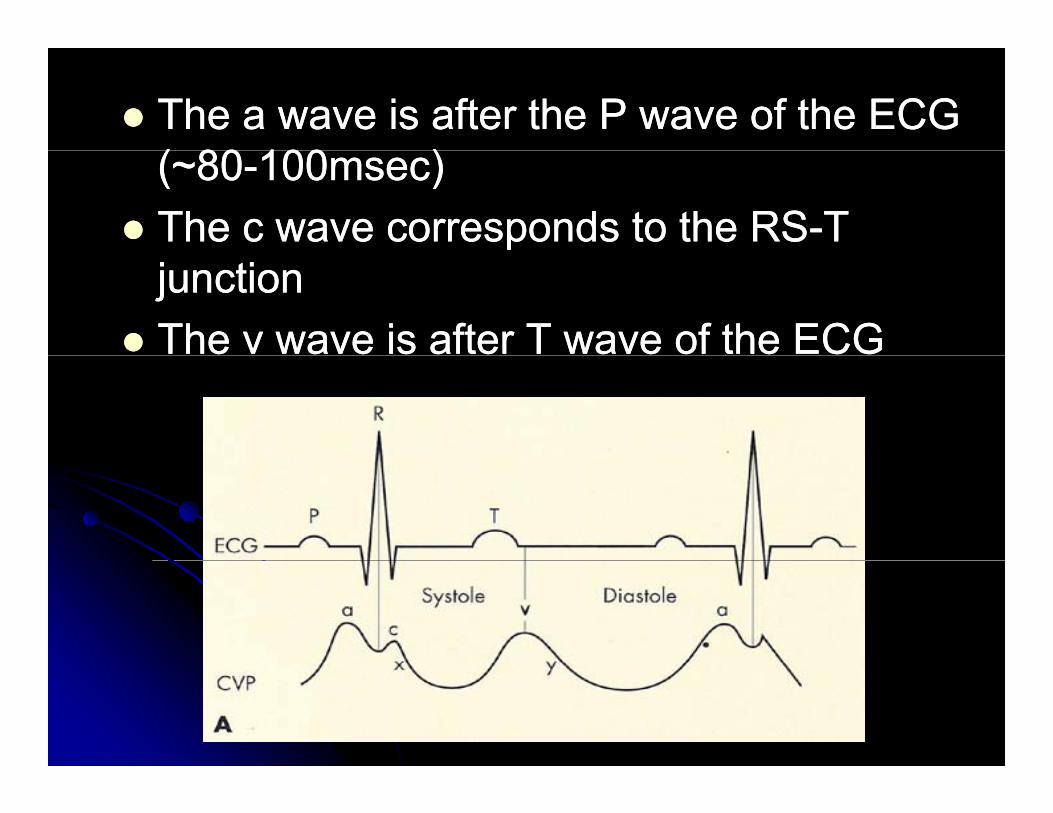
The a wave is after the P wave of the ECG The a wave is after the P wave of the ECG (( 8080 100100 ))(~(~8080--100100msec)msec)The c wave corresponds to the RSThe c wave corresponds to the RS--T T junctionjunctionThe v wave is after T wave of the ECGThe v wave is after T wave of the ECG
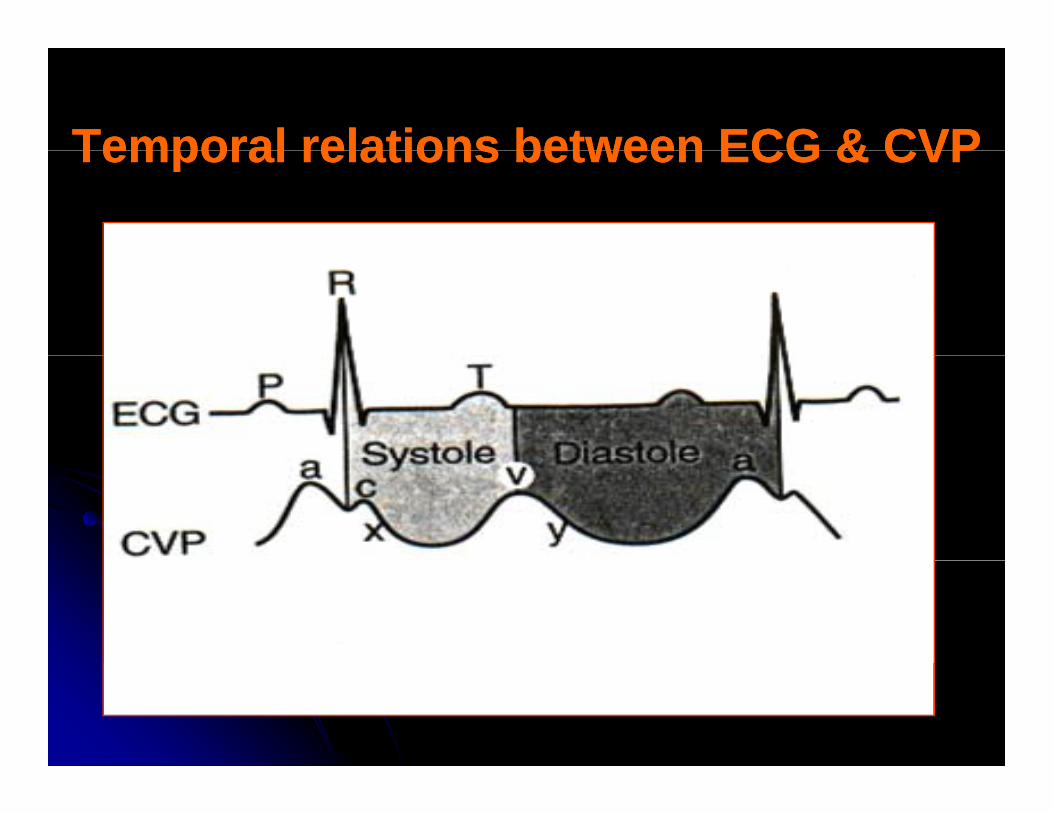
Temporal relations between ECG & CVPTemporal relations between ECG & CVPTemporal relations between ECG & CVPTemporal relations between ECG & CVP
Relative ContraindicationsRelative ContraindicationsRelative Contraindications Relative Contraindications
Bleeding disordersBleeding disordersBleeding disordersBleeding disordersAnticoagulation or thrombolytic therapyAnticoagulation or thrombolytic therapyDi t t d l l tDi t t d l l tDistorted local anatomyDistorted local anatomyCellulitisCellulitis, burns, severe dermatitis at site, burns, severe dermatitis at siteVasculitisVasculitis
PostPost--Catheter PlacementCatheter PlacementPostPost Catheter PlacementCatheter Placement
Aspirate blood from each portAspirate blood from each portAspirate blood from each portAspirate blood from each portFlush with saline or sterile waterFlush with saline or sterile waterS th t ith tS th t ith tSecure catheter with suturesSecure catheter with suturesCover with sterile dressing (tegaCover with sterile dressing (tega--derm)derm)Obtain chest xObtain chest x--ray for IJ and SC linesray for IJ and SC linesWrite a procedure noteWrite a procedure noteWrite a procedure noteWrite a procedure note
ComplicationsComplicationsComplications Complications VascularVascular
Ai b lAi b lAir embolusAir embolusArterial punctureArterial punctureArteriovenous fistulaArteriovenous fistulaHematomaHematomaBlood clotBlood clot
InfectiousInfectiousSepsis, cellulitis, osteomyelitis, septic arthritisSepsis, cellulitis, osteomyelitis, septic arthritis
Miscellaneous Miscellaneous DysrhythmiasDysrhythmiasDysrhythmiasDysrhythmiasCatheter knotting or malpositionCatheter knotting or malpositionNerve injuryNerve injuryPneumothorax hemothorax hydrothorax hemomediastinumPneumothorax hemothorax hydrothorax hemomediastinumPneumothorax, hemothorax, hydrothorax, hemomediastinumPneumothorax, hemothorax, hydrothorax, hemomediastinumBowel or bladder perforationBowel or bladder perforation
Abnormal CVP findingsAbnormal CVP findingsAbnormal CVP findingsAbnormal CVP findings
Elevated CVPElevated CVPElevated CVPElevated CVPRV failureRV failureTS TR PSTS TR PSTS, TR, PSTS, TR, PSCardiac Cardiac tamponadetamponadeConstrictiveConstrictive pericarditispericarditisConstrictive Constrictive pericarditispericarditisPulmonary hypertensionPulmonary hypertensionLV f ilLV f ilLV failureLV failureVolume overloadVolume overload
Abnormal CVP findingsAbnormal CVP findingsAbnormal CVP findingsAbnormal CVP findingsGiant a wave: Giant a wave:
TSTSCanon a wave:Canon a wave:
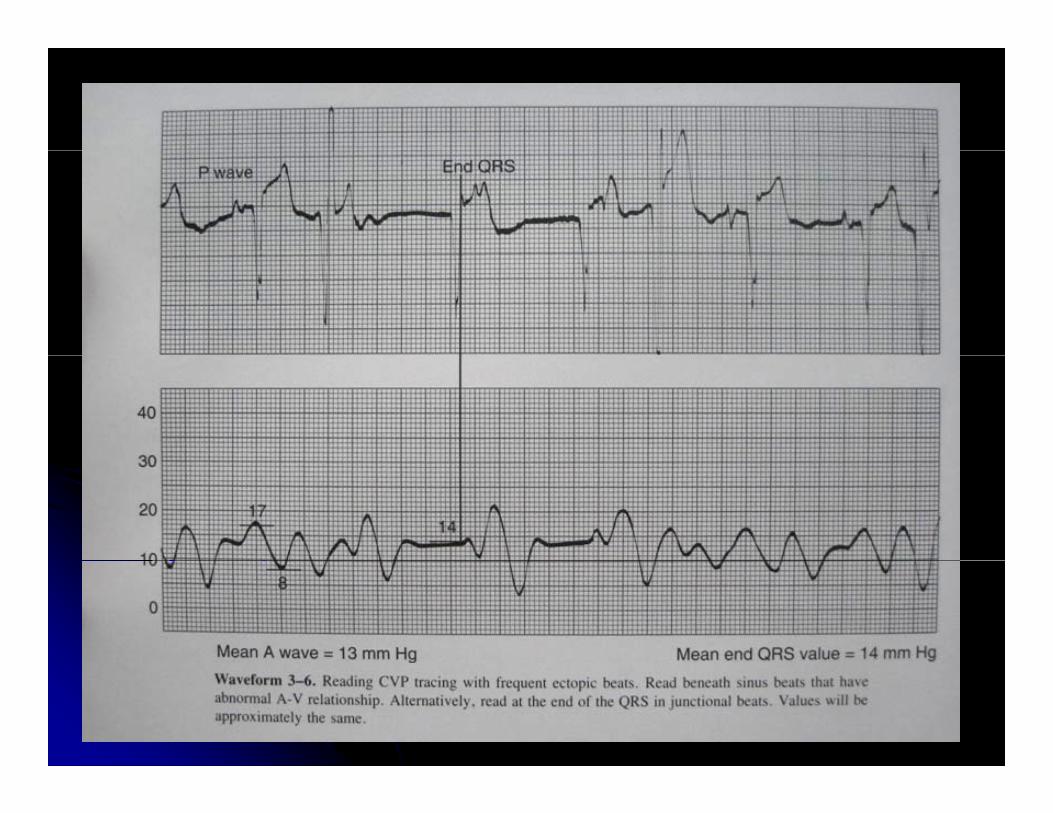
AV di i i (AV di i i (33 dd AVB VT PVCAVB VT PVCAV dissociation (AV dissociation (33rdrd AVB, VT, PVC, AVB, VT, PVC, Junctional rhythm)Junctional rhythm)
Giant v wave:Giant v wave:Giant v wave:Giant v wave:TRTR
Dominant x descent with a very short or absent y Dominant x descent with a very short or absent y dddescent:descent:
TamponadeTamponadePredominant y descent:Predominant y descent:Predominant y descent:Predominant y descent:
Constrictive pericarditisConstrictive pericarditis
RA waveform & arrhythmiaRA waveform & arrhythmiaRA waveform & arrhythmiaRA waveform & arrhythmia
Ab tAb t AFAFAbsent a waves: Absent a waves: AFAF
Sawtooth f waves:Sawtooth f waves: Atrial flutterAtrial flutterSawtooth f waves:Sawtooth f waves: Atrial flutterAtrial flutter
Cannon a waves:Cannon a waves: AV dissociationAV dissociation
SVTSVT
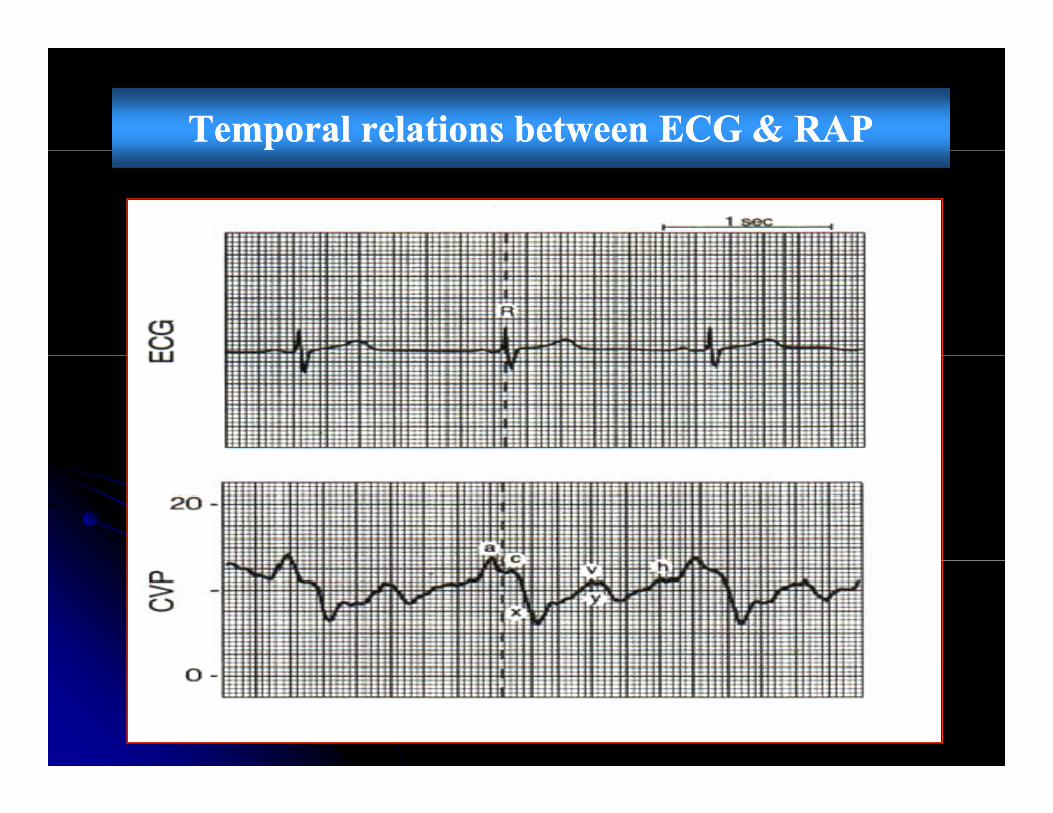
Temporal relations between ECG & RAPTemporal relations between ECG & RAP
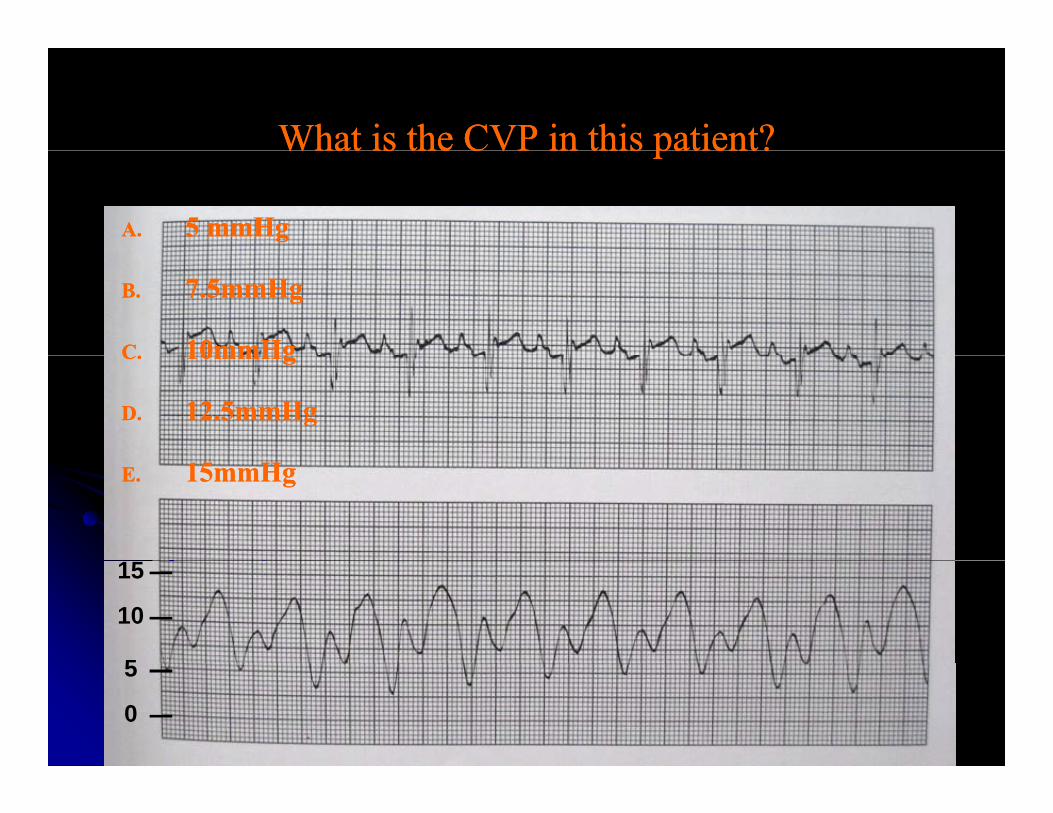
What is the CVP in this patient?What is the CVP in this patient?What is the CVP in this patient?What is the CVP in this patient?
A.A. 5 5 mmHgmmHg
B.B. 77..55mmHgmmHg
CC 1010mmHgmmHgC.C. 1010mmHgmmHg
D.D. 1212..55mmHgmmHg
E.E. 1515mmHgmmHg
15
10
5
0
5
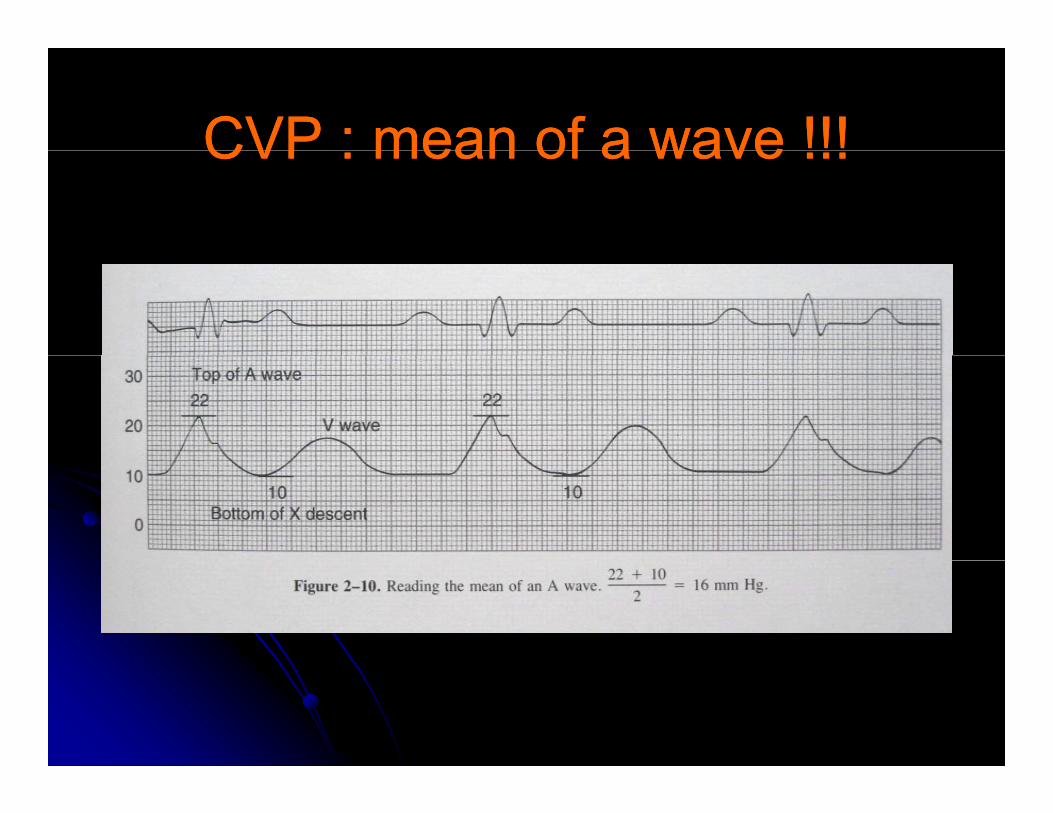
CVP : mean of a wave !!!CVP : mean of a wave !!!CVP : mean of a wave !!!CVP : mean of a wave !!!
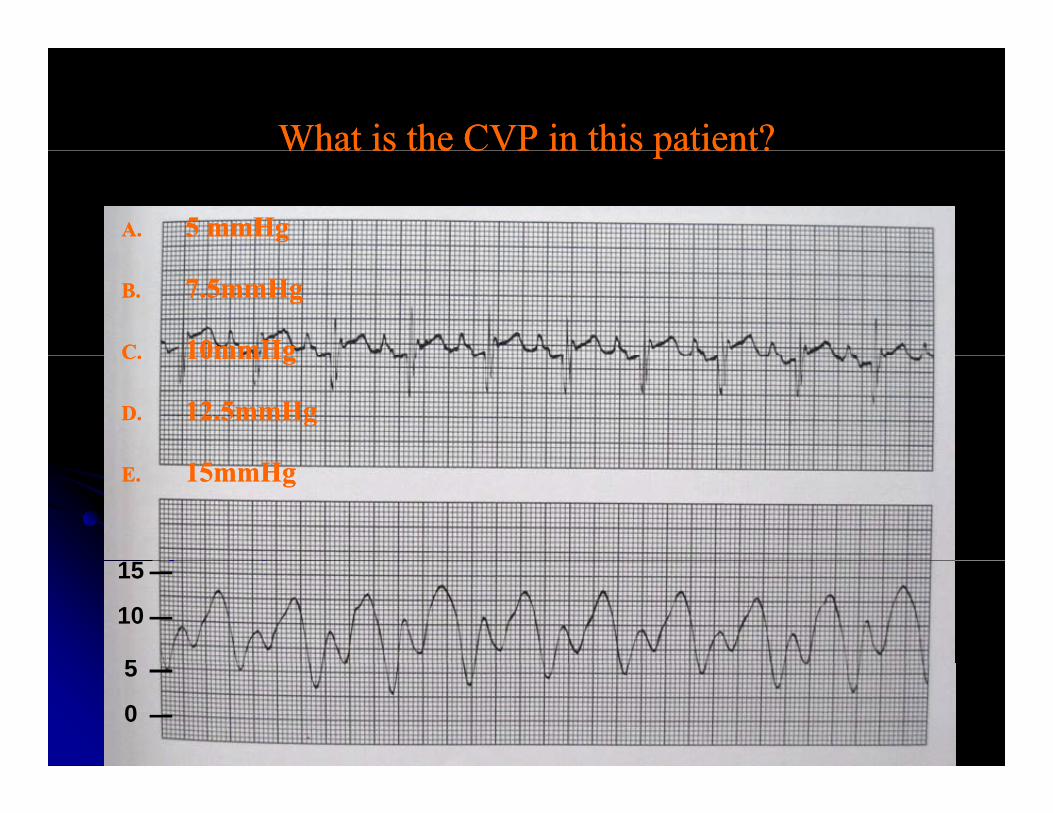
What is the CVP in this patient?What is the CVP in this patient?What is the CVP in this patient?What is the CVP in this patient?
A.A. 5 5 mmHgmmHg
B.B. 77..55mmHgmmHg
CC 1010mmHgmmHgC.C. 1010mmHgmmHg
D.D. 1212..55mmHgmmHg
E.E. 1515mmHgmmHg
15
10
5
0
5
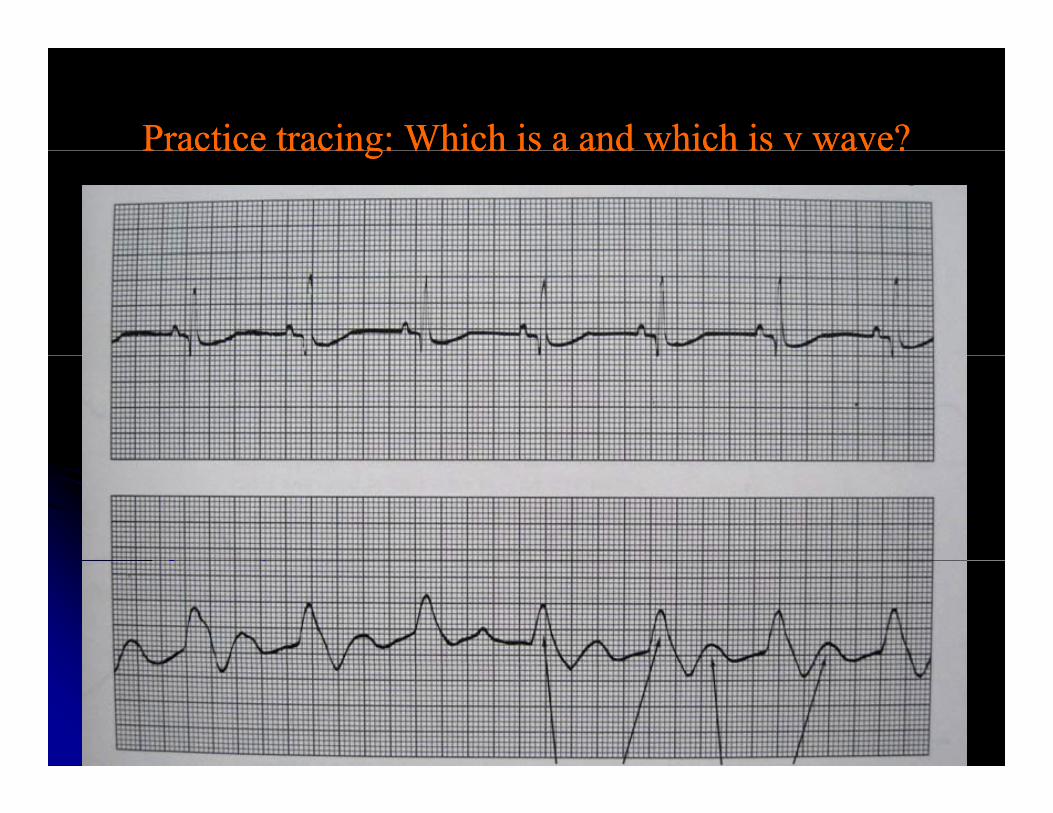
Practice tracing: Which is a and which is v wave?Practice tracing: Which is a and which is v wave?Practice tracing: Which is a and which is v wave?Practice tracing: Which is a and which is v wave?
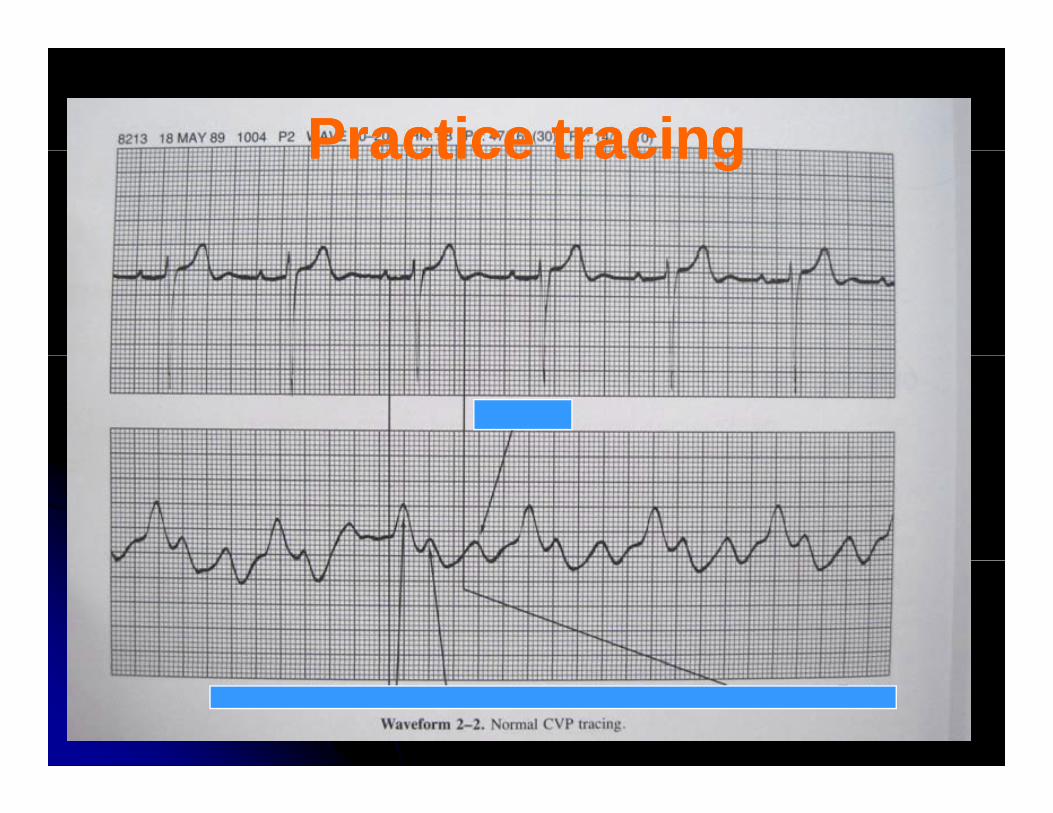
Practice tracingPractice tracingPractice tracingPractice tracing
How to measure CVP How to measure CVP if th i if th i NONO “ ” “ ” if there is if there is NONO “a” wave“a” wave
Junctional rhythmJunctional rhythmAFAFVTVT
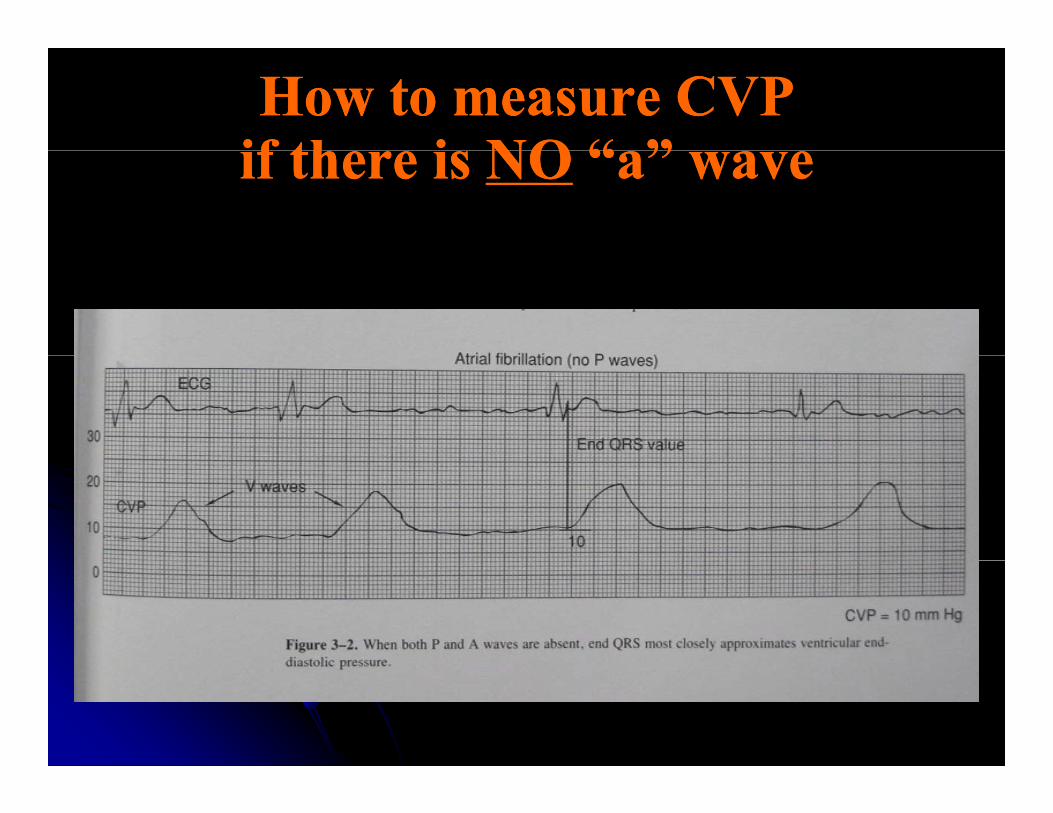
How to measure CVP How to measure CVP if th i if th i NONO “ ” “ ” if there is if there is NONO “a” wave“a” wave
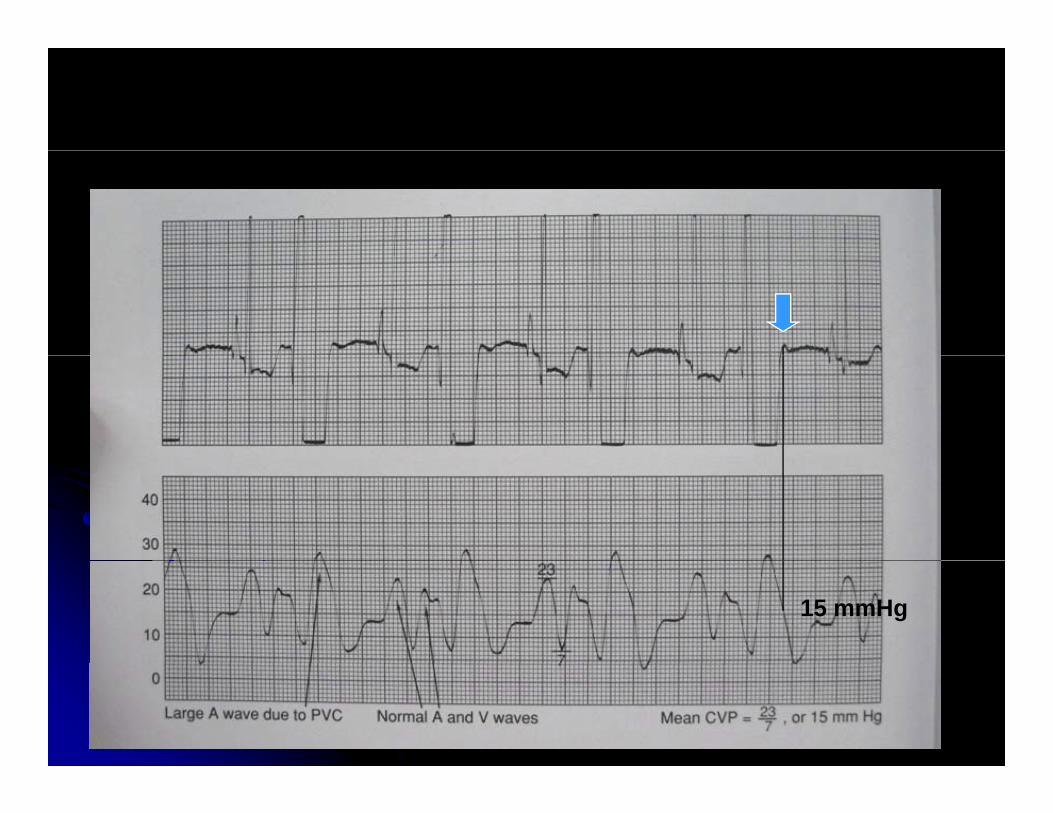
15 mmHg
CVP monitoringCVP monitoringCVP monitoringCVP monitoring
In shock keep CVPIn shock keep CVP 88--1212 mmHgmmHgIn shock keep CVP In shock keep CVP 88 12 12 mmHgmmHg
Fl id h ll t t (Fl id h ll t t (22//55 l )l )Fluid challenge test (Fluid challenge test (22//5 5 rule)rule)
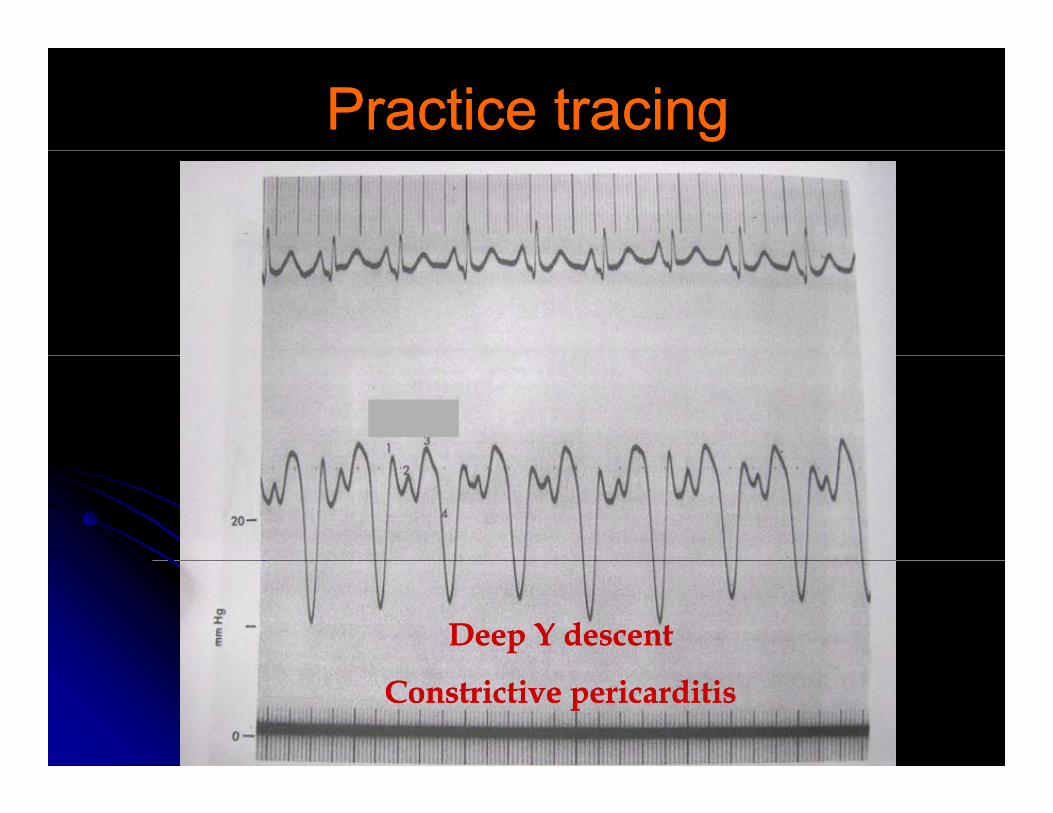
Practice tracingPractice tracing
Deep Y descent Deep Y descent
Constrictive pericarditisConstrictive pericarditis
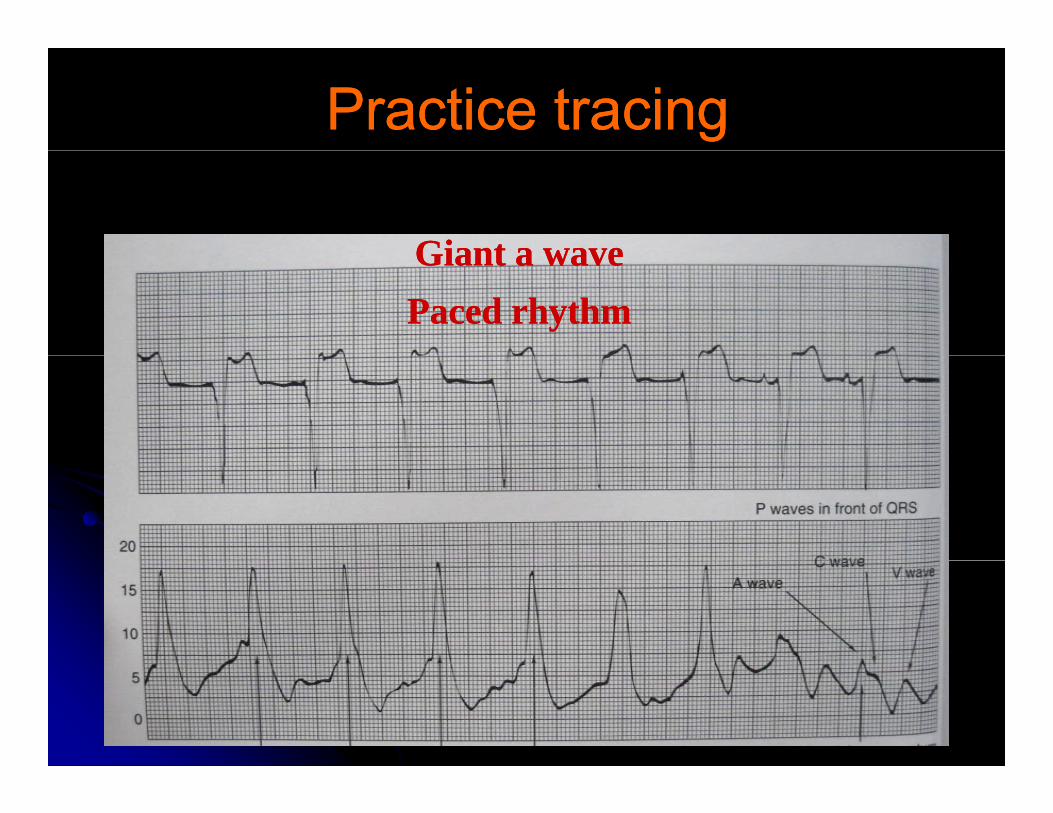
Practice tracingPractice tracing
Giant a waveGiant a waveGiant a wave Giant a wave Paced rhythmPaced rhythm
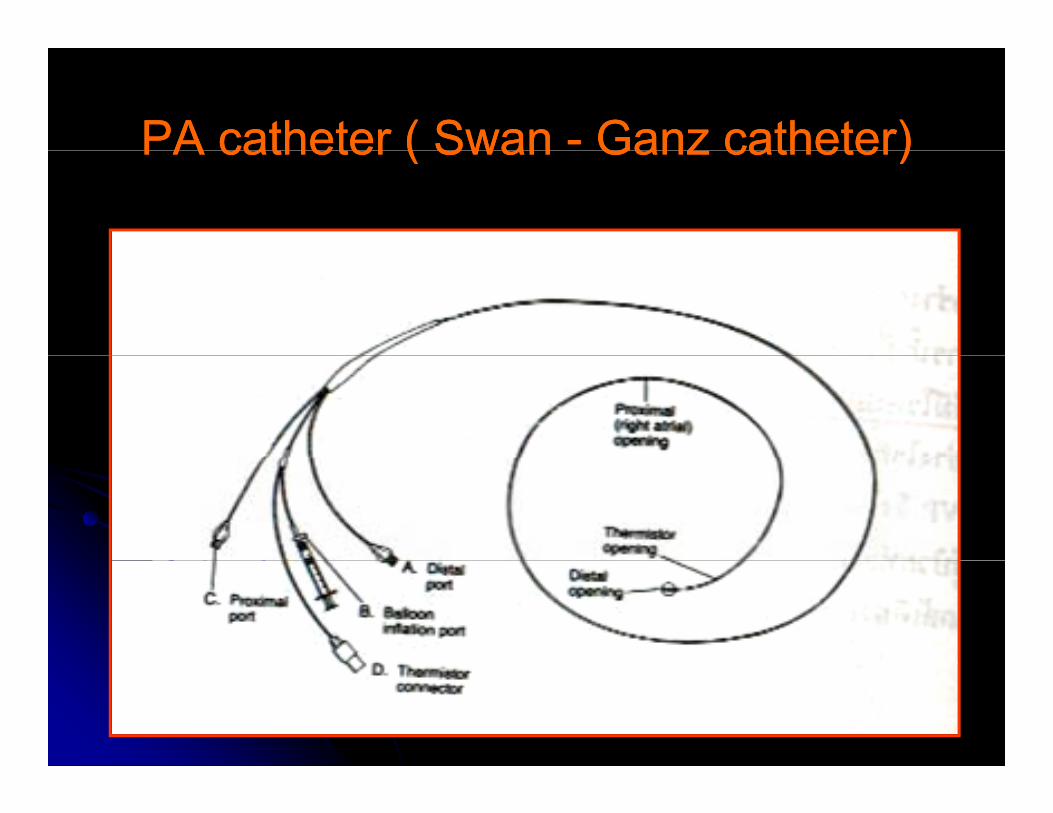
PA catheter ( SwanPA catheter ( Swan -- Ganz catheter)Ganz catheter)PA catheter ( Swan PA catheter ( Swan Ganz catheter)Ganz catheter)
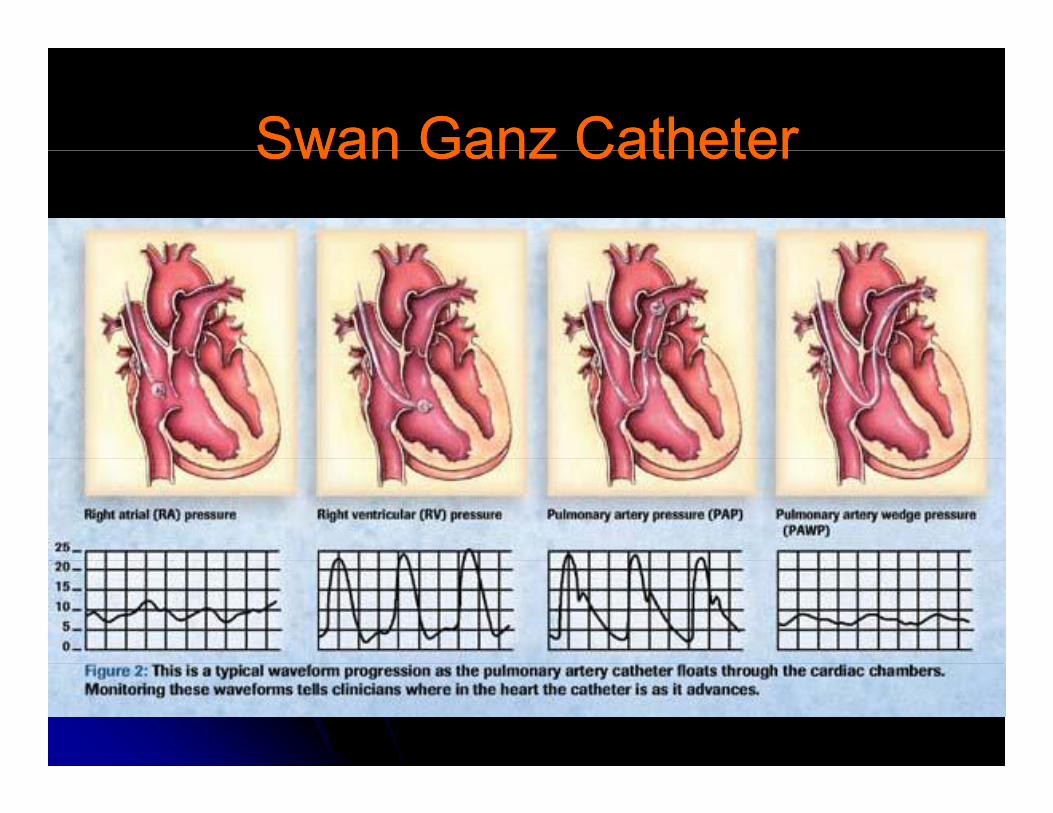
Swan Ganz CatheterSwan Ganz CatheterSwan Ganz CatheterSwan Ganz Catheter
SwanSwan--Ganz catheterGanz catheterSwanSwan Ganz catheterGanz catheter
Intravascular volume statusIntravascular volume statusIntravascular volume statusIntravascular volume statusDifferentiation of pathophysiologic shock Differentiation of pathophysiologic shock statesstatesstatesstatesEtiologies of respiratory and cardiac failureEtiologies of respiratory and cardiac failureCardiac constriction, RCM, tamponadeCardiac constriction, RCM, tamponadeMR, TRMR, TR,,Intracardiac shuntIntracardiac shunt
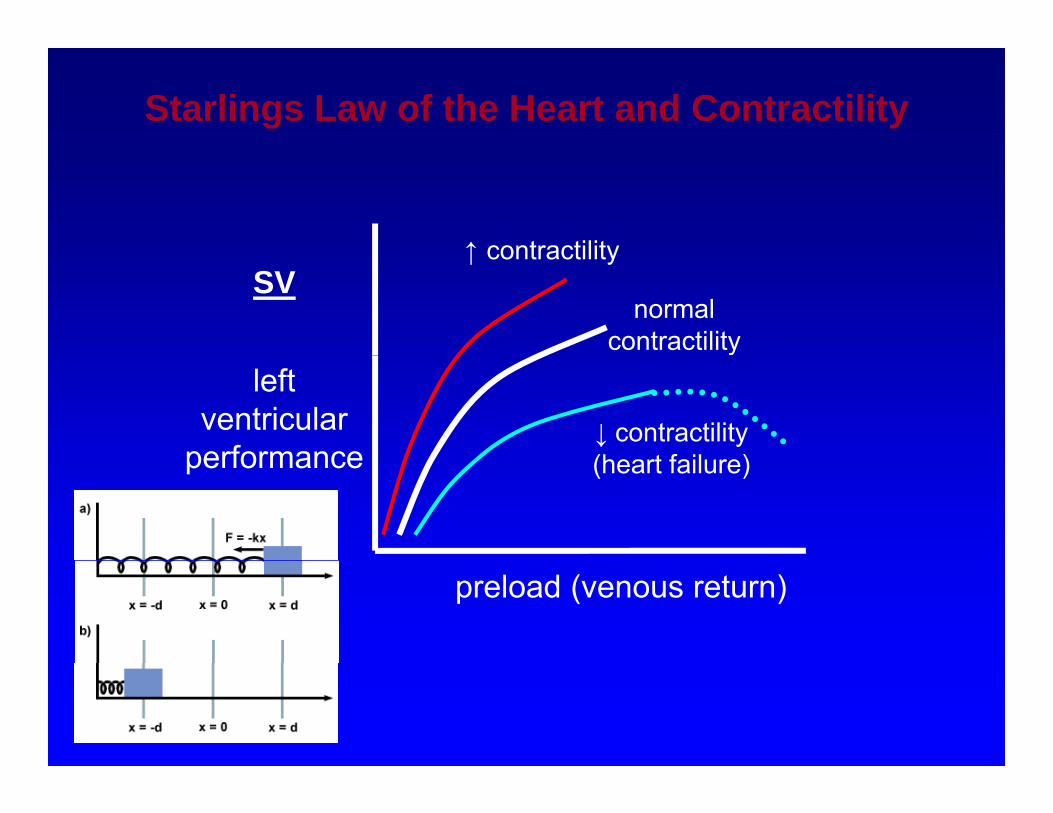
Starlings Law of the Heart and Contractility
↑ contractilitySV
↑ contractility
normal contractility
leftventricular
performance↓ contractility(h t f il )performance (heart failure)
preload (venous return)
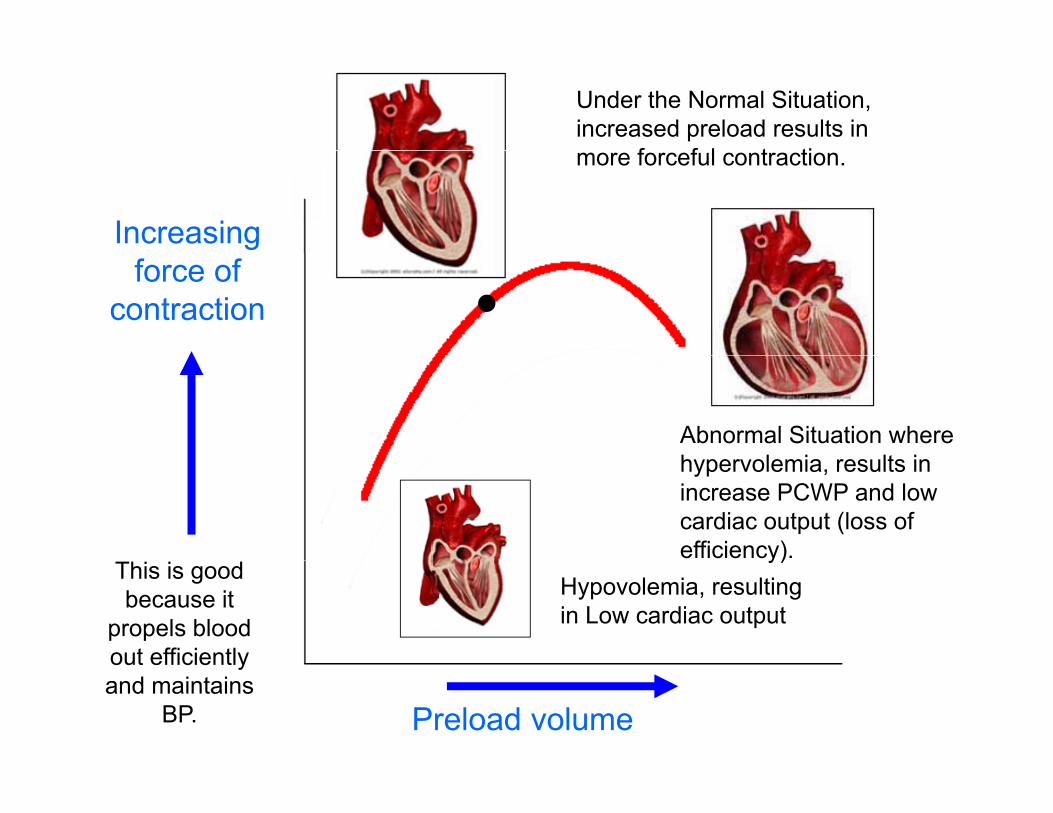
Under the Normal Situation, increased preload results in
f f l t ti
Increasing
more forceful contraction.
force of contraction
Abnormal Situation where h l i lt ihypervolemia, results in increase PCWP and low cardiac output (loss of efficiency).
This is good because it
propels blood out efficiently
Hypovolemia, resulting in Low cardiac output
y)
Preload volume
out efficiently and maintains
BP.
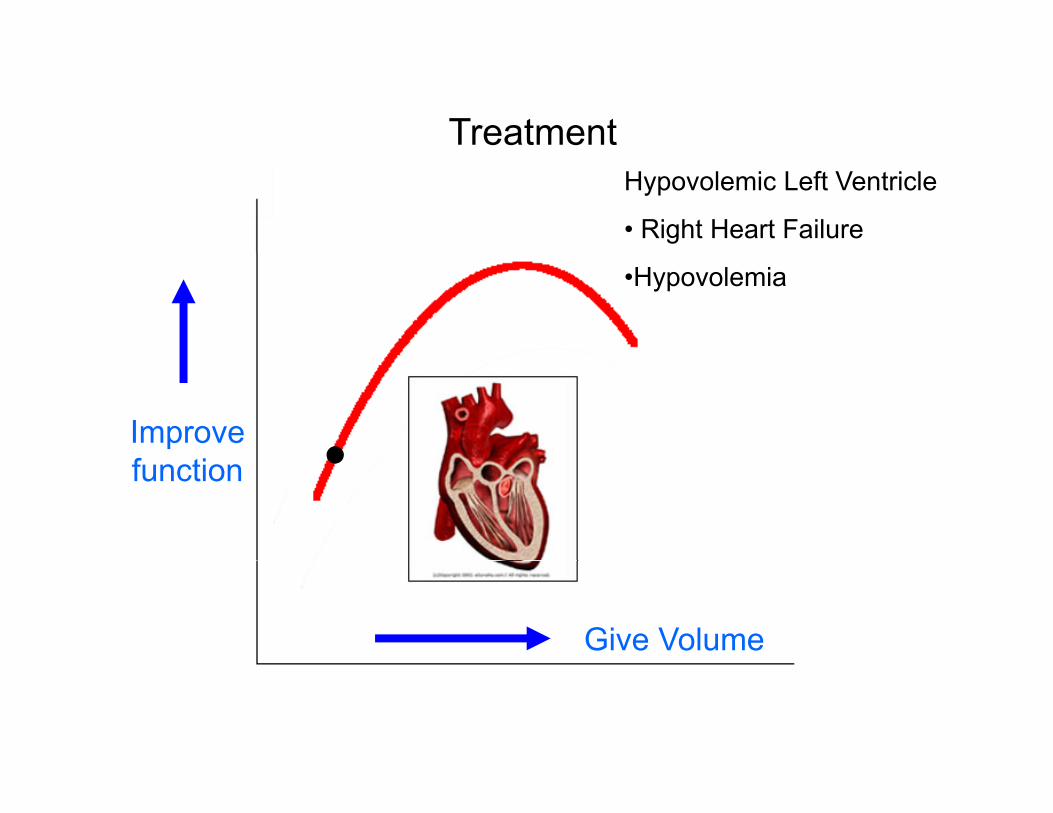
TreatmentHypovolemic Left Ventricle
• Right Heart Failure
•Hypovolemia
Improve ffunction
Give Volume
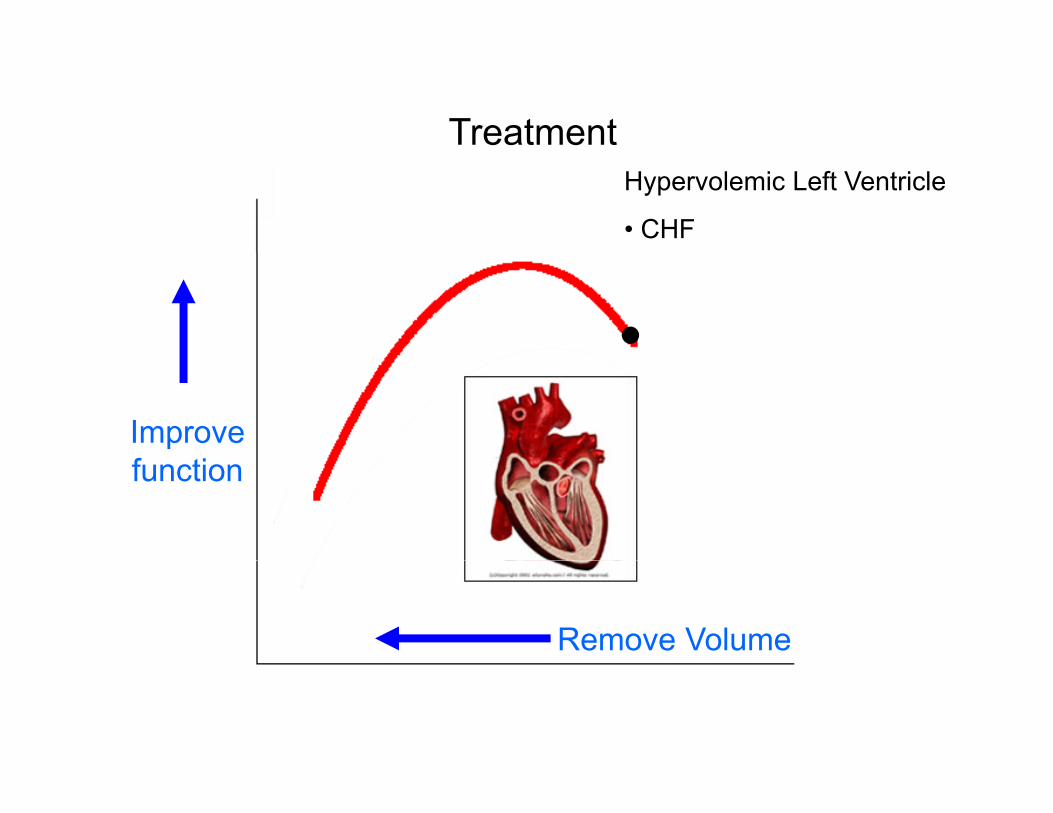
TreatmentHypervolemic Left Ventricle
• CHF
Improve ffunction
Remove Volume
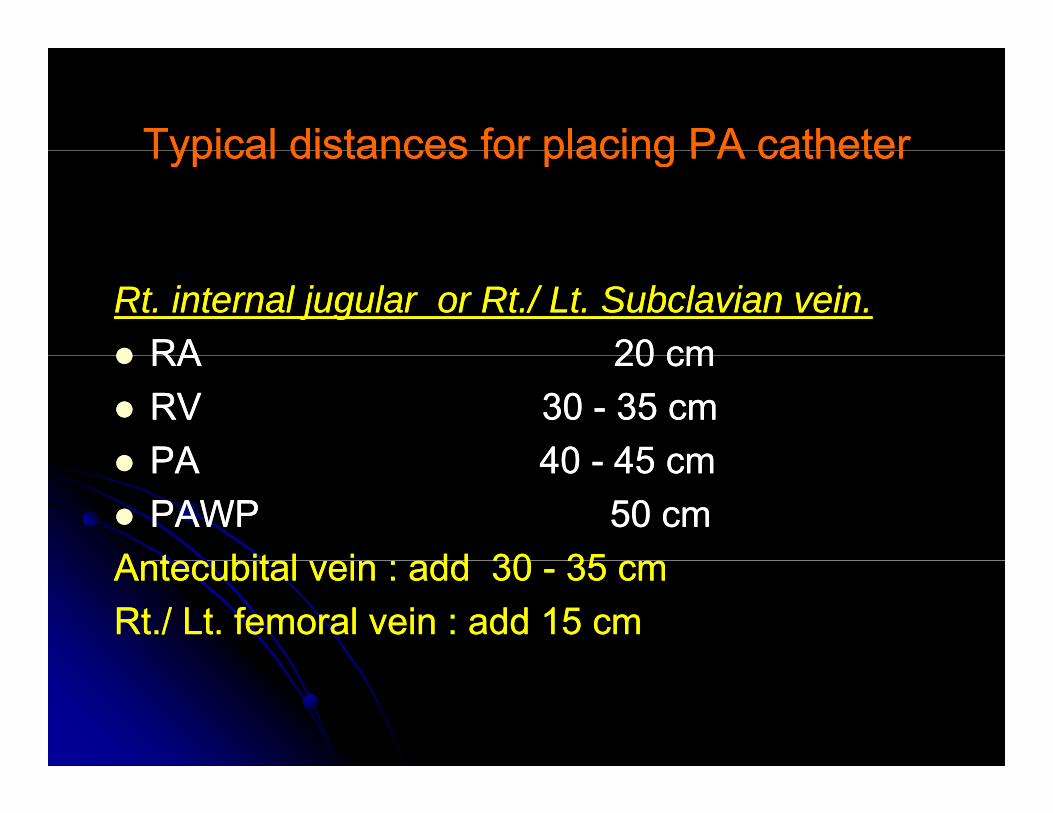
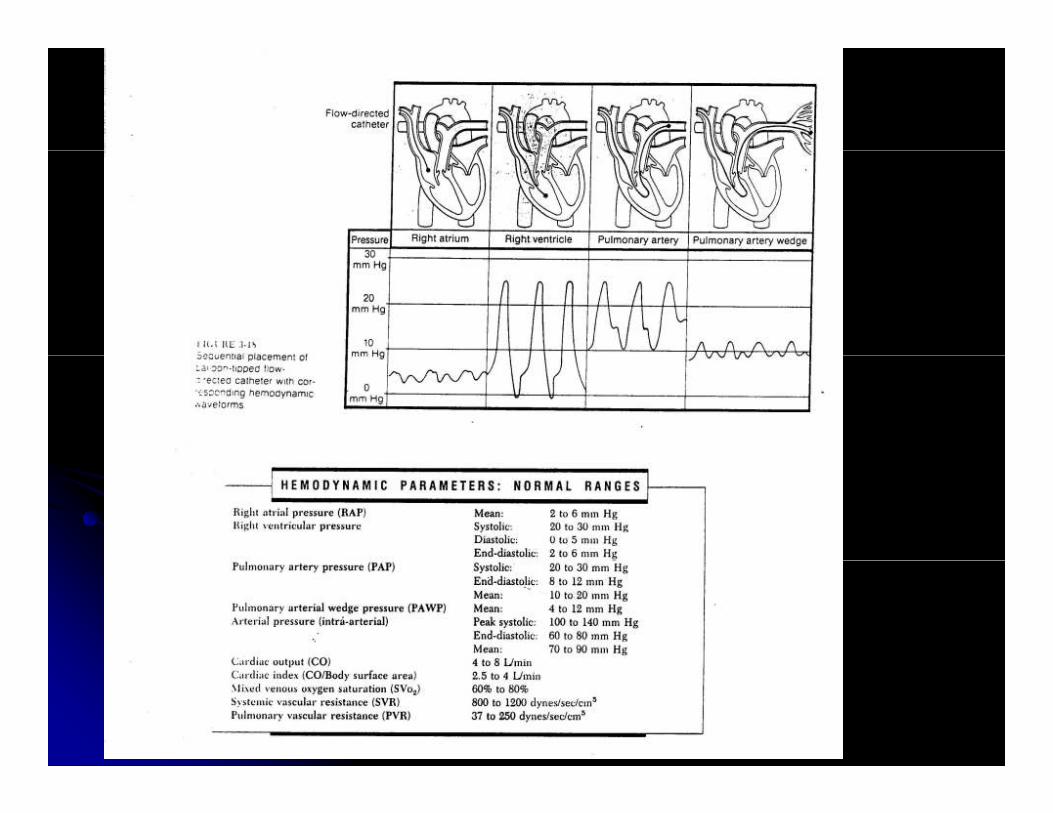
Typical distances for placing PA catheterTypical distances for placing PA catheterTypical distances for placing PA catheterTypical distances for placing PA catheter
Rt. internal jugular or Rt./ Lt. Subclavian vein.Rt. internal jugular or Rt./ Lt. Subclavian vein.RARA 2020 cmcmRA RA 20 20 cmcmRV RV 30 30 -- 35 35 cmcmPAPA 4040 4545 cmcmPA PA 40 40 -- 45 45 cmcmPAWP PAWP 50 50 cmcm
A t bit l i ddA t bit l i dd 3030 3535Antecubital vein : add Antecubital vein : add 30 30 -- 35 35 cmcmRt./ Lt. femoral vein : add Rt./ Lt. femoral vein : add 15 15 cmcm
PAWP waveformPAWP waveformPAWP waveformPAWP waveform
Similar to RA waveformSimilar to RA waveformSimilar to RA waveformSimilar to RA waveformElectromechanical delay is longerElectromechanical delay is longer
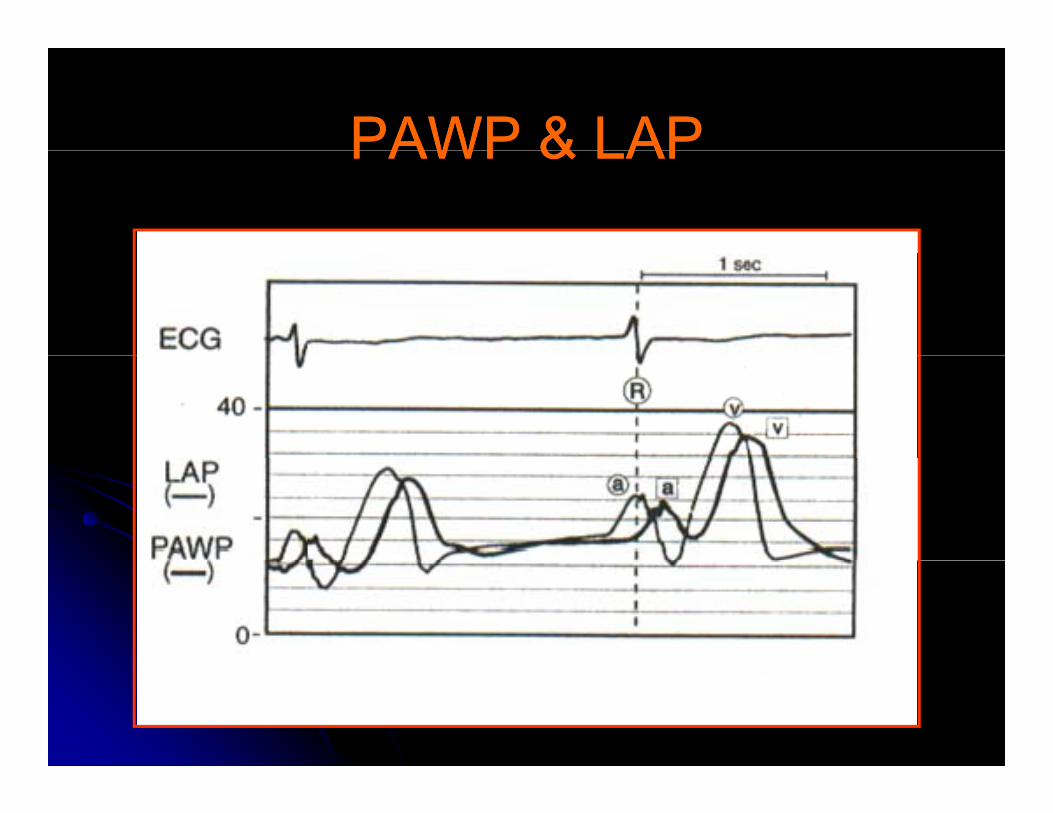
PAWP & LAPPAWP & LAPPAWP & LAPPAWP & LAP
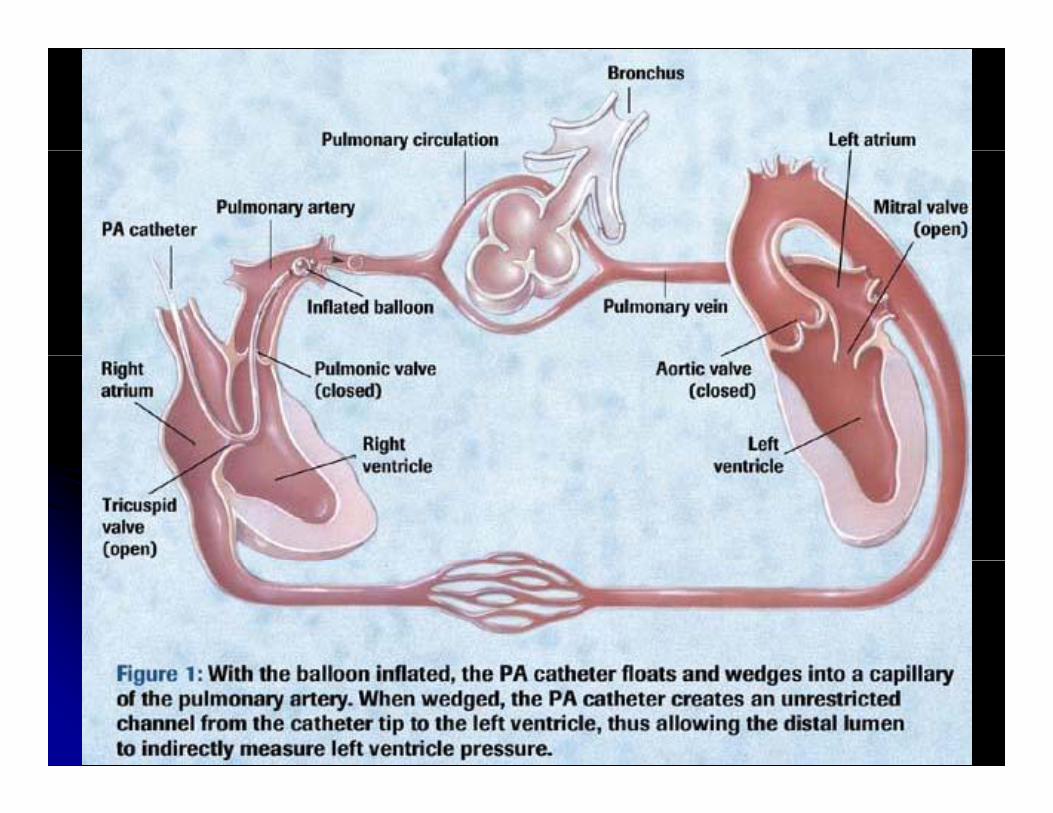
What is wedge pressure?What is wedge pressure?What is wedge pressure?What is wedge pressure?PAWP reflects pulmonary venous pressure and PAWP reflects pulmonary venous pressure and p y pp y pLAP, unless resistance to flow in the large LAP, unless resistance to flow in the large pulmonary v.pulmonary v.PAWP is a delayed presentation of LAP.PAWP is a delayed presentation of LAP.3 3 values of PAWPvalues of PAWP
a wave : the most predictor for LVEDPa wave : the most predictor for LVEDPv wave : assess severity of MRv wave : assess severity of MRyy
mean PAWP : mean LAP, predict risk for mean PAWP : mean LAP, predict risk for pulmonary edema pulmonary edema
PAWP waveformPAWP waveformPAWP waveformPAWP waveform
Elevation of a waveElevation of a waveElevation of a waveElevation of a waveMitral stenosisMitral stenosisLV dysfunction (systolic/diastolic)LV dysfunction (systolic/diastolic)LV dysfunction (systolic/diastolic)LV dysfunction (systolic/diastolic)LV volume overloadLV volume overloadMyocardialMyocardial ischaemiaischaemia/infarction (↓compliance)/infarction (↓compliance)Myocardial Myocardial ischaemiaischaemia/infarction (↓compliance)/infarction (↓compliance)
PAWP waveformPAWP waveformPAWP waveformPAWP waveform
Elevation of v waveElevation of v waveElevation of v waveElevation of v waveMRMRAcute volume overload to LA (eg acute VSD)Acute volume overload to LA (eg acute VSD)Acute volume overload to LA (eg acute VSD)Acute volume overload to LA (eg acute VSD)
Giant v is neither sensitive nor specific for Giant v is neither sensitive nor specific for MRMRsevere MRsevere MR
Swan Ganz catheterSwan Ganz catheterSwan Ganz catheterSwan Ganz catheter
Right lower lobe is the most commonRight lower lobe is the most commonRight lower lobe is the most common Right lower lobe is the most common positionpositionCareful not to inflate balloon >Careful not to inflate balloon > 1010 min espmin espCareful not to inflate balloon > Careful not to inflate balloon > 10 10 min esp min esp when PAP > when PAP > 5050mmHg to avoid pulmonary mmHg to avoid pulmonary infarctioninfarctioninfarctioninfarctionDeep inspiration and advancement of Deep inspiration and advancement of
th t ith h ill h lth t ith h ill h lcatheter with cough will helpcatheter with cough will help
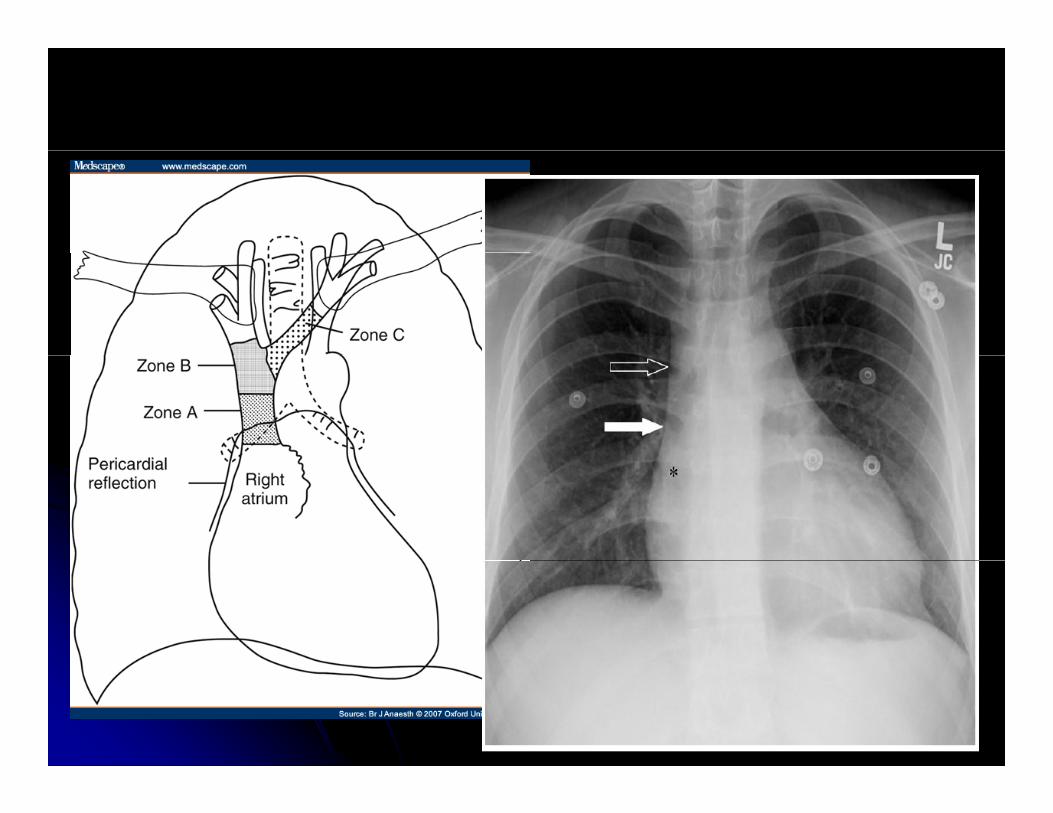
Lung zoneLung zoneLung zoneLung zone
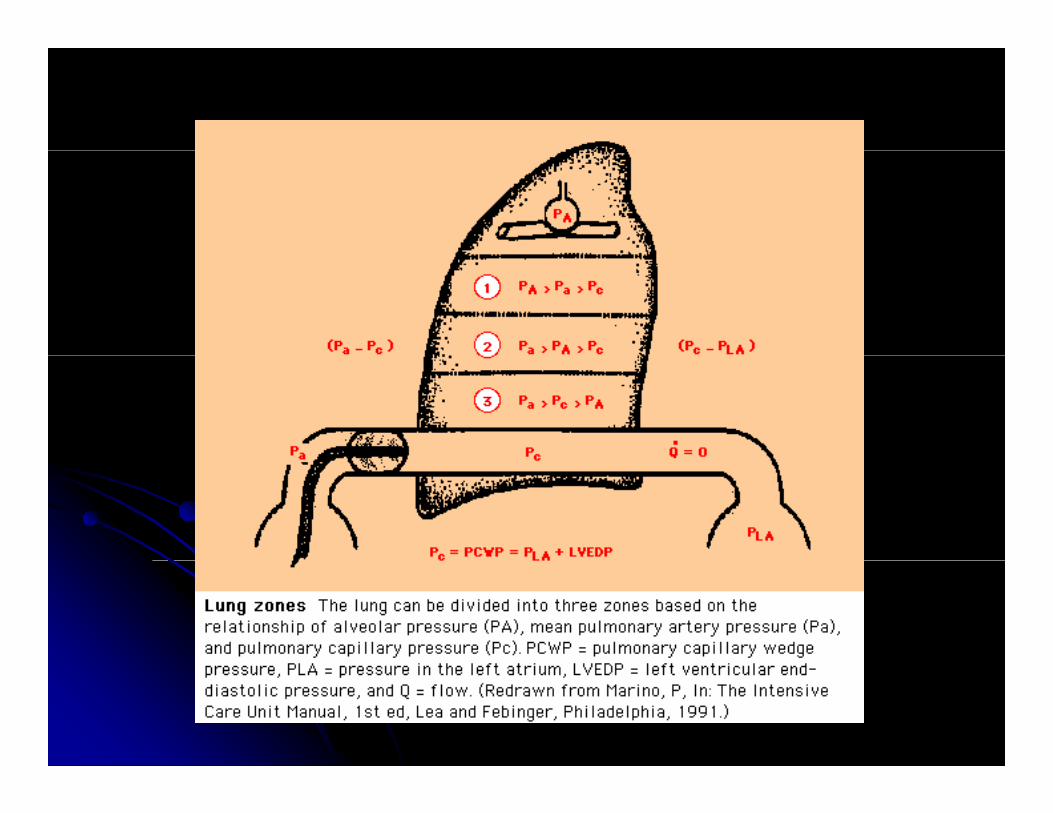
PAWP is accurate when pulmonaryPAWP is accurate when pulmonaryPAWP is accurate when pulmonary PAWP is accurate when pulmonary capillary pressure > mean alveolar pressurecapillary pressure > mean alveolar pressureZoneZone 33Zone Zone 33Tip of catheter should ideally be positioned Tip of catheter should ideally be positioned b l th l l f LAb l th l l f LAbelow the level of LAbelow the level of LAOnly Only 6060% of catheter insertion % of catheter insertion
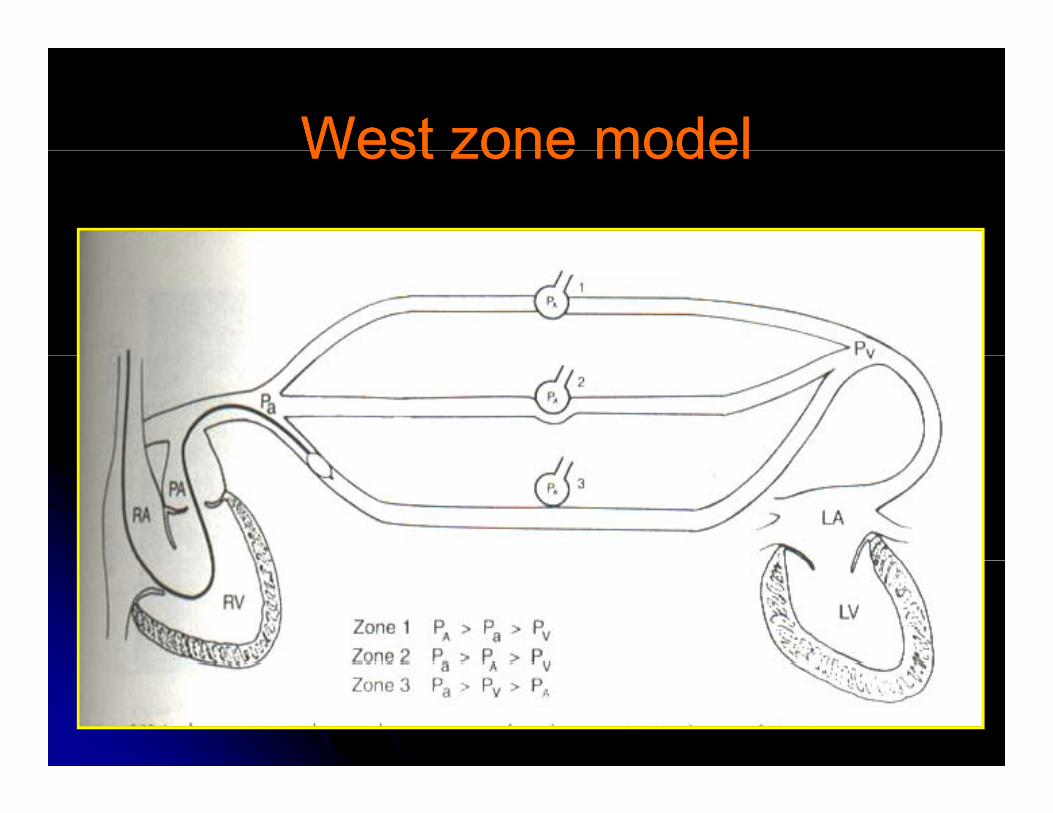
West zone modelWest zone modelWest zone modelWest zone model

Indicators for nonIndicators for non--zonezone 33Indicators for nonIndicators for non zone zone 33
Abnormal position in lateral CXRAbnormal position in lateral CXRAbnormal position in lateral CXRAbnormal position in lateral CXRMarked respiratory variation in PAWPMarked respiratory variation in PAWPPAWPPAWP 5050% f th t f PEEP% f th t f PEEP↑PAWP > ↑PAWP > 5050% of the amount of PEEP % of the amount of PEEP
appliedapplied
PEEP EffectPEEP EffectPEEP EffectPEEP Effect
PEEPPEEPPEEPPEEP
Effect of PEEP to PAWP usually not to beEffect of PEEP to PAWP usually not to beEffect of PEEP to PAWP usually not to be Effect of PEEP to PAWP usually not to be considered clinically significant considered clinically significant
In ZoneIn Zone 33: no airway pressure should be: no airway pressure should beIn Zone In Zone 33: no airway pressure should be : no airway pressure should be transmitted to vasculaturetransmitted to vasculaturePEEP may alter PWAP but that pressure isPEEP may alter PWAP but that pressure isPEEP may alter PWAP but that pressure is PEEP may alter PWAP but that pressure is the effective filling pressure of LVthe effective filling pressure of LV
PEEPPEEPPEEPPEEP
Estimated trueEstimated true transmuraltransmural filling pressurefilling pressureEstimated true Estimated true transmuraltransmural filling pressurefilling pressureNormal lung compliance: Normal lung compliance: PAWPPAWP--11//22PEEPPEEPReduced lung compliance:Reduced lung compliance: PAWPPAWP--11//44PEEPPEEPReduced lung compliance: Reduced lung compliance: PAWPPAWP 11//44PEEPPEEP
10 10 cmHcmH20 20 77..77mmHg so the effect of mmHg so the effect of PEEP is usually smallPEEP is usually smallyyRespiratory variation in PAWP>PA Respiratory variation in PAWP>PA nonnon--zonezone3 3 position of catheterposition of catheterppNOT recommend to turn off PEEP while NOT recommend to turn off PEEP while measure PAWPmeasure PAWP
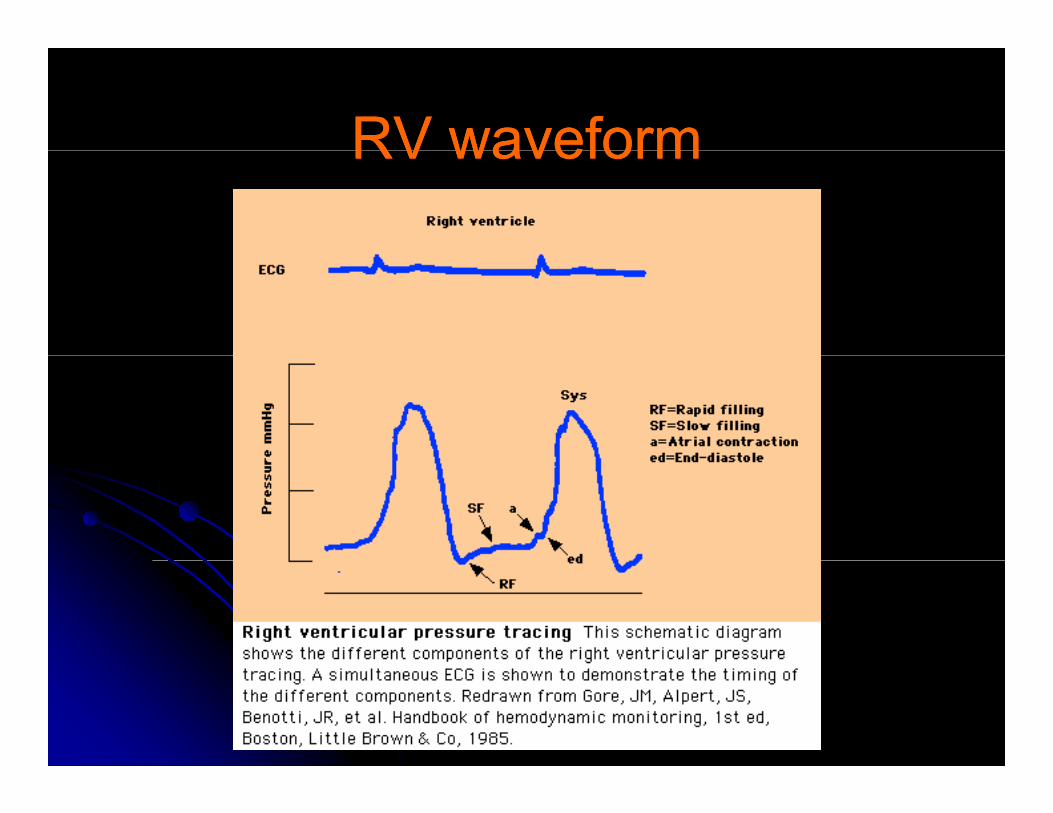
RV waveformRV waveformRV waveformRV waveform
RV waveformRV waveformRV waveformRV waveform
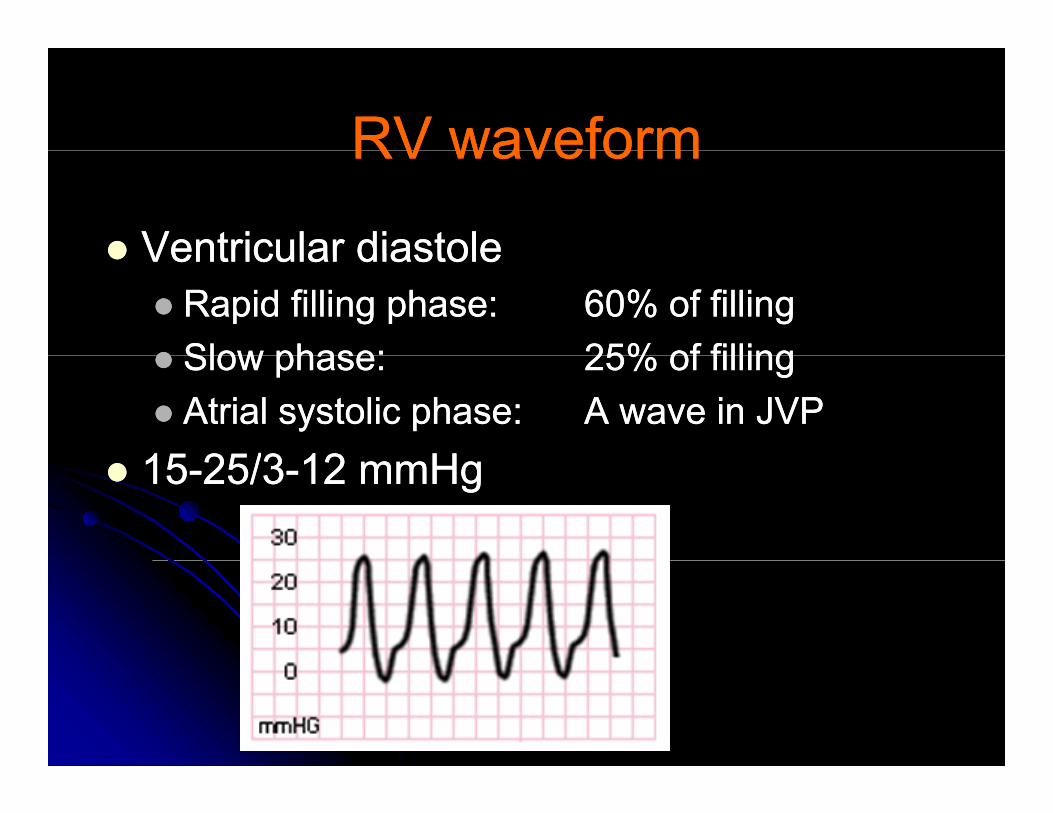
Ventricular diastoleVentricular diastoleVentricular diastoleVentricular diastoleRapid filling phase: Rapid filling phase: 6060% of filling% of fillingSlow phase:Slow phase: 2525% of filling% of fillingSlow phase:Slow phase: 2525% of filling% of fillingAtrial systolic phase:Atrial systolic phase: A wave in JVPA wave in JVP
1515 2525//33 1212 HH1515--2525//33--12 12 mmHgmmHg
High RV systolic pressure inHigh RV systolic pressure inHigh RV systolic pressure in High RV systolic pressure in PHTPHTPSPSPS PS
Acute PE may cause elevation of RV Acute PE may cause elevation of RV b t l >b t l > 4040 5050 HHpressure but rarely > pressure but rarely > 4040--5050mmHg.mmHg.
High endHigh end--diastolic RV pressurediastolic RV pressureHigh endHigh end diastolic RV pressurediastolic RV pressureRV infarction, ischaemiaRV infarction, ischaemiaAny form of cardiomyopathyAny form of cardiomyopathyAny form of cardiomyopathyAny form of cardiomyopathyConstriction, tamponadeConstriction, tamponade
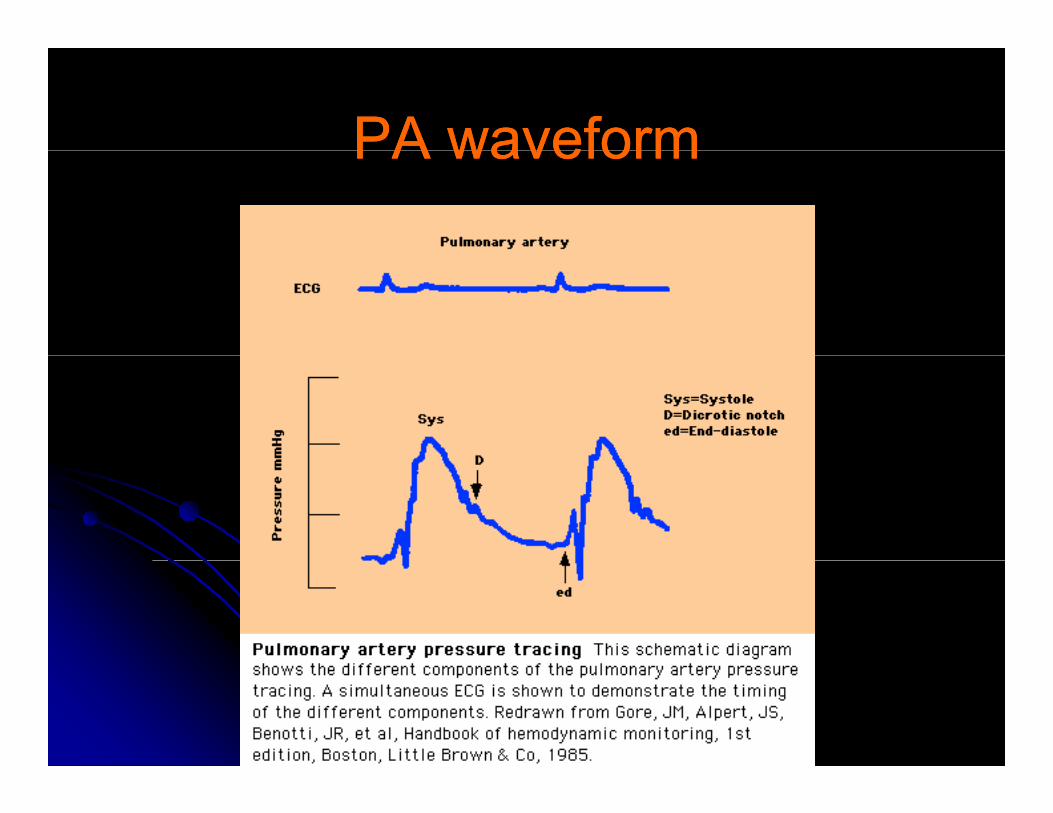
PA waveformPA waveformPA waveformPA waveform
PA waveformPA waveformPA waveformPA waveform
1515--2525//88--1515mmHgmmHg1515 2525//88 1515mmHgmmHgHigh PA pressureHigh PA pressure
V l l dV l l dVolume overloadVolume overloadIncreased PVR: all forms of lung disease, Increased PVR: all forms of lung disease, PPHT PE hypoxemia LV failure MV diseasePPHT PE hypoxemia LV failure MV diseasePPHT, PE, hypoxemia, LV failure, MV diseasePPHT, PE, hypoxemia, LV failure, MV disease
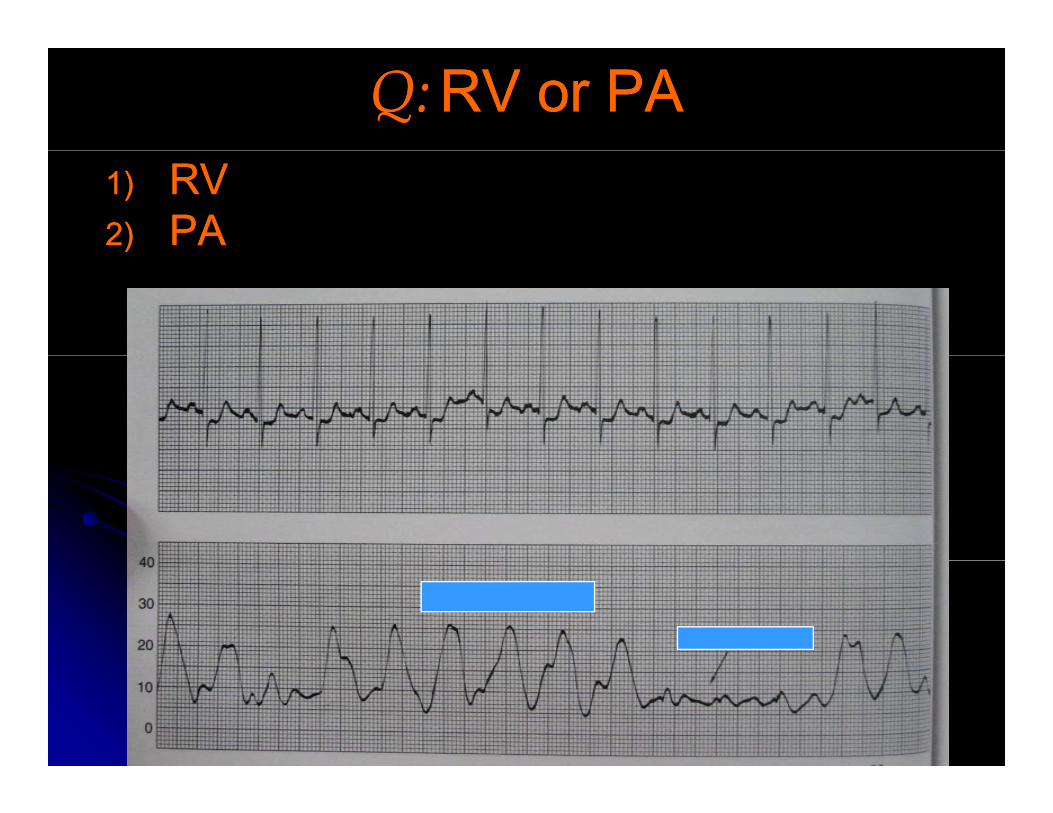
Q:Q: RV or PARV or PA1)1) RVRV2)2) PAPA
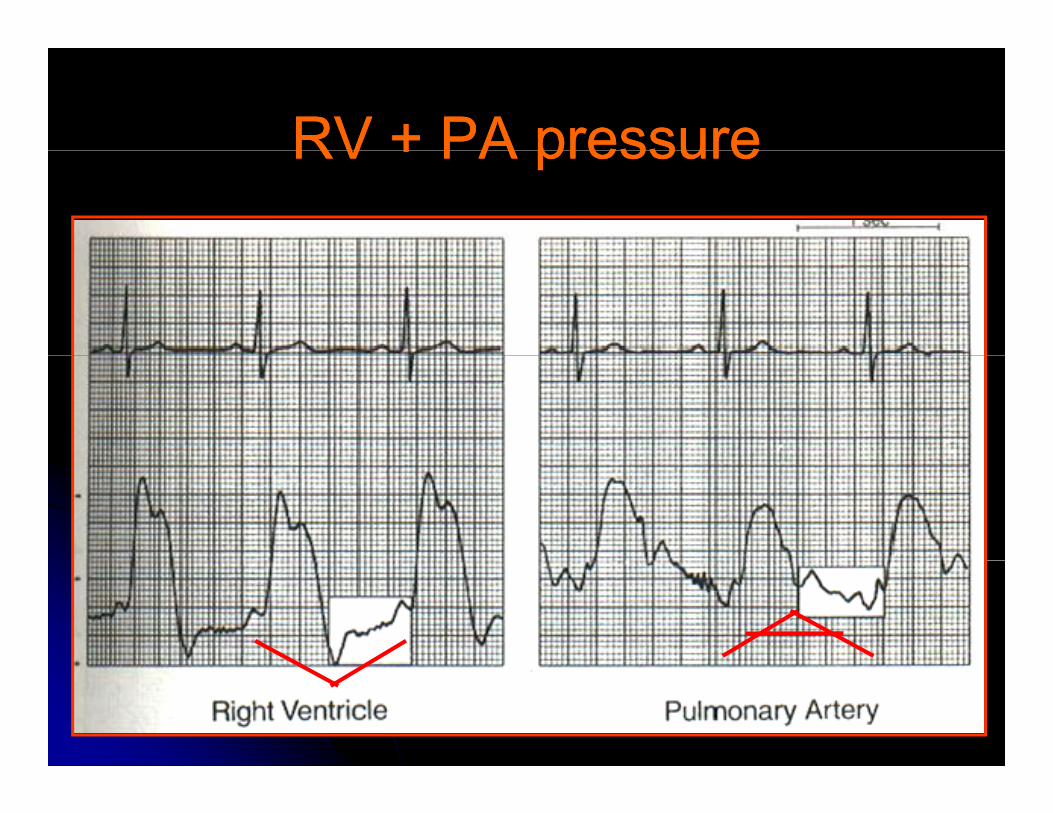
RV + PA pressureRV + PA pressureRV + PA pressureRV + PA pressure
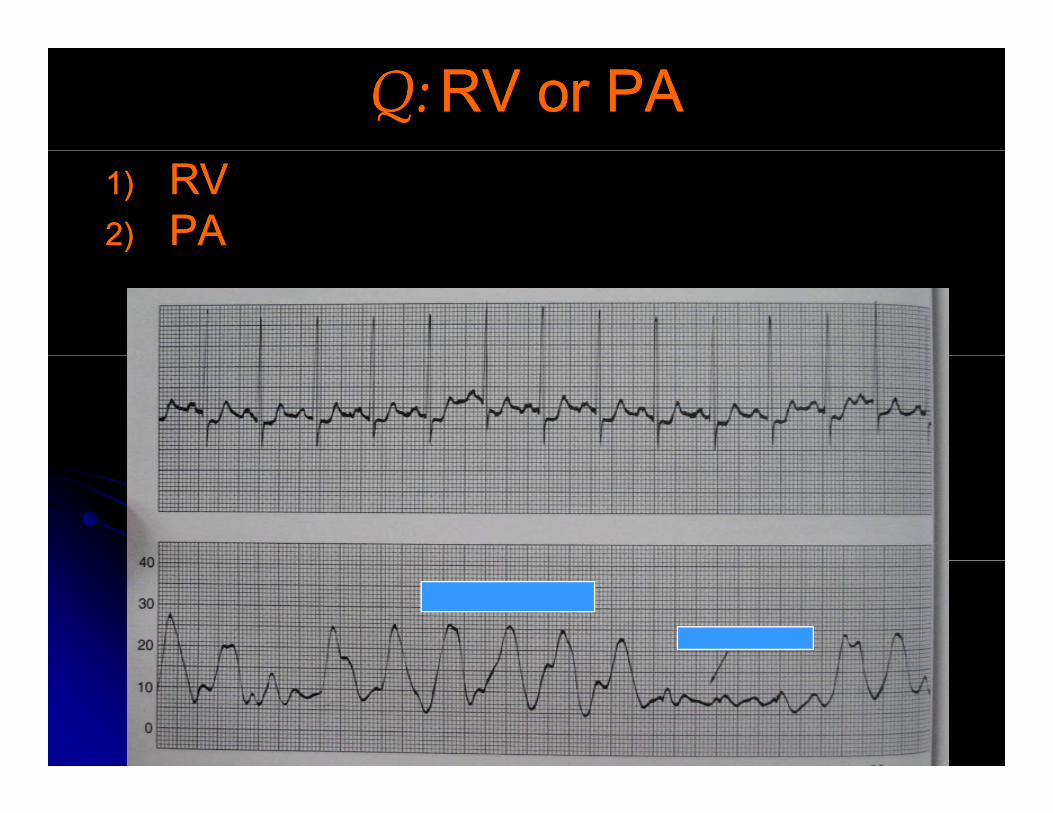
Q:Q: RV or PARV or PA1)1) RVRV2)2) PAPA
SHUNTSHUNTSHUNTSHUNT
OO22 step upstep upOO2 2 step up step up RA > RA > 77%%RV >RV > 55%%RV > RV > 55%%PA > PA > 55%%
PA OPA O22sat > sat > 8585

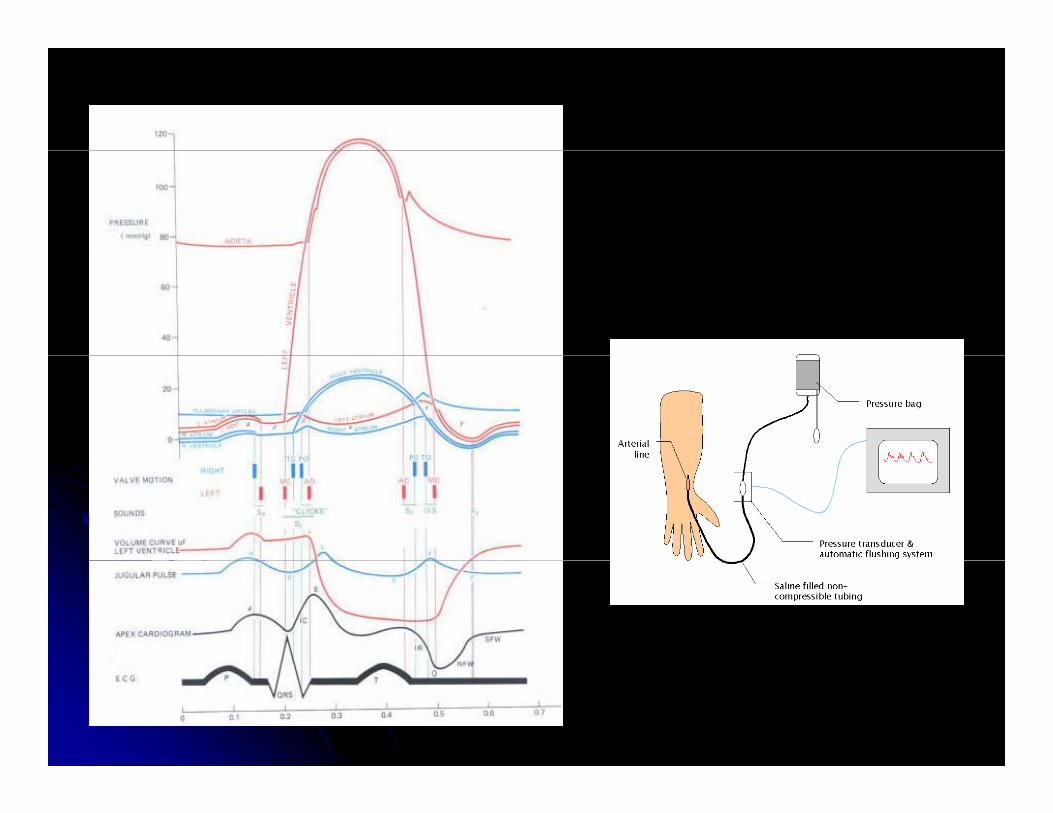
AA--linelineAA lineline
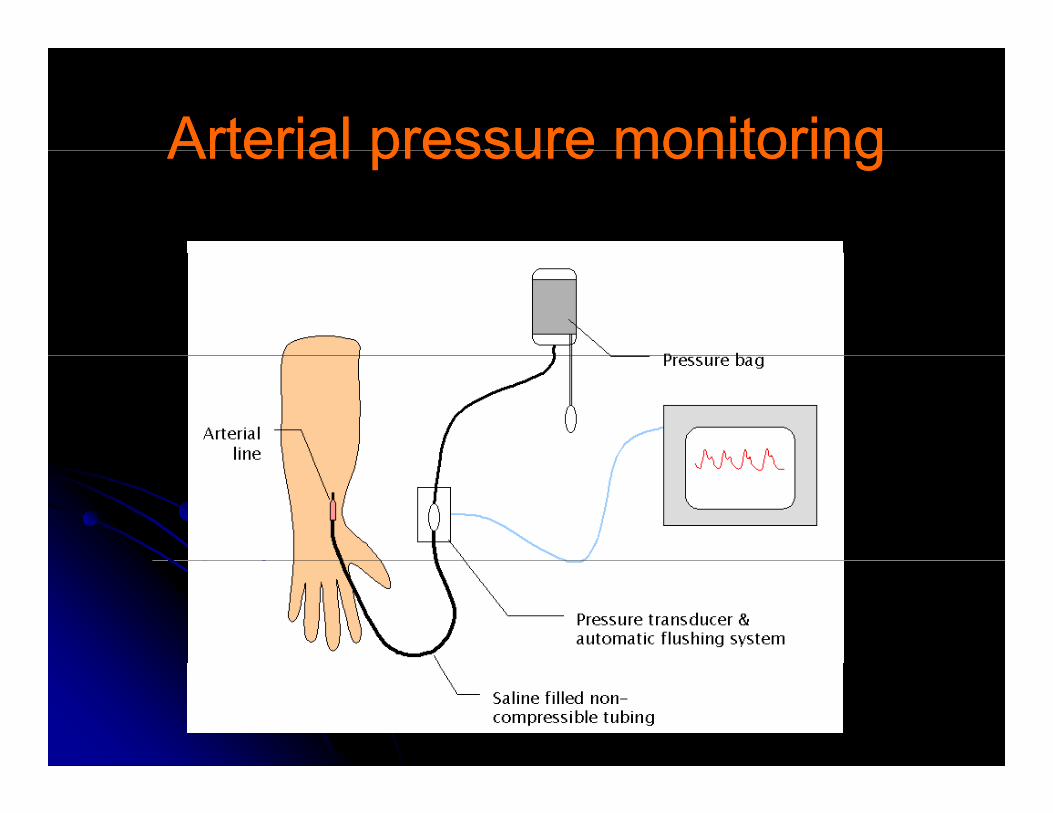
Arterial pressure monitoringArterial pressure monitoringArterial pressure monitoringArterial pressure monitoring
Arterial blood pressureArterial blood pressureArterial blood pressureArterial blood pressure
วัดความดนัวัดความดนั 22 ขาง ขาง :: diagnosis of many disordersdiagnosis of many disordersวดความดนวดความดน 22 ขาง ขาง : : diagnosis of many disordersdiagnosis of many disorders
วัดความดนัวัดความดนั 22 ทา ทา : : postural hypotensionpostural hypotension
L lL lLevelLevelWaveformWaveformECGECG
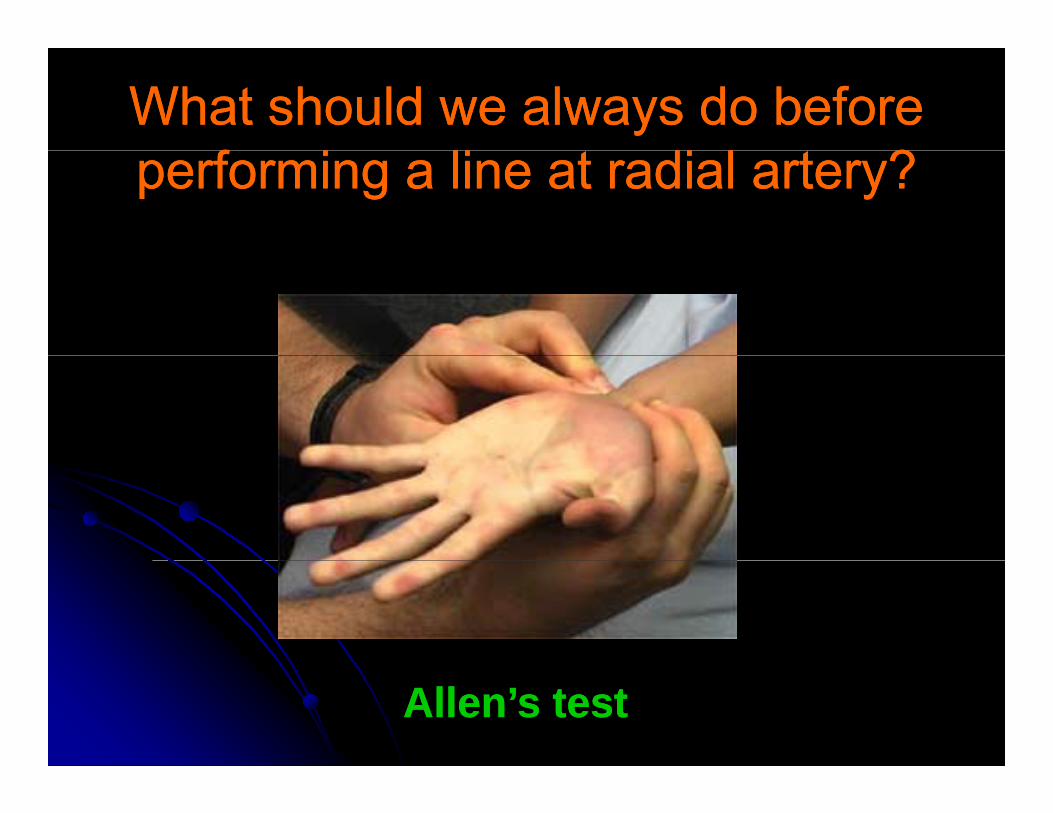
What should we always do before What should we always do before f i li di l ?f i li di l ?performing a line at radial artery?performing a line at radial artery?
Allen’s testAllen’s test
Postural hypotensionPostural hypotensionPostural hypotensionPostural hypotension
11 HypovolumiaHypovolumia1.1. HypovolumiaHypovolumia2.2. Abnormal autonomic nervous systemAbnormal autonomic nervous system
TT22DMDM-- TT22DMDM-- ElderlyElderly-- DrugsDrugs-- Shy Drager syndromeShy Drager syndromeShy Drager syndromeShy Drager syndrome
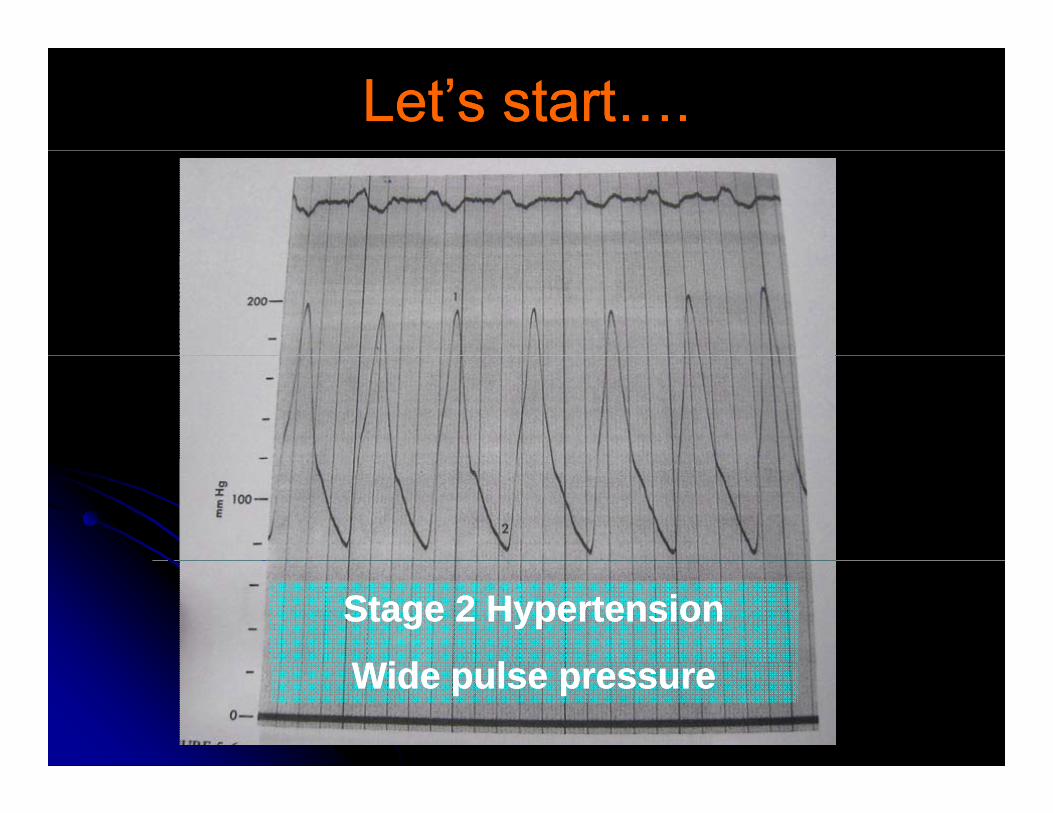
Let’s start….Let’s start….
Stage Stage 2 2 HypertensionHypertension
Wid lWid lWide pulse pressureWide pulse pressure
Wide pulse pressureWide pulse pressureWide pulse pressureWide pulse pressureAtheroAtheroHeart blockHeart blockThyroxThyroxRegurRegurRegurRegurHypertensionHypertensionสําคัญสําคัญ anemiaanemiaออนเพลียออนเพลีย beri beriberi beri44p p ทีเด็ดทีเด็ด
เบ็ดเสร็จ เบ็ดเสร็จ aneurysmaneurysmอยาลืมอยาลืม AVMAVM
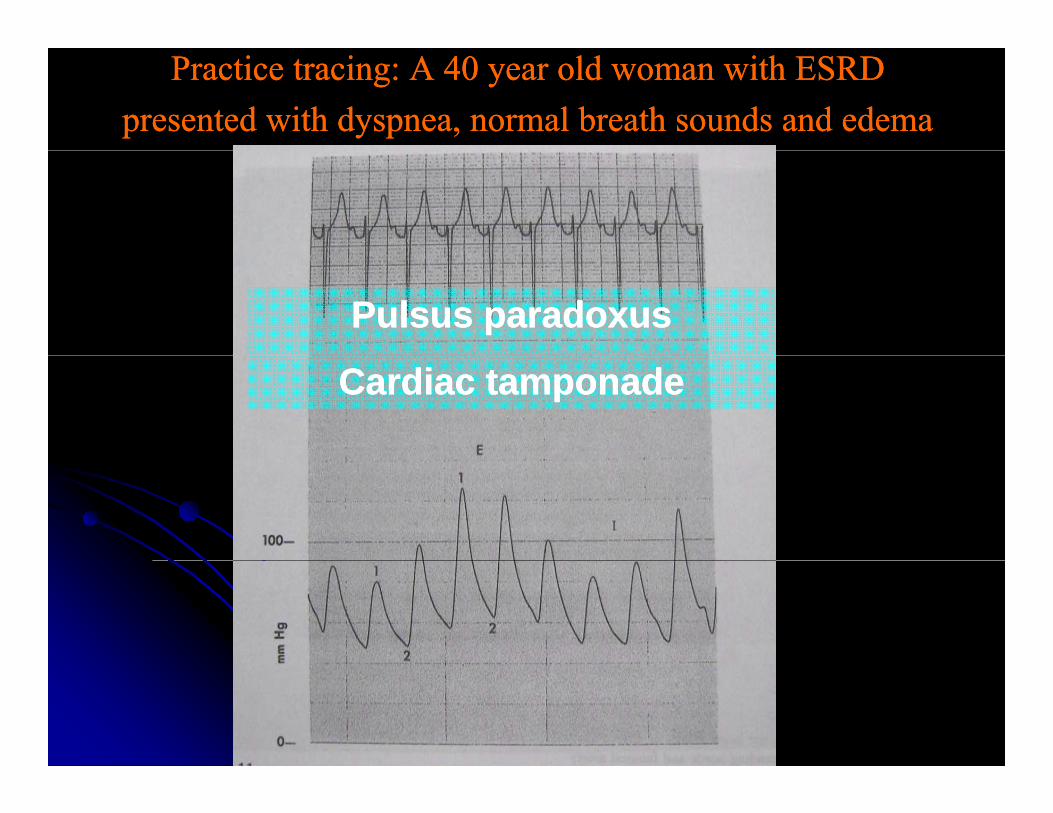
Practice tracing: A Practice tracing: A 40 40 year old woman with ESRD year old woman with ESRD presented with dyspnea, normal breath sounds and edemapresented with dyspnea, normal breath sounds and edema
Pulsus paradoxusPulsus paradoxus
Cardiac tamponadeCardiac tamponade
Pulsus paradoxusPulsus paradoxusPulsus paradoxusPulsus paradoxus
Contrictive pericarditisContrictive pericarditisContrictive pericarditisContrictive pericarditisRestrictive cardiomyopathyRestrictive cardiomyopathyS i di (COPD)S i di (COPD)Severe airway disease (COPD)Severe airway disease (COPD)Pulmonary embolismPulmonary embolismRV infarctionRV infarction
Tamponade with no pulsus Tamponade with no pulsus ddparadoxusparadoxus
Elevated LVEDPElevated LVEDPElevated LVEDPElevated LVEDPASDASDA ti it tiA ti it tiAortic regurgitationAortic regurgitationPHTPHT
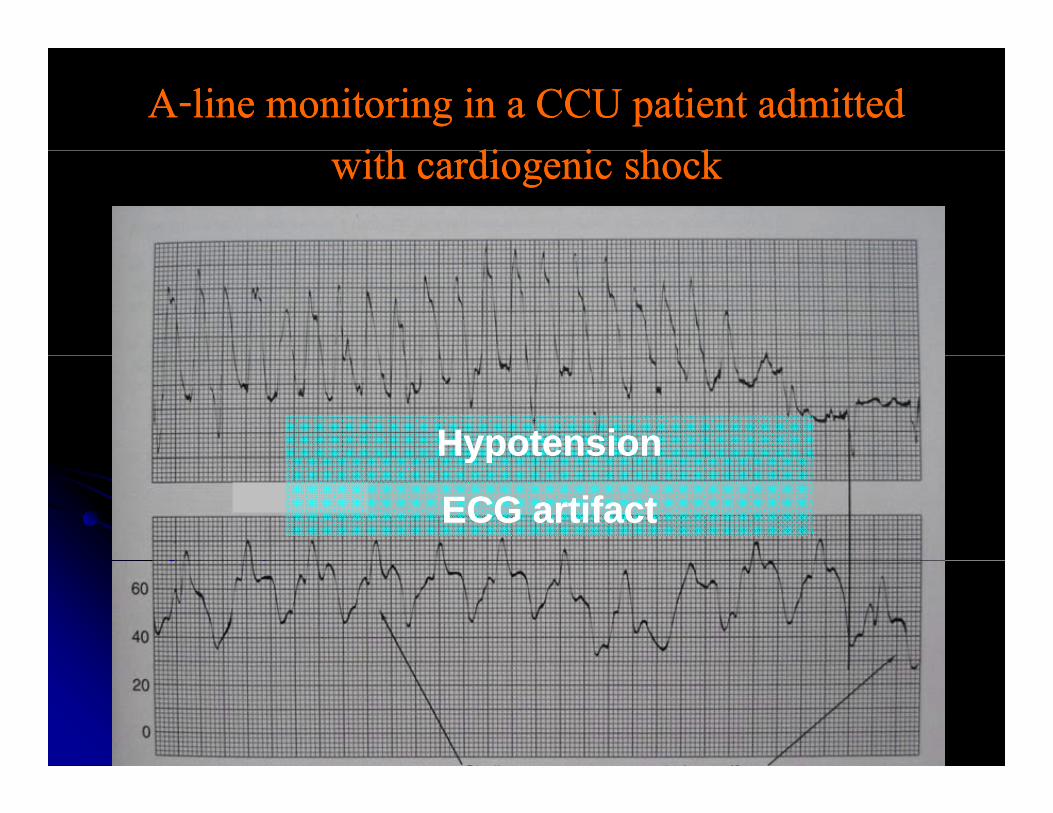
AA--line monitoring in a CCU patient admitted line monitoring in a CCU patient admitted i h di i h ki h di i h kwith cardiogenic shockwith cardiogenic shock
HypotensionHypotensionypyp
ECG artifactECG artifact
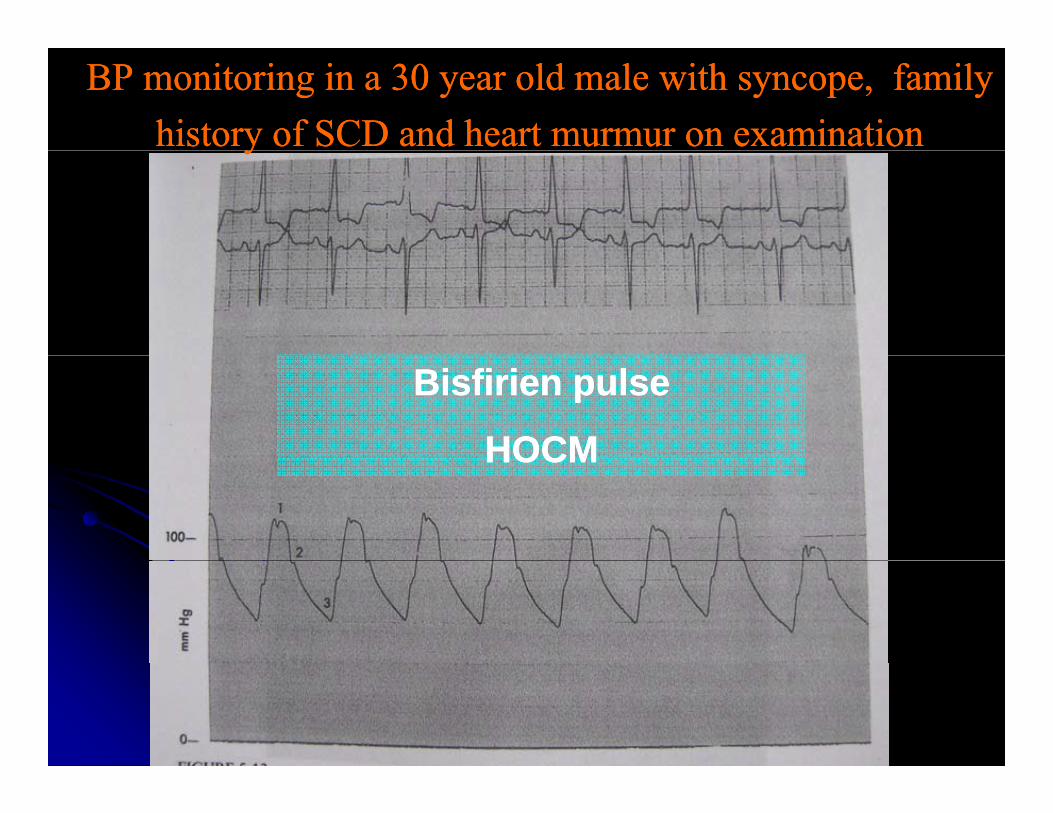
BP monitoring in a BP monitoring in a 30 30 year old male with syncope, family year old male with syncope, family history of SCD and heart murmur on examinationhistory of SCD and heart murmur on examinationyy
Bisfirien pulseBisfirien pulse
HOCMHOCMHOCMHOCM
Pulsus bisfirienPulsus bisfirienPulsus bisfirienPulsus bisfirien
HCMHCMHCMHCMARARAS ith ARAS ith ARAS with ARAS with AR
IABP patientIABP patient
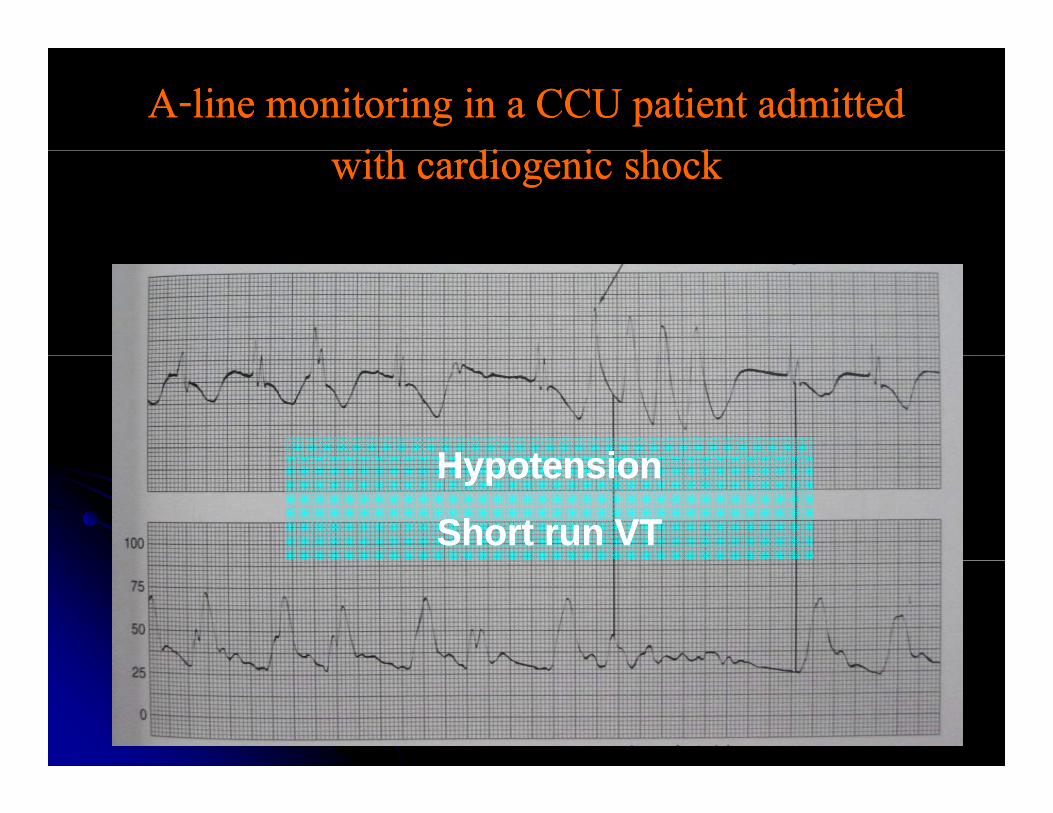
AA--line monitoring in a CCU patient admitted line monitoring in a CCU patient admitted i h di i h ki h di i h kwith cardiogenic shockwith cardiogenic shock
H t iH t iHypotensionHypotension
Short run VTShort run VT
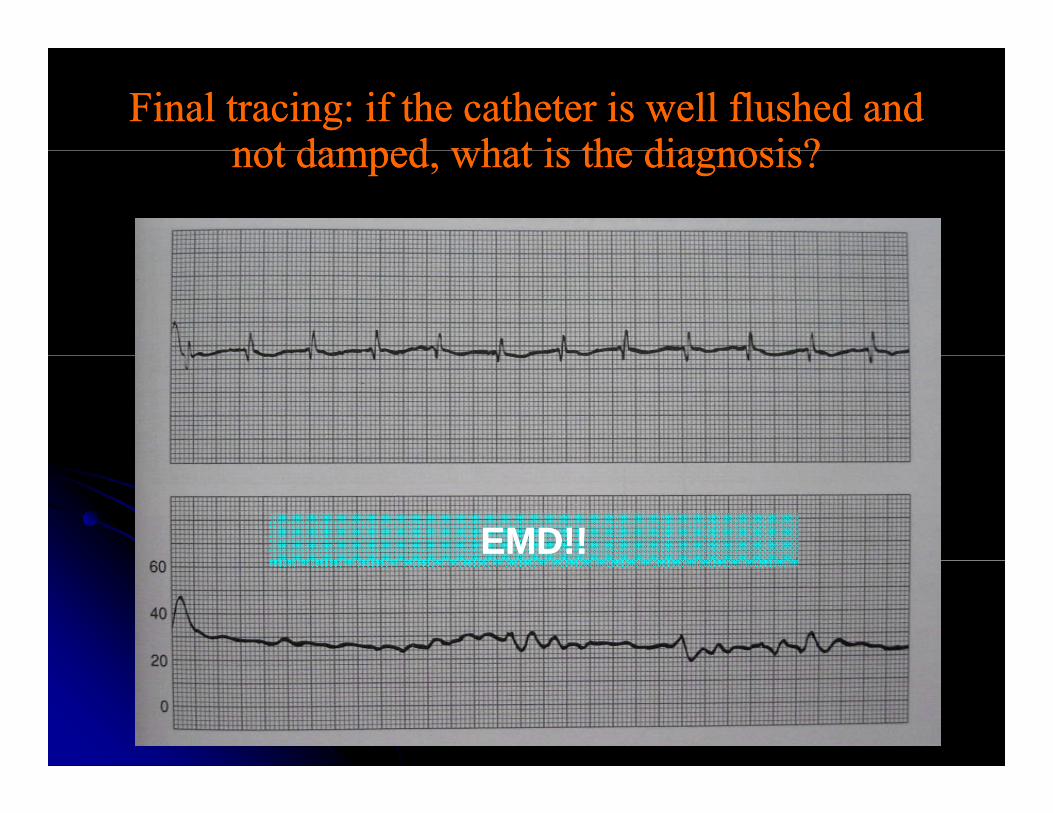
Final tracing: if the catheter is well flushed and Final tracing: if the catheter is well flushed and not damped what is the diagnosis?not damped what is the diagnosis?not damped, what is the diagnosis?not damped, what is the diagnosis?
EMD!!EMD!!

Endothelial erosion – the endothelium is largely absent, macrophages have tt h d t th d i ti (SEM)attached to the exposed intima (SEM)