when musculoskeletal conditions and mental disorders occur
TRANSCRIPT

bulle
tin
80Bulletin 80 • September 2010
When musculoskeletal conditions and mental disorders occur together
Summary• Musculoskeletalconditionsandmentaldisorderscausefewdeathsbutmuchpain,
disabilityanddistress.Botharecommonandarerecognisedasmajorhealthconcerns.Theiroccurrencetogetherinthesameperson(knownascomorbidity)complicatestheirtreatmentandmanagement.
• Thisbulletinpresentsthemostreliable,robustandup-to-dateestimatesofthenumberofpeoplewithbothmusculoskeletalconditionsandmentaldisorders;estimatesthatareimportantinassessingtheneedforintegratedcare.
• Morethan6.1millionAustraliansaged16–85yearssufferfromamusculoskeletalconditionatapointintime(38%ofthatpopulation)and3.2million(20%)experienceamentaldisorderina12-monthperiod.
ContentsSummary .................................................................................................................................................................................................... 1Introduction ............................................................................................................................................................................................... 2The nature of musculoskeletal conditions .................................................................................................................................................. 3The nature of mental disorders .................................................................................................................................................................. 5Comorbidity—its causes and consequences ............................................................................................................................................. 7Prevalence of comorbidity .......................................................................................................................................................................... 8Observed and expected prevalence of comorbidity ................................................................................................................................. 10Comorbidity among people with musculoskeletal conditions ................................................................................................................. 10Comorbidity among people with mental disorders ..................................................................................................................................11Types of mental disorders in people with musculoskeletal conditions .....................................................................................................12Conclusion .................................................................................................................................................................................................14Acknowledgments ....................................................................................................................................................................................14References .................................................................................................................................................................................................15Appendix: Statistical table and methods ................................................................................................................................................. 16
(summary continued overleaf)

WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
2
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
• Over1.5millionpeople(10%ofAustraliansaged16–85years)hadatleastonemusculoskeletalconditionandonementaldisorderinthepreceding12months.Thenumberoffemalesexperiencingthiscomorbidity(862,000)wasgreaterthanthenumberofmales(671,000).Theextentofcomorbidityincreasedsharplyineachsuccessiveagegroupuntil45–54years,afterwhichitdecreasedsharply.
• Therewere470,000moreAustralianswhohadbothamusculoskeletalconditionandamentaldisorderin2007thanwouldbeexpectedifoccurrencesofthetwoconditionswereindependentofoneanother.
• Publishedstudiessuggestthatcausalpathwaysaremorelikelytobefrommusculoskeletalconditionstomentaldisordersthanthereverse,althoughthelattercanalsooccur.Overall,in2007,25%ofpeoplewithamusculoskeletalconditionalsohadamentaldisorder,themostcommonofwhichwereanxietydisorders.
• Theclearassociationbetweenmusculoskeletalconditionsandmentaldisordersfoundinthisstudyemphasisestheneedforhealth-careproviderstobeawareofandprovideforamultidisciplinaryapproachtothemanagementofthiscomorbidity.
Introduction
Musculoskeletalconditionsandmentaldisorderscanbebothsevereandpersistentillnesses,contributingsignificantlytolevelsofillhealth.Musculoskeletalconditions,whichincludearthritis,osteoporosisandbackpain,resultinfewdeathsbutcausesignificantpainanddisability.Theyseverelylimitaperson’sabilitytoperformeverydaytasksathomeandatwork(AIHW2008).Mentaldisordersincludethecommondisordersofanxietyanddepression,aswellaslesscommonorlow-prevalencedisorders,suchasschizophrenia.Althoughfewerdeathsareattributedtomentaldisorders(otherthantheirhighassociationwithsuicide)thanotherleadinghealthproblems,theyarethecauseofmuchdistressanddisabilityinthepopulation(AIHW2010).
Theoccurrencetogetherofmusculoskeletalconditionsandmentaldisordersinthesameperson,knownascomorbidity,oftencomplicatestreatmentandmanagementplans.Whilesomeissuesremainspecifictoeachconditionordisorder,thestandardtreatmentofmentaldisordersmayneedtobemodifiedinviewofthephysicalchangesassociatedwithamusculoskeletalconditionorwiththemedicationusedforitstreatment.Similarly,themanagementofmusculoskeletalconditionsmayneedtobemodifiedinthepresenceofamentaldisorder.
Sincetheclinicalmanagementofpeoplewithcomorbidconditionscanbemorecomplexandtimeconsumingthanforthosewithsingleconditions,informationabouttheprevalenceofcomorbidityshouldhelpassesstheneedformoreintegratedcare.ThisbulletindocumentsthecomorbidityofmusculoskeletalconditionsandmentaldisordersinAustraliawiththataiminmind.
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
Bulletin 80 • September 2010
3
The nature of musculoskeletal conditions
Musculoskeletalconditionsarecommonandvaried.Theyarecharacterisedbyhighprevalence,generallylateageofonset,longdurationandlowfatality.Theyarealsosignificantcontributorstophysicaldisability.
Therearemorethan200formsofmusculoskeletalconditions,includingvarioustypesofarthritis,whichaffectthejoints,bones,musclesandtheirattachmentstoeachother.Theirsymptomsandproblemsmayarisefromtheoveruseofjoints,congenitalanomalies,metabolicorbiochemicalabnormalities,infections,inflammation,traumaandcancer.
Themostcommonlyoccurringmusculoskeletalconditionsarebackpainandvariousformsofarthritis.Otherwell-knownconditionsincludeosteoporosis,slippeddisk,gout,systemiclupuserythmatosus(SLEorlupus),‘frozenshoulder’andscoliosis.AbriefdescriptionofsomecommonmusculoskeletalconditionsisgiveninBox1.
Box 1: Common musculoskeletal conditionsArthritis A group of conditions involving inflammation of the joints, causing
pain, stiffness, deformity and disability. More than 100 different forms of arthritis are recognised, prominent among which are osteoarthritis, rheumatoid arthritis and gout.
Osteoarthritis The most common form of arthritis, caused mainly by the accumulated wear of the cartilage in joints. This wear and tear disrupts the normal function of the joint, causing pain and functional limitations. The condition affects mainly the hands, spine, and weight-bearing joints, such as the hips, knees and ankles.
Rheumatoid arthritis A chronic, inflammatory, autoimmune disease in which the immune system attacks the tissues lining the joints. The inflamed joints often cause pain, heat and swelling, and can lead to functional limitations and severe disability.
Gout Gout is characterised by painful swelling in various joints, in particular the great toe. The condition, resulting from poor handling of uric acid by the body, affects the entire body but manifests chiefly in joints.
Back pain Pain coming from the spine, muscles, nerves or other structures in the back. It mostly arises as a direct result of disease or injury involving spinal tissues. However, the pain arising from disease or injury of tissues and organs outside the spine can also be perceived as coming from the back (referred pain).
Osteoporosis A condition where the bone density thins and weakens, resulting in an increased risk of fracture—sometimes described as ‘porous bones’. Osteoporotic fractures are common among the elderly, with the spine, hip and wrist being common sites.

WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
4
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
Symptoms and complications
Akeysymptominmusculoskeletalconditionsispain(acuteorchronic).Acutepainlastsafewsecondsorlongerbutwanesashealingoccurs.Chronicpain,ontheotherhand,suchasthatseeninpeoplewitharthritisandbackpain,rangesfrommildtosevere,andcanlastweeks,months,years,oralifetime.Thepainmayoriginatefromdifferentsources,suchasinflammationofthetissuethatlinesthejoints,thetendonsandtheligaments,musclestrainandfatigue.Acombinationofthesefactorsmaycontributetotheintensityofthepain.Anothercommonpresentationofmusculoskeletalconditionsisstiffness,occurringmorecommonlywithrheumatoidarthritis.
Musculoskeletalconditionscanaffectvariousorgansofthebodyandcanleadtoavarietyofnon-musculoskeletalcomplications.Poorhealthoutcomes,suchasosteoporoticfractures,deformitiesandinabilitytomovearound,canaddtothephysicallimitations.
Age of onset
Theageofonsetofmusculoskeletalconditionsrangesfromchildhoodtooldage,dependingonthespecificcondition.Whiletheonsetofjuvenilearthritisisbydefinitionlimitedtopersonsyoungerthan16years,osteoarthritisandosteoporosismostlybegininolderadults.Rheumatoidarthritisontheotherhandtendstodevelopusuallyaroundages25to45years,whilemostcasesofosteoporosiscommenceatages45yearsandover.
Prevalence
Over38%(6.1million)Australiansaged16–85yearshaveamusculoskeletalcondition.Prevalenceisloweratyoungeragesandincreasessteadilyinolderages.Overallprevalenceishigheramongfemalesthanmalesineachagegroup(Figure1).
Source: AIHW analysis of ABS 2007 Survey of Mental Health and Wellbeing CURF.
Figure 1: Prevalence of musculoskeletal conditions, by age and sex, 2007
0
10
20
30
40
50
60
70
80
16–24 25–34 35–44 45–54 55–64 65–74 75–85
Per cent
Age group (years)
Males
Females

WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
Bulletin 80 • September 2010
5
Differentgroupsofmusculoskeletalconditionshavequitedifferentagedistributions,reflectingdifferencesintheirageofonset,variationinincidenceandtheirrelativelylowdeathrates.Whilebackpainanddiscdisordersarecommonamongyoungadultsandcontinuetoremainprominentthroughmid-life,osteoarthritisisthemajormusculoskeletalconditionintheolderagegroups.Osteoporosisismostprominentinages55yearsandover.
Inviewoftheirdifferingagedistributionsandprevalence,aswellasavailabledata,musculoskeletalconditionsarebroadlygroupedintotwocategoriesforthisreport,asfollows:
• arthritis,rheumatismandgout
• backandneckproblems.
The nature of mental disorders
Mentaldisordersaffecttheperceptions,emotions,behavioursandresultingwellbeingofindividuals.Thereareseveraltypesofmentaldisorderswithvaryingdegreesofseverity.Useoftheterm‘mentaldisorder’impliestheexistenceofaclinicallyrecognisablesetofsymptomsorbehaviours,associatedinmostcaseswithdistressandinterferencewithpersonalfunctions(WHO1992).Mentaldisordersoftenrequiretreatment,includinghospitalisation,toalleviatethesymptomsandforrehabilitation(AIHW1998).
Major types of mental disorders
SomeofthemajortypesofmentaldisordersinAustraliaareanxietydisorders,depression,schizophreniaandsubstance-usedisorders.ThesearedescribedinBox2.Themorecommontypesofmentaldisorders,namelyanxiety,affectiveandsubstance-usedisorders,wereincludedinthe2007AustralianBureauofStatistics(ABS)NationalSurveyofMentalHealthandWellbeingandarethuscoveredinthisreport.
Box 2: Major types of mental disordersAnxiety disorders, characterised by symptoms of anxiety, fear and avoidance behaviour, include panic disorders, phobias, obsessive–compulsive disorder and post-traumatic stress disorder. Anxiety disorders have a lifetime adult prevalence rate of more than 26% in Australia (ABS 2008).Depression is a mood disorder characterised by feelings of sadness, loss of interest or pleasure in nearly all activities, feelings of hopelessness and suicidal thoughts or self-blame. It is one of the most common mental disorders in the community. Depression, along with dysthymia (a mild form of depression) and bipolar affective disorder, collectively referred to as affective disorders, have a lifetime adult prevalence rate of 15% in Australia (ABS 2008). Substance-use disorders result from harmful use or dependence on drugs and/or alcohol. Their lifetime prevalence rate in Australian adults is around 25% (ABS 2008).Schizophrenia is a group of severe psychiatric disorders that are characterised by major disturbances in thought, emotion and behaviour. The symptoms may include delusions, hallucinations, and disorganised thoughts and behaviours. Schizophrenia usually starts in late adolescence or early adult life, and occurs in less than 1% of the adult population.

WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
6
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
Age of onset
Manymentaldisordersbegininchildhoodoradolescence,withapproximatelyhalfofallmentaldisordersstartinginmid-teensandthree-quartersbythemid-20s(Kessleretal.2007;Scottetal.2008).Certainanxietyandaffectivedisordershavetheearliestageofonset.Themedianageofonsetofsomeanxietydisordersis7–11years;foraffectivedisordersitisabitlaterinadulthood.Substance-usedisordersoftenstartinearlyadulthood(18–29years).
Earlyageofonsetofmentaldisordersisoftenassociatedwithgreaterseverity,persistenceandlackoftreatmentresponse(Kessler&Wang2008).
Prevalence
Twentypercent(3.2million)ofAustraliansaged16–85yearshavementaldisorders,withtheirprevalencehigheramongfemalesthanmalesateachagegroup(Figure2).Unliketheagedistributionobservedformusculoskeletalconditions,whereprevalenceincreaseswithage,theprevalenceofmentaldisordersdecreaseswithage.Thepatternandsymptomsofmentaldisordersdifferbetweenthesexes.Whileanxietydisordersandaffectivedisorders,includingdepression,aremorecommoninfemales,substance-usedisordersoccurmorecommonlyamongmales(Klose&Jacobi2004).
Source: AIHW analysis of ABS 2007 Survey of Mental Health and Wellbeing CURF.
Figure 2: Prevalence of mental disorders, by age and sex, 2007
0
10
20
30
40
16–24 25–34 35–44 45–54 55–64 65–74 75–85
Per cent
Age group (years)
Males
Females
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
Bulletin 80 • September 2010
7
Comorbidity—its causes and consequences
What is comorbidity?
Comorbidityoccurswhenapersonhastwoormorehealthconditionsatthesametime.Inthisreport,comorbidityreferstothepresenceofanymusculoskeletalconditionwithoneormorementaldisorders.
Causes of comorbidity
Thesimultaneousoccurrenceofheathconditionscanhappenbychancealone.Someconditionscancoexistinonepersonbycoincidence,withoutanycausalrelationshipbetweenthem.However,oftenhealthconditionsoccurtogetherbecauseofsomedirectorindirectcausalrelationshipsbetweenthem.
Thereisagrowingrecognitionthatfunctionallimitationsandchronicpainassociatedwithmusculoskeletalconditionspredisposepeopletoavarietyofmentalhealthproblems.Long-termfunctionallimitationsandactivityrestrictionsmaycontributetoanxiety,depressionandfeelingsofhelplessness.Chronicpaincanfurtheraddtoirritability,insomniaandexhaustion,oftenaccompaniedbywithdrawalfromworkandsocialactivities.Thesefactorstogethermayalsoleadtosubstanceabuseandothersocio-behaviouralproblems.
Whilethefunctionallimitationsandpainaspectsofmusculoskeletalconditionscouldbeasignificantcontributoryfactorinthedevelopmentorexacerbationofmentalproblems,thereisgrowingevidencethatmentaldisorderscanalsohaveadeleteriouseffectonphysicalillness,painanddisability(Moussavietal.2007).Thepathwaysareproposedtobethroughtheimmune,endocrineandnervoussystems,alongwithbehaviouralriskfactors,suchaspoordiet,lackofphysicalactivityandsubstanceuse.
The evidence so far
Mostoftheclinicalandcommunitystudiesthathaveshowncrediblerelationshipsbetweenmusculoskeletalconditionsandmentaldisordershavebeenbetweenspecificconditionsanddisorders,suchasarthritisanddepression.Arthritis,inparticularrheumatoidarthritis,hasbeenreportedtobeassociatedwithmoodandanxietydisorders(Dickensetal.2002;Krishnanetal.2002;Sareenetal.2006).Studiesofchronicbackorneckpainhavealsobeenshowntobeassociatedwithdepression(Carrolletal.2004;Currie&Wang2004).Mostofthereportedassociationsarestrongerinparticularagesegments,suchasyoungpeopleorolderpersons(Keefeetal.2002;LeBovidgeetal.2003),andnotacrossthefullagespectrum.Limitedornoassociationhasbeennotedbetweenarthritisandsubstance-usedisorders(Brownetal.1996;Heetal.2008;Shihetal.2006).
Nobroad-levelpopulation-basedstudiesofcomorbiditybetweenthemusculoskeletalconditionsandmentaldisordershavepreviouslybeenreportedinAustralia.Thispossiblyreflectsconcernthatanystudyofassociationatthislevelofassessmentwouldhavelimited

WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
8
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
publichealthrelevancebecauseofthelimitedoverlapbetweentheagesofonsetofthetwosetsofconditionsandtheirverydifferentlifecourses.Whilemostofthementalhealthproblemsanddisordersariseearlyinlifebuthavelowprevalenceinolderagegroups,thebulkofmusculoskeletalconditionsarisesandpersistsinolderagegroups.Thismakescomorbiditydifficulttoquantifythroughcommunity-basedpopulationsurveysalone.
This report
ThereportexaminesthecurrentextentofcomorbidityinAustraliabetweenmusculoskeletalconditionsandmentaldisorders.Estimatesarepresentedbyagegroup,andformalesandfemalesseparately.Theobservedprevalenceratesofcomorbidityarecomparedwiththosethatmightbeexpectedtooccurpurelybychancealone.
TheestimatesinthisreportarederivedfromtheConfidentialisedUnitRecordFile(CURF)oftheNationalSurveyofMentalHealthandWellbeingconductedbytheABSfromAugusttoDecember2007.Thesurveycollectedinformationfromapproximately8,800Australiansaged16–85years.
Unlessotherwisestated,theprevalenceofpeoplewithmusculoskeletalconditionsrelatestothosewithalong-termconditionatthetimeofthesurvey,andprevalenceofpeoplewithmentaldisordersrelatestothe12-monthperiodpriortotheinterview.
Prevalence of comorbidity
During2007,over1.5millionpeople(10%ofthepopulationaged16–85years)hadatleastonemusculoskeletalconditionlongtermandatleastonementaldisorderintheprevious12months(Figure3andTableA1).Thenumberoffemalesexperiencingthiscomorbidity(862,000)wasgreaterthanthenumberofmales(671,000).
Note: The estimates are for people aged 16–85 years.Source: AIHW analysis of ABS 2007 Survey of Mental Health and Wellbeing CURF.
Figure 3: People with musculoskeletal conditions, mental disorders and their comorbidity, by sex, 2007
0
2,000
4,000
6,000
8,000
10,000
2,114
671 731
Males
2,497
862
934
Females
4,610
1,534
1,664
Persons
Number (’000)
Mental disorders without musculoskeletal conditions
Comorbidity
Musculoskeletal conditions without mental disorders

WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
Bulletin 80 • September 2010
9
Theage-specificprevalencerateofcomorbidityincreasedsharplyineachsuccessiveagegroupuntil45–54years,afterwhichitdecreasedsharply.Ratesweregenerallyhigherinfemalesthaninmalesbutthepatternsovertheentireagerangeweresimilar(Figure4).
Source: AIHW analysis of ABS 2007 Survey of Mental Health and Wellbeing CURF.
Figure 4: Age-specific prevalence rates of comorbidity between musculoskeletal conditions and mental disorders, by sex, 2007
ThereasonforthispatternisshowninFigure5.Theprevalenceofmusculoskeletalconditionsislowerintheyoungeragegroupsandgreaterintheolderagegroups,whilethereverseistrueformentaldisorders.Theprevalenceofcomorbidityreflectstheincreasingprevalenceofmusculoskeletalconditionsinyoungeragegroupsandthedecreasing(andlower)prevalenceofmentaldisordersinolderagegroups.
Source: AIHW analysis of ABS 2007 Survey of Mental Health and Wellbeing CURF.
Figure 5: Age-specific prevalence rates of musculoskeletal conditions, mental disorders and their comorbidity, 2007
0
2
4
6
8
10
12
14
16
18
16–24 25–34 35–44 45–54 55–64 65–74 75–85
Per cent
Age group (years)
Persons Males Females
16–24 25–34 35–44 45–54 55–64 65–74 75–85
Per cent
Age Age group (years)
0
10
20
30
40
50
60
70 Musculoskeletal conditions (includes comorbidity) Mental disorders (includes comorbidity) Observed comorbidity Expected comorbidity

WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
10
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
Observed and expected prevalence of comorbidity
Musculoskeletalconditionsandmentaldisordersmayoccurtogetherbychance.Undertheassumptionthattheoccurrenceofmusculoskeletalconditionsandmentaldisordersareindependent,theexpectedcomorbidityrateisestimatedbymultiplyingthetwoobservedprevalenceratestogether.Forexample,inTable1,theobservedprevalenceratesformusculoskeletalconditionsandmentaldisordersforages16–24yearsare12.4%and26.4%respectively.Multiplyingthesetogethergivesanexpectedcomorbidityrateof3.3%.Thiscompareswithanobservedrateof6.1%,adifferenceof2.8%,whichisequivalentto72,000people(2.8%of2,545,000,seeTableA1).Thedifferencebetweentheobservedandexpectednumbersofpeoplewithbothmusculoskeletalconditionsandmentaldisordersislabelled‘excesscomorbidity’inTable1.Thiscalculationwasperformedforeachagegroupandsummedacrosstheagegroups.
In2007,theobservedcomorbiditybetweenmusculoskeletalconditionsandmentaldisorderswasgreaterthanthatexpectedateachagegroupandtotalled470,000peopleoverall(Table1).Thehigherthanexpectedcomorbiditysuggestsanassociationbetweenthetwoconditions.
Table 1: Observed and expected comorbidity, musculoskeletal conditions and mental disorders
Age groupMusculoskeletal
conditionsMental
disordersObserved
comorbidityExpected
comorbidityExcess
comorbidity
Rate (per cent) Number
16–24 12.4 26.4 6.1 3.3 72,000
25–34 22.2 24.8 8.5 5.5 85,000
35–44 34.1 23.3 11.8 8.0 117,000
45–54 47.3 21.5 14.3 10.2 119,000
55–64 55.4 13.6 9.7 7.6 49,000
65–74 62.5 8.6 6.4 5.4 15,000
75–85 64.1 5.9 5.2 3.8 13,000
Total 38.4 20.0 9.6 7.7 470,000
Note: See Table A1 for population numbers. Excess comorbidity is estimated as the observed comorbidity rate x population – expected comorbidity rate x population for each age group. The total is the sum of the age-specific estimates.
Source: AIHW analysis of ABS 2007 Survey of Mental Health and Wellbeing CURF.
Comorbidity among people with musculoskeletal conditions
Figure6showsthenumberofpeoplewithmusculoskeletalconditions,partitionedintothosewithmentaldisordersandthosewithout.Atages16–24years,almostone-half(49%)ofpeoplewithamusculoskeletalconditionalsohadamentaldisorder.Thisproportiondecreasedto8%intheoldestagegroup.Overall,25%ofpeoplewithamusculoskeletalconditionhadamentaldisorder.

WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
Bulletin 80 • September 2010
11
Source: AIHW analysis of ABS 2007 Survey of Mental Health and Wellbeing CURF.
Figure 6: Presence of mental disorders in people with musculoskeletal conditions, 2007
Comorbidity among people with mental disorders
Figure7showsthenumberofpeoplewithmentaldisorders,partitionedintothosewithmusculoskeletalconditionsandthosewithoutthem.Atages16–24years,aboutaquarter(23%)ofpeoplewithamentaldisorderhadamusculoskeletalcondition.Thisproportionincreasedto87%intheoldestagegroup.Overall,48%ofpeoplewithamentaldisorderhadamusculoskeletalcondition.
Source: AIHW analysis of ABS 2007 Survey of Mental Health and Wellbeing CURF.
Figure 7: Presence of musculoskeletal conditions in people with mental disorders, 2007
16–24 25–34 35–44 45–54 55–64 65–74 75–85 Age group (years)
0
200
400
600
800
1,000
1,200
1,400
1,600
Number (’000)
Musculoskeletal conditions without mental disorders
Musculoskeletal conditions with mental disorders
16–24 25–34 35–44 45–54 55–64 65–74 75–85 Age group (years)
Mental disorders without musculoskeletal conditions
Mental disorders with musculoskeletal conditions
0
200
400
600
800
Number (’000)
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
12
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
Types of mental disorders in people with musculoskeletal conditions
Thissectionexaminestheprevalenceofsomebroadtypesofmentaldisordersinpeoplewithbroadgroupsofmusculoskeletalconditionsandidentifieswhichcombinationsofmusculoskeletalconditionsandmentaldisordersaremostcommon.Itonlyincludespeoplewhohavebothamusculoskeletalconditionandamentaldisorder.Musculoskeletalconditionsaretakenasthereferencepopulationbecausethecausalpathwaysaremorelikelytobefrommusculoskeletalconditionstomentaldisordersthantheotherwayaround.
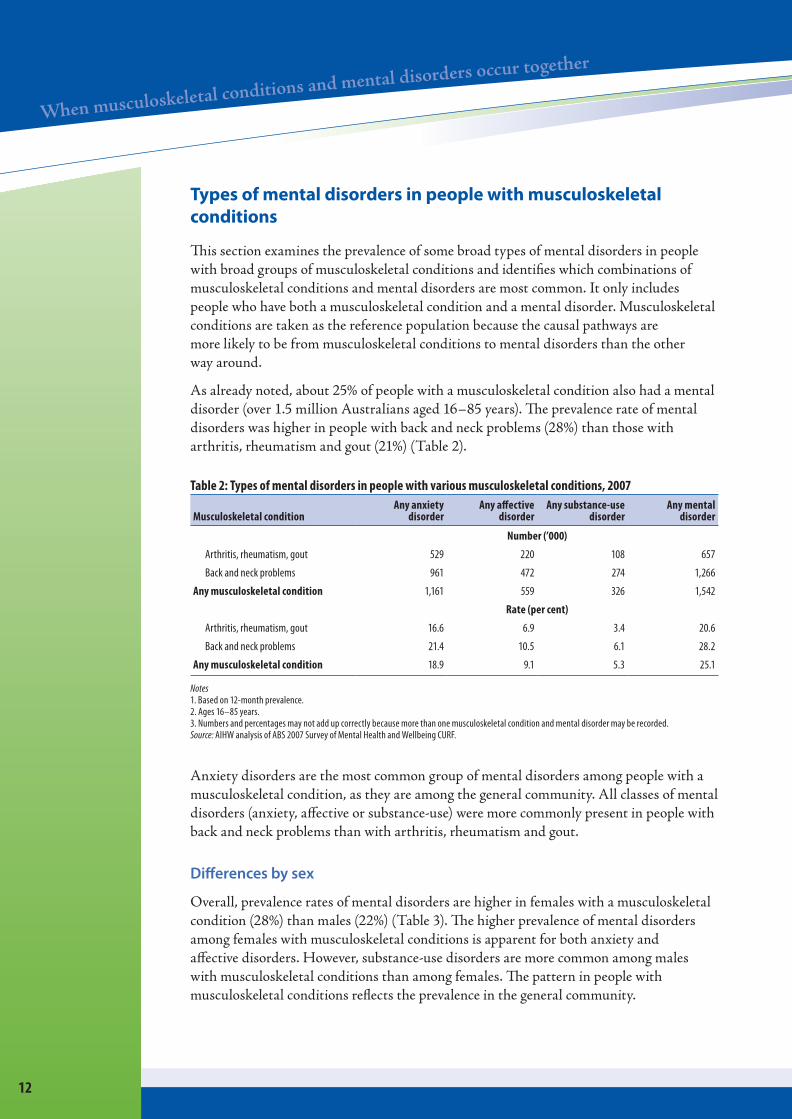
Asalreadynoted,about25%ofpeoplewithamusculoskeletalconditionalsohadamentaldisorder(over1.5millionAustraliansaged16–85years).Theprevalencerateofmentaldisorderswashigherinpeoplewithbackandneckproblems(28%)thanthosewitharthritis,rheumatismandgout(21%)(Table2).
Table 2: Types of mental disorders in people with various musculoskeletal conditions, 2007
Musculoskeletal conditionAny anxiety
disorderAny affective
disorderAny substance-use
disorderAny mental
disorder
Number (’000)
Arthritis, rheumatism, gout 529 220 108 657
Back and neck problems 961 472 274 1,266
Any musculoskeletal condition 1,161 559 326 1,542
Rate (per cent)
Arthritis, rheumatism, gout 16.6 6.9 3.4 20.6
Back and neck problems 21.4 10.5 6.1 28.2
Any musculoskeletal condition 18.9 9.1 5.3 25.1
Notes 1. Based on 12-month prevalence. 2. Ages 16–85 years. 3. Numbers and percentages may not add up correctly because more than one musculoskeletal condition and mental disorder may be recorded. Source: AIHW analysis of ABS 2007 Survey of Mental Health and Wellbeing CURF.
Anxietydisordersarethemostcommongroupofmentaldisordersamongpeoplewithamusculoskeletalcondition,astheyareamongthegeneralcommunity.Allclassesofmentaldisorders(anxiety,affectiveorsubstance-use)weremorecommonlypresentinpeoplewithbackandneckproblemsthanwitharthritis,rheumatismandgout.
Differences by sex
Overall,prevalenceratesofmentaldisordersarehigherinfemaleswithamusculoskeletalcondition(28%)thanmales(22%)(Table3).Thehigherprevalenceofmentaldisordersamongfemaleswithmusculoskeletalconditionsisapparentforbothanxietyandaffectivedisorders.However,substance-usedisordersaremorecommonamongmaleswithmusculoskeletalconditionsthanamongfemales.Thepatterninpeoplewithmusculoskeletalconditionsreflectstheprevalenceinthegeneralcommunity.
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
Bulletin 80 • September 2010
13
Table 3: Types of mental disorders in people with musculoskeletal conditions, by sex, 2007
SexAny anxiety
disorderAny affective
disorderAny substance-use
disorderAny mental
disorder
Number (’000)
Males 469 222 201 671
Females 697 334 128 862
Persons 1,165 556 323 1,534
Rate (per cent)
Males 16.8 7.9 7.2 21.9
Females 20.8 9.9 3.6 28.2
Persons 18.9 9.1 5.3 25.1
Notes 1. Based on 12-month prevalence. 2. Ages 16–85 years. 3. Numbers and percentages may not add up correctly because more than one musculoskeletal condition and mental disorder may be recorded. Source: AIHW analysis of ABS 2007 Survey of Mental Health and Wellbeing CURF.
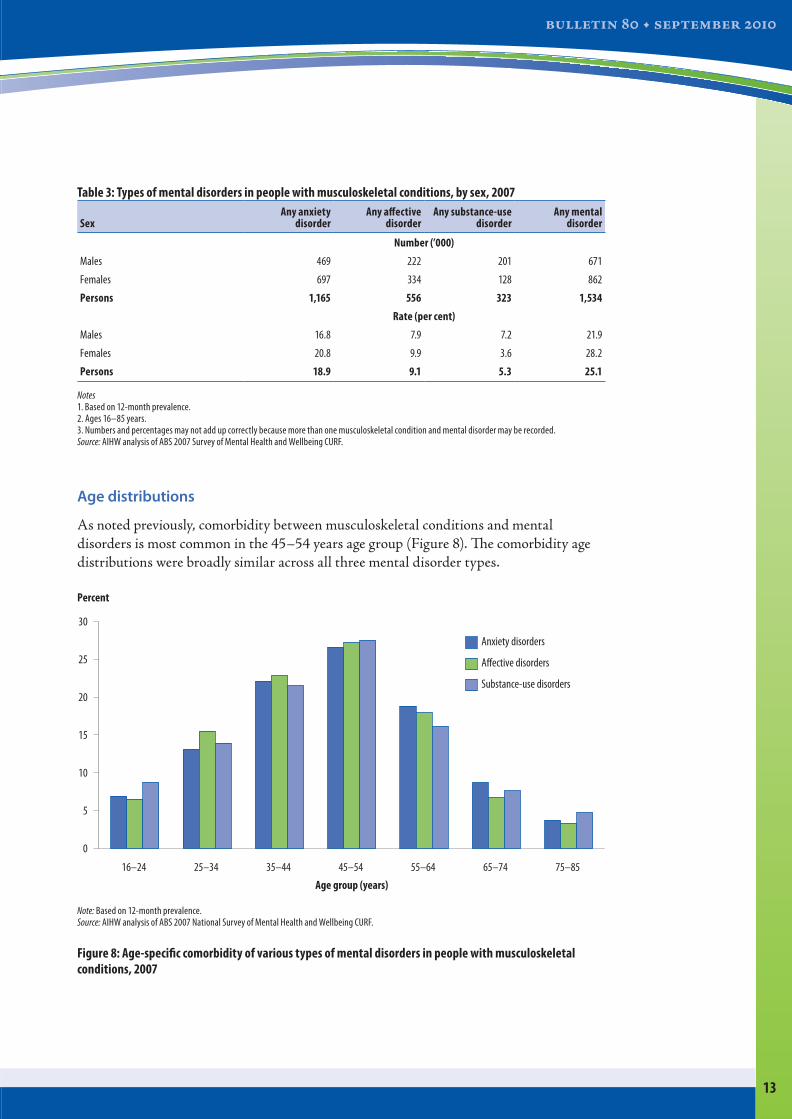
Age distributions
Asnotedpreviously,comorbiditybetweenmusculoskeletalconditionsandmentaldisordersismostcommoninthe45–54yearsagegroup(Figure8).Thecomorbidityagedistributionswerebroadlysimilaracrossallthreementaldisordertypes.
Note: Based on 12-month prevalence.Source: AIHW analysis of ABS 2007 National Survey of Mental Health and Wellbeing CURF.
Figure 8: Age-specific comorbidity of various types of mental disorders in people with musculoskeletal conditions, 2007
16–24 25–34 35–44 45–54 55–64 65–74 75–85
Age group (years)
0
5
10
15
20
25
30
Percent
Anxiety disorders
A�ective disorders
Substance-use disorders

WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
14
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
Conclusion
Thisstudyshowsthereissignificantcomorbiditybetweenmusculoskeletalconditionsandmentalhealthproblems.One-quarterofadultsaged16–85yearswithamusculoskeletalconditionalsohadamentaldisorder.Fromtheotherperspective,nearlyhalfofallpeopleinthatagegroupwithamentalhealthdisorderalsohadamusculoskeletalcondition.Thisresultsin1.5millionpeople(10%ofthoseaged16–85years)havingatleastonemusculoskeletalconditionandonementalhealthdisorder.
Thisalsosuggeststheexistenceofanunderlyingrelationshipbetweenthetwoconditions,withtheobservedcomorbiditybeinghigherthanexpected.Whilethecausaldirectionsarenotfullyunderstood,theirhighcomorbidityindicatestheneedforhealth-careproviderstobeawareofthecomplextreatmentandmanagementrequirementsofpeoplewithlong-termmusculoskeletalconditions.
Acknowledgments
ThisreportwaspreparedbyNailaRahman,KuldeepBhatiaandStanBennett.
TheNationalCentreforMonitoringArthritisandMusculoskeletalConditionsattheAustralianInstituteofHealthandWelfare(AIHW)acknowledgestheinputofLyleBaker,MarkCooper-Stanbury,LynelleMoonandvariousmembersoftheArthritisDataWorkingGroup/SteeringCommitteeinthepreparationofthisreport.
TheAustralianGovernmentDepartmentofHealthandAgeingfundedthepreparationandpublicationofthisreport.

WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
Bulletin 80 • September 2010
15
ReferencesABS(AustralianBureauofStatistics)2008.NationalSurveyofMentalHealthandWellbeing:
summaryofresults.ABScat.no.4326.0.Canberra:ABS.AIHW(AustralianInstituteofHealthandWelfare)1998.Australia’shealth1998:thesixth
biennialhealthreportoftheAustralianInstituteofHealthandWelfare.Canberra:AIHW.AIHW2008.ArthritisandosteoporosisinAustralia2008.Arthritisseriesno.8.
Cat.no.PHE106.Canberra:AIHW.AIHW2010.Australia’shealth2010.Australia’shealthseriesno.12.Cat.no.AUS122.
Canberra:AIHW.BrownRL,PattersonJJ,RoundsLA&PapasouliotisO1996.Substanceabuseamongpatients
withchronicbackpain.JournalofFamilyPractice43:152–160.CarrollLJ,CassidyJD&CoteP2004.Depressionasariskfactorforonsetofanepisodeof
troublesomeneckandlowbackpain.Pain107:134-139.CurrieSR&WangJ2004.ChronicbackpainandmajordepressioninthegeneralCanadian
population.Pain107:54–60.DickensC,McGowenL,Clark-CarterD&CreedF2002.Depressioninrheumatoidarthritis:a
systematicreviewoftheliteraturewithmeta-analysis.PsychosomaticMedicine64:52–60.HeY,ZhangM,LinEH,BruffaertsR,Posada-VillaJ,AngermeyerMCetal.2008.Mental
disordersamongpersonswitharthritis:resultsfromtheWorldMentalHealthSurveys.PsychologicalMedicine38(11):1639–1650.
KeefeFJ,SmithSJ,BuffingtonALH,GibsonJ,StudtsJL&CaldwellDS2002.Recentadvancesandfuturedirectionsinthebiopsychosocialassessmentandtreatmentofarthritis.JournalofConsultingandClinicalPsychology70:640–655.
KesslerRC,AngermeyerM,AnthonyJC,GraafRD,DemyttenaereK&GasquetI2007.Lifetimeprevalenceandage-of-onsetdistributionsofmentaldisordersintheWorldHealthOrganisation’sWorldMentalHealthSurveyInitiative.WorldPsychiatry6(3):168–176.
KesslerRC&WangPS2008.ThedescriptiveepidemiologyofcommonlyoccurringmentaldisordersintheUnitedStates.AnnualReviewofPublicHealth29:115-129.
KloseM&JacobiF2004.Cangenderdifferencesintheprevalenceofmentaldisordersbeexplainedbysociodemographicfactors?ArchivesofWomen’sMentalHealth7(2):133–148.
KrishnanKRR,DelongM,KraemerH,CarneyR,SpiegelD&GordonC2002.Comorbidityofdepressionwithothermedicaldiseasesintheelderly.BiologicalPsychiatry52:559–588.
LeBovidgeJS,LavigneJV,DonenbergGR,MillerML2003.Psychologicaladjustmentofchildrenandadolescentswithchronicarthritis:ameta-analyticreview.JournalofPaediatricPsychology28:29–39.
MoussaviS,ChatterjiS,VerdesE,TandonA,PatelV&UstunB2007.Depression,chronicdiseasesanddecrementsinhealth:resultsfromtheWorldHealthSurveys.Lancet370:851–858.
SareenJ,JacobiF&CoxBJ2006.Disabilityandpoorqualityoflifeassociatedwithcomorbidanxietydisordersandphysicalconditions.ArchivesofInternalMedicine166:2109–2116.
ScottKM,VonKorffM,AlonsoJ,AngermeyerM,BrometEJ&BruffaertsR2008.AgepatternsintheprevalenceofDSM-IVdepressive/anxietydisorderswithandwithoutphysicalco-morbidity.PsychologicalMedicine38(11):1659–1669.
ShihM,HootmanJM,StrineTW,ChapmanDP&BradyTJ2006.SeriouspsychologicaldistressinU.S.adultswitharthritis.JournalofGeneralInternalMedicine21(11):1160–1166.
WHO(WorldHealthOrganization)1992.TheICD-10classificationofmentalandbehaviouraldisorders:clinicaldescriptionsanddiagnosticguidelines.Geneva:WHO.

WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
16
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
Appendix: Statistical table and methods
Table A1: People with musculoskeletal conditions, mental disorders and their comorbidity by age and sex, 2007
Age group
Population Musculoskeletal conditions Mental disorders Comorbidity
Number (’000)
Number (’000)
Rate (per cent)
Number (’000)
Rate (per cent)
Number (’000)
Rate (per cent)
Persons
16–24 2,545 315.9 12.4 671.1 26.4 155.6 6.1
25–34 2,812 622.9 22.2 698.4 24.8 239.5 8.5
35–44 3,070 1,046.2 34.1 716.4 23.3 361.4 11.8
45–54 2,859 1,352.5 47.3 613.7 21.5 409.5 14.3
55–64 2,324 1,287.8 55.4 316.7 13.6 225.0 9.7
65–74 1,434 896.1 62.5 123.8 8.6 92.4 6.4
75–85 971 622.6 64.1 57.7 5.9 50.3 5.2
16–85 16,015 6,143.9 38.4 3,197.8 20.0 1,533.7 9.6
Males
16–24 1,299 122.9 9.5 296.3 22.8 59.2 4.6
25–34 1,414 272.3 19.3 322.5 22.8 105.6 7.5
35–44 1,534 512.4 33.4 319.0 20.8 180.1 11.7
45–54 1,405 617.8 44.0 262.1 18.6 184.5 13.1
55–64 1,159 588.2 50.8 126.5 10.9 86.9 7.5
65–74 699 403.2 57.7 53.8 7.7 36.6 5.2
75–85 440 268.2 60.8 21.9 5.0 18.5 4.2
Total 7,952 2,784.9 35.0 1,402.1 17.6 671.4 8.4
Females
16–24 1,246 193.0 15.5 374.8 30.1 96.4 7.7
25–34 1,398 350.6 25.1 375.8 26.9 133.9 9.6
35–44 1,536 533.8 34.8 397.5 25.9 181.3 11.8
45–54 1,453 734.7 50.6 351.6 24.2 225.0 15.5
55–64 1,165 699.6 60.1 190.2 16.3 138.1 11.9
65–74 735 492.9 67.1 70.0 9.5 55.8 7.6
75–85 530 354.4 66.8 35.8 6.8 31.7 6.0
Total 8,064 3,359.0 41.7 1,795.8 22.3 862.3 10.7
NotesMusculoskeletal conditions and mental disorders include comorbidity.Comorbidity in the occurrence of musculoskeletal conditions and mental disorders together in one person. Rate is the number as a percentage of the corresponding population.
Source: AIHW analysis of ABS 2007 National Survey of Mental Health and Wellbeing CURF.
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
Bulletin 80 • September 2010
17
Definitions and methods
Prevalence
Prevalencereferstothenumberorproportion(ofcases,instances,etc.)presentinapopulationatagiventime.Prevalencedataprovideanindicationoftheextentofthepresenceofaconditionandmayhaveimplicationsfortheprovisionofservicesinacommunity.Theformulaforcalculatingprevalenceis:
Mostoftheinformationavailableontheprevalenceofarthritisandmusculoskeletalconditionsisbasedupontheexistenceoftheseconditionslongterm,thatistheconditionshavebeenpresentorarelikelytobepresentfor6monthsormore.Acute,one-offcases,lastinglessthan6months,areexcludedfromthecount.
Age-specific rates
Age-specificratesarecalculatedbydividingthenumberofcasesoccurringineachspecifiedagegroupbytheestimatedresidentpopulationforthatagegroup.Inthispublication,theratesareexpressedascasesper100population(that is,asapercentage).
Excess comorbidity
Excesscomorbidityisestimatedasthedifferencebetweentheobservedcomorbidityandtheexpectedcomorbidity,thatis:
Excess comorbidity = observed comorbidity – expected comorbidity.
Theobservedcomorbidityisthenumberofpeoplewhohadatleastonemusculoskeletalconditionandatleastonementaldisorder.
Theexpectedcomorbidityistheestimatednumberofpeoplewhomightbeexpectedtohavehadatleastonemusculoskeletalconditionsandonementaldisorder.Assumingthattheoccurrenceofmusculoskeletalconditionsandmentaldisordersareindependent,theexpectedcomorbidityistheproductofthetwoobservedprevalenceratestimesthepopulationnumber.
Note:Thismethodproducesaconservative(underestimate)of‘excess’comorbidity.
Prevalence =
* during speci�ed time period
Number of existing cases*
Population at risk*

WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW
18
Worked example
Forexample,usingTableA1:
Forpersonsaged16–24yearstheobservedcomorbidityis155,600(arateof6.1%).
Theobservedprevalenceratesare12.4%formusculoskeletalconditionsand26.4%formentaldisorders.Theirproductis3.3%whichistheexpectedcomorbidityrate.Thecomorbidity(number)is3.3%×2,545,000=83,300.
Excesscomorbidity=155,600–83,300=72,000(tothenearestthousand).

WWWW WWWWWWWWWWWWWWW WWWWWWWWWW WWW WWWWWW WWWWWWWWW WWWWW WWWWWWWW

© Australian Institute of Health and Welfare 2010
This work is copyright. Apart from any use as permitted under the Copyright Act 1968, no part may be reproduced without prior written permission from the Australian Institute of Health and Welfare. Requests and enquiries concerning reproduction and rights should be directed to the Head, Communications, Media and Marketing Unit, Australian Institute of Health and Welfare, GPO Box 570, Canberra ACT 2601.
This publication is part of the Australian Institute of Health and Welfare’s Bulletin series. A complete list of the Institute’s publications is available from the Institute’s website <www.aihw.gov.au>.
ISSN 1446-9820 ISBN 978-1-74249-063-2
AIHW bulletin no. 80
Suggested citation
Australian Institute of Health and Welfare 2010. When musculoskeletal conditions and mental disorders occur together. Cat. no. AUS 129. Canberra: AIHW.
Australian Institute of Health and Welfare
Board Chair Hon. Peter Collins, AM, QC
Director Penny Allbon
Any enquiries about or comments on this publication should be directed to:
Dr Naila Rahman National Centre for Monitoring Arthritis and Musculoskeletal Conditions Australian Institute of Health and Welfare GPO Box 570 Canberra ACT 2601 Phone: (02) 6244 1057 Email: [email protected]
Published by the Australian Institute of Health and Welfare
Printed by PMP Limited