exercise and work-related musculoskeletal disorders in ... · pdf fileexercise and...
TRANSCRIPT

Exercise and work-related musculoskeletaldisorders in neck, shoulders and low back
Exercise and work-related musculoskeletal disorders in neck,Exercise and work-related musculoskeletal disorders in neck,Exercise and work-related musculoskeletal disorders in neck,Exercise and work-related musculoskeletal disorders in neck,Exercise and work-related musculoskeletal disorders in neck,shoulders and low backshoulders and low backshoulders and low backshoulders and low backshoulders and low back© Mogens Theisen Pedersen 2003Institute of Exercise and Sport Sciences, University of Copenhagen
PhD thesis
Submitted August 2003Defended November 2003
Opponents:Overlæge, dr.med. Fin Biering-Sørensen, Rigshospitalet, TH 2091 - ???
Associate professor A.J. van der Beek, Dept. of Social Medicine, Institute forResearch in extramural Medicin, VU University Medical Centre, Amsterdam.
Chairman, Professor Jens Bo Nielsen, Institute of Exercise and Sport Sciences,University of Copenhagen
Layout: Allis Skovbjerg JepsenPrinted By: A3 Tryk & Reklame, SilkeborgISBN: 87 89361 98 9

Mogens Theisen Pedersen
Exercise and work-related musculoskeletaldisorders in neck, shoulders and low back
PhD Thesis
National Institute of Occupational HealthDepartment of Physiology
Institute of Exercise and Sport SciencesFaculty of Science, University of Copenhagen, Denmark
2003
4
ANOVA analysis of varianceEMG electromyographyLBP low back painMVC maximal voluntary static contraction forceRFD rate of force developmentRCT randomised controlled studySL sudden back loadingWMSDs work related musculoskeletal disorders
List of Abbreviations
5
Content
List of List of List of List of List of AbbreviationsAbbreviationsAbbreviationsAbbreviationsAbbreviations ................................................................................................................................................................................................................................................................................................................................................................... 44444
ContentContentContentContentContent ........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................... 55555
PrefacePrefacePrefacePrefacePreface ................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................ 77777
AcknowledgementsAcknowledgementsAcknowledgementsAcknowledgementsAcknowledgements ....................................................................................................................................................................................................................................................................................................................................................................................... 88888
List of papersList of papersList of papersList of papersList of papers .................................................................................................................................................................................................................................................................................................................................................................................................................................... 99999
IntroductionIntroductionIntroductionIntroductionIntroduction ......................................................................................................................................................................................................................................................................................................................................................................................................................................... 1010101010Individual risk factors for upper neck, shoulder and back pain 13The „traditional“ view: Muscle strength and endurance 13
Neck and shoulder 13Low back 14
The „newcomer“: motor control aspects 14Modification of individual physical capacity as a preventive
measure: Results from intervention studies 16Shoulder and neck 16Low back 17
Aims and hypothesesAims and hypothesesAims and hypothesesAims and hypothesesAims and hypotheses ......................................................................................................................................................................................................................................................................................................................................................... 1818181818
Material and methodsMaterial and methodsMaterial and methodsMaterial and methodsMaterial and methods ............................................................................................................................................................................................................................................................................................................................................... 1919191919Overall design 19Material 21Training 22Sudden back loading (SL) 27Electromyography 28Neck-shoulder complaints 29Questionnaires about training and the effect of training 29Statistics 30

6
ResultsResultsResultsResultsResults ...................................................................................................................................................................................................................................................................................................................................................................................................................................................................................... 3232323232Training effect on muscular complaints 32Training effect on muscle strength, muscle endurance and
mechanical motor control variables 33Training effect on EMG in the motor control studies 34Participants perception of the training programs and
the effect of training 35Study I 35Study III 37Study IV 37
DiscussionDiscussionDiscussionDiscussionDiscussion ........................................................................................................................................................................................................................................................................................................................................................................................................................................................ 3838383838Effect of training on physical capacity 38Changes in musculoskeletal complaints; Intervention
study design 40Participants perception of the training programmes 41Implications of the effect of readiness training 42The effect of training – physiological changes 43
ConclusionsConclusionsConclusionsConclusionsConclusions .............................................................................................................................................................................................................................................................................................................................................................................................................................................. 4646464646
ReferencesReferencesReferencesReferencesReferences........................................................................................................................................................................................................................................................................................................................................................................................................................................................ 4848484848
SummarySummarySummarySummarySummary .................................................................................................................................................................................................................................................................................................................................................................................................................................................................. 5858585858
Dansk resuméDansk resuméDansk resuméDansk resuméDansk resumé .......................................................................................................................................................................................................................................................................................................................................................................................................................... 5959595959
7
Preface
This PhD- project is the result of co-operation between the Institute ofExercise and Sport Sciences (IESS), Copenhagen, and the National Instituteof Occupational Health (NIOH), Copenhagen (Department of Physiology).The first study (I) was also performed in collaboration with Clinic ofOccupational Medicine, Glostrup Hospital. Senior researcher PhD Nils Fallen-tin, NIOH, associate professor DSc Kurt Jørgensen, IESS, and associate pro-fessor DMSc PhD Lars Bo Andersen, IESS, provided mentorship.
Study I was financed by the Danish Working Environment Fund. The Instituteof Exercise and Sport Sciences and the National Institute of OccupationalHealth financed the other studies.
Study I was part of a large-scale prospective epidemiological study on workrelated musculoskeletal disorders (The PRIM study). Study II, III, and IVwere parts of a major research project concerning occupational risk factors oflow back disorders among health care workers.
The project has been approved by the ethical committee of Copenhagen andFrederiksberg, Denmark ((KF) 01-104/94 and (KF) 01-224/01).
Mogens Theisen PedersenCopenhagen, September 2003
8
I would like to thank my colleagues at the Department of Physiology at theNational Institute of Occupational Health and at The National Institute ofExercise and Sport Sciences, who have all been kind and supportive through-out the project.
In particular I would like to thank the following people• My supervisor Kurt Jørgensen for invaluable support and professional
advice during the preparations of the PhD-study and for support and pro-fessional advice throughout.
• My supervisor Nils Fallentin for having always been there when I neededhelp and for a lot of invaluable professional help and advice.
• My statistics supervisor Lars Bo Andersen for professional advice.• Bente Shibye for securing the implementation of the studies and for pro-
fessional advice.• Jørgen Skotte for invaluable technical support and computer programming.• Morten Essendrop for close co-operation, practical help, numerous discus-
sions, computer programming and for having always been helpful.• Gisela Sjøgaard for discussions and for involvement in the project.• Jesper Strøyer and Helene Garde for statistical help and discussions.• Gunilla Harrit at Vordingborg Hospital for positive co-operation.• Leaders, managers, participants and controls from Dansk Supermarked,
FDB and Vordingborg Hospital.
Acknowledgements
9
The present thesis is based on four studies represented by 4 papers. In thetext they will be referred to by their Roman numerals:
I: Pedersen MT, Mikkelsen S, and Fallentin N.The effect of muscle strength and endurance training on musculoskeletalcomplaints in the shoulder/neck region of cashier checkout workers. Interna-tional Ergonomics Association. XIVth Triennial Congress and Human Factors andErgonomics Society 44th Annual Meeting. Ergonomics for the New Millennium; 2000Jul 29- Aug 4; San Diego, California. Santa Monica (Proceeding).
II: Skotte JH, Fallentin N, Pedersen MT, Essendrop M, Strøyer J and SchibyeB.A new set-up for studying sudden loading of the low back. J Biomech (Sub-mitted).
III: Pedersen MT, Essendrop M, Skotte JH, Jørgensen K, Fallentin N.Training can modify back muscle response to sudden trunk loading. EuropeanSpine Journal (The paper is submitted, and accepted (March 15th) on the condit-ion of a minor revision including addressing comments of the reviewers. Thishas been done and send to the Editor (April 15th)).
IV: Pedersen MT, Essendrop M, Skotte JH, Jørgensen K, Fallentin N.Back muscle response to sudden trunk loading can be modified by trainingamong health care workers. Spine (Submitted).
List of papers
OBS!!!
10
Introduction
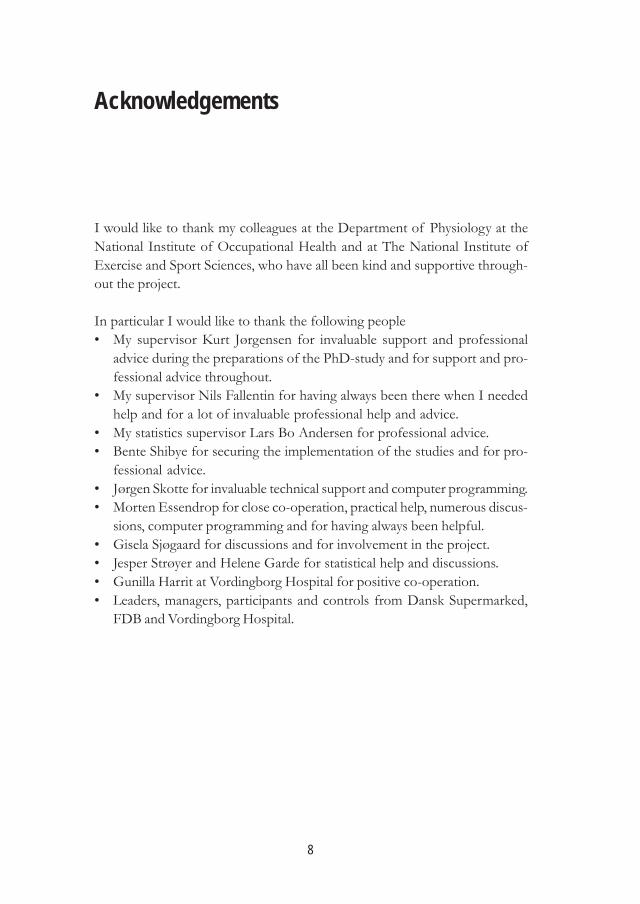
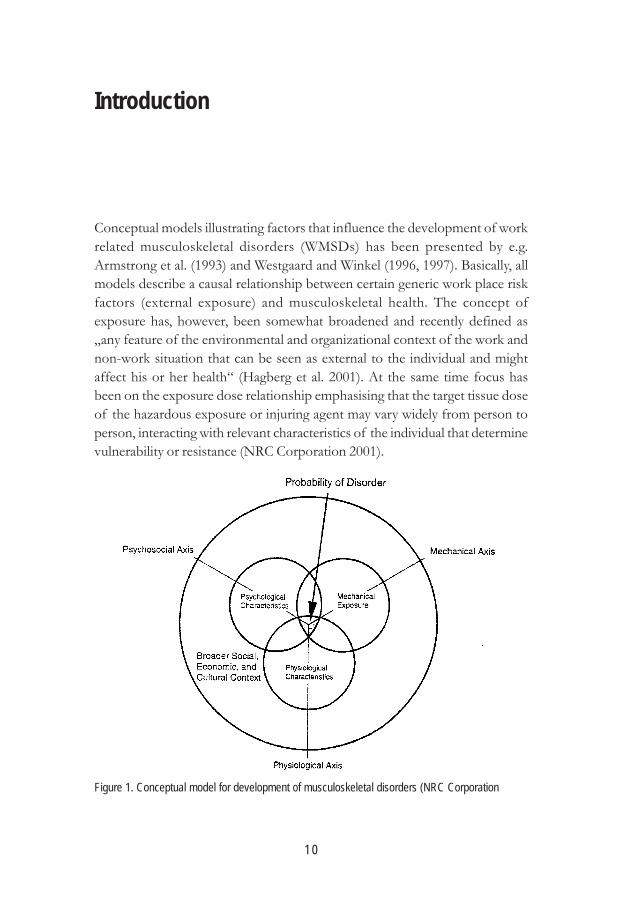
Conceptual models illustrating factors that influence the development of workrelated musculoskeletal disorders (WMSDs) has been presented by e.g.Armstrong et al. (1993) and Westgaard and Winkel (1996, 1997). Basically, allmodels describe a causal relationship between certain generic work place riskfactors (external exposure) and musculoskeletal health. The concept ofexposure has, however, been somewhat broadened and recently defined as„any feature of the environmental and organizational context of the work andnon-work situation that can be seen as external to the individual and mightaffect his or her health“ (Hagberg et al. 2001). At the same time focus hasbeen on the exposure dose relationship emphasising that the target tissue doseof the hazardous exposure or injuring agent may vary widely from person toperson, interacting with relevant characteristics of the individual that determinevulnerability or resistance (NRC Corporation 2001).
Figure 1. Conceptual model for development of musculoskeletal disorders (NRC Corporation
11
Introduction
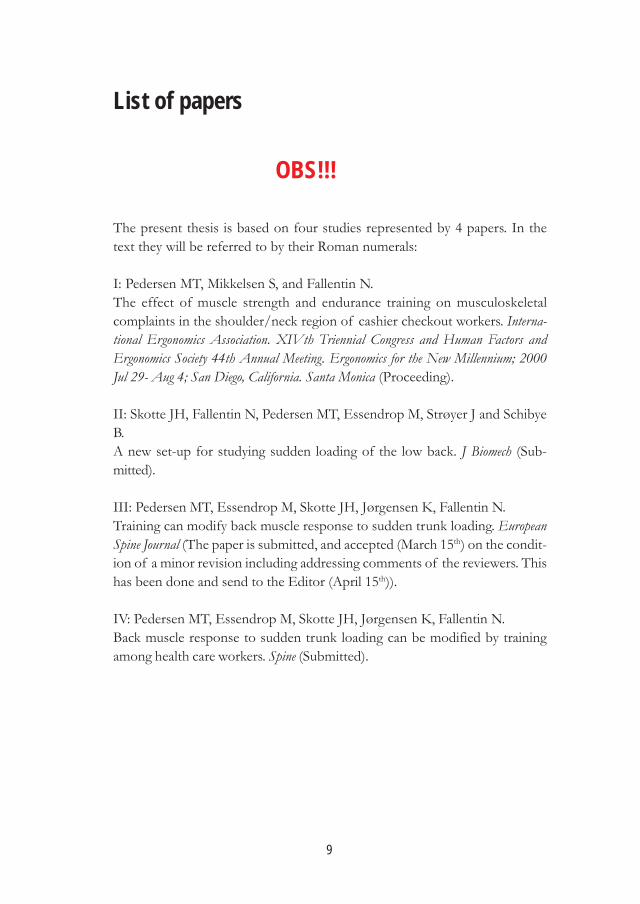
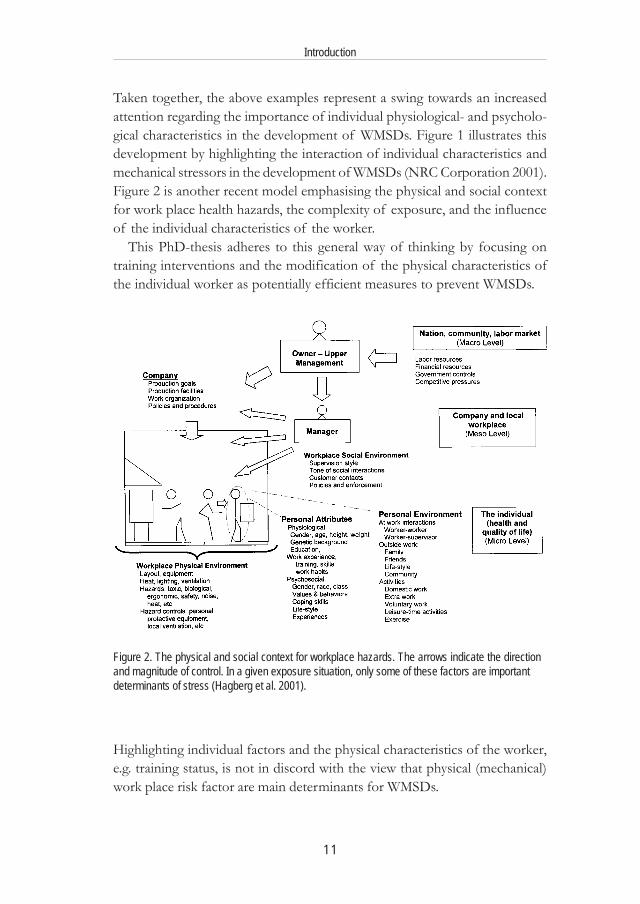
Taken together, the above examples represent a swing towards an increasedattention regarding the importance of individual physiological- and psycholo-gical characteristics in the development of WMSDs. Figure 1 illustrates thisdevelopment by highlighting the interaction of individual characteristics andmechanical stressors in the development of WMSDs (NRC Corporation 2001).Figure 2 is another recent model emphasising the physical and social contextfor work place health hazards, the complexity of exposure, and the influenceof the individual characteristics of the worker.
This PhD-thesis adheres to this general way of thinking by focusing ontraining interventions and the modification of the physical characteristics ofthe individual worker as potentially efficient measures to prevent WMSDs.
Highlighting individual factors and the physical characteristics of the worker,e.g. training status, is not in discord with the view that physical (mechanical)work place risk factor are main determinants for WMSDs.
Figure 2. The physical and social context for workplace hazards. The arrows indicate the directionand magnitude of control. In a given exposure situation, only some of these factors are importantdeterminants of stress (Hagberg et al. 2001).

12
Introduction
Two major reviews issued by NIOSH and the National Academy of Sciencein the US convincingly presents the epidemiological evidence for a causalrelationship between physical work place risk factors and development ofWMSDs:
For upper extremity disorders there is evidence of a causal relationship with thefollowing risk factors: repetitive tasks, forceful tasks, the combination of repe-tition and force and the combination of repetition and cold (NRC Corporation2001). The neck, shoulders and upper arms operate as a functional unit, whichmakes it difficult to estimate specific exposure factors for the neck/shoulderregion beyond that of job or job tasks (NRC Corporation 2001). Still for theshoulder documented risk factors have been attributed to high repetitiveness,awkward work positions, static work, repeated or continued shoulder positionswith more than 60 degrees flexion or abduction (Bernard 1997). For the neckdocumented risk factors have been attributed to high repetitiveness involvingarm and hand movements and neck movements, forceful arm and handmovements, high static neck load, continuous static load and extreme neck-working-postures (Ariens et al. 2000; Bernard 1997; Viikari-Juntura et al. 2001).
Documented risk factors for work related low back pain (LBP) are heavyphysical work, lifting and/or carrying heavy weights, forceful movements,awkward working postures (frequent bending and twisting) and whole bodyvibrations (Bernard 1997; NRC Corporation 2001). An important fraction ofLBP-cases seem to be due to sudden back loading (SL) such as e.g. slips whilecarrying a heavy weight or catching a falling object (Manning et al. 1984;Marras et al. 1987). Cholewicki and McGill (1995) stated that even light bur-dens could be a risk factor for sudden LBP because of the risk of buckling inthe relaxed state. Pope suggested in a post hearing comment on the OccupationalSafety and Health Administration’s (OSHA’s) proposed standard on ergonomics,that the standard should recognize unexpected SL as an ergonomic risk factor(Pope 2000).
The concept of specificity of association – i.e. that a risk factor is associatedwith one specific outcome and not others – needs to be considered withcaution in relation to WMSDs. There are, however, frequent observationsindicating that jobs with characteristic exposure profiles exhibit a preponderanceof WMSDs in certain body regions, and the two job groups studied in thepresent study (supermarket checkout workers and health care personnel)represent highly different exposure/response profiles.
There is a high frequency of WMSDs in the upper extremities (shoulder/neck) among supermarket checkout workers (Ayoub 1990; Harber et al. 1992;

13
Introduction
Lundberg et al. 1999). The introduction of electronic scanning check-out sy-stems seem to have increased the frequency of disorders due to an increasedworking pace (Grant and Habes 1995). Grant and Habes (1995) found basedon a literature review that 37-56% of grocery cashiers experience regular painin the upper extremity. Lundberg et al. (1999) found an incidence of 60-75%of neck and shoulder disorders among employees working at supermarkets.
Work-related LBP is more frequent among health-care personnel (Estryn-Behar et al. 1990; Jensen et al. 1995; Smedley et al. 1995). In a Danish studyamong health care workers 67% reported LBP within the last year against 45%among employees from various other occupations (Jensen et al. 1995). Patienthandling including SL and lifting heavy weights were risk factors for LBP(Jensen et al. 1995).
Individual risk factors for upper neck, shoulder and back pain
Pinpointing individual characteristics expected to have the most prominenteffect on musculoskeletal outcomes have hitherto focussed mainly on twoinherent muscle characteristics: muscle strength (including lifting capacity)and muscle endurance. In recent years, however, more subtle aspects of mo-tor control and local reflex mechanisms have received increased attention.
The „traditional“ view: Muscle strength and endurance
Neck and shoulderThe association between muscle strength/endurance and the frequency ofmusculoskeletal disorders in the shoulder and neck is not clear-cut. In aprospective study female care assembly-workers with low static shoulderstrength and low muscle endurance had a greater risk for shoulder/-neckdisorders compared to their colleagues (Kilbom 1988). Car assembly-workersperformed their job standing and walking lifting weights up to 100N. In astudy among female workers in the electronic industry there were no associa-tion between shoulder function and development of shoulder/neck symptoms(Kilbom 1988). These workers did precision work while being exposed tostatic postural load. A prospective study among bank caschiers (Takala andViikari-Juntura 1991) did not show any association between shoulder strengthand endurance and the development of neck/-shoulder symptoms.
14
Introduction
Low backSeveral prospective studies have examined the association between back musclefunction and LBP. Maximal isometric back and abdominal strength failed toshow any association to the development of LBP in a number of studies(Kujala et al. 1996; Nordgren et al. 1980). Likewise there was no associationbetween development of LBP and maximal lifting capacity (Battié et al. 1989;Luoto et al. 1995; Newton et al. 1993; Newton and Waddell 1993).
Isokinetic measurements did not show the expected association betweenlow strength and development of LBP (Newton et al. 1993; Newton andWaddell 1993; Takala and Viikari-Juntura 1997). On the contrary Masset et al.(1998) found that individuals performing dynamic trunk tests at high velocitiesappeared to be at greater risk of LBP.
Biering-Sørensen (1984) found that low static back endurance was associatedwith the development of LBP among men without an earlier history of LBP.This was supported by Jørgensen (1997). Luoto et al. (1995) showed thatindividuals with low static back endurance (from 4 different job categories)had a three-fold risk of developing LBP.
Studies have failed to document associations between dynamics back orabdominal endurance and development of LBP (Kujala et al. 1996; Leino et al.1987; Luoto et al. 1995).
The „newcomer“: motor control aspects
Edwards (1988) presented a hypothesis suggesting, that improper motor controlcould be the key aspect in WMSDs. Eleven years later the motor controlaspect has been the „hot topic“ in discussion of low back disorders and atCalgary McGill summarized the new trend by emphasizing: „New evidencepoints to the loss of fitness of the motor control system where the mostappropriate motor patterns are not produced following injury leading to therisk of injury exacerbation. This leads to unstable shearing and bending motionswhich damage tissue“ (McGill 1999).
Lumbar stability models emphasize that the mechanical stability of the spineprior to loading, and the reflex response of the muscles immediately afterloading combine to determine the kinematics response of the trunk andsubsequent likelihood of injury (Cholewicki 1999; Ebenbichler et al. 2001;McGill 2001; Morris et al. 1961). In the absence of muscle contraction bucklingof the lumbar spine occurs under compressive loads as little as 2 kg (Morris et

15
Introduction
al. 1961)). The muscles have been shown repeatedly to be the most importantfactor in spinal stability under various conditions (Cholewicki and McGill1995; Ebenbichler et al. 2001; Solomonow et al. 1998). The degree of muscleactivity may be regulated by the gamma system and proprioceptive, kinesthetic,and nociceptive information from the spinal ligaments, disks and joint capsulesplay a key role in the control of back muscles (Ebenbichler et al. 2001; Johanssonand Sojka 1991). Sjölander and Johansson (1997) stated that „proprioceptivetriggering which is a feed back process by which proprioceptive input aboutthe position and velocity of a moving joint can be used by the central nervoussystem to trigger other motor responses during the execution of a movement“.Feed back by proprioceptive triggering is supposed to function during fastmovements (like trunk movements during sudden spine loading) in contrast tofeed back servo regulation of slow movements (Sjölander and Johansson 1997).Injury, fatigue, disturbed muscle metabolism, psychosocial stress, biomechanicalconstraints (e.g. in connection with precision work or conflicting motor pro-grams (Ebenbichler et al. 2001; Oddsson et al. 1999)) will influence the quality– and/or the „interpretation“ – of the information from the sensory systemwhich is decisive of normal and appropriate motor control.
Magnusson et al. (1996) and Wilder et al. (1996) showed that low backpatients had longer erector spinae EMG reaction times (or onset latencies)during a sudden back loading incident than their matched controls. During aquick-release test patients had longer reaction times for muscles shutting off(70ms) and switching on (83ms) and in addition patients had a different muscleresponse pattern (Radebold et al. 2000). A different muscular function accom-panying low back pain has also been documented in other studies: delayedonset of specific torso muscles during sudden events (Hodges and Richardson1996, 1999; Radebold et al. 2001); changes in torso agonist/antagonist activityduring gait (Arendt-Nielsen et al. 1995) and asymmetric muscle output duringisokinetic torso extensor effort (Grabiner et al. 1992). Luoto et al. (1996) andTaimela et al. (1993) found a decrease in eye-hand reaction time among lowback patients compared to non-patients. These motor-control differencesbetween patients and healthy controls can be a reaction to the injury itself, orit may, alternatively, reflect an individual predisposing factor to low back injuries.
The efficiency of reflexive motor patterns are thus vital for maintainingstability during sudden events (Cholewicki et al. 2000) and may also be ofmajor importance in adapting the individual capacities to meet occupationaldemands.

16
Introduction
Modification of individual physical capacity as a preventive measure:Results from intervention studies
Hypothetically a high level of fitness of the musculoskeletal and cardiovascularsystem in workers in physically demanding jobs could benefit the worker andprevent the development of WMSDs (due to a reduced relative work loadcompared to the load on less fit workers). Heavy occupational work doeshowever not automatically promote the fitness and training status of the workforce – some studies actually indicate a degradation and reduction of fitness(Nygård et al. 1994; Schibye and Hansen 1999) - and a number of interventionstudies have tried to implement exercise training as a means of increasingindividual physical capacity and reduce the incidence of WMSDs.
Shoulder and neckThere is conflicting evidence about the effectiveness of exercise programsfor management of neck and shoulder pain. Results from studies of trainingprograms initiated in order to prevent musculoskeletal disorders in neck andupper extremity are far from being consistent. Dyrssen et al. (1990) found apositive effect of intensive strength training (30 min 3 times a week for 3months) on musculoskeletal complaints in neck and shoulder among officeworkers. Intensive neck strengthening (for 8-11 weeks) has been shown todecrease pain among female office workers and patients (Berg et al. 1994;Bronfort et al. 2001; Levoska and Keinanen-Kiukaanniemi 1993). In a rando-mized controlled study (RCT) among insurance workers Grønningsäter et al.(1992) found a significant effect of aerobic, strength, flexibility and relaxationexercises (10weeks, 2 times per day, 55 min, 3 times a week) on neck pain at 6months follow up. Silverstein et al. (1988), however, found no effect ofcombined strength, endurance and stretch training 14 minutes a day for oneyear on the incidence of complaints among assembly workers. Takala et al.(1994) found no effect of 45 minutes of light gymnastics a day for 10 weeks.
In conclusion, Barondes et al. (NRC Corporation 2001) and Mior (2001)summarized the results from literature reviews by stating „that the evidenceof effectiveness of exercise in management of neck and shoulder pain waslimited except for fibromyalgia (Mior 2001)“.
17
Introduction
Low backThe evidence for a positive effect of exercise for management of LBP appearsto be more consistent. The evidence, however, is mainly based on studies ofrehabilitation and reoccurrence LBP. In the study by Grønningsäter et. al.(described above) there was a significant effect of 10 weeks of aerobic, strength,flexibility and relaxation exercises on LBP.
In a RCT among hospital employees Gundewall et al. (1993) found a posi-tive effect of back muscle strength training (13 months, 2-6 times per week, 20min) on low back complaints and the intensity of pain.
In another study among hospital workers Oldervoll et al. (2001) comparedthe effect of two different physical exercise programs on LBP. Both enduranceand strength promoting training reduced pain compared to the changes in thecontrol group with no difference between intervention groups.
In a RCT among a population with a history of LBP an active back school,comprising of 20 one hour lessons of 20 min theoretical and 40 min exercisepart (35 min circle-strength training and 5 min stretching exercises), the re-occurrence and severity of new LBP episodes at 5 and 12 and 36 monthsfollow up was reduced (Glomsrod et al. 2001; Lonn et al. 1999). Soukup et al.(1999) also in a RCT found a reduction in reoccurrence of new LBP episodesat 12 month follow up after 20 one-hour group sessions of a Mensendieckprogram among a population with history of LBP. The Mensendieck approachcombined ergonomic education and strength and endurance exercises as wellas coordination exercises for the hip, pelvic and upper body.
Mior (2001) concluded in a review that exercise is effective for the manage-ment of chronic LBP for up to one year after treatment, but no particularexercise program is favoured. Two of three recent high quality studiesdocumented a positive effect of exercise on LBP (NRC Corporation 2001).
Magnusson et al. (1996) have demonstrated that training can alter the backmuscle response to SL in patients: after 2 weeks of rehabilitation includingspecific training of coordination and posture control, EMG reaction time andamplitude decreased. The change in motor-control resulting in a quicker and„more efficient“ reaction to unexpected SL was supposed to reduce themechanical load on the spine and thus decrease the risk of new back pain.
In a recent review Proper et al. (2003) stated that there is strong evidencefor a positive effect of worksite physical activity programs on muskuloskeletaldisorders but more high qualitative studies are needed taking into accountcriteria such as randomisation, blinding and compliance.

18
Based on the information presented in the above sections the PhD-study wasinitiated with the aims of:1) Providing new insight into the effect of a traditional muscle strength and
endurance training program on shoulder/neck disorders in cashier check-out workers (study I).
2) Elucidating the potential possibilities of improving motor control aspectsand the individual adaptive responses to SL among health care workers(study II, III, IV).
The hypotheses were:1) In a well-designed and controlled study muscle strength and endurance
training can be shown to be efficient in preventing the development ofneck and shoulder complaints among cashier checkout workers.
2) Motor control training can improve neuro-muscular reactions and spinalprotective mechanisms in individuals exposed to SL.
Aims and hypotheses

19
Material and methods
For an overall description of the methods readers are referred to the originalpapers. This section elaborates certain methodological aspects related to thephysical training programs, the SL-measurements and the EMG-data analysesand describes shortly the use of questionnaires for evaluating the effect oftraining.
Overall design
Study I was designed to investigate the health effect of a muscle strength andendurance training program on shoulder/neck disorders in cashier checkoutworkers. The study was primarily initiated on the basis of conflicting evidenceabout the effectiveness of exercise programs for management of neck andshoulder pain combined with the fact that a negative association had beenfound between muscle strength and development of shoulder neck- painamong workers exposed to high repetitiveness including high loads (Kilbom1988).
Study II was a method study necessary for carrying out study III and IV.In study III and IV the effect of training on the response to SL among
untrained healthy individuals (study III) and health care workers (study IV)was investigated. The studies were primarily initiated on the background thatstrength and endurance training has been effective for the management ofchronic LBP, but studies on coordination training for improving the reactionto SL had only been performed in low back patients.
Cullen (1990) has published a model with four necessary steps required forbuilding up the evidence base for nationwide prevention programs (step 5):1. Etiological studies2. Case studies3. Controlled intervention trials.4. Population studies
20
Material and methods
Inervention StudiesPaper Intervention MeasurementsSubjects
30 training sessions of45 minutes musclestrength and enduran-ce training during a15-weeks period. Thetraining was progres-sive resistance trainingwith dumbbells forneck and shoulders.
training control before theintervention
after theintervention
I 29 cashiercheckoutworkers
24 cashiercheckoutworkers
Isometric strengthin neck/shoulderDynamic shoulderenduranceMedical exami-nation includingquestionnaire onshoulder/neckcomplaints.
Isometric strengthin neck/shoulderDynamic shoulderenduranceMedical exami-nation includingquestionnaires onshoulder/neckcomplaintsQuestionnaire a-bout the trainingand the effect oftraining.
10 sessions of 45 mi-nutes of readiness trai-ning during a 4-weeksperiod. The training wasfocused on reactions toa variety of expected andunexpected suddentrunk loadings includingbalance and coordina-tion exercises.
19 untrainedhealthy officeworkers andresearchers
19 untrainedhealthy officeworkers andresearchers
Questionnaireabout health andphysical training(for inclusion)Reaction to suddenunexpected SL1
Questionnaireabout the trainingand the effect oftrainingReaction to suddenunexpected SL1
Questionnaireabout the trainingand the effect oftrainingReaction to suddenexpected andunexpected SL1
Questionnaireabout health andphysical training(for inclusion)Reaction to suddenexpected andunexpected SL1
23 employeesworking at ageriatric ward
14 employeesworking at ageriatric ward
18 sessions of 1 hourreadiness training du-ring a 9 weeks period.The training was fo-cused on reactions to avariety of expected andunexpected suddentrunk loadings inclu-ding balance and coor-dination exercises.
III
IV
Method Study
Paper MeasurementsSubjectsII 19 male construction site workers
1 EMG activity from the erector spinae muscles and trunk movement data were recorded during SL’s.
Reaction to sudden expected and unexpected SL1
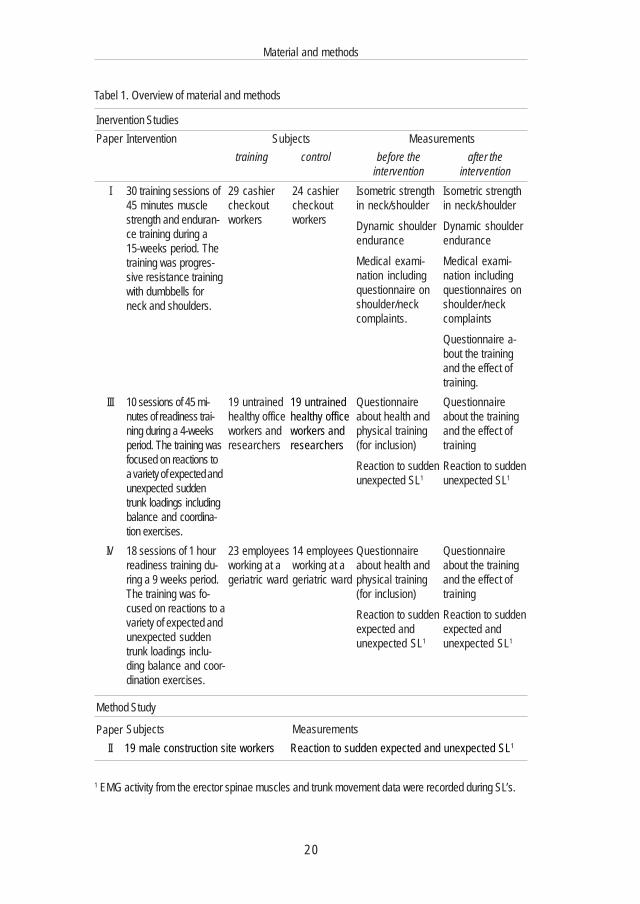
Tabel 1. Overview of material and methods

21
Material and methods
In this thesis study I represents a study at step 3 in the model. Study III and IVare also controlled trials, but represent a more basic approach focusing onmechanisms and potential etiologic factors (step 1 research).
In table 1 an overview of material and methods (including procedure) forthe 4 studies is presented.
Material
In study I all 107 workers at the cashier checkouts in two supermarkets wereinvited to participate in the project. 75 (70%) accepted, 26 men and 49 women.Their average age was 25 years (range 18 to 61 years). Sixty-five had cashiercheckout work only, while 10 were service workers with more varied workand only few hours at the cashier checkout. The median working hours were19 hours/week (range 8 - 40 hours/week). The median working hours at thecheckout were 14 hours/week (range 0 - 40 hours/week). Eighteen (24%)worked at the checkout 0-9 hours, 20 (27%) 10 -14 hours, 22 (29%) 15 -34hours and 15 (20%) 35 hours or more. Before the intervention started, theparticipants were allocated to at training group (n=42) and to a control group(n=33). The training group was made a little larger than the control group asmore dropouts were expected in the training group. The allocation to the twogroups was made at random from 4 complaint strata, recorded by the NordicMusculoskeletal Questionnaire(Kourinka et al. 1987; Palmer et al. 1999): 1)subjects without any pain or discomfort in the neck or shoulders during thelast 12 months; 2) subjects with pain or discomfort in one region (neck or oneof the shoulders); 3) subjects with pain in two regions (neck and one shoulderor both shoulders); and 4) subjects with pain in all three regions (neck andboth shoulders). However, the initial randomisation could not be strictlyadhered to in practice. Five subjects selected for training were not at workduring the training sessions. Therefore these persons were exchanged withsubjects from the control group with similar complaints (complaints or notwithin 12 months in left- right shoulder and neck). It turned out that thesubstitutes in the training group had the same frequency of complaints as theplanned participants, but the intensity of pain was higher. Also 2 persons, whohad not filled the questionnaires before the intervention, were not randomised.But quantitatively the most important problem was that the dropout in thetraining group (13 subjects) was highest among persons without initial complaints.
These non-random events have introduced a skewed distribution of initial

22
Material and methods
complaints in the final training and control group, i.e. those of the originaltraining group who participated in more than 50% of the training sessions(n=29) and those of the control group that participated in all examinations(n=24).
In study III 19 subjects in the training group (3 men and 16 women; meanage 35 years, range 23-54 years) were matched on the bases of age,anthropometrical measurements, job function and physical activity to 19 controls(5 men and 14 women; mean age 35 years, range 24-52 years). All were untrainedoffice workers and researchers at the National Institute of Occupational Health.Study IV included 23 participants (21 women 2 men; mean age 41, range 24-58) and 14 controls (14 women; mean age 44, range 22-58) working at a geriatricward as nursing aides, orderlies, physiotherapists or occupational therapists.Working schedules was the key factor for allocating subjects to the control ortraining group. Randomisation or matching was not possible. A bias due to thedistribution of participants and controls was not expected because the jobfunctions and the amount of spare time physical activity in the control andtraining group were comparable.
In study II there was one group of 19 male construction site workers(mean age 39, range 27-55).
Training
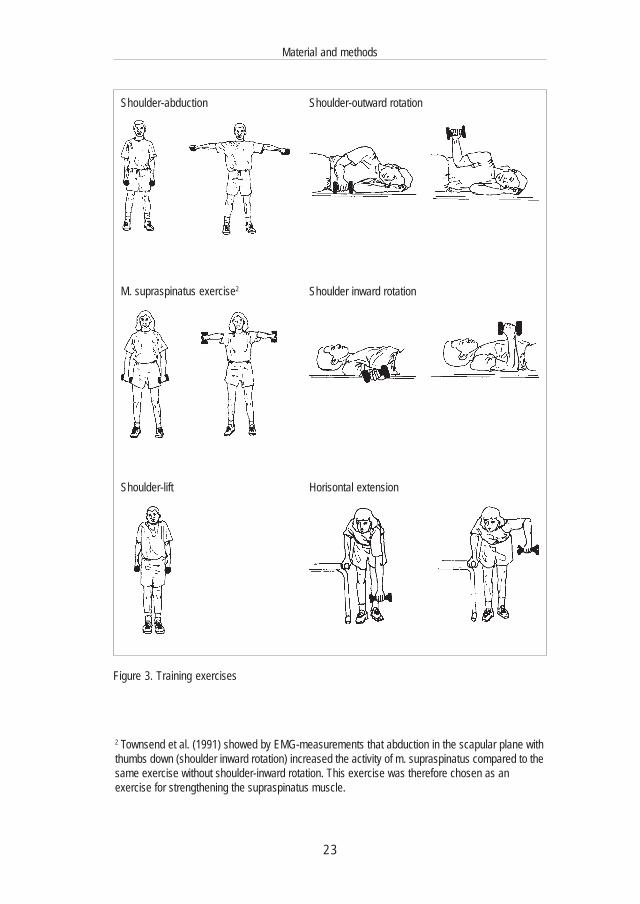
In all training studies the control group worked as usual and was not offeredany form of training. In study I the training group was given the opportunityto participate in 30 training sessions two times a week during working hours.The training was done in small groups of 6-8 people and each session consistedof 5 minutes of warming-up to music and 30 minutes of strength and muscle-endurance training with dumbbells. At each session the same 6 shoulder/neckmuscle exercises (figure 3) were done twice with a repetition maximum (RM)of 10-15 repetitions. If a participant could do more than 15 repetitions in anexercise, the weight was increased at the next performance of the same exercise.An instructor supervised the training each time.
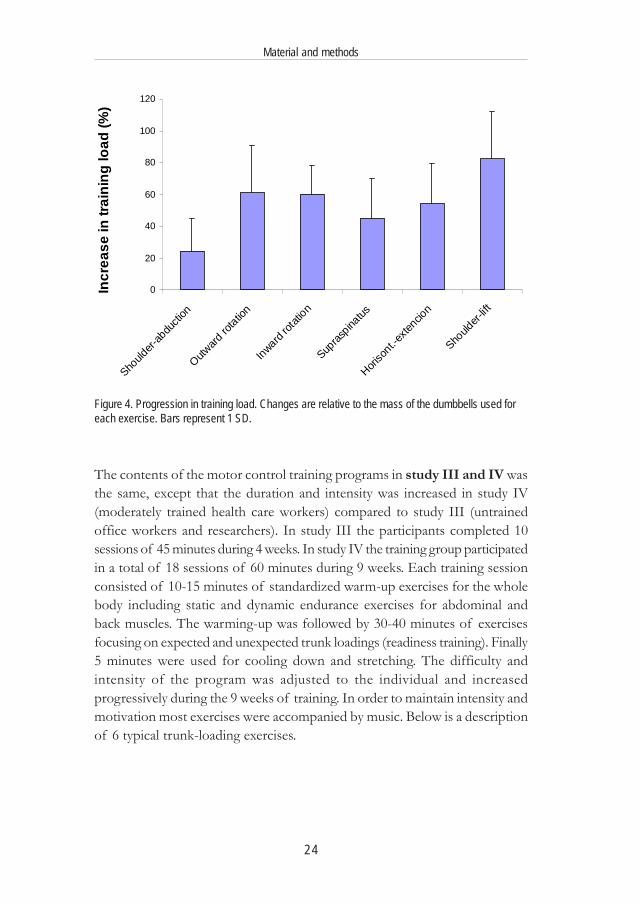
At every training session participants filled in a training-diary with informa-tion about training load and number of repetitions for each exercise. Therelative increases in load for each exercise during the intervention period areillustrated in figure 4. The increase is relative to the starting load at the thirdtraining session (after getting used to the training).
23
Material and methods
Figure 3. Training exercises
Shoulder-abduction Shoulder-outward rotation
M. supraspinatus exercise2 Shoulder inward rotation
Horisontal extensionShoulder-lift
2 Townsend et al. (1991) showed by EMG-measurements that abduction in the scapular plane withthumbs down (shoulder inward rotation) increased the activity of m. supraspinatus compared to thesame exercise without shoulder-inward rotation. This exercise was therefore chosen as anexercise for strengthening the supraspinatus muscle.
24
Material and methods
0
20
40
60
80
100
120
Should
er-ab
ducti
on
Outward
rotatio
n
Inward rot
ation
Supras
pinatus
Horiso
nt.-exte
ncion
Should
er-lift
Incr
ease
in tr
aini
ng lo
ad (%
)
Figure 4. Progression in training load. Changes are relative to the mass of the dumbbells used foreach exercise. Bars represent 1 SD.
The contents of the motor control training programs in study III and IV wasthe same, except that the duration and intensity was increased in study IV(moderately trained health care workers) compared to study III (untrainedoffice workers and researchers). In study III the participants completed 10sessions of 45 minutes during 4 weeks. In study IV the training group participatedin a total of 18 sessions of 60 minutes during 9 weeks. Each training sessionconsisted of 10-15 minutes of standardized warm-up exercises for the wholebody including static and dynamic endurance exercises for abdominal andback muscles. The warming-up was followed by 30-40 minutes of exercisesfocusing on expected and unexpected trunk loadings (readiness training). Finally5 minutes were used for cooling down and stretching. The difficulty andintensity of the program was adjusted to the individual and increasedprogressively during the 9 weeks of training. In order to maintain intensity andmotivation most exercises were accompanied by music. Below is a descriptionof 6 typical trunk-loading exercises.
25
Material and methods
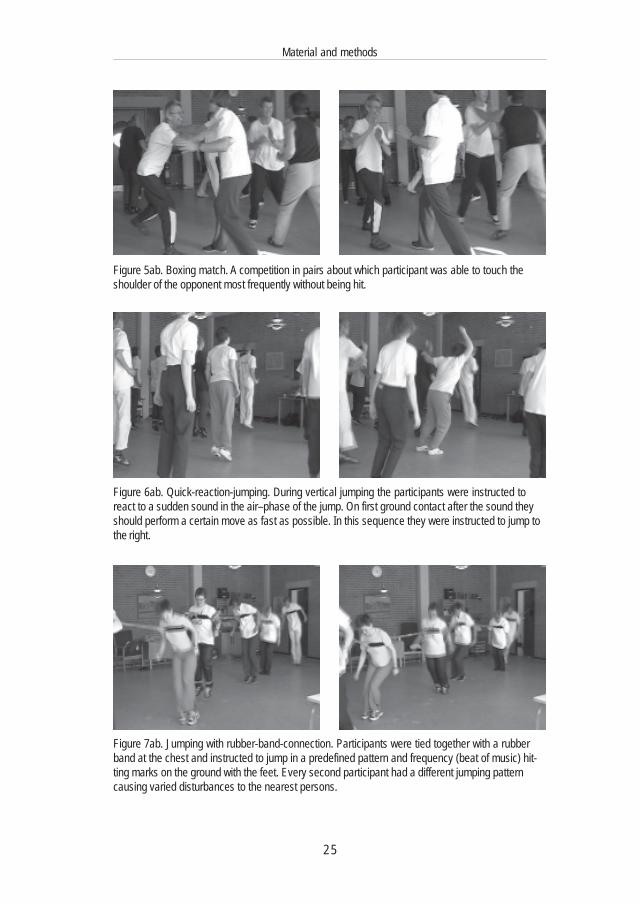
Figure 5ab. Boxing match. A competition in pairs about which participant was able to touch theshoulder of the opponent most frequently without being hit.
Figure 7ab. Jumping with rubber-band-connection. Participants were tied together with a rubberband at the chest and instructed to jump in a predefined pattern and frequency (beat of music) hit-ting marks on the ground with the feet. Every second participant had a different jumping patterncausing varied disturbances to the nearest persons.
Figure 6ab. Quick-reaction-jumping. During vertical jumping the participants were instructed toreact to a sudden sound in the air–phase of the jump. On first ground contact after the sound theyshould perform a certain move as fast as possible. In this sequence they were instructed to jump tothe right.
26
Material and methods
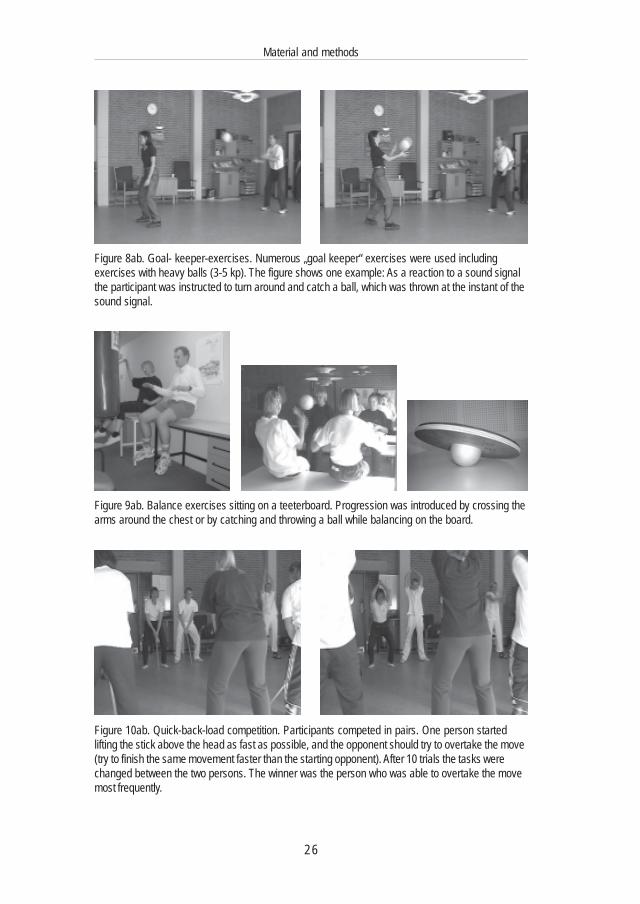
Figure 8ab. Goal- keeper-exercises. Numerous „goal keeper“ exercises were used includingexercises with heavy balls (3-5 kp). The figure shows one example: As a reaction to a sound signalthe participant was instructed to turn around and catch a ball, which was thrown at the instant of thesound signal.
Figure 9ab. Balance exercises sitting on a teeterboard. Progression was introduced by crossing thearms around the chest or by catching and throwing a ball while balancing on the board.
Figure 10ab. Quick-back-load competition. Participants competed in pairs. One person startedlifting the stick above the head as fast as possible, and the opponent should try to overtake the move(try to finish the same movement faster than the starting opponent). After 10 trials the tasks werechanged between the two persons. The winner was the person who was able to overtake the movemost frequently.
27
Material and methods
Sudden back loading (SL)
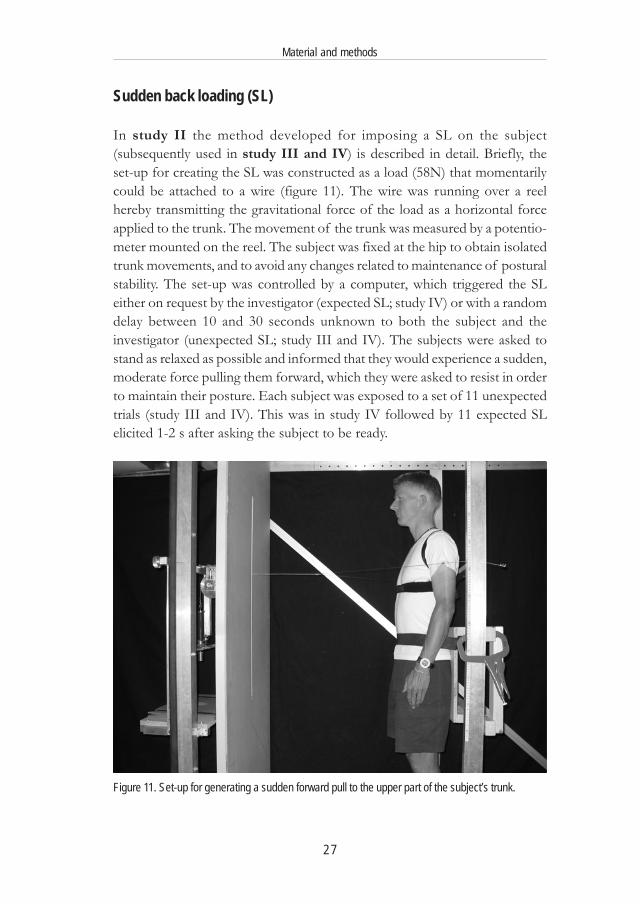
In study II the method developed for imposing a SL on the subject(subsequently used in study III and IV) is described in detail. Briefly, theset-up for creating the SL was constructed as a load (58N) that momentarilycould be attached to a wire (figure 11). The wire was running over a reelhereby transmitting the gravitational force of the load as a horizontal forceapplied to the trunk. The movement of the trunk was measured by a potentio-meter mounted on the reel. The subject was fixed at the hip to obtain isolatedtrunk movements, and to avoid any changes related to maintenance of posturalstability. The set-up was controlled by a computer, which triggered the SLeither on request by the investigator (expected SL; study IV) or with a randomdelay between 10 and 30 seconds unknown to both the subject and theinvestigator (unexpected SL; study III and IV). The subjects were asked tostand as relaxed as possible and informed that they would experience a sudden,moderate force pulling them forward, which they were asked to resist in orderto maintain their posture. Each subject was exposed to a set of 11 unexpectedtrials (study III and IV). This was in study IV followed by 11 expected SLelicited 1-2 s after asking the subject to be ready.
Figure 11. Set-up for generating a sudden forward pull to the upper part of the subject’s trunk.
28
Material and methods
Electromyography
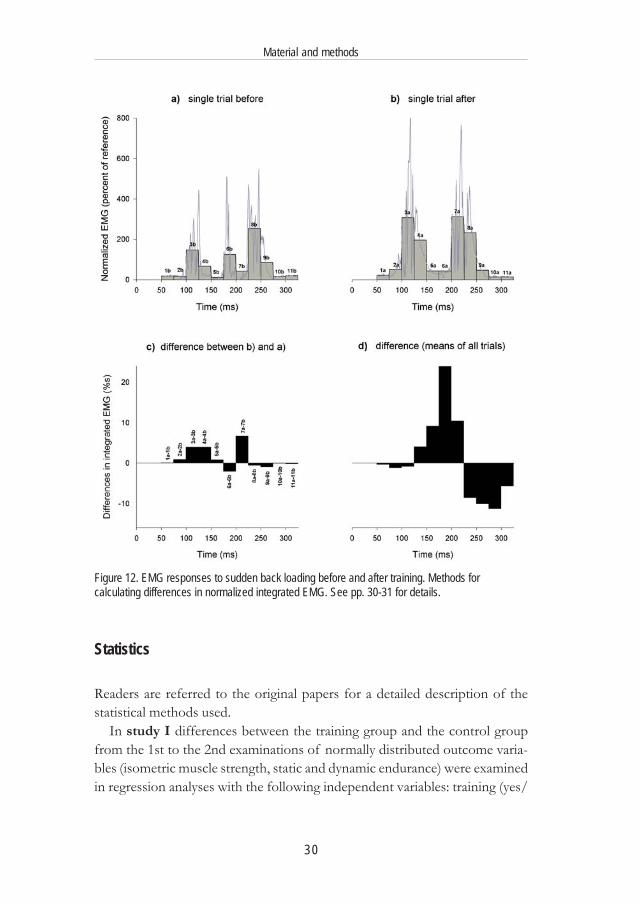
In study II, III & IV pre-gelled Ag/AgCl surface electrodes were used torecord the EMG activity of the erector spinae muscles during the SL trial.The electrodes were placed 3 cm apart on both sides of L3, approximately 3cm lateral to the spinal column in the middle of the muscle belly. EMGsignals were pre-amplified (25 times), high-pass filtered with a cut-off frequencyof 10 Hz (1st order), further amplified (variable gain) and low-pass filteredwith a cut-off frequency of 400 Hz with an 8th order Butterworth filter. Theamplified and filtered EMG signals were sampled with 1000 Hz. The EMGrecordings were high pass filtered (2nd order) with a cut-off frequency of 25Hz and rectified. In study III the EMG-signal was rectified and normalizedaccording to EMG-signals obtained from a standardized sub maximal staticback extension, which was performed at the test before and after the trainingintervention. In order to analyse EMG-amplitude the normalized signal wasintegrated in time intervals of 25 ms in the period from 50 ms to 325 ms afterthe SL. Below is a detailed description of how the differences in the time wisedistribution of the EMG response in subjects before and after training wereanalyzed:
Figure 12a shows the normalized rectified EMG signal (R-erector spinae)for one trial before the intervention. The columns illustrate the area under theEMG-curve (integrated EMG) in intervals of 25 ms from 50-325 ms after theSL. Column 1b represents the area under the EMG-curve from 50ms to 75ms, column 2b the area from 75 ms to 100 ms… In the same way figure 12bshows the EMG signal and integrated EMG for one trial for the same subjectafter the intervention. Figure 12c shows the differences (after-before) inintegrated EMG illustrated in intervals of 25 ms for one trial. The bars illustratedifferences in integrated EMG calculated as the differences of the bars infigure 12b and 12a e.g.:
75-100 ms: differences in integrated EMG = 2a-2b
The means of the differences in intervals of 25 ms for all trials of unexpectedSL for the subjects in the training group in study III are illustrated in fig 12d(as also seen under results in figure 13).
In study III and IV the differences (after-before) in the relative time wisedistribution of the EMG signal were also presented (figure 14 and 15) as itwas considered to be less sensitive to differences in background EMG noise.In addition it is a sensible way to compare the effect without interfering withnormalization problems (as described in study IV).

29
Material and methods
The relative values for the integrated EMG-data presented in figure 12a forone trial before the intervention was calculated as:
50-75 ms: (1b/(1b+2b+3b+4b+5b…+11b)75-100 ms: (2b/(1b+2b+3b+4b+5b…+11b)
In the same way the relative values for the EMG-data presented in figure 12bfor one trial after the intervention were calculated as:
50-75 ms: (1a/(1a+2a+3a+4a+5a…+11a)
The difference in relative area for one trial was calculated as:50-75 ms: (1a/(1a+2a+3a+4a+5a…+11a) - (1b/(1b+2b+3b+4b+5b…+11b)
The mean of the relative differences in rectified normalized EMG for alltrials of unexpected SL for the subjects in the training group in study III andIV is presented under results in figure 14 and 15.
Neck-shoulder complaints
In study I participants filled in a questionnaire on shoulder-neck complaintsimmediately before and one week after the intervention. For each of the 3regions (neck, right shoulder and left shoulder) the participants were asked 4questions about the intensity of complaints: 1) worst complaints within thelast 3 months; 2) average complaints within the last 3 months; 3) functionalimpairment due to complaints within the last 3 months; and 4) complaintswithin the last 7 days. The intensity of complaints was registered on a scalefrom 0 to 9, where 0 indicated no complaints at all and 9 indicated the worstpossible pain. For each region a complaint score for the four questions wascomputed as the sum of the 4 scores (0-36) (Brauer et al. 2003).
Questionnaires about training and the effect of training
After the training interventions participants in study I and IV filled in aquestionnaire about training and the effect of training (Appendix 1, 2). Includedwere some joint questions to the training and control groups. In study IIIparticipants were asked to send a mail containing information about their per-ception of the training and the effect of the training program.
30
Material and methods
Figure 12. EMG responses to sudden back loading before and after training. Methods forcalculating differences in normalized integrated EMG. See pp. 30-31 for details.
Statistics
Readers are referred to the original papers for a detailed description of thestatistical methods used.
In study I differences between the training group and the control groupfrom the 1st to the 2nd examinations of normally distributed outcome varia-bles (isometric muscle strength, static and dynamic endurance) were examinedin regression analyses with the following independent variables: training (yes/

31
Material and methods
no), value of the variable at the 1st examination, age and sex. A change inmusculoskeletal complaint score from the 1st to the 2nd examination wasconsidered to be present if the difference in the complaint score was 2 ormore. The results were dichotomised and depending on the direction, thechange was considered either an improvement or deterioration. Fisher’s exacttest was used to assess the effect of training on improvement and deteriorationof complaints.
In study II, III and IV a two-way ANOVA with subjects (random) andtrials (fixed) as factors were used to look for differences between trials, andmultiple comparisons were carried out by the post hoc Tukey method.
In study III and IV the effect of training on stopping time, distance movedbefore stopping, EMG-latency and integrated EMG was analysed by a mixedmodel ANOVA with subjects as random factor and group (training/control)and time (before/after) as categorical fixed factors with interaction term betweengroup and time.
If variables could not match the conditions of normal distributed residualsand variance homogeneity a Box-Cox transformation was used in the two-wayand mixed model ANOVA. Paired sample t-tests were used to test for diffe-rence between the 2 test protocols.
The level of significance used was p< 0.05.
32
This section presents the main findings from the studies. For a completepresentation of the results readers are referred to the papers.
Training effect on muscular complaints
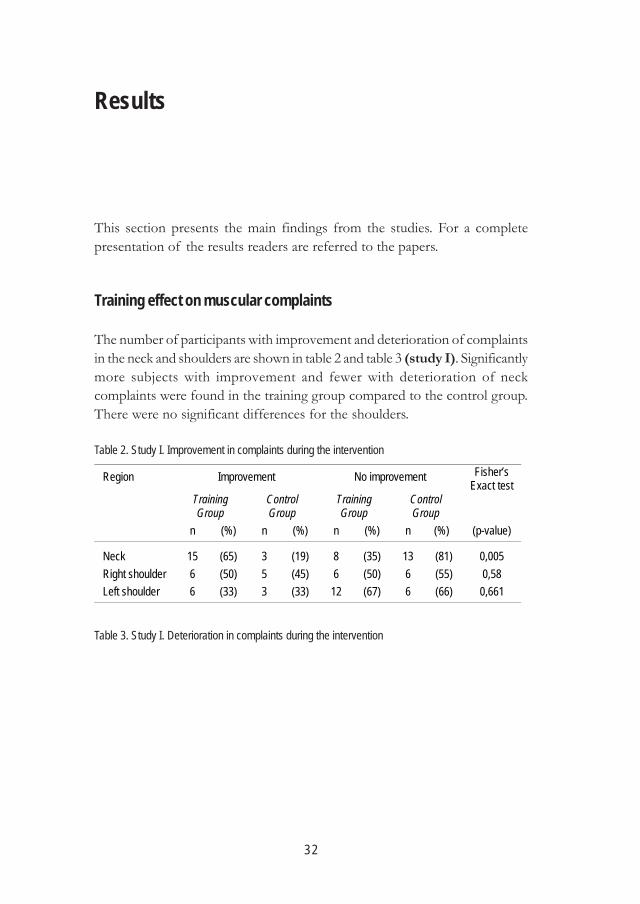
The number of participants with improvement and deterioration of complaintsin the neck and shoulders are shown in table 2 and table 3 (study I). Significantlymore subjects with improvement and fewer with deterioration of neckcomplaints were found in the training group compared to the control group.There were no significant differences for the shoulders.
Results
Table 2. Study I. Improvement in complaints during the intervention
Table 3. Study I. Deterioration in complaints during the intervention
Region Improvement No improvement Fisher’s Exact test
Training Group
Control Group
Training Group
Control Group
n (%) n (%) n (%) n (%) (p-value) Neck
15
(65)
3
(19)
8
(35)
13
(81)
0,005
Right shoulder 6 (50) 5 (45) 6 (50) 6 (55) 0,58 Left shoulder 6 (33) 3 (33) 12 (67) 6 (66) 0,661
33
Results
Mean Before Intervention
Mean After Intervention Difference
(%) Effect size
Study I
n =29 R-shoulder lift (N) 421 571 35,7 0,71 L-shoulder lift (N) 436 574 31,8 0,59 R-abduction (Nm) 40,1 45,7 14,0 0,28 L-abduction (Nm) 39,4 44,7 13,5 0,28 R-inward rotation (Nm) 34,0 42,2 24,1 0,52 L-inward rotation (Nm) 31,4 38,0 21,0 0,49 R-outward rotation (Nm) 22 25,2 14,5 0,39 L-outward rotation (Nm) 20,7 24,11 16,5 0,42 Dynamic endurance (s) 82 108 31,7 0,58
Study III
n =19 Stopping time (ms) Unexpected 338 311 -7,9 0,53
Study IV
n =20 Stopping time (ms) Unexpected 322 279 -13,4 0,62 Expected 281 258 -8,2 0,35 Distance moved (cm) Unexpected 4,7 3,8 -18,8 0,57 Expected 3,7 3,3 -10,3 0,29
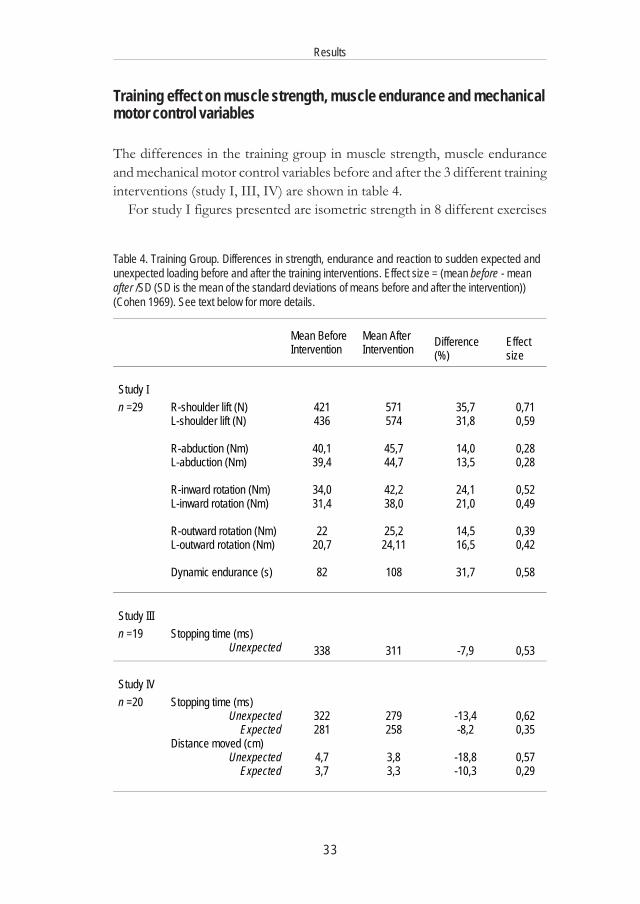
Training effect on muscle strength, muscle endurance and mechanicalmotor control variables
The differences in the training group in muscle strength, muscle enduranceand mechanical motor control variables before and after the 3 different traininginterventions (study I, III, IV) are shown in table 4.
For study I figures presented are isometric strength in 8 different exercises
Table 4. Training Group. Differences in strength, endurance and reaction to sudden expected andunexpected loading before and after the training interventions. Effect size = (mean before - meanafter /SD (SD is the mean of the standard deviations of means before and after the intervention))(Cohen 1969). See text below for more details.
34
Results
and dynamic endurance for shoulder abduction. For study III and IV all figuresrepresent measurements of reactions to SL (se study III+IV for more details).All differences in the three studies were significant compared to the differencesin the control groups except for R-shoulder lift, L-outward shoulder rotationand expected SL.
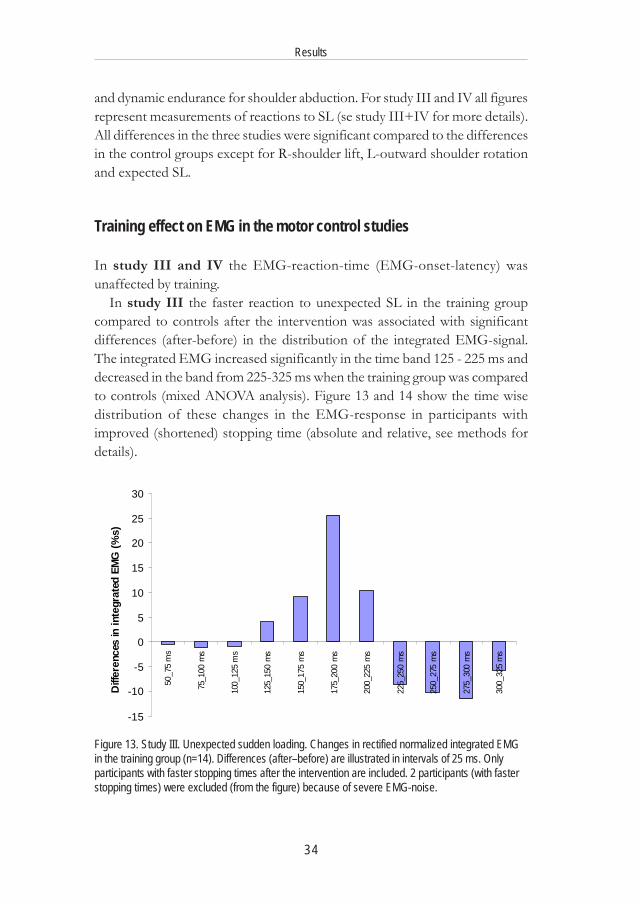
Training effect on EMG in the motor control studies
In study III and IV the EMG-reaction-time (EMG-onset-latency) wasunaffected by training.
In study III the faster reaction to unexpected SL in the training groupcompared to controls after the intervention was associated with significantdifferences (after-before) in the distribution of the integrated EMG-signal.The integrated EMG increased significantly in the time band 125 - 225 ms anddecreased in the band from 225-325 ms when the training group was comparedto controls (mixed ANOVA analysis). Figure 13 and 14 show the time wisedistribution of these changes in the EMG-response in participants withimproved (shortened) stopping time (absolute and relative, see methods fordetails).
-15
-10
-5
0
5
10
15
20
25
30
50_7
5 m
s
75_1
00 m
s
100_
125
ms
125_
150
ms
150_
175
ms
175_
200
ms
200_
225
ms
225_
250
ms
250_
275
ms
275_
300
ms
300_
325
ms
Diff
eren
ces
in in
tegr
ated
EM
G (%
s)
Figure 13. Study III. Unexpected sudden loading. Changes in rectified normalized integrated EMGin the training group (n=14). Differences (after–before) are illustrated in intervals of 25 ms. Onlyparticipants with faster stopping times after the intervention are included. 2 participants (with fasterstopping times) were excluded (from the figure) because of severe EMG-noise.
35
Results
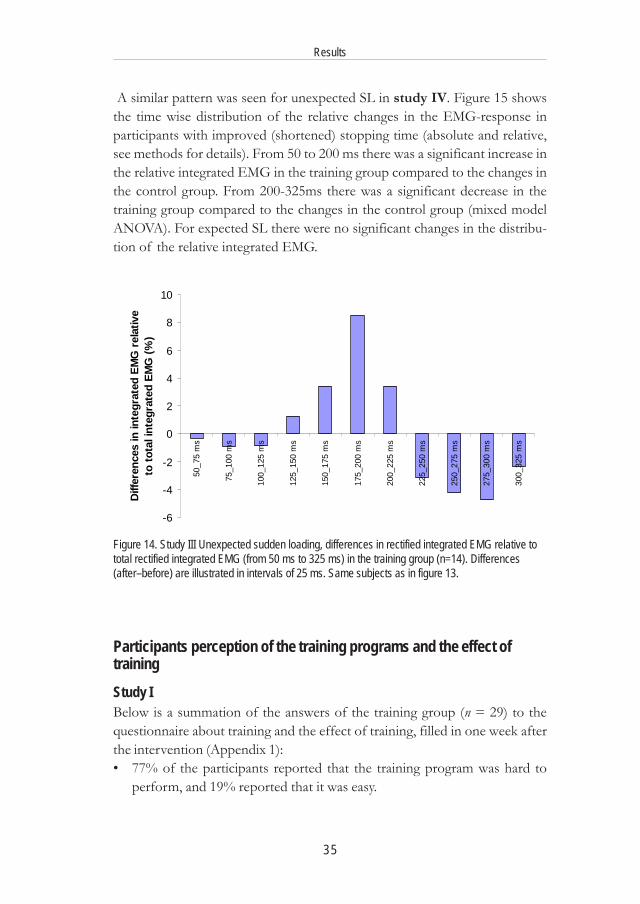
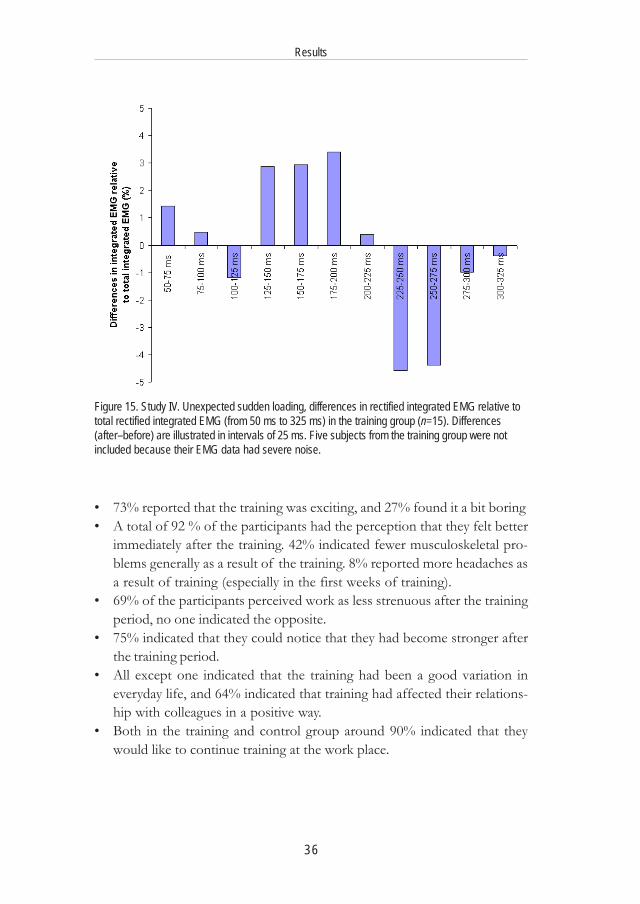
A similar pattern was seen for unexpected SL in study IV. Figure 15 showsthe time wise distribution of the relative changes in the EMG-response inparticipants with improved (shortened) stopping time (absolute and relative,see methods for details). From 50 to 200 ms there was a significant increase inthe relative integrated EMG in the training group compared to the changes inthe control group. From 200-325ms there was a significant decrease in thetraining group compared to the changes in the control group (mixed modelANOVA). For expected SL there were no significant changes in the distribu-tion of the relative integrated EMG.
Participants perception of the training programs and the effect oftrainingStudy IBelow is a summation of the answers of the training group (n = 29) to thequestionnaire about training and the effect of training, filled in one week afterthe intervention (Appendix 1):• 77% of the participants reported that the training program was hard to
perform, and 19% reported that it was easy.
Figure 14. Study III Unexpected sudden loading, differences in rectified integrated EMG relative tototal rectified integrated EMG (from 50 ms to 325 ms) in the training group (n=14). Differences(after–before) are illustrated in intervals of 25 ms. Same subjects as in figure 13.
-6
-4
-2
0
2
4
6
8
10
50_7
5 m
s
75_1
00 m
s
100_
125
ms
125_
150
ms
150_
175
ms
175_
200
ms
200_
225
ms
225_
250
ms
250_
275
ms
275_
300
ms
300_
325
ms
Diff
eren
ces
in in
tegr
ated
EM
G r
elat
ive
to to
tal i
nteg
rate
d EM
G (%
)
36
Results
Figure 15. Study IV. Unexpected sudden loading, differences in rectified integrated EMG relative tototal rectified integrated EMG (from 50 ms to 325 ms) in the training group (n=15). Differences(after–before) are illustrated in intervals of 25 ms. Five subjects from the training group were notincluded because their EMG data had severe noise.
• 73% reported that the training was exciting, and 27% found it a bit boring• A total of 92 % of the participants had the perception that they felt better
immediately after the training. 42% indicated fewer musculoskeletal pro-blems generally as a result of the training. 8% reported more headaches asa result of training (especially in the first weeks of training).
• 69% of the participants perceived work as less strenuous after the trainingperiod, no one indicated the opposite.
• 75% indicated that they could notice that they had become stronger afterthe training period.
• All except one indicated that the training had been a good variation ineveryday life, and 64% indicated that training had affected their relations-hip with colleagues in a positive way.
• Both in the training and control group around 90% indicated that theywould like to continue training at the work place.
37
Results
Study IIIBelow is a summation of the qualitative information received in e-mails (fromthe participants, n = 19) containing information on their perception of thetraining and the effect of the training program:• The training had been exciting and amusing• Training had affected participant’s relationship with colleagues in a positive
way.• Training had been a good variation in everyday life, and the participants
wanted to continue training at the work place. Training was a good start ofthe day (2 times a week in the morning).
• Training had influenced their working hours and spare time in a positiveway like: better mood, improved fitness generally, better balance
Study IVBelow is a summation of the answers of the training group (n = 20) to thequestionnaire about training and the effect of training, filled in a few daysafter the intervention (Appendix 2).• 50% of the participants reported that they perceived the training as easy
and, 50% perceived it as somewhat hard.• 80% found the training exciting and 85% found it amusing. None perceived
the training as boring.• 75% reported that training had affected their relationship with colleagues
in a positive way. 25% indicated no change.• 60% reported that the training had improved their fitness generally, and
55% indicated stronger back and abdominal muscles. 25% indicated nochange in physical capacity. 35% indicated more springiness as a result oftraining and 35% reported better balance.
• 50% indicated that training had influenced their working hours and sparetime in a positive way like:
Better moodMore well-beingMore happinessBetter balance
• All indicated that the training had been a good variation in everyday lifeand wanted to continue training at the work place.
38
Discussion
Effect of training on physical capacity
The 3 training studies (paper I, III, IV) demonstrated that work place trainingcould improve the physical capacity of the employees (table 4).
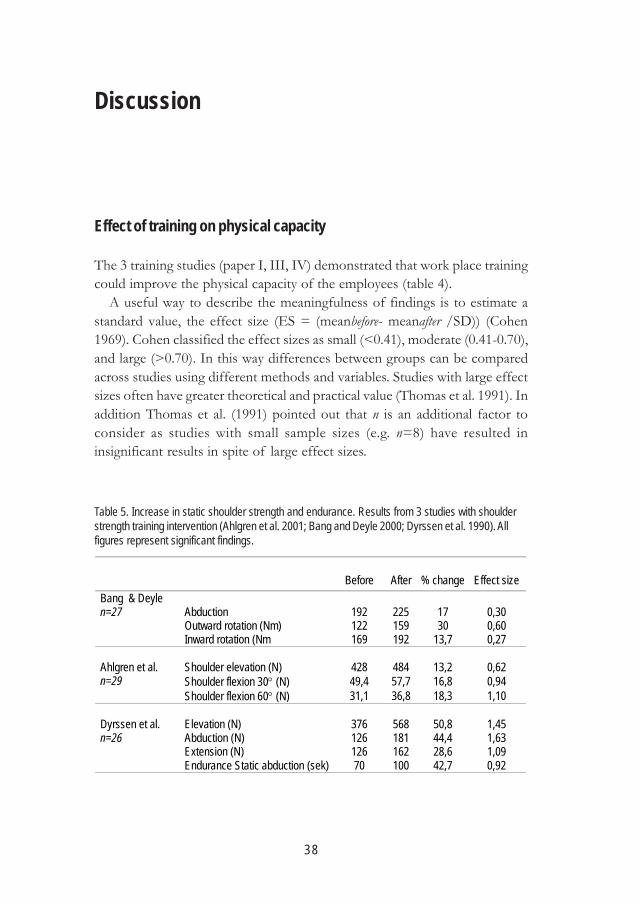
A useful way to describe the meaningfulness of findings is to estimate astandard value, the effect size (ES = (meanbefore- meanafter /SD)) (Cohen1969). Cohen classified the effect sizes as small (<0.41), moderate (0.41-0.70),and large (>0.70). In this way differences between groups can be comparedacross studies using different methods and variables. Studies with large effectsizes often have greater theoretical and practical value (Thomas et al. 1991). Inaddition Thomas et al. (1991) pointed out that n is an additional factor toconsider as studies with small sample sizes (e.g. n=8) have resulted ininsignificant results in spite of large effect sizes.
Table 5. Increase in static shoulder strength and endurance. Results from 3 studies with shoulderstrength training intervention (Ahlgren et al. 2001; Bang and Deyle 2000; Dyrssen et al. 1990). Allfigures represent significant findings.
Before After % change Effect size
Abduction 192 225 17 0,30 Outward rotation (Nm) 122 159 30 0,60
Bang & Deyle n=27
Inward rotation (Nm 169 192 13,7 0,27 Shoulder elevation (N)
428
484
13,2
0,62
Shoulder flexion 30° (N) 49,4 57,7 16,8 0,94
Ahlgren et al. n=29
Shoulder flexion 60° (N) 31,1 36,8 18,3 1,10 Elevation (N)
376
568
50,8
1,45
Abduction (N) 126 181 44,4 1,63 Extension (N) 126 162 28,6 1,09
Dyrssen et al. n=26
Endurance Static abduction (sek) 70 100 42,7 0,92

39
Discussion
Table 5 shows the results including n and effect size from 3 supervised shoulderstrength training intervention studies with exercises comparable to the onesused in study I:1. Dyrssen et al. (1990): 3 months 3 times 30 min a week for 3 months, office
workers in work. All had at some time within a year consulted the companyphysician for pain in shoulders, neck and/or upper back. All were at workduring the intervention.
2. Ahlgren et al. (2001): 1 hour 3 times a week for 10 weeks, workers withtrapezius myalgia, but still at work.
3. Bang and Deyle (2000): 2 times a week for 3 weeks, patients with shoulderimpingement syndrome.
The results presented in table 4 for study I can be compared to the 3 studiesjust mentioned (table 5). All studies showed significant improvements instrength and Dyrsen et al. also measured increased muscle endurance. Theabsolute differences (14-35%), and differences in effect size (mostly moderate(0.28-0.71)) in study I, are comparable to the results Bang & Deyle. The hugeincreases and effect sizes shown by Dyrsen et al. might be due tomethodological problems as the control group also increased significantly instrength and endurance (13-19%). Genaidy et al. (1992) in a literature review(aiming at „reviewing techniques available in exercise physiology literature forincreasing human capacity in industry“) reported improvements in upperextremity dynamic endurance and concluded that a short muscle enduranceprogram could improve static and dynamic endurance significantly.
The fact that patients with shoulder impingement syndrome participating invery few strengthening exercise sessions can increase strength considerately(Bang and Deyle 2000) supports the established fact that untrained individualshave a greater potential for improvement than more well trained individuals(Aastrand and Rodahl 1986). Similarly in study III among untrained officeworkers a 4 weeks readiness training program had a significant impact onstopping time comparable to the effect of a more long lasting and intensivetraining program among more well trained hospital workers (study IV, table 4).Study III and IV are the first studies to examine the effect of training on thereaction to SL among healthy individuals. The results in table 4 for study IIIand IV are in line with other studies of training of physical capacity amonghealthy individuals with typical improvements between 10-30% after 3 monthsof training (Aastrand and Rodahl 1986).

40
Discussion
Changes in musculoskeletal complaints; Intervention study design
In study I the allocation to the training and control groups was made by meansof the Nordic Musculoskeletal Questionnaire (Kourinka et al. 1987; Palmer etal. 1999). Palmer et al. (1999) assessed the repeatability and validity of theNordic-style questionnaire for upper limb and neck complaints and found thatsymptom reports for pain in the upper limb and neck (pain interfering withphysical activities and neurological symptoms) were highly reliable (kappa =0.63-0.90). They concluded that the Nordic questionnaire is reliable and sensi-tive.
In study I the effect of training on muscular complaints was studied. Therewas no clear pattern in the changes in the degree of shoulder complaints forthe training group compared with the control group and no significantdifferences were found. However, the figures were small, and reliableconclusions could not be made. In the case of the neck, significant differencesin the complaints in the training group and control group could be observed.This is suggestive of a positive effect of weight training on neck complaints inline with the results from Dyrsen et al. (1990), Bang and Deyle (2000) andAhlgren et al. (2001). However, the results from the neck disorders are difficultto interpret because of the skewed distribution of initial complaints in thefinal training and control groups. The observed improvement indicated a trainingeffect, but could have been due to differences in the baseline. The traininggroup had greater chances of improvement because of a higher base level ofneck complaints. This underlines the importance of successful randomisationin training intervention studies (Westgaard and Winkel 1997) and raises thequestion whether the randomisation in study I could have been more successful?
The initial skew-ness in the allocation of the subjects to the training andcontrol groups could probably have been reduced, but quantitatively the mostimportant problem was, that the dropout in the training group (13 subjects)was highest among persons without initial complaints introducing an evenmore skewed distribution of initial complaints in the final training and controlgroups. It is impossible to be well guarded against these circumstances. Thecompliance to training was influenced by the amount of pain in neck andshoulders. Subjects with pain from start in the training group were motivatedto stay in the training group due to the expected or perceived health effect ofthe training. It thus appeared that a natural change not under influence of theresearchers was the main reason for the skewed distribution of initial complaints.Compliance is a general concern in intervention studies, and intervention stu-
41
Discussion
dies should generate measures with a tangible impact on the worker (Westgaardand Winkel 1997). The effect of training might not have been sufficientlytangible for participants without initial pain.
The gold standard of study design for evaluation of treatment in clinicaltrials includes random selection of subjects to intervention and control groups,with blinding of the subjects and researchers to group membership and pla-cebo treatment of the control group (Westgaard and Winkel 1997), but thisdesign is generally not achievable in ergonomic intervention research. Theblinding of subjects and researchers was not possible in the interventionstudies (I, III, IV) and randomisation was only attempted in study I. Study IIIand IV were training intervention studies aiming at improving the response toSL.
In study III subjects in the training group were matched to subjects in thecontrol group. In study IV practical considerations in relation to workingschedule was the key factor for allocating subjects to the control or traininggroup.
This raises some problems concerning the validity of the studies (alreadymentioned for study I). Concern was mainly on age, job function and trainingbackground as better-trained individuals (or individuals at different ages) wereexpected to react differently to physical test and training. In study III and IVbias due to the distribution of participants and controls was not likely as thedistribution of age, job functions and the amount of leisure time physicalactivity in the control and training group were comparable.
Participants perception of the training programmes
In study I the qualitative analysis of the answers to the questionnaire showedthat 69% perceived their job as less strenuous as a result of training. Additionallythey felt better immediately after training. In all 3 training intervention studiesparticipants reported a positive social effect of training. The indication of apositive psychosocial effect of the intervention might have importantconsequences in a longer perspective, as there is evidence of associationsbetween psychosocial work factors and musculoskeletal disease (Bongers etal. 1993). Lundberg (1999) showed an association between work stress,psychosomatic symptoms and musculoskeletal pain among supermarket cashiers.One hypothesis explaining this is that psychological stress may induce sustainedactivation of small, low-threshold motor units that may lead to degenerative

42
Discussion
processes, damage, and pain. Analysis of short periods of very low muscularelectrical activity (EMG gaps) show that female workers with a high frequencyof EMG gaps seem to have less risk of developing myalgia problems than doworkers with fewer gaps (Lundberg et al. 1999).
There are thus indications that, in the future, it will be necessary to distinguishmore precisely between the expected effect of the physical training (on e.g.strength, endurance and motor control) and the effect of the actual activity(psychosocial effect). Griffiths (1996) points out, in a review article about theadvantages of physical training programmes for employees, that there is somesupport for the hypothesis that physical activity in itself (irrespective of thephysical training effect) has a positive influence on mental health and mood.Thus it seems to be important to evaluate physical training programs byincluding a psychological health point of view, rather than to concentrate in agoal-directed way on increases in the physical capacity.
In study I, III and IV there were mainly positive expressions about thetraining sessions being integrated in the working schedules (on the job training).A Swedish study (Josephson M et al. 1995) where an exercise room had beenfitted out for medical secretaries to be used freely for one hour weekly duringworking hours showed a very low percentage of participation (12% regularlywent to training, in spite of 95% interest in participation). A guilty conscience(or other problems) about leaving work was the most important reason for nottraining! One of the conclusions after interviewing the participants in study I(Pedersen et al. 1998) was that if training is to function in connection withwork, it was important that training was scheduled at fixed times and guided byan instructor.
Implications of the effect of readiness training
A shorter stopping time is supposed to reduce the risk of low-back injuriesbecause a faster reaction can decrease the amount of kinetic energy accumulatedin the trunk before the slowing down of a forward movement. This indicatesthat a training intervention (as in study III and IV) has the potential to modifythe risk of low-back injuries in e.g. nursing personnel exposed to suddentrunk perturbations during patient handling.
The reaction to SL (study II, III, IV) was measured as the reaction to asudden stepwise increase in the loading of the low back with a peak forcearound 75N (study II). This peak force is rather low compared to the expected
43
Discussion
peak forces during SL-situations at work, e.g. accidents during patient hand-ling. The type of reaction to these „real“ situations could therefore be somewhatdifferent from the reactions studied (paper II, III, IV). At present studies arebeing carried out at the National Institute of Occupational Health to investigatethe reactions to sudden trunk loading with very high loads (Essendrop et al.2003). The participants are judo fighters that are used to sudden trunk loadingswith very high impacts.
The observation that a 9 week training intervention without increments inmuscle force generating capacity (MVC and RFD, (study IV)) can modify theresponse to unexpected SL to the extent were response patterns are as efficientas seen during expected perturbations of the trunk has a number of implicationsfor the risk management in the health care sector. Unexpected sudden loadingaccidents during patient handling occur infrequently as episodic events thatare very difficult to prevent. If a training intervention can reduce the risk ofsudden low back trouble due to SL the cost benefit ratio could be favourable.A large-scale epidemiological study is however needed to document theexpected preventive effect of readiness training on the incidence of LBP.
The effect of training – physiological changes
The increase in strength among the cashier workers after 15 weeks of training(study I) can be explained either by adaptive changes within the nervoussystem or by changes within the trained muscles (Sale 1988), or both. Probablythe early increases observed in the start of the training program were due toneuronal changes such as increased activation of prime movers. Later onhypertrophy of the muscle fibres involved in the progressive resistance trainingmay have followed, as in e.g. Andersen and Aagaard (2000) who found ahypertrophy of 16% in type II fibres after 3 months of heavy-load resistancetraining. In study I, though, the training load was not quite as high as in thestudy by Andersen & Aagaard.
In study III and IV the time elapsed until stopping after a SL decreasedsignificantly in the training group compared to the control group. In study IVthere were no differences in strength or maximal rate of force development(not measured in study II) before and after training. Differences in these strengthcharacteristics were not expected in these two studies because the trainingwas focused on development of coordination (not strength). The differencesobserved are therefore likely to be explained mainly by changes in motor

44
Discussion
control aspects. The importance of training induced modulation of motorresponses for the improved mechanical responses found in the studies wasclearly reflected in the EMG analysis - characterized by an increase in theearly parts of the response (up to around 200ms) and a subsequent decreaselater on (study III+IV, figure 13, 14, 15). Readers are referred to the originalpapers for a detailed discussion of the relative changes in EMG levels indifferent time bands shown in figure 14 and 15. Considering an electromechanicaldelay of erector spinae muscle around 130 ms (van Dieen et al. 1991) the shiftto the left of the integrated EMG – with peak changes around 175-200ms –fits nicely with an improved stopping time of around 300 ms after training.
In study III+IV readiness training induced improvements in responsecharacteristics to unexpected SL took place without concomitant decreases inEMG latency. These findings appear to be in discord with results from trainingstudies with low back patients where patients decreased EMG-latency aftertraining rehabilitation (Magnusson et al. 1996). It is, however, conceivable thatlow back patients respond to training in a different manner than normalindividuals and may have pre-training latencies that are longer than in healthycontrols. Part of the discrepancies may however be due to the methodologicaldifficulties in assessing EMG latencies in the presence of high EMG activityprior to the SL event (Skotte et al. 2002). As subjects suffering from low-backdisorders are known to show higher pre-EMG activity than healthy subjects(Pope et al. 2000), it is possible that part of the measured improvement inthese studies (Magnusson et al. 1996; Wilder et al. 1996) in EMG reaction timehas been biased by a simultaneous reduction in pre- EMG activity as a resultof less pain.
Data suggesting that training can modify different components of the stretchreflex has previously been presented by Nielsen et al. (1993) – lookingspecifically at H-reflexes – and Mortimer and Webster (1983) studying the M3component in karate trained subjects. Study III+IV, however, appear to besome of the first to demonstrate that the response to SL can be improved innormal subjects without an increase in pre-activation and associated trunkstiffness (Lavender et al. 1993).
Part of the reflex response to SL seem to be pre-programmed (Magnussonet al. 1996). The widest definition of a motor program is „ a set of musclecommands that is structured before a movement sequence begins, and thatallows the entire sequence to be carried out uninfluenced by peripheral feedback“ (Keele 1968). In accordance with study III & IV Lofthus and Hanson(1981) found a decrease in reaction time with no difference in EMG firing

45
Discussion
latencies after training of quick arm-flexion as reaction to a light stimulus. Onthe bases of the unchanged EMG- latencies they suggested a motor programresponsible for the quick move. Kizuka et al. (1997) showed that the degree oflong latency reflex modulation (M2) directly reflects the individual motorcontrol to perform quick wrist movements. The motor cortex seems to play animportant part in the pre-programming of long latency reflexes. Capaday et al.(1991) also showed evidence for a contribution of the motor cortex to thelong latency reflex of human thumb. Capaday et al. (1991) and Latash et al.(2003) found support for the hypothesis that transcranial magnetic stimulationcan activate cortical neurons interposed in a transcortical long latency loopleading to pre-programmed reactions to perturbations.
The plasticity in motor control and motor systems of the spinal cord andcortex has previously been demonstrated in well-trained athletes and profes-sional dancers, but this study has demonstrated that motor control aspectsmay also be of importance in adapting the individual capacities to meetoccupational demands. Changes in the responses have been documented, butthe exact nature of the changes in the motor control system is difficult todistinguish.
46
Conclusions
• It is possible to develop strength, endurance and coordination of employeesconsiderately by on the job training.
• Training can lead to work being perceived as less stressful.• In study I no effect of training on shoulder complaints could be shown.
An improvement of neck complaints seemed to indicate a positive effectof training, but could also be due to the fact that the training group hadmore neck complaints before the training than the control group.
• Successful randomisation is important in training intervention studies.• Back muscle response to SL can be improved by on the job training in
healthy subjects without an increase in pre-activation and associated trunkstiffness.
• The results indicate a possibility for a training induced modification of therisk of low back injuries in e.g. health care workers exposed to suddentrunk perturbations during patient handling.
A large-scale epidemiological study is needed to document the preventiveeffect of readiness training on the incidence of sudden LBP.
This Ph.D. study was initiated to:1. Investigate the effect of a traditional muscle strength and endurance training
program on shoulder/neck disorders in cashier checkout workers.2. Elucidate the potential possibilities of improving motor control aspects
and the individual adaptive responses to SL among health care workers.
Unfortunately it was not possible to confirm or reject a positive effect ofmuscle strength and endurance training on the development of neck andshoulder complaints among cashier checkout workers. The evidence of theeffectiveness of exercise in management of neck and shoulder pain remainslimited except for fibromyalgia (Mior 2001; NRC Corporation 2001). Thehypothesis that „motor control training can improve neuro-muscular reactionsand spinal protective mechanisms in individuals exposed to SL“ was confirmed,

47
Conclusions
but the practical implication that this kind of training can „reduce the risk ofsudden LBP due to sudden loading accidents“ needs more research before alarge scale exercise based intervention can be implemented.
48
References
Aastrand, P.O. and K. Rodahl. 1986. Textbook of work physiology. Physiologicalbases of exercise. McGRAW-HILL BOOK COMPANY.
Ahlgren, C., K. Waling, F. Kadi, M. Djupsjobacka, L.E. Thornell and G. Sundelin.2001. „Effects on physical performance and pain from three dynamic trainingprograms for women with work-related trapezius myalgia.“ J.Rehabil.Med. 33:162-169.
Andersen, J.L. and P. Aagaard. 2000. „Myosin heavy chain IIX overshoot inhuman skeletal muscle.“ Muscle Nerve. 23:1095-1104.
Arendt-Nielsen, L., T. Graven-Nielsen, H. Svarrer and P. Svensson. 1995.„The influence of low back pain on muscle activity and coordination duringgait: a clinical and experimental study.“ Pain. 64:231-240.
Ariens, G.A., W. van Mechelen, P.M. Bongers, L.M. Bouter and G. van der Wal.2000. „Physical risk factors for neck pain.“ Scand.J.Work Environ.Health. 26:7-19.
Armstrong, T.J., P. Buckle, L.J. Fine, M. Hagberg, B. Jonsson, A. Kilbom, I.A.Kuorinka, B.A. Silverstein, G. Sjogaard and E.R. Viikari-Juntura. 1993. „Aconceptual model for work-related neck and upper-limb musculoskeletaldisorders.“ Scandinavian Journal of Work, Environment and Health. 19:73-84.
Ayoub, M.A. 1990. „Ergonomic deficiencies: I. Pain at work.“ J.Occup.Med.32:52-57.
Bang, M.D. and G.D. Deyle. 2000. „Comparison of supervised exercise withand without manual physical therapy for patients with shoulder impingementsyndrome.“ J.Orthop.Sports Phys.Ther. 30:126-137.
Battié, M.C., S.J. Bigos, L.D. Fisher, T.H. Hansson, M.E. Jones and M.D. Wortley.1989. „Isometric lifting strength as a predictor of industrial back pain reports.“Spine. 14:851-856.
49
References
Berg, H.E., G. Berggren and P.A. Tesch. 1994. „Dynamic neck strength trainingeffect on pain and function.“ Arch.Phys.Med.Rehabil. 75:661-665.
Bernard, B. 1997. Musculoskeletal disorders and workplace factors: A criticalreview of epidemiologic evidence for work-related musculoskeletal disordersof the neck, upper extremity, and low back. U.S. Department of Health andHuman Services, NIOSH. Cincinnati, USA.
Biering-Sørensen, F. 1984. „Physical measurements as risk indicators for low-back trouble over a one-year period.“ Spine. 9:106-119.
Bongers, P.M., C.R. de Winter, M.A. Kompier and V.H. Hildebrandt. 1993.„Psychosocial factors at work and musculoskeletal disease.“ Scand.J.WorkEnviron.Health. 19:297-312.
Brauer, C., J.F. Thomsen, I.P. Loft and S. Mikkelsen. 2003. „Can we rely onretrospective pain assessments?“ Am.J.Epidemiol. 157:552-557.
Bronfort, G., R. Evans, B. Nelson, P.D. Aker, C.H. Goldsmith and H. Vernon.2001. „A randomized clinical trial of exercise and spinal manipulation forpatients with chronic neck pain.“ Spine. 26:788-797.
Capaday, C., R. Forget, R. Fraser and Y. Lamarre. 1991. „Evidence for a con-tribution of the motor cortex to the long-latency stretch reflex of the humanthumb“ J.Physiol. 440:243-255.
Cholewicki, J. Muscle activation in the lumbar spine stability models. Abstracts,XVIIth ISB Congress, Calgary, August 8-13th . 1999.
Cholewicki, J. and S.M. McGill. 1995. „Mechanical stability of the in vivolumbar spine: implications for injury and chronic low back pain.“ ClinicalBiomechanics. 11:1-15.
Cholewicki, J., A.P. Simons and A. Radebold. 2000. „Effects of external trunkloads on lumbar spine stability.“ J.Biomech. 33:1377-1385.
Cohen, J. 1969. Statistical power analysis for the behavioral sciences. AcademicPress. New York.
Cullen, J.W. Phases in cancer control: interventionresearch. In: Hakama M,Beral V, Cullen JW, Parkin V (eds). Evaluating effectiveness of primary
50
References
prevention of cancer. Lyon: International Agency for Research on Cancer.1990. IARC Scientific Publications.
Dyrssen, T., J.Pasikivi and M.Svedenkrans. 1990. Beneficial exercise programmefor office workers with shoulder and neck complaints. In: Berlinguet, L.,Berthelette, D. (Eds.), Work with display units 89. Elsevier, Amsterdam, pp129-138.“.
Ebenbichler, G.R., L.I. Oddsson, J. Kollmitzer and Z. Erim. 2001. „Sensory-motor control of the lower back: implications for rehabilitation.“ Med.Sci.SportsExerc. 33:1889-1898.
Edwards, R.H.T. 1988. „Hypotheses of peripheral and central mechanismsunderling occupational muscle pain and injury.“ Eur Appl Physiol. 57:275-281.
Essendrop, M., B. Schibye and J. Skotte. 2003. „Fast development of highintra-abdominal pressure when a trained participant is exposed to heavy suddentrunk loads.“ Spine (in press).
Estryn-Behar, M., M. Kaminski, E. Peigne, M.F. Maillard, A. Pelletier, C. Bert-hier, M.F. Delaporte, M.C. Paoli and J.M. Leroux. 1990. „Strenuous workingconditions and musculo-skeletal disorders among female hospital workers.“International Archives of Occupational and Environmental health. 62:47-57.
Genaidy, A.M., W. Karwowksi, L. Guo, J. Hidalgo and G. Garbutt. 1992. „Physicaltraining: a tool for increasing work tolerance limits of employees engaged inmanual handling tasks.“ Ergonomics. 35:1081-1102.
Glomsrod, B., J.H. Lonn, M.G. Soukup, K. Bo and S. Larsen. 2001. „“Activeback school“, prophylactic management for low back pain: three-year follow-up of a randomized, controlled trial.“ J.Rehabil.Med. 33:26-30.
Grabiner, M.D., T.J. Koh and A. el Ghazawi. 1992. „Decoupling of bilateralparaspinal excitation in subjects with low back pain.“ Spine. 17:1219-1223.
Grant, K.A. and D.J. Habes. 1995. „An analysis of scanning postures amonggrocery cashiers and its relationship to checkstand design.“ Ergonomics.38:2078-2090.
Griffiths, A. 1996. „ The benefits of employee exercise programmes: a review.“Work & Stress. 10, No. 1:5-23.
51
References
Grønningsäter, H., K. Hytten, G. Skauli, C.C. Christensen and H. Ursin. 1992.„Improved health and coping by physical exersice or cognitive behavioralstress management training in a work invironment.“ Psychol Health. 7:147-163.
Gundewall, B., M. Liljeqvist and T. Hansson. 1993. „Primary prevention ofback symptoms and absence from work. A prospective randomized study amonghospital employees.“ Spine. 18:587-594.
Hagberg, M., L. Punnet, U. Bergquist, A. Härenstam, A. Burdurf, T.S. Kristen-sen, L. Lillienberg, M. Quinn, T.J. Schmidt and H. Westberg. 2001. „Broadeningthe view of exposure assessment. Consensus Report from „Exposure assesmentin epidemiologi and practice“, a conference held in Goteborg, Sweeden, on10-13 june 2001.“ Scandinavian Journal of Work, Environment and Health.27(5):354-357.
Harber, P., L. Pena, G. Bland and J. Beck. 1992. „Upper extremity symptoms insupermarket workers.“ American Journal of Industrial Medicine. 22:873-884.
Hodges, P.W. and C.A. Richardson. 1996. „Inefficient muscular stabilization ofthe lumbar spine associated with low back pain. A motor control evaluation oftransversus abdominis.“ Spine. 21:2640-2650.
Hodges, P.W. and C.A. Richardson. 1999. „Altered trunk muscle recruitmentin people with low back pain with upper limb movement at different speeds.“Arch.Phys.Med.Rehabil. 80:1005-1012.
Jensen, L.D., J.H. Andersen and P. Ryom. 1995. Kroniske lænderygsmerter hossygehjælpere 7491. Arbejdsmiljøfondet. København.
Johansson, H. and P. Sojka. 1991. „Pathophysiological mechanisms involved ingenesis and spread of muscular tension in occupational muscle pain and inchronic musculoskeletal pain syndromes: a hypothesis.“ Med.Hypotheses.35:196-203.
Josephson, M., E.W. Hjelm, M. Hagberg and G. Tjernström. 1995. Faktorersom påvirker deltagenet i fysisk træning under arbejdstid- et studie blandtläkersekreterare. Arbejdsmiljöinstitutet. Undersökningsrapport No. 4.
Jørgensen, K. 1997. „Human trunk extensor muscles. Physiology andergonomics.“ Acta Physiologica Scandinavica. 160:1-58.
52
References
Keele, S.W. 1968. „Movement control in skilled motor performance.“Psychological Bulletin. 70:387-403.
Kilbom, Å. 1988. „Isometric strength and occupational muscle disorders.“European Journal of Applied Physiology and Occupational Physiology. 57:322-326.
Kizuka, T., T. Asami and K. Tanii. 1997. „Relationship between the degree ofinhibited stretch reflex activities of the wrist flexor and reaction time duringquick extension movements“ Electroencephalogr.Clin.Neurophysiol. 105:302-308.
Kourinka, I., B. Jonsson, A. Kilbom, H. Vinterberg, F. Biering-Sørensen, G.Anderssson and K. Jørgensen. 1987. „Nordic Questionares for the analysis ofmusculoskeletal symptoms.“ Applied Ergonomics. 18:233-237.
Kujala, U.M., S. Taimela, T. Viljanen, H. Jutila, J.T. Viitasalo, T. Videman andM.C. Battie. 1996. „Physical loading and performance as predictors of backpain in healthy adults. A 5-year prospective study.“ Eur.J.Appl.PhysiolOccup.Physiol. 73:452-458.
Latash,M.L., F.Danion, and M.Bonnard. 2003. „Effects of transcranial magne-tic stimulation on muscle activation patterns and joint kinematics within a two-joint motor synergy.“ Brain Res. 961:229-242.
Lavender, S.A., W.S. Marras and R.A. Miller. 1993. „The developement ofresponse strategies in preparation for sudden loading to the torso.“ Spine.18:2097-2105.
Leino, P., S. Aro and J. Hasan. 1987. „Trunk muscle function and low backdisorders: a ten-year follow-up study.“ J.Chronic.Dis. 40:289-296.
Levoska, S. and S. Keinanen-Kiukaanniemi. 1993. „Active or passivephysiotherapy for occupational cervicobrachial disorders? A comparison oftwo treatment methods with a 1-year follow-up.“ Arch.Phys.Med.Rehabil.74:425-430.
Lofthus, G.K. and C.J. Hanson. 1981. „Fractionated reaction times andperformance times as a function of practice.“ Am.J.Phys.Med. 60:190-197.
53
References
Lonn, J.H., B. Glomsrod, M.G. Soukup, K. Bo and S. Larsen. 1999. „Activeback school: prophylactic management for low back pain. A randomized,controlled, 1-year follow-up study.“ Spine. 24:865-871.
Lundberg, U. 1999. „Stress responses in low-status jobs and their relationshipto health risks: musculoskeletal disorders.“ Ann.N.Y.Acad.Sci. 896:162-172.
Lundberg, U., I.E. Dohns, B. Melin, L. Sandsjo, G. Palmerud, R. Kadefors, M.Ekstrom and D. Parr. 1999. „Psychophysiological stress responses, muscletension, and neck and shoulder pain among supermarket cashiers.“ Journal ofOccupational Health Psychology. 4, No 3:245-255.
Luoto, M. Heliövaara, H. Hurri and H. Alaranta. 1995. „Static back enduranceand the risk of low-back pain.“ Clinical Biomechanics. 10(6):323-324.
Luoto, S., S. Taimela, H. Hurri, H. Aalto, I. Pyykko and H. Alaranta. 1996.„Psychomotor speed and postural control in chronic low back pain patients Acontrolled follow-up study.“ Spine. 21:2621-2627.
Magnusson, M.L., A. Aleksiev, D.G. Wilder, M.H. Pope, K. Spratt, S.H. Lee,V.K. Goel and J.N. Weinstein. 1996. „Unexpected load and asymmetric post-ure as etiologic factors in low back pain.“ European Spine Journal. 5:23-35.
Manning, D.P., R.G. Mitchell and L.P. Blanchfield. 1984. „Body movementsand events contributing to accidental and nonaccidental back injuries.“ Spine.9:734-739.
Marras, W.S., S.L. Rangarajulu and S.A. Lavender. 1987. „Trunk loading andexpectation.“ Ergonomics. 30:551-562.
Masset, D.F., A.G. Piette and J.B. Malchaire. 1998. „Relation between functionalcharacteristics of the trunk and the occurrence of low back pain. Associatedrisk factors.“ Spine. 23:359-365.
McGill, S.M. 1999. Challinging biomechanical spine models to enhance healthybacks. Abstracts, XVII-th ISB Congress, Calgary, August 8-13-th.
McGill, S.M. 2001. „Low back stability: from formal description to issues forperformance and rehabilitation.“ Exerc.Sport Sci.Rev. 29:26-31.
54
References
Mior, S. 2001. „Exercise in the treatment of chronic pain.“ Clin.J.Pain. 17:S77-S85.
Morris, J.M., D.M. Lucas and B. Bresler. 1961. „Role of the trunk in the stabilityof the spine.“ J Boin Joint Surg.[Am.]. 43:327-351.
Mortimer, J.A. and D.D. Webster. 1983. „Dissociated changes of short- andlong-latency myotatic responses prior to a brisk voluntary movement in normals,in karate experts, and in Parkinsonian patients.“ Adv.Neurol. 39:541-554.
Newton, M., M. Thow, D. Somerville, I. Henderson and G.Waddell. 1993.„Trunk strength testing with iso-machines. Part 2: Experimental evaluation ofthe cybex II back testing system in normal subjects and patients with chroniclow back pain.“ Spine. 18:812-824.
Newton, M. and G. Waddell. 1993. „Trunk strength testing with iso-machines.Part 1: Review of a decade of scientific evidence.“ Spine. 18(7):801-811.
Nielsen, J., C. Crone and H. Hultborn. 1993. „H-reflexes are smaller in dancersfrom The Royal Danish Ballet than in well-trained athletes.“ Eur.J.Appl.PhysiolOccup.Physiol. 66:116-121.
Nordgren, B., R. Schele and K. Linroth. 1980. „Evaluation and prediction ofback pain during military field service.“ Scand.J.Rehabil.Med. 12:1-8.
NRC Corporation. 2001. Musculosketal Disorders and The Workplace. Lowback and upper extremeties. National Research Council (NRC). Institute ofMedicine. Washington D.C. National Academy Press.
Nygård, C.-H., Å. Kilbom, E.W. Hjelm and J. Winkel. 1994. „Life-timeoccupational exposure to heavy work and individual physical capacity.“ Inter-national Journal of Industrial Ergonomics. 14:365-372.
Oddsson, L.I., T. Persson, A.G. Cresswell and A. Thorstensson. 1999.„Interaction between voluntary and postural motor commands during pertur-bed lifting.“ Spine. 24:545-552.
Oldervoll, L.M., M. Ro, J.A. Zwart and S. Svebak. 2001. „Comparison of twophysical exercise programs for the early intervention of pain in the neck,shoulders and lower back in female hospital staff.“ J.Rehabil.Med. 33:156-161.
55
References
Palmer, K., G. Smith, S. Kellingray and C. Cooper. 1999. „Repeatability andvalidity of an upper limb and neck discomfort questionnaire: the utility of thestandardized Nordic questionnaire.“ Occup.Med.(Lond). 49:171-175.
Pope, M.H. 2000. Dr. Malcom Pope’s post-hearing comments concerningchanges to Occupational Safety and Health Administration’s (OSHA’s) proposedrule. Published letter to Ocupational safety of Health, U.S. department ofhealth.
Pope, M.H., A. Aleksiev, N.D. Panagiotacopulos, J.S. Lee, D.G. Wilder, K.Friesen, W. Stielau and V.K. Goel. 2000. „Evaluation of low back musclesurface EMG signals using wavelets.“ Clin Biomech (Bristol., Avon.). 15:567-573.
Pedersen, M.T, S. Mikkelsen and N. Fallentin. 1998.Intensiv fysisk træningsom forebyggelse af besvær i nakke og skuldre ved kassearbejde. Arbejdsmiljø-fondet (forskningsrapport).
Proper, K.I., M. Koning, A.J. van der Beek, V.H. Hildebrandt, R.J. Bosscher,and W. van Mechelen. 2003. „The effectiveness of worksite physical activityprograms on physical activity, physical fitness, and health.“ Clin.J Sport Med.13:106-117.
Radebold, A., J. Cholewicki, M.M. Panjabi and T.C. Patel. 2000. „Muscleresponse pattern to sudden trunk loading in healthy individuals and in patientswith chronic low back pain.“ Spine. 25:947-954.
Radebold, A., J. Cholewicki, G.K. Polzhofer and H.S. Greene. 2001. „Impairedpostural control of the lumbar spine is associated with delayed muscle responsetimes in patients with chronic idiopathic low back pain.“ Spine. 26:724-730.
Sale, D.G. 1988. „Neural adaptation to resistance training.“ Med.Sci.SportsExerc. 20:S135-S145.
Schibye, B. and A.F. Hansen. 1999. Arbejdsfysiologiske kapacitetsmålinger påskraldemænd i relation til alder/anciennitet. 22, 1-38. København, Arbejsmiljø-instituttet. Sikkerhed og sundhed ved affald og genanvendelse.
Silverstein, B.A., T.J. Armstrong, A. Longmate and D. Woody. 1988. „Can in-plant exercise control musculoskeletal symptoms?“ J.Occup.Med. 30:922-927.
56
References
Sjölander, P. and H. Johansson. 1997. „Sensory Endings in Ligaments: ResponseProperties and Effects on Proprioception and Motor control.“ In L.H. Yahia,editor, Ligaments and Ligamentoplasties. Springer Verlag. Berlin Heidelberg.39-83.
Skotte, J.H., N. Fallentin, M.T. Pedersen, M. Essendrop, J. Strøyer and B.Schibye. 2002. „A new set-up for studying sudden loading of the low back.“Journal of Biomechanics. (Submitted).
Smedley, J., P. Egger, C. Cooper and D. Coggon. 1995. „Manual handlingactivities and risk of low back pain in nurses.“ Occupational and EnvironmentalMedicine. 52:160-163.
Solomonow, M., B.H. Zhou, M. Harris, Y. Lu and R.V. Baratta. 1998. „Theligamento-muscular stabilizing system of the spine.“ Spine. 23:2552-2562.
Soukup, M.G., B. Glomsrod, J.H. Lonn, K. Bo and S. Larsen. 1999. „The effectof a Mensendieck exercise program as secondary prophylaxis for recurrentlow back pain. A randomized, controlled trial with 12- month follow-up.“Spine. 24:1585-1591.
Taimela, S., K. Osterman, H. Alaranta, A. Soukka and U.M. Kujala. 1993. „Longpsychomotor reaction time in patients with chronic low-back pain: preliminaryreport.“ Arch.Phys.Med.Rehabil. 74:1161-1164.
Takala, E.-P. and E. Viikari-Juntura. 1991. „Muscle force, endurance and neck-shoulder symptoms of sedentary workers. An experimental study on bankcashiers with and without symptoms..“ International Journal of IndustrialErgonomics. 7:123-132.
Takala, E.-P. and E. Viikari-Juntura. 1997. Muskeli II 8: Healthy and functionalcapacity of the musculoskeletal system: Methods of testing. Books of abstracts.IEA 97.
Takala, E.-P., E. Viikari-Juntura and E.-M. Tynkkynen. 1994. „Does groupgymnastics at the workplace help in neck pain?“ Scandinavian Journal of Re-habilitation Medicine. 26:17-20.
Thomas, J.R., W. Salazar and D.M. Landers. 1991. „What is missing in p lessthan .05? Effect size.“ Res.Q.Exerc.Sport. 62:344-348.

57
References
Townsend, H., F.W. Jobe, M. Pink and J. Perry. 1991. „Electromyographic analysisof the glenohumeral muscles during a baseball rehabilitation program.“Am.J.Sports Med. 19:264-272.
van Dieen, J.H., C.E. Thissen, A.J. van de Ven and H.M. Toussaint. 1991. „Theelectro-mechanical delay of the erector spinae muscle: influence of rate offorce development, fatigue and electrode location.“ Eur.J.Appl.PhysiolOccup.Physiol. 63:216-222.
Viikari-Juntura, E., R. Martikainen, R. Luukkonen, P. Mutanen, E.P. Takala andH. Riihimaki. 2001. „Longitudinal study on work related and individual riskfactors affecting radiating neck pain.“ Occup.Environ.Med. 58:345-352.
Westgaard, R.H. and J. Winkel. 1996. „Guidelines for occupationalmusculoskeletal load as a basis for intervention: a critical review.“ AppliedErgonomics. 27:79-88.
Westgaard, R.H. and J. Winkel. 1997. „Review article. Ergonomic interventionresearch for improved musculoskeletal health: a critical review.“ InternationalJournal of Industrial Ergonomics. 20:463-500.
Wilder, D.G., A.R. Aleksiev, M.L. Magnusson, M.H. Pope, K.F. Spratt andV.K. Goel. 1996. „Muscular response to sudden load.“ Spine. 21:2628-2639.

58
Individual physiological- and psychological characteristics may play a majorrole in the development of work related musculoskeletal disorders. The aimof this thesis was to provide new insight into the preventive effect of atraditional muscle strength and endurance training program on shoulder/neckdisorders in cashier checkout workers and to elucidate the potential possibilitiesof improving motor control aspects and the individual adaptive responses tosudden back loading among health care workers. An improved reaction tosudden trunk loading is supposed to reduce the risk of work related low backpain
Study I was a physical training intervention study among cashier checkoutworkers with measurements of neck and shoulder complaints before and afterthe intervention. Study II was a method study focusing on recording thereactions to sudden trunk loading. Study III and IV were training interventionstudies aiming at improving the reaction to sudden trunk loading among untrainedworkers at the National Institute of Occupational Health (study III) and amonghealth care workers (study IV). The three training studies were all controlledstudies.
It was possible to develop strength and endurance considerately by on thejob training among cashier checkout workers, in addition training resulted inwork being perceived as less stressful (study I). In this study no effect oftraining on shoulder complaints could be shown. The improvement of neckcomplaints indicated a positive effect of training, but could also be due a non-successful randomisation explained mainly by dropouts in the training group,especially among participants without neck-complaints. In study III and IVparticipants improved their reaction to sudden trunk loading. The results indicatea potential for a training induced modification of the risk of low back injuriesin e.g. health care workers exposed to sudden trunk perturbations during pa-tient handling. A large-scale epidemiological study is needed to document thepreventive effect of „readiness“-training on the incidence sudden low backpain.
Summary

59
I de senere år er der kommet øget fokus på sammenhængen mellem individu-elle fysiske- og psykosociale faktorer og udviklingen af arbejdsrelateret mus-koloskeletalt besvær. Formålet med dette ph.d.-projekt var dels at undersøgehelbredseffekten af styrke- og muskeludholdenhedstræning på udviklingen afnakke- og skulderbesvær hos kasseassistenter dels at undersøge om specifiktræning kunne forbedre evnen til at reagere på pludselige rygbelastende hæn-delser. En forbedret evne til at reagere på pludselige rygbelastninger forven-tes at kunne reducere udviklingen af arbejdsrelateret lænderygbesvær.
Studie I var et interventionsstudie med styrke- og udholdenhedstræning afkasseassistenter og målinger af nakke- og skulderbesvær før og efter trænings-perioden. Studie II var et metodestudie som forberedelse til studie III og IV,der begge var træningsinterventionsstudier rettet mod at forbedre evnen til atreagere på pludselige rygbelastninger. Studie III blev udført blandt utrænedeforskere og kontorpersonale på Arbejdsmiljøinstituttet. Studie IV blev udførtblandt sundhedspersonale på Vordingborg Sygehus.
Det var muligt at udvikle muskelstyrke og -udholdenhed betydeligt hoskasseassistenter i forbindelse med træning på jobbet. Træningen medførte des-uden at kassearbejdet føltes mindre anstrengende end før interventionen. Idette studie blev der ikke fundet nogen effekt af træning på skulderbesvær.Den målte forbedring i nakkebesvær indikerer en positiv træningseffekt, menkan også være forårsaget af problemer med randomisering af trænings ogkontrolgruppen (hovedsageligt forårsaget af at frafaldet i træningsgruppen varstørst blandt deltagere uden nakkebesvær). I studie III og IV blev reaktion påpludselige rygbelastninger forbedret ved træning på jobbet. Resultaterne anty-der et potentiale for en træningsinduceret reduktion i risikoen for akut lænde-rygbesvær forårsaget af pludselig rygbelastning. Dokumentation for en præ-ventiv effekt af „parathedstræning“ på incidensen af lænderygbesvær forud-sætter dog en egentlig epidemiologisk opfølgningsundersøgelse.
Dansk resumé