vitamines et oligo-éléments
TRANSCRIPT

Vitamines et oligo-éléments
ULB – 2011/2012
Certificat de Gastro-entérologie

Vitamins and trace elements
Substances not synthesized by the
organism (or in very small quantities)
but essential for its functioning


Vitamin B1 (thiamine)
• Vitamin B1 (thiamine) is a cofactor for
enzymes involved in AA and CH
metabolism
• Sources: Yeast, pork, rice, legumes
• Absorption in the duodenum
• Deficiency:
– Alcoholics
– Anorexia nervosa
– Bariatric surgery (RYBP)

Clinical spectrum of B1 deficiency
• Beri-beri (malnutrition, bariatric surgery)
• Peripheral neuropathy with sensory and motor
impairments
• Cardiomyopathy, congestive heart failure, tachycardia
• Wernicke-Korsakoff syndrome (alcoholics)
• Wernicke’s encephalopathy: acute form with
nystagmus, opthalmoplegia, ataxia, confusion
• Korsakoff syndrome: chronic condition with short-term
memory loss and confabulation
Galvin et al, Eur J Neurol 2010
Aasheim et al, Ann Surg 2008

Christoforidis et al, AJR 2000

Management of B1 deficiency
• Diagnosis based on clinical presentation
• Lab tests:
• Blood thiamine concentration
• Erythrocyte thiamine transketolase
• Lactate/puryvate ratio (nl <10/1)
• MRI for Wernicke encephalopathy
• IV administration of 100mg thiamine (Vitamine B1
Sterop® 100mg) for 7-14 days followed by per
mouth maintenance therapy (Benerva ® 300mg)

Vitamin B3 (Niacin)
• Pellagra (“raw skin”): photosensitive pigmented
dermatitis, diarrhea and dementia
• Epidemic amongst the corn eating population of SE
USA in the beginning of the 20th century
• Nowadays:
– alcoholics, anorexia nervosa, bariatric surgery, dietary
deficiencies in some regions in China, India, Africa
– Carcinoid syndrome (abnormal metabolism of
tryptophane)
– Prolonged use of isoniazid
• Source: yeast, liver, cereals, seeds

Management of vitamin B3 deficiency
• Ucemine PP ® (Nicotinamide 100mg tablets)
initial dosage: 500-1000mg/day

Vitamin B12 (cobalamin)
• Vitamin B12 (cobalamin) is a cofactor
and coenzyme
– DNA synthesis
– Methionine synthesis from homocysteine
• Animal products (fish, meat, eggs, milk
and milk products, poultry, fortified
breakfast cereals)

• 6-9 µg / day
• According to different diets
Vitamin B12 and food intake
Vegans
0.4 µg
+ milk and
eggs
2.4 µg
+ fish
5 µg
omnivores
7.2 µg

Passive absorption 1-20%
1. Food intake 2. Gastric acid to liberate Cb from binding proteins 3. Pancreatic protease to free Cb from binding to R-factors 4. Secretion of IF from gastric parietal cells 5. Cb-IF receptors in the ileum

Causes of Vitamin B12 deficiency
Dali-Youcef et al, Q J Med 2009

Pernicious anaemia
• B12 malabsorption because of loss of IF secretion
• Prevalence: 2% in the general population • More frequent in the elderly and in
patients with type I diabetes • Characterized by
– Atrophic gastritis – Achlorydria – Hypergastrinemia – IF antibodies – Abnormal schilling test

Food-cobalamin malabsorption
• Decrease in gastric secretion and acidity inability to release cobalamin
from food
• Normal absorption of crystalline free cobalamin
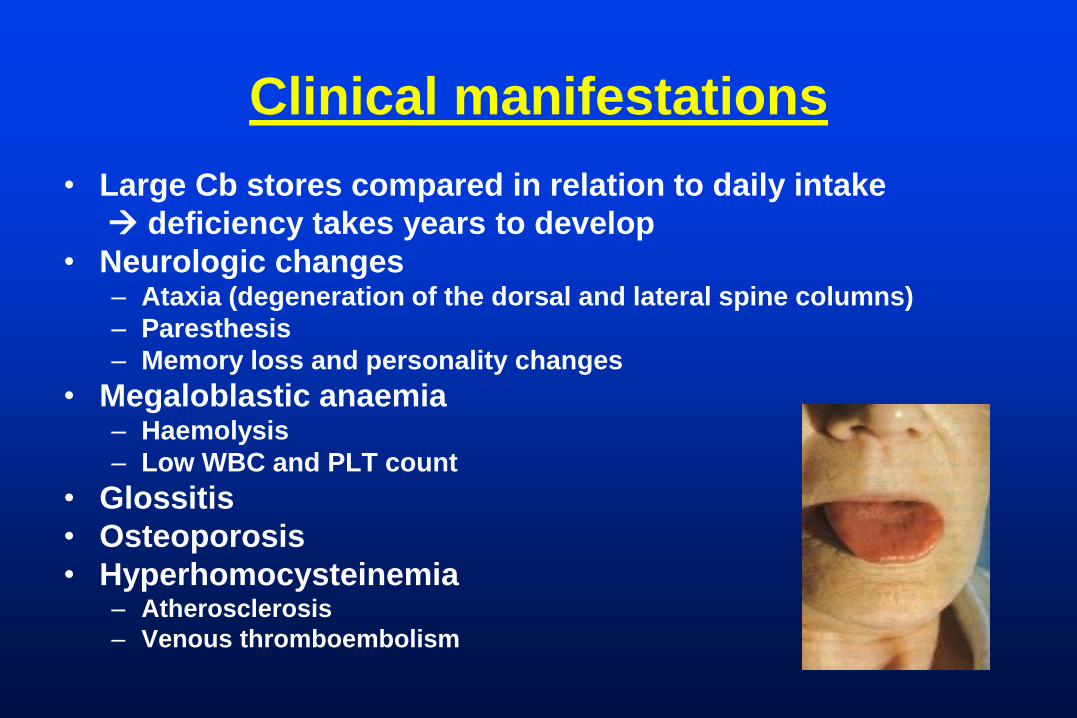
Clinical manifestations
• Large Cb stores compared in relation to daily intake
deficiency takes years to develop
• Neurologic changes – Ataxia (degeneration of the dorsal and lateral spine columns)
– Paresthesis
– Memory loss and personality changes
• Megaloblastic anaemia – Haemolysis
– Low WBC and PLT count
• Glossitis
• Osteoporosis
• Hyperhomocysteinemia – Atherosclerosis
– Venous thromboembolism

Diagnosis
• Lab tests
– Macrocytosis (! Iron deficiency =normal volume)
– IF antibodies (Sn: 50-84%, Sp: 95%)
– High homocysteine levels
• Schilling test
• Upper GI endoscopy
– Atrophic gastritis

B12 supplementation • Parenteral cobalamin (IM)
– Pernicious anemia, malabsorption, ileal resection, gastrectomy
– Dosage: 1mg/day for 7 days, 1mg/week for 4 weeks, 1mg/month
– Vitamine B12 Sterop® (cyanocobalamine, 1 mg/1ml vials)
– Hepavit® (hydroxycyanocobolamine, 5 mg/2ml)
• Oral cobalamin – High dose (1-2 mg/day) in maintenance therapy
• Intranasal (nasal spray) and sublingual forms – Under investigation

Response to B12 supplementation
• After onset of treatment:
– 1-2 days: Hemolysis improves
– 4 days: Hypokaliemia because increase in uptake
– 4 days: Reticulocytosis and decrease in RBC mean
volume
– 10 days: Rise in Hb
– 8 week: Normalisation of Hb
– 3 months: Improvement of neurological symptoms with
maximum at 6-12 months

Folic acid (B9)
• Source: liver, green vegetables, yeast
• Deficiency:
– Alcoholism (inhibition of absorption)
– Poor diet
– Patients with increased requirements
(pregnancy, chronic haemolytic anaemia,
exfoliative skin disease, chemotherapy)
– Patients taking drugs interfering with folate
metabolism (Daraprim, methotrexate)

Acide folique B9
• B9 synthèse méthionine (< homocystéine) et
bases puriques
• Carence en B9 ralentissement des mitoses
– anémie (mégaloblastique)
– troubles immunité
– hyperhomocystéinémie
• risques cardio-vasculaires
• En cas de grossesse :
– défaut de fermeture du tube neural
– retard de croissance intra-utéro

Folic acid deficiency
• Symptoms: – Megaloblastic anemia
– No neurological changes (only in associated B12 deficiency)
• Deficiency can occur within a few months after intake is diminished
• Dosage: – Plasma concentration of folate
• Supplementation: – Oral folic acid (Folavit ® 4mg tablets)

Vitamin C (ascorbic acid)
• Oldest vitamin deficiency described (scurvy)
• Sources: Citrus fruits, tomatoes, strawberries,
spinach
• Strong antioxidant
– Fatty acid transport
– Collagen synthesis
– Neurotrasnmitters
– Prostaglandin metabolism
• Deficiency:
– Severe malnutrition
– Alcohol and drug abusers

Vitamin C deficiency
• Symptoms:
– Ecchymoses
– Bleeding gums
– Impaired wound healing
– Hyperkeratosis
• Supplementation:
– 300-1000 mg daily for 1 month (Redoxon® 500mg)
• Cancer prevention? Not clearly established in RCT

Vitamin D
• Vitamin D is essential in bone
metabolism
• Possible role in decreasing the risk
of other diseases
– Infectious and autoimmune diseases
– Cancers
– Cardio-vascular diseases

Vitamine D
Sources
Alimentation D2 (ergocalciferol) végétaux
D3 (cholecalciferol) produits
d’origine animale
Soleil/peau D3 (< 7-dehydrocholestérol)
Métabolisme
D3 Foie rein (1,25 dihydroxycholecalciferol)

Sources of Vitamin D
• Sunlight
– 5-10 min exposure to sunlight (3000 IU D3)
• Diet
– Salmon (600-1000 IU D3/100 gr)
– Cod liver oil (400-1000 IU D3/tps)
– Egg yolk (20 IU D3)
– Shitake mushrooms (100 IU D3/100 gr)
• Dietary supplements

Holick, NEJM 2007; 357: 266-281

Vitamin D deficiency
• Normal range 20-100 ng/ml • Preferred range 30-60 ng/ml • Groups at risk:
– Elderly – Infants, children and adolescents – Subjects living in higher latitudes – Subjects with dark skin – European countries (no food fortification) – Malabsorption (chronic pancreatitis, IBD, celiac
disease) – Chronic liver disease – Chronic kidney failure – Bariatric surgery

In Belgium
• Recent cross-sectional survey in 401 subjects (40-60 years) living in Belgium for minimum 40 years
• Four different ethnic backgrounds • Autochthonous Belgian
• Moroccan
• Turkish
• Congolese
• 77% (n=306) subjects had vitamin D levels below 20 ng/mL
• Immigrants seemed to be at greater risk
Moreno-Reyes et al, Eur J Nutr 2009; 48: 31-7
Clinical manifestations
• Osteoporosis and bone fractures
• Muscle weakness with increased risk of falls
• Other actions:
• Immunomodulation
• Cell proliferation
• Cardiovascular function

Guidelines to prevent and treat
vitamin D deficiency Prevention Deficiency
Adults
•Inadequate skin
exposure
•Aging (> 50 y)
800-1000 IU Vita D3/day
Or
50,000 IU every 2w or mo
50,000 IU every w
for 8 weeks
Repeat if
necessary
Malabsorption syndroms 50,000 IU every w 50,000 IU every day
or every 2 days
Holick, NEJM 2007; 357: 266-281
One vial of colécalciferol (D3) (D-Cure) 25,000 UI
Drops 10 ml, 2400 IU/ml/30 drops
Is there a need for vitamin D fortification in food?
In case of renal disease 1,25-dihydroxyD3 (1-alpha Leo® 2µgr/day)


Vitamine E
Rôle anti-oxydant





Trace elements
• Minerals that are required in amounts
between 1 to 100 mg/day
• Found in human diet and essential for normal
health and function
• Chromium, copper, fluoride, iodine, iron,
manganese, selenium, zinc

Iron
• Sources:
– Heme iron: meat, poultry, fish
– Non-heme iron: vegetable, fruit,
iron-fortified cereals
• Deficiency
– Microcytic anemia: weakness, headache,
irritability, tachycardia, exercise intolerance


Management
• Oral iron therapy: simple, inexpensive
– First line therapy
• Parenteral iron therapy: complex, expensive, serious adverse effects
– In case of severe intolerance to oral iron therapy or malabsorption
• Blood transfusion
– Active bleeding with hemodynamic instability or end-organ ischemia

Oral iron therapy
• Absorption in the duodenum and proximal jejunum
• In between meals (phosphates, phytates and tannates in food
bind the iron and impair its absorption)
• Avoid concomitant use of anti-acids
• Recommended dose: 150-200mg/day of elemental iron
• Ferrous sulfate (Fe++): better absorption in acidic milieu
– Fero-Grad 500® (105mg Fe++) with ascorbic acid
• Ferric salts (Fe+++):
– Ferricure ®(150 mg Fe+++) tablet or liquid preparation

Response to oral therapy
• Side effects: abdominal discomfort,
nausea/vomiting, diarrhea/constipation (20%)
– Related to the amount ingested
• Within few days of therapy: improved sense of
well-being
• 7-10 days: reticulosis
• 3 weeks: Hb rise of 2 gr/dl
• Normalisation of Hb within 6-8 weeks

Failure to respond to oral therapy
• Coexisting diseases interfering with marrow response – Infection
– Inflammatory disorders
– Malignancy
– Other vitamin deficiency (B12 or folic acid)
• Incorrect diagnosis – Thalassemia
– Lead poisoning
– Copper deficiency
• Lack of compliance
• Lack of absorption – Enteric coated product
– Coeliac disease
– Other medications (anti-acids, tetracycline)
• Continued blood loss

Parenteral iron therapy
• Intravenous administration if major intolerance to
oral forms or malabsorption (IBD, dialysis patients...)
• Fercayl® (Iron dextran) IM (high rate of side effects-
local reaction to anaphylactic shock)
• Venofer® (Iron sucrose) IV
– Vials of 5ml (100mg Fe+++)
– 200 mg = 1 blood unit
– 200 mg 3x/week (maximum dosage)
– Test dose

Zinc
• Usual intake: 4-14 mg/day
• Cofactor in more than 70 enzyme systems
• Important for growth, tissue repair, wound
healing and immune response
• Sources: animal products (meat, seafood, milk)
• Absorbed in the small bowel
Zinc deficiency
• Aetiology
– Dietary zinc depletion (children and adolescents in
developing countries)
– Inherited defect in zinc absorption
– Crohn’s disease
– Cystic fibrosis
– Sickle cell disease
– Liver disease
– Bariatric surgery

Clinical manifestations
• Depressed immunity
• Impaired taste and smell
• Dermatitis (acrodermatitis enteropathica)
• Onset of night blindness
• Alopecia
• Decreased spermatogenesis

Zinc supplementation
• Zinc sulfate tablets 150 mg /day
• Zinc inhibits intestinal absorption of copper! (zinc
toxicity can lead to copper deficiency)
– Preparations containing zinc and copper
Parenteral Nutrition
• Fortification with vitamin complex (Cernevit®) – Thiamine (B1), riboflavine (B2), pyridoxine
(B6), biotin, nicotinamide (B3), panthotenic acid (B5), folic acid, B12,
– A,D, E – No vitamin K (complementary 1 vial/w)
• Trace elements complex (Nonan Novum®) – Iron, zinc, copper, cobalt, manganese, fluoride,
iodine, selenium, molybdene – In case of digestive fluid losses (fistula,
diarrhea, malabsorption) add Zinc and selenium

Gastric restriction and malabsorption
Frequent surgical treatment of obesity
Post-operative
complications
• Malabsorption
• Dumping syndrome
• Vitamin deficiency
Bariatric surgery: RYGB

Mechanisms of nutritional deficiencies
• Insufficient intake
• Decrease in gastric acid secretion (B12 and
iron)
• Duodenal by-pass (main absorption site for
calcium, iron and B1)
• Asynergia between bolus and bilio-
pancreatic secretions (A, D, E, K)
Most frequent deficiencies: iron, B1, folate,
vit D and calcium
Poitou Bernet et al, Diabetes and Metabolism 2007
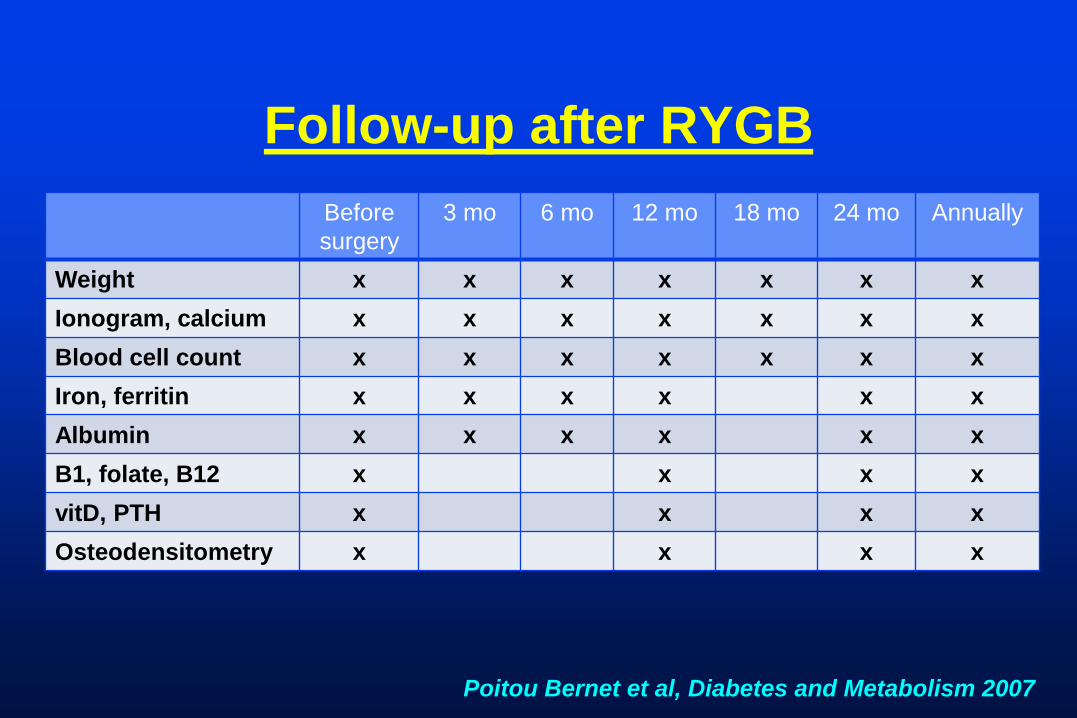
Before
surgery
3 mo 6 mo 12 mo 18 mo 24 mo Annually
Weight x x x x x x x
Ionogram, calcium x x x x x x x
Blood cell count x x x x x x x
Iron, ferritin x x x x x x
Albumin x x x x x x
B1, folate, B12 x x x x
vitD, PTH x x x x
Osteodensitometry x x x x
Follow-up after RYGB
Poitou Bernet et al, Diabetes and Metabolism 2007

Prevention
• No RCT
• Multivitamin supplements
• Protein intake: 0.8 gr/kg/day
• Supplements of Calcium (1200-1500 mg/day) and
vitamin D (400 UI/day)
• Iron supplements (50-100 mg/day)
• In case of severe or prolonged hair loss: Zinc
• Supplementation on demand according to follow-up
Poitou Bernet et al, Diabetes and Metabolism 2007

Oligo-éléments
• Manganèse :
– carence : rare
– toxicité (en cas de cholestase) : dépôt dans le
cerveau avec pseudo-Parkinson
• Sélénium :
– anti-oxydant
– immunité
• Cuivre : carence : anémie, leucopénie, douleurs
osseuses
• Chrome : carence : résistance à l’insuline

Vitamines Toxicité
Vitamine A hépatopathie
Vitamine D hypercalcémie
B3 (PP) hépatopathie
vasodilatation
B6 (pyridoxine) neuropathie à très forte dose
