vascular phase vasodilatation and separation of the cells of the vascular endothelium. leucotrienes...
TRANSCRIPT

Vascular Phase
• Vasodilatation and separation of the cells of the vascular endothelium. Leucotrienes appear to mediate this response.
• Capillaries are damaged and become permeable to plasma proteins causing focal edema (swelling).
• Itch and heat and soreness and pain, mediated by several powerful endogenous agents.

Function Mediators
Increased vascular permeability Histamine, serotonin, bradykinin,C3a, C5a, PGE2, LTC4,
of small blood vessels LTD4, prostacyclins, activated Hagemanfactor, high-molecular-weight kininogenfragments, fibrinopeptides
Vasoconstriction TXA2, LTB4, LTC4, LTD4, C5a, N-formylpeptides
Smooth muscle contraction C3a, C5a, histamine, LTB4, LTC4, LTD4,TXA2, serotonin, PAF, bradykinin
Increased endothelial cell IL-1, TNF-, MCP, endotoxin, LTB4
stickiness
Mast cell degranulation C5a, C3a
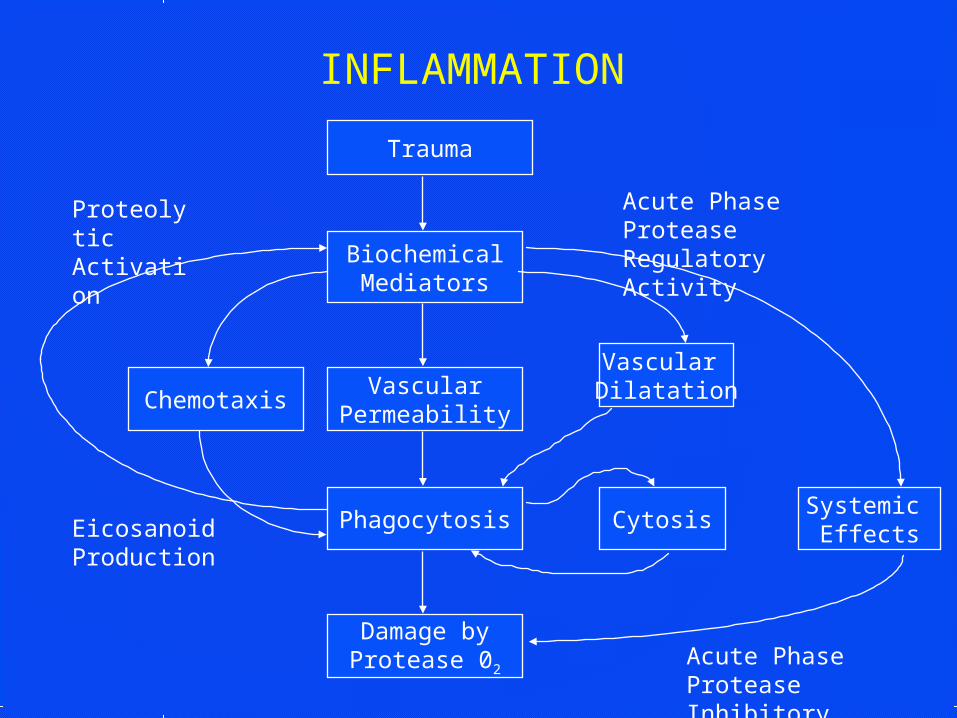
INFLAMMATION
Trauma
Chemotaxis
Damage byProtease 02
BiochemicalMediators
Vascular Dilatation
Cytosis
VascularPermeability
Systemic Effects
Phagocytosis
Acute Phase ProteaseInhibitory Activity
EicosanoidProduction
ProteolyticActivation
Acute Phase ProteaseRegulatory Activity

Cellular Phase
• Swelling of damaged vascular endothelium and adhesion of platelets.
• CHEMOTAXIS-- leukocytes functioning anaerobically infiltrate and release lysosomes.
• Sludging of blood (hyperemia, redness) lack of adequate microcirculation.
• Decrease O2 tension and hypoxia, tissue necrosis ensues.

Function Mediators
Phagocytes
Stem cell proliferation IL-3, G-CSF, GM-CSF, M-CSF
Recruitment from bone marrow CSFs, IL-1
Adherence/aggregation iC3b, IgG, fibronectin, lectins
Chemotaxis C5a, LTB4, IL-8 and other chemokines,PAF, histamine (for eosinophils), laminin, N-formyl peptides, collagen fragments,lymphocyte-derived chemotactic factor,fibrinopeptides
Lysosomal granule release C5a, IL-8, PAF, most chemoattractants,phagocytosis

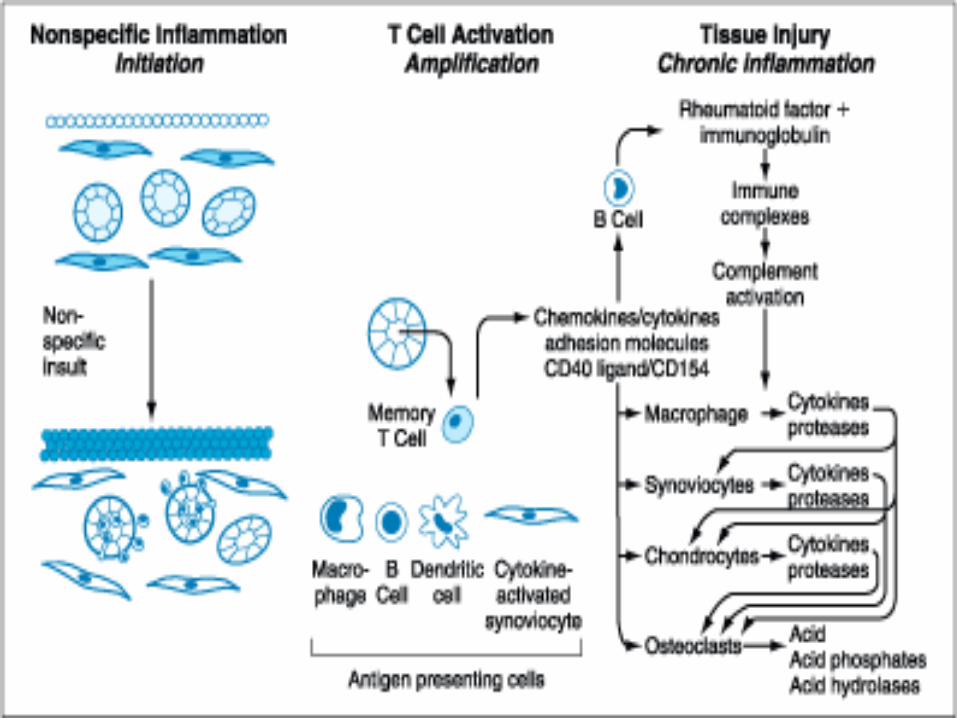
ARTHRITIS
• Rheumatoid arthritis is an inflammatory condition.
• Acute and Chronic phases of inflammation.
• Autoimmune in nature.– Ab’s produced against IgG– (The defective IgG molecules have
changes in microheterogeneity)

Adverse Effects of NSAIDs
• Gastrointestinal tract: gastric irritation, peptic ulcers, bleeding, perforation
• Kidney: decreased renal blood flow, decreased creatinine clearance rarely interstitial nephritis or nephrotic syndrome
• CNS: headaches, confusion, tinnitus, aseptic meningitis (rare)
• Hematopoietic system: bleeding, inhibited platelet adhesion (irreversible effect with aspirin persisting 10-12 days)
Page et al. 1997

ADME/Side Effects of NSAIDs• The T1/2 of the different NSAIDs vary from short, less
than 1 hr., to longer than 12 hrs.• NSAIDs are heavily bound, 60%-90%, to plasma
proteins.• NSAIDs are metabolized in the liver in a fashion
similar to ASA.
• Virtually all NSAIDs can cause dyspepsia and GI toxicity including ulceration.
• All except the nonacetylated salycilates can effect bleeding time. This is reversible except for aspirin which lasts the life of the platelet.

ADME/Side Effects Continued
• NSAIDs decrease renal blood flow, cause fluid retention, and may cause renal failure in some patients, particularly the elderly.
• NSAIDs can cause central-nervous-system (CNS) effects such as dizziness, anxiety, drowsiness, and confusion; these symptoms may occur initially and disappear with further use.
• NSAIDs frequently cause small increases in hepatic enzyme activity, but life-threatening hepatic toxicity is rare.

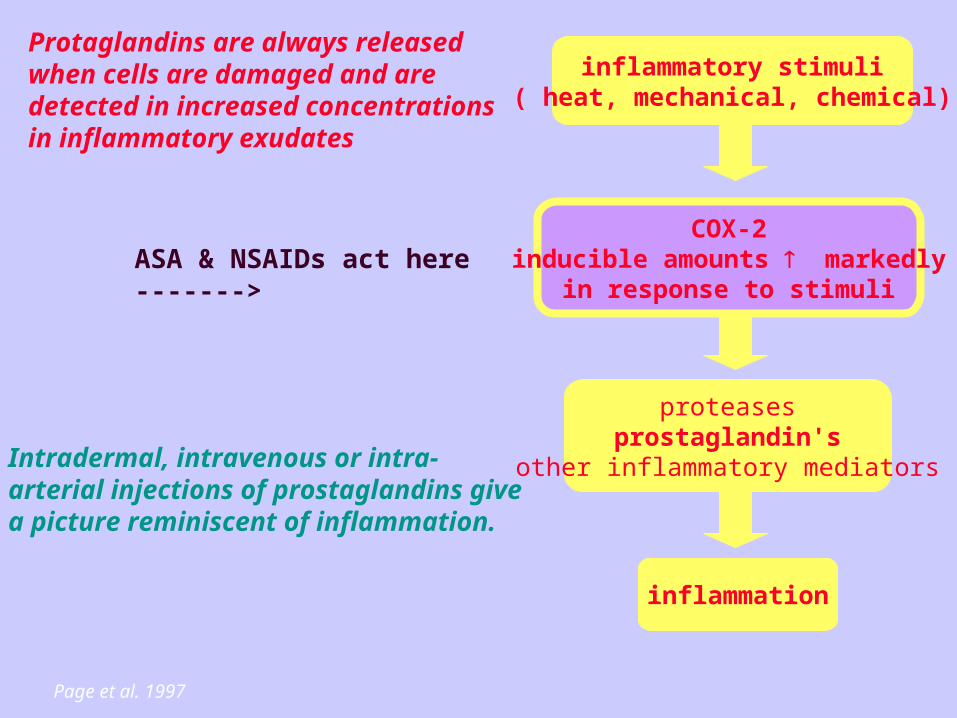
inflammatory stimuli( heat, mechanical, chemical)
COX-2inducible amounts markedly
in response to stimuli
proteasesprostaglandin's
other inflammatory mediators
inflammation
Page et al. 1997
Protaglandins are always released when cells are damaged and are detected in increased concentrations in inflammatory exudates
ASA & NSAIDs act here ------->
Intradermal, intravenous or intra-arterial injections of prostaglandins give a picture reminiscent of inflammation.

arachidonic acid
lipoxygenase cyclooxygenase
leukotrienes prostaglandinsthromboxane
phagocytemobilization,changes invascular permeability,inflammation
inflammation
12

DMARDs• PENICILLAMINE (Depen, Cuprimine).• SULFASALAZINE (Azuifidine).• GOLD - Gold salts. Gold sodium thiomalate (Myochrysine) and
aurothioglucose (Solganal) injectable; Auranofin, oral.• METHOTREXATE (Rheumatrex).• HYDROXYCHLOROQUINE (Plaquenil).• AZATHIOPRINE (Imuran).• CYCLOPHOSPHAMIDE (Cytoxan)
• New treatment models for rheumatoid arthritis suggests that more aggressive approaches earlier in treatment can avoid or slow the progress of the disease.

PENICILLAMINE• Penicillamine is effective in acute, severe rheumatoid
arthritis in most patients able to tolerate the drug.
• Reductions in joint pain, edema, and stiffness are seen.
• Inhibits T-cell function and antigen presentation.
• Modification of trace metal metabolism and an effect on macromolecules could contribute to its efficacy in rheumatoid arthritis.
• It is readily absorbed from the gastrointestinal tract and is rapidly excreted in the urine, largely as the intact molecule.
• Toxicities include Aplastic anemia, thrombocytopenia, obliterative bronchitis, polymyositis.

METHOTREXATE• This antimetabolite drug, when administered in low
doses, is effective in the treatment of rheumatoid arthritis.
• Decreases PMN chemotaxis, alters DNA synthesis.
• At low doses methotrexate appears to be acting more as an antiinflammatory agent than as an antimetabolite.
• Dose levels much be watched because of toxicity as the drug accumulates. Toxicity includes, hepatic fibrosis, acute interstitial pneumonia, bone marrow suppression.
• Toxicity threshold varies form organ to organ with bone marrow and GI the most susceptible.

Azathioprine and Cyclophosphamide
• Cyclophosphamide and azathioprine, can reduce arthritic signs and symptoms in a significant proportion of patients able to tolerate the therapy.
• A reduction in new joint erosions were found in patients receiving these agents.
• Interferes with DNA synthesis. Inhibits lymphocyte proliferation.
• Side effects associated with the cytostatic-cytotoxic drugs severely limit the use of such drugs.
• Twofold increase in non-Hodgkin's lymphoma.

HYDROXYCHLOROQUINE (Antimalarials)
• The aminoquinolines act on polymorphonuclear leukocyte function which may be the key to their antiinflammatory activity.
• The 4-aminoquinolines may “stabilize” lysosomal membranes reducing the release of destructive enzymes in the joints.
• The antimalarials are useful for the treatment of rheumatoid disease showing long term antirheumatic effects.

GOLD SALTS
• Gold salts suppress the function of t cells. Inhibit PMN function and macrophage activation.
• Gold therapy suppresses the increased phagocytic activity that occurs in patients with rheumatoid arthritis.
• Aurothiomalate and aurothioglucose are given by injection (i.m.) whereas aurafin is orally active.
• Aurothiomalate reduces the numbers of circulating lymphocytes and aurafin inhibits the release of PGE2
from synovial cells and the release of LTB4 and LTC4 from polymorphonuclear leukocytes.
Gold Continued
• Gold is difficult to tolerate and can produce significant toxicity. Serious reactions occur in 5% of patients.
• The most frequent ADRs with the oral agent aurafin are-diarrhea, abdominal pain, neusea, anorexia. With all agents pruritus and dermatitis.
• The therapeutic efficacy of gold salts is delayed 4-12 weeks after initiation of therapy.

Recent Progress in Arthritis Therapy
• New treatment models for rheumatoid arthritis suggests that more aggressive approaches earlier in treatment can avoid or slow progress of the disease.
• A new class of drugs called leumedins are identified that could block the destructive inflammation in diseases such as rheumatoid arthritis.
• Recent studies find that the body uses IL-1ra to turn off the excessive inflammation typical of some forms of arthritis.

GOUT
• Gout is an inflammatory reaction to crystals of sodium urate.
• Sodium urate is the end product of purine metabolism.
• Not everybody who is hyperuric has gout but those with gout are hyperuric.
• 3-6.5 mg % in blood - gout pop 6-14 mg %.• Blood concentration of 6.7 mg % is a saturated
solution. Less soluble in low pH(e.g. joints).

Two Phases of Gout Treatment
• Treatment of the acute attacks where quick relief from painful inflammation is highly desirable.
• Long-term lowering of plasma urate concentrations.
• For acute attacks: Indomethacin, Colchicine.• Treatment of chronic hyperuricemia:
Probenecid, Allopurinol, Sulfinpyrazone
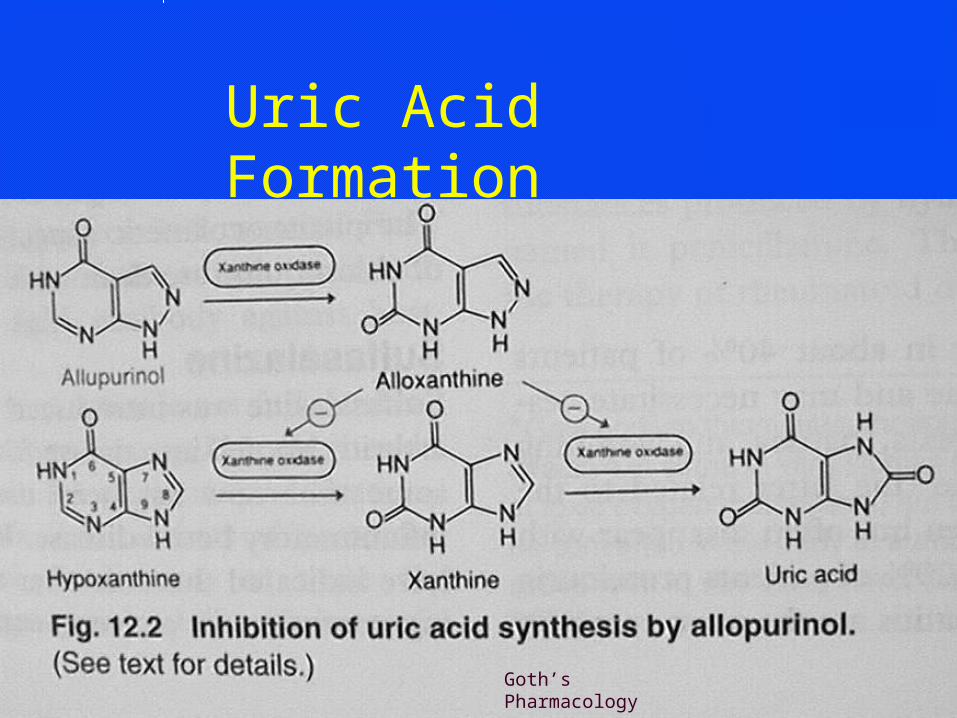
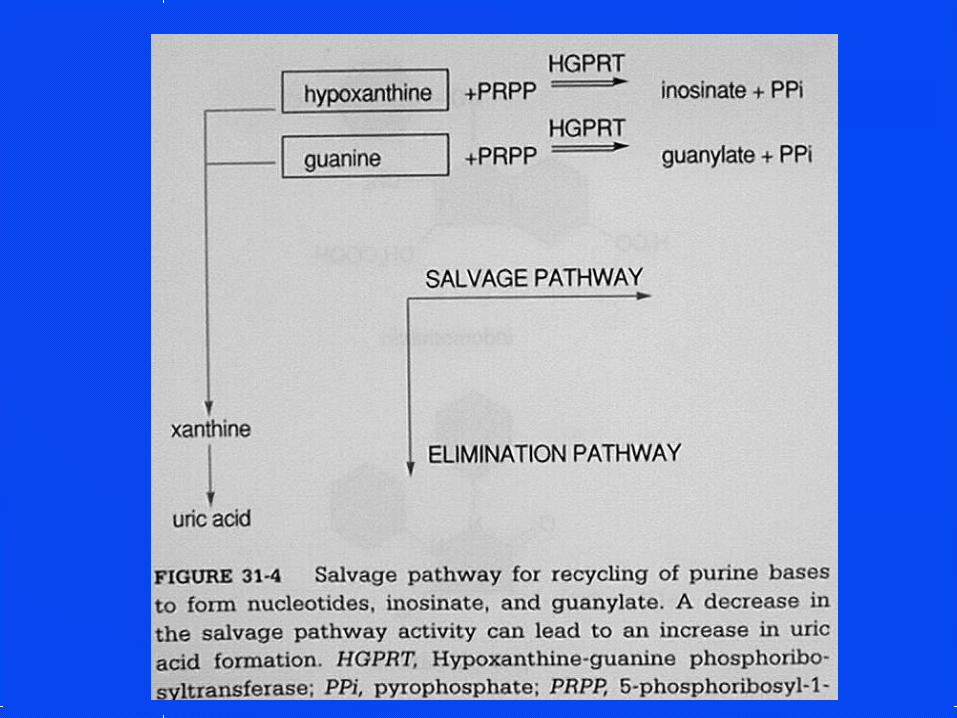
Uric Acid Formation
Goth’s Pharmacology