use of intestinal segments in urinary diversion by dr.turky al-mouhissen r3 at kkngh
TRANSCRIPT
Use of Intestinal Segments in Use of Intestinal Segments in Urinary DiversionUrinary Diversion
By By
Dr.Turky Al-MouhissenDr.Turky Al-Mouhissen
R3 at KKNGHR3 at KKNGH

outlineoutline General indications of urinary diversionGeneral indications of urinary diversion Intestinal segments used Intestinal segments used General complications General complications Renal Function necessary for Urinary Renal Function necessary for Urinary
DiversionDiversion Use of antireflux mechanism Use of antireflux mechanism Metabolic abnormalities associated Metabolic abnormalities associated Neuromechanical AspectsNeuromechanical Aspects
Indications for urinary diversionIndications for urinary diversion
PostcystectomyPostcystectomy Before transplantation in pt with bladder that Before transplantation in pt with bladder that
cannot adequately receive the transplanted cannot adequately receive the transplanted ureterureter
Dysfunctional bladders that result in Dysfunctional bladders that result in persistent bleedingpersistent bleeding obstructed uretersobstructed ureters poor compliance with upper tract deteriorationpoor compliance with upper tract deterioration inadequate storage with total urinary inadequate storage with total urinary
incontinenceincontinence
What part of intestine can we use What part of intestine can we use in urinary diversion?in urinary diversion?
StomachStomach Small bowelSmall bowel
IleumIleum JejunumJejunum
Large bowelLarge bowel TransverseTransverse SigmoidSigmoid IleocecalIleocecal

Use of stomach in diversionUse of stomach in diversion
AdvantagesAdvantages decreased electrolyte abnormalities – (less permeable decreased electrolyte abnormalities – (less permeable
to urinary solutes)to urinary solutes) acidifies the urineacidifies the urine produces less mucus produces less mucus less stonesless stones avoids acidosis ( has a net secretion of chloride and avoids acidosis ( has a net secretion of chloride and
protons rather than absorption)protons rather than absorption) behaves urodynamically as other intestinal segmentsbehaves urodynamically as other intestinal segments less infection ( less incidence of bacteruria )less infection ( less incidence of bacteruria ) easy tunnelling of uretereasy tunnelling of ureter outside field of radiationoutside field of radiation

DisadvantagesDisadvantages
less surgical familiarityless surgical familiarity ulcersulcers hemmorrhagehemmorrhage dysuria/hematuria secondary to acid pHdysuria/hematuria secondary to acid pH

complicationscomplications (Early ) (Early ) gastric retention, hemorrhage, hiccups, pancreatitis, gastric retention, hemorrhage, hiccups, pancreatitis,
dudenal injurydudenal injury
(Late complications)(Late complications) B12 anemia B12 anemia iron deficiency anemiairon deficiency anemia uncontrollable metabolic alkalosis in patients with chronic renal failure uncontrollable metabolic alkalosis in patients with chronic renal failure hematuria-dysuria syndrome bilious vomiting bilious vomiting afferent loop syndromeafferent loop syndrome dumping syndromedumping syndrome
Note: many of these complications are related to the Bilroth 1 Note: many of these complications are related to the Bilroth 1 gastroduodenostomygastroduodenostomy

When to consider stomach?When to consider stomach?
rarely indicated and may carry with them rarely indicated and may carry with them difficult problems of stomal maintenance difficult problems of stomal maintenance
when use of other intestinal segments when use of other intestinal segments would result in malabsorptionwould result in malabsorption
pts with much bowel irradiatedpts with much bowel irradiated pts with multiple small and large bowel pts with multiple small and large bowel
adhesionadhesion
Use of jejunum in diversionUse of jejunum in diversion
usually not employedusually not employed
has major electrolyte abnormalitieshas major electrolyte abnormalities Mainly, Na, Cl, K metabolic aciodosis Mainly, Na, Cl, K metabolic aciodosis
with azotemiawith azotemia

IndicationsIndications
no other acceptable bowel for useno other acceptable bowel for use extensive radiation to the ileumextensive radiation to the ileum severe adhesions / inflammation of ileum severe adhesions / inflammation of ileum
and absence of large boweland absence of large bowel

contraindicationscontraindications
severe bowel nutritional disorderssevere bowel nutritional disorders presence of another acceptable segmentpresence of another acceptable segment
( use as distal segment as possible if must ( use as distal segment as possible if must use this diversion )use this diversion )

Use of ileum in diversionUse of ileum in diversion
Advantages:Advantages: simplest type of conduit diversionsimplest type of conduit diversion associated with fewest number of intraoperative associated with fewest number of intraoperative
& postop. complications & postop. complications familiarfamiliar decreased bacteruria compared to colondecreased bacteruria compared to colon decreased stone compared to colondecreased stone compared to colon decreased contractilitydecreased contractility adequate length availableadequate length available decreased mucous compared to colondecreased mucous compared to colon
contraindicationscontraindications
pts with short bowel syndromepts with short bowel syndrome
inflammatory small bowel diseaseinflammatory small bowel disease
those whose ileum has received extensive those whose ileum has received extensive radiation, often as a consequence of prior radiation, often as a consequence of prior radiation to a pelvic malignancy radiation to a pelvic malignancy
DisadvantagesDisadvantages
malabsorption (Vit B12, fat, lack of bile salt malabsorption (Vit B12, fat, lack of bile salt resorption)resorption)
often in radiated fieldoften in radiated field higher incidence of bowel obstruction compared higher incidence of bowel obstruction compared
to colon ( 10% vs. 4%)to colon ( 10% vs. 4%) difficulty in mobilization depending on mesenterydifficulty in mobilization depending on mesentery more difficult to do non refluxing ureteric more difficult to do non refluxing ureteric
reimplantreimplant Cl metabolic acidosisCl metabolic acidosis

Use of a colon in diversionUse of a colon in diversion
AdvantagesAdvantages
easier to tunnel uretereasier to tunnel ureter less post op bowel obstruction less post op bowel obstruction
( larger diameter)( larger diameter)
better mobility than ileumbetter mobility than ileum

DisadvantagesDisadvantages
more bacteruriamore bacteruria more mucusmore mucus more stonesmore stones more infectionmore infection higher cancer rate ( ureterosigmoidostomy)higher cancer rate ( ureterosigmoidostomy)
Three types of colon conduits are commonly Three types of colon conduits are commonly used: used: transversetransverse SigmoidSigmoid IleocecalIleocecal
The transverse colonThe transverse colon pts who received pts who received extensive pelvic irradiationextensive pelvic irradiation It is an excellent segment when an intestinal It is an excellent segment when an intestinal
pyelostomy neededpyelostomy needed

The sigmoid conduit The sigmoid conduit
good choice in pts undergoing a good choice in pts undergoing a pelvic pelvic exenterationexenteration who will have a colostomy who will have a colostomy ( no bowel anastomosis needed ) ( no bowel anastomosis needed )
It allows nonrefluxing submucosal reimplantation It allows nonrefluxing submucosal reimplantation
Precaution :Precaution :
Extensive pelvic irradiation Extensive pelvic irradiation

ileocecal conduitileocecal conduit
Provides long segment of ileum when long Provides long segment of ileum when long segments of ureter need replacement segments of ureter need replacement
advantage of providing colon for the stomaadvantage of providing colon for the stoma
Contraindications to the use of transverse, Contraindications to the use of transverse, sigmoid, and ileocecal conduits include sigmoid, and ileocecal conduits include
inflammatory large bowel diseaseinflammatory large bowel disease
severe chronic diarrheasevere chronic diarrhea
Complications associated Complications associated with urinary diversionwith urinary diversion

Complications in the use of ilial conduit not listed includeComplications in the use of ilial conduit not listed include: : hypertensionhypertension renal failurerenal failure decreased renal functiondecreased renal function
These complications in large part depend on the These complications in large part depend on the concomitant procedure performed concomitant procedure performed the length of follow-up the length of follow-up status of the kidneys before diversionstatus of the kidneys before diversion
Over the long term (Over the long term (20 years20 years), ), 7%7% of patients have of patients have renal failure requiring dialysis, and renal failure requiring dialysis, and 60%60% show show morphological deterioration of the upper tractsmorphological deterioration of the upper tracts

After salvage cystectomyAfter salvage cystectomy, complications , complications are increased so that 1/3 pts have one of are increased so that 1/3 pts have one of the early complications the early complications
The complication rate is increased in pts The complication rate is increased in pts requiring renal transplantationrequiring renal transplantation



Complications in the use of large bowel Complications in the use of large bowel not listed include :not listed include :
Chronic diarrheaChronic diarrhea renal failurerenal failure renal deteriorationrenal deterioration

Interestingly, early reports suggested a Interestingly, early reports suggested a lowerlower incidence of renal deterioration with colon incidence of renal deterioration with colon conduitsconduits
Some more recent series suggest incidence Some more recent series suggest incidence of these complications is about the same of these complications is about the same
However, there appears to be However, there appears to be 7.6%7.6% incidence of pyelonephritis incidence of pyelonephritis 78%78% incidence of preservation of the upper tracts incidence of preservation of the upper tracts
over the long-term over the long-term

Renal Function necessary for Renal Function necessary for Urinary DiversionUrinary Diversion
Renal function in urinary diversion is Renal function in urinary diversion is affected by: affected by: type of urinary intestinal diversion created type of urinary intestinal diversion created time the urine is exposed to the intestinal time the urine is exposed to the intestinal
mucosamucosa
greater degree of renal function needed for greater degree of renal function needed for continentcontinent diversions rather than conduit diversions rather than conduit diversionsdiversions

patients with patients with normal urinary proteinnormal urinary protein and serum and serum creatinine below 2.0 mg/dLcreatinine below 2.0 mg/dL do well with diversion do well with diversion
can do continent diversion ifcan do continent diversion if urine osmolality of 600 mOsm/kg or greater in urine osmolality of 600 mOsm/kg or greater in
response to water deprivationresponse to water deprivation GFR > 35 mL/minGFR > 35 mL/min minimal proteinuriaminimal proteinuria achieve urine pH of 5.8 or less following ammonium achieve urine pH of 5.8 or less following ammonium
chloride loadchloride load

Use of antireflux mechanism in Use of antireflux mechanism in urinary diversion urinary diversion
In a group of pts who had nonrefluxing colon conduits Anastomoses remained nonrefluxing had a lesser
incidence of renal deterioration than those in whose the antireflux anastomosis failed
F/U for 9-20 years revealed that F/U for 9-20 years revealed that 79%79% (22 of 28 patients) (22 of 28 patients) of the refluxing renal units deteriorated, whereas only of the refluxing renal units deteriorated, whereas only 22%22% (11 of 51 pts) of the nonrefluxing units deteriorated (11 of 51 pts) of the nonrefluxing units deteriorated ((Elder et al, 1979; et al, 1979; Husmann et al, 1989) et al, 1989)
Others reported in continent diversions, the Others reported in continent diversions, the majoritymajority of pts who experience reflux show upper of pts who experience reflux show upper tract dilatation and deterioration, whereas few show tract dilatation and deterioration, whereas few show upper tract deterioration when a nonrefluxing upper tract deterioration when a nonrefluxing anastomosis is present anastomosis is present ((Kock et al, 1978) et al, 1978)
If a If a nonrefluxingnonrefluxing mecahnism is used, mecahnism is used, only only 7%7% of the renal units show evidence of of the renal units show evidence of pyelonephritic scarring after 3 months, pyelonephritic scarring after 3 months, whereas if a whereas if a refluxing refluxing anastomosis is constructed, anastomosis is constructed, 83%83%
of the renal units show scarring. Half the conduits in both of the renal units show scarring. Half the conduits in both groups have significant bacteriuria groups have significant bacteriuria ((Richie and Skinner, 1975) and Skinner, 1975)

Others have not found the same high incidence of renal Others have not found the same high incidence of renal deterioration associated with ureteral intestinal refluxdeterioration associated with ureteral intestinal reflux
One group noted One group noted no differenceno difference in the incidence of renal in the incidence of renal deterioration regardless of whether the colon conduit deterioration regardless of whether the colon conduit experienced refluxexperienced reflux 17%17% (5 of 29) of nonrefluxing renal units showed deterioration (5 of 29) of nonrefluxing renal units showed deterioration
compared with compared with 18%18% (5 of 27) of refluxing units (5 of 27) of refluxing units ((Hill and Ransley, 1983) and Ransley, 1983)
In another series, only In another series, only 3 of 1353 of 135 renal units with refluxing renal units with refluxing ureteral intestinal anastomoses that were unobstructed ureteral intestinal anastomoses that were unobstructed showed evidence of renal deterioration showed evidence of renal deterioration (Shapiro et al, 1975)(Shapiro et al, 1975)
It does not appear that conduit pressures are It does not appear that conduit pressures are transmitted to the renal pelvistransmitted to the renal pelvis
The pressure within the renal pelvis in refluxing The pressure within the renal pelvis in refluxing diversions is not elevated above normal, and it is diversions is not elevated above normal, and it is independent on the segment of bowel used independent on the segment of bowel used (Magnus, 1977; Kamizaki and Cass, 1978; Hayashi et al, 1986) (Magnus, 1977; Kamizaki and Cass, 1978; Hayashi et al, 1986)
Peristaltic ureteral contractions apparently dampen Peristaltic ureteral contractions apparently dampen pressure transmission from intestine to renal pelvis, pressure transmission from intestine to renal pelvis, emphasizing the emphasizing the importance of normal uretersimportance of normal ureters
The voiding pressure is blunted by the The voiding pressure is blunted by the distensible bowel segmentdistensible bowel segment
Moreover, in renal function measured 2 to 5 Moreover, in renal function measured 2 to 5 years postoperatively, there is years postoperatively, there is no difference in no difference in ileal and colon conduitsileal and colon conduits between those who between those who experience reflux and those who do not experience reflux and those who do not (Mansson et al, 1984)(Mansson et al, 1984)
The successful creation of an antirefluxing The successful creation of an antirefluxing anastomosis does not prevent bacterial anastomosis does not prevent bacterial colonization of the renal pelviscolonization of the renal pelvis

Metabolic complications of the use Metabolic complications of the use of intestinal segment in diversionof intestinal segment in diversion
(1) electrolyte abnormalities(1) electrolyte abnormalities(2) altered sensorium(2) altered sensorium(3) abnormal drug metabolism(3) abnormal drug metabolism(4) osteomalacia(4) osteomalacia(5) growth retardation(5) growth retardation(6) persistent and recurrent infections(6) persistent and recurrent infections(7) formation of renal and reservoir calculi(7) formation of renal and reservoir calculi(8) short bowel & nutritional problems(8) short bowel & nutritional problems(9) development of urothelial / intestinal cancer (9) development of urothelial / intestinal cancer
Many of these complications are a consequence Many of these complications are a consequence of altered solute absorption across the intestinal of altered solute absorption across the intestinal segmentsegment
The factors that influence the amount of The factors that influence the amount of solute and type of absorption are solute and type of absorption are segment of bowel usedsegment of bowel used surface area of the bowelsurface area of the bowel amount of time the urine is exposed to bowelamount of time the urine is exposed to bowel concentration of solutes in the urineconcentration of solutes in the urine renal functionrenal function pH of the fluidpH of the fluid

Electrolyte abnormalitiesElectrolyte abnormalities
Stomach :Stomach :
Cl, K metabolic alkalosisCl, K metabolic alkalosis HCl secretion by gastric segment is coupled HCl secretion by gastric segment is coupled
with systemic HCO3 releasewith systemic HCO3 release The renal HCO3 excretion ( compensation ) is The renal HCO3 excretion ( compensation ) is
impaired in persons with compromised renal impaired in persons with compromised renal function & exacerbate alkalosisfunction & exacerbate alkalosis
This is generally not a significant problem unless This is generally not a significant problem unless the patient has the patient has concomitant renal failureconcomitant renal failure


Rx of metabolic abnormalities with the Rx of metabolic abnormalities with the use of stomach in urinary diversionuse of stomach in urinary diversion::
electrolyte disorder may be difficult to treat electrolyte disorder may be difficult to treat Proton pump blockers (omeprazole)Proton pump blockers (omeprazole) Histamine ( H2 ) receptor blockerHistamine ( H2 ) receptor blocker but often when this occurs, the segment must but often when this occurs, the segment must
be taken down and replaced with ileum or be taken down and replaced with ileum or colon colon

Electrolyte abnormalitiesElectrolyte abnormalities
JejunumJejunum
Na, Cl, K, azotemia, and metabolic Na, Cl, K, azotemia, and metabolic acidosisacidosis particularly when proximal particularly when proximal jejunum is usedjejunum is used
incidence varies incidence varies 25% - 75%25% - 75% pts pts Severe abnormalities may occur in 4% Severe abnormalities may occur in 4%
when short segments are employed when short segments are employed

mechanismmechanism
jejunal segment jejunal segment loses NaCl ( secretes) and loses NaCl ( secretes) and reabsorbs K & Hreabsorbs K & H
Na and Cl carry water with it which leads to Na and Cl carry water with it which leads to dehydrationdehydration
dehydration results in hypovolemia dehydration results in hypovolemia renin renin increased as is aldosteroneincreased as is aldosterone
Na reabsorbed by kidney and K lostNa reabsorbed by kidney and K lost when this urine is presented to the jejunal when this urine is presented to the jejunal
segment , a favorable concentration gradient segment , a favorable concentration gradient exists for loss of Na and increased reabsorbtion exists for loss of Na and increased reabsorbtion of K (of K (Na rich, K poor urine)Na rich, K poor urine)
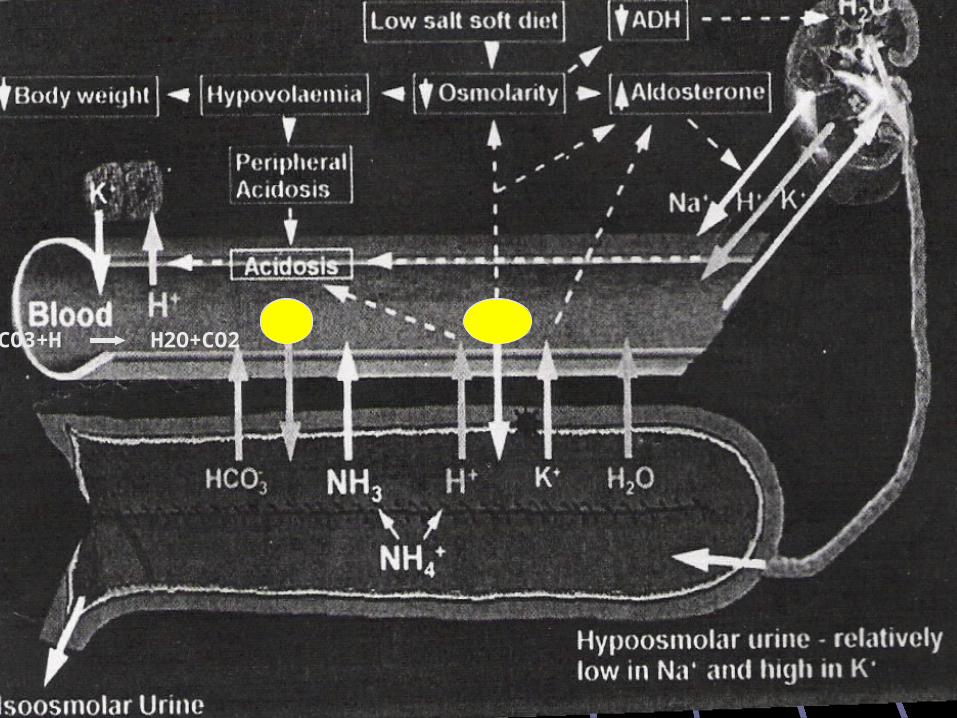
HCO3+H H2O+CO2

SymptomsSymptoms
lethargylethargy nausea and vomitingnausea and vomiting dehydrationdehydration muscle weaknessmuscle weakness elevated tempelevated temp made worse if on TPN made worse if on TPN ( mechanism unclear) ( mechanism unclear) worse with more proximal segments of jejunumworse with more proximal segments of jejunum

treatmenttreatment
rehydration with Na Clrehydration with Na Cl
correction of acidosis with Na HCO3correction of acidosis with Na HCO3
Provided that renal function is normal, hyperkalemia is Provided that renal function is normal, hyperkalemia is corrected by renal secretioncorrected by renal secretion
A diuretic may be helpful to correct the hyperkalemiaA diuretic may be helpful to correct the hyperkalemia
After restoration of normal electrolyte balance, long-term After restoration of normal electrolyte balance, long-term therapy involves oral supplements with sodium chloridetherapy involves oral supplements with sodium chloride
A thiazide diuretic has also been useful in selected cases A thiazide diuretic has also been useful in selected cases to control hyperkalemia over the long term to control hyperkalemia over the long term
Electrolyte abnormalitiesElectrolyte abnormalities
ileum & colonileum & colon
Cl metabolic acidosis, +/- hypokalemea
Acidosis occurs in most pts but in minor degree
Hyperchloremic acidosis has been reported with a frequency of 68% (19 of 28 pts—10 of 19 cases were severe enough to require treatment) in
pts with ileal conduits (Castro and Ram, 1970) In another study, 70% of patients with ileal conduits followed for 4 years or
more had a decreased serum bicarbonate level (Malek et al, 1971)
Severe electrolyte disturbances occur to a much lesser degree reported to be major problem in 18% (8 of 45) of pts with intestinal
cystoplasties (Whitmore and Gittes, 1983) in 10% (17 of 178) of patients with ileal conduits (Schmidt et al, 1973) in 80% (112 of 141) of patients with ureterosigmoidostomies
mechanismmechanism
Due to the ionized transport of Due to the ionized transport of ammoniumammonium ammonium substitutes for Na in the Na/H ammonium substitutes for Na in the Na/H
antiportantiport exchange of NH4 for H+ is coupled with the exchange of NH4 for H+ is coupled with the
exchange of Cl for HCO3exchange of Cl for HCO3 ammonium chloride is absorbed across the ammonium chloride is absorbed across the
intestinal lumen in exchange for carbonic intestinal lumen in exchange for carbonic acid ( CO2 + H20)acid ( CO2 + H20)

CO2+H2O H+HCO3

hypokalemeahypokalemea
more common in more common in ureterosigmoidostomies ureterosigmoidostomies
In one study, pts with ureterocolonic diversions had a 30% reduction
in total body K, those with ileal conduits had no significant alteration in
total body K; individually
some had 14% reduction in total body K (Williams et al, 1967)
The K depletion is due to renal K wasting as The K depletion is due to renal K wasting as a consequence ofa consequence of
renal damagerenal damage osmotic diuresisosmotic diuresis loss through intestinal secretionloss through intestinal secretion
it has been shown that when exposed to high concentrations of K in the urine, ileal segments reabsorb some of the K, whereas colon is less likely to do so (Koch et al, 1990) Rx must involve both replacement of K and
correction of the acidosis with HCO3
SymptomsSymptoms
fatigabilityfatigability anorexiaanorexia weight lossweight loss polydipsiapolydipsia LethargyLethargy Flaccid paralysis in case of severe hypokalemeaFlaccid paralysis in case of severe hypokalemea Those with ureterosigmoidostomies also have Those with ureterosigmoidostomies also have
an exacerbation of diarrheaan exacerbation of diarrhea

treatmenttreatment
alkalinizing agentsalkalinizing agents ( sodium bicarbonate, potassium citrate) ( sodium bicarbonate, potassium citrate)
chlorpromazine or nicotinic acidchlorpromazine or nicotinic acid They inhibit cAMP and thereby impede Cl transport They inhibit cAMP and thereby impede Cl transport Used in pts in whom persistent hyperchloremic Used in pts in whom persistent hyperchloremic
metabolic acidosis occurs and in whom excessive Na metabolic acidosis occurs and in whom excessive Na loads are undesirableloads are undesirable
These agents used alone do not correct the acidosis These agents used alone do not correct the acidosis in humans, but they limit its development and thus in humans, but they limit its development and thus reduce the need for alkalinizing agentsreduce the need for alkalinizing agents
Metabolic abnormalitiesMetabolic abnormalities Water deprivation test for renal function is Water deprivation test for renal function is
inappropriate test in diversion inappropriate test in diversion Bcs the bowel transports solutes and its membrane is not Bcs the bowel transports solutes and its membrane is not
particularly watertight, osmolality generally re-equilibrates across particularly watertight, osmolality generally re-equilibrates across the bowel wallthe bowel wall
The bowel also makes the contents more The bowel also makes the contents more alkalinealkaline impossible to determine the ability of the impossible to determine the ability of the
kidney to acidify simply by measuring urinary pH in kidney to acidify simply by measuring urinary pH in pts with urinary intestinal diversionpts with urinary intestinal diversion
As urea and creatinine are reabsorbed by both the As urea and creatinine are reabsorbed by both the ileum and the colon, ileum and the colon, serum concentrations of urea serum concentrations of urea and creatinine do not necessarily accurately reflect and creatinine do not necessarily accurately reflect renal functionrenal function


Altered SensoriumAltered Sensorium
causescauses
Altered ammonium metabolismAltered ammonium metabolism (most common) (most common) Magnesium deficiencyMagnesium deficiency Drug intoxicationDrug intoxication Amoniagenic coma Amoniagenic coma CirrhoticsCirrhotics Abn. liver function without cirrhosisAbn. liver function without cirrhosis Normal hepatic functionNormal hepatic function
Most common with ureterosigmoidostomyMost common with ureterosigmoidostomy
TreatmentTreatment
draining intestinal diversion to prevent exposure of draining intestinal diversion to prevent exposure of bowel to urine ( Foley or rectal tube (if ureterosig) bowel to urine ( Foley or rectal tube (if ureterosig)
Neomycin po to reduce ammonia loadNeomycin po to reduce ammonia load decrease protein intakedecrease protein intake lactulose P.O or P.R ( complexes ammonia and lactulose P.O or P.R ( complexes ammonia and
prevents absorption)prevents absorption) IV Arginine glutamate 50 g in 1 Litre D5W IV Arginine glutamate 50 g in 1 Litre D5W
(in severe cases)(in severe cases)

Abnormal Drug absorptionAbnormal Drug absorption
Drug intoxication has been reported in pts with diversionsDrug intoxication has been reported in pts with diversions Drugs more likely to be a problem are those that are Drugs more likely to be a problem are those that are
absorbed by the GI and excreted unchanged by the absorbed by the GI and excreted unchanged by the kidneykidney
The excreted drug is re-exposed to the intestinal segment, The excreted drug is re-exposed to the intestinal segment, which then reabsorbs it, and toxic serum levels develop which then reabsorbs it, and toxic serum levels develop
Reported for phenytoin & antimetabolites (methotrexate)Reported for phenytoin & antimetabolites (methotrexate) in pts with continent diversions who are receiving in pts with continent diversions who are receiving
chemotherapy, consideration should be given to draining chemotherapy, consideration should be given to draining the pouch during the period of time the toxic drugs are the pouch during the period of time the toxic drugs are being administeredbeing administered

Osteomalacia ( renal rickets)Osteomalacia ( renal rickets)
mineralized bone is reduced and osteoid mineralized bone is reduced and osteoid component becomes excessivecomponent becomes excessive
Causes:Causes: acidosis ( excess protons are buffered by the acidosis ( excess protons are buffered by the
bone with release of bone calcium)bone with release of bone calcium) correction of acidosis results in remineralization correction of acidosis results in remineralization
Vit D resistance ( renal in origin)Vit D resistance ( renal in origin) excessive calcium loss by the kidneyexcessive calcium loss by the kidney
Growth and DevelopmentGrowth and Development
urinary intestinal diversion has a detrimental effect urinary intestinal diversion has a detrimental effect on growth and developmenton growth and development
In a study of 93 myelodysplasia pts followed for 17 to 23 In a study of 93 myelodysplasia pts followed for 17 to 23 years, significant aberrations in growth were noted when years, significant aberrations in growth were noted when morphometric parameters were analyzedmorphometric parameters were analyzed
Anthropomorphic measurements in those with urinary Anthropomorphic measurements in those with urinary intestinal diversion showed a decrease in linear growth in all intestinal diversion showed a decrease in linear growth in all indices measured, with a statistically significant decrease in indices measured, with a statistically significant decrease in biachromial span and in elbow-hand length (Koch et al, 1992)biachromial span and in elbow-hand length (Koch et al, 1992)
patients are more prone to fractures and complications patients are more prone to fractures and complications after orthopedic proceduresafter orthopedic procedures
InfectionInfection
increased incidence of bacteruria, bacteremia and sepsis
many patients do well with chronic bacteruria pts with Proteus or Pseudomonas are more likely
to deteriorate their upper tracts, therefore those with pure cultures of one of these organisms should be treated
pts with mixed cultures may generally be observed, provided that they are Asymptomatic

StonesStones ** #1 stone calcium ammonium magnesium phosphate** #1 stone calcium ammonium magnesium phosphate
Factors:Factors:
hyperchloremic metabolic acidosishyperchloremic metabolic acidosis preexisting pyelonephritispreexisting pyelonephritis UTI with urea splitting organismsUTI with urea splitting organisms StaplesStaples
Incidence:Incidence:
continent cecal resevoirs (koch) 20%continent cecal resevoirs (koch) 20% colon conduit 4%colon conduit 4% ileal conduit 10-12%ileal conduit 10-12%
Short bowel and Nutritional Short bowel and Nutritional ProblemsProblems
B12 malabsorptioon bile salt malabsorption loss of Ileocecal valve
bacterial growth in ileum B12, bile salt, fat malabsorption
jejunal loss -- > malabsorption of Ca folic acid and fat

CancerCancer ureterosigmoidostomy 11% risk 10-20 year delay histologically:
adenocarcinoma adenomatous polyp sarcoma TCC
cause: transitional epithelium in contact with colonic epithelium and both are exposed to urine and feces
routine colonoscopy in these patients
neuromechanical aspectsneuromechanical aspects
Volume pressureVolume pressure goalgoal create a sphere, with high volume create a sphere, with high volume over time if conduit is filled its volume will increaseover time if conduit is filled its volume will increase
LaplaceLaplace’’s Laws Law for a sphere, tension of wall is proprtional to radius X pressurefor a sphere, tension of wall is proprtional to radius X pressure The greater the radius, the smaller the pressure which is desirable The greater the radius, the smaller the pressure which is desirable
to prevent upper tract deteriorationto prevent upper tract deterioration
Motor activityMotor activity detubularizing bowel interrupts coordinated motor activity for at least detubularizing bowel interrupts coordinated motor activity for at least
3 months, eventually returns to N state3 months, eventually returns to N state persistaltic waves are thought to reappearpersistaltic waves are thought to reappear reconfiguring bowel increase volumereconfiguring bowel increase volume


REFFERENCESREFFERENCES
The Journal Of Urology, The Journal Of Urology, Vol. 161, 1057-1066, April 1999Vol. 161, 1057-1066, April 1999
www.mdconsult.com, Urologic Clinics of www.mdconsult.com, Urologic Clinics of North America, North America, Vol. 24, No. 4, Nov.1997Vol. 24, No. 4, Nov.1997
Campbell`s Urology, Campbell`s Urology, 88thth Edition, 2002 Edition, 2002
