understanding precision medicine in cancer€¦ · and precision medicine center during the...
TRANSCRIPT
volume 17, issue 3 - Fall 2018
Understanding Precision Medicine in Cancer
2 | Oncologistics
2019 Meeting ScheduleMeeting Date Meeting Name Location Venue
January 25 Multiple Myeloma Orlando, FL Renaissance Sea World
January 25-26 ASH Review Orlando, FL Renaissance Sea World
March 8-9 Oral Therapies Plano, TX Renaissance Plano
May 16-17 Smart ID Charlotte, NC Westin Charlotte
May 17-18National Healthcare Practitioners
Charlotte, NC Westin Charlotte
*Meeting Dates Subject to Change*
Registration will be available approximately 60 days prior to each event. To register, visit www.iononline.com.
Educational Programs
As true leaders in industry, true innovators in care
and true partners in service, ION Solutions has
been dedicated to fighting for community oncology for 20 years.
One of the ways we demonstrate our
commitment to independent community
oncology is through our advocacy efforts on
Capitol Hill.
Since 2015, Community Counts has raised
awareness on the impact of sequestration,
the Part B Demo Project, and other issues
paramount to the viability of the community
setting. Just last year, more than 500
individuals contacted 280 legislators through
this outreach program.
True leaders.
True innovators.
True partners.
YEARS
ION SOLUTIONS
CommunityCountsAdvocacy.org
Table of ContentsFall 2018
6 Understanding Precision Medicine in Cancer
9 ION Solutions Launches Precision Medicine
Testing Recommendations
10 What’s News at ION
22 Reimbursement Watch
Medicare Changes Rules for How Contractors
Make Local Coverage Decisions
23 MIPS Tips
Changes in the MIPS 2019 Proposed Rule
volume 17, issue 3 - Fall 2018
Editorial & Design staff:
· Chris Vorce Senior Director, Marketing & Communications, ION Solutions
· Tricia Musslewhite Manager, Marketing & Communications, ION Solutions
· Sylvia Melton Manager, Graphic Design, ION Solutions
oncologisticsION Solutions article and advertising submissions:
Article submissions and suggestions, as well as advertising inquiries, may be sent to:
Tricia MusslewhiteManaging Editor, Oncologisticsc/o ION Solutions3101 Gaylord ParkwayFrisco, TX 75034
Information presented in Oncologistics is not intended as a substitute for the personalized advice given by a healthcare provider. The opinions expressed on the pages of Oncologistics magazine are those of the authors and do not necessarily reflect the views of ION Solutions or AmerisourceBergen. Although Oncologistics strives to present only current and accurate information, readers should not consider it as professional advice or endorsement of any position. Although great care has been taken in compiling and checking the information given in this publication to ensure accuracy, the authors, ION Solutions, and its employees or agents shall not be responsible or in any way liable for the continued currency of the information or for any errors, omissions, or inaccuracies in this magazine, whether arising from negligence or otherwise or for any consequence arising therefrom. The staff of Oncologistics provides columns and other editorial support. In no way are they responsible for the specific views presented in Oncologistics. Oncologistics magazine is published by ION Solutions, an AmerisourceBergen company.
All archived issues of Oncologistics are available online at www.iononline.com.
oneononewith Brian Ansay
In September, ION Solutions held our inaugural Precision Medicine Summit and launched our new testing recommendations for various tumor types. These recommendations were developed by your peers — fellow oncologists, pharmacists, nurses and administrative staff — to give you guidance for genetic and genomic testing. Learn more beginning on page six and then visit the Precision Medicine Center, which is now available for all ION members at www.iononline.com.
The Centers for Medicare & Medicaid Services (CMS) recently issued its Proposed Rule for 2019 under the Quality Payment Program (QPP). We expect the Final Rule to be released in November and will have resources available to answer your questions and help your practice report. In the meantime, become familiar with what CMS is proposing to change on page 23.
The QPP is just one example of how we operate in an ever-evolving market. Priorities change. Regulations shift. The path forward is not always easily traced. But I stand behind the work we’ve done in three areas – contracting, dispensing and distribution – and I firmly believe that we’ve proven to be an essential partner in this space. I also know that the work is never complete; we can never be satisfied with resting on past accomplishments. We’re committed to evolving and expanding our offerings to you so that we can continue to serve as your partner in enhancing patient care.
Thank you for your partnership,
Brian Ansay President, ION Solutions

6 | Oncologistics Oncologistics | 7
Understanding Precision Medicine in Cancer
Personalized medicine is the tailored treatment approach for a specific individual–and many agree that the treatment of any patient is considered personalized. Personalized medicine continues to evolve as doctors understand more about how certain patients respond to treatment and how mutations of cancer might happen in one patient, yet not in another.
Genomic Testing or Genetic TestingPatients often confuse the terms genomic testing with genetic testing. Genomic testing refers to the examination of unique abnormalities or mutations that occur in the cancer cells. Some or all of these abnormalities may be driving the cancer cells to grow. Genetic testing will provide information on an inherited predisposition to a specific cancer.
With a cancer diagnosis, you can have two individuals diagnosed at the same stage, yet the same chemotherapy treatment can produce completely different outcomes. That can often be attributed to the molecular make-up of their tumors. Depending on the test or panel ordered, healthcare providers can use results for either diagnostic purposes or use the results for additional monitoring.
As an example in understanding genetic versus genomic testing, breast cancer is considered. Patients with breast cancer can potentially have the BRCA1 or BRCA2 gene mutations, which are associated with a genetic predisposition to the cancer and can be passed down through generations. Those individuals who have the mutation have more frequent screenings like earlier mammograms, and sometimes undergo prophylactic mastectomies. Finding the BRCA1 and BRCA2 mutations can be done through genetic testing. But that genetic testing will not tell how a particular tumor will respond to therapy.
Precision medicine is an approach to care that allows doctors to select treatments that are most likely to help patients based on a genetic understanding of their disease.
Cancer can typically start in the body based on three almost equal factors: heredity, environment and chance. Despite all efforts to create a healthy lifestyle by avoiding tobacco, eating healthy and exercising, your heredity and even chance continue to play a part.
Every person also has potential cancer cells in their body. There may be even the slightest misalignment in the DNA. You are born with cells that will mutate, but your immune system has been designed to fight them off in the early stages. When your immune system does not kill off those cells, that is when they become their own type of organism and it can turn into cancer.
“As a body lives and grows, its cells are constantly dividing, copying their DNA—this vast genetic library—and bequeathing it to the daughter cells. They in turn pass it to their own progeny: copies of copies of copies. Along the way, errors inevitably occur. Some are caused by carcinogens but most are random misprints.”1
As you age and your cells replicate, your risk for a diagnosis of cancer increases.
Precision Medicine vs. Personalized MedicineThe phrases precision medicine and personalized medicine
are often used interchangeably when discussing a
patient’s health. In a report from the National Research
Council in 2011, scientists defined precision medicine
as an exploration of how treatment or prevention
approaches can be developed based on the combination
of genetic, environmental and social factors targeted to
individuals or populations.
“To be sure, precision medicine and personalized medicine are highly related and genomics plays a big role in both. However, even highly personalized information may or may not lead to improved health outcomes. Moreover, precision medicine approaches may lead to non-personalized interventions that can be used population-wide.”2
Precision medicine is an approach to care that allows doctors to select treatments that are most likely to help patients based on a genetic understanding of their disease. This genetic understanding is done by testing blood, tumor tissue or saliva to get a molecular analysis of the cells.
Understanding Precision Medicine in Cancer
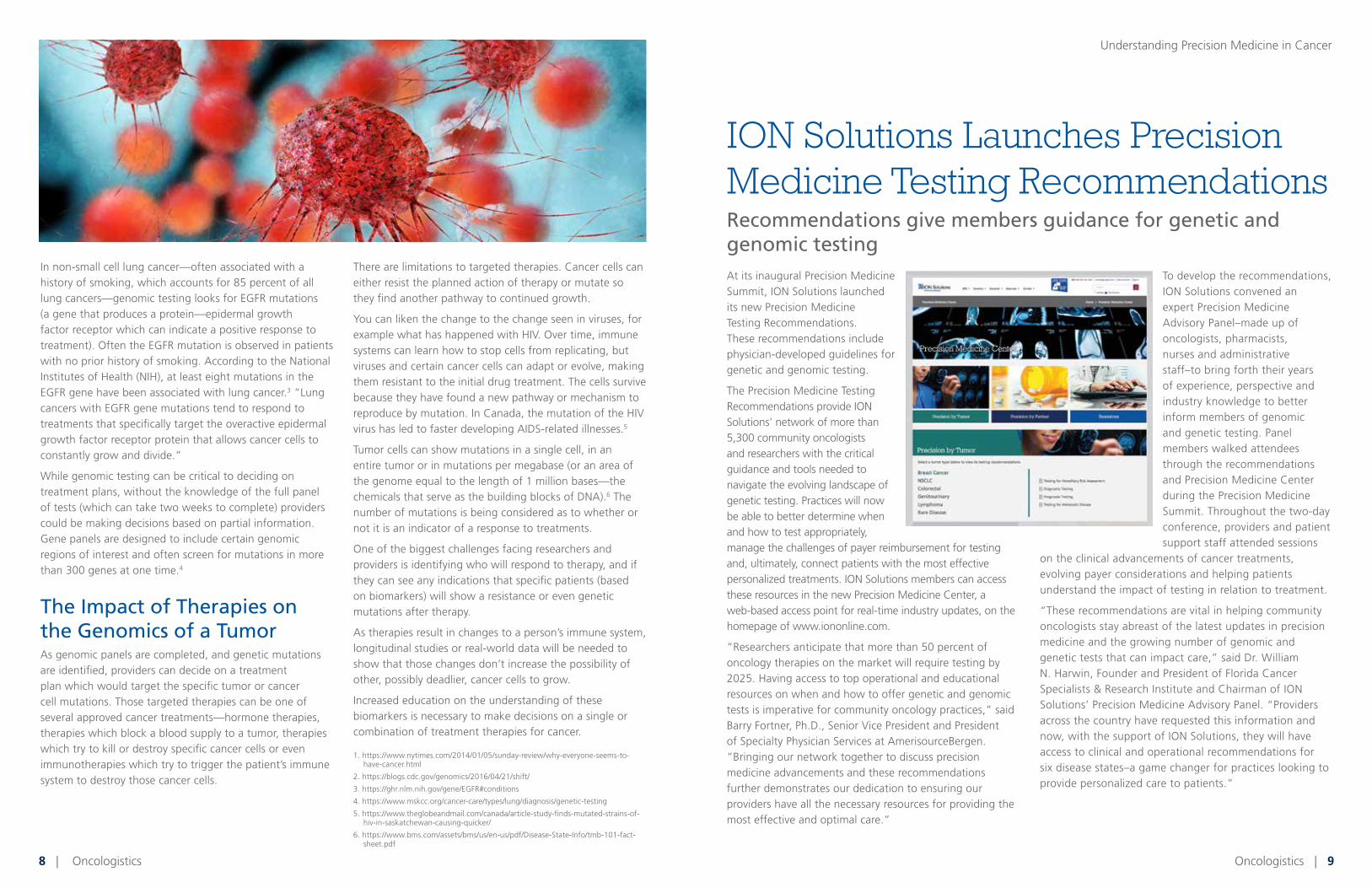
At its inaugural Precision Medicine Summit, ION Solutions launched its new Precision Medicine Testing Recommendations. These recommendations include physician-developed guidelines for genetic and genomic testing.
The Precision Medicine Testing Recommendations provide ION Solutions’ network of more than 5,300 community oncologists and researchers with the critical guidance and tools needed to navigate the evolving landscape of genetic testing. Practices will now be able to better determine when and how to test appropriately, manage the challenges of payer reimbursement for testing and, ultimately, connect patients with the most effective personalized treatments. ION Solutions members can access these resources in the new Precision Medicine Center, a web-based access point for real-time industry updates, on the homepage of www.iononline.com.
“Researchers anticipate that more than 50 percent of oncology therapies on the market will require testing by 2025. Having access to top operational and educational resources on when and how to offer genetic and genomic tests is imperative for community oncology practices,” said Barry Fortner, Ph.D., Senior Vice President and President of Specialty Physician Services at AmerisourceBergen. “Bringing our network together to discuss precision medicine advancements and these recommendations further demonstrates our dedication to ensuring our providers have all the necessary resources for providing the most effective and optimal care.”
To develop the recommendations, ION Solutions convened an expert Precision Medicine Advisory Panel–made up of oncologists, pharmacists, nurses and administrative staff–to bring forth their years of experience, perspective and industry knowledge to better inform members of genomic and genetic testing. Panel members walked attendees through the recommendations and Precision Medicine Center during the Precision Medicine Summit. Throughout the two-day conference, providers and patient support staff attended sessions
on the clinical advancements of cancer treatments, evolving payer considerations and helping patients understand the impact of testing in relation to treatment.
“These recommendations are vital in helping community oncologists stay abreast of the latest updates in precision medicine and the growing number of genomic and genetic tests that can impact care,” said Dr. William N. Harwin, Founder and President of Florida Cancer Specialists & Research Institute and Chairman of ION Solutions’ Precision Medicine Advisory Panel. “Providers across the country have requested this information and now, with the support of ION Solutions, they will have access to clinical and operational recommendations for six disease states–a game changer for practices looking to provide personalized care to patients.”
8 | Oncologistics Oncologistics | 9
In non-small cell lung cancer—often associated with a history of smoking, which accounts for 85 percent of all lung cancers—genomic testing looks for EGFR mutations (a gene that produces a protein—epidermal growth factor receptor which can indicate a positive response to treatment). Often the EGFR mutation is observed in patients with no prior history of smoking. According to the National Institutes of Health (NIH), at least eight mutations in the EGFR gene have been associated with lung cancer.3 “Lung cancers with EGFR gene mutations tend to respond to treatments that specifically target the overactive epidermal growth factor receptor protein that allows cancer cells to constantly grow and divide.”
While genomic testing can be critical to deciding on treatment plans, without the knowledge of the full panel of tests (which can take two weeks to complete) providers could be making decisions based on partial information. Gene panels are designed to include certain genomic regions of interest and often screen for mutations in more than 300 genes at one time.4
The Impact of Therapies on the Genomics of a TumorAs genomic panels are completed, and genetic mutations are identified, providers can decide on a treatment plan which would target the specific tumor or cancer cell mutations. Those targeted therapies can be one of several approved cancer treatments—hormone therapies, therapies which block a blood supply to a tumor, therapies which try to kill or destroy specific cancer cells or even immunotherapies which try to trigger the patient’s immune system to destroy those cancer cells.
There are limitations to targeted therapies. Cancer cells can either resist the planned action of therapy or mutate so they find another pathway to continued growth.
You can liken the change to the change seen in viruses, for example what has happened with HIV. Over time, immune systems can learn how to stop cells from replicating, but viruses and certain cancer cells can adapt or evolve, making them resistant to the initial drug treatment. The cells survive because they have found a new pathway or mechanism to reproduce by mutation. In Canada, the mutation of the HIV virus has led to faster developing AIDS-related illnesses.5
Tumor cells can show mutations in a single cell, in an entire tumor or in mutations per megabase (or an area of the genome equal to the length of 1 million bases—the chemicals that serve as the building blocks of DNA).6 The number of mutations is being considered as to whether or not it is an indicator of a response to treatments.
One of the biggest challenges facing researchers and providers is identifying who will respond to therapy, and if they can see any indications that specific patients (based on biomarkers) will show a resistance or even genetic mutations after therapy.
As therapies result in changes to a person’s immune system, longitudinal studies or real-world data will be needed to show that those changes don’t increase the possibility of other, possibly deadlier, cancer cells to grow.
Increased education on the understanding of these biomarkers is necessary to make decisions on a single or combination of treatment therapies for cancer.
1. https://www.nytimes.com/2014/01/05/sunday-review/why-everyone-seems-to-have-cancer.html
2. https://blogs.cdc.gov/genomics/2016/04/21/shift/
3. https://ghr.nlm.nih.gov/gene/EGFR#conditions
4. https://www.mskcc.org/cancer-care/types/lung/diagnosis/genetic-testing
5. https://www.theglobeandmail.com/canada/article-study-finds-mutated-strains-of-hiv-in-saskatchewan-causing-quicker/
6. https://www.bms.com/assets/bms/us/en-us/pdf/Disease-State-Info/tmb-101-fact-sheet.pdf
ION Solutions Launches Precision Medicine Testing RecommendationsRecommendations give members guidance for genetic and genomic testing
Understanding Precision Medicine in Cancer

10 | Oncologistics Oncologistics | 11
The Financial Impact of the Sequester Cut to Medicare Part B Drug Reimbursement in Community Oncology
In a recent article for the American Journal of Managed Care (AJMC), Dr. Lucio Gordon, head of Quality and Medical Informatics for Florida Cancer Specialists; Cass Schaedig, vice president, InfoDive, ION Solutions; and Susan Weidner, MBA, MS, senior vice president of IntrinsiQ Specialty Solutions; discuss the financial impact of the sequester cuts to Medicare Part B drug reimbursements to community oncology practices. They report a correlation between sequester cuts and community practice closures. To read the study visit https://www.ajmc.com/contributor/coa/2018/08/the-financial-impact-of-the-sequester-cut-to-medicare-part-b- drug-reimbursement-in-community-oncology.
AmerisourceBergen Comments on Trump Administration Blueprint for Lowering Drug Pricing
ION Solutions and Oncology Supply leadership submitted comments on behalf of AmerisourceBergen on more than 150 concepts laid out by the U.S. Department of Health and Human Services (HHS) Secretary Alex Azar to reduce prescription drug prices and improve affordability for patients. The comments focused on protecting the future of community oncology:
◾ Support for eliminating prohibition on pharmacists alerting consumers to lower cost prescription options (gag clauses)
◾ Support for greater access and availability to biosimilars and generic products
◾ Oppose moving Medicare Part B drugs to Part D and reinstitution of Medicare Competitive Acquisition Program (CAP)
◾ Support patient copayment assistance programs
◾ Support for value-based purchasing arrangements
To read the letter visit www.iononline.com.
Senate Passes Comprehensive Opioid Legislation
On Sept. 17, the Senate passed The Substance Use-Disorder Prevention that Promotes Opioid Recovery and Treatment (SUPPORT) for Patients and Communities Act (H.R. 6), comprehensive legislation intended to help mitigate the opioid epidemic. AmerisourceBergen supports many provisions in the bill, specifically Sec. 3202, sponsored by Sens. Feinstein (D-CA), Grassley (R-IA), Capito (R. WV) and Durbin (D-IL.); and Sec. 3602, sponsored by Sens. Hassan (D-N.H.) and Grassley—which will enhance critical data sharing between distributors
and the DEA, as well as state regulatory agencies and local law enforcement. Consistent with AmerisourceBergen’s repeated calls for increased data transparency between DEA and industry, these provisions also provide greater visibility around the overall number of controlled substances shipped, as well as establish a more streamlined approach to reporting suspicious orders through the creation of a centralized database.
AmerisourceBergen provided technical expertise to the bill sponsors throughout this process and we remain committed to advancing additional policies we believe can help detect potentially suspicious orders before they are shipped. There are significant differences between the Senate and previously passed House opioid legislation. Following the conference negotiations, the final bill will be sent to President Trump for signature likely later this year.
What’s News at ION
200 FIFTH AVENUE NEW YORK, NY 10010
LEGAL RELEASE STATUS
AD APPROVAL
Release has been obtained Legal Coord:
Acct Mgmt: Print Prod:
Art Director: Proofreader:
Copywriter: Studio:
JOB #: ELIAHU-Q80204_BASE_Pg1_REV2 PROOF: 2
CLIENT: ELI LILLY & COMPANY OP: CV, JS
SPACE/SIZE: B: 8.75” x 11.25” T: 7.875” x 10.5” S: 7” x 10”
DATE:
THIS ADVERTISEMENT PREPARED BY TOWNHOUSE
CLIENT: ELI LILLY & COMPANY SIZE, SPACE: 7.875” x 10.5”, Journal Ad
PRODUCT: ABEMACICLIB US HCP PUBS: NCCN Journal Ad
JOB#: ELIAHU-Q80204_BASE_Pg1_REV2 ISSUE: 2018
ART DIRECTOR: J. Goody COPYWRITER: None
Diarrhea occurred in 81% of patients receiving Verzenio plus an aromatase inhibitor in MONARCH 3, 86% of patients receiving Verzenio plus fulvestrant in MONARCH 2 and 90% of patients receiving Verzenio alone in MONARCH 1. Grade 3 diarrhea occurred in 9% of patients receiving Verzenio plus an aromatase inhibitor in MONARCH 3, 13% of patients receiving Verzenio plus fulvestrant in MONARCH 2 and in 20% of patients receiving Verzenio alone in MONARCH 1. Episodes of diarrhea have been associated with dehydration and infection.Diarrhea incidence was greatest during the fi rst month of Verzenio dosing. In MONARCH 3, the median time to onset of the first diarrhea event was 8 days, and the median duration of diarrhea for Grades 2 and 3 were 11 and 8 days, respectively. In MONARCH 2, the median time to onset of the fi rst diarrhea event was 6 days, and the median duration of diarrhea for
Grades 2 and 3 were 9 days and 6 days, respectively. In MONARCH 3, 19% of patients with diarrhea required a dose omission and 13% required a dose reduction. In MONARCH 2, 22% of patients with diarrhea required a dose omission and 22% required a dose reduction. The time to onset and resolution for diarrhea were similar across MONARCH 3, MONARCH 2, and MONARCH 1.Instruct patients that at the fi rst sign of loose stools, they should start antidiarrheal therapy such as loperamide, increase oral fl uids, and notify their healthcare provider for further instructions and appropriate follow-up. For Grade 3 or 4 diarrhea, or diarrhea that requires hospitalization, discontinue Verzenio until toxicity resolves to ≤Grade 1, and then resume Verzenio at the next lower dose.
Select Important Safety Information
Please see additional Important Safety Information and Brief Summary of full Prescribing Information for Verzenio on the following pages.
For patients with HR+, HER2− MBC,
including those with concerning clinical characteristics1-14†
Along the MBC journey*—
explore Verzenio1
Verzenio is indicated for the treatment of hormone receptor−positive (HR+), human epidermal growth factor receptor 2−negative (HER2−) advanced or metastatic breast cancer (MBC):
In combination with fulvestrant for women with disease progression following endocrine therapy
In combination with an aromatase inhibitor (AI) for postmenopausal women as initial endocrine-based therapy
As a single agent for adult patients with disease progression following endocrine therapy and prior chemotherapy in the metastatic setting
* Patients who received prior therapy with a CDK4 & 6 inhibitor were excluded from the MONARCH trials.2-4 There are currently no data regarding the use of Verzenio following use of another CDK4 & 6 inhibitor.
† Disease characteristics that typically confer a less favorable prognosis. Visceral disease and progression on ET and prior chemotherapy in the metastatic setting were concerning clinical characteristics in MONARCH 1. Primary resistance and visceral disease were concerning clinical characteristics in MONARCH 2. Liver metastases and treatment-free interval <36 months were concerning clinical characteristics in MONARCH 3. Exploratory subgroup analyses of PFS were performed for patients with liver metastases and for patients with a treatment-free interval <36 months.2-14
CDK4 & 6=cyclin-dependent kinases 4 and 6; ET=endocrine therapy; PFS=progression-free survival.
S:7”S:10”
T:7.875”T:10.5”
B:8.75”B
:11.25”

12 | Oncologistics
200 FIFTH AVENUE NEW YORK, NY 10010
LEGAL RELEASE STATUS
AD APPROVAL
Release has been obtained Legal Coord:
Acct Mgmt: Print Prod:
Art Director: Proofreader:
Copywriter: Studio:
JOB #: ELIAHU-Q80204_Spread_1_REV2 PROOF: 2
CLIENT: ELI LILLY & COMPANY OP: CV
SPACE/SIZE: B: 17.25” x 11.25” T: 15.75” x 10.5” S: 14.75” x 10”
DATE:
THIS ADVERTISEMENT PREPARED BY TOWNHOUSE
CLIENT: ELI LILLY & COMPANY SIZE, SPACE: 15.75” x 10.5”, 4C
PRODUCT: ABEMACICLIB US DTC PUBS: MAGAZINE
JOB#: ELIAHU-Q80204_Spread_1_REV2 ISSUE: 2018
ART DIRECTOR: J. Goody COPYWRITER: None
Pg 2 Pg 3
Verzenio + fulvestrant
Verzenio + AI as fi rst-line endocrine-based therapy1,3 Verzenio + fulvestrant in patients who recurred
or progressed on or after ET1
PFS results in women with concerning clinical characteristics
were consistent with the ITT population1,3,9-14§
PFS results in women with concerning clinical characteristics
were consistent with the ITT population1,2,5-8‡
§Disease characteristics that typically confer a less favorable prognosis. Liver metastases and treatment-free interval <36 months were concerning clinical characteristics in MONARCH 3.
‡Disease characteristics that typically confer a less favorable prognosis. Primary resistance and visceral disease were concerning clinical characteristics in MONARCH 2.
*In patients with measurable disease; N=267 for the Verzenio + AI arm, N=132 for the AI alone arm.1 †Based upon confi rmed responses.1‡PR defi ned as ≥30% reduction in target lesion size per RECIST 1.1.3,15
CI=confi dence interval; CR=complete response; DoR=duration of response; HR=hazard ratio; ITT=intent-to-treat; NR=not reached; ORR=objective response rate; PR=partial response; RECIST 1.1= Response Evaluation Criteria in Solid Tumors version 1.1.
*N=318 for the Verzenio + fulvestrant arm; N=164 for the fulvestrant alone arm.1†PR defi ned as ≥30% reduction in target lesion size per RECIST 1.1.2,15
For women with HR+, HER2− MBC For women with HR+, HER2− MBC
Exploratory subgroup analyses
>28-month median PFS as initial endocrine-based therapy1
>16-month median PFS in women who recurred or progressed on or after ET1
The percentage of events at the time of analysis was 42.1% (n=138) and 65.5% (n=108) in the Verzenio + AI and AI alone arms, respectively1
At the time of the PFS analysis, 19% of patients had died, and overall survival data were immature1
The percentage of events at the time of analysis was 49.8% (n=222) and 70.4% (n=157) in the Verzenio + fulvestrant and fulvestrant alone arms, respectively1
At the time of the primary analysis of PFS, overall survival data were not mature (20% of patients had died)1
Exploratory subgroup analyses of PFS were performed for the subgroups of patients with liver metastases or with treatment-free interval <36 months after completion of adjuvant ET. Estimated HRs and CIs for the within group analyses that were adjusted for treatment interaction are shown. The analyses were not adjusted for multiplicity and the study was not powered to test the eff ect of Verzenio + AI among subgroups.13,14 Preplanned subgroup analyses of PFS were performed for stratifi cation factors of disease site, including visceral disease, and endocrine
resistance, including primary resistance. The analyses were not adjusted for multiplicity and the study was not powered to test the eff ect of Verzenio + fulvestrant among subgroups16
MONARCH 3 was a multicenter trial that enrolled 493 patients with HR+, HER2− locoregionally recurrent or MBC in combination with a nonsteroidal AI as initial endocrine-based therapy. The median patient age was 63 years (range, 32 to 88 years). Forty-seven percent of patients had received prior ET and 39% of patients had received chemotherapy in the adjuvant setting. Patients were randomized 2:1 to Verzenio + AI or placebo + AI. Patients received either letrozole (80%) or anastrozole (20%). Verzenio was dosed continuously until disease progression or unacceptable toxicity. The primary endpoint was PFS. Key secondary endpoints were ORR and DoR.1,3
MONARCH 2 was a phase III, randomized, double-blind, placebo-controlled trial that enrolled 669 patients with HR+, HER2− MBC who progressed on ET. Patients were randomized 2:1 to Verzenio + fulvestrant or placebo + fulvestrant. Verzenio was dosed on a continuous dosing schedule until disease progression or unacceptable toxicity. The primary endpoint was PFS. Key secondary endpoints were ORR, overall survival, and DoR.1,2
ORR in patients with measurable disease1,3*†‡
ORR was defi ned as the proportion of patients with CR + PR and does not include stable disease1
ORR in patients with measurable disease1,2*†
ORR was defi ned as the proportion of patients with CR + PR, and does not include stable disease1,15†
ITT1
28.2monthsmPFS
(95% CI: 23.5-NR) vs 14.8 months with AI alone (95% CI: 11.2-19.2) HR=0.540 (95% CI: 0.418-0.698) P<.00011
(95% CI: 7.4-23.7) (n=47) vs7.2 months median PFS with AI alone (95% CI: 2.1-14.0) (n=31) HR=0.477 (95% CI: 0.272-0.837)
15.0months
Liver metastases13
(95% CI: 11.6-NR) (n=44) vs 9.0 months median PFS with AI alone (95% CI: 3.7-14.2) (n=32) HR=0.441 (95% CI: 0.241-0.805)
29.5months
Treatment-free interval <36 months14
(95% CI: 14.4-19.3) vs 9.3 months with fulvestrant alone (95% CI: 7.4-12.7) HR=0.553 (95% CI: 0.449-0.681) P<.00011
16.4monthsmPFS
ITT1
(95% Cl: 12.4-24.1) (n=111) vs 7.9 months with fulvestrant alone (95% Cl: 5.7-11.4) (n=58) HR=0.454 (95% CI: 0.306-0.674)
15.3months
Primary resistance16
(95% Cl: 13.0-17.4) (n=245) vs 6.5 months with fulvestrant alone (95% Cl: 5.6-8.7) (n=128) HR=0.481 (95% CI: 0.369-0.627)
14.7months
Visceral disease16
Select Important Safety Information (cont’d)
Select Important Safety Information (cont’d)
Neutropenia occurred in 41% of patients receiving Verzenio plus an aromatase inhibitor in MONARCH 3, 46% of patients receiving Verzenio plus fulvestrant in MONARCH 2 and 37% of patients receiving Verzenio alone in MONARCH 1. A Grade ≥3 decrease in neutrophil count (based on laboratory fi ndings) occurred in 22% of patients receiving Verzenio plus an aromatase inhibitor in MONARCH 3, 32% of patients receiving Verzenio plus fulvestrant in MONARCH 2 and in 27% of patients receiving Verzenio alone in MONARCH 1. In MONARCH 3, the median time to fi rst episode of Grade ≥3 neutropenia was 33 days, and in MONARCH 2 and MONARCH 1, was 29 days. In MONARCH 3, median duration of Grade ≥3 neutropenia was 11 days, and for MONARCH 2 and MONARCH 1 was 15 days.Monitor complete blood counts prior to the start of Verzenio therapy, every 2 weeks for the fi rst 2 months, monthly for the next 2 months,
and as clinically indicated. Dose interruption, dose reduction, or delay in starting treatment cycles is recommended for patients who develop Grade 3 or 4 neutropenia.Febrile neutropenia has been reported in <1% of patients exposed to Verzenio in the MONARCH studies. Two deaths due to neutropenic sepsis were observed in MONARCH 2. Inform patients to promptly report any episodes of fever to their healthcare provider.Grade ≥3 increases in alanine aminotransferase (ALT) (6% versus 2%) and aspartate aminotransferase (AST) (3% versus 1%) were reported in the Verzenio and placebo arms, respectively, in MONARCH 3. Grade ≥3 increases in ALT (4% versus 2%) and AST (2% versus 3%) were reported in the Verzenio and placebo arms respectively, in MONARCH 2.
In MONARCH 3, for patients receiving Verzenio plus an aromatase inhibitor with Grade ≥3 increases in ALT or AST, median time to onset was 61 and 71 days, respectively, and median time to resolution to Grade <3 was 14 and 15 days, respectively. In MONARCH 2, for patients receiving Verzenio plus fulvestrant with Grade ≥3 increases in ALT or AST, median time to onset was 57 and 185 days, respectively, and median time to resolution to Grade <3 was 14 and 13 days, respectively.For assessment of potential hepatotoxicity, monitor liver function tests (LFTs) prior to the start of Verzenio therapy, every 2 weeks for the fi rst 2 months, monthly for the next 2 months, and as clinically indicated. Dose interruption, dose reduction, dose discontinuation, or delay in starting treatment cycles is recommended for patients who develop persistent or recurrent Grade 2, or Grade 3 or 4, hepatic transaminase elevation.
Venous thromboembolic events were reported in 5% of patients treated with Verzenio plus an aromatase inhibitor as compared to 0.6% of patients treated with an aromatase inhibitor plus placebo in MONARCH 3. Venous thromboembolic events were reported in 5% of patients treated with Verzenio plus fulvestrant in MONARCH 2 as compared to 0.9% of patients treated with fulvestrant plus placebo. Venous thromboembolic events included deep vein thrombosis, pulmonary embolism, pelvic venous thrombosis, cerebral venous sinus thrombosis, subclavian and axillary vein thrombosis, and inferior vena cava thrombosis. Across the clinical development program, deaths due to venous thromboembolism have been reported.
100
80
60
40
20
0VERZENIO + Al PLACEBO + Al
PATI
ENTS
(%)
(N=267) (N=132)
3.4% CR(n=9)
52.1% PR(n=139) 40.2% PR
(n=53)
55.4%ORR
(95% Cl: 49.5-61.4)
40.2% ORR(95% Cl: 31.8-48.5)
100
80
60
40
20
0VERZENIO + FULVESTRANT PLACEBO + FULVESTRANT
(95% Cl: 42.6-53.6)
21.3% ORR
PATI
ENTS
(%)
(95% Cl: 15.1-27.6)
(N=318) (N=164)
48.1%ORR
3.5% CR(n=11)
44.7% PR(n=142)
21.3% PR(n=35)
Please see additional Important Safety Information and Brief Summary of full Prescribing Information for Verzenio on the following pages.
Primary resistance is defi ned as relapse while on the fi rst 2 years of adjuvant endocrine therapy, or progressive disease within the fi rst 6 months of fi rst-line endocrine therapy for metastatic breast cancer1
Visceral disease was defi ned as at least 1 lesion on an internal organ or in the third space and could have included lung, liver, pleural, or peritoneal metastatic involvement17
Verzenio + AI
S:14.75”S:10”
T:15.75”T:10.5”
B:17.25”B
:11.25”
200 FIFTH AVENUE NEW YORK, NY 10010
LEGAL RELEASE STATUS
AD APPROVAL
Release has been obtained Legal Coord:
Acct Mgmt: Print Prod:
Art Director: Proofreader:
Copywriter: Studio:
JOB #: ELIAHU-Q80204_Spread_2_REV2 PROOF: 2
CLIENT: ELI LILLY & COMPANY OP: CV, JS
SPACE/SIZE: B: 17.25” x 11.25” T: 15.75” x 10.5” S: 14.75” x 10”
DATE:
THIS ADVERTISEMENT PREPARED BY TOWNHOUSE
CLIENT: ELI LILLY & COMPANY SIZE, SPACE: 15.75” x 10.5”, 4C
PRODUCT: ABEMACICLIB US DTC PUBS: MAGAZINE
JOB#: ELIAHU-Q80204_Spread_2_REV2 ISSUE: 2018
ART DIRECTOR: J. Goody COPYWRITER: None
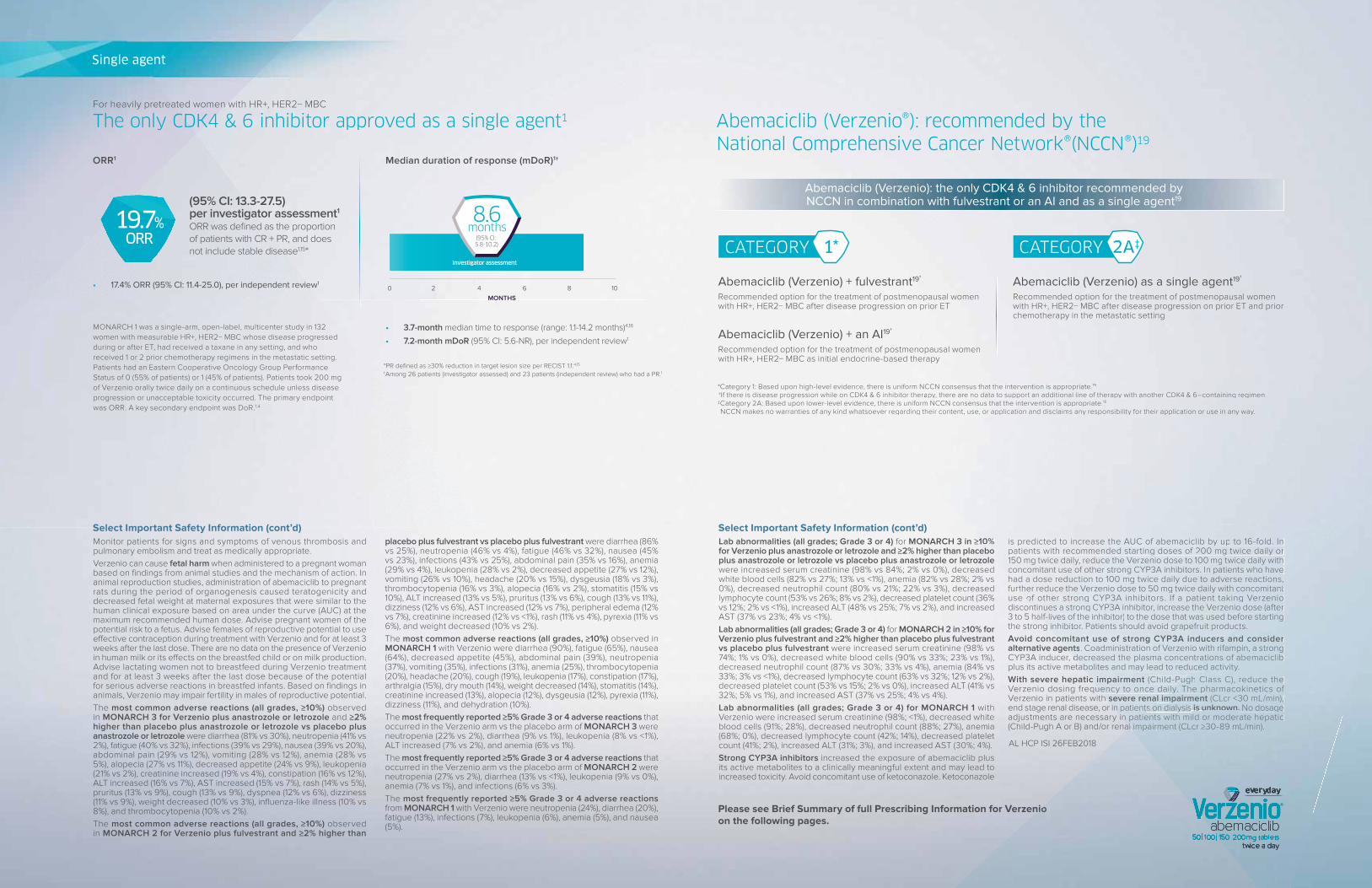
Abemaciclib (Verzenio®): recommended by the
National Comprehensive Cancer Network®(NCCN®)19
Please see Brief Summary of full Prescribing Information for Verzenio on the following pages.
Abemaciclib (Verzenio) as a single agent19†
Recommended option for the treatment of postmenopausal women with HR+, HER2− MBC after disease progression on prior ET and prior chemotherapy in the metastatic setting
Abemaciclib (Verzenio) + fulvestrant19†
Recommended option for the treatment of postmenopausal women with HR+, HER2− MBC after disease progression on prior ET
Abemaciclib (Verzenio) + an AI19†
Recommended option for the treatment of postmenopausal women with HR+, HER2− MBC as initial endocrine-based therapy
*Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate.19
†If there is disease progression while on CDK4 & 6 inhibitor therapy, there are no data to support an additional line of therapy with another CDK4 & 6–containing regimen.‡Category 2A: Based upon lower-level evidence, there is uniform NCCN consensus that the intervention is appropriate.19
NCCN makes no warranties of any kind whatsoever regarding their content, use, or application and disclaims any responsibility for their application or use in any way.
Abemaciclib (Verzenio): the only CDK4 & 6 inhibitor recommended by NCCN in combination with fulvestrant or an AI and as a single agent19
CATEGORY 2A‡CATEGORY 1*
Select Important Safety Information (cont’d)Select Important Safety Information (cont’d)Monitor patients for signs and symptoms of venous thrombosis and pulmonary embolism and treat as medically appropriate.Verzenio can cause fetal harm when administered to a pregnant woman based on fi ndings from animal studies and the mechanism of action. In animal reproduction studies, administration of abemaciclib to pregnant rats during the period of organogenesis caused teratogenicity and decreased fetal weight at maternal exposures that were similar to the human clinical exposure based on area under the curve (AUC) at the maximum recommended human dose. Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential to use eff ective contraception during treatment with Verzenio and for at least 3 weeks after the last dose. There are no data on the presence of Verzenio in human milk or its eff ects on the breastfed child or on milk production. Advise lactating women not to breastfeed during Verzenio treatment and for at least 3 weeks after the last dose because of the potential for serious adverse reactions in breastfed infants. Based on fi ndings in animals, Verzenio may impair fertility in males of reproductive potential.The most common adverse reactions (all grades, ≥10%) observed in MONARCH 3 for Verzenio plus anastrozole or letrozole and ≥2% higher than placebo plus anastrozole or letrozole vs placebo plus anastrozole or letrozole were diarrhea (81% vs 30%), neutropenia (41% vs 2%), fatigue (40% vs 32%), infections (39% vs 29%), nausea (39% vs 20%), abdominal pain (29% vs 12%), vomiting (28% vs 12%), anemia (28% vs 5%), alopecia (27% vs 11%), decreased appetite (24% vs 9%), leukopenia (21% vs 2%), creatinine increased (19% vs 4%), constipation (16% vs 12%), ALT increased (16% vs 7%), AST increased (15% vs 7%), rash (14% vs 5%), pruritus (13% vs 9%), cough (13% vs 9%), dyspnea (12% vs 6%), dizziness (11% vs 9%), weight decreased (10% vs 3%), infl uenza-like illness (10% vs 8%), and thrombocytopenia (10% vs 2%).The most common adverse reactions (all grades, ≥10%) observed in MONARCH 2 for Verzenio plus fulvestrant and ≥2% higher than
placebo plus fulvestrant vs placebo plus fulvestrant were diarrhea (86% vs 25%), neutropenia (46% vs 4%), fatigue (46% vs 32%), nausea (45% vs 23%), infections (43% vs 25%), abdominal pain (35% vs 16%), anemia (29% vs 4%), leukopenia (28% vs 2%), decreased appetite (27% vs 12%), vomiting (26% vs 10%), headache (20% vs 15%), dysgeusia (18% vs 3%), thrombocytopenia (16% vs 3%), alopecia (16% vs 2%), stomatitis (15% vs 10%), ALT increased (13% vs 5%), pruritus (13% vs 6%), cough (13% vs 11%), dizziness (12% vs 6%), AST increased (12% vs 7%), peripheral edema (12% vs 7%), creatinine increased (12% vs <1%), rash (11% vs 4%), pyrexia (11% vs 6%), and weight decreased (10% vs 2%).The most common adverse reactions (all grades, ≥10%) observed in MONARCH 1 with Verzenio were diarrhea (90%), fatigue (65%), nausea (64%), decreased appetite (45%), abdominal pain (39%), neutropenia (37%), vomiting (35%), infections (31%), anemia (25%), thrombocytopenia (20%), headache (20%), cough (19%), leukopenia (17%), constipation (17%), arthralgia (15%), dry mouth (14%), weight decreased (14%), stomatitis (14%), creatinine increased (13%), alopecia (12%), dysgeusia (12%), pyrexia (11%), dizziness (11%), and dehydration (10%). The most frequently reported ≥5% Grade 3 or 4 adverse reactions that occurred in the Verzenio arm vs the placebo arm of MONARCH 3 were neutropenia (22% vs 2%), diarrhea (9% vs 1%), leukopenia (8% vs <1%), ALT increased (7% vs 2%), and anemia (6% vs 1%).The most frequently reported ≥5% Grade 3 or 4 adverse reactions that occurred in the Verzenio arm vs the placebo arm of MONARCH 2 were neutropenia (27% vs 2%), diarrhea (13% vs <1%), leukopenia (9% vs 0%), anemia (7% vs 1%), and infections (6% vs 3%).The most frequently reported ≥5% Grade 3 or 4 adverse reactions from MONARCH 1 with Verzenio were neutropenia (24%), diarrhea (20%), fatigue (13%), infections (7%), leukopenia (6%), anemia (5%), and nausea (5%).
The only CDK4 & 6 inhibitor approved as a single agent1
*PR defi ned as ≥30% reduction in target lesion size per RECIST 1.1.4,15
†Among 26 patients (investigator assessed) and 23 patients (independent review) who had a PR.1
For heavily pretreated women with HR+, HER2− MBC
ORR1 Median duration of response (mDoR)1†
17.4% ORR (95% CI: 11.4-25.0), per independent review1
3.7-month median time to response (range: 1.1-14.2 months)4,18
7.2-month mDoR (95% CI: 5.6-NR), per independent review1
(95% CI: 13.3-27.5) per investigator assessment1
ORR was defi ned as the proportion of patients with CR + PR, and does not include stable disease1,15*
19.7%ORR
0 2 4 6 8 10
MONTHS
8.6 months
(95% CI: 5.8-10.2)
Investigator assessment
MONARCH 1 was a single-arm, open-label, multicenter study in 132 women with measurable HR+, HER2− MBC whose disease progressed during or after ET, had received a taxane in any setting, and who received 1 or 2 prior chemotherapy regimens in the metastatic setting. Patients had an Eastern Cooperative Oncology Group Performance Status of 0 (55% of patients) or 1 (45% of patients). Patients took 200 mg of Verzenio orally twice daily on a continuous schedule unless disease progression or unacceptable toxicity occurred. The primary endpoint was ORR. A key secondary endpoint was DoR.1,4
Lab abnormalities (all grades; Grade 3 or 4) for MONARCH 3 in ≥10% for Verzenio plus anastrozole or letrozole and ≥2% higher than placebo plus anastrozole or letrozole vs placebo plus anastrozole or letrozole were increased serum creatinine (98% vs 84%; 2% vs 0%), decreased white blood cells (82% vs 27%; 13% vs <1%), anemia (82% vs 28%; 2% vs 0%), decreased neutrophil count (80% vs 21%; 22% vs 3%), decreased lymphocyte count (53% vs 26%; 8% vs 2%), decreased platelet count (36% vs 12%; 2% vs <1%), increased ALT (48% vs 25%; 7% vs 2%), and increased AST (37% vs 23%; 4% vs <1%).Lab abnormalities (all grades; Grade 3 or 4) for MONARCH 2 in ≥10% for Verzenio plus fulvestrant and ≥2% higher than placebo plus fulvestrant vs placebo plus fulvestrant were increased serum creatinine (98% vs 74%; 1% vs 0%), decreased white blood cells (90% vs 33%; 23% vs 1%), decreased neutrophil count (87% vs 30%; 33% vs 4%), anemia (84% vs 33%; 3% vs <1%), decreased lymphocyte count (63% vs 32%; 12% vs 2%), decreased platelet count (53% vs 15%; 2% vs 0%), increased ALT (41% vs 32%; 5% vs 1%), and increased AST (37% vs 25%; 4% vs 4%).Lab abnormalities (all grades; Grade 3 or 4) for MONARCH 1 with Verzenio were increased serum creatinine (98%; <1%), decreased white blood cells (91%; 28%), decreased neutrophil count (88%; 27%), anemia (68%; 0%), decreased lymphocyte count (42%; 14%), decreased platelet count (41%; 2%), increased ALT (31%; 3%), and increased AST (30%; 4%). Strong CYP3A inhibitors increased the exposure of abemaciclib plus its active metabolites to a clinically meaningful extent and may lead to increased toxicity. Avoid concomitant use of ketoconazole. Ketoconazole
is predicted to increase the AUC of abemaciclib by up to 16-fold. In patients with recommended starting doses of 200 mg twice daily or 150 mg twice daily, reduce the Verzenio dose to 100 mg twice daily with concomitant use of other strong CYP3A inhibitors. In patients who have had a dose reduction to 100 mg twice daily due to adverse reactions, further reduce the Verzenio dose to 50 mg twice daily with concomitant use of other strong CYP3A inhibitors. If a patient taking Verzenio discontinues a strong CYP3A inhibitor, increase the Verzenio dose (after 3 to 5 half-lives of the inhibitor) to the dose that was used before starting the strong inhibitor. Patients should avoid grapefruit products. Avoid concomitant use of strong CYP3A inducers and consider alternative agents. Coadministration of Verzenio with rifampin, a strong CYP3A inducer, decreased the plasma concentrations of abemaciclib plus its active metabolites and may lead to reduced activity. With severe hepatic impairment (Child-Pugh Class C), reduce the Verzenio dosing frequency to once daily. The pharmacokinetics of Verzenio in patients with severe renal impairment (CLcr <30 mL/min), end stage renal disease, or in patients on dialysis is unknown. No dosage adjustments are necessary in patients with mild or moderate hepatic (Child-Pugh A or B) and/or renal impairment (CLcr ≥30-89 mL/min).
AL HCP ISI 26FEB2018
Single agent
nce, there is uniform NCCN connsensensusus hthat the intervention is appropriate.19
K4 & 6 inhibitor therarapypy, tthere are no data to support an additional line of therapy with another CDK4 & 6–containing regimen.ce, there is unifniform NCCN consensus that the intervention is appropriate.19
ever regagardding their content, use, or application and disclaims any responsibility for their application or use in any way.
≥10%bo
e
is predicted to increase the AUC of abemaciclib by by uup to 16-fold. In patients with recommended starting doses oof 2f 200 mg twice e daidailyly or 150 mg twice daily, reduce the Verzenio dodosse to 100 mgg twtwiceice daily with concomitant use of other strong CYP3P3A inhibitors I. In pn patients who have had a dose reduction to 100 mgmg twtwice dailyy dudue to adverse reactions,
rther reduce the Verzenio dodose to 50 mgmg twice daily with concomitant of other strong CYP3P3A inhibititorors. If a patient taking Verzenntinues a strong CYCYP3A inhibhibitor, increase the Verzenio dose
alf-lives of thehe inhibitor)r) tto the dose that was used before g inhibittoor. Patientsnts should avoid grapefruit products
omomitant usese of strong CYP3A inducers aents. CCooadministration of Verzenio with r
deecreased the plasma concentratiabolites and may lead to reduce
c impairment (Child-Puuency to once daily
h severe renal imin patients o
in patieal i
nio
al
nt enio
se (after re stastartirtingng
cts.s and consider
h rifampin, a strong ations of abebemaccicliclibib
uced activt ityy.Pughg ClaClassss C), reduce the
ilyily. T. Thehe pharmacokinetics of l imimpairment (CLcr <30 mL/min),
s on dialysis is unknown. No dosage atients with mild or moderate hepatic
l impairment (CLcr ≥30-89 mL/min).
Pg 4 Pg 5
S:14.75”S:10”
T:15.75”T:10.5”
B:17.25”B
:11.25”
200 FIFTH AVENUE NEW YORK, NY 10010
LEGAL RELEASE STATUS
AD APPROVAL
Release has been obtained Legal Coord:
Acct Mgmt: Print Prod:
Art Director: Proofreader:
Copywriter: Studio:
JOB #: ELIAHU-Q80204_BASE_Pg6_REV2 PROOF: 1
CLIENT: ELI LILLY & COMPANY OP: CV, JS
SPACE/SIZE: B: 8.75” x 11.25” T: 7.875” x 10.5” S: 7” x 10”
DATE:
THIS ADVERTISEMENT PREPARED BY TOWNHOUSE
CLIENT: ELI LILLY & COMPANY SIZE, SPACE: 7.875” x 10.5”, Journal Ad
PRODUCT: ABEMACICLIB US HCP PUBS: NCCN Journal Ad
JOB#: ELIAHU-Q80204_BASE_Pg6_REV2 ISSUE: 2018
ART DIRECTOR: J. Goody COPYWRITER: None
Please see Brief Summary of full Prescribing Information for Verzenio on the following pages.
References: 1. Verzenio [package insert]. Indianapolis, IN: Eli Lilly and Company; 2018. 2. Sledge GW Jr, Toi M, Neven P, et al. MONARCH 2: abemaciclib in combination with fulvestrant in women with HR+/HER2− advanced breast cancer who had progressed while receiving endocrine therapy. J Clin Oncol. 2017;35:2875-2884. 3. Goetz MP, Toi M, Campone M, et al. MONARCH 3: abemaciclib as initial therapy for advanced breast cancer. J Clin Oncol. 2017;35:3638-3646. 4. Dickler MN, Tolaney SM, Rugo HS, et al. MONARCH 1, a phase II study of abemaciclib, a CDK4 and CDK6 inhibitor, as a single agent, in patients with refractory HR+/HER2- metastatic breast cancer. Clin Cancer Res. 2017;23:5218-5224. 5. Imkampe A, Bendall S, Bates T. The signifi cance of the site of recurrence to subsequent breast cancer survival. Eur J Surg Oncol. 2007;33:420-423. 6. Largillier R, Ferrero JM, Doyen J, et al. Prognostic factors in 1038 women with metastatic breast cancer. Ann Oncol. 2008;19:2012-2019 7. Solomayer EF, Diel IJ, Meyberg GC, Gollan C, Bastert G. Metastatic breast cancer: clinical course, prognosis and therapy related to the fi rst site of metastasis. Breast Cancer Res Treat. 2000;59:271-278. 8. Cardoso F, Costa A, Senkus E, et al. 3rd ESO–ESMO international consensus guidelines for advanced breast cancer (ABC 3). Breast. 2017;31:244-259. 9. Gerratana L, Fanotto V, Bonotto M, et al. Pattern of metastasis and outcome in patients with breast cancer. Clin Exp Metastasis. 2015;32:125-133. 10. Vogel CL, Azevedo S, Hilsenbeck S, East DR, Ayub J. Survival after fi rst recurrence of breast cancer: the Miami experience. Cancer. 1992;70:129-135. 11. Chang J, Clark GM, Allred DC, Mohsin S, Chamness G, Elledge RM. Survival of patients with metastatic breast carcinoma: importance of prognostic markers of the primary tumor. Cancer. 2003;97:545-553. 12. Yamamoto N, Watanabe T, Katsumata N, et al. Construction and validation of a practical prognostic index for patients with metastatic breast cancer. J Clin Oncol. 1998;16:2401-2408. 13. Data on fi le. Lilly USA, LLC. ONC20180108a. 14. Data on fi le. Lilly USA, LLC. ONC20180328a. 15. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228-247. 16. Data on fi le. Lilly USA, LLC. ONC20180103a. 17. Data on fi le. Lilly USA, LLC. ONC20171128a. 18. Data on fi le. Lilly USA, LLC. ONC20171201a. 19. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Breast Cancer V.1.2018. © National Comprehensive Cancer Network, Inc. 2018. All rights reserved. Accessed March 22, 2018. To view the most recent and complete version of the guideline, go online to NCCN.org.
PP-AL-US-0970 05/2018 ©Lilly USA, LLC 2018. All rights reserved. Verzenio® is a registered trademark owned or licensed by Eli Lilly and Company, its subsidiaries or affi liates.
verzenio.com/hcp MORE DATA ATDISCOVER
S:7”
S:10”
T:7.875”
T:10.5”
B:8.75”
B:11.25”
200 FIFTH AVENUE NEW YORK, NY 10010
LEGAL RELEASE STATUS
AD APPROVAL
Release has been obtained Legal Coord:
Acct Mgmt: Print Prod:
Art Director: Proofreader:
Copywriter: Studio:
JOB #: ELIAHU-Q80146_Base PROOF: 1
CLIENT: Eli Lilly & Co OP: ND
SPACE/SIZE: B: None T: 7” x 10” S: None
DATE:
THIS ADVERTISEMENT PREPARED BY TOWNHOUSE
CLIENT: Eli Lilly & Co SIZE, SPACE: 7” x 10”, BW
PRODUCT: Abemaciclib PUBS: magazine
JOB#: ELIAHU-Q80146_Base ISSUE: 2018
ART DIRECTOR: J. Goody COPYWRITER: J. Wood
VERZENIO™ (abemaciclib) tablets, for oral use AL HCP BS 26FEB2018 VERZENIO™ (abemaciclib) tablets, for oral use AL HCP BS 26FEB2018
Verzenio, AL HCP BS 26FEB2018 - 7 x 10 PRINTER VERSION 1 OF 5
VERZENIO™ (abemaciclib) tablets, for oral use
Initial U.S. Approval: 2017
BRIEF SUMMARY: Consult the package insert for complete prescribing information.
INDICATIONS AND USAGE
VERZENIO™ (abemaciclib) is indicated:
breast cancer.
CONTRAINDICATIONS: None
WARNINGS AND PRECAUTIONS
Diarrhea
and MONARCH 1.
Neutropenia
.
Hepatotoxicity
Venous Thromboembolism
Embryo-Fetal Toxicity
ADVERSE REACTIONS Clinical Studies Experience
Postmenopausal Women with HR-positive, HER2-negative locoregionally recurrent or metastatic breast cancer with no prior systemic therapy in this disease setting
T:7”
T:10”
200 FIFTH AVENUE NEW YORK, NY 10010
LEGAL RELEASE STATUS
AD APPROVAL
Release has been obtained Legal Coord:
Acct Mgmt: Print Prod:
Art Director: Proofreader:
Copywriter: Studio:
JOB #: ELIAHU-Q80146_Base PROOF: 1
CLIENT: Eli Lilly & Co OP: ND
SPACE/SIZE: B: None T: 7” x 10” S: None
DATE:
THIS ADVERTISEMENT PREPARED BY TOWNHOUSE
CLIENT: Eli Lilly & Co SIZE, SPACE: 7” x 10”, BW
PRODUCT: Abemaciclib PUBS: magazine
JOB#: ELIAHU-Q80146_Base ISSUE: 2018
ART DIRECTOR: J. Goody COPYWRITER: J. Wood
VERZENIO™ (abemaciclib) tablets, for oral use AL HCP BS 26FEB2018 VERZENIO™ (abemaciclib) tablets, for oral use AL HCP BS 26FEB2018
Verzenio, AL HCP BS 26FEB2018 - 7 x 10 PRINTER VERSION 2 OF 5
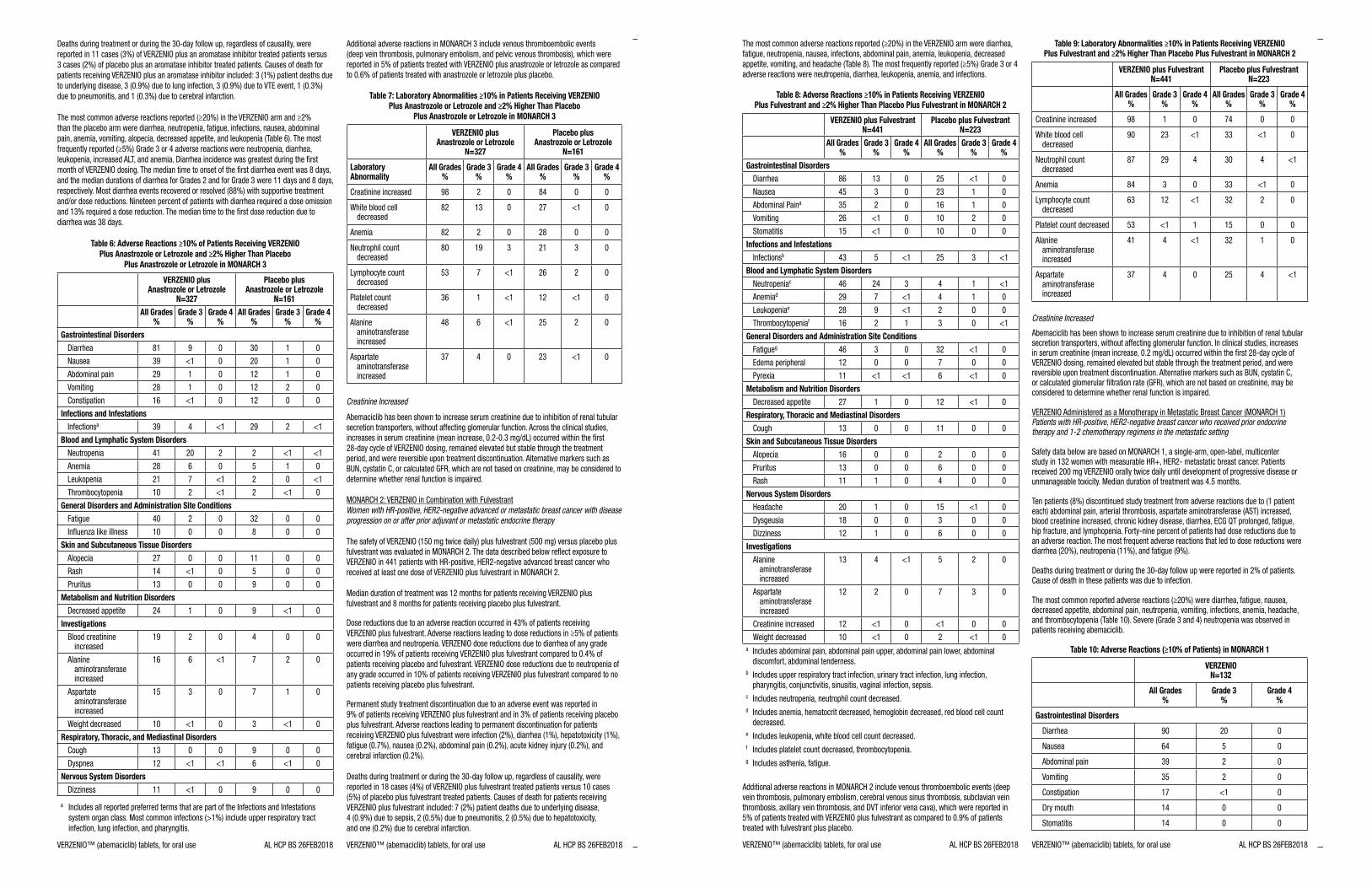
Table 6: Adverse Reactions ≥10% of Patients Receiving VERZENIO
Plus Anastrozole or Letrozole and ≥2% Higher Than Placebo
Plus Anastrozole or Letrozole in MONARCH 3
VERZENIO plusAnastrozole or Letrozole
N=327
Placebo plusAnastrozole or Letrozole
N=161
All Grades%
Grade 3%
Grade 4%
All Grades%
Grade 3%
Grade 4%
Gastrointestinal Disorders
81 9 0 30 1 0
39 0 20 1 0
29 1 0 12 1 0
28 1 0 12 2 0
16 0 12 0 0
Infections and Infestationsa 39 29 2
Blood and Lymphatic System Disorders
20 2 2
Anemia 28 6 0 5 1 0
21 7 2 0
10 2 2 0
General Disorders and Administration Site Conditions
2 0 32 0 0
10 0 0 8 0 0
Skin and Subcutaneous Tissue Disorders
27 0 0 11 0 0
0 5 0 0
13 0 0 9 0 0
Metabolism and Nutrition Disorders
1 0 9 0
Investigations
Blood creatinine increased
19 2 0 0 0
Alanine
increased
16 6 7 2 0
increased
15 3 0 7 1 0
10 0 3 0
Respiratory, Thoracic, and Mediastinal Disorders
13 0 0 9 0 0
12 6 0
Nervous System Disorders
Dizziness 11 0 9 0 0
a
Table 7: Laboratory Abnormalities ≥10% in Patients Receiving VERZENIO
Plus Anastrozole or Letrozole and ≥2% Higher Than Placebo
Plus Anastrozole or Letrozole in MONARCH 3
VERZENIO plusAnastrozole or Letrozole
N=327
Placebo plusAnastrozole or Letrozole
N=161
Laboratory Abnormality
All Grades%
Grade 3%
Grade 4%
All Grades%
Grade 3%
Grade 4%
Creatinine increased 98 2 0 0 0
decreased82 13 0 27 0
Anemia 82 2 0 28 0 0
decreased80 19 3 21 3 0
decreased53 7 26 2 0
decreased36 1 12 0
Alanine
increased
6 25 2 0
increased
37 0 23 0
Creatinine Increased
Women with HR-positive, HER2-negative advanced or metastatic breast cancer with disease
progression on or after prior adjuvant or metastatic endocrine therapy
T:7”
T:10”
200 FIFTH AVENUE NEW YORK, NY 10010
LEGAL RELEASE STATUS
AD APPROVAL
Release has been obtained Legal Coord:
Acct Mgmt: Print Prod:
Art Director: Proofreader:
Copywriter: Studio:
JOB #: ELIAHU-Q80146_Base PROOF: 1
CLIENT: Eli Lilly & Co OP: ND
SPACE/SIZE: B: None T: 7” x 10” S: None
DATE:
THIS ADVERTISEMENT PREPARED BY TOWNHOUSE
CLIENT: Eli Lilly & Co SIZE, SPACE: 7” x 10”, BW
PRODUCT: Abemaciclib PUBS: magazine
JOB#: ELIAHU-Q80146_Base ISSUE: 2018
ART DIRECTOR: J. Goody COPYWRITER: J. Wood
VERZENIO™ (abemaciclib) tablets, for oral use AL HCP BS 26FEB2018 VERZENIO™ (abemaciclib) tablets, for oral use AL HCP BS 26FEB2018
Verzenio, AL HCP BS 26FEB2018 - 7 x 10 PRINTER VERSION 3 OF 5
Table 8: Adverse Reactions ≥10% in Patients Receiving VERZENIO Plus Fulvestrant and ≥2% Higher Than Placebo Plus Fulvestrant in MONARCH 2
VERZENIO plus FulvestrantN=441
Placebo plus FulvestrantN=223
All Grades%
Grade 3%
Grade 4%
All Grades%
Grade 3%
Grade 4%
Gastrointestinal Disorders
86 13 0 25 0
3 0 23 1 0
Abdominal Paina 35 2 0 16 1 0
26 0 10 2 0
Stomatitis 15 0 10 0 0
Infections and Infestationsb 5 25 3
Blood and Lymphatic System Disordersc 3 1
Anemiad 29 7 1 0e 28 9 2 0 0
16 2 1 3 0
General Disorders and Administration Site Conditions
3 0 32 0
12 0 0 7 0 0
11 6 0
Metabolism and Nutrition Disorders
27 1 0 12 0
Respiratory, Thoracic and Mediastinal Disorders
13 0 0 11 0 0
Skin and Subcutaneous Tissue Disorders
16 0 0 2 0 0
13 0 0 6 0 0
11 1 0 0 0
Nervous System Disorders
20 1 0 15 0
18 0 0 3 0 0
Dizziness 12 1 0 6 0 0
Investigations
Alanine
increased
13 5 2 0
increased
12 2 0 7 3 0
Creatinine increased 12 0 0 0
10 0 2 0
a
b
c
d
decreased.
e
Table 9: Laboratory Abnormalities ≥10% in Patients Receiving VERZENIO Plus Fulvestrant and ≥2% Higher Than Placebo Plus Fulvestrant in MONARCH 2
VERZENIO plus FulvestrantN=441
Placebo plus FulvestrantN=223
All Grades%
Grade 3%
Grade 4%
All Grades%
Grade 3%
Grade 4%
Creatinine increased 98 1 0 0 0
decreased90 23 33 0
decreased87 29 30
Anemia 3 0 33 0
decreased63 12 32 2 0
53 1 15 0 0
Alanine
increased
32 1 0
increased
37 0 25
Creatinine Increased
Patients with HR-positive, HER2-negative breast cancer who received prior endocrine therapy and 1-2 chemotherapy regimens in the metastatic setting
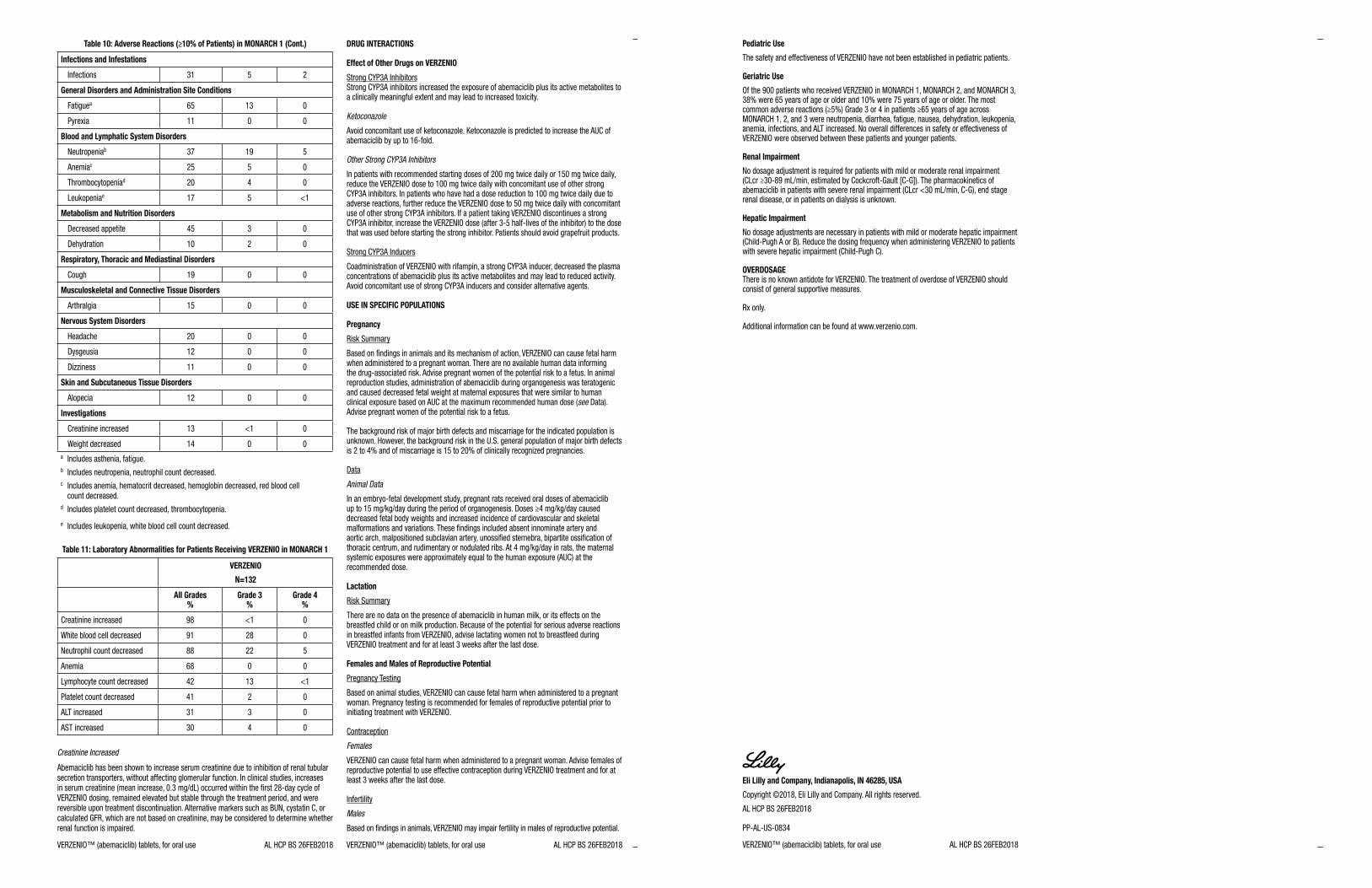
Table 10: Adverse Reactions (≥10% of Patients) in MONARCH 1
VERZENIO N=132
All Grades %
Grade 3 %
Grade 4 %
Gastrointestinal Disorders
90 20 0
5 0
39 2 0
35 2 0
17 0
0 0
Stomatitis 0 0
T:7”
T:10”
200 FIFTH AVENUE NEW YORK, NY 10010
LEGAL RELEASE STATUS
AD APPROVAL
Release has been obtained Legal Coord:
Acct Mgmt: Print Prod:
Art Director: Proofreader:
Copywriter: Studio:
JOB #: ELIAHU-Q80146_Base PROOF: 1
CLIENT: Eli Lilly & Co OP: ND
SPACE/SIZE: B: None T: 7” x 10” S: None
DATE:
THIS ADVERTISEMENT PREPARED BY TOWNHOUSE
CLIENT: Eli Lilly & Co SIZE, SPACE: 7” x 10”, BW
PRODUCT: Abemaciclib PUBS: magazine
JOB#: ELIAHU-Q80146_Base ISSUE: 2018
ART DIRECTOR: J. Goody COPYWRITER: J. Wood
VERZENIO™ (abemaciclib) tablets, for oral use AL HCP BS 26FEB2018 VERZENIO™ (abemaciclib) tablets, for oral use AL HCP BS 26FEB2018
Infections and Infestations
31 5 2
General Disorders and Administration Site Conditions
a 65 13 0
11 0 0
Blood and Lymphatic System Disorders
b 37 19 5
Anemiac 25 5 0
d 20 0
e 17 5
Metabolism and Nutrition Disorders
3 0
10 2 0
Respiratory, Thoracic and Mediastinal Disorders
19 0 0
Musculoskeletal and Connective Tissue Disorders
15 0 0
Nervous System Disorders
20 0 0
12 0 0
Dizziness 11 0 0
Skin and Subcutaneous Tissue Disorders
12 0 0
Investigations
Creatinine increased 13 0
0 0
a
b
c
d
e
Table 11: Laboratory Abnormalities for Patients Receiving VERZENIO in MONARCH 1
VERZENIO
N=132
All Grades %
Grade 3 %
Grade 4 %
Creatinine increased 98 0
91 28 0
88 22 5
Anemia 68 0 0
13
2 0
ALT increased 31 3 0
AST increased 30 0 Creatinine Increased
DRUG INTERACTIONS Effect of Other Drugs on VERZENIO
Ketoconazole
Other Strong CYP3A Inhibitors
USE IN SPECIFIC POPULATIONS Pregnancy
see Data).
Data Animal Data
recommended dose. Lactation
Females and Males of Reproductive Potential
Females
Males
Table 10: Adverse Reactions (≥10% of Patients) in MONARCH 1 (Cont.)
T:7”
T:10”
200 FIFTH AVENUE NEW YORK, NY 10010
LEGAL RELEASE STATUS
AD APPROVAL
Release has been obtained Legal Coord:
Acct Mgmt: Print Prod:
Art Director: Proofreader:
Copywriter: Studio:
JOB #: ELIAHU-Q80146_Base PROOF: 1
CLIENT: Eli Lilly & Co OP: ND
SPACE/SIZE: B: None T: 7” x 10” S: None
DATE:
THIS ADVERTISEMENT PREPARED BY TOWNHOUSE
CLIENT: Eli Lilly & Co SIZE, SPACE: 7” x 10”, BW
PRODUCT: Abemaciclib PUBS: magazine
JOB#: ELIAHU-Q80146_Base ISSUE: 2018
ART DIRECTOR: J. Goody COPYWRITER: J. Wood
Verzenio, AL HCP BS 26FEB2018 - 7 x 10 PRINTER VERSION 5 OF 5
Pediatric Use
Geriatric Use
Renal Impairment
Hepatic Impairment
OVERDOSAGE
Eli Lilly and Company, Indianapolis, IN 46285, USA
AL HCP BS 26FEB2018
T:7”
T:10”
22 | Oncologistics Oncologistics | 23
Medicare Changes Rules for Local Coverage DeterminationsBy Aileen Soper
in the development of an LCD. MACs can host CAC meetings in various ways (eg, in-person, telephone, video, webinar). MACs determine how frequently these meetings occur based on the appropriateness and volume of LCDs requiring CAC input. CAC meetings will be open to the public.
◾ Opening CAC membership to include patients and non-physician healthcare professionals such as nurses and social workers
◾ Opening meetings in the MAC jurisdiction to present proposed coverage, including evidence and rationale of decisions
◾ Retiring proposed policies if they are not finalized within one year of the original posting date
◾ Removing codes such as International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) and Current Procedure Terminology (CPT®) diagnosis and procedure codes from LCDs. The codes will instead be listed in coverage articles that can be linked to the LCD.
◾ Linking MAC responses to public comments to the final LCD and maintaining them in the Medicare Coverage Database indefinitely
◾ Creating a reconsideration process for LCDs that is consistent with the NCD reconsideration process
Stakeholders can submit feedback to CMS on their experiences with the revised LCD process to [email protected]. The agency says it will consider future revisions to the LCD process requirements based on the feedback.
1. Centers for Medicare & Medicaid Services (CMS). CMS Accelerates Innovation and Promotes Patient Access to Medical Technology. October 3, 2018. https://www.cms.gov/newsroom/press-releases/cms-accelerates-innovation-and-promotes-patient-access-medical-technology. Accessed October 5, 2018.
2. Centers for Medicare & Medicaid Services (CMS). Fact Sheet: Summary of Significant Changes to the Medicare Program Integrity Manual Chapter 13 – Local Coverage Determinations. October 3, 2018. https://www.cms.gov/newsroom/fact-sheets/summary-significant-changes-medicare-program-integrity-manual-chapter-13-local-coverage. Accessed October 5, 2018.
Aileen Soper is assistant director, Reimbursement Strategy and Tactics, with Xcenda, a part of AmerisourceBergen.
The Centers for Medicare & Medicaid Services (CMS) is overhauling the process its contractors follow to develop local coverage policies.
The policies, known as local coverage determinations (LCD), determine how most things—from injectable oncolytics to evaluation and management services for cancer patients—are covered under the Medicare Part A and B benefits.
Medicare Administrative Contractors (MAC) can issue LCDs when national coverage determinations (NCD) do not exist or when MACs need to further define covered services. In cases where a MAC does not have an LCD or there is no applicable NCD, services are reviewed for coverage on a case-by-case basis.
The updated instructions, policies and procedures will be added to chapter 13 of the Medicare Program Integrity Manual. The move is how the Medicare program is addressing Congress’ requirement in section 4009 of the 21st Century Cures Act for a more transparent LCD process.
The reforms are intended to increase transparency and patient engagement to ensure that Medicare beneficiaries have access to the latest therapies and devices, CMS said in a news release.1
According to a CMS fact sheet, the changes to the LCD process include:2
◾ Publishing a step-by-step description of the LCD process in language intended to be accessible to all stakeholders
◾ Standardizing presentation of clinical evidence that supports LCD decisions and rationale for MAC coverage determinations
◾ Providing an option to request an informal meeting with the MAC to discuss potential LCD requests
◾ Implementing a new process by which interested parties in a MAC jurisdiction can request a new LCD
◾ Restructuring Contractor Advisory Committee (CAC) meetings. CAC members serve in an advisory capacity to review the quality of the evidence used
Reimbursement Watch
MIPS TipsInformation to help your practice successfully meet all MIPS measures
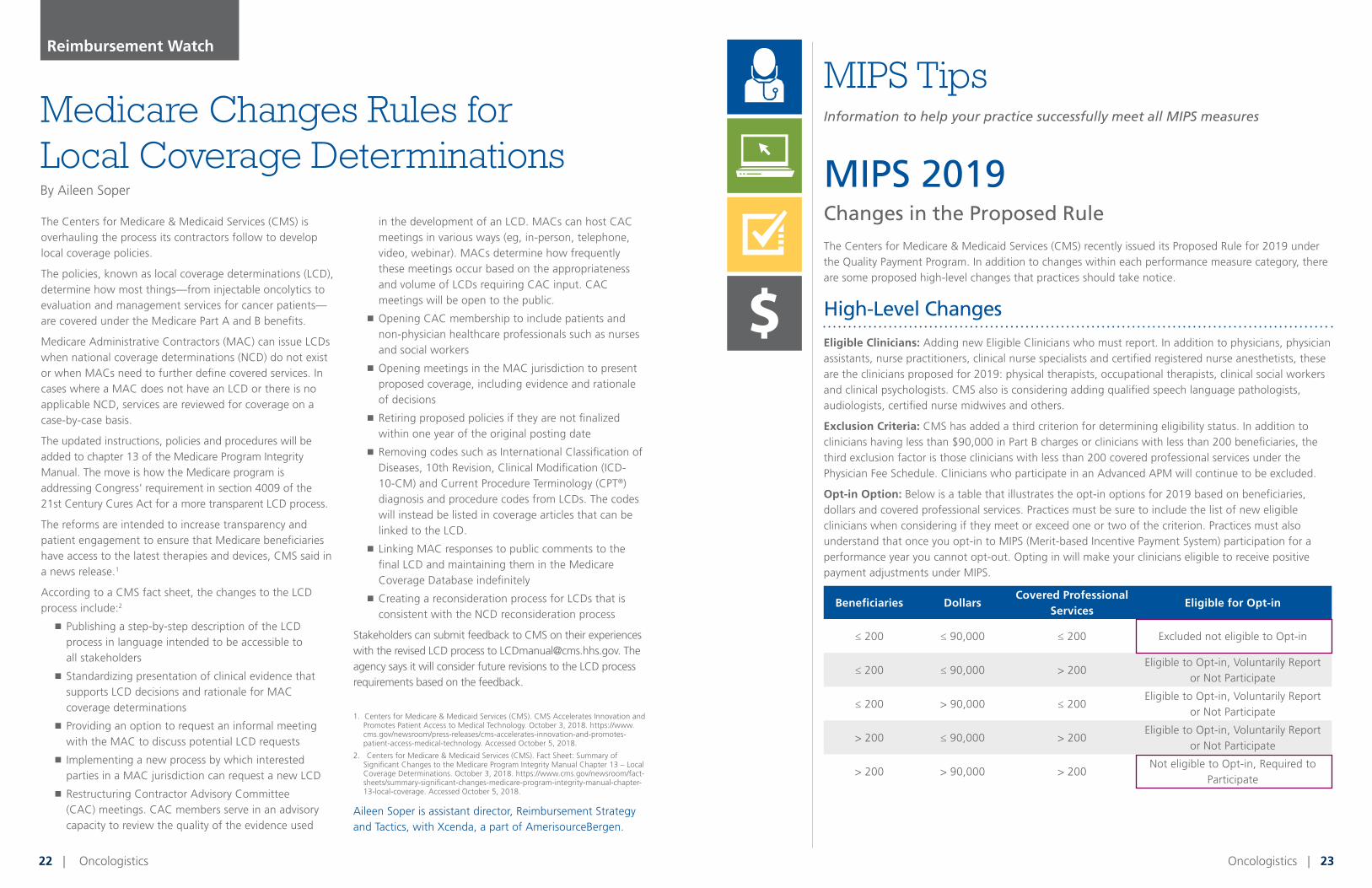
MIPS 2019 Changes in the Proposed Rule The Centers for Medicare & Medicaid Services (CMS) recently issued its Proposed Rule for 2019 under the Quality Payment Program. In addition to changes within each performance measure category, there are some proposed high-level changes that practices should take notice.
High-Level Changes
Eligible Clinicians: Adding new Eligible Clinicians who must report. In addition to physicians, physician assistants, nurse practitioners, clinical nurse specialists and certified registered nurse anesthetists, these are the clinicians proposed for 2019: physical therapists, occupational therapists, clinical social workers and clinical psychologists. CMS also is considering adding qualified speech language pathologists, audiologists, certified nurse midwives and others.
Exclusion Criteria: CMS has added a third criterion for determining eligibility status. In addition to clinicians having less than $90,000 in Part B charges or clinicians with less than 200 beneficiaries, the third exclusion factor is those clinicians with less than 200 covered professional services under the Physician Fee Schedule. Clinicians who participate in an Advanced APM will continue to be excluded.
Opt-in Option: Below is a table that illustrates the opt-in options for 2019 based on beneficiaries, dollars and covered professional services. Practices must be sure to include the list of new eligible clinicians when considering if they meet or exceed one or two of the criterion. Practices must also understand that once you opt-in to MIPS (Merit-based Incentive Payment System) participation for a performance year you cannot opt-out. Opting in will make your clinicians eligible to receive positive payment adjustments under MIPS.
Beneficiaries DollarsCovered Professional
ServicesEligible for Opt-in
≤ 200 ≤ 90,000 ≤ 200 Excluded not eligible to Opt-in
≤ 200 ≤ 90,000 > 200Eligible to Opt-in, Voluntarily Report
or Not Participate
≤ 200 > 90,000 ≤ 200Eligible to Opt-in, Voluntarily Report
or Not Participate
> 200 ≤ 90,000 > 200Eligible to Opt-in, Voluntarily Report
or Not Participate
> 200 > 90,000 > 200Not eligible to Opt-in, Required to
Participate
Option 1
QUALITYADVANCING CARE
INFORMATION
IMPROVEMENTACTIVITIES
QUALITY
ADVANCING CAREINFORMATION
IMPROVEMENTACTIVITIES
COST
COST
Option 2
Option 3
24 | Oncologistics Oncologistics | 25
The comment period for the
2019 Proposed Rule closed in
September. We expect the Final
Rule on the proposals to be
released in November.
Performance Threshold Points: The minimum number of points needed to avoid a downward adjustment in reimbursement moves from 15 points to 30 points in 2019.
Category Reweighting: Categories are reweighted in 2019 to include Quality at 45 percent, Promoting Interoperability at 25 percent, Cost at 15 percent and Improvement Activities at 15 percent.
Payment Adjustments: Payment adjustment for the performance year of 2017 (payment year of 2019) are +/-4 percent; in the 2018 performance year (payment year of 2020) it is +/- 5 percent; in the 2019 performance year (payment year of 2021) the payment adjustment increases to +/-7 percent.
Quality Category
CMS will apply the general rules as the agency has done before in the proposed Quality category. Practices or providers will report six measures with one being an outcome measure. The category continues to be 45 percent of the final score and data completeness is at 60 percent. Eligible clinicians and groups can report Quality measures across multiple collection types, including registry, EHRs and claims.
One of their most significant proposed changes is to the measures that can be selected for reporting. CMS plans to implement 10 new measures, but also to eliminate 33 other measures. Some practices may currently be using those measures in reporting, so CMS encouraged practices to review both sets of measures—those new and those scheduled for removal. The change in measures may impact some practices, especially those measuring Hypertension: Improvement in Blood Pressure or performing a Functional Status Assessment for Total Knee Replacement, as two examples of measures being removed.
CMS also has proposed to create new terms around Collection Type (eCQMs in place of EHR reporting), Submitter Type and Submission Type (Direct submission indicating computer to computer instead of EHR reporting).
As part of the focus on prescription drug abuse, high-priority measures will now encompass opioid-related measures.
In 2019, small practices (15 or fewer eligible clinicians) will automatically receive three bonus points in the Quality category. Bonus point caps will continue, using 10 percent of the total possible points for high-priority bonus points and CEHRT bonus points.
CMS is also considering measure reweighting. If clinical guidelines greatly impact a measure during the performance year, CMS would reweight the measure to zero to protect patient safety; and if your practice opted to report CAHPS but did not have enough beneficiaries to meet the case minimum, CMS will reweight the measure to zero.
Promoting Interoperability
CMS has proposed several changes to the Promoting Interoperability category (formerly Meaningful Use and Advancing Care Information) for 2019, including significantly reducing the number of measures that are available. It is expected that the proposed changes will make it more difficult for practices to achieve the full 25 points in this category.
As an example, to earn the full 25 points for the category in 2018, practices or eligible clinicians need to earn 100 out of 165 points available. In 2019, only 110 total points are available in the category, and that includes a 10-point bonus if you are able to report on a new measure and EPCS (Electronic Prescriptions for Controlled Substances) is available in your state. The following year, 2020, practices will have to earn the entire 100 total points in the category to gain those 25 composite points.
The measures proposed for removal in this category include:
◾ Patient-specific Education
◾ Secure Messaging
◾ View, Download and Transmit
◾ Patient-generated Health Data
◾ Clinical Information Reconciliation*
◾ Request/Accept Summary of Care*
(*These last two measures will be combined into a new category called Support Electronic Referral Loops Receiving and Incorporating Health Information.)
More emphasis will be placed on the issue of prescription drug abuse. New measures to address those include Query of Prescription Drug Monitoring (PDMP) and Verify Opioid Treatment Agreement. Practices will be excluded from reporting on these measures if the practice or provider cannot e-prescribe Schedule II opioids.
In addition, a Security Risk Analysis is not a scored measure, but it still will be required to achieve any points in this category.
MIPS TIPS
Practices will have to report a minimum of 90 days up to the full calendar year for 2019 measures and will be required to use the 2015 Edition CEHRT. The 2014 Edition will not be an option.
Keep in Mind:
◾ The reporting period is a minimum of 90 days.
◾ Claiming exclusions does not always help you. If you can meet the measure, that will help your score.
◾ Be prepared to use secure transmission methods to send and receive referrals. Check with other providers involved in your patient’s care to understand their methods so you are prepared to accept and send.
◾ Check with your EHR vendor on available transmission methods; PDMP and Opioid Agreement verification for those bonus points; and EPCS, if allowed in your state.
Improvement Activities
CMS does not plan to change the weighting to the final score from 15 percent (as it was in the 2018 performance year). They also maintain that activities are to be performed for at least a continuous 90 days during the performance period.
CMS is proposing to remove the previous bonus points to align with the new Promoting Interoperability scoring requirements.
For the number of activities, clinicians will still need to reach a total of 40 points but will have six new Improvement Activities (IA), five activities will be modified and one existing activity will be removed from the IA inventory. The number of activities for small practices or clinicians located in rural or HPSAs has not changed. They will continue to report on no more than two medium or one high-weighted activity to reach the highest score.
Cost
CMS continues to place increasing emphasis on cost and quality for MIPS Reporting.
In the Cost category, CMS will continue to look at claims data, but the performance measure will be weighted more heavily each year. The percentage increases five percent each year, topping off at 30 percent of the total. In 2019, the proposed weighting will be 15 percent, up from 10 percent in the 2018 performance year.
The Total Per Capita Cost (TPCC) and Medicare Spending per Beneficiary (MSPB) measures will work similar to past years. Benchmarks will be made based on comparisons to your peers in your specialty but will not look at historical data.
If your practice does not meet the minimums (applicable to your practice or provider), your cost category moves to additional weighting on your Quality performance measure. You will be scored on as many measures that meet the case minimum. If only one measure can be scored, that score will be the total Cost category score.
CMS is proposing to add eight new episode-based measures that were field tested in 2017. The measures include:
◾ Elective Outpatient Percutaneous Coronary Intervention (PCI)
◾ Knee Arthroplasty
◾ Revascularization for Lower Extremity Chronic Critical Limb Ischemia
◾ Routine Cataract Removal with Intraocular Lens (IOL) Implantation
◾ Intracranial Hemorrhage or Cerebral Infarction
◾ Simple Pneumonia with Hospitalization
◾ ST-Elevation Myocardial Infarction (STEMI) with Percutaneous Coronary Intervention (PCI)
The comment period for the 2019 Proposed Rule closed in September. We expect the Final Rule on the proposals above to be released in November.
If you have additional questions about the 2019 Proposed Rule or questions about MIPS reporting, call 877-570-8721 x2 or send an email to [email protected].
Changes in the MIPS 2019 Proposed Rule
26 | Oncologistics Oncologistics | 27Visit IONonline.com/Precision to learn more.
Precision Medicine Center
NOW AVAILABLE
The ION Solutions Precision Medicine Center is your gateway to a single,
centralized library of precision medicine testing recommendations and
resources. Access all of the testing recommendations created by our
physician- and pharmacist-based advisory panel as well as resources
curated by ION Solutions and our precision medicine partners to help you
make informed decisions for your patients.
View testing recommendations by tumor categories:
■ Breast Cancer
■ NSCLC
■ Colorectal
■ Genitourinary
■ Lymphoma
■ Rare Disease
As precision medicine continues to evolve, ION will continue to provide the
tools that you need for your practice.

This is more than just lip-service.
As the pioneers of performance-based contracting, we have
always been focused on the future of community oncology. That
long-standing commitment remains as the healthcare landscape
evolves due to changing regulations and industry standards.
Your success is our success.
Our purpose is to ensure your viability as an independent
practice and to help you grow. That can’t be fulfilled if we are
not providing the results and resources that you need-
and that forges lasting partnerships.
Care for you, so that you can care for patients.
As patient needs evolve, so do the tools and resources you
depend upon to meet those needs. We do our part by
investing in technology, research and other resources to
help you elevate the quality of patient care.
The True Purpose of your GPO
True partners in service.
True leaders in industry.
True innovators in care.
www.iononline.com