umblical masses 17/09/2011 by: mohammed alsaidan
TRANSCRIPT
Umblical Masses 17/09/2011
BY: MOHAMMED ALSAIDAN


Umbilical granuloma

Umbilical granuloma
• Umbilical granuloma is is the most common cause of an umbilical mass.
• It is a soft, moist, pink, pedunculated, friable granulation tissue that varies in size from 3 to 10 mm in length which can secrete a small amount of serous or serosanguineous drainage

Umbilical granuloma
• Following separation of the cord, incomplete epithelialization may occur and reddish granulation tissue appear in the first few weeks of life
• More likely to occur when there is inflammation of the umbilical cord usually due to infection, which also delays cord separation.
• Granulation is a normal stage in wound healing, but may overgrow and result in the formation of umbilical granuloma

Treatment
• Eliminating the friction of a wet diaper , air drying with alcohol wipes may allow the granulation tissue to epithelialize
• The most common treatment is topical 75% silver nitrate, usually applied by a wooden applicator
• The lesion is treated once or twice/week for several weeks, but generally only a few applications are required for successful treatment.
• Silver nitrate can cause chemical burns or staining of the surrounding skin.
Umbilical granuloma
• Cryosurgery, electrocautery, salt, and ligature are other treatment options
• cryosurgery • associated with skin depigmentation, • repeated applications were unnecessary.• more rapid healing compared with the use of chemicals and
electrocautery.
• Twice daily application of common table salt to umbilical pyogenic granulomas for three days is a simple, cost-effective, and curative method that can be performed by parents at home.
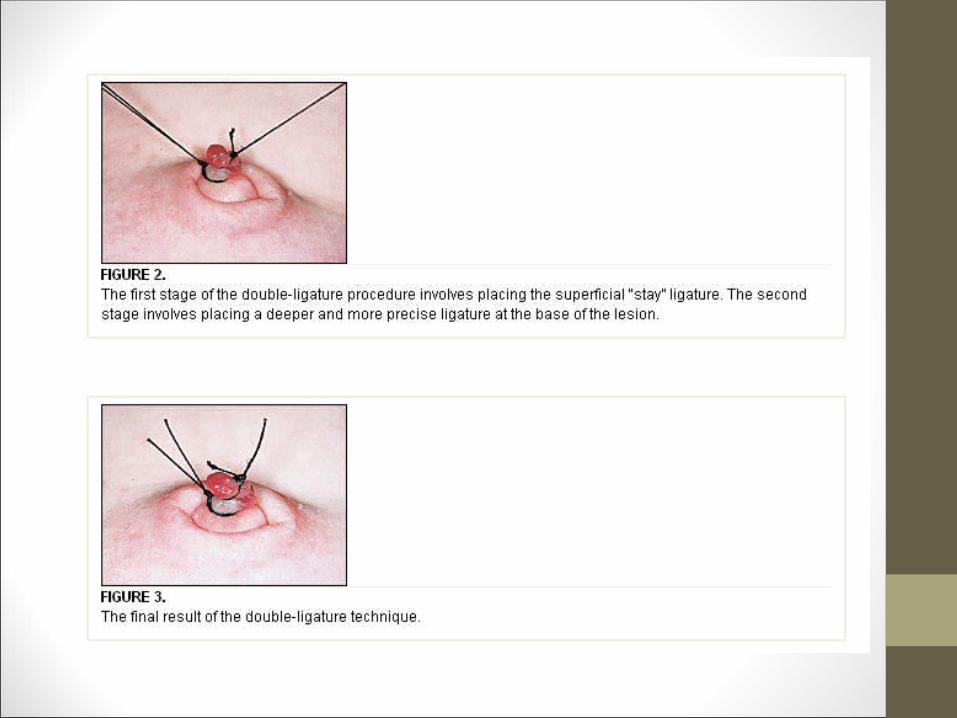
• The application of a double-ligature can be considered for pedunculated umbilical pyogenic granulomas.
Umbilical granuloma
• Ligation can be performed in the office without discomfort
• Before ligation, the umbilicus should be carefully examined to rule out other causes of umbilical masses
• The granuloma becomes necrotic and drops off within 7 to 14 days, similar to the original umbilical cord remnant
• Failure of the granuloma to resolve with ligation and/or silver nitrate should also increase the suspicion that the lesion is actually an umbilical polyp.

Umbilical granuloma
• Larger granulomas or those that do not resolve with the above measures may require surgical excision
• Contraindications for this double-ligature technique are the large sessile umbilical granulomas with a wide base, small deep lesions and very friable lesions
• The complications of this technique are minor and include bleeding, especially with large sessile umbilical granulomas. Some larger granulomas may require more than one double-ligature
Umbilical polyp
Umbilical polyp
• rare
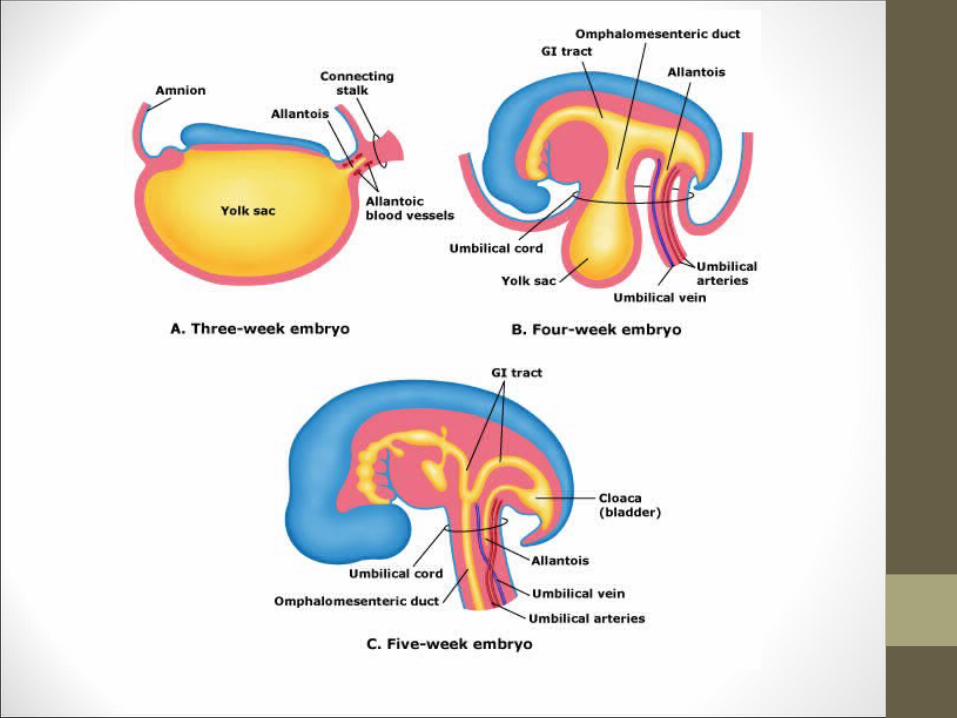
• Firm masses comprised of intestinal epithelium or uroepithelium, which are omphalomesenteric ductal or urachal embryologic remnants
• Often larger than granulomas



Umbilical polyp
• They do not respond to silver nitrate therapy, and require surgical excision.
• Histopathologic evaluation should be performed if it cannot be differentiated from granuloma
• If a polyp is diagnosed, further evaluation for associated embryologic anomalies
Umbilical polyp
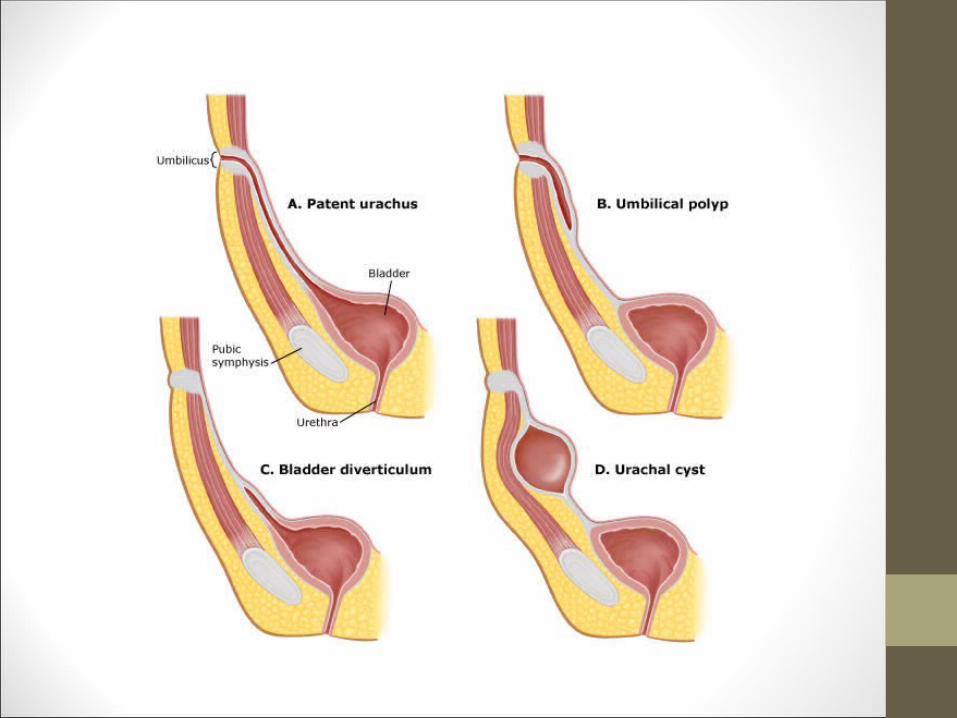
• For omphalomesenteric ductal anomalies ultrasonography and possibly a Meckel scan (99m technetium) should be performed
• For urachal embryologic remnants ,a sinogram (radiocontrast injection into urachal opening) is diagnostic for patent urachus and urachal sinus
• Renal ultrasound and voiding cystourethrogram should be obtained in all patients with urachal anomalies.
Umbilical hernia


Umbilical hernia
• After birth, the umbilical fascial opening closes spontaneously with continued growth of the rectus abdominis muscles toward one another
• Closure of the umbilical ring is complete in almost all children by 5 years of age, but may be slower in black children
• Vast majority of pediatric patients with umbilical hernias are asymptomatic, unless complicated
Umbilical hernia
• Detected during the newborn abdominal examination, particularly during crying, easily reduced , rarely become incarcerated or strangulated .
• In general, asymptomatic children can be observed.
• Surgical intervention is required if incarcerated or without any decrease in the size over the first two years of life, specially if greater than 1.5 cm

Other differential diagnosis
Other DDx of umbilical mass
• Ectopic tissue : • Ectopic tissue in the umbilical cord is a rare lesion that presents
as a solid mass.
• Ectopic tissue can include pancreatic , or hepatic tissue .
• Surgical excision is required for its removal.

Other DDx of umbilical mass
• Hamartomas,• Nevi• Inclusion cysts• Hemangiomas• Dermatofibromas• Neurofibromas,• Lipomas• granular cell tumors, desmoid tumors• melanoma, squamous cell carcinoma, and basal cell
carcinoma.
Omphalitis
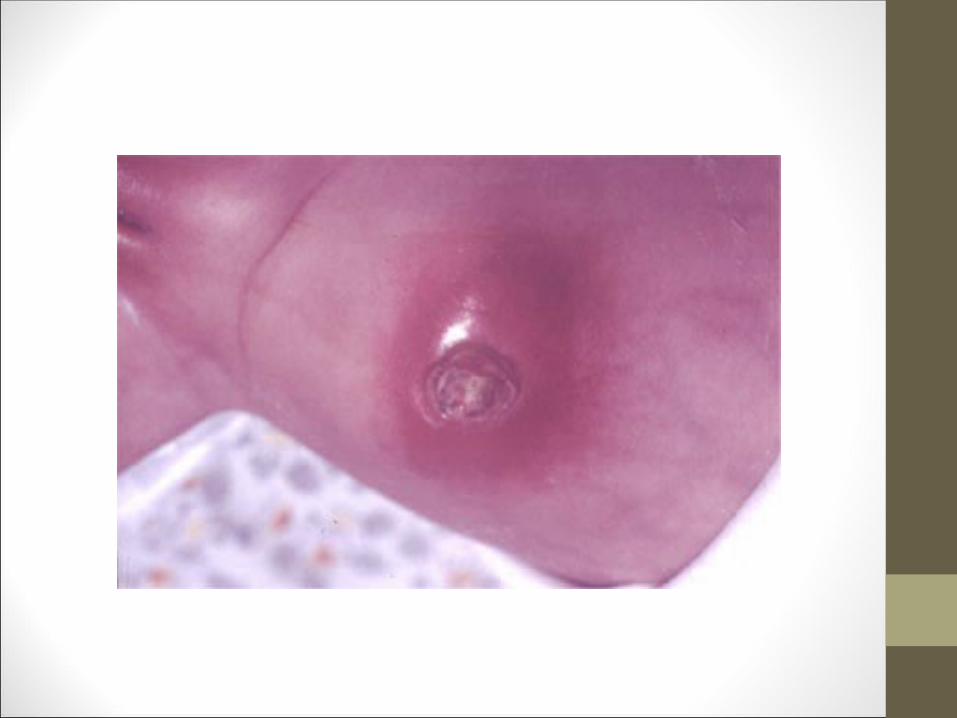
• It is a polymicrobial infection of the umbilicus and/or surrounding tissues.
• It is predominantly a disease of the neonate and is characterized by purulent discharge from the umbilical cord stump with surrounding induration, erythema, and tenderness +/- bleeding
• Complications include sepsis and necrotizing fasciitis, which has a high mortality rate.
• Antibiotic treatment of omphalitis is required with initial parenteral administration of antistaphylococcal and aminoglycoside agents to reduce the risk of severe complications

Thank you
