treatment pathways for intravitreal therapies in diabetic ...yorkshireretinasociety.com/pdfs/talks...
TRANSCRIPT
Treatment pathways for Intravitreal therapies in
Diabetic Macular Oedema (DMO)
Louise DowneyConsultant OphthalmologistMBChB BSc PhD FRCOphth
Disclosures and acknowledgements
bull Financial disclosuresbull Alcon Alimera Allergan Bayer Novartis Thrombogenics Orayabull Advisory board work travel grants speakers fees research studies
bull Elements of this slide deck were taken from Bayer published slide deck (UK DMO slide deck v 13) plus Allergan Alimera and Novartis slide decks
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull 1)What treatment should I start with at baselinebull 2)Re-treatment algorithms for intravitreal DMO
therapiesbull 3)When should I switchcombine therapiesbull 4)The bigger picture
bull Other eyeperipheral retinopathybull The patient as a wholebull The service -coping with capacity ndash compromises
DMO ndash treatment options1)What treatments should I use at baseline
bull ETDRS based laser therapies
bull ADJUNCT
bull Surgery ndash VMTERM
bull Pan-retinal photocoagulation
bull INTRAVITREAL
bull ANTI-VEGF
bull Lucentis (Ranibizumab)
bull Eylea (Aflibercept)
bull Avastin (Bevacizumab)
bull STEROIDS
bull Iluvien (Fluocinolone)
bull Ozurdex (Dexamethasone)
RCO recommendations for the treatment of CSMO
The Royal College of Ophthalmologists Diabetic Retinopathy Guidelines 2012
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
Fluocinolone is an option for eyes unresponsive to other treatments but potential side effects must be considered Triamcinolone +- adjunctive laser or fluocinolone may be considered for eyes unresponsive to other treatments
6
ETDRS based laser therapies = Clinically significant macular oedema (CSMO)
bull The ETDRS defined CSMO as DMO that threatens the centre of the macula (fovea)1 and forms the basis of current recommendations for the treatment of CSMO2
bull CSMO is diagnosed if any of the following parameters are met1
1 ETDRS Research Group Arch Ophthalmol 19851031796ndash1806 2 Bandello F et al Eye (Lond) 201226(4)485ndash493
1 Retinal thickening within 500 microm of the centre of the macula
2 Hard exudates within 500 microm of the centre of the macula if associated with thickening of the adjacent retina
3 Retinal thickening of gt1 disc area in size any part of which is located within 1 disc diameter of the centre of the macula
500 microm
500 microm
1 discdiameter
ge 1 discdiameter
Fovea
7
ETDRS = Early Treatment Diabetic Retinopathy Study
Date of Prep Jan 2015 LGB0820157252f
DMO ndash treatment optionsWhat treatments should I use at baseline
ETDRS based laser therapies = Clinically significant macular oedema (CSMO)
bull The ETDRS defined CSMO as DMO that threatens the centre of the macula (fovea)1 and forms the basis of current recommendations for the treatment of CSMO2
bull CSMO is diagnosed if any of the following parameters are met1
1 ETDRS Research Group Arch Ophthalmol 19851031796ndash1806 2 Bandello F et al Eye (Lond) 201226(4)485ndash493
1 Retinal thickening within 500 microm of the centre of the macula
2 Hard exudates within 500 microm of the centre of the macula if associated with thickening of the adjacent retina
3 Retinal thickening of gt1 disc area in size any part of which is located within 1 disc diameter of the centre of the macula
500 microm
500 microm
1 discdiameter
ge 1 discdiameter
Fovea
8
ETDRS = Early Treatment Diabetic Retinopathy Study
LASER
RCO recommendations for the treatment of CSMO
The Royal College of Ophthalmologists Diabetic Retinopathy Guidelines 2012
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
9
ILUVIEN (chronicunresponsive)
OZURXEX (no improvement)
DMO ndash treatment optionsWhat treatments should I use at baseline
bull ETDRS based laser therapies
bull ADJUNCT
bull Surgery ndash VMTERM
bull Pan-retinal photocoagulation
bull INTRAVITREAL
bull ANTI-VEGF
bull Lucentis (Ranibizumab)
bull Eylea (Aflibercept)
bull Avastin (Bevacizumab)
bull STEROIDS
bull Iluvien (Fluocinolone)
bull Ozurdex (Dexamethasone)
11
BOLT
RESOLVERISE and RIDERELIGHT
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
DMO ndash treatment optionsWhat treatments should I use at baseline ndash based on evidence from RCT data
What therapy do I choose for my patient at baselineWhich treatments can I access
NICE TA 274 Lucentis for DMO April 2013NICE TA 346 Eylea for DMO July 2015
NICE TA 301 Iluvien for DMO Nov 2013NICE TA 349 Ozurdex for DMO July 2015
OCT gt400um1st line if OCT suitable
bull Chronic DMObull PSEUDOPHAKICbull Patients ldquoinsufficiently responsive
to existing therapiesrdquo
bull PSEUDOPHAKICbull ldquoNot improved with non-
corticosteroid or such treatment is not suitable for themrdquo
What therapy do I choose for my patient at baseline
bull ANTI-VEGF
bull Superior to ETDRS argon laser in terms of efficacy
RESTORE 36 month Lucentis prn extension studyLucentis monotherapy vs Lucentis plus laser vs laser aloneSchmidt-Erfuth U et al Ophthalmology 2014 121(5) 1045-1053
23
Months
12
10
8
6
4
2
0
minus22 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Extension study (ranibizumab 05 mg PRN)Core study
Me
an o
f th
e c
han
ge in
ETD
RS
BC
VA
Prior ranibizumab 05 mg + active laser (n=83)
Prior sham injections + active laser (n=74)
Prior ranibizumab 05 mg + sham laser (n=83)
79
71 606780
Core study assessment
Full analysisstudy completionInterim analysis
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
15
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
RISE amp RIDE
Date of Prep Dec 2014 LGB0820147252X
02 Laser
125 2q4
107 2q8
0
Mea
n ch
ange
in B
CVA
lette
r sco
re
2
101214
02
6
10
14
4
8
12
468
09 Laser
115 2q4
111 2q8
VISTA Week 100
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
12 Laser
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
105 2q4
107 2q8VIVID Week 100
Week Laser 2q4 2q8
07 Laser
114 2q4
94 2q8
Eylea =VIVID and VISTA Mean change in BCVA to week 100Korobelnik J-F et al Ophthalmology 2014 121 (11) 2247ndash2254 Brown DM et al Ophthalmology 2015 Jul 18 [Epub ahead of print]
Plt00001 vs laser VIVID Laser n=132 2q4 n=136 2q8 n=135 VISTA Laser n=154 2q4 n=154 2q8 n=151Full analysis set 2q4 2 mg every 4 weeks 2q8 2 mg every 8 weeks BCVA best corrected visual acuity ETDRS Early Treatment Diabetic Retinopathy Study
What therapy do I choose for my patient at baseline
bull ANTI-VEGF helliphellipif OCT gt 400um
bull Sohellip Which one
Key trials in DMO
18
BOLT
RESOLVERISE and RIDE
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you
Disclosures and acknowledgements
bull Financial disclosuresbull Alcon Alimera Allergan Bayer Novartis Thrombogenics Orayabull Advisory board work travel grants speakers fees research studies
bull Elements of this slide deck were taken from Bayer published slide deck (UK DMO slide deck v 13) plus Allergan Alimera and Novartis slide decks
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull 1)What treatment should I start with at baselinebull 2)Re-treatment algorithms for intravitreal DMO
therapiesbull 3)When should I switchcombine therapiesbull 4)The bigger picture
bull Other eyeperipheral retinopathybull The patient as a wholebull The service -coping with capacity ndash compromises
DMO ndash treatment options1)What treatments should I use at baseline
bull ETDRS based laser therapies
bull ADJUNCT
bull Surgery ndash VMTERM
bull Pan-retinal photocoagulation
bull INTRAVITREAL
bull ANTI-VEGF
bull Lucentis (Ranibizumab)
bull Eylea (Aflibercept)
bull Avastin (Bevacizumab)
bull STEROIDS
bull Iluvien (Fluocinolone)
bull Ozurdex (Dexamethasone)
RCO recommendations for the treatment of CSMO
The Royal College of Ophthalmologists Diabetic Retinopathy Guidelines 2012
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
Fluocinolone is an option for eyes unresponsive to other treatments but potential side effects must be considered Triamcinolone +- adjunctive laser or fluocinolone may be considered for eyes unresponsive to other treatments
6
ETDRS based laser therapies = Clinically significant macular oedema (CSMO)
bull The ETDRS defined CSMO as DMO that threatens the centre of the macula (fovea)1 and forms the basis of current recommendations for the treatment of CSMO2
bull CSMO is diagnosed if any of the following parameters are met1
1 ETDRS Research Group Arch Ophthalmol 19851031796ndash1806 2 Bandello F et al Eye (Lond) 201226(4)485ndash493
1 Retinal thickening within 500 microm of the centre of the macula
2 Hard exudates within 500 microm of the centre of the macula if associated with thickening of the adjacent retina
3 Retinal thickening of gt1 disc area in size any part of which is located within 1 disc diameter of the centre of the macula
500 microm
500 microm
1 discdiameter
ge 1 discdiameter
Fovea
7
ETDRS = Early Treatment Diabetic Retinopathy Study
Date of Prep Jan 2015 LGB0820157252f
DMO ndash treatment optionsWhat treatments should I use at baseline
ETDRS based laser therapies = Clinically significant macular oedema (CSMO)
bull The ETDRS defined CSMO as DMO that threatens the centre of the macula (fovea)1 and forms the basis of current recommendations for the treatment of CSMO2
bull CSMO is diagnosed if any of the following parameters are met1
1 ETDRS Research Group Arch Ophthalmol 19851031796ndash1806 2 Bandello F et al Eye (Lond) 201226(4)485ndash493
1 Retinal thickening within 500 microm of the centre of the macula
2 Hard exudates within 500 microm of the centre of the macula if associated with thickening of the adjacent retina
3 Retinal thickening of gt1 disc area in size any part of which is located within 1 disc diameter of the centre of the macula
500 microm
500 microm
1 discdiameter
ge 1 discdiameter
Fovea
8
ETDRS = Early Treatment Diabetic Retinopathy Study
LASER
RCO recommendations for the treatment of CSMO
The Royal College of Ophthalmologists Diabetic Retinopathy Guidelines 2012
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
9
ILUVIEN (chronicunresponsive)
OZURXEX (no improvement)
DMO ndash treatment optionsWhat treatments should I use at baseline
bull ETDRS based laser therapies
bull ADJUNCT
bull Surgery ndash VMTERM
bull Pan-retinal photocoagulation
bull INTRAVITREAL
bull ANTI-VEGF
bull Lucentis (Ranibizumab)
bull Eylea (Aflibercept)
bull Avastin (Bevacizumab)
bull STEROIDS
bull Iluvien (Fluocinolone)
bull Ozurdex (Dexamethasone)
11
BOLT
RESOLVERISE and RIDERELIGHT
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
DMO ndash treatment optionsWhat treatments should I use at baseline ndash based on evidence from RCT data
What therapy do I choose for my patient at baselineWhich treatments can I access
NICE TA 274 Lucentis for DMO April 2013NICE TA 346 Eylea for DMO July 2015
NICE TA 301 Iluvien for DMO Nov 2013NICE TA 349 Ozurdex for DMO July 2015
OCT gt400um1st line if OCT suitable
bull Chronic DMObull PSEUDOPHAKICbull Patients ldquoinsufficiently responsive
to existing therapiesrdquo
bull PSEUDOPHAKICbull ldquoNot improved with non-
corticosteroid or such treatment is not suitable for themrdquo
What therapy do I choose for my patient at baseline
bull ANTI-VEGF
bull Superior to ETDRS argon laser in terms of efficacy
RESTORE 36 month Lucentis prn extension studyLucentis monotherapy vs Lucentis plus laser vs laser aloneSchmidt-Erfuth U et al Ophthalmology 2014 121(5) 1045-1053
23
Months
12
10
8
6
4
2
0
minus22 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Extension study (ranibizumab 05 mg PRN)Core study
Me
an o
f th
e c
han
ge in
ETD
RS
BC
VA
Prior ranibizumab 05 mg + active laser (n=83)
Prior sham injections + active laser (n=74)
Prior ranibizumab 05 mg + sham laser (n=83)
79
71 606780
Core study assessment
Full analysisstudy completionInterim analysis
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
15
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
RISE amp RIDE
Date of Prep Dec 2014 LGB0820147252X
02 Laser
125 2q4
107 2q8
0
Mea
n ch
ange
in B
CVA
lette
r sco
re
2
101214
02
6
10
14
4
8
12
468
09 Laser
115 2q4
111 2q8
VISTA Week 100
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
12 Laser
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
105 2q4
107 2q8VIVID Week 100
Week Laser 2q4 2q8
07 Laser
114 2q4
94 2q8
Eylea =VIVID and VISTA Mean change in BCVA to week 100Korobelnik J-F et al Ophthalmology 2014 121 (11) 2247ndash2254 Brown DM et al Ophthalmology 2015 Jul 18 [Epub ahead of print]
Plt00001 vs laser VIVID Laser n=132 2q4 n=136 2q8 n=135 VISTA Laser n=154 2q4 n=154 2q8 n=151Full analysis set 2q4 2 mg every 4 weeks 2q8 2 mg every 8 weeks BCVA best corrected visual acuity ETDRS Early Treatment Diabetic Retinopathy Study
What therapy do I choose for my patient at baseline
bull ANTI-VEGF helliphellipif OCT gt 400um
bull Sohellip Which one
Key trials in DMO
18
BOLT
RESOLVERISE and RIDE
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull 1)What treatment should I start with at baselinebull 2)Re-treatment algorithms for intravitreal DMO
therapiesbull 3)When should I switchcombine therapiesbull 4)The bigger picture
bull Other eyeperipheral retinopathybull The patient as a wholebull The service -coping with capacity ndash compromises
DMO ndash treatment options1)What treatments should I use at baseline
bull ETDRS based laser therapies
bull ADJUNCT
bull Surgery ndash VMTERM
bull Pan-retinal photocoagulation
bull INTRAVITREAL
bull ANTI-VEGF
bull Lucentis (Ranibizumab)
bull Eylea (Aflibercept)
bull Avastin (Bevacizumab)
bull STEROIDS
bull Iluvien (Fluocinolone)
bull Ozurdex (Dexamethasone)
RCO recommendations for the treatment of CSMO
The Royal College of Ophthalmologists Diabetic Retinopathy Guidelines 2012
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
Fluocinolone is an option for eyes unresponsive to other treatments but potential side effects must be considered Triamcinolone +- adjunctive laser or fluocinolone may be considered for eyes unresponsive to other treatments
6
ETDRS based laser therapies = Clinically significant macular oedema (CSMO)
bull The ETDRS defined CSMO as DMO that threatens the centre of the macula (fovea)1 and forms the basis of current recommendations for the treatment of CSMO2
bull CSMO is diagnosed if any of the following parameters are met1
1 ETDRS Research Group Arch Ophthalmol 19851031796ndash1806 2 Bandello F et al Eye (Lond) 201226(4)485ndash493
1 Retinal thickening within 500 microm of the centre of the macula
2 Hard exudates within 500 microm of the centre of the macula if associated with thickening of the adjacent retina
3 Retinal thickening of gt1 disc area in size any part of which is located within 1 disc diameter of the centre of the macula
500 microm
500 microm
1 discdiameter
ge 1 discdiameter
Fovea
7
ETDRS = Early Treatment Diabetic Retinopathy Study
Date of Prep Jan 2015 LGB0820157252f
DMO ndash treatment optionsWhat treatments should I use at baseline
ETDRS based laser therapies = Clinically significant macular oedema (CSMO)
bull The ETDRS defined CSMO as DMO that threatens the centre of the macula (fovea)1 and forms the basis of current recommendations for the treatment of CSMO2
bull CSMO is diagnosed if any of the following parameters are met1
1 ETDRS Research Group Arch Ophthalmol 19851031796ndash1806 2 Bandello F et al Eye (Lond) 201226(4)485ndash493
1 Retinal thickening within 500 microm of the centre of the macula
2 Hard exudates within 500 microm of the centre of the macula if associated with thickening of the adjacent retina
3 Retinal thickening of gt1 disc area in size any part of which is located within 1 disc diameter of the centre of the macula
500 microm
500 microm
1 discdiameter
ge 1 discdiameter
Fovea
8
ETDRS = Early Treatment Diabetic Retinopathy Study
LASER
RCO recommendations for the treatment of CSMO
The Royal College of Ophthalmologists Diabetic Retinopathy Guidelines 2012
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
9
ILUVIEN (chronicunresponsive)
OZURXEX (no improvement)
DMO ndash treatment optionsWhat treatments should I use at baseline
bull ETDRS based laser therapies
bull ADJUNCT
bull Surgery ndash VMTERM
bull Pan-retinal photocoagulation
bull INTRAVITREAL
bull ANTI-VEGF
bull Lucentis (Ranibizumab)
bull Eylea (Aflibercept)
bull Avastin (Bevacizumab)
bull STEROIDS
bull Iluvien (Fluocinolone)
bull Ozurdex (Dexamethasone)
11
BOLT
RESOLVERISE and RIDERELIGHT
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
DMO ndash treatment optionsWhat treatments should I use at baseline ndash based on evidence from RCT data
What therapy do I choose for my patient at baselineWhich treatments can I access
NICE TA 274 Lucentis for DMO April 2013NICE TA 346 Eylea for DMO July 2015
NICE TA 301 Iluvien for DMO Nov 2013NICE TA 349 Ozurdex for DMO July 2015
OCT gt400um1st line if OCT suitable
bull Chronic DMObull PSEUDOPHAKICbull Patients ldquoinsufficiently responsive
to existing therapiesrdquo
bull PSEUDOPHAKICbull ldquoNot improved with non-
corticosteroid or such treatment is not suitable for themrdquo
What therapy do I choose for my patient at baseline
bull ANTI-VEGF
bull Superior to ETDRS argon laser in terms of efficacy
RESTORE 36 month Lucentis prn extension studyLucentis monotherapy vs Lucentis plus laser vs laser aloneSchmidt-Erfuth U et al Ophthalmology 2014 121(5) 1045-1053
23
Months
12
10
8
6
4
2
0
minus22 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Extension study (ranibizumab 05 mg PRN)Core study
Me
an o
f th
e c
han
ge in
ETD
RS
BC
VA
Prior ranibizumab 05 mg + active laser (n=83)
Prior sham injections + active laser (n=74)
Prior ranibizumab 05 mg + sham laser (n=83)
79
71 606780
Core study assessment
Full analysisstudy completionInterim analysis
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
15
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
RISE amp RIDE
Date of Prep Dec 2014 LGB0820147252X
02 Laser
125 2q4
107 2q8
0
Mea
n ch
ange
in B
CVA
lette
r sco
re
2
101214
02
6
10
14
4
8
12
468
09 Laser
115 2q4
111 2q8
VISTA Week 100
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
12 Laser
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
105 2q4
107 2q8VIVID Week 100
Week Laser 2q4 2q8
07 Laser
114 2q4
94 2q8
Eylea =VIVID and VISTA Mean change in BCVA to week 100Korobelnik J-F et al Ophthalmology 2014 121 (11) 2247ndash2254 Brown DM et al Ophthalmology 2015 Jul 18 [Epub ahead of print]
Plt00001 vs laser VIVID Laser n=132 2q4 n=136 2q8 n=135 VISTA Laser n=154 2q4 n=154 2q8 n=151Full analysis set 2q4 2 mg every 4 weeks 2q8 2 mg every 8 weeks BCVA best corrected visual acuity ETDRS Early Treatment Diabetic Retinopathy Study
What therapy do I choose for my patient at baseline
bull ANTI-VEGF helliphellipif OCT gt 400um
bull Sohellip Which one
Key trials in DMO
18
BOLT
RESOLVERISE and RIDE
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull 1)What treatment should I start with at baselinebull 2)Re-treatment algorithms for intravitreal DMO
therapiesbull 3)When should I switchcombine therapiesbull 4)The bigger picture
bull Other eyeperipheral retinopathybull The patient as a wholebull The service -coping with capacity ndash compromises
DMO ndash treatment options1)What treatments should I use at baseline
bull ETDRS based laser therapies
bull ADJUNCT
bull Surgery ndash VMTERM
bull Pan-retinal photocoagulation
bull INTRAVITREAL
bull ANTI-VEGF
bull Lucentis (Ranibizumab)
bull Eylea (Aflibercept)
bull Avastin (Bevacizumab)
bull STEROIDS
bull Iluvien (Fluocinolone)
bull Ozurdex (Dexamethasone)
RCO recommendations for the treatment of CSMO
The Royal College of Ophthalmologists Diabetic Retinopathy Guidelines 2012
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
Fluocinolone is an option for eyes unresponsive to other treatments but potential side effects must be considered Triamcinolone +- adjunctive laser or fluocinolone may be considered for eyes unresponsive to other treatments
6
ETDRS based laser therapies = Clinically significant macular oedema (CSMO)
bull The ETDRS defined CSMO as DMO that threatens the centre of the macula (fovea)1 and forms the basis of current recommendations for the treatment of CSMO2
bull CSMO is diagnosed if any of the following parameters are met1
1 ETDRS Research Group Arch Ophthalmol 19851031796ndash1806 2 Bandello F et al Eye (Lond) 201226(4)485ndash493
1 Retinal thickening within 500 microm of the centre of the macula
2 Hard exudates within 500 microm of the centre of the macula if associated with thickening of the adjacent retina
3 Retinal thickening of gt1 disc area in size any part of which is located within 1 disc diameter of the centre of the macula
500 microm
500 microm
1 discdiameter
ge 1 discdiameter
Fovea
7
ETDRS = Early Treatment Diabetic Retinopathy Study
Date of Prep Jan 2015 LGB0820157252f
DMO ndash treatment optionsWhat treatments should I use at baseline
ETDRS based laser therapies = Clinically significant macular oedema (CSMO)
bull The ETDRS defined CSMO as DMO that threatens the centre of the macula (fovea)1 and forms the basis of current recommendations for the treatment of CSMO2
bull CSMO is diagnosed if any of the following parameters are met1
1 ETDRS Research Group Arch Ophthalmol 19851031796ndash1806 2 Bandello F et al Eye (Lond) 201226(4)485ndash493
1 Retinal thickening within 500 microm of the centre of the macula
2 Hard exudates within 500 microm of the centre of the macula if associated with thickening of the adjacent retina
3 Retinal thickening of gt1 disc area in size any part of which is located within 1 disc diameter of the centre of the macula
500 microm
500 microm
1 discdiameter
ge 1 discdiameter
Fovea
8
ETDRS = Early Treatment Diabetic Retinopathy Study
LASER
RCO recommendations for the treatment of CSMO
The Royal College of Ophthalmologists Diabetic Retinopathy Guidelines 2012
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
9
ILUVIEN (chronicunresponsive)
OZURXEX (no improvement)
DMO ndash treatment optionsWhat treatments should I use at baseline
bull ETDRS based laser therapies
bull ADJUNCT
bull Surgery ndash VMTERM
bull Pan-retinal photocoagulation
bull INTRAVITREAL
bull ANTI-VEGF
bull Lucentis (Ranibizumab)
bull Eylea (Aflibercept)
bull Avastin (Bevacizumab)
bull STEROIDS
bull Iluvien (Fluocinolone)
bull Ozurdex (Dexamethasone)
11
BOLT
RESOLVERISE and RIDERELIGHT
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
DMO ndash treatment optionsWhat treatments should I use at baseline ndash based on evidence from RCT data
What therapy do I choose for my patient at baselineWhich treatments can I access
NICE TA 274 Lucentis for DMO April 2013NICE TA 346 Eylea for DMO July 2015
NICE TA 301 Iluvien for DMO Nov 2013NICE TA 349 Ozurdex for DMO July 2015
OCT gt400um1st line if OCT suitable
bull Chronic DMObull PSEUDOPHAKICbull Patients ldquoinsufficiently responsive
to existing therapiesrdquo
bull PSEUDOPHAKICbull ldquoNot improved with non-
corticosteroid or such treatment is not suitable for themrdquo
What therapy do I choose for my patient at baseline
bull ANTI-VEGF
bull Superior to ETDRS argon laser in terms of efficacy
RESTORE 36 month Lucentis prn extension studyLucentis monotherapy vs Lucentis plus laser vs laser aloneSchmidt-Erfuth U et al Ophthalmology 2014 121(5) 1045-1053
23
Months
12
10
8
6
4
2
0
minus22 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Extension study (ranibizumab 05 mg PRN)Core study
Me
an o
f th
e c
han
ge in
ETD
RS
BC
VA
Prior ranibizumab 05 mg + active laser (n=83)
Prior sham injections + active laser (n=74)
Prior ranibizumab 05 mg + sham laser (n=83)
79
71 606780
Core study assessment
Full analysisstudy completionInterim analysis
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
15
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
RISE amp RIDE
Date of Prep Dec 2014 LGB0820147252X
02 Laser
125 2q4
107 2q8
0
Mea
n ch
ange
in B
CVA
lette
r sco
re
2
101214
02
6
10
14
4
8
12
468
09 Laser
115 2q4
111 2q8
VISTA Week 100
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
12 Laser
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
105 2q4
107 2q8VIVID Week 100
Week Laser 2q4 2q8
07 Laser
114 2q4
94 2q8
Eylea =VIVID and VISTA Mean change in BCVA to week 100Korobelnik J-F et al Ophthalmology 2014 121 (11) 2247ndash2254 Brown DM et al Ophthalmology 2015 Jul 18 [Epub ahead of print]
Plt00001 vs laser VIVID Laser n=132 2q4 n=136 2q8 n=135 VISTA Laser n=154 2q4 n=154 2q8 n=151Full analysis set 2q4 2 mg every 4 weeks 2q8 2 mg every 8 weeks BCVA best corrected visual acuity ETDRS Early Treatment Diabetic Retinopathy Study
What therapy do I choose for my patient at baseline
bull ANTI-VEGF helliphellipif OCT gt 400um
bull Sohellip Which one
Key trials in DMO
18
BOLT
RESOLVERISE and RIDE
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

DMO ndash treatment options1)What treatments should I use at baseline
bull ETDRS based laser therapies
bull ADJUNCT
bull Surgery ndash VMTERM
bull Pan-retinal photocoagulation
bull INTRAVITREAL
bull ANTI-VEGF
bull Lucentis (Ranibizumab)
bull Eylea (Aflibercept)
bull Avastin (Bevacizumab)
bull STEROIDS
bull Iluvien (Fluocinolone)
bull Ozurdex (Dexamethasone)
RCO recommendations for the treatment of CSMO
The Royal College of Ophthalmologists Diabetic Retinopathy Guidelines 2012
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
Fluocinolone is an option for eyes unresponsive to other treatments but potential side effects must be considered Triamcinolone +- adjunctive laser or fluocinolone may be considered for eyes unresponsive to other treatments
6
ETDRS based laser therapies = Clinically significant macular oedema (CSMO)
bull The ETDRS defined CSMO as DMO that threatens the centre of the macula (fovea)1 and forms the basis of current recommendations for the treatment of CSMO2
bull CSMO is diagnosed if any of the following parameters are met1
1 ETDRS Research Group Arch Ophthalmol 19851031796ndash1806 2 Bandello F et al Eye (Lond) 201226(4)485ndash493
1 Retinal thickening within 500 microm of the centre of the macula
2 Hard exudates within 500 microm of the centre of the macula if associated with thickening of the adjacent retina
3 Retinal thickening of gt1 disc area in size any part of which is located within 1 disc diameter of the centre of the macula
500 microm
500 microm
1 discdiameter
ge 1 discdiameter
Fovea
7
ETDRS = Early Treatment Diabetic Retinopathy Study
Date of Prep Jan 2015 LGB0820157252f
DMO ndash treatment optionsWhat treatments should I use at baseline
ETDRS based laser therapies = Clinically significant macular oedema (CSMO)
bull The ETDRS defined CSMO as DMO that threatens the centre of the macula (fovea)1 and forms the basis of current recommendations for the treatment of CSMO2
bull CSMO is diagnosed if any of the following parameters are met1
1 ETDRS Research Group Arch Ophthalmol 19851031796ndash1806 2 Bandello F et al Eye (Lond) 201226(4)485ndash493
1 Retinal thickening within 500 microm of the centre of the macula
2 Hard exudates within 500 microm of the centre of the macula if associated with thickening of the adjacent retina
3 Retinal thickening of gt1 disc area in size any part of which is located within 1 disc diameter of the centre of the macula
500 microm
500 microm
1 discdiameter
ge 1 discdiameter
Fovea
8
ETDRS = Early Treatment Diabetic Retinopathy Study
LASER
RCO recommendations for the treatment of CSMO
The Royal College of Ophthalmologists Diabetic Retinopathy Guidelines 2012
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
9
ILUVIEN (chronicunresponsive)
OZURXEX (no improvement)
DMO ndash treatment optionsWhat treatments should I use at baseline
bull ETDRS based laser therapies
bull ADJUNCT
bull Surgery ndash VMTERM
bull Pan-retinal photocoagulation
bull INTRAVITREAL
bull ANTI-VEGF
bull Lucentis (Ranibizumab)
bull Eylea (Aflibercept)
bull Avastin (Bevacizumab)
bull STEROIDS
bull Iluvien (Fluocinolone)
bull Ozurdex (Dexamethasone)
11
BOLT
RESOLVERISE and RIDERELIGHT
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
DMO ndash treatment optionsWhat treatments should I use at baseline ndash based on evidence from RCT data
What therapy do I choose for my patient at baselineWhich treatments can I access
NICE TA 274 Lucentis for DMO April 2013NICE TA 346 Eylea for DMO July 2015
NICE TA 301 Iluvien for DMO Nov 2013NICE TA 349 Ozurdex for DMO July 2015
OCT gt400um1st line if OCT suitable
bull Chronic DMObull PSEUDOPHAKICbull Patients ldquoinsufficiently responsive
to existing therapiesrdquo
bull PSEUDOPHAKICbull ldquoNot improved with non-
corticosteroid or such treatment is not suitable for themrdquo
What therapy do I choose for my patient at baseline
bull ANTI-VEGF
bull Superior to ETDRS argon laser in terms of efficacy
RESTORE 36 month Lucentis prn extension studyLucentis monotherapy vs Lucentis plus laser vs laser aloneSchmidt-Erfuth U et al Ophthalmology 2014 121(5) 1045-1053
23
Months
12
10
8
6
4
2
0
minus22 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Extension study (ranibizumab 05 mg PRN)Core study
Me
an o
f th
e c
han
ge in
ETD
RS
BC
VA
Prior ranibizumab 05 mg + active laser (n=83)
Prior sham injections + active laser (n=74)
Prior ranibizumab 05 mg + sham laser (n=83)
79
71 606780
Core study assessment
Full analysisstudy completionInterim analysis
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
15
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
RISE amp RIDE
Date of Prep Dec 2014 LGB0820147252X
02 Laser
125 2q4
107 2q8
0
Mea
n ch
ange
in B
CVA
lette
r sco
re
2
101214
02
6
10
14
4
8
12
468
09 Laser
115 2q4
111 2q8
VISTA Week 100
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
12 Laser
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
105 2q4
107 2q8VIVID Week 100
Week Laser 2q4 2q8
07 Laser
114 2q4
94 2q8
Eylea =VIVID and VISTA Mean change in BCVA to week 100Korobelnik J-F et al Ophthalmology 2014 121 (11) 2247ndash2254 Brown DM et al Ophthalmology 2015 Jul 18 [Epub ahead of print]
Plt00001 vs laser VIVID Laser n=132 2q4 n=136 2q8 n=135 VISTA Laser n=154 2q4 n=154 2q8 n=151Full analysis set 2q4 2 mg every 4 weeks 2q8 2 mg every 8 weeks BCVA best corrected visual acuity ETDRS Early Treatment Diabetic Retinopathy Study
What therapy do I choose for my patient at baseline
bull ANTI-VEGF helliphellipif OCT gt 400um
bull Sohellip Which one
Key trials in DMO
18
BOLT
RESOLVERISE and RIDE
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

RCO recommendations for the treatment of CSMO
The Royal College of Ophthalmologists Diabetic Retinopathy Guidelines 2012
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
Fluocinolone is an option for eyes unresponsive to other treatments but potential side effects must be considered Triamcinolone +- adjunctive laser or fluocinolone may be considered for eyes unresponsive to other treatments
6
ETDRS based laser therapies = Clinically significant macular oedema (CSMO)
bull The ETDRS defined CSMO as DMO that threatens the centre of the macula (fovea)1 and forms the basis of current recommendations for the treatment of CSMO2
bull CSMO is diagnosed if any of the following parameters are met1
1 ETDRS Research Group Arch Ophthalmol 19851031796ndash1806 2 Bandello F et al Eye (Lond) 201226(4)485ndash493
1 Retinal thickening within 500 microm of the centre of the macula
2 Hard exudates within 500 microm of the centre of the macula if associated with thickening of the adjacent retina
3 Retinal thickening of gt1 disc area in size any part of which is located within 1 disc diameter of the centre of the macula
500 microm
500 microm
1 discdiameter
ge 1 discdiameter
Fovea
7
ETDRS = Early Treatment Diabetic Retinopathy Study
Date of Prep Jan 2015 LGB0820157252f
DMO ndash treatment optionsWhat treatments should I use at baseline
ETDRS based laser therapies = Clinically significant macular oedema (CSMO)
bull The ETDRS defined CSMO as DMO that threatens the centre of the macula (fovea)1 and forms the basis of current recommendations for the treatment of CSMO2
bull CSMO is diagnosed if any of the following parameters are met1
1 ETDRS Research Group Arch Ophthalmol 19851031796ndash1806 2 Bandello F et al Eye (Lond) 201226(4)485ndash493
1 Retinal thickening within 500 microm of the centre of the macula
2 Hard exudates within 500 microm of the centre of the macula if associated with thickening of the adjacent retina
3 Retinal thickening of gt1 disc area in size any part of which is located within 1 disc diameter of the centre of the macula
500 microm
500 microm
1 discdiameter
ge 1 discdiameter
Fovea
8
ETDRS = Early Treatment Diabetic Retinopathy Study
LASER
RCO recommendations for the treatment of CSMO
The Royal College of Ophthalmologists Diabetic Retinopathy Guidelines 2012
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
9
ILUVIEN (chronicunresponsive)
OZURXEX (no improvement)
DMO ndash treatment optionsWhat treatments should I use at baseline
bull ETDRS based laser therapies
bull ADJUNCT
bull Surgery ndash VMTERM
bull Pan-retinal photocoagulation
bull INTRAVITREAL
bull ANTI-VEGF
bull Lucentis (Ranibizumab)
bull Eylea (Aflibercept)
bull Avastin (Bevacizumab)
bull STEROIDS
bull Iluvien (Fluocinolone)
bull Ozurdex (Dexamethasone)
11
BOLT
RESOLVERISE and RIDERELIGHT
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
DMO ndash treatment optionsWhat treatments should I use at baseline ndash based on evidence from RCT data
What therapy do I choose for my patient at baselineWhich treatments can I access
NICE TA 274 Lucentis for DMO April 2013NICE TA 346 Eylea for DMO July 2015
NICE TA 301 Iluvien for DMO Nov 2013NICE TA 349 Ozurdex for DMO July 2015
OCT gt400um1st line if OCT suitable
bull Chronic DMObull PSEUDOPHAKICbull Patients ldquoinsufficiently responsive
to existing therapiesrdquo
bull PSEUDOPHAKICbull ldquoNot improved with non-
corticosteroid or such treatment is not suitable for themrdquo
What therapy do I choose for my patient at baseline
bull ANTI-VEGF
bull Superior to ETDRS argon laser in terms of efficacy
RESTORE 36 month Lucentis prn extension studyLucentis monotherapy vs Lucentis plus laser vs laser aloneSchmidt-Erfuth U et al Ophthalmology 2014 121(5) 1045-1053
23
Months
12
10
8
6
4
2
0
minus22 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Extension study (ranibizumab 05 mg PRN)Core study
Me
an o
f th
e c
han
ge in
ETD
RS
BC
VA
Prior ranibizumab 05 mg + active laser (n=83)
Prior sham injections + active laser (n=74)
Prior ranibizumab 05 mg + sham laser (n=83)
79
71 606780
Core study assessment
Full analysisstudy completionInterim analysis
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
15
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
RISE amp RIDE
Date of Prep Dec 2014 LGB0820147252X
02 Laser
125 2q4
107 2q8
0
Mea
n ch
ange
in B
CVA
lette
r sco
re
2
101214
02
6
10
14
4
8
12
468
09 Laser
115 2q4
111 2q8
VISTA Week 100
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
12 Laser
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
105 2q4
107 2q8VIVID Week 100
Week Laser 2q4 2q8
07 Laser
114 2q4
94 2q8
Eylea =VIVID and VISTA Mean change in BCVA to week 100Korobelnik J-F et al Ophthalmology 2014 121 (11) 2247ndash2254 Brown DM et al Ophthalmology 2015 Jul 18 [Epub ahead of print]
Plt00001 vs laser VIVID Laser n=132 2q4 n=136 2q8 n=135 VISTA Laser n=154 2q4 n=154 2q8 n=151Full analysis set 2q4 2 mg every 4 weeks 2q8 2 mg every 8 weeks BCVA best corrected visual acuity ETDRS Early Treatment Diabetic Retinopathy Study
What therapy do I choose for my patient at baseline
bull ANTI-VEGF helliphellipif OCT gt 400um
bull Sohellip Which one
Key trials in DMO
18
BOLT
RESOLVERISE and RIDE
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

ETDRS based laser therapies = Clinically significant macular oedema (CSMO)
bull The ETDRS defined CSMO as DMO that threatens the centre of the macula (fovea)1 and forms the basis of current recommendations for the treatment of CSMO2
bull CSMO is diagnosed if any of the following parameters are met1
1 ETDRS Research Group Arch Ophthalmol 19851031796ndash1806 2 Bandello F et al Eye (Lond) 201226(4)485ndash493
1 Retinal thickening within 500 microm of the centre of the macula
2 Hard exudates within 500 microm of the centre of the macula if associated with thickening of the adjacent retina
3 Retinal thickening of gt1 disc area in size any part of which is located within 1 disc diameter of the centre of the macula
500 microm
500 microm
1 discdiameter
ge 1 discdiameter
Fovea
7
ETDRS = Early Treatment Diabetic Retinopathy Study
Date of Prep Jan 2015 LGB0820157252f
DMO ndash treatment optionsWhat treatments should I use at baseline
ETDRS based laser therapies = Clinically significant macular oedema (CSMO)
bull The ETDRS defined CSMO as DMO that threatens the centre of the macula (fovea)1 and forms the basis of current recommendations for the treatment of CSMO2
bull CSMO is diagnosed if any of the following parameters are met1
1 ETDRS Research Group Arch Ophthalmol 19851031796ndash1806 2 Bandello F et al Eye (Lond) 201226(4)485ndash493
1 Retinal thickening within 500 microm of the centre of the macula
2 Hard exudates within 500 microm of the centre of the macula if associated with thickening of the adjacent retina
3 Retinal thickening of gt1 disc area in size any part of which is located within 1 disc diameter of the centre of the macula
500 microm
500 microm
1 discdiameter
ge 1 discdiameter
Fovea
8
ETDRS = Early Treatment Diabetic Retinopathy Study
LASER
RCO recommendations for the treatment of CSMO
The Royal College of Ophthalmologists Diabetic Retinopathy Guidelines 2012
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
9
ILUVIEN (chronicunresponsive)
OZURXEX (no improvement)
DMO ndash treatment optionsWhat treatments should I use at baseline
bull ETDRS based laser therapies
bull ADJUNCT
bull Surgery ndash VMTERM
bull Pan-retinal photocoagulation
bull INTRAVITREAL
bull ANTI-VEGF
bull Lucentis (Ranibizumab)
bull Eylea (Aflibercept)
bull Avastin (Bevacizumab)
bull STEROIDS
bull Iluvien (Fluocinolone)
bull Ozurdex (Dexamethasone)
11
BOLT
RESOLVERISE and RIDERELIGHT
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
DMO ndash treatment optionsWhat treatments should I use at baseline ndash based on evidence from RCT data
What therapy do I choose for my patient at baselineWhich treatments can I access
NICE TA 274 Lucentis for DMO April 2013NICE TA 346 Eylea for DMO July 2015
NICE TA 301 Iluvien for DMO Nov 2013NICE TA 349 Ozurdex for DMO July 2015
OCT gt400um1st line if OCT suitable
bull Chronic DMObull PSEUDOPHAKICbull Patients ldquoinsufficiently responsive
to existing therapiesrdquo
bull PSEUDOPHAKICbull ldquoNot improved with non-
corticosteroid or such treatment is not suitable for themrdquo
What therapy do I choose for my patient at baseline
bull ANTI-VEGF
bull Superior to ETDRS argon laser in terms of efficacy
RESTORE 36 month Lucentis prn extension studyLucentis monotherapy vs Lucentis plus laser vs laser aloneSchmidt-Erfuth U et al Ophthalmology 2014 121(5) 1045-1053
23
Months
12
10
8
6
4
2
0
minus22 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Extension study (ranibizumab 05 mg PRN)Core study
Me
an o
f th
e c
han
ge in
ETD
RS
BC
VA
Prior ranibizumab 05 mg + active laser (n=83)
Prior sham injections + active laser (n=74)
Prior ranibizumab 05 mg + sham laser (n=83)
79
71 606780
Core study assessment
Full analysisstudy completionInterim analysis
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
15
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
RISE amp RIDE
Date of Prep Dec 2014 LGB0820147252X
02 Laser
125 2q4
107 2q8
0
Mea
n ch
ange
in B
CVA
lette
r sco
re
2
101214
02
6
10
14
4
8
12
468
09 Laser
115 2q4
111 2q8
VISTA Week 100
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
12 Laser
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
105 2q4
107 2q8VIVID Week 100
Week Laser 2q4 2q8
07 Laser
114 2q4
94 2q8
Eylea =VIVID and VISTA Mean change in BCVA to week 100Korobelnik J-F et al Ophthalmology 2014 121 (11) 2247ndash2254 Brown DM et al Ophthalmology 2015 Jul 18 [Epub ahead of print]
Plt00001 vs laser VIVID Laser n=132 2q4 n=136 2q8 n=135 VISTA Laser n=154 2q4 n=154 2q8 n=151Full analysis set 2q4 2 mg every 4 weeks 2q8 2 mg every 8 weeks BCVA best corrected visual acuity ETDRS Early Treatment Diabetic Retinopathy Study
What therapy do I choose for my patient at baseline
bull ANTI-VEGF helliphellipif OCT gt 400um
bull Sohellip Which one
Key trials in DMO
18
BOLT
RESOLVERISE and RIDE
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

ETDRS based laser therapies = Clinically significant macular oedema (CSMO)
bull The ETDRS defined CSMO as DMO that threatens the centre of the macula (fovea)1 and forms the basis of current recommendations for the treatment of CSMO2
bull CSMO is diagnosed if any of the following parameters are met1
1 ETDRS Research Group Arch Ophthalmol 19851031796ndash1806 2 Bandello F et al Eye (Lond) 201226(4)485ndash493
1 Retinal thickening within 500 microm of the centre of the macula
2 Hard exudates within 500 microm of the centre of the macula if associated with thickening of the adjacent retina
3 Retinal thickening of gt1 disc area in size any part of which is located within 1 disc diameter of the centre of the macula
500 microm
500 microm
1 discdiameter
ge 1 discdiameter
Fovea
8
ETDRS = Early Treatment Diabetic Retinopathy Study
LASER
RCO recommendations for the treatment of CSMO
The Royal College of Ophthalmologists Diabetic Retinopathy Guidelines 2012
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
9
ILUVIEN (chronicunresponsive)
OZURXEX (no improvement)
DMO ndash treatment optionsWhat treatments should I use at baseline
bull ETDRS based laser therapies
bull ADJUNCT
bull Surgery ndash VMTERM
bull Pan-retinal photocoagulation
bull INTRAVITREAL
bull ANTI-VEGF
bull Lucentis (Ranibizumab)
bull Eylea (Aflibercept)
bull Avastin (Bevacizumab)
bull STEROIDS
bull Iluvien (Fluocinolone)
bull Ozurdex (Dexamethasone)
11
BOLT
RESOLVERISE and RIDERELIGHT
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
DMO ndash treatment optionsWhat treatments should I use at baseline ndash based on evidence from RCT data
What therapy do I choose for my patient at baselineWhich treatments can I access
NICE TA 274 Lucentis for DMO April 2013NICE TA 346 Eylea for DMO July 2015
NICE TA 301 Iluvien for DMO Nov 2013NICE TA 349 Ozurdex for DMO July 2015
OCT gt400um1st line if OCT suitable
bull Chronic DMObull PSEUDOPHAKICbull Patients ldquoinsufficiently responsive
to existing therapiesrdquo
bull PSEUDOPHAKICbull ldquoNot improved with non-
corticosteroid or such treatment is not suitable for themrdquo
What therapy do I choose for my patient at baseline
bull ANTI-VEGF
bull Superior to ETDRS argon laser in terms of efficacy
RESTORE 36 month Lucentis prn extension studyLucentis monotherapy vs Lucentis plus laser vs laser aloneSchmidt-Erfuth U et al Ophthalmology 2014 121(5) 1045-1053
23
Months
12
10
8
6
4
2
0
minus22 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Extension study (ranibizumab 05 mg PRN)Core study
Me
an o
f th
e c
han
ge in
ETD
RS
BC
VA
Prior ranibizumab 05 mg + active laser (n=83)
Prior sham injections + active laser (n=74)
Prior ranibizumab 05 mg + sham laser (n=83)
79
71 606780
Core study assessment
Full analysisstudy completionInterim analysis
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
15
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
RISE amp RIDE
Date of Prep Dec 2014 LGB0820147252X
02 Laser
125 2q4
107 2q8
0
Mea
n ch
ange
in B
CVA
lette
r sco
re
2
101214
02
6
10
14
4
8
12
468
09 Laser
115 2q4
111 2q8
VISTA Week 100
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
12 Laser
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
105 2q4
107 2q8VIVID Week 100
Week Laser 2q4 2q8
07 Laser
114 2q4
94 2q8
Eylea =VIVID and VISTA Mean change in BCVA to week 100Korobelnik J-F et al Ophthalmology 2014 121 (11) 2247ndash2254 Brown DM et al Ophthalmology 2015 Jul 18 [Epub ahead of print]
Plt00001 vs laser VIVID Laser n=132 2q4 n=136 2q8 n=135 VISTA Laser n=154 2q4 n=154 2q8 n=151Full analysis set 2q4 2 mg every 4 weeks 2q8 2 mg every 8 weeks BCVA best corrected visual acuity ETDRS Early Treatment Diabetic Retinopathy Study
What therapy do I choose for my patient at baseline
bull ANTI-VEGF helliphellipif OCT gt 400um
bull Sohellip Which one
Key trials in DMO
18
BOLT
RESOLVERISE and RIDE
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

RCO recommendations for the treatment of CSMO
The Royal College of Ophthalmologists Diabetic Retinopathy Guidelines 2012
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
9
ILUVIEN (chronicunresponsive)
OZURXEX (no improvement)
DMO ndash treatment optionsWhat treatments should I use at baseline
bull ETDRS based laser therapies
bull ADJUNCT
bull Surgery ndash VMTERM
bull Pan-retinal photocoagulation
bull INTRAVITREAL
bull ANTI-VEGF
bull Lucentis (Ranibizumab)
bull Eylea (Aflibercept)
bull Avastin (Bevacizumab)
bull STEROIDS
bull Iluvien (Fluocinolone)
bull Ozurdex (Dexamethasone)
11
BOLT
RESOLVERISE and RIDERELIGHT
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
DMO ndash treatment optionsWhat treatments should I use at baseline ndash based on evidence from RCT data
What therapy do I choose for my patient at baselineWhich treatments can I access
NICE TA 274 Lucentis for DMO April 2013NICE TA 346 Eylea for DMO July 2015
NICE TA 301 Iluvien for DMO Nov 2013NICE TA 349 Ozurdex for DMO July 2015
OCT gt400um1st line if OCT suitable
bull Chronic DMObull PSEUDOPHAKICbull Patients ldquoinsufficiently responsive
to existing therapiesrdquo
bull PSEUDOPHAKICbull ldquoNot improved with non-
corticosteroid or such treatment is not suitable for themrdquo
What therapy do I choose for my patient at baseline
bull ANTI-VEGF
bull Superior to ETDRS argon laser in terms of efficacy
RESTORE 36 month Lucentis prn extension studyLucentis monotherapy vs Lucentis plus laser vs laser aloneSchmidt-Erfuth U et al Ophthalmology 2014 121(5) 1045-1053
23
Months
12
10
8
6
4
2
0
minus22 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Extension study (ranibizumab 05 mg PRN)Core study
Me
an o
f th
e c
han
ge in
ETD
RS
BC
VA
Prior ranibizumab 05 mg + active laser (n=83)
Prior sham injections + active laser (n=74)
Prior ranibizumab 05 mg + sham laser (n=83)
79
71 606780
Core study assessment
Full analysisstudy completionInterim analysis
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
15
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
RISE amp RIDE
Date of Prep Dec 2014 LGB0820147252X
02 Laser
125 2q4
107 2q8
0
Mea
n ch
ange
in B
CVA
lette
r sco
re
2
101214
02
6
10
14
4
8
12
468
09 Laser
115 2q4
111 2q8
VISTA Week 100
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
12 Laser
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
105 2q4
107 2q8VIVID Week 100
Week Laser 2q4 2q8
07 Laser
114 2q4
94 2q8
Eylea =VIVID and VISTA Mean change in BCVA to week 100Korobelnik J-F et al Ophthalmology 2014 121 (11) 2247ndash2254 Brown DM et al Ophthalmology 2015 Jul 18 [Epub ahead of print]
Plt00001 vs laser VIVID Laser n=132 2q4 n=136 2q8 n=135 VISTA Laser n=154 2q4 n=154 2q8 n=151Full analysis set 2q4 2 mg every 4 weeks 2q8 2 mg every 8 weeks BCVA best corrected visual acuity ETDRS Early Treatment Diabetic Retinopathy Study
What therapy do I choose for my patient at baseline
bull ANTI-VEGF helliphellipif OCT gt 400um
bull Sohellip Which one
Key trials in DMO
18
BOLT
RESOLVERISE and RIDE
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

DMO ndash treatment optionsWhat treatments should I use at baseline
bull ETDRS based laser therapies
bull ADJUNCT
bull Surgery ndash VMTERM
bull Pan-retinal photocoagulation
bull INTRAVITREAL
bull ANTI-VEGF
bull Lucentis (Ranibizumab)
bull Eylea (Aflibercept)
bull Avastin (Bevacizumab)
bull STEROIDS
bull Iluvien (Fluocinolone)
bull Ozurdex (Dexamethasone)
11
BOLT
RESOLVERISE and RIDERELIGHT
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
DMO ndash treatment optionsWhat treatments should I use at baseline ndash based on evidence from RCT data
What therapy do I choose for my patient at baselineWhich treatments can I access
NICE TA 274 Lucentis for DMO April 2013NICE TA 346 Eylea for DMO July 2015
NICE TA 301 Iluvien for DMO Nov 2013NICE TA 349 Ozurdex for DMO July 2015
OCT gt400um1st line if OCT suitable
bull Chronic DMObull PSEUDOPHAKICbull Patients ldquoinsufficiently responsive
to existing therapiesrdquo
bull PSEUDOPHAKICbull ldquoNot improved with non-
corticosteroid or such treatment is not suitable for themrdquo
What therapy do I choose for my patient at baseline
bull ANTI-VEGF
bull Superior to ETDRS argon laser in terms of efficacy
RESTORE 36 month Lucentis prn extension studyLucentis monotherapy vs Lucentis plus laser vs laser aloneSchmidt-Erfuth U et al Ophthalmology 2014 121(5) 1045-1053
23
Months
12
10
8
6
4
2
0
minus22 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Extension study (ranibizumab 05 mg PRN)Core study
Me
an o
f th
e c
han
ge in
ETD
RS
BC
VA
Prior ranibizumab 05 mg + active laser (n=83)
Prior sham injections + active laser (n=74)
Prior ranibizumab 05 mg + sham laser (n=83)
79
71 606780
Core study assessment
Full analysisstudy completionInterim analysis
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
15
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
RISE amp RIDE
Date of Prep Dec 2014 LGB0820147252X
02 Laser
125 2q4
107 2q8
0
Mea
n ch
ange
in B
CVA
lette
r sco
re
2
101214
02
6
10
14
4
8
12
468
09 Laser
115 2q4
111 2q8
VISTA Week 100
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
12 Laser
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
105 2q4
107 2q8VIVID Week 100
Week Laser 2q4 2q8
07 Laser
114 2q4
94 2q8
Eylea =VIVID and VISTA Mean change in BCVA to week 100Korobelnik J-F et al Ophthalmology 2014 121 (11) 2247ndash2254 Brown DM et al Ophthalmology 2015 Jul 18 [Epub ahead of print]
Plt00001 vs laser VIVID Laser n=132 2q4 n=136 2q8 n=135 VISTA Laser n=154 2q4 n=154 2q8 n=151Full analysis set 2q4 2 mg every 4 weeks 2q8 2 mg every 8 weeks BCVA best corrected visual acuity ETDRS Early Treatment Diabetic Retinopathy Study
What therapy do I choose for my patient at baseline
bull ANTI-VEGF helliphellipif OCT gt 400um
bull Sohellip Which one
Key trials in DMO
18
BOLT
RESOLVERISE and RIDE
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

11
BOLT
RESOLVERISE and RIDERELIGHT
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
DMO ndash treatment optionsWhat treatments should I use at baseline ndash based on evidence from RCT data
What therapy do I choose for my patient at baselineWhich treatments can I access
NICE TA 274 Lucentis for DMO April 2013NICE TA 346 Eylea for DMO July 2015
NICE TA 301 Iluvien for DMO Nov 2013NICE TA 349 Ozurdex for DMO July 2015
OCT gt400um1st line if OCT suitable
bull Chronic DMObull PSEUDOPHAKICbull Patients ldquoinsufficiently responsive
to existing therapiesrdquo
bull PSEUDOPHAKICbull ldquoNot improved with non-
corticosteroid or such treatment is not suitable for themrdquo
What therapy do I choose for my patient at baseline
bull ANTI-VEGF
bull Superior to ETDRS argon laser in terms of efficacy
RESTORE 36 month Lucentis prn extension studyLucentis monotherapy vs Lucentis plus laser vs laser aloneSchmidt-Erfuth U et al Ophthalmology 2014 121(5) 1045-1053
23
Months
12
10
8
6
4
2
0
minus22 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Extension study (ranibizumab 05 mg PRN)Core study
Me
an o
f th
e c
han
ge in
ETD
RS
BC
VA
Prior ranibizumab 05 mg + active laser (n=83)
Prior sham injections + active laser (n=74)
Prior ranibizumab 05 mg + sham laser (n=83)
79
71 606780
Core study assessment
Full analysisstudy completionInterim analysis
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
15
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
RISE amp RIDE
Date of Prep Dec 2014 LGB0820147252X
02 Laser
125 2q4
107 2q8
0
Mea
n ch
ange
in B
CVA
lette
r sco
re
2
101214
02
6
10
14
4
8
12
468
09 Laser
115 2q4
111 2q8
VISTA Week 100
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
12 Laser
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
105 2q4
107 2q8VIVID Week 100
Week Laser 2q4 2q8
07 Laser
114 2q4
94 2q8
Eylea =VIVID and VISTA Mean change in BCVA to week 100Korobelnik J-F et al Ophthalmology 2014 121 (11) 2247ndash2254 Brown DM et al Ophthalmology 2015 Jul 18 [Epub ahead of print]
Plt00001 vs laser VIVID Laser n=132 2q4 n=136 2q8 n=135 VISTA Laser n=154 2q4 n=154 2q8 n=151Full analysis set 2q4 2 mg every 4 weeks 2q8 2 mg every 8 weeks BCVA best corrected visual acuity ETDRS Early Treatment Diabetic Retinopathy Study
What therapy do I choose for my patient at baseline
bull ANTI-VEGF helliphellipif OCT gt 400um
bull Sohellip Which one
Key trials in DMO
18
BOLT
RESOLVERISE and RIDE
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

What therapy do I choose for my patient at baselineWhich treatments can I access
NICE TA 274 Lucentis for DMO April 2013NICE TA 346 Eylea for DMO July 2015
NICE TA 301 Iluvien for DMO Nov 2013NICE TA 349 Ozurdex for DMO July 2015
OCT gt400um1st line if OCT suitable
bull Chronic DMObull PSEUDOPHAKICbull Patients ldquoinsufficiently responsive
to existing therapiesrdquo
bull PSEUDOPHAKICbull ldquoNot improved with non-
corticosteroid or such treatment is not suitable for themrdquo
What therapy do I choose for my patient at baseline
bull ANTI-VEGF
bull Superior to ETDRS argon laser in terms of efficacy
RESTORE 36 month Lucentis prn extension studyLucentis monotherapy vs Lucentis plus laser vs laser aloneSchmidt-Erfuth U et al Ophthalmology 2014 121(5) 1045-1053
23
Months
12
10
8
6
4
2
0
minus22 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Extension study (ranibizumab 05 mg PRN)Core study
Me
an o
f th
e c
han
ge in
ETD
RS
BC
VA
Prior ranibizumab 05 mg + active laser (n=83)
Prior sham injections + active laser (n=74)
Prior ranibizumab 05 mg + sham laser (n=83)
79
71 606780
Core study assessment
Full analysisstudy completionInterim analysis
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
15
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
RISE amp RIDE
Date of Prep Dec 2014 LGB0820147252X
02 Laser
125 2q4
107 2q8
0
Mea
n ch
ange
in B
CVA
lette
r sco
re
2
101214
02
6
10
14
4
8
12
468
09 Laser
115 2q4
111 2q8
VISTA Week 100
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
12 Laser
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
105 2q4
107 2q8VIVID Week 100
Week Laser 2q4 2q8
07 Laser
114 2q4
94 2q8
Eylea =VIVID and VISTA Mean change in BCVA to week 100Korobelnik J-F et al Ophthalmology 2014 121 (11) 2247ndash2254 Brown DM et al Ophthalmology 2015 Jul 18 [Epub ahead of print]
Plt00001 vs laser VIVID Laser n=132 2q4 n=136 2q8 n=135 VISTA Laser n=154 2q4 n=154 2q8 n=151Full analysis set 2q4 2 mg every 4 weeks 2q8 2 mg every 8 weeks BCVA best corrected visual acuity ETDRS Early Treatment Diabetic Retinopathy Study
What therapy do I choose for my patient at baseline
bull ANTI-VEGF helliphellipif OCT gt 400um
bull Sohellip Which one
Key trials in DMO
18
BOLT
RESOLVERISE and RIDE
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you
What therapy do I choose for my patient at baseline
bull ANTI-VEGF
bull Superior to ETDRS argon laser in terms of efficacy
RESTORE 36 month Lucentis prn extension studyLucentis monotherapy vs Lucentis plus laser vs laser aloneSchmidt-Erfuth U et al Ophthalmology 2014 121(5) 1045-1053
23
Months
12
10
8
6
4
2
0
minus22 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Extension study (ranibizumab 05 mg PRN)Core study
Me
an o
f th
e c
han
ge in
ETD
RS
BC
VA
Prior ranibizumab 05 mg + active laser (n=83)
Prior sham injections + active laser (n=74)
Prior ranibizumab 05 mg + sham laser (n=83)
79
71 606780
Core study assessment
Full analysisstudy completionInterim analysis
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
15
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
RISE amp RIDE
Date of Prep Dec 2014 LGB0820147252X
02 Laser
125 2q4
107 2q8
0
Mea
n ch
ange
in B
CVA
lette
r sco
re
2
101214
02
6
10
14
4
8
12
468
09 Laser
115 2q4
111 2q8
VISTA Week 100
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
12 Laser
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
105 2q4
107 2q8VIVID Week 100
Week Laser 2q4 2q8
07 Laser
114 2q4
94 2q8
Eylea =VIVID and VISTA Mean change in BCVA to week 100Korobelnik J-F et al Ophthalmology 2014 121 (11) 2247ndash2254 Brown DM et al Ophthalmology 2015 Jul 18 [Epub ahead of print]
Plt00001 vs laser VIVID Laser n=132 2q4 n=136 2q8 n=135 VISTA Laser n=154 2q4 n=154 2q8 n=151Full analysis set 2q4 2 mg every 4 weeks 2q8 2 mg every 8 weeks BCVA best corrected visual acuity ETDRS Early Treatment Diabetic Retinopathy Study
What therapy do I choose for my patient at baseline
bull ANTI-VEGF helliphellipif OCT gt 400um
bull Sohellip Which one
Key trials in DMO
18
BOLT
RESOLVERISE and RIDE
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

RESTORE 36 month Lucentis prn extension studyLucentis monotherapy vs Lucentis plus laser vs laser aloneSchmidt-Erfuth U et al Ophthalmology 2014 121(5) 1045-1053
23
Months
12
10
8
6
4
2
0
minus22 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Extension study (ranibizumab 05 mg PRN)Core study
Me
an o
f th
e c
han
ge in
ETD
RS
BC
VA
Prior ranibizumab 05 mg + active laser (n=83)
Prior sham injections + active laser (n=74)
Prior ranibizumab 05 mg + sham laser (n=83)
79
71 606780
Core study assessment
Full analysisstudy completionInterim analysis
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
15
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
RISE amp RIDE
Date of Prep Dec 2014 LGB0820147252X
02 Laser
125 2q4
107 2q8
0
Mea
n ch
ange
in B
CVA
lette
r sco
re
2
101214
02
6
10
14
4
8
12
468
09 Laser
115 2q4
111 2q8
VISTA Week 100
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
12 Laser
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
105 2q4
107 2q8VIVID Week 100
Week Laser 2q4 2q8
07 Laser
114 2q4
94 2q8
Eylea =VIVID and VISTA Mean change in BCVA to week 100Korobelnik J-F et al Ophthalmology 2014 121 (11) 2247ndash2254 Brown DM et al Ophthalmology 2015 Jul 18 [Epub ahead of print]
Plt00001 vs laser VIVID Laser n=132 2q4 n=136 2q8 n=135 VISTA Laser n=154 2q4 n=154 2q8 n=151Full analysis set 2q4 2 mg every 4 weeks 2q8 2 mg every 8 weeks BCVA best corrected visual acuity ETDRS Early Treatment Diabetic Retinopathy Study
What therapy do I choose for my patient at baseline
bull ANTI-VEGF helliphellipif OCT gt 400um
bull Sohellip Which one
Key trials in DMO
18
BOLT
RESOLVERISE and RIDE
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
15
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
RISE amp RIDE
Date of Prep Dec 2014 LGB0820147252X
02 Laser
125 2q4
107 2q8
0
Mea
n ch
ange
in B
CVA
lette
r sco
re
2
101214
02
6
10
14
4
8
12
468
09 Laser
115 2q4
111 2q8
VISTA Week 100
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
12 Laser
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
105 2q4
107 2q8VIVID Week 100
Week Laser 2q4 2q8
07 Laser
114 2q4
94 2q8
Eylea =VIVID and VISTA Mean change in BCVA to week 100Korobelnik J-F et al Ophthalmology 2014 121 (11) 2247ndash2254 Brown DM et al Ophthalmology 2015 Jul 18 [Epub ahead of print]
Plt00001 vs laser VIVID Laser n=132 2q4 n=136 2q8 n=135 VISTA Laser n=154 2q4 n=154 2q8 n=151Full analysis set 2q4 2 mg every 4 weeks 2q8 2 mg every 8 weeks BCVA best corrected visual acuity ETDRS Early Treatment Diabetic Retinopathy Study
What therapy do I choose for my patient at baseline
bull ANTI-VEGF helliphellipif OCT gt 400um
bull Sohellip Which one
Key trials in DMO
18
BOLT
RESOLVERISE and RIDE
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

02 Laser
125 2q4
107 2q8
0
Mea
n ch
ange
in B
CVA
lette
r sco
re
2
101214
02
6
10
14
4
8
12
468
09 Laser
115 2q4
111 2q8
VISTA Week 100
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
12 Laser
100928068645652403628201240 8 16 24 32 44 48 60 72 76 84 88 96
105 2q4
107 2q8VIVID Week 100
Week Laser 2q4 2q8
07 Laser
114 2q4
94 2q8
Eylea =VIVID and VISTA Mean change in BCVA to week 100Korobelnik J-F et al Ophthalmology 2014 121 (11) 2247ndash2254 Brown DM et al Ophthalmology 2015 Jul 18 [Epub ahead of print]
Plt00001 vs laser VIVID Laser n=132 2q4 n=136 2q8 n=135 VISTA Laser n=154 2q4 n=154 2q8 n=151Full analysis set 2q4 2 mg every 4 weeks 2q8 2 mg every 8 weeks BCVA best corrected visual acuity ETDRS Early Treatment Diabetic Retinopathy Study
What therapy do I choose for my patient at baseline
bull ANTI-VEGF helliphellipif OCT gt 400um
bull Sohellip Which one
Key trials in DMO
18
BOLT
RESOLVERISE and RIDE
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

What therapy do I choose for my patient at baseline
bull ANTI-VEGF helliphellipif OCT gt 400um
bull Sohellip Which one
Key trials in DMO
18
BOLT
RESOLVERISE and RIDE
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Key trials in DMO
18
BOLT
RESOLVERISE and RIDE
DA VINCI
VIVID and VISTA
vs laser
vs sham
Steroids
(in combination
with laser)
Anti-VEGF
(in combination
with laser)
DRCRnet (Protocol I)
ETDRS
READ-2
RESTORE
RETAIN
REVEAL
DRCRnet (Protocol B)
FAMEMEAD
vs laser
vs sham
RanibizumabAflibercept
Bevacizumab
Triamcinolone
Fluocinolone acetonide Dexamethasone
Anti-VEGF Laser Steroids
DRCRnet PROTOCOL T
PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

PROTOCOL T (DRCRnet)
bull Aflibercept Bevacizumab or Ranibizumab for Diabetic Macular Edema
bull N Engl J Med 2015 Mar 26372(13)1193-203
The Diabetic retinopathy Clinical Research Network February 18 2015
USA study NIHR funded
n=660
Lucentis 03mg not 05mg Eylea 2mg Avastin 125mg
Eylea protocol not the licensed regime
Avastin unlicensed
RETREATMENT protocol
First 6 months ndash inject every month 95 of patients UNLESS VA=66 AND OCT DRY
Then 2nd six months ndash if no change after 3 visits DEFER otherwise keep injecting monthly
Recurs ndash need at least 2 injections ie 3 months of stability
STABILITY = 10 Oct change or VA 5 letter change
STABILITY and residual OCT thickness gt250um LASER
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you
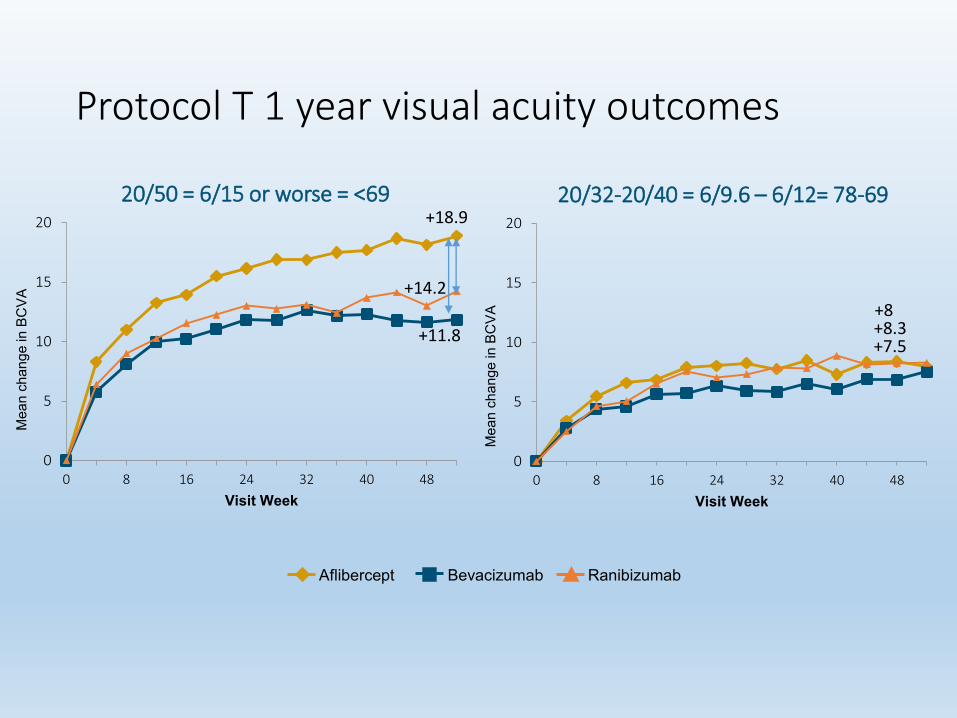
Protocol T 1 year visual acuity outcomes
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2032-2040 = 696 ndash 612= 78-69
0
5
10
15
20
0 8 16 24 32 40 48
Visit Week
2050 = 615 or worse = lt69
Mea
n ch
ange
in B
CV
A
Mea
n ch
ange
in B
CV
A
Aflibercept Bevacizumab Ranibizumab
+189
+142
+118+75
+8+83
Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Protocol T OCT outcomes year 1
-250
-200
-150
-100
-50
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Visit Week
Aflibercept Bevacizumab Ranibizumab
Mea
n ch
ange
in C
ST
Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Conclusions ndash Protocol T year 1 data
bull Eylea was statistically superior in terms of visual acuity to 03mg Lucentisand to Avastin FOR PATIENTS WITH VA worse than 69 letters
bull Eylea and Lucentis were statistically superior in terms of OCT CRT reduction to Avastin for all patients regardless of baseline vision
bull No safety differences between the three drugs
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you
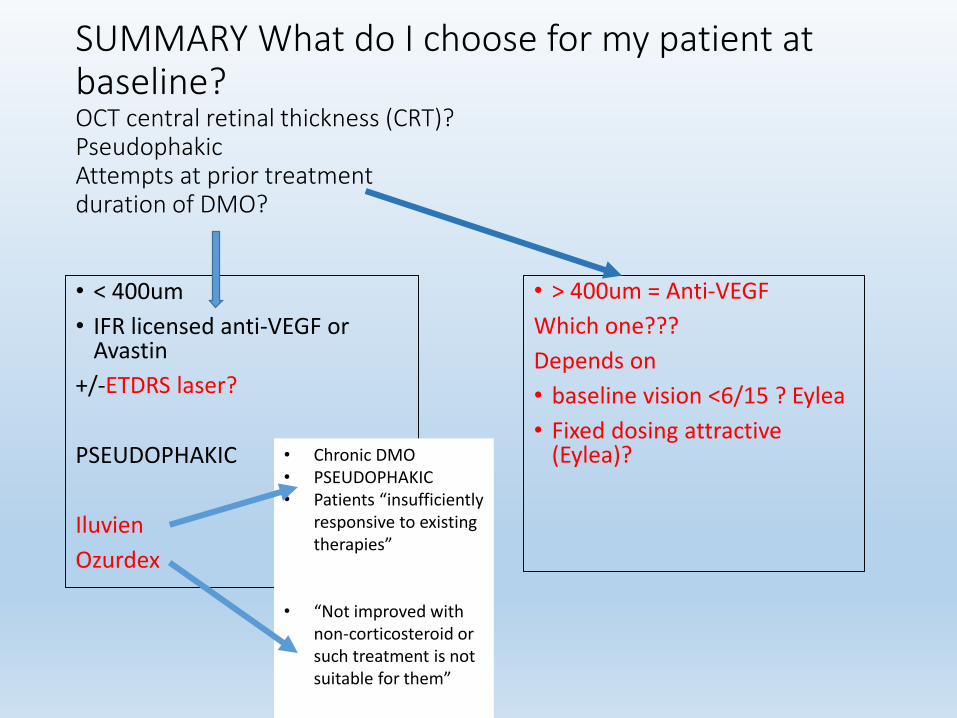
SUMMARY What do I choose for my patient at baselineOCT central retinal thickness (CRT)PseudophakicAttempts at prior treatment duration of DMO
bull lt 400um
bull IFR licensed anti-VEGF or Avastin
+-ETDRS laser
PSEUDOPHAKIC
Iluvien
Ozurdex
bull gt 400um = Anti-VEGF
Which one
Depends on
bull baseline vision lt615 Eylea
bull Fixed dosing attractive (Eylea)bull Chronic DMO
bull PSEUDOPHAKICbull Patients ldquoinsufficiently
responsive to existing therapiesrdquo
bull ldquoNot improved with non-corticosteroid or such treatment is not suitable for themrdquo
Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Which steroid ndash Ozurdex or Iluvien
bull No head to head data
bull Revisit this when we think about switching from ANTI-VEGF to steroid
Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Assuming we have started with an anti-VEGF agent ndash what are the re-treatment algorithms in DMO
Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Treatment posologies
ldquoTreatment is initiated with one injection per month until maximum VA is achieved andor there are no signs of disease activity ie no change in VA and in other signs and
symptoms of the disease under continued treatment
In patients withhellipDMOhellip initially three or more consecutive monthly injections may be needed Thereafter monitoring and treatment intervals
should be determined by the physician and should be based on disease activity as
assessed by VA andor anatomical parametershellip
If patients are being treated according to a treat-and-extend regimen once maximum VA is achieved andor there are no
signs of disease activity the treatment intervals can be extended stepwise until signs of
disease activity or visual impairment recur The treatment intervalhellipmay be extended by up to one month
at a time for DMOrdquo
1 Novartis Pharmaceuticals UK Ltd 30 October 2014 Available at httpwwwmedicinesorgukemcmedicine19409 Accessed 04 September 2015
2 Bayer Pharma AG February 2015 Available at httpwwwmedicinesorgukemcmedicine27224 Accessed 04 September 2015
Ranibizumab1 Aflibercept2
ldquohelliptreatment is initiated with one injection per month for five consecutive doses followed by
one injection every two months There is no requirement for monitoring between injectionshellip
After the first 12 months of treatmenthellipthe treatment interval may be extended based
on visual andor anatomic outcomes The schedule for monitoring should
be determined by the treating physicianrdquo
DMO diabetic macular oedema VA visual acuity
Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Re-treatment algorithms for anti-VEGF agents in DMO
bull LOADING PHASE
bull Lucentis label = monthly until stability
bull Eylea label = 5 x 112 then every 8 weeks ie fixed regime year 1
bull DRCRnet protocol T = effectively 6 x112 for majority (95) BUT actually only mandated for first 3 months then prn
bull helliphellip likely that majority will receive injections monthly for first 6 months
bull INDIVIDUALISED PHASE
bull Once ldquostablerdquo ndash based on VA and OCT
bull NB May never get a ldquodryrdquo OCT so treat to stability
bull THEN
bull Treat and extend
bull prn
What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

What does Treat and Extend mean
Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Pathway overview = Lucentis prn
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then observe UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Pathway overview = Treat and Extend
Jan
Loading phase = injections every 4 weeks until ldquostablerdquo for 3 visits or Eyleayear 1
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then keep injecting but extend the interval between injections gradually ie keep treating even if perfect
If reactivates need at least 2 injections until stable again over 3 visits
Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Pathway overview = Eylea fixed dosing year 1
Jan
Eylea = 5 x 112 injection then every 8 weeks
Average 6 injections yr 2 Beyond that
helliphelliphellip
Feb OctSepAugJulJunMayAprMar
MarFebJan
DecNov
DecNovOctSepAugJulJunMayApr
Then individualised UNTIL VA decreases or OCT increase = prn
Once reactivates need at least 2 injections until stable again over 3 visits
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Pros and cons of Treat and Extend vs Prn
T+E PRN
PROS bull Proactive patient and service get advance warning of injection ndash capacity and demand planning easier
bull One ndashstopbull Fewer visits than prnbull Overtreatment
advantageous for peripheral retinopathy
bull Only treated when active ieno overtreatment
bull Aggressive year 1 protocols (DRCRN I ndash few injections needed thereafter
bull DMO tolerant of reactivations ()
CONS bull Overtreatment = riskexpenseinconvenience
bull Evidence base scantbull Bilateral disease tricky
bull Reactive so need enoughemergency capacity to inject when disease flares up
bull No advance warning to patientservice that injection needed
bull NEED TO DO IT WELL ndashNHS real life audits prn based regimes not good resultsUndertreatment in year 1 Affects long term prognosis and treatment burden
DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

DMO ndash anti-VEGF Treat and Extend
bull Retain study ndash the only RCT data
bull Br J Ophthalmol 2015 Oct 9 pii bjophthalmol-2015-307249 doi 101136bjophthalmol-2015-307249 [Epub ahead of print]
bull Ranibizumab 05 mg treat-and-extend regimen for diabetic macular oedema the RETAIN study
bull Pruumlnte C1 Fajnkuchen F2 Mahmood S3 Ricci F4 Hatz K5 Studnička J6 Bezlyak V7 Parikh S7 Stubbings WJ7 Wenzel A7 Figueira J8 and the RETAIN Study Group
RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

RETAIN Phase III trial evaluating the efficacy of lsquotreat and extendrsquo regimen (ARVO 2014)
bull Patients with DMO and visual impairment (n = 372) were randomised 111
to one of three groups for 24 months
bull Two phases to dosing schedule
bull Phase A
bull Patients in all groups were initially treated with monthly ranibizumab until BCVA remained
stable
bull Phase B
bull Patients in the TampE groups whose vision remained stable had treatment- free intervals
that were increased incrementally by 1 month for a maximum of 3 months
bull Patients in the PRN group had ongoing monthly monitoring
bull In all groups Phase A was resumed if a decrease in BCVA was observed at a visit
Ranibizumab 05 mg monotherapy
in TampE regimen
Ranibizumab 05 mg in TampE regimen
plus laser
Ranibizumab 05 mg PRN
35
RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

RETAIN Visual acuity endpoints
Pruumlnte C ARVO 2014 Annual Meeting Abstracts Abstract 1700
Mean average change in BCVAat 12 months (primary endpoint)
Mean change in BCVA at 24 months
Mea
n av
erag
e ch
ange
in B
CVA
(ETD
RS
lette
rs)
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
RanibizumabTampE
RanibizumabTampE + laser
RanibizumabPRN
Mea
n ch
ange
in B
CVA
(ETD
RS
lette
rs)
plt00001 for both ranibizumab TampE groups versus PRN for primary endpoint
36
RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

RETAIN Patient visits and monitoring with TampE regimen over 24 months
bull The TampE regimen provided an approximately 40 reduction in the number of treatment visits required compared with the ranibizumab PRN regimen
bull Approximately 70 of patients receiving TampE regimens had monitoring intervals ge2 months compared with ongoing monthly monitoring in the ranibizumab PRN group
bull Informed the license for Lucentis in DMO (extend by 1 month at a time)
37
INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

INTRAVITREAL STEROIDSWhich intravitreal steroid is better
bull Licensed steroids ndash Ozurdex (Dexamethasone) and Iluvien (Fluocinoloneacetonide
bull Which steroid is best in terms of VA outcomes hellipWE DONrsquoT KNOW FOR SURE ndash no head to head studies for licensed drugs either between steroids or between anti-VEGF and steroids
bull STEROIDS ARE efficacious in DMO
bull MEAD
bull FAME
bull DRCRnet protocol I
bull NICE ndash Ozurdex and Iluvien ndash second-line agents
Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Ozurdex
bull A biodegradable co-polymer implant ndash degrades in time to lactic and glycolic acid releasing Dexamethasone
bull 22gauge injectionbull MEAD study
bull N=1048
bull Dex 07mg vs 035mg vs sham
bull No rescue therapy
bull 3 year follow up max 6 monthly dosing ie 7 over 3 years
Gan IM et al Greafes Acrh Clin Exp Ophthalmol 2005
MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

MEAD studyMean BCVA change from baseline based on baseline lens status
-2
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Mea
n C
hang
e Fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
DEX Implant 07 mg (n = 86)
Sham (n = 101)
Boyer DS et al Ophthalmology 20141211904ndash14
Results analyzed in the ITT population with LOCF for missing values
Pseudophakic
Total
0
5
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39
DEX 700 (n=351)
Sham (n=350)
10
8
6
4
2
0
Mea
n C
hang
e fr
om
Bas
elin
e B
CVA
(Let
ters
)
Month
07mg dose is approved as Ozurdexreg by the FDA and EMA 035mg dose not commercially available
1 Boyer DS et al Ophthalmology 2014 121 1904-1914
bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

bull Nonbioerodible micro implant (polyimide) containing 190microg of fluocinolone acetonide (FAc)
bull Consistent daily submicrogram delivery of 02 microgd FAc for up to 36 months
bull Posterior point of release
bull 35 mm times 037 mm non-bioerodable micro implant
bull 25-gauge injector creates self-sealing wound
bull No measurable systemic exposure
ILUVIEN Implant Technology
FAcimplant
ILUVIEN SPC httpwwwmedicinesorgukemcmedicine27636
0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

0 6 12 18 24 30 36
ILUVIEN 02 microgd FAc(n = 376)05 microgd FAc (n = 395)Control sham injection(n = 185)
Design of Phase 3 FAME Study (FAME A and B = same protocol)
Additional laser therapy allowed after week 6a
Retreatment any time after month 12 (if eligibleb)
Study ends
N = 956Randomisation
221Primary readout
Patients with DMO and
bull At least 1 previous laser tx
bull BCVA ge19 and le68 letters
bull TD-OCT FTH ge250 μm
Month
BCVA = best corrected visual acuity DMO = diabetic macular oedema TD-OCT=time domain optical coherence tomography FTH = foveal thicknessa At masked investigatorrsquos discretion b If BCVA loss ge5 letters or retinal thickening ge50 microm from best reading in previous 12 months
ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

ge15 letter Gain is Greater in Chronic DMO Patients
ge 15
-Let
ter I
mpr
ovem
ent
in B
CVA
Fro
m B
asel
ine
Δ = 98
Months
Full Population Patients With Chronic DMO
Months
Δ = 206
287
189134
34
Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Steroid re-treatments
bullOzurdexbull Longer half-life than anti-VEGF in the eye
bull Redosing regimes not very helpful from RCT data eg MEAD study only 612 dosing
bull In reality re-treatment interval may be shorter
bull POSOLOGY
bull Patients treated with OZURDEX who have experienced an initial response and in the physicians opinion may benefit from retreatment without being exposed to significant risk should be considered for retreatment Retreatment may be performed after approximately 6 months if the patient experiences decreased vision andor an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bullIluvienbull 70 of patients in FAE only needed 1
injection over 3 years
bull BUT additional rescue treatments allowed
bull POSOLOGY
bull Each ILUVIEN implant releases fluocinolone acetonide for up to 36 months An additional implant may be administered after 12 months if the patient experiences decreased vision or an increase in retinal thickness secondary to recurrent or worsening diabetic macular oedema
bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

bull Patients receiving escape medication were exited from MEAD before administration1
bull Macular laser rescue treatment allowed in RISERIDE (Lucentisreg) from 3 months2
bull Focalgrid laser allowed in FAME (Iluvienreg) from 6 weeks3
MEAD TREATMENT PROTOCOL
bull First treatment given at randomisation (day 0) bull Patients assessed for retreatment eligibility every 3 months from
months 6ndash36bull Patients were eligible for retreatment if
OCT optical coherence tomography
ge6 months since most recent
study treatment
Retinal thickness in 1 mm central macular
subfield by OCT gt175 microm
Evidence of residual retinal oedema (intraretinal cysts or
any regions of increased retinal thickening) as assessed by
investigator from OCT
AND OR
MEA
D
Amendment in May 2010 revised anatomic criterion for retreatment before this time the threshold was gt225 microm1Boyer DS et al Ophthalmology 2014 121 1904-19142Nguyen QD et al Ophthalmology 20121191064minus10773Campochiaro PA et al Ophthalmology 2011118626ndash635
Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Treatment burdenILUVIEN
Control(n =112)
02 microgd FAc(n =209)
Study Treatments(sham injection or ILUVIEN 02 microgday or FAc 05microgday)
1 treatment 661 761
2 treatments 277 187
ge 3 treatments 63 53
Rescue Laser Treatments (at masked physicianrsquos discretion after week 6)
Patients 607 407
Off-Protocol Treatments (IVTA bevacizumab ranibizumab intravitreal dexamethasone)
Patients 295 115
OZURDEX = 23injections year 1 41 by year 3
No other Rx
Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Summary of side effects with intravitreal steroids
Drug device Evidence base Cataract risk IOP rise (requiring drops)
Glaucoma surgery
endophthalmitis
ILUVIEN FAME studies 80 cat surgery(273 sham)
384(14 control)
48 0
Ozurdex MEAD 592 had cataract surgery(72 sham)
215 (end of study)(34 sham)
06 0
Trivaris+ laser vs Luc+laserx2 vs laser
Protocol IOphthalmology 2010
15 42(ONE OFgt10mmHg risegt30mmHGStart drops)
2186 0
NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

NICE guidance for intravitreal steroids in DMO
bull Iluvien
bull NICE TA 301 Iluvien for DMO Nov 2013
bull hellipfor treating chronic diabetic macular oedema that is insufficiently responsive to available therapies only if
bull the implant is to be used in an eye with an intraocular
(pseudophakic) lens and
bull the manufacturer provides fluocinolone acetonide intravitreal implant with the discount agreed in the patient access scheme
NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

NICE guidance for intravitreal steroids in DMO
bull Ozurdex
bull NICE TA 349 Ozurdex for DMO July 2015
bull there is an artificial lens in the eye to be treated and
bull their diabetic macular oedema has not improved with
non-corticosteroid treatment or such treatment is not suitable for them
Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Steroids = second line therapyWhen do I switch
bull Anti-VEGF first line for centre involving DMObull NICE TA ndash ldquoinsufficiently responsiverdquo ldquo ldquonot improvedrdquo ldquonot suitablerdquo ndash
OTHER TREATMENTS
bull 2 scenariosbull 1) Anti-VEGF canrsquot be funded ie OCTlt400um + PSEUDOPHAKIC
bull 2) Already had a course of treatment with laseranti-VEGF + PSEUDOPHAKIC ie SWITCHING from anti-VEGF to steroid
bull Plus
bull ldquochronicrdquo DMO ndash 3 years duration in FAME (18months) for ILUVIEN
bull Chronic DMO not essential for Ozurdex
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Protocol T ndash patients may not improve in first 6 months
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you
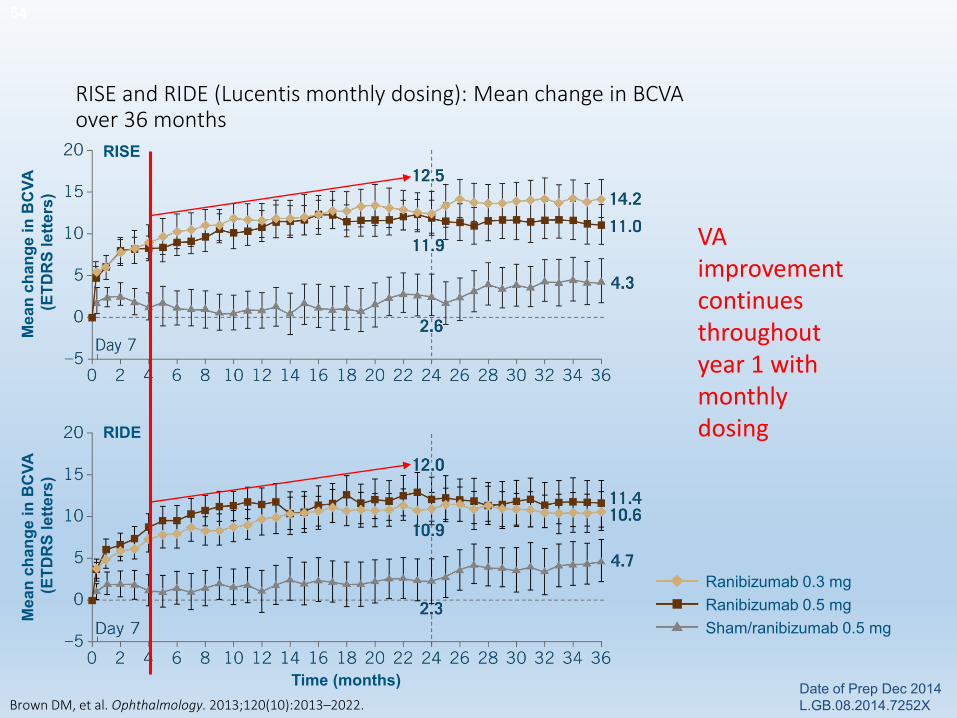
RIDE
RISE
Mea
n ch
ange
in B
CVA
(E
TDR
S le
tters
)M
ean
chan
ge in
BC
VA
(ETD
RS
lette
rs)
Time (months)
RISE and RIDE (Lucentis monthly dosing) Mean change in BCVA over 36 months
Brown DM et al Ophthalmology 2013120(10)2013ndash2022
54
Ranibizumab 03 mgRanibizumab 05 mgShamranibizumab 05 mg
Date of Prep Dec 2014 LGB0820147252X
VA improvement continues throughout year 1 with monthly dosing
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user ndash more than protocol
I
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
DRCRN protocol I5 year outcomesInjections 8-9 in year 1Year 2 = 2-3Year 3= 1-2Year 4 = 0-1Year 5 = 0
FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

FACTORS AFFECTING DECISION TO SWITCH FROM ANTI-VEGF TO STEROID
bull Drug response bull Patient factorsbull Heavy user
bull VA improved but ldquonot far enoughrdquo ie needs to regain driving license
bull Struggles with intra-vitrealtechnique
NO RESPONSEVA no changeOCT no change
SUBOPTIMALVA bettersameOCT improved but plateau
GOODBut frequent recurrences and re-dosing at 1 month intervals
Wait for plateau = stability in protocol T laserPatient factors again
Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Judgement of response to anti-VEGF ndashtimeframe
bull Wait 6 months in poor responders
bull Wait 1 year for heavy users
bull Tempting to try steroids earlier than this ifbull No glaucoma ndash not a deal breaker Ozurdex better short term optionbull Pseudophakic
bull Clues from the diseasebull chronic
bull PATIENT FACTORS
bull Any eyes avoid steroids ndash advanced glaucomaCSCR Or prior viral retinitis RARE
bull Any eyes avoid anti-VEGF pregnancytrying to concieve recent CVA
BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

BIOMARKERS AT BASELINE WOULD BE USEFULRESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you
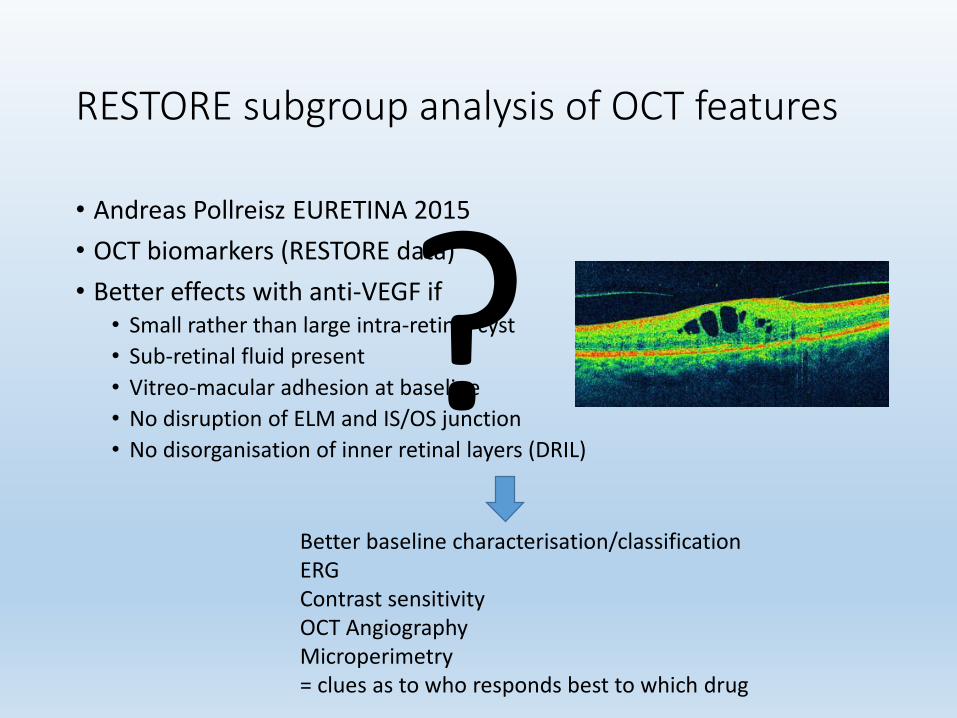
RESTORE subgroup analysis of OCT features
bull Andreas Pollreisz EURETINA 2015
bull OCT biomarkers (RESTORE data)
bull Better effects with anti-VEGF ifbull Small rather than large intra-retinal cyst
bull Sub-retinal fluid present
bull Vitreo-macular adhesion at baseline
bull No disruption of ELM and ISOS junction
bull No disorganisation of inner retinal layers (DRIL)
Better baseline characterisationclassificationERG Contrast sensitivityOCT AngiographyMicroperimetry= clues as to who responds best to which drug
Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Plan for this presentation helliphellipa long list
bull What treatment options are available for DMO (evidence base)
bull What treatment should I start with at baselinebull Re-treatment algorithms for intravitreal DMO therapiesbull When should I switchcombine therapiesbull The bigger picture
bull Other eyebull The patient as a wholebull The service -coping with capacity ndash compromises
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you
The bigger pictureOther eyeThe patient as a wholeThe service -coping with capacity ndash compromises
bull OTHER EYE ndash may create problems
bull Treat and extend ndash ldquoreduce of visitsrdquo plus Eylea license ndash ldquono need for monitoringrdquo may not benefit if lots of visits due to PDR other eye
bull PERIPHERAL RETINA anti-VEGF supresses proliferative disease - Rebound on stopping Rx
bull PATIENT
bull Anti-VEGF ndash heavy user - Will comply
bull One stop much better than two stop for patient ndash Treat and extend
bull SERVICE
bull Capacity and demand planning = fixedT+E more predictable at least 1 month in advance ndash flexible nurse injectors
bull Steroids ndash even if well controlled (Iluvien for 3 years) need IOP check
bull Need pan-retinal examination both eyes ndash separate visits
Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Summary
CSMO
No centre involvement
Photocoagulation
Centre involvement
gt 78 letters(normalminimally reduced VA)
Photocoagulation
VA 78ndash24 letters
Phakic
Anti-VEGF
Pseudophakic
Anti-VEGF
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you
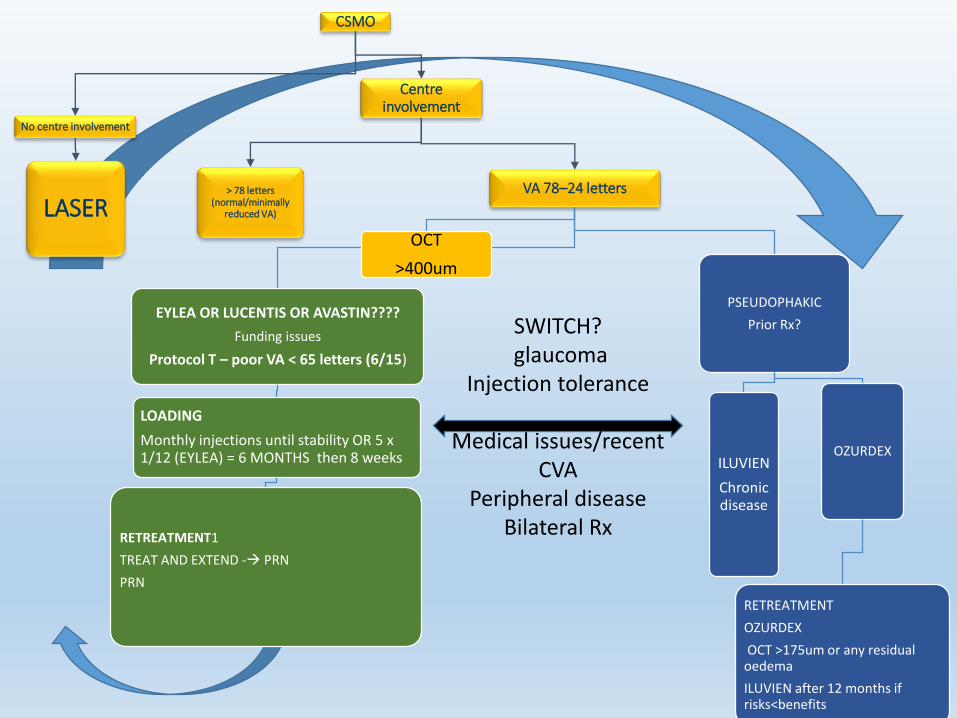
SWITCHglaucoma
Injection tolerance
Medical issuesrecent CVA
Peripheral diseaseBilateral Rx
CSMO
No centre involvement
LASER
Centre involvement
gt 78 letters(normalminimally
reduced VA)
VA 78ndash24 letters
EYLEA OR LUCENTIS OR AVASTIN
Funding issues
Protocol T ndash poor VA lt 65 letters (615)
LOADING
Monthly injections until stability OR 5 x 112 (EYLEA) = 6 MONTHS then 8 weeks
RETREATMENT1
TREAT AND EXTEND - PRN
PRN
PSEUDOPHAKIC
Prior Rx
ILUVIEN
Chronic disease
OZURDEX
RETREATMENT
OZURDEX
OCT gt175um or any residual oedema
ILUVIEN after 12 months if risksltbenefits
OCT
gt400um
bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

bull FACE TO FACE CLINICS RUNNING IN PARALLEL
bull = MAC002 every 6 months (optom or doctor) routine check for cataracttolerance of injectionsglaucoma issues etc
bull =MAC003 (DOCTOR) for problems as needed no fixed intervalDischargestop treatmentDeclines treatment diagnosis CSR overlay etcswitch drugs
bull =RV002- (DOCTOR) every 6 months
bull =DM002 ndash (DOCTOR) variable interval determined by last assessing doctor
bull First visit at 6 months from 1st injection if mild NPDR
bull Otherwise determined by retinopathy generally
LOADING PHASE
EyleaLucentis 1 within 48hrs of baseline
EyleaLucentis 2 (and LogMAR VA plus OCT same visit)
EyleaLucentis 3 (and LogMAR VA plus OCT same visit)
EyleaLucentis 4 (TEinj)(and Logmar VA plus OCT same visit
AFTER INJECTION 4 data goes off to be reviewed immediately as a hellip
TREAT AND EXTEND assessment ndash the next interval will depend on the response to the loading phase
NB -DMO patients ndash majority (95) will need 6 injctions x 112 of Lucentis
OR Eylea 5 x 112 then 8 weekly
ONCE STABLE for 3 x injection in TE phase
VIRTUAL CLINIC MONITORING OF MACULOPATHY AND PRN RETREATMENT
ANTI-VEGF INJECTION PATHWAYS Baseline visitMAC001 for wet AMDRV001 for CRVOBRVOMed ret clinic for DMO
Pathways ndash too many directions
Better that thanhellip
Thank you

Pathways ndash too many directions
Better that thanhellip
Thank you

Thank you