treatment of myeloma - royal bournemouth hospital · initial treatment with vad type regimen and...
TRANSCRIPT
Treating myeloma
Dr Rachel Hall
Royal Bournemouth Hospital
Treatment overview
• When to treat ?
• Aim of treatment
• Which treatment ?
• Monitoring response to treatment
• Prevention of complications
• What happens at relapse ?
• New treatments
Myeloma
• Treatable but not curable
• After many years with little change – several new drugs
• Survival improving
• Area of very active research – clinical trials
• Initial treatment – good information from trials –current standard treatments
• Relapsed disease – no standard but several options now

Treating myeloma is more than
just anti-myeloma drugs
• Symptom control
• Supportive care
– Transfusions, EPO
– Treatment of infections etc
• General measures – back care, hydration etc
• Pastoral / spiritual care

When to treat ?
• Calcium increased
• Renal Impairment
• Anaemia
• Bone disease
• Hyperviscosity
• Spinal Cord compression

Emergency treatment
• Steroids
• Emergency radiotherapy
Other treatments: antibiotics,
transfusion, pain killers,
bisphophonates + fluids,
dialysis
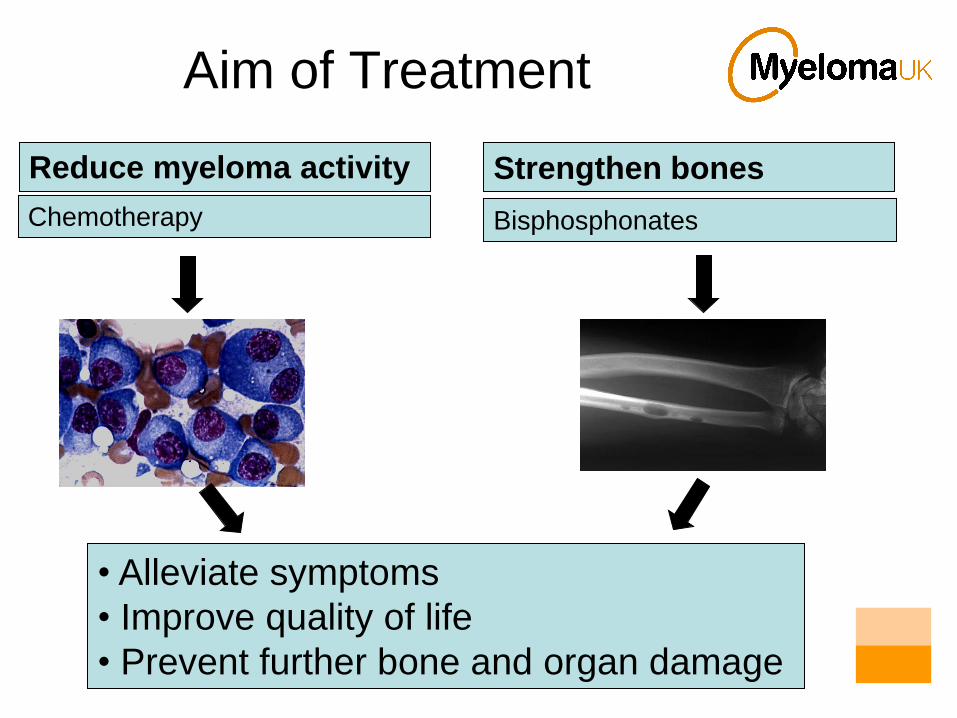
Aim of Treatment
Reduce myeloma activity
Chemotherapy
• Alleviate symptoms
• Improve quality of life
• Prevent further bone and organ damage
Strengthen bones
Bisphosphonates

Treatment of bone disease
BISPHOSPHONATESSodium clodronate tablets
Zeledronate intravenously
Pamidronate intravenously
• Strengthen bones
• Stop myeloma driven bone breakdown
• Direct anti-myeloma effect
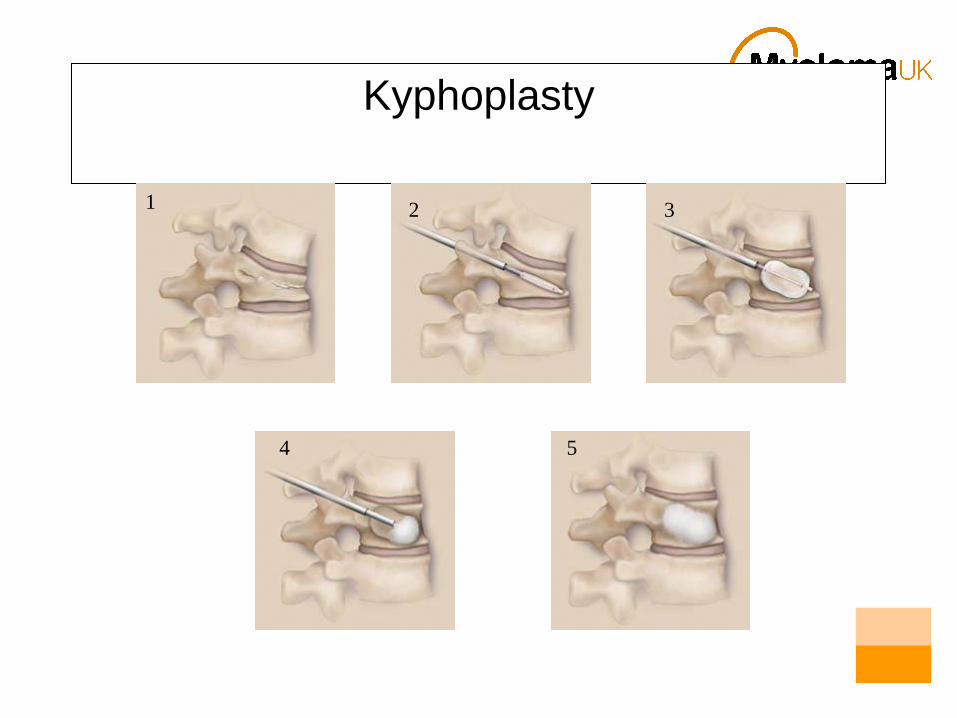
Kyphoplasty
1 2 3
4 5

Chemotherapy
Chemotherapy Cancer

Myeloma treatment – initial
Divided into two groups:
• Younger patients (<70 years) who are
candidates for autologous stem cell transplant
• Older patients, other patients not fit for
autologous stem cell transplant

Younger patients
• The aim of standard initial treatment is
– to induce remission
– to spare stem cells (avoid melphalan at this
stage)
• Then collect stem cells (peripheral blood)
• Then proceed to high dose melphalan
(200mg/m2) followed by blood stem cell rescue
(autograft / autologous transplant)

Which chemotherapy in newly diagnosed myeloma ?
Myeloma IX Trial
Induction
Consolidation
Maintenance
Eligible for
TransplantationNot eligible for
Transplantation
C-VAD or CTD
Stem cell harvest
Autologous transplantation
Consider mini-allogeneic
transplantation
No treatment or thalidomide
MP or attenuated CTD
Maximal response
Induction chemotherapy
• High response rates
• Most regimens are given as an outpatient
• May require a tunnelled central line insertion
• Steroids important component & synergistic

Intravenous treatment : C-VAD
• Cyclophosphamide weekly orally day 1,8,15
Vincristine and Adriamycin intravenously via pump day 1-4
Dexamethasone (steroids) days 1-4 and 12-15
• Cycle repeated every 3 weeks
• 4-6 cycles
• Alternatives: VAD, C-VAMP, Z-DEX
One cycle

Thalidomide: How it works

Thalidomide: Side effects
• Dose 50 - 200mg daily
• Side effects : drowsinessconstipationperipheral neuropathythrombosis

Oral treatments
• Cyclophosphamide weekly
Thalidomide daily
Dexamethasone in pulses
• Cycle repeated 3-4 weekly
• 4-9 courses
• Melphalan day 1-7
Prednisolone day 1-7
Thalidomide daily 1-28
• Cycle repeated 4 weekly
• 6-9 courses
MPT CTD
Which regimen for which patient?
• MPT
• Generally patients
>70
• Very well tolerated
• Not ideal in renal
failure or if stem cell
collection planned
• CTD (a)
• Generally patients <70
• Patients in whom stem cell collection being considered
• Dexamethasone can give SEs
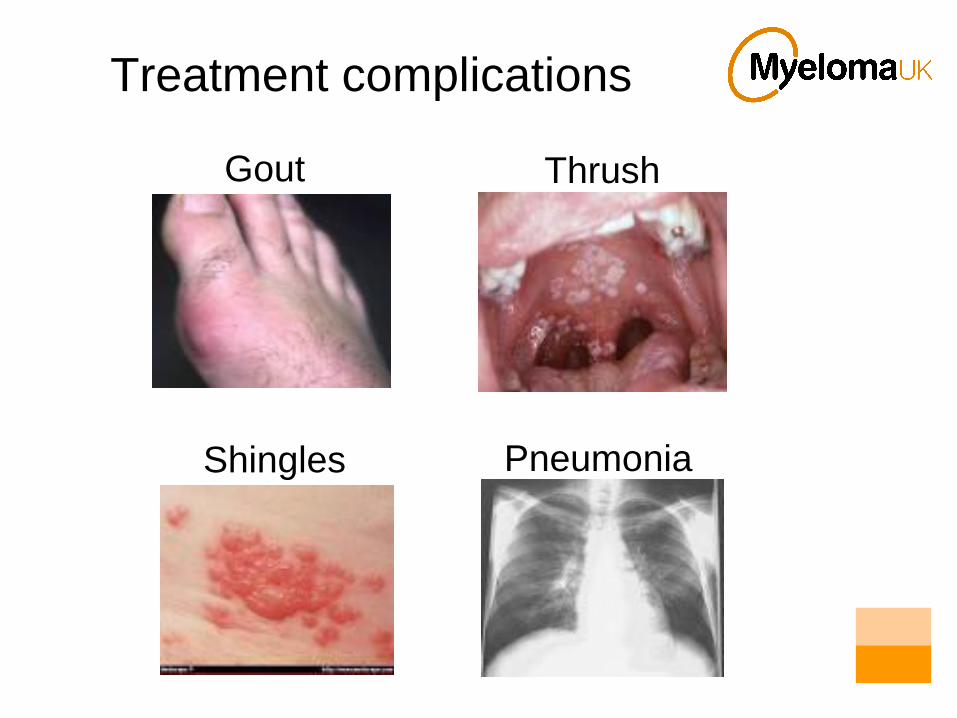
Treatment complications
Gout Thrush
Shingles Pneumonia
Treatment prophylaxis
Drugs needed in addition to the chemotherapy to
prevent side effects / complications:
Anti-nausea drugs Anti-gout drugs
Antacids (omeprazole) Antibiotics
Antivirals (aciclovir) Antifungals (fluconazole)
Laxatives Blood thinners (clexane)
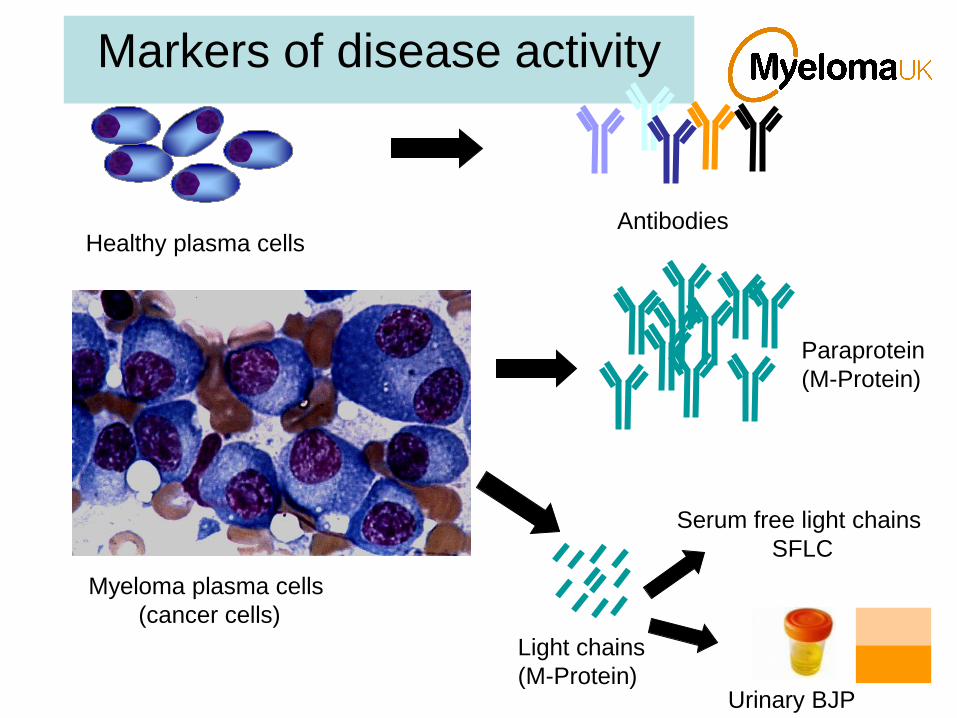
Markers of disease activity
Healthy plasma cellsAntibodies
Myeloma plasma cells
(cancer cells)
Paraprotein
(M-Protein)
Light chains
(M-Protein)Urinary BJP
Serum free light chains
SFLC

Response to treatment
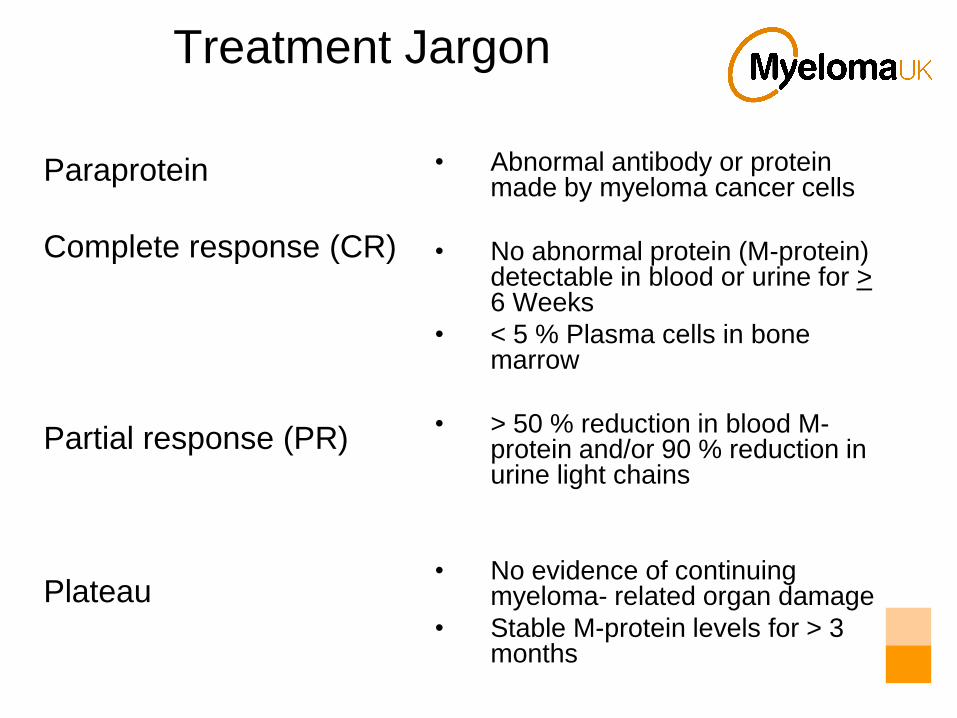
Treatment Jargon
Paraprotein
Complete response (CR)
Partial response (PR)
Plateau
• Abnormal antibody or protein made by myeloma cancer cells
• No abnormal protein (M-protein) detectable in blood or urine for > 6 Weeks
• < 5 % Plasma cells in bone marrow
• > 50 % reduction in blood M-protein and/or 90 % reduction in urine light chains
• No evidence of continuing myeloma- related organ damage
• Stable M-protein levels for > 3 months

Autologous stem cell transplant
• Used in selected younger patients (<70yrs)
• Used to consolidate the response and increase
the duration of response
• Stem cells collected with chemo and GCSF
• High dose melphalan (HDM) used and the bone
marrow „rescued‟ with patients own stem cells
• High risk chemotherapy with many side-effects.
Mortality 1-3 %

How to replace the bone marrow –
autologous stem cell
transplantation
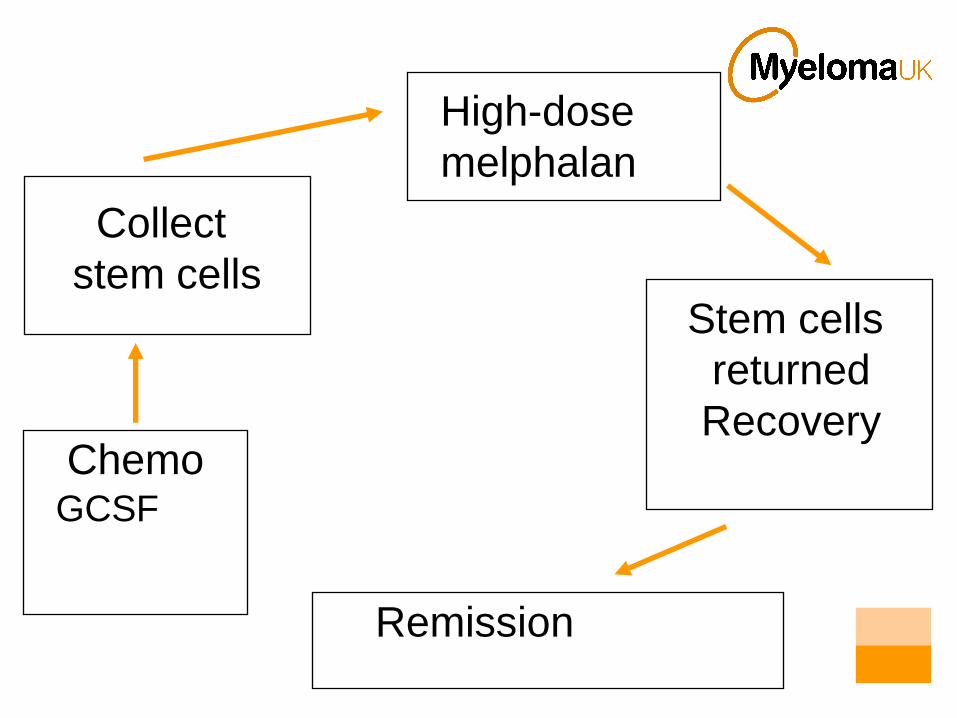
Collect
stem cells
High-dose
melphalan
Stem cells
returned
RecoveryChemo
GCSF
Remission

Side-effects of stem cell
transplant
• Mucositis
• Infection
– Bleeding
– Fluid retention
– Breathing difficulties

Maintenance treatment
Reference: Attal, M. et al. Blood 2006;108:3289-3294
Figure 1. Event-free survival according to treatment arm
Thalidomide

Treatment of relapsed myeloma
• If first remission lengthy (>1 year) – consider same treatment again
• If not already had thalidomide – consider thalidomide (with dexamethasone)
• Bortezomib (with dexamethasone)
• Bortezomib with liposomal doxorubicin
• Lenalidomide with dexamethasone
• Clinical trials
• Dexamethasone alone
• Supportive care
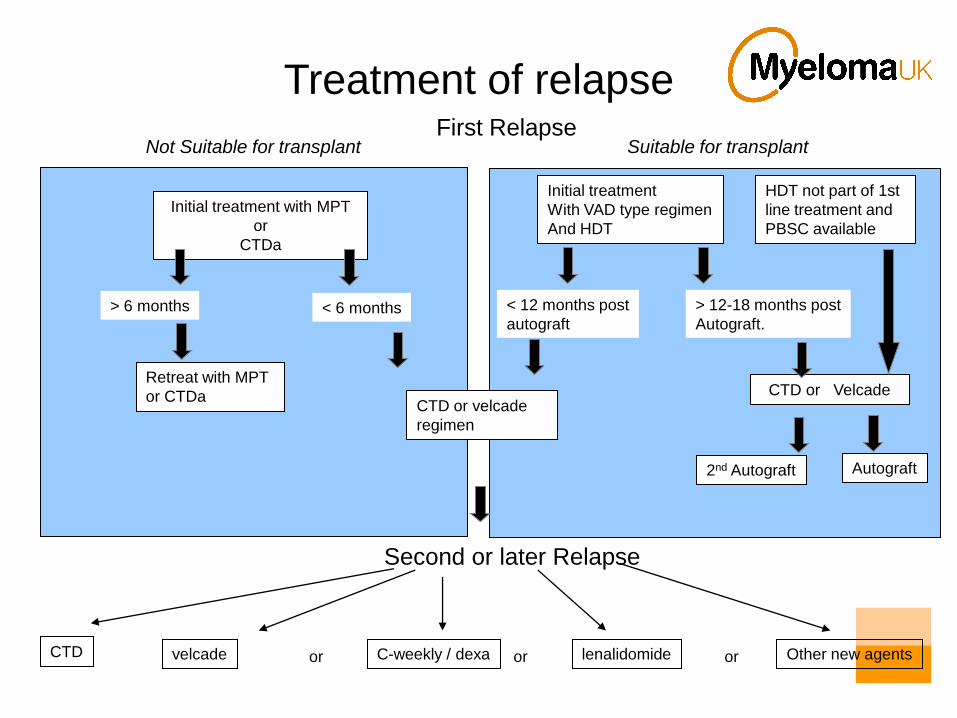
First Relapse
Second or later Relapse
Initial treatment with MPT
or
CTDa
Initial treatment
With VAD type regimen
And HDT
> 6 months < 6 months < 12 months post
autograft
> 12-18 months post
Autograft.
Suitable for transplantNot Suitable for transplant
HDT not part of 1st
line treatment and
PBSC available
Autograft2nd Autograft
CTD or VelcadeCTD or velcade
regimen
Retreat with MPT
or CTDa
orvelcade C-weekly / dexa lenalidomide Other new agentsor or
Treatment of relapse
CTD

Jacky Pickles, Janice Wrigglesworth and Marie
Morton
29th March 2007: The National
Institute for Health and Clinical
Excellence’s (NICE) announced
a review of its own ruling
denying patients NHS access
to Bortezomib (Velcade)
The “Velcade three”

Velcade : How it works

Side-effects of bortezomib
• Nausea
• Constipation
• Diarrhoea
• Low platelets
• Neuropathy
• Bortezomib, an inhibitor of proteasomes (sites
of protein degradation in cells), has activity
against advanced multiple myeloma
• This study compared bortezomib with high-
dose dexamethasone in relapsed myeloma
• Bortezomib was superior to dexamethasone in
all end points and prolonged overall survival
Bortezomib or High-Dose
Dexamethasone for Relapsed
Multiple Myeloma (APEX study)
Bortezomib
(Velcade)
• Response in 35- 38 % as single agent
• Response 50 % if used with dexamethasone
• Licensed for relapsed and refractory disease
• Major toxicities are neuropathy,
thrombocytopenia
• IV therapy 1.3 mg/m2 days 1,4,8 and 11.
• Dexamethasone tablets days 1,2,4,5,8,9,11,12
Lenalidomide

Lenalidomide
• Strong data for 2nd line use onwards
– Weber D et al Lenalidomide plus Dexamethasone for
Relapsed Multiple Myeloma in North America. NEJM
2007;357:21
– Dimopoulos M et al Lenalidomide plus Dexamethasone
for Relapsed or Refractory Multiple Myeloma. NEJM
2007;357:21
– 700 patients in these trials
– Lena + Dexa vs Placebo + Dexa
– Patients who had progressed after >= 1 therapy
– 48 weeks Lena arm vs 20 weeks Dexa alone
– ORR 65%

Lenalidomide
• Related to thalidomide
• Oral medication taken D1 – 21 in a 28 day cycle
• Well tolerated
• Less sleepiness, constipation, neuropathy
• Clots
• Much more suppression of bone marrow (low white cells and platelets)
• fatigue

Future
• Risk stratified treatment
• Development of new targeted treatments
• New regimes using thalidomide, velcade and
lenalidomide
• Development of other thalidomide analogs
• Continue to improve quality of life

www.myeloma.org.uk