transverse growth of maxilla and mandible
DESCRIPTION
kkkTRANSCRIPT

scdsmsEeavad(tagt
Transverse Growth of Maxilla and MandibleRam Nanda, Stephen F. Snodell, and Prashanti Bollu
Growth in the transverse plane has not received due emphasis in the
diagnosis of craniofacial and dentoalveolar anomalies. Because the research
focus has largely been on sagittal and vertical planes of the face, inferences
on normal and abnormal growth patterns have been limited to these planes.
This article is based on a section of the extensive research done on growth
and development of dentofacial structures at the University of Oklahoma.
Nine transverse craniofacial and dentoalveolar measurements were made
on anteroposterior radiographs of 25 male and 25 female subjects between
the ages of 6 and 18 years. The average measurements at each age are
presented. Regression models suggest a strong prediction of adult size at
age 12. Large prospective longitudinal studies using regression models are
needed to validate this evidence. (Semin Orthod 2012;18:100-117.) © 2012
Elsevier Inc. All rights reserved.
tpoaclmvtnt
octaqolccgstotwll
G rowth of the human face is a multidimen-sional and dynamic continuum. To mea-
ure and interpret the incremental changes oc-urring during growth, the use of appropriateiagnostic tools is paramount. A comprehen-ive analysis of craniofacial growth includesonitoring growth changes in all 3 planes of
pace, that is, transverse, sagittal and vertical.ach plane offers unique information on thextent and direction of growth status, ultimatelyiding in the overall treatment planning. Trans-erse growth changes shed light on dentofacialsymmetries, expanded/constricted jaws, andental crossbites. The sagittal or anteroposteriorAP) dimension offers a great deal of informa-ion on facial profile, arch length discrepancies,nd excessive/inadequate overjets. Verticalrowth patterns allow visualizing facial propor-ions, deep bites, and open bites.
Professor Emeritus, Department of Orthodontics, College of Den-tistry, University of Oklahoma, Oklahoma City, OK; Orthodontist,Private Practice, Cedar Park, TX; Orthodontic Resident, College ofDental Medicine, Roseman University of Health Sciences, Hender-son, NV.
Address correspondence to Ram Nanda, BDS, DDS, MS, PhD,Department of Orthodontics, College of Dentistry, University ofOklahoma, 7600 Dorset Drive, Oklahoma City, OK 73116.E-mail: [email protected]
© 2012 Elsevier Inc. All rights reserved.1073-8746/12/1802-0$30.00/0
ddoi:10.1053/j.sodo.2011.10.007
100 Seminars in Orthodontics, Vol 18, N
The timing of orthodontic intervention is of-en challenging to even the most experiencedractitioners. A good understanding is neededn the growth of jaws, including the totalmount of growth, timing of growth spurts, andessation or near completion of growth. Manyongitudinal growth studies have been done to
easure these incremental changes and to de-elop normative values. Although it is importanto note that individual variations exist, theseorms serve as a useful guide for the clinician in
he overall decision process.An invaluable aid in the proper diagnosis and
rthodontic treatment planning of a growinghild is the ability to predict future growth po-ential. Assessment of growth potential requires
thorough knowledge on the extent and se-uence of growth completion. Although devel-pment and maturation continue throughout
ife, growth reaches its maximum potential at aertain age. In assessing the completion ofraniofacial growth, it is important to note thatrowth in all 3 dimensions does not stop at theame time. Several longitudinal studies have at-empted to identify the age at near completionf growth of the jaws. More congruence exists onhe sequence of growth patterns than the age athich maximum growth is achieved. Growth fol-
ows the sequential completion of cranium fol-owed by facial width (transverse), then facial
epth (sagittal), and lastly height (vertical).1 Al-o 2 (June), 2012: pp 100-117

alc
uhfit
immiadhdinitomt
mw
djmvttSaoFwfi
mfd
hcaotuwte
101Transverse Growth of Maxilla and Mandible
though AP and vertical growth continue wellinto adulthood, Class II, Class III relations andrelapse of deep bites and open bites are oftenseen.2 These continued structural changes arelso responsible for deterioration of occlusal re-ationships and the relapse of malocclusion afterompletion of orthodontic treatment.3
Interestingly, facial width, the largest facialdimension at infancy, shows the least relativegrowth rate compared with the facial depth andheight.4 Transverse growth is found to achievenear completion by late adolescence; however,sagittal and vertical growth continue well intoadulthood. Recent research, however, conteststhis accepted phenomenon on sequential com-pletion and shows evidence of overlap in 3 di-mensions, indicating that although growth ofsome transverse dimensions, such as cranial andinterjugal width, end much before AP and ver-tical growth, interzygomatic and intergonialwidths continue to increase well into adult-hood.5 Careful attention to these details is im-portant in effective orthodontic treatment man-agement, especially during the retention periodto control for the effects of late growth changes.
Developing an effective orthodontic diagnos-tic workup is a challenging process. Severalcephalometric radiographic analyses developedover the years assist the clinician in diagnosingtransverse relationships between jaws. TheRocky Mountain analysis6 and the Ricketts anal-ysis7 are among the most popular and widely
sed cephalometric analyses. These analyses,owever, represent a certain demographic pro-le, and hence, caution must be applied in using
hem as true norms.Annual growth increments assist in measur-
ng the growth extent and rate. Various land-arks have been used to monitor growth incre-ents. Transverse craniofacial measurements
nclude widths of cranial, facial, nasal, maxillary,nd mandibular structures. The use of interjugalistance (bijugale) in measuring maxillary widthas been validated by previous studies.8-10 Man-ibular width, however, has been measured us-
ng the distance between gonions10 and antego-ial notches.8,11 Hesby et al9 measured both
ntergonial and interantegonial distances. Den-al arch dimensions change gradually as a resultf growth and as a result of orthodontic treat-ent. These changes in the transverse plane are
ypically measured at the intercanine, interpre- d
olar, and intermolar regions of the maxilla asell as the mandible.
To measure transverse growth changes in theentoalveolar structures of upper and lower
aws, previous studies used dental casts, whereasore recent studies used posteroanterior (PA)
iews. Arch width measurements are usuallyaken at the intercanine, interpremolar, and in-ermolar areas of the maxilla and mandible.ome studies recorded the intermolar distancest first as well as second molars. Different meth-ds have been used in measuring these widths.or instance, intermolar width measurementsere done between bilateral gingival points ofrst molars,9 central fossae of maxillary first
molars, and distobuccal cusp tips of mandibu-lar first molars.12,13 Other studies used the
ost prominent lateral points on buccal sur-aces of the molars to measure the intermolaristance.14
An overview of recent scientific literatureshows the limited emphasis and evidence avail-able on the transverse growth of jaws. A signifi-cant number of people present with transversejaw discrepancies, demanding special attentionto this plane of space. Intraarch asymmetries arefound to be more severe in the transverse thanin the AP plane.15 Early diagnosis is critical forthe correction and treatment of such discrepan-cies. The multifactorial etiology behind the de-velopment of transverse discrepancies makesidentifying and eliminating the etiologic factordifficult. The goal of the present article is toprovide an in-depth summary on transversegrowth changes of the craniofacial and dentoal-veolar complex. In addition, the potential forpredictive growth changes at 6 years and 12 yearswill be presented.
Methods
The research16 done at the University of Okla-oma presents information on longitudinal re-ords of 25 males and 25 females between theges of 6 and 18 years. All subjects had Class Icclusion with absence of crossbites and no his-ory of orthodontic treatment. The current studyses the same data to investigate the age athich predictive potential of future growth is
he strongest. The information recorded as av-rage size and annual increments of 9 transverse
imensions (Fig. 1) identified relationships be-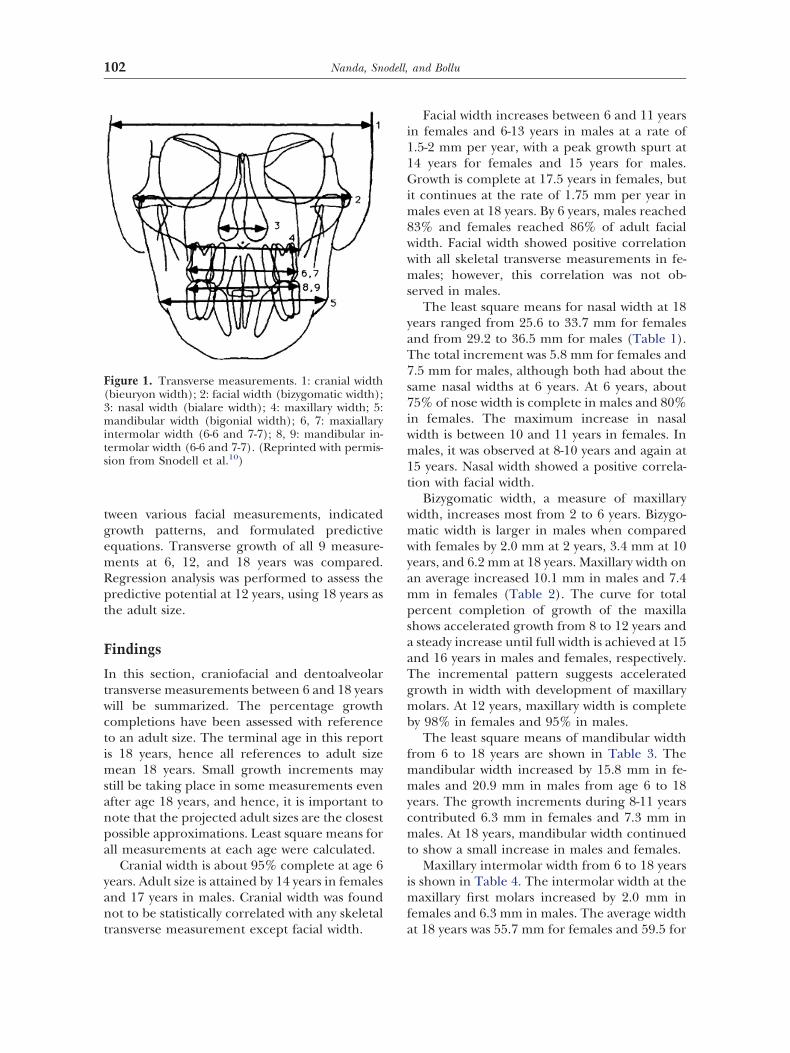
102 Nanda, Snodell, and Bollu
tween various facial measurements, indicatedgrowth patterns, and formulated predictiveequations. Transverse growth of all 9 measure-ments at 6, 12, and 18 years was compared.Regression analysis was performed to assess thepredictive potential at 12 years, using 18 years asthe adult size.
Findings
In this section, craniofacial and dentoalveolartransverse measurements between 6 and 18 yearswill be summarized. The percentage growthcompletions have been assessed with referenceto an adult size. The terminal age in this reportis 18 years, hence all references to adult sizemean 18 years. Small growth increments maystill be taking place in some measurements evenafter age 18 years, and hence, it is important tonote that the projected adult sizes are the closestpossible approximations. Least square means forall measurements at each age were calculated.
Cranial width is about 95% complete at age 6years. Adult size is attained by 14 years in femalesand 17 years in males. Cranial width was foundnot to be statistically correlated with any skeletal
Figure 1. Transverse measurements. 1: cranial width(bieuryon width); 2: facial width (bizygomatic width);3: nasal width (bialare width); 4: maxillary width; 5:mandibular width (bigonial width); 6, 7: maxiallaryintermolar width (6-6 and 7-7); 8, 9: mandibular in-termolar width (6-6 and 7-7). (Reprinted with permis-sion from Snodell et al.10)
transverse measurement except facial width.
Facial width increases between 6 and 11 yearsin females and 6-13 years in males at a rate of1.5-2 mm per year, with a peak growth spurt at14 years for females and 15 years for males.Growth is complete at 17.5 years in females, butit continues at the rate of 1.75 mm per year inmales even at 18 years. By 6 years, males reached83% and females reached 86% of adult facialwidth. Facial width showed positive correlationwith all skeletal transverse measurements in fe-males; however, this correlation was not ob-served in males.
The least square means for nasal width at 18years ranged from 25.6 to 33.7 mm for femalesand from 29.2 to 36.5 mm for males (Table 1).The total increment was 5.8 mm for females and7.5 mm for males, although both had about thesame nasal widths at 6 years. At 6 years, about75% of nose width is complete in males and 80%in females. The maximum increase in nasalwidth is between 10 and 11 years in females. Inmales, it was observed at 8-10 years and again at15 years. Nasal width showed a positive correla-tion with facial width.
Bizygomatic width, a measure of maxillarywidth, increases most from 2 to 6 years. Bizygo-matic width is larger in males when comparedwith females by 2.0 mm at 2 years, 3.4 mm at 10years, and 6.2 mm at 18 years. Maxillary width onan average increased 10.1 mm in males and 7.4mm in females (Table 2). The curve for totalpercent completion of growth of the maxillashows accelerated growth from 8 to 12 years anda steady increase until full width is achieved at 15and 16 years in males and females, respectively.The incremental pattern suggests acceleratedgrowth in width with development of maxillarymolars. At 12 years, maxillary width is completeby 98% in females and 95% in males.
The least square means of mandibular widthfrom 6 to 18 years are shown in Table 3. Themandibular width increased by 15.8 mm in fe-males and 20.9 mm in males from age 6 to 18years. The growth increments during 8-11 yearscontributed 6.3 mm in females and 7.3 mm inmales. At 18 years, mandibular width continuedto show a small increase in males and females.
Maxillary intermolar width from 6 to 18 yearsis shown in Table 4. The intermolar width at themaxillary first molars increased by 2.0 mm infemales and 6.3 mm in males. The average width
at 18 years was 55.7 mm for females and 59.5 for
igpS
inim
103Transverse Growth of Maxilla and Mandible
males. Interestingly, by 6 years of age, the max-imum intermolar width achieved was 96% infemales and 88% in males. Maxillary intermolarwidth at second molars showed an increase of1.4 mm in females, whereas the males showed anincrease of 3.7 mm (Table 5).
The least square means of mandibular inter-molar width are shown in Table 6. Transversegrowth change in this area was found to be little,with a slight decrease until 11 years. The man-dibular intermolar width at the second molars(Table 7) decreased by 2.1 mm in females and1.2 mm in males from age 12 to 18 years.
Table 8 presents the percentage completionof each transverse craniofacial dimension at 6years and at age at which 100% growth wasfound to be complete. All dental measurementswere found to be highly correlated with eachother. Although most skeletal and dental trans-verse growth was almost complete before 18years in females, mandibular width continued togrow beyond 18 years. Mandibular intermolarwidth at first and second molars, however, wasfully complete before 15 years in both males and
Table 1. LSMean, SD, Min, and Max Values for NasaYears
Age (Years) Gender Subjects
6 M 22F 17
7 M 19F 20
8 M 21F 22
9 M 21F 21
10 M 19F 22
11 M 19F 21
12 M 21F 23
13 M 20F 22
14 M 16F 21
15 M 18F 17
16 M 19F 14
17 M 20F 15
18 M 11F 9
LSMean, least squares mean; SD, standard deviation; Min, m
females. In males, except for facial width, most
skeletal and dentoalveolar measurements con-tinued to increase beyond 18 years.
Predictions of Dental Arch Widths
Different approaches have been proposed topredict the maxillary and mandibular archwidths. Some well-recognized indices to predictmaxillary arch width include analyses by Pont,17
Howe et al,18 and Schwarz and Gratzinger.19
Mandibular arch width measurements havebeen done in several different ways. Bonwill20
used the sum of 6 anterior teeth to predict man-dibular arch width. Many earlier studies devel-oped indices based on limited variables leadingto potential biases. Recent investigations by Nim-karn et al21 criticized the inaccuracies inherentn several indices. The advantages of using re-ression analyses over indices in making growthredictions of dental arches were first used bynodell et al10 (Figs. 2–19) and more recently by
Alvaran et al.22
Our research at University of Oklahoma indi-cates that growth at 6, 12, and 18 years showed
dth in Millimeters for Males and Females Aged 6-18
SMean SD Min Max
22.93 1.92 18.21 26.9822.88 1.66 19.87 26.4223.48 2.03 20.77 27.5023.17 2.10 19.13 26.7824.56 1.87 20.13 27.8624.09 2.16 20.16 27.9724.70 2.06 21.05 28.8824.58 2.42 21.83 29.6026.12 2.11 23.30 29.7224.94 2.55 20.09 29.8726.49 1.77 23.98 29.7226.14 2.23 20.09 29.8727.39 2.54 23.02 32.2026.55 2.45 21.38 30.5827.84 2.44 23.54 32.7027.14 2.60 21.10 32.4027.81 2.64 22.93 31.9327.70 2.15 25.08 33.0628.98 2.66 25.48 33.8828.12 2.50 25.31 34.0829.10 2.42 24.57 35.0728.32 3.13 22.90 33.2529.88 2.40 24.81 35.2628.76 3.12 21.72 34.6230.48 2.07 29.25 36.5528.64 2.49 25.56 33.68
um; Max, maximum; F, females; M, males.
l Wi
L
reliable and discernible patterns. Our investiga-

fo
T
inim
104 Nanda, Snodell, and Bollu
tion highlights the correlation between strengthof predictability and percentage growth-relatedchanges. Cranial width increased only by 4%-6%between 6 and 18 years, indicating that most ofthe transverse cranial width is completed by thisage, and that growth at 6 years could serve as avaluable reference point when predicting trans-verse growth. However, predictability of growthcompletion based on growth at 12 years wasmore significant than that at 6 years (Table 9).At 12 years, maxillary width is complete by 98%in females and 95% in males.
Factors Influencing Transverse Growth
Genetics
“It is estimated that about two-thirds of the25000 human genes are involved in the complexprocess of craniofacial development.”2 Externalor internal influences on this process could alterthe pattern of craniofacial growth and develop-ment. Developmental disturbances, such asclefts in the lip and palate, may adversely influ-
Table 2. LSMean, SD, Min, and Max Values for Max6-18 Years
Age (Years) Gender Subjects
6 M 22F 17
7 M 21F 21
8 M 21F 24
9 M 22F 23
10 M 19F 22
11 M 21F 22
12 M 21F 23
13 M 23F 22
14 M 18F 20
15 M 15F 17
16 M 20F 14
17 M 20F 15
18 M 11F 9
LSMean, least squares mean; SD, standard deviation; Min, m
ence growth in the transverse dimension. b
Age
Age is an important determinant of skeletal aswell as dental maturation. In this context, it isimportant to emphasize that chronologic ageand dental age do not match quite often. Al-though most transverse craniofacial growth iscomplete by age 18 years, our research showsthat dental transverse measurements (maxillaryand mandibular intermolar widths) reach adultsize by age 6 years. The timing of the adolescentgrowth spurt largely influences treatment deci-sions, and hence, it is important to seek appro-priate diagnostic measures, such as hand-wristx-rays or cervical vertebrae, to identify peak ofthe adolescent growth spurt. Transverse growthof the maxilla, for instance, shows a distinctadolescent peak at 14-15 years.23 The findingsrom our research substantiate further the rolef age in understanding transverse growth.
Gender
ransverse dimensional differences between
Width in Millimeters for Males and Females Aged
SMean SD Min Max
56.17 2.34 51.13 60.1954.44 1.86 51.28 59.0057.67 2.23 53.66 61.6455.52 2.10 51.28 60.0458.63 2.16 54.76 62.5556.71 2.23 51.34 62.4560.04 2.53 55.83 64.5658.06 2.39 54.60 63.4061.37 2.88 57.18 66.4258.86 2.34 55.25 64.0762.81 2.82 58.17 68.7359.73 2.68 55.03 65.3063.03 2.99 59.69 68.9060.26 2.79 56.73 66.6863.51 2.99 59.69 68.9060.83 2.57 56.73 66.6864.16 3.20 59.20 68.6961.42 3.19 56.65 68.4065.81 3.17 62.41 72.0762.09 3.06 57.65 68.3266.02 3.56 60.49 72.2261.96 2.49 57.42 64.8466.17 3.34 60.73 71.5161.88 2.54 56.32 64.8666.24 3.12 61.08 70.8061.80 2.97 58.67 66.88
um; Max, maximum; F, females; M, males.
illary
L
oys and girls were most notable at age 16 years

lmmdpwwmooy
ri
Rieg
cwp
t
L inim
105Transverse Growth of Maxilla and Mandible
in the maxilla and at age 17-18 years in themandible.10,11 Gender differences in arch widthswere reported at later ages by some authors24
and at younger ages by others.13,22 Boys havearger arch widths than girls, which become
ore prominent in adolescence. Girls showore arch dimensional changes than boys. Gen-
er differences in intermolar widths were moreronounced than interpremolar or intercanineidths with boys having larger intermolaridths.22 The difference in facial widths betweenales and females is more prominent at the end
f adolescence, with males having a facial widthf �3.4 mm at 10 years and �6.2 mm at 18ears.25 The adolescent growth spurt was found
to be 1-3 years later in boys when compared withgirls.23 Transverse growth changes were found toeach near completion by about 15 years of agen females and about 17 years of age in males.
Race and Ethnicity
ace is one of the biggest challenges in develop-ng or using normative data. The transverse skel-tal and dentoalveolar measurements, mean
Table 3. LSMean, SD, Min, and Max Values for ManAged 6-18 Years
Age (Years) Gender Subjects
6 M 23F 17
7 M 22F 23
8 M 21F 24
9 M 22F 23
10 M 19F 21
11 M 22F 23
12 M 21F 24
13 M 23F 22
14 M 18F 23
15 M 18F 17
16 M 20F 14
17 M 20F 14
18 M 11F 9
SMean, least squares mean; SD, standard deviation; Min, m
rowth rates, and maximum extent vary signifi- e
antly between races. Chinese adults presentith significantly larger facial widths when com-ared with the American white population.26
Another parallel phenomenon is the issue ofsecular changes. Cranial size and morphologyhave experienced a notable change over the pastcentury. Although mandibular body width andbigonial breadth show significant decrease, themandibular body length has increased. Thesesecular changes were more pronounced inwhites than blacks.27
Growth Patterns
Growth of the craniofacial region occurs aroundan axis of rotation. There appears to be a defi-nite correlation between maxillary and mandib-ular transverse dimensional changes.28 The ex-tent of transverse growth has been found to havea relation to the morphogenetic facial pattern.Vertical growers with a high mandibular planeangle have been hypothesized to have lessertransverse growth, and thereby lesser gain inintermolar width. Wagner and Chung8 studiedhis relation in a final sample of 81 patients
lar Width in Millimeters for Males and Females
SMean SD Min Max
78.43 4.42 72.48 90.1576.33 2.77 72.37 81.1480.99 4.92 75.43 93.4078.56 3.40 71.57 83.1783.17 5.07 72.94 95.0880.72 3.22 73.36 85.5785.15 4.85 77.82 95.9882.67 3.68 74.42 88.9786.65 5.61 78.83 97.7684.16 3.21 78.07 90.4788.43 5.11 79.97 99.9485.51 3.84 77.02 90.0089.66 5.27 80.73 100.4087.03 3.89 77.72 92.8291.20 5.25 82.60 103.3088.29 4.20 79.10 93.9992.81 5.25 83.74 104.5390.21 4.06 80.75 96.6295.71 6.36 85.95 108.5590.94 3.87 81.55 96.6297.24 6.20 86.31 110.5391.80 5.06 83.63 98.5898.47 6.46 88.45 112.4691.86 4.90 83.30 97.5799.36 5.17 89.70 108.9292.17 3.96 84.89 96.39
um; Max, maximum; F, females; M, males.
dibu
L
xtracted from the Bolton and Burlington stud-

inim
106 Nanda, Snodell, and Bollu
ies, including low, average, and high mandibularplane angles. Intermolar width increased gradu-ally from 6 to 14 years and plateaued by age 14in high-angle patients. Growth continued, al-though at a slower rate in patients with low andaverage mandibular plane angles. This studyconfirms that the vertical growth pattern exhib-ited by high-angle patients has a correlation tolesser gain in intermolar widths. Chen et al29
Table 4. LSMean, SD, Min, and Max Values for Maxand Females Aged 6-18 Years
Age (Years) Gender Subjects
6 M 9F 10
7 M 12F 15
8 M 18F 24
9 M 22F 23
10 M 19F 22
11 M 21F 23
12 M 21F 22
13 M 21F 22
14 M 17F 22
15 M 17F 16
16 M 21F 14
17 M 18F 15
18 M 10F 9
LSMean, least squares mean; SD, standard deviation; Min, m
Table 5. LSMean, SD, Min, and Max Values for Maxand Females Aged 12-18 Years
Age (Years) Gender Subjects
12 M 9F 11
13 M 12F 14
14 M 14F 18
15 M 16F 17
16 M 21F 14
17 M 20F 15
18 M 11F 9
LSMean, least squares mean; SD, standard deviation; Min, minim
analyzed 3-dimensional relationships betweenmaxilla and mandible in relation to the mandib-ular plane angle in a Japanese sample of 56subjects between 8 and 14 years. They found thatthe ratio of maxillary and mandibular width ([J-J/Ag-Ag] Jugale-Jugale and Antegonion–Ante-gonion) decreased and reported a higherchange in the low-angle group. Greater widthincreases were noticed in the mandible when
Intermolar Width (6-6) in Millimeters for Males
SMean SD Min Max
53.18 2.66 50.98 58.4553.67 2.58 49.13 56.7955.40 2.43 51.14 59.2853.87 2.25 49.07 57.0055.25 2.80 51.22 60.7254.55 2.22 48.60 57.4756.95 2.66 52.60 61.3954.55 2.42 48.70 58.2057.46 2.86 53.85 61.6754.88 1.90 50.85 58.4358.00 2.75 54.04 62.1755.41 2.17 49.63 58.6258.22 2.69 57.23 64.9555.63 2.19 49.77 59.9558.25 2.91 53.98 62.8355.72 2.03 49.53 58.2758.38 3.02 53.85 63.3655.55 2.07 48.93 58.2958.65 3.27 52.38 63.4055.86 2.58 48.95 60.2558.98 3.25 53.98 64.1155.98 2.77 48.01 59.5359.41 3.54 53.35 65.0556.17 2.70 53.54 64.4759.46 2.71 54.26 63.3955.67 1.51 54.60 59.29
um; Max, maximum; F, females; M, males.
Intermolar Width (7-7) in Millimeters for Males
SMean SD Min Max
61.27 3.54 57.89 67.0359.32 3.09 54.78 64.3461.94 3.24 57.94 67.1360.26 2.88 54.20 64.1862.51 2.77 57.16 66.2260.53 3.04 54.40 65.9763.20 3.47 57.96 68.9060.86 2.79 54.16 65.8464.05 3.53 58.43 69.7860.73 2.87 52.93 64.5264.32 3.43 59.83 69.1660.87 2.77 53.54 64.4765.01 3.10 60.53 70.1260.72 2.07 58.58 64.00
illary
L
illary
L
um; Max, maximum; F, females; M, males.

aatswle
inim
107Transverse Growth of Maxilla and Mandible
compared with the maxilla, confirming the find-ings of previous studies.11
Habits
Habits, such as mouth breathing, have a pro-found effect on the extent of transversegrowth of the jaws. An absolute correlationexists between respiratory pattern and cranio-facial growth. Although muscular imbalance
Table 6. LSMean, SD, Min, and Max Values for ManFemales Aged 6-18 Years
Age (Years) Gender Subjects
6 M 10F 13
7 M 18F 20
8 M 20F 23
9 M 22F 23
10 M 19F 22
11 M 21F 22
12 M 20F 24
13 M 22F 22
14 M 18F 22
15 M 17F 17
16 M 21F 14
17 M 20F 15
18 M 10F 9
LSMean, least squares mean; SD, standard deviation; Min, m
Table 7. LSMean, SD, Min, and Max Values for Manand Females Aged 12-18 Years
Age (Years) Gender Subjects
12 M 12F 16
13 M 21F 21
14 M 17F 23
15 M 17F 17
16 M 20F 14
17 M 19F 15
18 M 10F 9
LSMean, least squares mean; SD, standard deviation; Min, minim
has been regarded as one of the main contrib-utors,30 the true mechanism responsible forrch constriction is beyond the scope of thisrticle. Paul and Nanda31 in their experimen-al study comparing mouth breathers with na-al breathers found that the maxillary archidth was highly constricted, but the arch
ength was much longer in the mouth breath-rs. Mouth breathers tend to have a poor lip
lar Intermolar Width in Millimeters for Males and
SMean SD Min Max
56.00 2.96 49.66 62.3854.10 2.17 49.45 59.8455.70 2.83 50.92 63.0354.22 2.08 50.33 60.1855.90 2.89 52.11 63.7753.90 2.04 48.00 57.3755.74 2.35 51.55 60.5454.30 1.97 48.38 57.3755.68 2.39 52.61 61.9054.19 1.67 51.14 57.2155.92 2.23 52.30 61.2254.17 2.07 48.30 57.5756.33 2.39 52.38 61.5654.32 2.33 47.56 58.2255.93 2.45 52.02 60.7554.03 2.34 47.17 57.2555.86 2.69 50.67 61.9254.23 2.61 45.56 57.6655.94 2.97 49.84 61.8954.07 2.74 45.93 57.8456.39 2.61 51.17 60.8853.84 2.91 46.45 57.1256.30 3.18 51.19 62.2054.05 3.21 45.91 57.4356.12 2.17 51.57 58.3953.72 1.55 52.28 56.98
um; Max, maximum; F, females; M, males.
lar Intermolar Width (7-7) in Millimeters for Males
SMean SD Min Max
64.55 3.24 58.13 68.8462.43 2.88 56.33 65.6563.72 2.73 58.25 67.6561.17 2.48 55.47 64.7463.03 2.43 57.00 66.6961.26 2.71 55.06 65.3463.21 3.39 56.52 71.0760.65 2.69 54.09 63.8963.46 3.06 57.74 70.8960.39 2.77 54.17 64.1463.72 3.77 58.29 72.5960.73 3.29 52.50 64.6363.36 2.71 57.20 66.4960.37 1.36 52.28 63.98
dibu
L
dibu
L
um; Max, maximum; F, females; M, males.

108 Nanda, Snodell, and Bollu
tonicity leading to increased growth in thesagittal plane. Hence, these patients oftenpresent with an increased overjet. The limitedarch width was more noticeable in the maxilla,whereas in the mandible, perhaps the tongue
Figure 2. Regression line and 95% confidence intervalfor cranial width in females. Values at ages 6 or 7 and 18
Table 8. Percentage Completion of Width at 6Years, with 100% Being Considered at 18 Years
TransverseMeasurement
Extent of GrowthCompleted at 6
Years (%)100% Completeat Age (Years)
Female Male Female Male
Facial width 83 86 18 17Nasal width 75 80 18 17Maxilla width 85 88 16 15Mandibular width 78 88 18 16Maxillary intermolar
width (6-6)89 89 17 17
Maxillary intermolarwidth (7-7)
94 94 14 18
Mandibularintermolar width(6-6)
100 101 — —
Mandibularintermolar width(7-7)
102 103 — —
or 19 years were used to calculate the regression line.
prevents the collapse of the arch form, therebypreserving the arch width.
Muscles
The role of muscles on facial dimensions andproportions has been studied extensively. Thereview article by Kiliardis32 explores this topicand identifies elevator muscles of the mandibleto exert an influence on the transverse and ver-tical facial dimensions. The biomechanics in-volved in this phenomenon are complex; heavymuscle forces because of masticatory muscle hy-per function, perhaps increase the suturalgrowth and bone apposition, ultimately result-ing in an increased transverse growth of themaxilla and broader bone bases for the dentalarches. A definite correlation seems to exist be-tween cross-sectional areas of temporalis andmasseter muscles with facial width.33 In thelower jaw, the tongue being a very strong muscleinfluences the arch width. Lateral growth of thelower jaw was significantly reduced in glossecto-mized animals, leading to highly constricted in-
Figure 3. Regression line and 95% confidence intervalfor facial width in males. Values at ages 6 or 7 and 18 or19 years were used to calculate the regression line.
tercanine and intermolar widths.34

d
hsl
tca
Btdtaw
109Transverse Growth of Maxilla and Mandible
Skeletal Differential
The mandibular posterior extent acts as a limit-ing factor to the width of the maxillary intermo-lar width. The review article by Vanarsdall35 pro-vides great insights into this concept of skeletaldifferential and highlights the importance ofearly diagnosis of transverse discrepancy. Thedifference in intermolar widths of the maxillaand mandible is referred to as posterior trans-verse interarch discrepancy. The clinical impli-cation is that mandibular posterior teeth affectthe maximum extent of maxillary expansionthat a clinician can expect to achieve.
Malocclusions
Transverse development of jaws has been foundto be influenced by malocclusions, such as open-bite36 or Class II division 1.12 Maxillary skeletalbase widths are smallest in the Class II division 1category, and the difference in maxillary andmandibular intermolar widths remained thesame from 7 to 15 years of age.37 The transverse
Figure 4. Regression line and 95% confidence inter-val for facial width in females. Values at ages 6 or 7and 18 or 19 years were used to calculate the regres-sion line.
eficiency seen in Class II malocclusion patients,
owever, may be due to a deficiency in the initialize and not because of growth differences inater stages. Bishara et al38 confirmed that no
differences were observed in the growth changesbetween normal and Class II subjects. Class IItendency is observed early on in the primarydentition and tends to persist into the mixeddentition.39,40 If this problem is not corrected inhe initial stages, the discrepancy will not self-orrect and the same discrepancy continues intodulthood.
Orthodontic Intervention
eside changes observed in growth, increases inransverse arch dimensions are often observeduring orthodontic treatment.41 A definite pat-
ern seems to exist between molar uprightingnd increase in transverse maxillary basal boneidth.9 Prolonged use of orthodontic appliances
could actually hinder growth.22
Discussion
Early growth studies were based on direct an-thropometric measurements of human faces or
Figure 5. Regression line and 95% confidence intervalfor nasal width in males. Values at ages 6 or 7 and 18 or
19 years were used to calculate the regression line.
tpppedico
csbvcpdwo
t
cacWpmatc
idicwaaa
110 Nanda, Snodell, and Bollu
dried skulls (craniometry).42 Variations in soft-issue thickness limited the accuracy of this ap-roach. Another major limitation of the anthro-ometry and craniometry is the inability toerform longitudinal studies.2 As radiographyvolved, numerous growth studies have beenone using lateral cephalograms as the primary
maging resource. Implants’ studies alongsideephalometry have since been used by severalther researchers to monitor growth changes.
Although lateral cephalometric radiographsan provide a good view to assess vertical andagittal growth, the frontal view (A-P) offers aetter perspective in measuring transverse andertical growth changes of the face. One majoroncern with PA views, however, has been theotential for magnification errors due to varyingistances between the objects and film. Theeaknesses inherent in PA views were pointedut by Woods43 several decades ago. For in-
stance, the intercanine width was argued to beless magnified than the bigonial width becausethe gonial angles are farther away from the film
Figure 6. Regression line and 95% confidence inter-val for nasal width in females. Values at ages 6 or 7 and18 or 19 years were used to calculate the regressionline.
when compared with the upper canines. Lack of
access to better imaging modalities has limitedresearchers to continue using PA views forgrowth studies. However, several geometrical ap-proaches have since been developed to correctthe magnification errors,44 thereby aiding in bet-er interpretation of the data from PA views.
Beside superimpositions and image magnifi-ations inherent in 2-dimensional images, anyttempts to extrapolate a multidimensional con-ept with 2-dimensional views are debatable.ith the increasing access to cone-beam com-
uted tomography technology, more studiesay be expected to use the benefits that this
dvanced imaging can offer. More importantly,he use of multiple views to evaluate growthhanges is warranted.
Chronologic age serves as a simple milestonen evaluating growth patterns and making pre-ictions of future growth. However, several stud-
es have investigated the accuracy of usinghronologic age as an indicator in comparisonith biological age.45,46 In an attempt to providegeneral guideline to the clinician when evalu-
ting growth patterns, we have used chronologicge as a marker to identify key growth mile-
Figure 7. Regression line and 95% confidence intervalfor maxillary width in males. Values at ages 6 or 7 and 18 or
19 years were used to calculate the regression line.
gt
diltorcb
111Transverse Growth of Maxilla and Mandible
stones, using observations from previous studies.It is imperative that the readers take into ac-count individual variations when making infer-ences on growth patterns and predictions.
A caveat to readers is the potential issue ofsecular changes. The longitudinal records usedin the current research article were taken fromarchives of the Child Research Council, Denver,CO. The records were collected from the early1930s to the mid-1960s of the 20th century. It ispossible that the growth behavior and size of thecurrent population may be earlier maturing andlarger.
A major limitation observed in the majority ofgrowth studies attempting to predict growth ex-tent is the use of a certain age as near comple-tion. Although transverse growth may be com-plete by late adolescence, growth is found tocontinue in other dimensions. Relative growthin other dimensions could erroneously hampertrue calculations when one attempts to identifythe complete extent of growth in 1 dimension.
Several studies showed that the skeletal and
Figure 8. Regression line and 95% confidence inter-val for mandibular width in males. Values at ages 6 or7 and 18 or 19 years were used to calculate the regres-sion line.
dentoalveolar growth increments are different
for the maxilla and the mandible. The mandib-ular width showed greater increase than themaxillary width.11,47,48 In contrast, the intermo-lar width showed greater increases in the maxillathan the mandible.10,14,24 This distinction is ofreat clinical significance in determining theiming and extent of expansion.
Overdependence on the linear dentoalveolarimensional changes carries the risk of overlook-
ng underlying skeletal discrepancies. To estab-ish sound treatment objectives, it is importanto recognize the correlation between dentoalve-lar and supporting skeletal structures. This cor-elation in transverse growth between craniofa-ial skeletal and dentoalveolar structures haseen highlighted several decades ago.49
A review of some recent literature on trans-verse growth follows. Using Bjork-type implants,Korn and Baumrind50 reported longitudinaldata on transverse dimensions of the maxillaand mandible on a sample of 31 subjects be-tween ages 8.5 and 15.5 years. Lateral and fron-tal radiographs were taken annually. Transversewidening was observed in the posterior-most
Figure 9. Regression line and 95% confidence inter-val for mandibular width in females. Values at ages 6or 7 and 18 or 19 years were used to calculate the
regression line.
idftplbmwi
112 Nanda, Snodell, and Bollu
area of the palate at a mean annual rate of 0.43mm.
With the goal of establishing normative data,Athanasiou et al14 performed a cross-sectionalnvestigation on a sample of 588 Australian chil-ren between 6 and 15 years of age. Findings
rom this study showed a gradual increase in theransverse skeletal dimensions during the studyeriod. The maxillary and mandibular intermo-
ar widths, however, remained relatively constantetween 9 and 12 years. The ratio between theaxillary intermolar width and interorbitalidth decreased between 8 and 13 years but
ncreased during 14 and 15 years.Cortella et al11 in an attempt to generate new
norms for PA cephalometric analyses used theBolton-Brush study sample to examine the trans-verse relationship between the maxilla and man-dible during growth. This study adjusted thenorms from Bolton-Brush study in accordancewith radiographic enlargement. Statistically sig-nificant increases in annual rates of growth wereobserved at 7 and 10 years. This study focused on
Figure 10. Regression line and 95% confidence in-terval for facial width in males. Values at ages 11 or 12and 18 or 19 years were used to calculate the regres-sion line.
the differences in growth patterns between boys
and girls. The authors found that the growthpatterns are similar in both genders until 11years, and some differences are observed beyond12 years.
The implant study by Gandini and Buschang28
was performed on a sample of 25 subjects between12 and 18 years of age. Using Bjork’s technique,51
implants were placed on the maxillary and man-dibular corpora. In the maxilla, implants wereplaced on either side of the anterior nasal spinefor anterior measurement and on the zygomaticprocess bilaterally for the posterior measurements.In the mandible, implants were placed inferior tothe first molar bilaterally for posterior measure-ment and in the midsymphyseal region anteriorly.Lateral and frontal radiographs were taken peri-odically during the study to capture the movementof the implants along with skeletal growth-relateddimensional changes. The anterior maxillary im-plants showed a decrease of 0.2 mm, whereas pos-teriorly, the distance increased by 0.6 mm in themandible and 0.8 mm in the maxilla. The maxil-lary growth was found to be 0.4 mm per year,whereas the mandibular growth rate was at 0.1 mmper year.
Figure 11. Regression line and 95% confidence intervalfor facial width in females. Values at ages 11 or 12 and 18
or 19 years were used to calculate the regression line.
oigabgwfacw
cdimtTmnp
wocyb
vaTsstwdm
mplcmlr
113Transverse Growth of Maxilla and Mandible
The longitudinal PA cephalometric study byLux et al13 used radiographs and dental models
f 18 normal occlusion subjects with the aim ofdentifying craniofacial and dental transverserowth patterns. These changes were observedt 2-year intervals from ages 7 to 15 years. Inoth males and females, statistically significantrowth changes were observed in the intermolaridths between 7 and 11 years. The authors
ound that except mandibular intermolar width,ll skeletal and dental transverse dimensions in-reased from 7 to 15 years. Gender differencesere found to be most pronounced at 15 years.
Stephens et al52 evaluated arch dimensionalhanges using radiographs of 21 Caucasian chil-ren between 2 and 20 years of age. An interest-
ng finding from this study was that the maxi-um arch width was achieved not soon after
ooth eruption but 2-3 years later, in general.he arch width gain was delayed further in theolar region. The maximum arch width wasoted about 6-8 years, following eruption in the
Figure 12. Regression line and 95% confidence in-terval for nasal width in males. Values at ages 11 or 12and 18 or 19 years were used to calculate the regres-sion line.
ermanent first molar region, whereas the same
as achieved at about 4-5 years later in the sec-nd molar region. Accelerated increases in theanine arch width were noted between 5 and 8ears. Maxillary arch width increase was found toe larger than that of the mandibular arch.
Yavuz et al47 investigated longitudinal trans-erse and vertical growth changes between 10nd 14 years in a Turkish sample of 45 subjects.he largest incremental width changes were ob-
erved in mandibular intermolar width for thetudy period. Gender differences were more no-able in the transverse skeletal measurementshen compared with the vertical changes. Man-ibular widths measured at 10 years were 93.2m in males and 92.3 mm in females.Hesby et al9 investigated the growth-related
olar movements and torque changes. They re-orted that maxillary and mandibular intermo-
ar crown torque changes are accompanied byoncurrent increases in the corresponding inter-olar widths. Maxillary skeletal and dentoalveo-
ar transverse measurements were found toeach adult extents by 16.5 years. Greatest width
Figure 13. Regression line and 95% confidence in-terval for nasal width in females. Values at ages 11 or12 and 18 or 19 years were used to calculate the
regression line.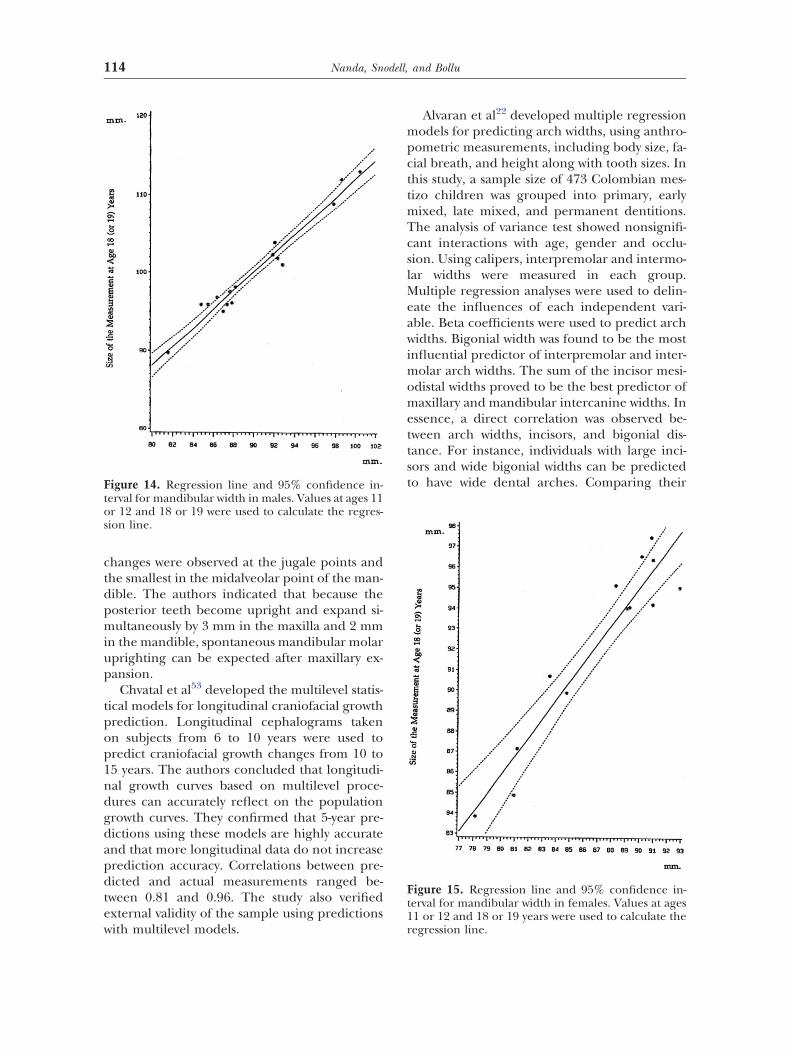
tpop1ndgdapdtew
mpcttmTcslMeawimomettst
114 Nanda, Snodell, and Bollu
changes were observed at the jugale points andthe smallest in the midalveolar point of the man-dible. The authors indicated that because theposterior teeth become upright and expand si-multaneously by 3 mm in the maxilla and 2 mmin the mandible, spontaneous mandibular molaruprighting can be expected after maxillary ex-pansion.
Chvatal et al53 developed the multilevel statis-ical models for longitudinal craniofacial growthrediction. Longitudinal cephalograms takenn subjects from 6 to 10 years were used toredict craniofacial growth changes from 10 to5 years. The authors concluded that longitudi-al growth curves based on multilevel proce-ures can accurately reflect on the populationrowth curves. They confirmed that 5-year pre-ictions using these models are highly accuratend that more longitudinal data do not increaserediction accuracy. Correlations between pre-icted and actual measurements ranged be-
ween 0.81 and 0.96. The study also verifiedxternal validity of the sample using predictions
Figure 14. Regression line and 95% confidence in-terval for mandibular width in males. Values at ages 11or 12 and 18 or 19 were used to calculate the regres-sion line.
ith multilevel models.
Alvaran et al22 developed multiple regressionodels for predicting arch widths, using anthro-
ometric measurements, including body size, fa-ial breath, and height along with tooth sizes. Inhis study, a sample size of 473 Colombian mes-izo children was grouped into primary, early
ixed, late mixed, and permanent dentitions.he analysis of variance test showed nonsignifi-ant interactions with age, gender and occlu-ion. Using calipers, interpremolar and intermo-ar widths were measured in each group.
ultiple regression analyses were used to delin-ate the influences of each independent vari-ble. Beta coefficients were used to predict archidths. Bigonial width was found to be the most
nfluential predictor of interpremolar and inter-olar arch widths. The sum of the incisor mesi-
distal widths proved to be the best predictor ofaxillary and mandibular intercanine widths. In
ssence, a direct correlation was observed be-ween arch widths, incisors, and bigonial dis-ance. For instance, individuals with large inci-ors and wide bigonial widths can be predictedo have wide dental arches. Comparing their
Figure 15. Regression line and 95% confidence in-terval for mandibular width in females. Values at ages11 or 12 and 18 or 19 years were used to calculate the
regression line.
115Transverse Growth of Maxilla and Mandible
results with Pont’s index, Schwarz analysis, andthe McNamara rule of thumb, the authors of thisstudy concluded that multiple regressions serveas better tools in predicting arch widths.
Summary
Longitudinal records of 50 (25 male, 25 female)AP cephalometric radiographs were selectedfrom the archives of Child Research Council,Denver, CO. From serial cephalometric mea-surements, growth was evaluated from the groupmeans. Annual increments for each variable andperiods of growth acceleration were identified.Growth spurts were defined as the rate of meanannual growth increment exceeding that in thepreceding annual interval by at least 0.75 mm.The following observations may be considered:
1. The transverse growth was completed for themajority of measurements for both males andfemales by age 18 years. Each of the measure-ments was complete by over 80% by age 6
Figure 16. Regression line and 95% confidence in-terval for maxillary width in males. Values at ages 11or 12 and 18 or 19 years were used to calculate theregression line.
years relative to the size at 18 years. Nasal
width was an exception that was only 75%complete by 6 years of age.
2. Statistically significant differences were foundbetween male and female measurements: atage 6 years, between mean width of cranium,face, and maxilla; at age 12 years, the differ-ences were between cranial width, maxillarywidth, and maxillary-mandibular intermo-lar(6-6) widths; at age 18 years, all variableswere different, except the nasal width andmandibular intermolar (6-6) width.
3. In females, the cranial and facial width spurtswere at 8 years and nasal width was at 11years. In males, the cranial width growthspurt was at 12 and 14 years, facial width wasat 7 and 15 years, and nasal width spurt was at10 and 17 years. No growth spurts in themaxillary and mandibular widths for femaleswere recorded.
4. Transverse growth of the face is near com-plete by age 18 years, although, nasal widthstill shows growth increments. As growth inthe width of the maxilla and the nose largelyoccurs between 7 and 11 years of age, patients
Figure 17. Regression line and 95% confidence in-terval for maxillary width in females. Values at ages 11or 12 and 18 or 19 years were used to calculate the
regression line.
5
1gso
ma
TY
X
116 Nanda, Snodell, and Bollu
requiring orthopedic expansion of the max-illa may be treated with advantage during thisperiod.
. Linear regression analysis at 6 years revealedstrong predictability (R2 � 0.60) in both gen-ders for cranial width, facial width, and man-dibular width. The predictability was onlymoderate (R2 � 0.40 � 0.60) for nasal widthand maxillary width. However, at age 12years, the predictability for all craniofacialand dentoalveolar transverse measurementswas strong.
Our data show a strong predictive potential at2 years of age when measuring transverserowth in the craniofacial and dentoalveolartructures. Considering the clinical implicationsf growth predictions in effective orthodontic treat-
Figure 18. Percentage change for each variable inmales and females from age 6 to 12 years expressed asa proportion of the value at age 6 years. (Color ver-sion of figure is available online.)
Figure 19. Percentage change for each variable inmales and females from age 6 to 18 years expressed asa proportion of the value at age 6 years. (Color ver-
sion of figure is available online.)ent planning, further research is warranted in thisrea.
References1. Goldstein MS: Changes in dimensions and form of the face
and head with age. Am J Phys Anthropol 22:37-89, 19362. Profitt WR, Fields HW, Sarver DM: Contemporary Or-
thodontics, 4th ed. St. Louis, MO: Mosby, 20073. Behrents RG: A Treatise on the Continuum of Growth in
the Aging Craniofacial Skeleton. Ann Arbor, MI, Universityof Michigan Center for Human Growth and Development,1984
4. Meredith HV: Changes in form of the head and faceduring childhood. Growth 24:215-264, 1960
5. Edwards CB, Marshall SD, Qian F, et al: Longitudinal studyof facial skeletal growth completion in 3 dimensions. Am JOrthod Dentofacial Orthop 132:762-768, 2007
6. Ricketts RM, Roth RH, Chaconas SJ, et al: OrthodonticDiagnosis and Treatment Planning, Denver, CO: RockyMountain Data Systems, 1982
7. Ricketts RM: Perspectives in the clinical application ofcephalometrics: The first fifty years. Angle Orthod 51:115-150, 1981
8. Wagner DM, Chung CH: Transverse growth of maxillaand mandible in untreated girls with low, average andMP-SN angles: A longitudinal study. Am J Orthod Dento-facial Orthop 128:716-723, 2005
9. Hesby RM, Marshall SD, Dawson DV, et al: Transverseskeletal and dentoalveolar changes during growth. Am JOrthod Dentofacial Orthop 130:721-731, 2006
10. Snodell SF, Nanda RS, Currier GF: A longitudinal cepha-lometric study of transverse and vertical craniofacialgrowth. Am J Orthod Dentofacial Orthop 104:471-483,1993
11. Cortella S, Shofer FS, Ghafari J: Transverse developmentof the jaws: Norms for the posteroanterior cephalomet-ric analysis. Am J Orthod Dentofacial Orthop 112:519-522, 1997
12. Tollaro I, Baccetti T, Franchi L, et al: Role of posteriorinterarch discrepancy in Class II, Division1 malocclusionduring the mixed dentition phase. Am J Orthod Dento-
able 9. Predictability for Each Variable at Ages 6ears and 12 Years
TransverseMeasurement
Male Female
6 Years 12 Years 6 Years 12 Years
Cranial width XXX XXX XXX XXXFacial width XXX XXX XXX XXXNasal width XX XXX X XXMaxillary width XX XXX XXX XXXMandibular width XXX XXX XXX XXXMaxillary intermolar
width (6-6)— XXX — XXX
Mandibularintermolar width(6-6)
— XXX — X
XX, strong; XX, moderate; X, weak.
facial Orthop 110:417-422, 1996

117Transverse Growth of Maxilla and Mandible
13. Lux CJ, Conradt C, Burden D, et al: Transverse develop-ment of the craniofacial skeleton and dentition between 7and 15 years of age—A longitudinal postero-anterior ceph-alometric study. Eur J Orthod 26:31-42, 2004
14. Athanasiou AE, Drosch H, Bosch C: Data and patterns oftransverse dentofacial structure of 6- to 15-year-old chil-dren: A posteroanterior cephalometric study. Am J Or-thod Dentofacial Orthop 101:465-471,1992
15. Maurice TJ, Kula K: Dental arch asymmetry in the mixeddentition. Angle Orthod 68:37-44, 1998
16. Snodell SF: A longitudinal study of transverse and verticalcraniofacial growth [master’s thesis]. Oklahoma City, OK,University of Oklahoma Health Sciences Center; 1991
17. Pont A: Der Zahn-index in der orthodontie. Z ZahnarztlOrthop 3:306-321,1909
18. Howe RP, McNamara JA, O’Connor KA: An examinationof dental crowding and its relationship to tooth size andarch dimension. Am J Orthod 83:363-373, 1983
19. Schwarz AM, Gratzinger M: Removable Orthodontic Ap-pliances. Philadelphia, PA: W. B. Saunders, 1966
20. Bonwill WG: Geometric and mechanical laws of articu-lation. Trans Odont Soc 119-133, 1885
21. Nimkarn Y, Miles PG, O’Reilly MT, et al: The validity ofmaxillary expansion indices. Angle Orthod 65:321-326,1995
22. Alvaran N, Roldan SI, Buschang PH: Maxillary and man-dibular arch widths of Colombians. Am J Orthod Dento-facial Orthop 135:649-656, 2009
23. Savara BS, Singh IJ: Norms of size and annual incre-ments of seven anatomical measures of maxilla in boysfrom 3 to 16 years of age. Angle Orthod 38:104-120, 1968
24. Sillman JH: Dimensional changes of the dental arches:Longitudinal study from birth to 25 years. Am J OrthodDentofacial Orthop 50:824-842, 1964
25. Meredith HV: Growth in bizygomatic face breadth dur-ing childhood. Growth 18:111-134, 1954
26. Wei SH: Craniofacial width dimensions. Angle Orthod40:141-147, 1970
27. Martin DC, Danforth ME: An analysis of secular changein the human mandible over the last century. Am J HumBiol 21:704-706, 2009
28. Gandini LG, Buschang PH: Maxillary and mandibularwidth changes studied using metallic implants. Am JOrthod Dentofacial Orthop 117:75-80, 2000
29. Chen F, Wu L, Terada K, et al: Longitudinal intermax-illary relationships in Class III malocclusions with lowand high mandibular plane angles. Angle Orthod 77:397-403, 2007
30. Hawkins AC: Mouth breathing as the cause of malocclusionand other facial abnormalities. Tex Dent J 83:10-15, 1965
31. Paul JL, Nanda RS: Effect of mouth breathing on dentalocclusion. Angle Orthod 43:201-206, 1973
32. Kiliaridis S: Masticatory muscle influence on craniofacialgrowth. Acta Odontol Scand 53:196-202, 1995
33. Weijs WA, Hillen B: Correlations between the cross-sectional area of the jaw muscles and craniofacial sizeand shape. Am J Phys Anthropol 70:423-431, 2005
34. Becker R, Hübner A, Pommerenke F, et al: The tongueas a factor in craniofacial growth. The influence of the
width of the lower jaw. Anat Anz 167:81-86, 198835. Vanarsdall RL: Transverse dimension and long-term sta-bility. Semin Orthod 5:171-180, 1999
36. Hsu BS: The nature of arch width difference and palataldepth of the anterior open bite. Am J Orthod Dentofa-cial Orthop 113:344-350, 1998
37. Lux CJ, Conradt C, Burden D, et al: Dental arch widthsand mandibular-maxillary base widths in Class II maloc-clusions between early mixed and permanent dentitions.Angle Orthod 73:674-685, 2003
38. Bishara SE, Bayati P, Jakobsen JR: Longitudinal compari-sons of dental arch changes in normal and untreated ClassII, Division 1 subjects and their clinical implications. Am JOrthod Dentofacial Orthop 110:483-489, 1996
39. Baccetti T, Franchi L, McNamara JA, et al: Early dento-facial features of Class II malocclusion: A longitudinalstudy from the deciduous through the mixed dentition.Am J Orthod Dentofacial Orthop 111:502-509, 1997
40. Nanda RS: The contributions of craniofacial growth toclinical orthodontics. Am J Orthod Dentofacial Orthop117:553-555, 2000
41. Fleming PS, Dibiase AT, Lee RT: Arch form and dimen-sional changes in orthodontics. Prog Orthod 9:58-64, 2008
42. Hellman M: An introduction to growth of the humanface from infancy to adulthood. Int J Orthodontia OralSurg Radiogr 18:777-798, 1932
43. Woods GA: Changes in width dimensions between cer-tain teeth and facial points during human growth. Am JOrthod Dentofacial Orthop 36:676-700, 1950
44. Hsiao TH, Chang HP, Liu KM: A method of magnifica-tion correction for postero-anterior radiographic ceph-alometry. Angle Orthod 67:137-142, 1997
45. Moorrees CFA, Chadha JM: Available space for the inci-sors during dental development—a growth study basedon physiologic age. Angle Orthod 35:12-22, 1965
46. Moorrees CF, Reed RB: Changes in dental arch dimen-sions expressed on the basis of tooth eruption as ameasure of biologic age. J Dent Res 44:129-141, 1965
47. Yavuz I, Ikbal A, Baydas B, et al: Longitudinal posteroan-terior changes in transverse and vertical craniofacialstructures between 10 and 14 years of age. Angle Orthod74:624-629, 2004
48. Huertas D, Ghafari J: New posteroanterior cephalomet-ric norms: A comparison with craniofacial measures ofchildren treated with palatal expansion. Angle Orthod71:285-292, 2001
49. Meredith HV, Higley LB: Relationship between dentalarch widths and widths of face and head. Am J OrthodDentofacial Orthop 37:193-204, 1951
50. Korn EL, Baumrind S: Transverse development of thehuman jaws between the ages of 8.5 and 15.5 years,studied longitudinally with use of implants. J Dent Res69:1298-1306, 1990
51. Bjork A: Facial growth in man, studied with the aid ofmetallic implants. Acta Odontol Scand 13:9-34, 1955
52. Stephens S, Currier F, Nanda RS: Growth of the dentalarches: A longitudinal study from 2-22years. J PaediatrDent Care 10:19-22, 2004
53. Chvatal BA, Behrents RG, Ceen RF, et al: Developmentand testing of multilevel models for longitudinal cranio-facial growth. Am J Orthod Dentofacial Orthop 128:45-
56, 2005