atrophic posterior maxilla and mandible: alveolar - … posterior maxilla and... · prosthetics and...
TRANSCRIPT

34 Alpha Omegan, Volume 98, Number 3, October 2005
Autogenous bone grafts have been used for manyyears for alveolar ridge augmentation and are still
considered to be the gold standard for jaw reconstruc-tion.1,2 The use of these grafts with osseointegratedimplants was originally discussed by Brånemark et al.,
who used the iliac crest as the donor site.3 For repairof most localized alveolar defects, however, bonegrafts from the mandible offer advantages over iliaccrest grafts. These include the proximity of donorand recipient sites, convenient surgical access,decreased donor site morbidity and decreased cost.
There is usually loss of alveolar bone height inthe posterior maxilla and mandible secondary totrauma, pathology and periodontal disease and aftertooth removal. Tooth loss results in buccal plate com-promise and a reduction in alveolar width. This boneresorption process continues in a medial directionuntil a knife-edged ridge forms and precludesimplant placement. The cortical plate may be mini-mal or absent, further complicating implant place-ment. In addition, alveolar height is decreased in theposterior maxilla as a result of pneumatization (par-tial or complete) of the maxillary sinus after toothloss. Finally, occlusal forces are greater in the poste-rior than in the anterior area of the mouth, necessi-tating appropriate surgical and prosthetic treatmentplanning for long-term success.
The recipient site must be evaluated for bothhard and soft tissue deficiencies, esthetic concernsand the overall health of the adjacent teeth. Somecases require soft tissue procedures to be done priorto or simultaneous with block grafting, as well as inconjunction with implant placement or stage IIsurgery. These include use of connective tissue grafts,palatal epithelial grafts and human dermis. Conven-tional radiographs are obtained and include periapi-cal, occlusal, panoramic and lateral cephalometricviews. Computed tomography and interactive soft-ware are also used for many cases. Mounted modelsare used to evaluate interocclusal relationships and
Michael A. Pikos, D.D.S.Dr. Michael A. Pikos is originally fromCampbell, Ohio. He attended Ohio StateUniversity where he graduated Summa CumLaude and Phi Beta Kappa. He also gradu-ated with honors from The Ohio State Uni-versity College of Dentistry. Dr. Pikos com-pleted residency training in Oral &Maxillofacial Surgery at the University of
Pittsburgh, Montefiore Hospital.He is a Diplomate of the American Board of Oral and Max-
illofacial Surgery, Diplomate of the American Board of OralImplantology/Implant Dentistry, Diplomate of The InternationalCongress of Oral Implantologists and Diplomate of the AmericanSociety of Osseointegration.
He is an adjunct assistant professor, Department of Oral andMaxillofacial Surgery, at the following institutions: The OhioState University, College of Dentistry, The University of Miami,School of Medicine, and Nova Southeastern University, Collegeof Dental Medicine. He is also a Courtesy Clinical Associate Pro-fessor, Department of Periodontology, at the University ofFlorida, College of Dentistry.
Dr. Pikos has extensive experience in implant surgery havingplaced more than 9,000 implants. He performs numerous hardand soft tissue graft procedures and emphasizes principles ofprosthetics and biomechanics that dictate the ultimate successof implants.
He is a well published author who has lectured extensively onimplants in North and South America, Europe, Asia, and theMiddle East. Dr. Pikos is the founder of the MAP Implant Insti-tute. Since 1990, Dr. Pikos has been teaching an Advanced BoneGrafting Course and a Soft Tissue Grafting Course to cliniciansthat now number more than 1600, and have come from all 50states as well as 26 countries. Dr. Pikos maintains a private prac-tice in Palm Harbor, FL which is limited exclusively to implantreconstructive surgery.
SCIENTIF IC ART ICLE
Atrophic Posterior Maxilla and Mandible:Alveolar Ridge Reconstruction with
Mandibular Block AutograftsMichael A. Pikos, D.D.S.

Alpha Omegan, Volume 98, Number 3, October 2005 35
ridge shape and provide valuable information forimplant placement. A diagnostic wax-up of the simu-lated reconstructed ridge and dentition is a usefulguide in obtaining presurgical information concern-ing graft size and shape, along with evaluating theocclusion. This also provides a base for template fab-rication. The primary goal of posterior arch implantreconstruction is to create a biomechanically soundsupport for the implant prosthetic complex.
A number of stress elements that affect the ulti-mate success of posterior maxillary and mandibularimplants need to be addressed. Biting forces areincreased. These forces are primarily directed perpen-dicular to the occlusal plane and are usually of shortduration. Recent studies have indicated that normalmaximal vertical biting forces on teeth or implants inthe arches range from 50 to 550 psi.4–6 Maximum bit-ing forces are found in the molar region. In addition,the opposing arch is a consideration. Typically, thereis either natural dentition or implant- or tooth-supported fixed prosthetics, allowing maximumocclusal transfer unlike that of an opposing denture.Treatment planning in the posterior maxilla mustinclude solutions to reduce stress. A primary factor isa plan that includes increasing the number ofimplants. No pontics are used, so one implant perbuccal root is the treatment planned for each case. Inaddition, no cantilevers are allowed. Splinting of allcrowns is also indicated for biomechanical force dis-tribution. Occlusal considerations include eliminatinglateral interferences during any excursive movements.The final factors involved in decreasing undesirablestress to the implants are interrelated. They includeincreasing the bone density and maximizing thediameter of the implants. These two goals are accom-plished with mandibular block grafts. The quality ofbone from the ramus buccal shelf is typically type I,and the symphysis normally exhibits type II and occa-sionally type I quality bone. These mandibular blockgrafts create areas for the use of larger-diameterimplants, which increase the surface area over whichthe stresses of occlusal forces are distributed.
This article focuses on posterior maxillary andmandibular osseous augmentation in a stagedapproach for implant placement. Both horizontal
and vertical deficiencies are addressed with the use ofsymphysis and ramus buccal shelf donor block bonevia case presentations.
Case 1
A healthy 65-year-old white female was referred forimplant evaluation. Clinical and radiographic exami-nation revealed missing maxillary left canine, bicus-pid and molar teeth (Figure 1). The edentulous spanexhibited a deficiency in width and a partially pneu-matized maxillary left sinus. The treatment planincluded sinus grafting and lateral ridge augmenta-tion prior to implant placement in preparation for afour-unit implant fixed restoration.
Staging of both bone grafting procedures, as wellas stage I surgery, is vital to the predictability and suc-cess of this case type. If primarily autogenous bone isused for the sinus graft, then simultaneous sinus andalveolar block grafting can be done because the healingtime for each graft type is the same. However, becausethe sinus graft material is composed of an allograft anda xenograft (necessitating approximately 8 to 9 monthsof incorporation), the autogenous block graft must beperformed some 5 months later, allowing adequatehealing time for both grafts to be incorporated enoughprior to stage I surgery. If the block is done simultane-ously with the sinus graft, then approximately 10+months of overall healing time may well result in par-tial resorption of the block graft.7–9
The first surgical procedure performed was a leftsinus augmentation (Figure 2). The graft materialconsisted of 50% by volume mineralized human
ATROPHIC POSTER IOR MAXILLA AND MANDIBLE
Figure 1 Atrophic left posterior maxilla.

36 Alpha Omegan, Volume 98, Number 3, October 2005
bone (Puros cancellous, Tutogen Medical GmbH,Germany) and 50% by volume bovine hydroxyapatite(Pepgen 15, Dentsply Friadent Ceramed, Manheim,Germany) (Figure 3). Approximately 5 monthspost–sinus graft, a left ramus buccal shelf block graftwas harvested as per the author’s protocol for lateralaugmentation of the left posterior maxillary edentu-lous site (Figure 4).10–13 Graft fixation was done using1.6 mm diameter × 12 mm length titanium alloyscrews (Figure 5). Platelet-rich plasma was also usedat the interface between the recipient site and blockbone. Finally, a collagen membrane (Colla Tape,Zimmer Dental, Carlsbad, CA) was used as a carrierto completely immerse the entire wound site withplatelet-rich plasma (Figure 6). This graft would thenrequire 4 months healing time prior to reentry (Fig-ure 7). At this point, the block graft and the sinusgraft were incorporated enough for stage I surgery.Four 3.75 mm diameter × 15 mm length hydroxyap-
atite-coated Spline Twist (Zimmer Dental) implantswere placed in a nonsubmerged mode (Figure 8).Impressions were taken to allow for custom com-puter abutments to be fabricated. After 5 months ofprovisionalization, the final four-unit implant-bornefixed restoration was cemented (Figures 9 and 10).
ATROPHIC POSTER IOR MAXILLA AND MANDIBLE
Figure 3 Reentry, left maxillary sinus graft at 6 months. Figure 6 Platelet-rich plasma and Colla Tape in place.
Figure 2 Completed sinus graft. Figure 4 Harvested left ramus buccal shelf block graft.
Figure 5 Mandibular block graft fixation for lateral augmentation.

Alpha Omegan, Volume 98, Number 3, October 2005 37
Figure 11 Edentulous right posterior maxilla.
Case 2 A healthy 62-year-old white female was referred for“my missing back teeth.” Clinical and radiographicexamination revealed missing maxillary right molarsand first bicuspid teeth (Figure 11). The edentuloussite exhibited a vertical alveolar deficiency, alongwith a relatively nonpneumatized maxillary sinus(Figures 12 and 13). Because the patient’s primeconcern was an esthetic one, the treatment planincluded approximately 4 mm of vertical augmenta-tion followed by placement of three implants for athree-unit fixed splinted restoration. Implant place-ment without vertical ridge augmentation wouldresult in long clinical crowns that would be revealedwith the patient’s high smile line.
A right ramus buccal shelf block graft was har-vested as per the author’s surgical protocol (Figures
14 to 17).10–13 The donor site was approached with amidcrestal incision in the right posterior edentulousridge, continuing in an anterior fashion within thesulcus with an anterior oblique release incision at the
ATROPHIC POSTER IOR MAXILLA AND MANDIBLE
Figure 7 Four-month reentry. Note excellent block graft incorporation.
Figure 8 Nonsubmerged placement of four threadedimplants.
Figure 9 Completed prosthetics. Figure 10 Radiograph indicating crestal bone stability at1-year post–prosthetic loading.

38 Alpha Omegan, Volume 98, Number 3, October 2005
mesial marginal ridge of the first bicuspid tooth. Thisincision extended into the depth of the vestibule. Themidcrestal incision continued superiorly in theascending ramus area with a small oblique release
incision into the buccinator muscle (see Figure 14). Afull-thickness mucoperiosteal flap was reflected,allowing for visualization of the right ramus buccalshelf. Appropriate osteotomies were then accom-
ATROPHIC POSTER IOR MAXILLA AND MANDIBLE
Figure 12 Note vertical alveolar deficiency. Figure 13 Right posterior maxilla indicating adequate alveo-lar bony height for implants without the need for sinus grafting.
Figure 14 Incision design for ramus buccal shelf block graftharvest.
Figure 15 Superior crestal, anterior and posterior verticalosteotomies completed.
Figure 16 Bone spreader used for block graft harvest. Figure 17 Harvested ramus buccal shelf block graft.

Alpha Omegan, Volume 98, Number 3, October 2005 39
plished with a 702L straight fissure bur. The samebur was used for the superior and both verticalosteotomies (see Figure 15). Next, a #8 round burwas used to connect the inferior aspect of both verti-cal osteotomies. The block graft was harvested afteroutfracture along the groove created by the roundbur and was placed into normal saline solution priorto contouring and fixation (see Figures 16 and 17).The wound site was packed with gauze soaked inplatelet-poor plasma. Attention was turned to theright posterior maxilla, where the recipient site hadbeen prepared with burnishing or decortication ofthe crestal component of the ridge, followed by per-forations with a 0.8 mm diameter drill (Figure18).14–17 Platelet-rich plasma was then applied at therecipient site, followed by placement of the con-toured block. The block had been perforated withthe same 0.8 mm bur. Three-point fixation wasaccomplished with 1.6 mm diameter × 12 mmlength titanium alloy screws (Figure 19). Soft tissueclosure was accomplished without tension, takingadvantage of both an anterior and a posterioroblique release incision. This allowed for completerelaxation of the flap, along with scoring of theunderlying periosteum and buccinator muscle.Additional augmentation was accomplished withdemineralized freeze-dried bone putty followed byplatelet-rich plasma and a collagen membrane as acarrier (Colla Tape). Primary closure was accom-plished with 4-0 Vicryl suture for crestal closure and5-0 chromic suture for release incision closure.
Attention was turned to the donor site, whereplatelet-rich plasma was used prior to closure with4-0 Vicryl suture and 4-0 chromic suture. For verti-cal augmentation with mandibular block grafts, theauthor recommends 5 months healing time prior tostage I surgery.13 Reentry was thus done at this pointin time, and the block graft was found to be wellincorporated, with no evidence of resorption (Fig-ures 20 and 21). Three 3.75 mm diameter × 13 mmlength hydroxyapatite-coated Spline Twist implantswere then placed in a nonsubmerged mode (Figure22). Approximately 3 months later, a three-unitimplant-borne fixed restoration was fabricated.
Case 3
A 56-year-old female physician was referred for fail-ing longspan bridgework of the right posteriormandible. Clinical and radiographic examinationrevealed alveolar width deficiency in the area of themissing mandibular right second bicuspid and firstmolar teeth (Figures 23 and 24). The treatment planincluded lateral ridge augmentation followed byimplant placement times three for implant-bornebridgework. A right ramus buccal shelf block graftwould be harvested for the augmentation followedby 5 months of healing and stage I surgery. Theimplants would be placed in a nonsubmerged mode,and 3 months later, the final restorative work wouldbe completed.
The recipient and donor site are in the samewound site, resulting in a common, single incision.
ATROPHIC POSTER IOR MAXILLA AND MANDIBLE
Figure 18 Recipient site development. Note crestal burnish-ing with perforations.
Figure 19 Block graft fixation.

40 Alpha Omegan, Volume 98, Number 3, October 2005
reflection revealed a knife-edged edentulous ridge(Figure 25). Recipient site preparation includeddecortication and perforation (Figure 26). Note thatdecortication involves creation of a rectangular recip-
ATROPHIC POSTER IOR MAXILLA AND MANDIBLE
Figure 21 Note fixation screws in proper alignment forimplant osteotomies.
Figure 22 Nonsubmerged placement of implants. Figure 23 Right posterior mandibular failed bridgework.Note lateral alveolar ridge deficiency.
Figure 24 Radiograph indicating failed longspan bridgework.
The incision design is similar to the last case in thatthe crestal and intrasulcular incision is used with ananterior oblique release in the area of the bicuspidcanine region. Full-thickness mucoperiosteal flap
Figure 20 Five-month reentry. Note excellent graft incorporation.
Figure 25 Note knife-edged atrophic ridge.

Alpha Omegan, Volume 98, Number 3, October 2005 41
Figure 29 Note lingual flap release of 7 to 8 mm.
ient site that has more bone removal in the mid–ver-tical region, extending in an apical direction. Theamount of bone reduction from the crest of the ridgeto the midpoint vertically is minimal compared withthe amount from the midpoint to the more apicalextent. An inferior shelf is created, allowing for theblock graft to be intimately morticed into this well-outlined recipient bed. Three screws were used forfixation (Figure 27). The importance in this locationfor soft tissue closure without tension cannot beoveremphasized. Initially, buccal flap release isaccomplished by scoring the periosteum with a #15blade. More importantly, however, is release of thelingual flap. This is done by extending the crestalincision into the lingual sulcus three to four teethanterior to the edentulous site to prevent flap tearing.The lingual flap is then reflected with an elevatorfrom the crest into the lingual sulcus followed by
blunt finger dissection in a more apical direction.This finger dissection includes stripping of the mylo-hyoid muscle in both an anterior and a posteriordirection and results in a gain of approximately 6 to8 mm of flap advancement (Figures 28 and 29).13
Prior to graft fixation, platelet-rich plasma was usedat the interface between the recipient site and blockbone. Finally, the entire wound site was immersedwith platelet-rich plasma, and a Colla Tape mem-brane acted as a carrier. Primary closure was accom-plished with 4-0 Vicryl suture for crestal closure and5-0 chromic suture for release incision closure. Five-month reentry revealed excellent graft incorporation,with no evidence of resorption (Figure 30).
Three 3.7 mm diameter × 11.5 mm lengthSpline-Twist implants were placed in a nonsub-merged mode (Figure 31). Three months later, therestorative work is completed (Figure 32).
ATROPHIC POSTER IOR MAXILLA AND MANDIBLE
Figure 26 Recipient site preparation. Note decorticationresulting in a rectangular inlay outline.
Figure 27 Block graft fixation.
Figure 28 Mylohyoid muscle release via blunt finger dissection.
42 Alpha Omegan, Volume 98, Number 3, October 2005
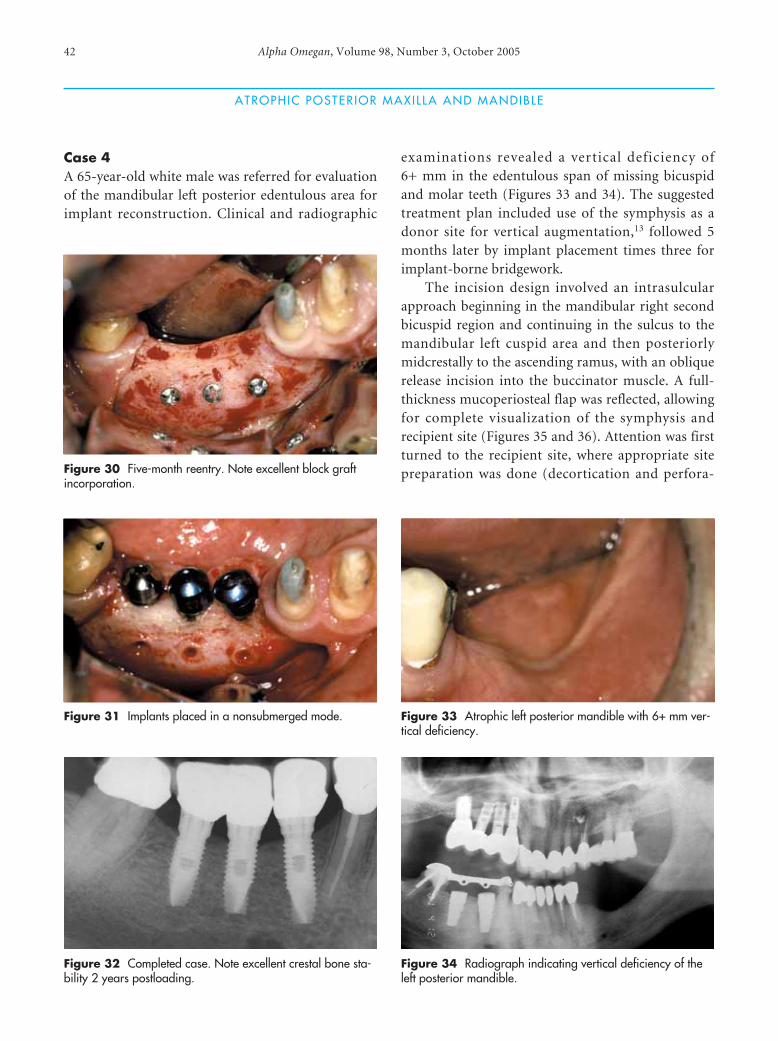
Case 4A 65-year-old white male was referred for evaluationof the mandibular left posterior edentulous area forimplant reconstruction. Clinical and radiographic
examinations revealed a vertical deficiency of6+ mm in the edentulous span of missing bicuspidand molar teeth (Figures 33 and 34). The suggestedtreatment plan included use of the symphysis as adonor site for vertical augmentation,13 followed 5months later by implant placement times three forimplant-borne bridgework.
The incision design involved an intrasulcularapproach beginning in the mandibular right secondbicuspid region and continuing in the sulcus to themandibular left cuspid area and then posteriorlymidcrestally to the ascending ramus, with an obliquerelease incision into the buccinator muscle. A full-thickness mucoperiosteal flap was reflected, allowingfor complete visualization of the symphysis andrecipient site (Figures 35 and 36). Attention was firstturned to the recipient site, where appropriate sitepreparation was done (decortication and perfora-
ATROPHIC POSTER IOR MAXILLA AND MANDIBLE
Figure 30 Five-month reentry. Note excellent block graftincorporation.
Figure 31 Implants placed in a nonsubmerged mode.
Figure 32 Completed case. Note excellent crestal bone sta-bility 2 years postloading.
Figure 33 Atrophic left posterior mandible with 6+ mm ver-tical deficiency.
Figure 34 Radiograph indicating vertical deficiency of theleft posterior mandible.

Alpha Omegan, Volume 98, Number 3, October 2005 43
Figure 37 Block graft fixation for 6+ mm vertical augmentation. Figure 38 Five-month reentry. Note excellent block graftincorporation.
tion). Please note the vertical step created distal tothe canine, allowing for a butt joint between theblock graft and recipient site. The extent of thisdefect required the symphysis to be used as a donorsite as opposed to the ramus buccal shelf (see Figure36). The block graft was harvested in two pieces,allowing for fixation of each block separately (Figure37). Marrow harvested from the donor site was mor-ticed into small gaps that were created between blockand the recipient bone. Platelet-rich plasma wasused at this interface, and the donor site was graftedwith demineralized freeze-dried putty and platelet-rich plasma. The wound site was immersed withplatelet-rich plasma prior to primary closure, whichwas accomplished with 4-0 Vicryl suture and 5-0chromic suture. Five months later, three root-formimplants were placed in a nonsubmerged mode into
the block graft site (Figures 38 and 39). The anteriorimplant was 11.5 mm in length, and the remainingtwo implants were 10 mm in length. Note the radi-ographically crestal bone maintenance of the graftedbone at 3 years post–functional load in Figure 40.
Discussion
Mandibular block autografts for maxillary andmandibular ridge augmentation are predictable andoffer many advantages. These grafts are primarilycortical in nature, exhibit minimal resorption andtend to incorporate exceptionally well with recipientbone within a relatively short time frame. They alsomaintain post–implant placement bone volume andretain the radiographic density to the augmented site.Despite the many advantages block grafts offer foralveolar ridge augmentation, however, complications
ATROPHIC POSTER IOR MAXILLA AND MANDIBLE
Figure 35 Intraoperative view indicating deficiency. Figure 36 Symphysis block graft outline.

44 Alpha Omegan, Volume 98, Number 3, October 2005
can occur when these grafts are used for both hori-zontal and vertical deficiencies of the posterior max-illa and mandible.
Morbidity with this grafting protocol is associatedwith both donor and recipient sites. Symphysis donorsite morbidity includes intraoperative complicationssuch as bleeding; mental nerve injury; soft tissueinjury of cheeks, lips and tongue; block graft fractureand potential bicortical harvest. Bleeding episodes areintrabony and can be taken care of with cautery, localanesthesia and collagen plugs. Injury to the mentalneurovascular bundle is avoidable with proper surgi-cal technique, especially with use of the sulcularapproach. Block fracture and bicortical block harvestcan also be prevented by following good surgical tech-nique. Pain, swelling and bruising occur as normalpostoperative sequelae and are not excessive in nature.Use of platelet-rich plasma has decreased overall softtissue morbidity. The infection rate is minimal (lessthan 1%). Neurosensory deficits include altered sen-sation of the lower lip and chin (temporary 19%; per-manent less than 1%) and dysesthesia of the anteriormandibular dentition (transient 53%; permanent lessthan 1%). No evidence of dehiscence was seen whenusing the sulcular approach.
The ramus buccal shelf harvest can also result inintraoperative complications, including bleeding,nerve injury, soft tissue injury, block fracture andmandible fracture. Intrabony and soft tissue bleedingcan be handled with cautery. Injury to the inferior
alveolar and lingual neurovascular bundle can beavoided with proper soft tissue manipulation andmeticulous osteotomy preparation. Block fracture isalso an avoidable problem with proper surgical tech-nique. Postoperative morbidity includes trismus(approximately 68%); however, this is transient andcan take up to 3+ weeks to resolve. Pain, swelling andbruising are typically mild to moderate and minimalwith the use of platelet-rich plasma. The infectionrate is less than 1%. Altered sensation of the lower lipor chin occurs approximately 8% of the time, withless than 1% being permanent. Altered sensation ofthe lingual nerve has also been reported but has beentransient only. Although altered sensation of themandibular dentition can occur (less than 1%), nonehave been permanent.
Recipient site morbidity includes trismus, bleed-ing, pain, swelling, bruising, infection, neurosensorydeficits, bone resorption, dehiscence and graft failure.Bleeding of the recipient bed is intentional secondaryto meticulous site preparation (decortication andperforation), but excessive bleeding, although rare,can occur secondary to both intrabony and soft tissuevessel transection. Pain, swelling and bruising aremild to moderate and are minimized with platelet-rich plasma. The infection rate is less than 1% and isusually secondary to graft exposure. Neurosensorydeficits can occur secondary to site preparation andblock fixation should normal anatomy be violated.Dehiscence and graft failure are seen secondary to
ATROPHIC POSTER IOR MAXILLA AND MANDIBLE
Figure 39 Implants placed in a nonsubmerged mode intotype I quality bone.
Figure 40 Completed prosthetics. Note excellent crestalbone stability at 3 years post–prosthetic loading.

Alpha Omegan, Volume 98, Number 3, October 2005 45
soft tissue closure with tension or prosthesis contactwith the graft site. Finally, block graft resorption atstage I surgery is minimal (0–20%) but can be exces-sive if dehiscence of the graft occurs. In summary,overall morbidity of mandibular block autografts foratrophic posterior maxillary and mandibular recon-struction is minimal. Most complications are pre-ventable. Those that occur can be handled pre-dictably with minimal adverse affects to the patient.
References1 Burchardt H. Biology of bone transplantation. Orthop Clin
North Am 1987; 18:187–195.
2. Marx RE. Biology of bone grafts. In: Kelly JPW, ed. OMS
knowledge update. Vol 1. Rosemont, IL: American Associa-
tion of Oral and Maxillofacial Surgeons, 1994:RCN3–
RCN17.
3. Brånemark P-I, Lindstrom J, Hallen O, et al. Reconstruction
of the defective mandible. Scand J Plast Reconstr Surg 1975;
9:116–128.
4. Helkimo E, Carlsson GE, Helkimo M. Bite force and state of
dentition. Acta Odontol Scand 1977; 35:297–303.
5. Haraldson T, Carlsson GE. Bite force and oral function in
patients with osseointegrated implants. Scand J Dent Res
1977; 85:200–208.
6. Braun S, Bantleon HP, Hnat WP, et al. A study of bite force:
part I. Relationship to various physical characteristics. Angle
Orthod 1995; 65:367–372.
7. Jensen J, Sindet-Pedersen S. Autogenous mandibular bone
grafts and osseointegrated implants for reconstruction of
the severely atrophied maxilla: a preliminary report. J Oral
Maxillofac Surg 1991; 49:1277–1287.
8. Jensen J, Sindet-Pedersen S, Oliver AJ. Varying treatment
strategies for reconstruction of maxillary atrophy with
implants: results in 98 patients. J Oral Maxillofac Surg 1994;
52:210–216.
9. Collins TA. Onlay bone grafting in combination with
Brånemark implants. Oral Maxillofac Surg Clin North Am
1991; 3:893–902.
10. Pikos MA. Block autografts for localized ridge augmenta-
tion: part I. The posterior maxilla. Implant Dent 1999;
8:279–284.
11. Pikos MA. Alveolar ridge augmentation with ramus buccal
shelf autografts and impacted third molar removal. Dent
Implantol Update 1999; 10:27–31.
12. Pikos MA. Alveolar ridge augmentation using mandibular
block grafts: clinical update. Alpha Omegan 2000; 93:14–21.
13. Jensen OT, Pikos MA, Simion M, Vercellotti T. Bone graft-
ing strategies for vertical alveolar augmentation. In: Peter-
son’s principles of oral and maxillofacial surgery. 2nd ed.
Hamilton, ON: BC Decker, 2004:12:223–232.
14. Frost H. The regional acceleratory phenomenon: a review.
Henry Ford Hosp Med J 1983; 31:3–9.
15. Frost H. The biology of fracture healing: an overview for
clinicians, part I. Clin Orthop 1989; 248:283–292.
16. Frost H. The biology of fracture healing: an overview for
clinicians, part II. Clin Orthop 1989; 248:294–309.
17. Shih MS, Norrdin RW. Regional acceleration of remodeling
during healing of bone defects in beagles of various ages.
Bone 1985; 6:377–379.
ATROPHIC POSTER IOR MAXILLA AND MANDIBLE
Please support our advertisers. Tell their representatives who call on you that you saw their advertisement in
Alpha Omegan and appreciate their support.Thank you!
Brasseler USA
Kerr Corporation
Towers Administrator’s, Inc.