tkcc/garvan cancer biology seminars triple negative breast
TRANSCRIPT

TKCC/Garvan Cancer Biology Seminars
Triple Negative Breast Cancer
Elgene Lim Lab Head: Connie Johnson Breast Cancer Laboratory
Snr Medical Oncologist: TKCC

Breast cancer is a molecularly heterogeneous disease
TCGA, Nature 2012

Biological questions
1) Is the differential breast cancer subtype
distribution between WT, BRCA1, and
BRCA2 mutants due to hormonal signaling?
2) How does modulating ER signaling reduce
the risk of BRCA1 and BRCA2 breast cancer?
• Oophorectomy & Tamoxifen chemoprevention ↓
BC risk ≈50% in both BRCA1 and 2 carriers
Lifetime risk General
Population BRCA1 BRCA2 C
Breast Ca 10% A 70-80% B 50-60%
ER+ 65-70% 20% 60-65%
TNBC 10-15% 80% 10-15%
Ovarian Ca 1-2% 50% 30%
BRCA mutation and cancer
A Similar prognosis to BRCA tumors at same stage. B Younger, high grade. C Asso with increased risk of pancreatic, prostate & male breast cancer.
Roy et al. Nat Rev Can 2011
BRCA1, Chrom 17, 220 kDA nuclear protein
BRCA2, Chrom 13, 384 kDA nuclear protein
HER2 Lum B Lum A Basal
BRCA1 BRCA2 Sorlie et al. PNAS 2003
A C
B

4
Characteristics
1) High Grade, frequent
mitosis, pleomorphic nuclei,
poorly differentiated
2) Pushing borders
3) Lymphocytic infiltrate
4) Associated with BRCA1 mut
Medullary Breast Cancer

Germline mutations in DNA repair
genes in TNBC
Domagala et al, Plos One 15

Germline mutations in DNA repair
genes in TNBC
Domagala et al, Plos One 15

Overview
• Heterogeneity of TNBC
• Therapeutic approaches to TNBC – Standard chemotherapy
– Platinums
– PAPR inhibitors
– Bevacizumab
• Novel targets in TNBC – CDK inhibitors
– Immunotherapy
7

TNBC Molecular subtypes
8 Lehmann et al. JCI 2011
(1) AR-positive (LAR), (2) claudin-low enriched
mesenchymal (M), (3) mesenchymal stem–like (MSL) (4) immune response (IM) and (5) 2 cell-cycle–disrupted basal
subtypes: (a) BL-1 and (b) BL-2.
Publically available breast cancer expression datasets Training set 386 TNBC Validation 201 TNBC

Differential therapeutic response
according to TNBC subtypes
9 Lehmann et al. JCI 2011

TNBC Molecular subtypes
10 Burstein et al. CCR 2015

TNBC Molecular subtypes
11 Burstein et al. CCR 2015
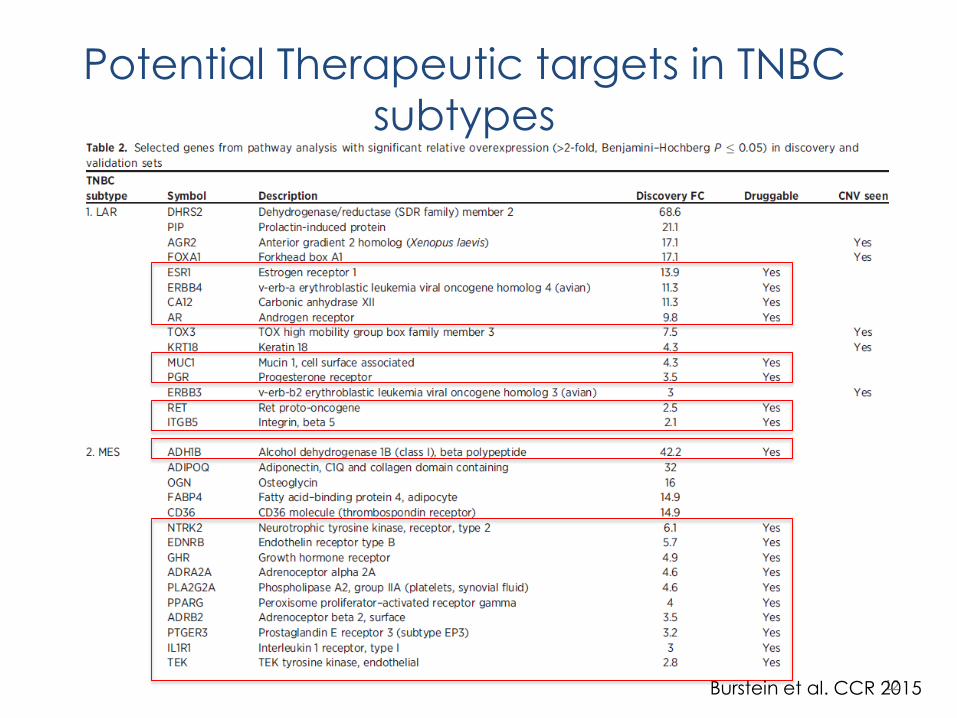
Potential Therapeutic targets in TNBC
subtypes
12 Burstein et al. CCR 2015

Potential Therapeutic targets in TNBC
subtypes
13 Burstein et al. CCR 2015

Overview
• Heterogeneity of TNBC
• Therapeutic approaches to TNBC – Standard chemotherapy
– Platinums
– PAPR inhibitors
– Bevacizumab
• Novel targets in TNBC – CDK inhibitors
– Immunotherapy
14

Standard Chemotherapy
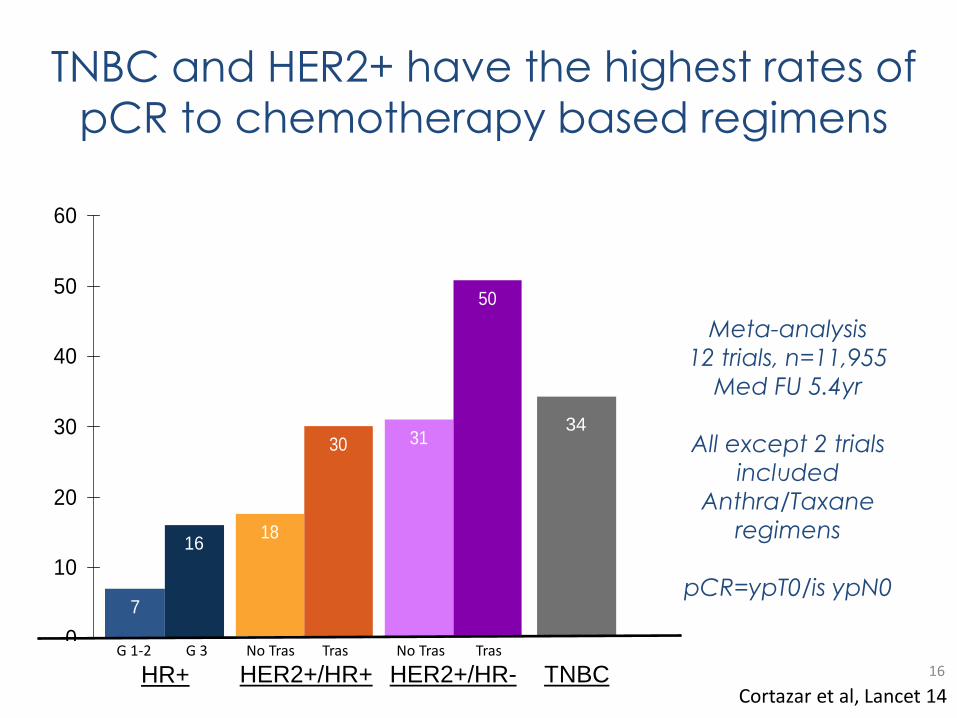
TNBC and HER2+ have the highest rates of
pCR to chemotherapy based regimens
16
Cortazar et al, Lancet 14 HR+ TNBC HER2+/HR+ HER2+/HR-
18
30 31
50
.
G 1-2 No Tras
34
G 3 Tras No Tras Tras
7
16
0
10
20
30
40
50
60
Meta-analysis
12 trials, n=11,955
Med FU 5.4yr
All except 2 trials
included
Anthra/Taxane
regimens
pCR=ypT0/is ypN0

pCR is associated with improved
outcomes compared to no pCR
17
Cortazar et al, Lancet 14
HR 0.48 (0.43 – 0.54)
HR 0.36 (0.31 – 0.42)
In analyses by subtype, the relationship held most true for the
“aggressive” subtypes, triple negative, HER2+ (especially ER-, HER2+)
and high grade ER+

Platinums in TNBC
18
Platinums in treatment naïve TNBC
Presented at SABCS 2015
– W Sikov, CALGB 40603 trial
– G Von Minckwitz, GeparSixto trial
– O Gluz, Adapt trial
19

20
CALGB 40603 Schema

21
Response: pCR

Survival outcomes
22

23

Concurrent Trastuzumab and Lapatinib in HER2+ subgroup. Concurrent Bev in TNBC subgroup.
24
GeparSixto Schema

25
TNBC Schema

26
pCR by subtype
27
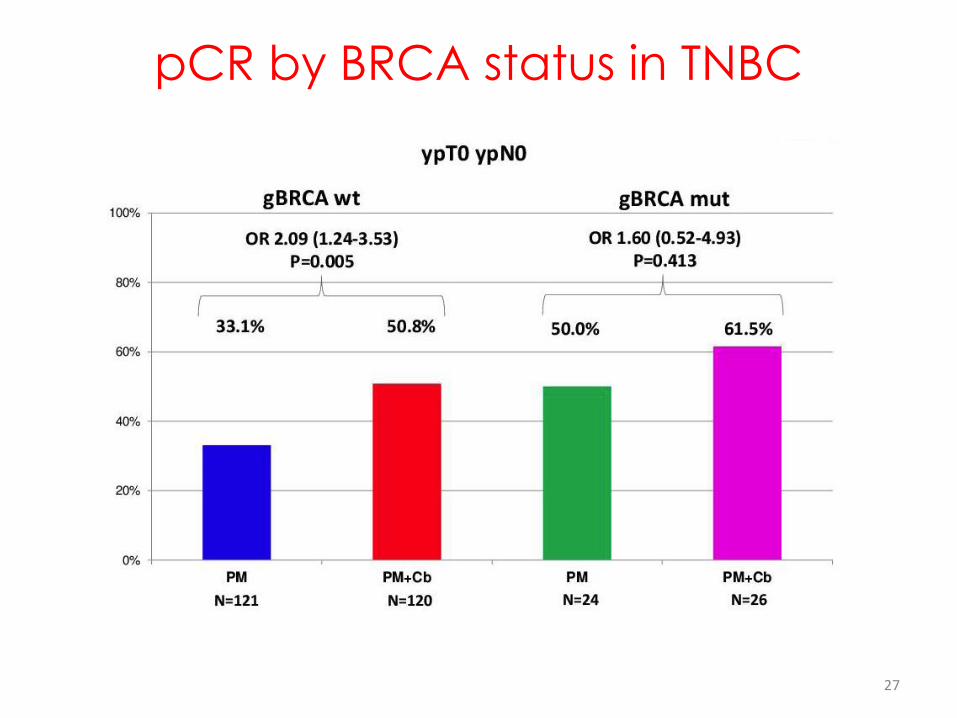
pCR by BRCA status in TNBC

28
DFS by subtype

29

PEP • pCR (ypT0/is ypN0) • pCR in early responders
vs non responders SEP • EFS and OS • Toxicity
4 x EC given as adjuvant tx to those without pCR
30
ADAPT Schema

31
Hypothesis

Pt characteristics
Consort Diagram
32
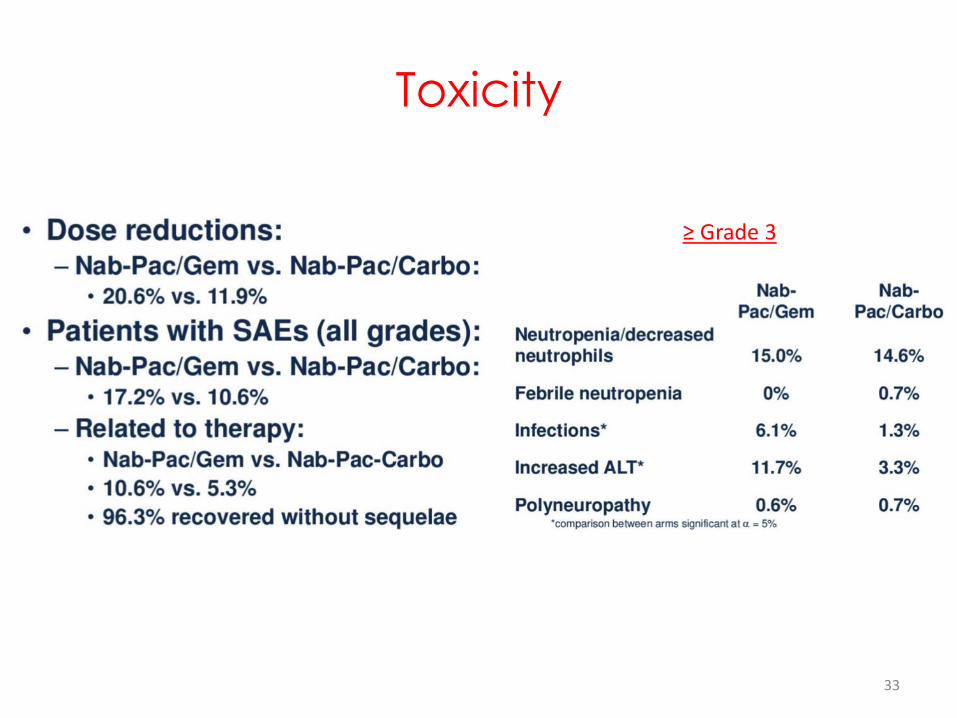
Toxicity
≥ Grade 3
33

Response: pCR
Subgroup Analysis
34

Conclusions – CALGB 40603
• Achievement of pCR is asso with significant improvements in EFS and OS,
however study was underpowered to determine if addition of Carbo or
Bevacizumab improves EFS/OS
• Previous studies (Beatrice, GeparQuinto, NSABP B-40) failed to
demonstrate improvements in long term outcomes with addition of
Bevacizumab in neoadjuvant setting.
• Despite high pCR rates, neither Carbo nor Bev have been shown to improve
RFS or OS when given as part of a neoadj regimen
35

Conclusions – GeparSixto
• Carbo improved EFS in TNBC (HR = 0.65, p<0.5) but not in
HER2+ BC
• DFS benefit of Carbo was predicted by pCR
• Unexpected improvement in EFS in BRCA WT pts and not in
BCRA mut carriers.
• Favorable prognosis after pCR is independent of BRCA status
36

Conclusions - Adapt
• Nab-Pac/Carbo is asso with less toxicity and is superior to
Nab-Pac/Gem in achieving pCR (45.9% vs 28.7%)
• Observed efficacy is comparable to longer and more toxic
anthracycline-taxane combination tx
• Early morphological changes predict for pCR irrespective of
treatment arm
• No predicitve factors for Carbo efficacy have been identified
so far
37

Survival outcomes across trials
38
GeparSixto
• More intensive
backbone
• Weekly Carbo - ?
Less time for DA
repair
• Concurrent Tx -
?Synergy

Do these data warrant routine use of
Carbo in TNBC?
• Hazard ratios suggest benefit, but not enough data
to be conclusive
• Chemo backbone and Carbo dose/schedule may
be critical to optimal efficacy
– CALGB 40603: Taxol
– GeparSixto: Taxol, Peg Doxo
– Adapt: Peg Taxol
• LT effects of added toxicity not known
39

9
.
48% (41-54%) 59% (52-65%)
Odds ratio: 1.58 p = 0.0089
n=218 n=215
Sikov et al, JCO 14
CALGB 40603: Neoadj
Chemotherapy +/- Bev in TNBC BEATRICE: Adjuvant Bev in TNBC
Cameron et al, Lancet Onc 13
Bevacizumab in TNBC

PARP inhibitors
Sonnenblick et al, Nat RV Clin Onc 15

PARPi in clinical development
Sonnenblick et al, Nat RV Clin Onc 15

PARPi in clinical development
Livarghi and Garber, BMC Med 15

PARPi in clinical development
Livarghi and Garber, BMC Med 15

Resistance to PARPi
Livarghi and Garber, BMC Med 15

Overview
• Heterogeneity of TNBC
• Therapeutic approaches to TNBC – Standard chemotherapy
– Platinums
– PARP inhibitors
– Bevacizumab
• Novel targets in TNBC – CDK inhibitors
– Immunotherapy
46

CDK complexes are involved in cell cycle
and other biological processes
Asghar et al. Nat Rv Drug Disc 2015
Palbociclib Ribociclib
Abemaciclib
Flavopiridol Seliciclib
Dinaciclib
TZH1/2
CDK12
CycK
47

Rationale for Combining PARP Inhibition with
Agents Targeting HR
HR-Proficient Cancers
• Goal is to selectively disrupt HR in cancer cells and sensitize to PARP inhibition
HR-Deficient Cancers
• (germline or somatic HR gene mutation, e.g. BRCA1/2)
• Acquired resistance to PARP inhibition often involves restoration of HR
• De novo resistsance to PARP inhibition exists (hypomorphic BRCA proteins)
• In PARP inhibitor-sensitive tumors, goal is to augment the extent and durability of response
Ashworth, Cancer Res 2008; Dhillon et al. Cancer Sci 2011; Jaspers et al. Cancer Discov 2012; Johnson et al. PNAS 2013; Bouwman et al. Clin Cancer Res 2014; Bunting et al. Mol Cell 2012
HR deficient HR proficient
Agents that inhibit HR
Platinum
or
PARP Inhibitor
+
48

Genome wide synthetic lethality identifies CDK12 as a determinant of PARPi sensitivity in Ov Ca
Bajrami et al., Can Res 2014 49
Mutations in CDK12 in TCGA Serous Ov Ca 2011 (n= 316)
Low CDK12 expression correlates with PARPi sensitivity in serous Ov Ca cell lines

Dinaciclib is a potent inhibitor of CDK9/12
50
44% homology in
Kinase Domain of
CDK9 and CDK12
Dinaciclib is the most
potent known
inhibitor of CDK12
(IC50 68nM)

Dinaciclib decreases BRCA1 and DNA repair genes
in DNA damage and repair pathways
Can Dinaciclib induce a BRCA1 deficient phenotype and PARPi sensitivity?
Ingenuity Pathway Analysis
BRCA1 in DNA repair pathway
51
Transcriptome of Dinaciclib tx vs untx MDA-MD-231 cells

Dinaciclib sensitizes BRCA1-proficient cells to PARPi
V
ehic
le
10
nM
D
inac
iclib
10
Gy
γ ir
rad
iati
on
BR
CA
1 p
rofi
cien
t TN
BC
ce
ll lin
es
52
In the presence of dinaciclib, the IC50 to veliparib was reduced
between 2.5 and 12.5-fold

Cisplatin & Olaparib Resistant BRCA2mut PDX derived from metastasis
BRCA mutant TNBC cells with acquired PARPi
resistance are resensitized by Dinaciclib
53
In vitro In vivo
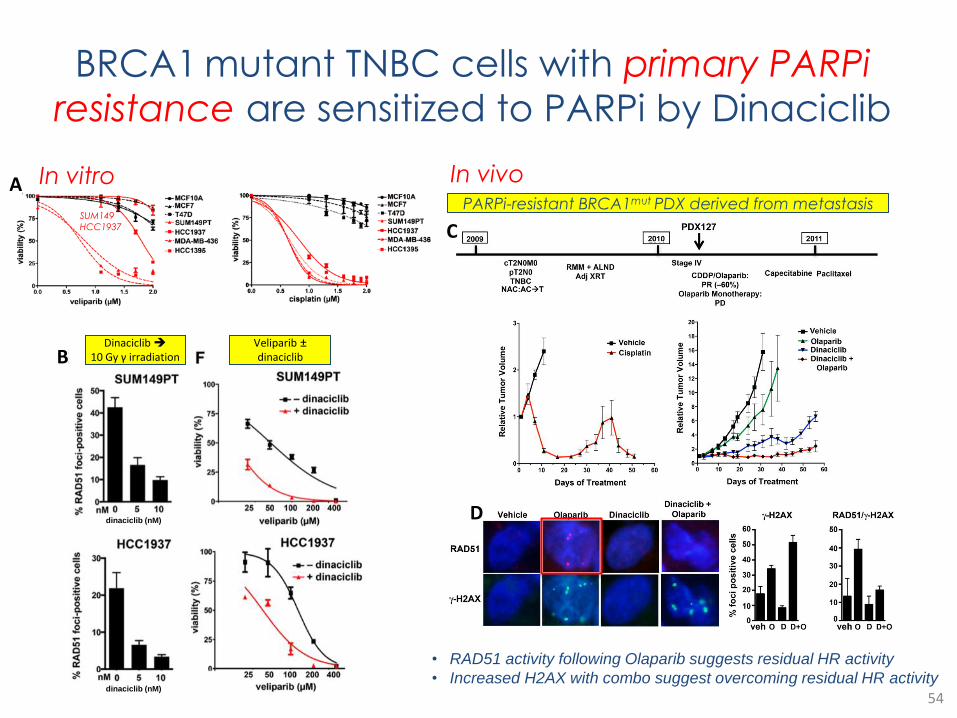
BRCA1 mutant TNBC cells with primary PARPi
resistance are sensitized to PARPi by Dinaciclib
54
Dinaciclib 10 Gy γ irradiation
dinaciclib (nM)
dinaciclib (nM)
Veliparib ± dinaciclib
SUM149
HCC1937
In vitro A
B
In vivo PARPi-resistant BRCA1mut PDX derived from metastasis
C
D
• RAD51 activity following Olaparib suggests residual HR activity
• Increased H2AX with combo suggest overcoming residual HR activity
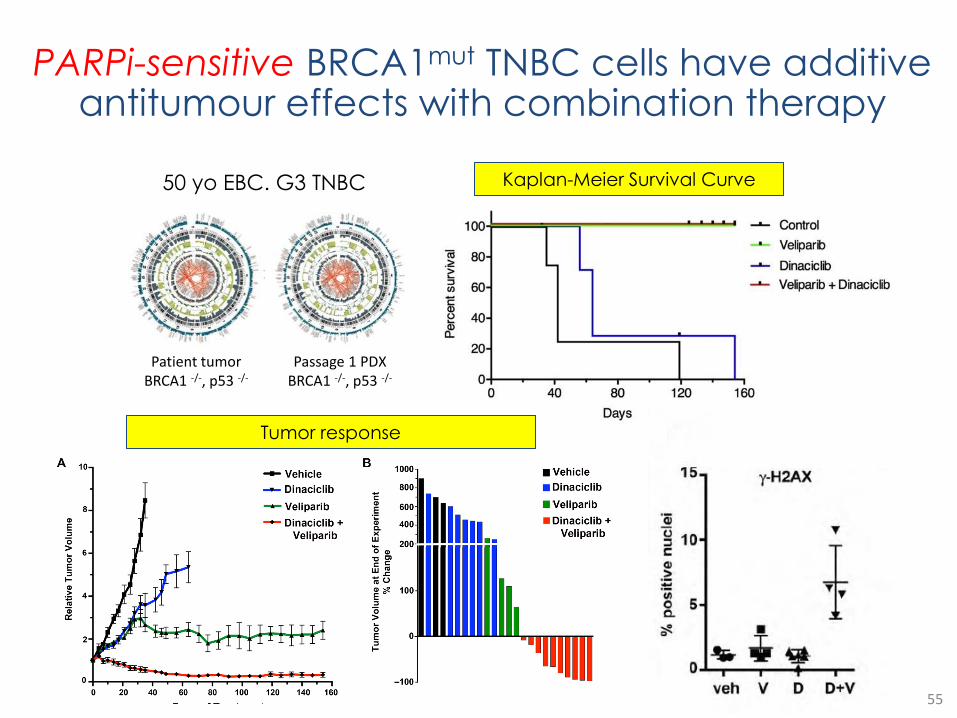
Patient tumor BRCA1 -/-, p53 -/-
Passage 1 PDX BRCA1 -/-, p53 -/-
50 yo EBC. G3 TNBC Kaplan-Meier Survival Curve
Tumor response
55
PARPi-sensitive BRCA1mut TNBC cells have additive antitumour effects with combination therapy

Minimal residual tumor after
combination treatment
End of Experiment
vehicle veliparib
dinaciclib combination

57
TZH1 binds selectively and irreversibly to CDK7, and inhibits
RNAPII CTD phosphorylation
GO Term analyses of 527 cell lines

58

Concept of Super-enhancers
Typical enhancers
• composed of transcription factor binding sites located at a
distance from the transcriptional start site that act through
chromosomal looping events to enhance transcription.
Super-enhancers
• consist of very large clusters of enhancers densely
occupied by transcription factors, co-factors and chromatin
regulators (e.g. BRD4)
• arise via gene amplification, translocation or transcription
factor overexpression
• facilitate high level of expression of genes involved in cell
identity, growth and proliferation; often genes and
encoded proteins have short half-life, so high-level
transcription is critical to maintenance of their expression
• highly sensitive to perturbation
Whyte et al. Cell 2013; 153: 307-19; Lovén et al. Cell 2013; 153: 320-34;
Chapuy et al. Cancer Cell 2013; 24: 777-90. 59

CDK7 inhibition selective targets TNBC
BC cell lines
Primary BC cell lines
Live (green)/Dead (red) Cell viability assay
60
B A
D C E
Selective induction of apoptosis and suppression of RNAPII CTD phosphorylation
Red: TNBC cell lines Blue: ER+ cell lines
Wang et al., Cell 2015

61
Differentially expressed TNBC genes are sensitive
to CDK7i and are critical for TNBC survival
BT549 MB-468 ZR-75-1
T47D
Enriched GO functional categories of TNBC genes sensitive to THZ1 tx
Signalling pathways and transcription factors comprising
Archilles Cluster of genes
40% of the genes in the Achilles cluster were associated with super-enhancers in TNBC cells
THZ1 treatment globally affects steady-state mRNA levels in TNBC
Genes differentially expressed between TNBC and ER/PR+ breast cancer lines.
Wang et al., Cell 2015

Summary
• CDK7 +/- CDK9 inhibitors may perturb superenhancer complexes that
govern expression of genes controlling the oncogenic state
• CDK7 is a relevant target in TNBC cells
• CDK12 is a relevant target for disrupting DNA repair pathways such as HR
and for sensitizing breast cancer cells to DNA damage or PARP inhibition
• Dinaciclib is a highly potent inhibitor of CDK12 and sensitizes BRCA wild-
type, HR-proficient TNBC cell lines to PARP inhibition
• Dinaciclib reverses acquired resistance and overcomes primary resistance to
PARP inhibition in BRCA-mutated cells
• Phase 1 trial of dinaciclib/veliparib is underway, with planned expansion cohort
work in BRCA WT and mutated TNBC
62
Immunotherapy and TNBC
63


65


How does this compare with other solid tumours?
67

TILS in TNBC outcomes
68

69
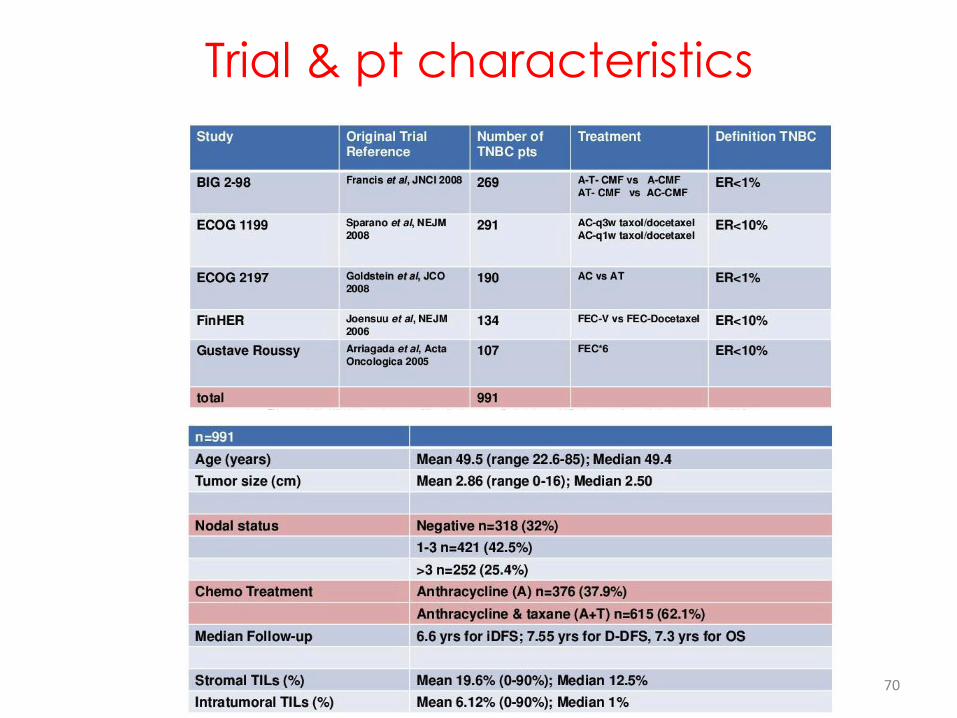
70
Trial & pt characteristics

71
Multivariate Cox Analyses (adjusted)

72
Conclusions

Basal-like 1: Cell cycle, DNA repair & proliferation genes
Basal-like 2: Growth factor signaling (EGFR, MET, Wnt, IGF1R)
IM: Immune cell processes (medullary breast cancer)
M: Cell motility and differentiation, EMT processes
MSL: Similar to M but growth factor signaling, low levels of proliferation genes (metaplastic cancers)
LAR: AR and downstream genes, luminal features
TNBC Subtypes: Potential Targets
PARPi, ± DNA damaging agents
EGFR (cetuximab, lapatinib) Self-renewal pathways (Wnt, Notch)
Immune check point (PD1/PDL1, CTLA4) Vaccines: MUC1, NYO-ESO1
AR modulators (enzalutamide, bicalutamide, etc)
PI3Ki, RAS/MEK/Erk,
MET, PTEN
etc, etc

1. Comprehensive Molecular Portraits of Human Breast tumours. TCGA. Nature 2012.
2. Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. JCI 2011.
3. Comprehensive Genomic Analysis Identifies Novel Subtypes and Targets of Triple-Negative Breast Cancer. Clin Cancer Res 2015
4. Dent R, Trudeau M, Pritchard KI, et al. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res 2007
5. Aromatase inhibitors versus tamoxifen in early breast cancer: patient-level meta-analysis of the randomised trials. EBCTCG. Lancet 2015.
6. Prognostic Value of Ki67 Expression After Short-Term Presurgical Endocrine Therapy for Primary Breast Cancer. Dowsett et al. JNCI 2007.
7. Randomized Trial of Letrozole Following Tamoxifen as Extended Adjuvant Therapy in Receptor + Breast Cancer. Goss et al. JNCI 2005.
8. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor + breast cancer: ATLAS, a randomised trial. Davies et al. Lancet 2013.
9. Adjuvant Ovarian Suppression in Premenopausal Breast Cancer. Francis et al. NEJM 2015.
10. A Multigene Assay to Predict Recurrence of Tamoxifen-Treated, Node-Negative Breast Cancer. Paik et al. NEJM 2004.
11. Combination Anastrozole and Fulvestrant in Metastatic Breast Cancer. Mehta et al. NEJM 2012.
12. Everolimus in Postmenopausal Hormone-Receptor + Advanced Breast Cancer. Baselga et al. NEJM 2012.
13. Palbociclib in Hormone-Receptor + Advanced Breast Cancer. Turner et al. NEJM 2015.
Suggested Readings