tối ưu hoá quy trình điều trị đột...
TRANSCRIPT

TỐI ƯU HOÁ QUY TRÌNH
CẤP CỨU ĐỘT QUỴ
Bs. ĐÀO VIỆT PHƯƠNG
Khoa Cấp cứu A9 – BV Bạch Mai
NỘI DUNG
Quy trình phân loại trước bệnh viện.
Rút ngắn Door to needle time.
Direct to CT/MRI protocol.
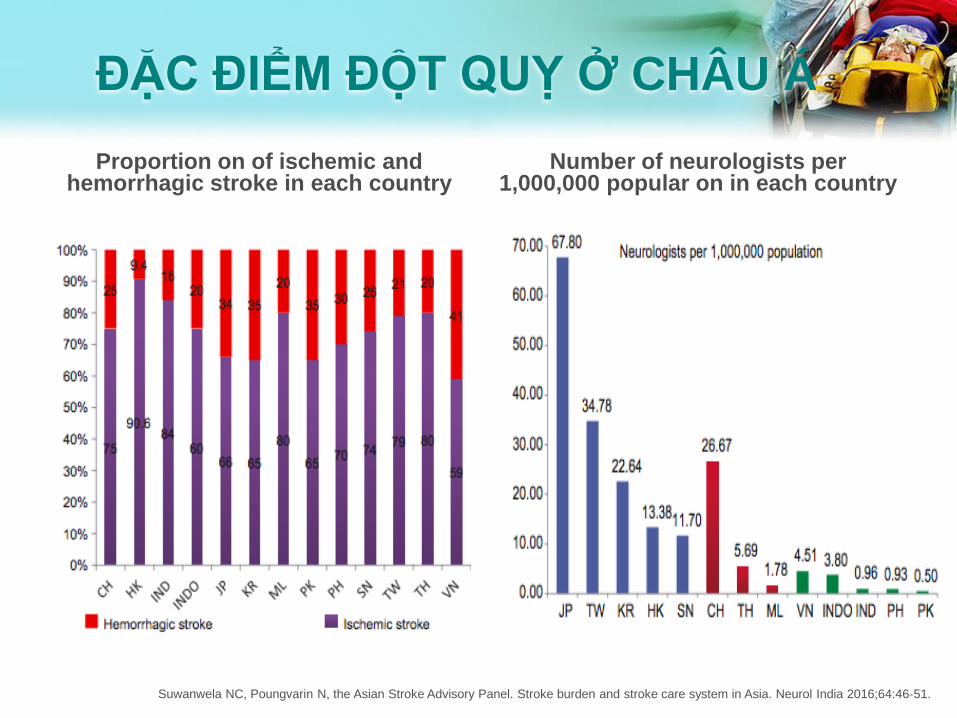
ĐẶC ĐIỂM ĐỘT QUỴ Ở CHÂU Á
Proportion on of ischemic and hemorrhagic stroke in each country
Number of neurologists per 1,000,000 popular on in each country
Suwanwela NC, Poungvarin N, the Asian Stroke Advisory Panel. Stroke burden and stroke care system in Asia. Neurol India 2016;64:46‐51.
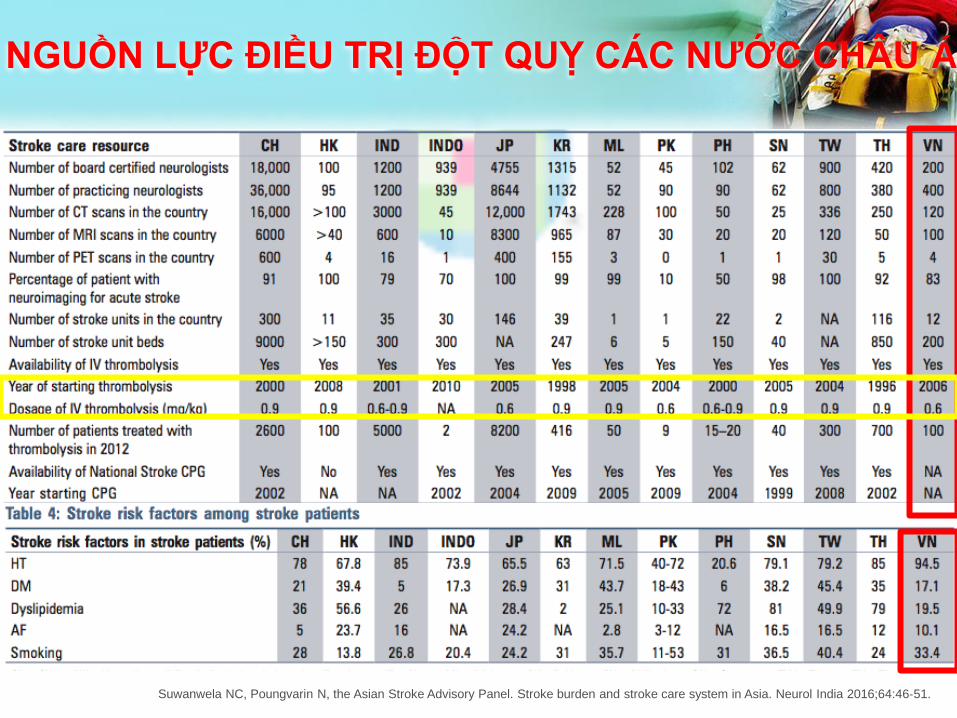
NGUỒN LỰC ĐIỀU TRỊ ĐỘT QUỴ CÁC NƯỚC CHÂU Á
Suwanwela NC, Poungvarin N, the Asian Stroke Advisory Panel. Stroke burden and stroke care system in Asia. Neurol India 2016;64:46‐51.

Johnston SC et al. Lancet Neurology 2009
TỈ LỆ TỬ VONG DO ĐỘT QUỴ

VAI TRÒ TÁI TƯỚI MÁU
Saver. Stroke 2006;37:263-266.González. Am J Neuroradiol 2006;27:728-735.
Donnan. Lancet Neurol 2002;1:417-425.
Cứ 1 phút trôi qua có 1,9
triệu neuron mất ở vùng
nhồi máu
Tái tưới máu làm giảm tổn
thương thiếu máu
Vùng lõi nhồi máu
Vùng tranh tối
tranh sáng
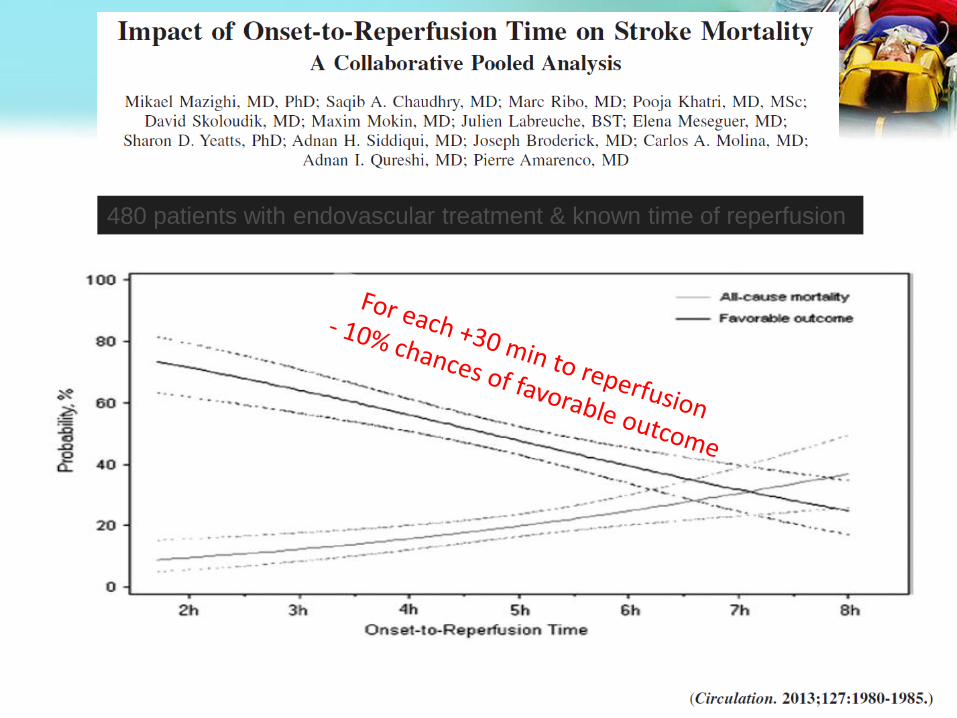
480 patients with endovascular treatment & known time of reperfusion
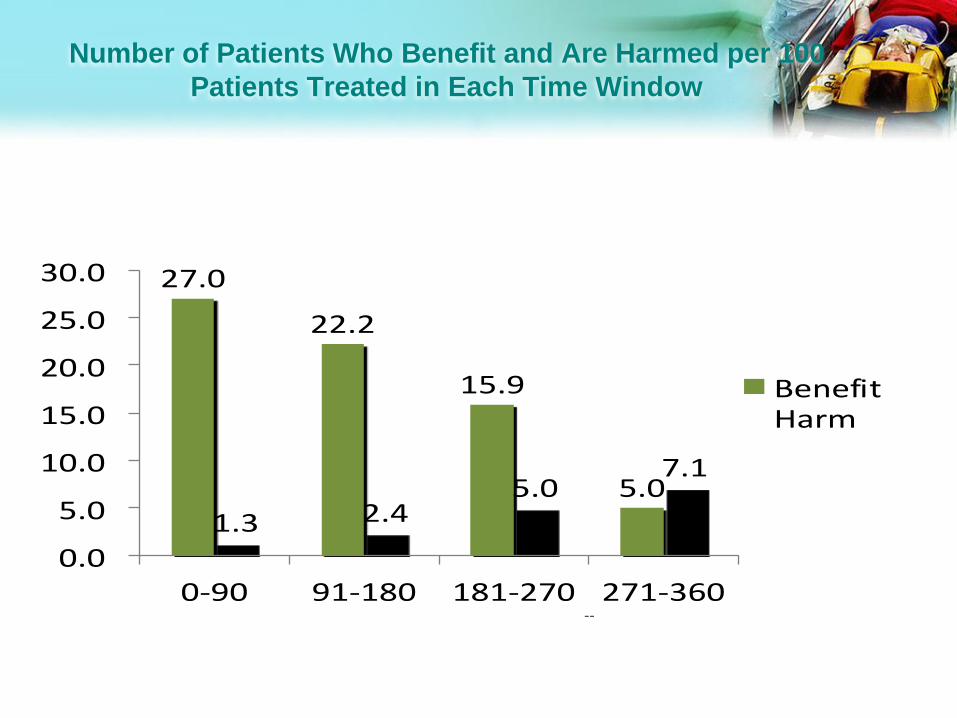
Number of Patients Who Benefit and Are Harmed per 100
Patients Treated in Each Time Window
27.0
22.2
15.9
5.0
1.3 2.45.0
7.1
0.0
5.0
10.0
15.0
20.0
25.0
30.0
0-90 91-180 181-270 271-360
BenefitHarm
--Lansberg et al, Stroke 2009
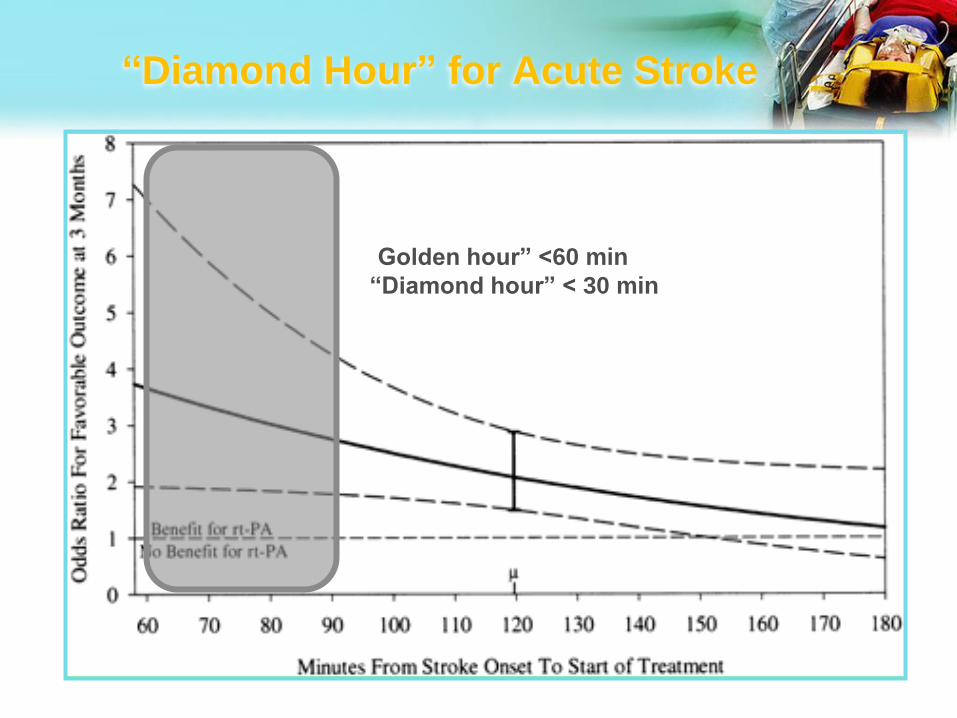
“Diamond Hour” for Acute Stroke
“Golden hour” <60 min
“Diamond hour” < 30 min

QUY TRÌNH TRƯỚC BỆNH VIỆN

VAI TRÒ CẤP CỨU TRƯỚC VIỆN
Phát hiện bệnh nhân nghi ngờ đột quỵ
Khởi động dây chuyền cấp cứu đột quỵ
Thông báo, vận chuyển bệnh nhân an toàn đến bệnh viện phù hợp.
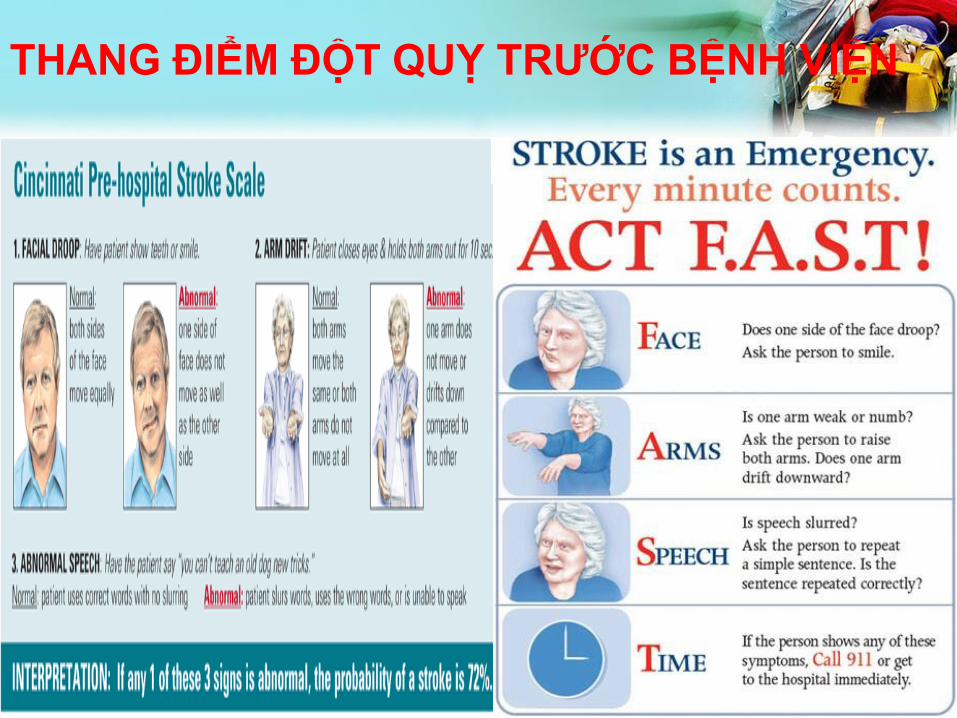
THANG ĐIỂM ĐỘT QUỴ TRƯỚC BỆNH VIỆN

SO SÁNH CÁC THANG ĐIỂM TRƯỚC BỆNH VIỆN
Adapted from Yew KS and Cheng E. Am Fam Physician 2009;80:33-40.
82%
(76 TO 88)
83%
(77 TO 89)
SENSITIVITY (95% CI) SPECIFICITY (95% CI)
≥1 ITEM: 85%
(80 TO 90)
≥1 ITEM: 79%
(73 TO 85)
FACE ARM SPEECH TEST (FAST)
STROKE SCREENING TOOL
CINCINNATI PREHOSPITAL STROKE SCREEN
(CPSS)
91%
(76 TO 98)
97%
(93 TO 99)
90%
(81 TO 96)
74%
(53 TO 88)
LOS ANGELES PREHOSPITAL STROKE
SCREEN (LAPSS)
MELBOURNE AMBULANCE STROKE SCREEN
(MASS)

VẬN CHUYỂN ĐẾN BỆNH VIỆN PHÙ HỢP

Patrik Michel, Stroke. 2017;48:247-249. DOI: 10.1161/STROKEAHA.116.015511

Stroke Ready Hospital Map

RÚT NGẮN DOOR TO NEEDLE
QUY TRÌNH TẠI BỆNH VIỆN

NINDS NIH website. Stroke proceedings. Latest update 2008.
T=0
Bn nghi ngờ
đột quỵ
cấp đến
viện
≤10 min
Đánh giá ban
đầu bởi bác sỹ
(hỏi tiền sử, xét
nghiệm & NIHSS)
≤ 15 min
Thông báo cho
nhóm đột quỵ
(gồm chuyên gia
thần kinh
≤ 25 min
Chụp hình
ảnh sọ não
≤ 45 min
Có kết quả xét
nghiệm và hình
ảnh sọ não
≤ 60 min
Dùng rt-PA
nếu có chỉ định
≤ 60 min
Từ khi
dùng thuốc
Tới khi can thiệp
MỤC TIÊU THỜI GIAN

Circ Cardiovasc Qual Outcomes. 2017
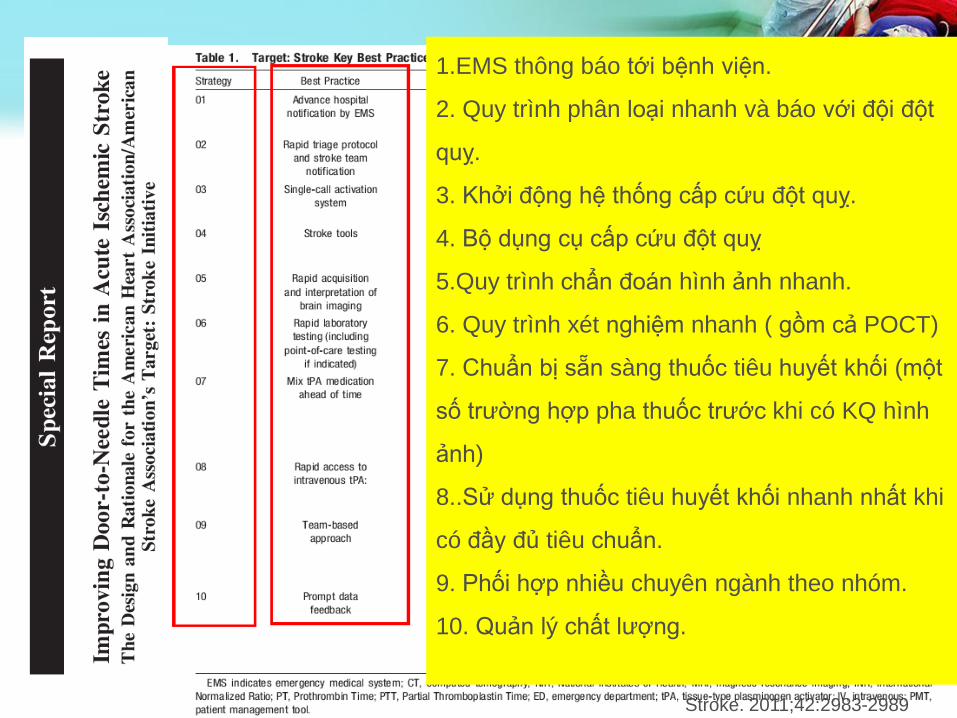
Stroke. 2011;42:2983-2989
1.EMS thông báo tới bệnh viện.
2. Quy trình phân loại nhanh và báo với đội đột
quỵ.
3. Khởi động hệ thống cấp cứu đột quỵ.
4. Bộ dụng cụ cấp cứu đột quỵ
5.Quy trình chẩn đoán hình ảnh nhanh.
6. Quy trình xét nghiệm nhanh ( gồm cả POCT)
7. Chuẩn bị sẵn sàng thuốc tiêu huyết khối (một
số trường hợp pha thuốc trước khi có KQ hình
ảnh)
8..Sử dụng thuốc tiêu huyết khối nhanh nhất khi
có đầy đủ tiêu chuẩn.
9. Phối hợp nhiều chuyên ngành theo nhóm.
10. Quản lý chất lượng.

Ying Xian et, Circ Cardiovasc Qual Outcomes. 2017
TỈ LỆ TUÂN THỦ PROTOCOL

Ying Xian et, Circ Cardiovasc Qual Outcomes. 2017
Ying Xian et, Circ Cardiovasc Qual Outcomes. 2017
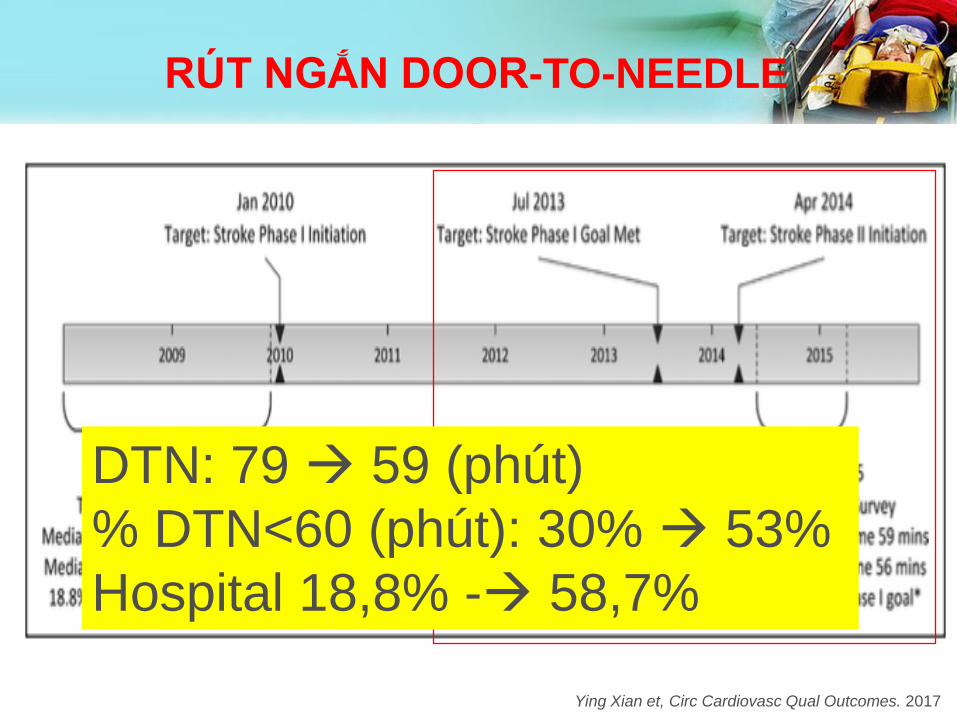
RÚT NGẮN DOOR-TO-NEEDLE
DTN: 79 59 (phút)
% DTN<60 (phút): 30% 53%
Hospital 18,8% - 58,7%
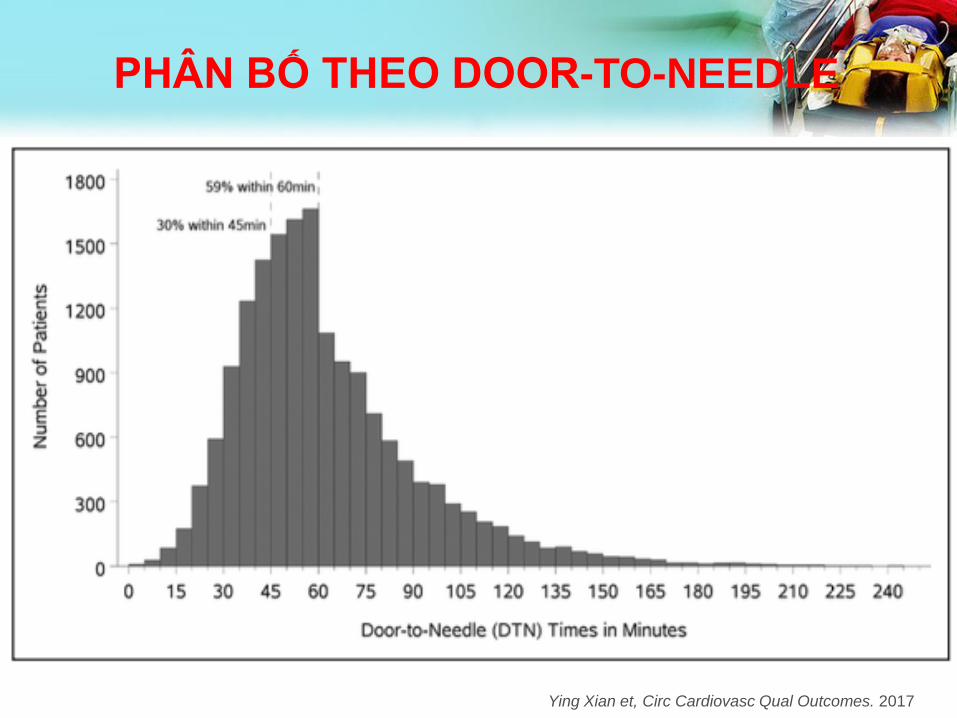
Ying Xian et, Circ Cardiovasc Qual Outcomes. 2017
PHÂN BỐ THEO DOOR-TO-NEEDLE

TỈ LỆ DOOR-TO-NEEDLE DƯỚI 60 PHÚT
JAMA. 2014;311(16):1632-1640. doi:10.1001/jama.2014.3203


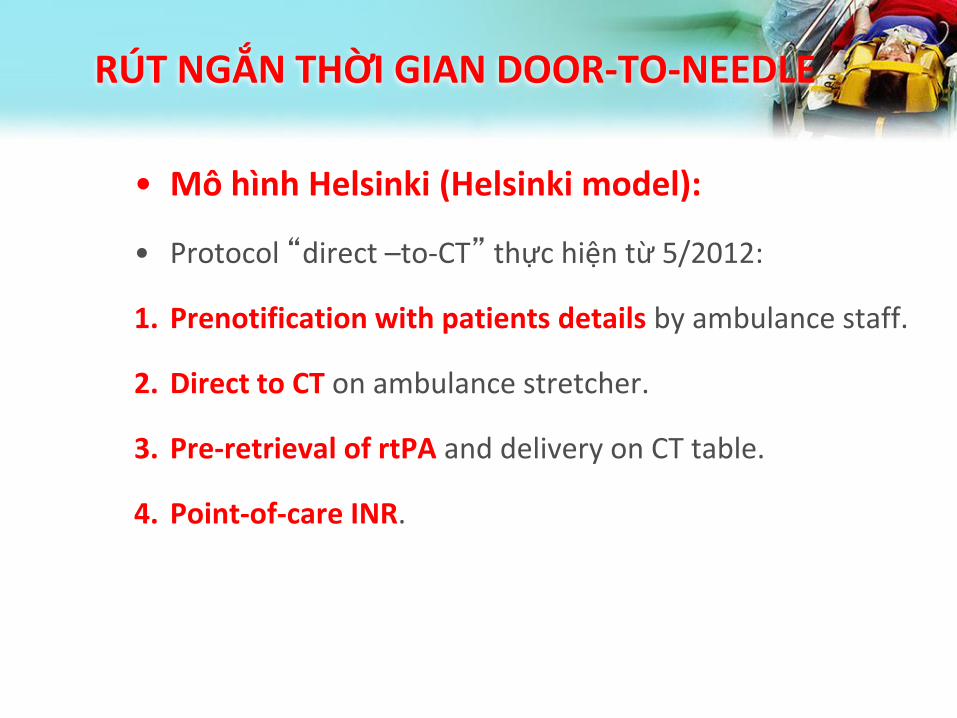
RÚT NGẮN THỜI GIAN DOOR-TO-NEEDLE
• Mô hình Helsinki (Helsinki model):
• Protocol “direct –to-CT” thực hiện từ 5/2012:
1. Prenotification with patients details by ambulance staff.
2. Direct to CT on ambulance stretcher.
3. Pre-retrieval of rtPA and delivery on CT table.
4. Point-of-care INR.

RÚT NGẮN THỜI GIAN DOOR-TO-NEEDLE


Neurology, 2013;81:1071–1076
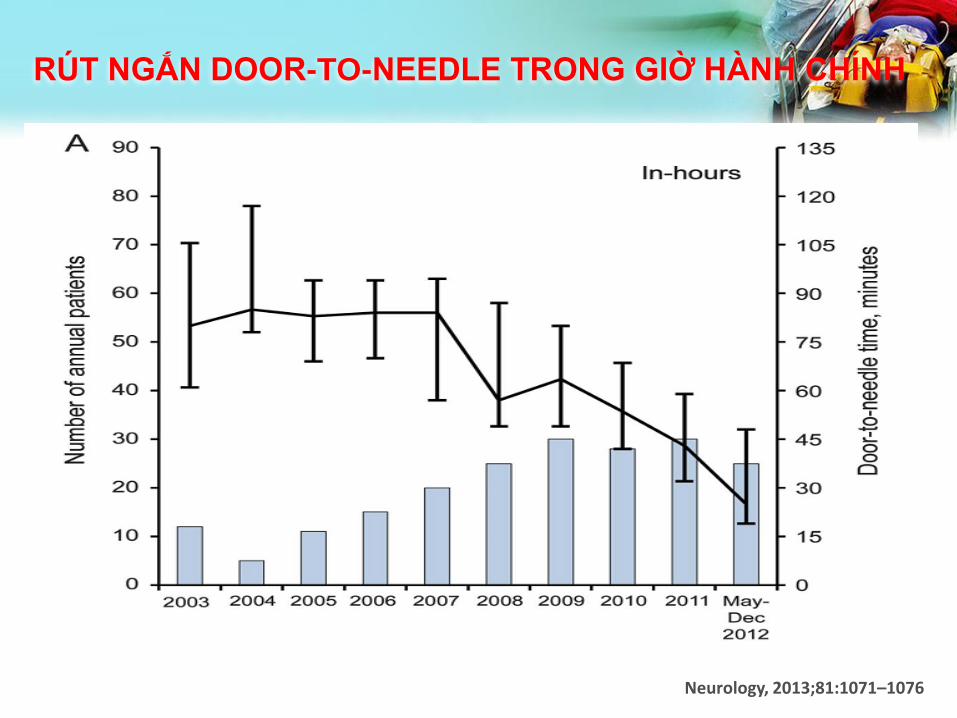
RÚT NGẮN DOOR-TO-NEEDLE TRONG GIỜ HÀNH CHÍNH
Neurology, 2013;81:1071–1076

Neurology, 2013;81:1071–1076
RÚT NGẮN DOOR-TO-NEEDLE NGOÀI GIỜ HÀNH CHÍNH

The Neurohospitalist, 2017, Vol. 7(2) 70-73

The Neurohospitalist, 2017, Vol. 7(2) 70-73

Giải pháp để giảm door to needle time
Túi cấp cứu đột quỵ:
- Chứa tất cả dụng cụ cần thiết cho BN đột
quỵ
- Cho phép BS dùng rtPA tại phòng CT
Bộ protocol, checklist:
- Checklist dành cho điều dưỡng
- Checklist dành cho bs cấp cứu
- Checklist dành cho bs đột quỵ
CÁC KHOÁ HUẤN LUYỆN
NIHSS training video
Body interact
Online
training
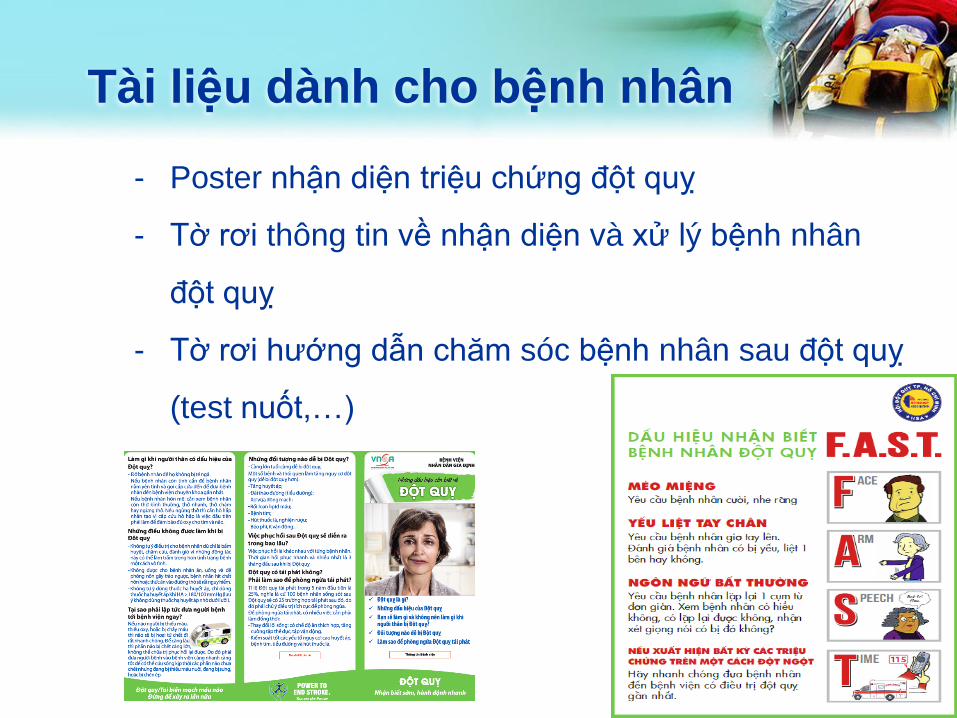
Tài liệu dành cho bệnh nhân
- Poster nhận diện triệu chứng đột quỵ
- Tờ rơi thông tin về nhận diện và xử lý bệnh nhân
đột quỵ
- Tờ rơi hướng dẫn chăm sóc bệnh nhân sau đột quỵ
(test nuốt,…)

QUẢN LÝ CHẤT LƯỢNG
Làm sao để biết chúng ta đang làm tốt?
Làm sao để biết chất lượng điều trị đột quỵ đang trở nên tốt hơn nếu chúng ta
không đo lường?

TIÊU CHUẨN CHẤT LƯỢNGTHEO ESO
1. Percent of acute stroke patients treated with intravenous thrombolysis having a door-to-needle time <60 minutes.
2. Recanalization procedure rate
3. Percent of brain imaging by CT or MRI in every suspected stroke.
4. Percent of ischemic stroke patients with antithrombotic therapy (antiplatelet medication) at discharge.
5. Corresponding antithrombotic therapy (anticoagulation) at discharge in patients with atrial fibrillation.
6. Percent of stroke unit patients screened for swallowing disorders
7. Percent of all acute patients with stroke as the predominant pathology admitted to the hospital treated on the stroke unit (or the ICU, if appropriate).
50%
5%
80%
80%
80%
80%

Registration
requirements
Registration criteria
met plus 20 patients
captured as
baseline
Registration criteria
met plus the criteria
below met for last
100 stroke patients
Registration criteria
met plus the criteria
below met for last
200 stroke patients
Registration criteria
met plus the criteria
below met for last
500 stroke patients
DTN time < 60 mins50% 75% 75%
DTN time < 45 mins50%
Recanalization
procedure rate 5% 15% 25%
% of stroke patients
that received CT or
MRI scan80% 85% 90%
% of ischemic stroke
patients with
antiplatelet therapy
at discharge
80% 85% 90%
% of ischemic stroke
patients with AF with
anticoagulation
at discharge
80% 85% 90%
% of stroke unit
patients screened for
swallowing disorders80% 85% 90%

TÓM TẮT
1. Quy trình trước viện:
– Phát hiện bệnh nhân nghi ngờ đột quỵ
– Thông báo bệnh viện phù hợp nhận bệnh
nhân
2. Quy trình tại bệnh viện:
– Rút ngắn door-to-needle time
– Quy trình “Direct to CT”.
– Quản lý chất lượng điều trị đột quỵ.

