the victorian congenital anomalies register … numbers of congenital anomalies notifications by...
TRANSCRIPT

The Victorian Congenital Anomalies Register (VCAR)
Diana Stubbs
Liaison Midwife

Statistic! Numbers of Congenital Anomalies notifications by Maternal & Child
Health Nurses
340 346
629
224
79 0
100
200
300
400
500
600
700
1999-2000 2005-06 2007-09 2013-14 2014-15
Nu
mb
ers
Years

Background
•The Victorian Perinatal Data Collection
(VPDC) collects information on all livebirths,
stillbirths and neonatal deaths where a
congenital anomaly may have been
identified.
•VPDC is responsible to the Consultative
Council on Obstetric and Paediatric Mortality
and Morbidity (CCOPMM)
•CCOPMM is the advisory body to the
Health Minister on maternal, perinatal and
paediatric morbidity and mortality

What is a Congenital Anomaly?
A ‘congenital anomaly’ is also called
•birth defect
•congenital malformation
•congenital disorder
Any abnormality of prenatal origin, either present following conception or
occurring before the end of pregnancy.
This includes structural, functional, genetic, chromosomal and biochemical
abnormalities.
These can be detected before birth, at birth, or in later years of life
What (possibly) causes a congenital anomaly? Unknown (65-75%) - polygenic, multifactorial, spontaneous errors in development, synergistic interactions of teratogens
Genetic (15-25%) eg. extra chromosome, new mutation, inherited
Environmental (10%)
* maternal conditions (4%) - alcoholism, diabetes, PKU, nutritional deficits
* infectious agents (3%) - rubella, toxoplasmosis, CMV
* mechanical problems -deformations (1-2%) - amniotic band constrictions, umbilical cord
* chemicals (<1%), drugs, radiation, hyperthermia
Brent RL. Pediatrics 2004: 113;957-968

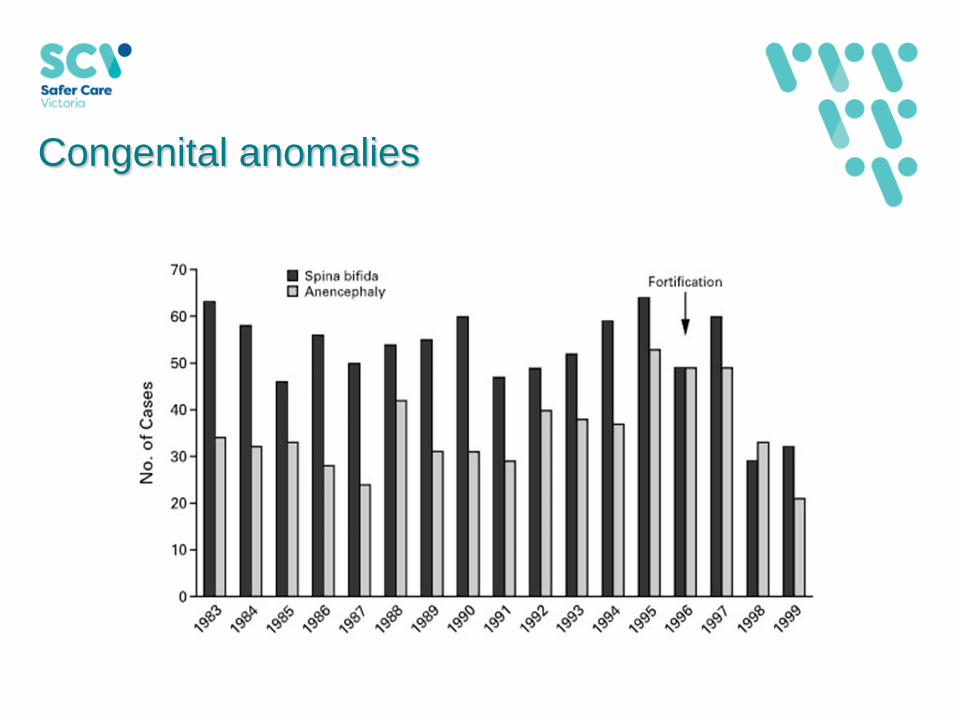
Examples of congenital anomalies collected
• Chromosomal anomalies eg. Down Syndrome
• Structural defects eg. anencephaly, missing fingers, hypospadias
• Inborn errors of metabolism eg. cystic fibrosis
• Haematological disorders eg. thalassaemia
• Congenital infections eg. CMV or rubella
• Neoplasms eg. cystic hygroma
• Developmental delay (of congenital origin only)
Why is it important to monitor congenital anomalies?
• Major cause of perinatal/infant deaths and hospitalisation
• Early diagnosis may improve chances of survival
• Correct diagnosis for counselling (e.g.. recurrence risk)
• Prevalence and survival data
(what is normal and what is abnormal)

VCAR – What do we collect?
The VCAR collects data on all congenital anomalies for:
• Live births (including neonatal deaths)
• Stillbirths
• Terminations of pregnancy
occurring since January 1, 1982 and was irrespective of age at diagnosis,
before 18 years of age.
From 2013 the scope of the collection has decreased to 6 years of age
(Reference: World Health Organization, and Centers for Disease Control and Prevention.
"Birth defects surveillance: a manual for programme managers." (2014).)

How do we collect information
Congenital Anomalies: Voluntary notification from multiple sources. All
records linked to VPDC data. Will eventually become mandatory using the
legislation in the Public Health and Wellbeing Act 2008
Terminations for malformations (before 20 weeks gestation) : separate
notification form from medical records departments at all hospitals with
maternity services

Where does the data come from?
In 2015-16:
Birth forms – All electronic (6,835) - 62.1%
Hospital sources (1,124) - 10.7%
M&CHN (79) - 0.7%
Other (19) - 0.2%
Cytogenetic reports (2898) - 26.3%
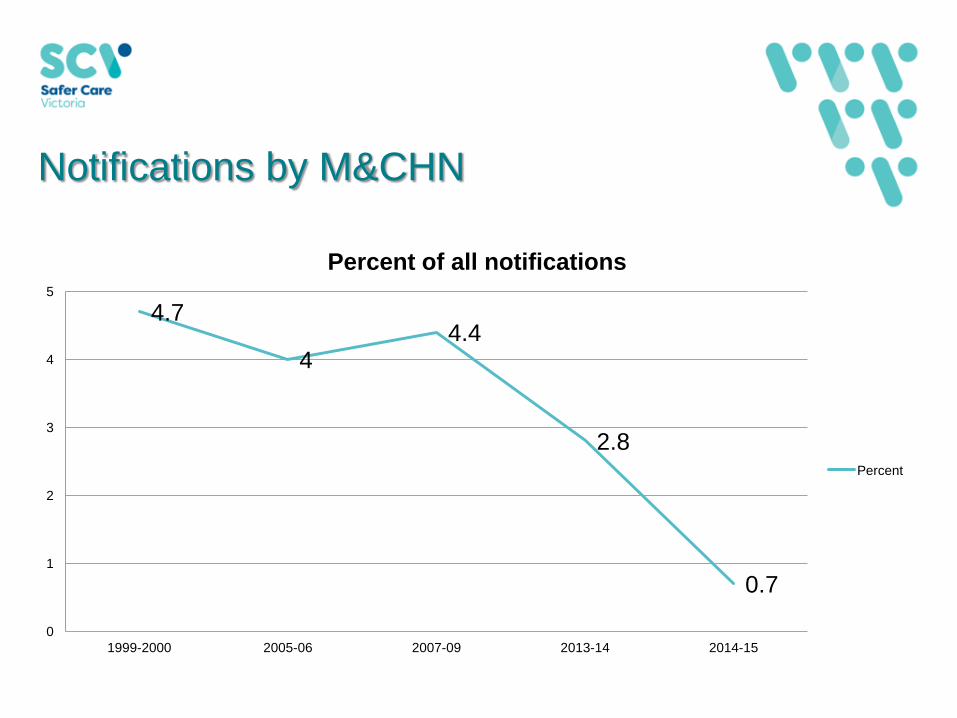
Notifications by M&CHN
4.7
4 4.4
2.8
0.7
0
1
2
3
4
5
1999-2000 2005-06 2007-09 2013-14 2014-15
Percent of all notifications
Percent

Objectives of VCAR
1. Determine how often congenital anomalies are occurring and
identify changing health service needs (prevalence and survival data).

Congenital anomalies in Victoria: 1983-2016
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
19
83
19
84
19
85
19
86
19
87
19
88
19
89
19
90
19
91
19
92
19
93
19
94
19
95
19
96
19
97
19
98
19
99
20
00
20
01
20
02
20
03
20
04
20
05
20
06
20
07
20
08
20
09
20
10
20
11
20
12
20
13
20
14
20
15
20
16
Pe
rce
nta
ge
of
se
lec
ted
pre
gn
an
cie
s
Years
Incidence of congenital anomalies from 1983 to 2016

Top Ten Congenital Anomalies: 2005-2016
2005/06 2007/09 2013/14 2015/16
Hypospadias (male) 1/135 1/123 1/234 1/190
Renal pelvis defects 1/250 1/230 1/357 1/383
Congenital Dislocation of Hip 1/364 1/332 1/579 1/823
Trisomy 21 1/339 1/297 1/803 1/331
Ventricular septal defect 1/311 1/326 1/588 1/593
Neural tube defects (comb) 1/788 1/910 1/1700 1/1831
Trisomy 18 1/1,190 1/922 1/3041 1/1294
Hydrocephalus 1/1,235 1/1,131 1/1296 1/3326
Cleft lip & palate 1/1,250 1/1,556 1/3294 1/2296
Renal agenesis/dysgenesis 1/1,471 1/1,556 1/2166 1/2547

Prevalence of T21 per 1000 pregnancies 1998-2016
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
Congenital anomalies
Congenital anomalies
0
0.5
1
1.5
2
2.5
0.0
0.5
1.0
1.5
2.0
2.5
Rat
e p
er 1
,000
pre
gnan
cies
Year
Victoria
Expected
Linear (Victoria)
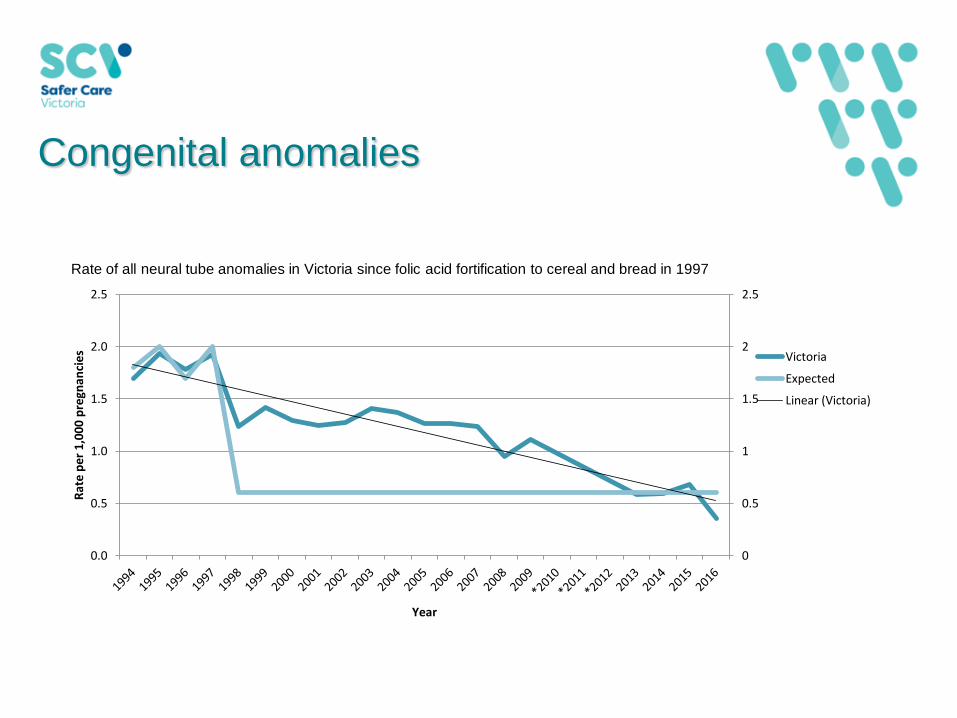
Rate of all neural tube anomalies in Victoria since folic acid fortification to cereal and bread in 1997
Notifying us
Notification Form.
Complete form online:
https://hnb.dhs.vic.gov.au/eForms/eForms.nsf/FormsForPreview/
3E5F862A69543DB5CA25768E001B5352?OpenDocument

Objectives of VCAR
2. Respond to requests for data from:
One of our many functions is to respond to data requests from people
involved in research and service provision.
Organisations responsible for planning and providing health care
facilities for those with congenital anomalies, or who provide
information to those concerned about having a baby with a congenital
anomaly
Requests for unpublished information should complete a ‘Request for data’ form at this link from our homepage:
https://hnb.dhs.vic.gov.au/eForms/eForms.nsf/FormsForPreview/3E5F862A69543DB5CA25768E001B535
2?OpenDocument
What do we do with the data?
3. Provide information through epidemiological research to increase
knowledge of aetiology and preventability of congenital anomalies
Research involving ART Increased risk of congenital anomalies, arising in the first 4 weeks of pregnancy, (blastogenesis ) after assisted reproductive technologies
BACKGROUND The reasons for increased congenital anomalies prevalence
following in-vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI) are
largely unknown.
Classification of congenital anomalies by pathology rather than organ system, and
examination of the role of embryo freezing and thawing may provide clues to the
mechanisms involved. This study aimed to investigate these two factors.
METHOD Data on 6946 IVF or ICSI singleton pregnancies were linked to perinatal
outcomes obtained from population-based data sets on births and congenital
anomalies occurring between 1991 and 2004 in Victoria, Australia. These were
compared with 20, 838 outcomes for singleton births in the same population,
conceived without IVF or ICSI. Congenital anomalies were classified according to
pathogenesis. (Haliday JL et al. Human reproduction. 2009 Oct 22:dep364.)

Research involving ART There was no strong evidence of risk differences between IVF and ICSI or
between fresh and thawed embryo transfer.
However, a specific group, blastogenesis congenital anomalies, were
markedly increased [adjusted OR 2.80, 95% CI: 1.63–4.81], with the increase
relative to the controls being significant for fresh embryo transfer (adjusted
OR 3.65; 95% CI: 2.02–6.59) but not for thawed embryo transfer (adjusted OR
1.60; 95% CI: 0.69–3.69).
CONCLUSION Our findings suggest that there is a specific risk of
blastogenesis congenital anomalies arising very early in pregnancy after
IVF or ICSI and that this risk may be lower with use of frozen-thawed
embryo transfer.

Beckwith-Wiedemann syndrome
1 in 15,000 - 1 in 70,000
Macroglossia
Pre/post natal overgrowth
Anterior abdominal wall defects
Neonatal hypoglycaemia
Ear pits/creases hemihypertrophy
Facial naeveus flammeus
Increased risk of abdominal tumours
IVF and Beckwith-Wiedemann syndrome
Aim: to determine whether there is an association between this congenital anomaly (a rare genetic overgrowth condition) and IVF
Method:All BWS children (cases) between 1983-2001, plus 4 controls per case from PDCU - record linkage to IVF databases
3% of births conceived by IVF in 2003, c/w 0.2% in 1983
Ethics approval from 6 organisations

Results
4/37 cases conceived by IVF = 10.8%
1/148 controls = 0.7%*
*0.7% average of 0.2% having IVF in 1983 to 3.0% in 2003
matched analysis (maternal age and baby date of birth)
Odds ratio = 16 (95% CI 1.8 - 143.1)
p value = 0.013

Objectives of VCAR
4. Assess effectiveness of primary prevention and screening for
congenital anomalies.

Role of the MCH Nurse in Notifying Defects to VCAR
Notify any congenital anomalies that are detected after the first week of life (eg cardiac anomalies).
Notify anomalies that may not have been reported from the hospital of birth.
Notify anomalies which may not require hospitalisation, but are treated by private paediatricians.
ie. Notify us of any children
you see in your Centre
with a Congenital Anomaly.
DON’T assume we already know about them

Practical Concerns for notifiers
Informing parents (beyond the perinatal period):
• If a parent objects
• Encourage the parent to ring the VCAR – 9096 2729
• Notify us with no names recorded but include: mother’s birthdate,
postcode, baby’s birth date, sex and birth anomaly.
Practical Concerns for notifiers
What to notify
Every suspected congenital anomaly

Practical Concerns for notifiers
If you suspect a cluster in your area contact the VPDC
either by phone and/or in writing. The Consultant
Epidemiologist will contact you to ascertain details, and to
undertake initial investigation, if it is warranted.

Publications CCOPMM Annual report 2015-2016
https://bettersafercare.vic.gov.au/reports-and-publications/victorian-perinatal-services-performance-indicators-2016-2017
Victorian Perinatal Services Performance Indicators Report 2015-2016
https://bettersafercare.vic.gov.au/reports-and-publications/victorian-perinatal-services-performance-indicators-reports
Koori Health counts: Koori Births in Victoria 2011-2012
https://www2.health.vic.gov.au/about/publications/data/Koori%20Health%20Counts%20201213
Congenital Anomalies in Victoria 2015-2016
https://bettersafercare.vic.gov.au/reports-and-publications/congenital-anomalies-in-victoria-2015-2016
Summary
•The VPDC collects data on all births, congenital anomalies and
deaths in Victoria - separate linked databases
•Confidentiality of individual persons and hospital sites assured
under the Public Health and Wellbeing Act 2008
•Congenital anomaly data collection requires major input from
midwives and M&CHN’s
•There are many ways in which the data is used - over and above
the public health aspects of routine monitoring and surveillance

Thank-you
https://bettersafercare.vic.gov.au/about-us/about-scv/councils/ccopmm