the sequence of sleep stages€¦ · web viewanother factor that affects sleep is a group of...
TRANSCRIPT

Individual Behaviour:
Sleep, Dreams and Disorders
On any normal day of our lives, each of us engages in two very distinct kinds of behaviours: sleeping and being awake. We all need and experience sleep We sleep up to a third of our lives We devote a third of our houses to sleep We all dream even if we don’t always remember
ConsciousnessThe main difference between being awake and being asleep is that in sleep, consciousness does not intervene. When you’re asleep it’s somewhat as if your brain were closing itself off and becoming a sort of “temporary autonomous zone”. In reality your brain is never completely cut off from the rest of the world even during the deepest stages of sleep. A strong enough stimulus from your environment will be perceived by your brain and cause you to wake up e.g. a baby crying. So sleep is a period of brain activity where external stimuli are not thoroughly attended to.
Why do we sleep? Think about this question for a moment and write down as many possible explanations as possible.
During this topic you will need to use three different approaches to explain sleep, dreams and disorders. We will consider the biological, cognitive and psychodynamic approaches.
Identify the main ideas/assumptions of each approach Which psychologists are associated with each approach? How do you think each approach would explain sleep? Why
would we need sleep according to each approach?
2
The Biological Approach to Sleep & Dreams
The nervous system & brain areasAs in other areas of psychology, the biological approach explains sleep and dreams in terms of which brain areas control behaviour.
The brain in general is directly in control of sleep. During the day, a chemical called adenosine builds up in our brain’s neurons as a natural by-product. When we sleep, this build-up is cleared, and the adenosine is replaced by energy in the form of glycogen. Evidence supporting this view is the fact that the stimulant drug caffeine blocks adenosine receptors, making the body less responsive to the build-up of adenosine, and reducing the feelings of tiredness.
Biological psychologists have identified particular areas of the brain that control circadian rhythms. The hypothalamus is responsible for homeostasis (your body trying to maintain a balance as described in the previous paragraph) and it contains an area called the superchiasmatic nucleus (SCN) that controls our circadian rhythms.
This approach also explains dreams biologically. Rather than look up the meaning of dreams, the biological approach thinks that dreams largely result from random brain activity during sleep and are therefore meaningless.
EvaluationThe explanation of sleep in terms of hormones and the brain is supported by studies of other animals. Even though sleep patterns vary between species, melatonin appears to play a key role among all vertebrates.
However, the biological approach is limited. The explanation of dreaming is particularly limited. Although the activation synthesis theory has been influential, many do not find the idea that our dreams are meaningless very satisfying. The theory struggles to explain some major facts such as that 70% of dreams make sense and that experiences from the previous day tend to appear during dreams.
The reductionist nature of the biological approach is oversimplified in that we can’t obtain a complete understanding of human behaviour by focusing only on biological factors. For example, various psychological, social and cultural factors influence the development of mental disorders such as depression and stress, and these factors are ignored within the biological approach. These factors may affect sleep.
3

Circadian Rhythms
All species have a timing mechanism, or internal body 'clock,' that controls periods of activity and inactivity across a day, a season or a year. These clocks can produce a circadian rhythm that fluctuates on a roughly 24-hour timetable. Sleep is part of a circadian rhythm.
circa = aboutdia = day
circadian = about one day
While many people refer to circadian rhythms as a single process, there are actually a number of body activities that oscillate throughout the day. For example, mental alertness tends to peak twice in a day but at different times to peak physical strength.
How Does Your Body "Keep Time?"Information from your eyes needs to get to the back of your brain. Part of the optic nerve from each eye crosses over to the other side of the head. This crossing-over point is called a chiasma. This happens almost in the centre of your head above the hypothalamus. In the hypothalamus is a cluster (nucleus) of about 20,000 neurons called the suprachiasmatic nucleus (SCN).
Supra = under Chiasma = crossing point
Nucleus = cluster of brain cells
The SCN is the main controller of many circadian rhythms and acts like an internal pacemaker. Changes in the environment are assessed by the brain and used to re-set the biological clock. Environmental cues like day length are important. Without these zeitgebers (“time-givers”) the body cannot entrain (re-correct) itself properly to the day-night cycle. When are you likely to face this sort of problem?
So how does a zeitgeber like sunlight affect your circadian rhythms? As the sunlight decreases at the close of the day, the visual system sends signals to the suprachiasmatic nucleus. Next, the SCN sends signals to the pineal gland further back in the brain to increase the production of the hormone melatonin. This hormone increase helps reduced activity and makes you feel increasingly sleepy.
ZeitgebersAnother factor that affects sleep is a group of environmental triggers called zeitgebers. The word is German for ‘time-giver’; it refers to environmental signals that affect our circadian rhythms and make our brain think that it is time to sleep or wake up. In our evolutionary past, we would start to feel sleepy as the day got late and it got darker. Light and darkness are both zeitgebers, telling our brain that it is time to sleep or wake up. Nowadays, of course, we use artificial lights and often stay awake (or get up) when it is dark outside.
4

Recently, researchers have realised that artificial light can disturb our circadian rhythms and affect the quality of sleep. In particular, light from some low-energy lightbulbs and screens contain a large proportion of blue wavelengths of light that have a strong effect in supressing sleep. In particular, they can supress the production of sleep hormones such as melatonin.
MYTH: TEENAGERS LOVE LYING IN BED A common assumption is that teenagers are lazy, moody and unmotivated to get out of bed in the morning. Carskadon et al (1983, 1997) showed real biological factors explain these types of behaviour. During puberty, a 2-3 hours delay occurs in the circadian rhythms and children of this age, particularly males, gradually shift their activity to 2-3 hours later than their parents. They still want a good night’s sleep of 9 hours but need to get up for school and so can be tired during the day.
5

What Happens When There is No Sunlight?When exposed to environmental sunlight signals which are zeitgebers, many of the body's rhythms operate on a very similar schedule. When all natural light cues are removed, these body clocks begin to operate on their own schedule. Siffre (1975) spent 6 months underground with no cues as to time. His circadian rhythm extended to 25hrs. This suggests that zeitgebers keep us entrained to a 24hr day-night cycle by resetting our SCN that would otherwise free-wheel for 25hrs.
Individuals who are blind from birth frequently have difficulty with their sleep-wake cycle because of the complete lack of environmental light cues. Why is this? How will they cope and entrain their internal body clocks?
Points to Remember: Your circadian rhythms are tied to environmental cues like sunlight called
zeitgebers. Disrupting these patterns can lead to poor or difficult sleep. Without light signals, people tend to operate on a 25-hour schedule. Circadian rhythms also impact body temperature, pain sensitivity, mental alertness,
physical strength, and the senses.
MYTH: EVERYONE NEEDS 8 HOURS SLEEP A NIGHT We’re not all the same when it come to the amount of sleep we need in order to function optimally the next day. About 10% of the adult population needs much more sleep a night than the average 7-8 hours. Around 5% of the population can get along fine with only 5 or 6 hours of sleep. There is no particular amount of sleep that is ideal in itself. The only criterion for whether you’re getting enough sleep is whether you feel in good shape during the day.
Sleep requirements also vary over our lifespan.
Stage Age Average amount of sleep
New-born 0 to 2 months 12 to 18 hoursInfants 3 to 11 months 14 to 15 hours
Toddlers 1 to 3 years 12 to 14 hoursPre-schoolers 3 to 5 years 11 to 13 hours
School children 5 to 10 years 10 to 11 hoursAdolescents 10 to 17 years 8.5 to 9.5 hours
Adults & elderly 17+ years 7 to 9 hoursPregnant women 8 + hours
People sleep less than they used to in the past. This is due in part to electrical lighting, which makes it easy to increase the number of hours of available light. What would this do to the brain?
6

People sleep less than they used to in the past. This is also due to the increasing emphasis placed on productivity-related values across the last century.
Factors that Affect Sleep:
DrugsOne factor that can affect sleep is the use of recreational or prescription drugs. Stimulant drugs have the effect of making people more alert or keeping them awake and can reduce the quality of sleep. One example of a stimulant is caffeine. This is the world’s most popular psychoactive drug and it is present in food and drinks such as coffee, tea, chocolate and most energy drinks. It can also be in tablet form. People drink coffee to keep them alert, but taking it in the evening can make it harder to get to sleep. Many people don’t realise that it can take over 5 hours for the level of caffeine in the blood just to drop to half of the level it was at after taking caffeine (Statland & Demas, 1980). Amphetamine (often called ‘speed’) is another stimulant – although it is a class B illegal drug, it is widely used for socialising and by some workers on long overnight shifts.
Alcohol can also affect sleep – usually making people feel sleepier. Many people like to drink alcohol in the evenings to help them get to sleep, which changes the proportions of REM and NREM sleep. However, tolerance to alcohol develops quickly, resulting in normal patterns of sleep for healthy people consuming moderate amounts of alcohol (Roehrs & Roth, 2001). Therefore, it is unlikely to be of any long-term use in treating insomnia.
Prescription drugs can interfere with sleep patterns as an undesired side effect, either by making it harder for us to sleep or by making us drowsy. Some drugs such as anti-histamines (taken for allergies) come in ‘non-drowsy’ versions.
LightWhile light of any kind can suppress the secretion of melatonin, blue light does so more powerfully. Harvard researchers and their colleagues conducted an experiment comparing the effects of 6.5 hours of exposure to blue light to exposure to green light
Activities
1. What does the term “circadian rhythm” translate as?2. Explain what a circadian rhythm is.3. What are zeitgebers? Give an example of one.4. How are circadian rhythms related to light cues, and melatonin secretion?5. Explain the myth of the lazy teenagers and how this links to their circadian
rhythms.6. What research was conducted by Siffre and what did he find?7. Draw your own circadian rhythm clock. Use the picture on page 4 to help you.
Take a full page in your notes to complete this.8. Look at the figures and see if you can explain the different sleep requirements
for different people.9. What age group(s) need the most sleep? Suggest an explanation for this.10.Why do people sleep less now than they did in the past?
7

of comparable brightness. The blue light suppressed melatonin for about twice as long as the green light and shifted circadian rhythms by twice as much (3 hours vs. 1.5 hours).
Use dim red lights for night lights. Red light has the least power to shift circadian rhythm and suppress melatonin.
Avoid looking at bright screens beginning two to three hours before bed. If you work a night shift or use a lot of electronic devices at night, consider
wearing blue-blocking glasses. Expose yourself to lots of bright light during the day, which will boost your ability
to sleep at night, as well as your mood and alertness during daylight.
Stages of Sleep
Most people have an idea about different kinds of sleep – for example shallow sleep, when you’re just waking up, and deep sleep, when you feel groggy. However most people won’t know that there are 4 distinct stages to sleep and just to complicate things, sleep does not progress through these stages in sequence!
Sleep begins in stage 1 and progresses into stages 2, 3 and 4. After stage 4 sleep, stage 3 and then stage 2 sleep are repeated before entering rapid eye movement (REM) sleep. Once REM sleep is over, the body usually returns to stage 2 sleep. Sleep cycles through these stages approximately four or five times throughout the night.
8

On average, we enter the REM stage approximately 90 minutes after falling asleep. The first cycle of REM sleep might last only a short amount of time, but each cycle becomes longer. REM sleep can last up to an hour.
Stage 1:Stage 1 is the beginning of the sleep cycle, and is a relatively light stage of sleep. Stage 1 can be considered a transition period between wakefulness and sleep. In Stage 1, the brain produces high amplitude theta waves, which are very slow brain waves. This period of sleep lasts only a brief time (around 5-10 minutes). If you awaken someone during this stage, they might report that they weren't really asleep.
Stage 2:Stage 2 is the second stage of sleep and lasts for approximately 20 minutes. The brain begins to produce bursts of rapid, rhythmic brain wave activity known as sleep spindles. Body temperature starts to decrease and heart rate begins to slow.
Stage 3:Deep, slow brain waves known as delta waves begin to emerge during stage 3 sleep. Stage 3 is a transitional period between light sleep and a very deep sleep.
Stage 4:Stage 4 is sometimes referred to as delta sleep because of the slow brain waves known as delta waves that occur during this time. Stage 4 is a deep sleep that lasts for approximately 30 minutes. Bed-wetting and sleepwalking are most likely to occur at the end of stage 4 sleep.
Stage 5 – REM (Rapid Eye Movement)Most dreaming occurs about an hour after we fall asleep during the fifth stage of sleep, known as rapid eye movement (REM) sleep. Dreaming occurs during REM sleep and is characterized by the rapid and random movement of the eyes as well as increased respiration rate and increased brain activity. We have around three to five REM episodes a night. REM sleep is also referred to as paradoxical sleep because while the brain and other body systems become more active, muscles become more relaxed. Dreaming occurs due because of increased brain activity, but voluntary muscles become paralysed. REM sleep in adult humans typically occupies 20-25% of total sleep, about 90-120 minutes of a night’s sleep. A new-born baby spends almost 9 hours a day in REM sleep. By the age of five or so, only slightly over two hours is spent in REM.
Regardless of whether people sleep 6 hours or 10 hours sleep per night, they all get about the same amount of deep non-REM sleep about 100 mins. People with more total hours sleep each night devote some of the extra time to REM sleep, but more of it to light non-REM sleep. Thus people who sleep less might be said to have a higher concentration of deep non-REM sleep than people who sleep more.
On average, we enter the REM stage approximately 90 minutes after falling asleep. Sleep cycles through the 5 stages approximately four or five times throughout the night with increasing REM duration up to an hour.
Quick summary of Non-REM sleep
Occurs at the beginning of the sleep cycle and the first stage of sleep cycle is a relatively light stage of sleep lasting approximately 5-10 minutes.
9

Stage 2 of the sleep cycle and lasts for approximately 20 minutes. The brain begins to produce bursts of activity known as sleep spindles.
Stage 3 of non-REM sleep is a transition between light and deep sleep. Stage 4 is a deep sleep when sleepwalking or bedwetting is most likely to occur.
The brain produces very slow brain waves known as theta waves and heart rate slows and body temperature drops.
The graph below shows the brain activity that a person experiences during their full cycle of sleep. These brainwaves are created using an EEG machine.
The diagram below shows a hypnogram for the average night’s sleep. Activities:
1. Outline what happens at each of the stages of sleep.
2. What happens after you go through stages 1-4 in the sleep pattern?
3. After REM sleep is over, what usually happens to the body?
4. How long does it usually take before entering the REM stage after falling asleep?
5. How long can REM sleep last?
6. Taking each of the stages of sleep, draw your own diagram to explain the process and stages.
7. What most surprises you about the different stages of sleep?
10

Measuring Sleep Activity & Studying Sleep
Experiments Polysomnography (PSG) Electroencephalogram (EEG) Questionnaires Observations
Nerve cells operate by sending electrical impulses. These small voltages can be detected using electrodes on the skin as an EEG.
An Electroencephalogram (EEG) produces a hypnogram (sleep picture) of your brain waves. With computer developments and the addition of information about eye movement under the eye lid and muscle tone, especially from the jaw muscles, the EEG is now part of Polysomnography (PSG). This is a comprehensive recording of the biophysiological changes that occur during sleep used in the study of sleep and as a diagnostic tool in sleep medicine.
This is an EEG.
1. Outline what happens at each of the stages of sleep.
2. What happens after you go through stages 1-4 in the sleep pattern?
3. After REM sleep is over, what usually happens to the body?
4. How long does it usually take before entering the REM stage after falling asleep?
5. How long can REM sleep last?
6. Taking each of the stages of sleep, draw your own diagram to explain the process and stages.
7. What most surprises you about the different stages of sleep?
11

To better visualise general patterns, researchers use a type of graph called a hypnogram. This is a minute by minute graphic record of a night’s sleep, as captured by an EEG. The hypnogram thus shows not only the sequence in which the various stages of sleep occur, but also the times at which each stage starts and ends.
If we analyse a typical hypnogram such as the one shown below, we see a few minutes after falling asleep, we slip deeper and deeper into non REM sleep, first into light non REM sleep (stages 1 and 2) and then into deep non-REM sleep (stages 3 and 4)
Polysomnography (PSG) a type of sleep study, is a multi-parametric test used in the study of sleep and as a diagnostic tool in sleep medicine. The test result is called a polysomnogram, also abbreviated PSG. Polysomnography is a comprehensive recording of the biophysiological changes that occur during sleep. It is usually performed
at night, when most people sleep, though some labs can accommodate shift workers and people with circadian rhythm sleep disorders, and do the test at other times of day. The PSG monitors many body functions including brain (EEG) eye movements (EOG), muscle activity or skeletal muscle activation (EMG) and heart rhythm (ECG) during sleep.
Activities:
1. What type of graph measures sleep patterns?2. What does this graph tell us about sleep?3. Outline which body functions a PSG measures4. What is polysomnography used for?5. Explain how polysomnography works6. What is the advantage of a home study?
12

Restoration Theory of Sleep
According to the Restoration theory of sleep (Oswald 1966), sleeping is essential for revitalising and restoring the physiological processes that keep the body and mind healthy and properly functioning after the day’s activities.
Restoration of the body Restoration of the brainBody can carry out repairs to cells during sleep Gives the brain a restSleep restores resources of energy Restores supplies of neurotransmittersSleep aids the removal of waste chemicals built up during the day
Restores supplies of brain proteins
This theory suggests that NREM sleep is important for restoring physiological functions, while REM sleep is essential in restoring mental functions. This is supported by the fact that new-born babies have a high proportion of REM sleep, where it makes up 50 to 60 percent of sleep time, gradually falling to the normal proportion of about 25 percent as the child grows. The month before and after birth are a time of rapid brain growth and development so that, if REM is a time when such processes occur, it is logical that the baby should show increased REM sleep. Support for this theory is provided by research that shows periods of REM sleep increase following periods of sleep deprivation and strenuous physical activity. During sleep, the body also increases its rate of cell division and protein synthesis, further suggesting that repair and restoration occurs during sleeping periods.
Sleep deprivation affects the immune system. Zager et al (2007) deprived rats of sleep for 24 hours. When compared with a control group, the blood tests of sleep-deprived rats indicated a 20% decrease in white blood cell count, a significant change in the immune system. Rats kept awake indefinitely develop skin lesions, loss of body mass, hypothermia and eventually, fatal sepsis when the body overreacts to an infection. Sleep loss impairs immune function and immune challenge alters sleep.
Evidence:The restoration theory found support from Shapiro et al (1981), in a study of runners. After an ultramarathon, it was found that their sleep lasted on average 90 minutes longer than usual over the next two nights. In particular, NREM sleep lengthened, rising from 25% to 45% of total sleep.
However, Horne (1978) reported that sleep deprivation did not interfere with participants’ ability to play sports or make them ill. It seems that sleep is not essential for physical functioning, at least in the short term.
Horne and Harley (1988) believed that a warming of the brain during exercise led to longer sleep in the Shapiro study, not wear and tear to the body. To test this, they heated people’s faces and heads using a hairdryer! Four out of the six participants were then found to have a longer period of NREM sleep. Their finding goes against the idea that sleep is needed to repair the body – but it could be repair of the brain that is the key function. Alternatively, perhaps some daytime activities such as exercise interfere with brain functions and the brain then needs to catch up on these during the day.
EvaluationEvidence seems to be growing that sleep is more important to restoration of the brain than the body, but this debate has not yet been fully resolved. It is clear that sleeping too little in humans seems to result in poorer performance (Peter Tripp). This supports restoration theory.
Sleep probably has multiple functions, and REM sleep and NREM sleep may have different functions. Therefore it is probably over-simplistic to suggest that sleep is just about restoration but this may well be one of the main functions of NREM sleep.
Hobson (2005) disagrees with the restoration theory. He states that sleep is entirely for the brain, noting that bodily restoration could be achieved by simply resting.
13

Sleep Deprivation
We all know how awful we feel when we have been deprived of sleep. Although there may be medical or environmental reasons why we don’t get enough sleep, like snoring or noisy neighbours, the main cause of sleep deprivation is most likely self-inflicted - staying up too late! Researchers in America analysed data from more than one million people in 2002, and found that getting less than 6 hours sleep a night was associated with an early death – as was getting over eight hours.
Studies on ratsRechtshaffen et al (1989) deprived rats of either REM or both REM and Non REM sleep. After a week of total deprivation they lost weight despite eating more. After 2 weeks they lost considerably more weight. After 4 weeks they died. During these 4 weeks body weight plummeted, despite increased food, and body temperature became more unstable.
Studies on HumansHowever humans do not seem to experience such marked changes in blood pressure, heart and breathing rates and body temperature, even when deprivation is for up to 200 hours. Webb and Bonnet (1979) limited participants to 2 hours sleep on one night and found they suffered no ill effects. They did however fall asleep more quickly and slept for longer than usual. Longer periods of sleep deprivation are more serious, yet people do not die like rats. Webb and Bonnet gradually reduced participants’ sleep from 8-4 hours a night over a 2 month period with no serious consequences.
Overall sleep deprivation has been found to have the following effects:
Memory & attention problems A weakening of your immune system Increased risk of motor vehicle accidents Increase in BMI (increased risk of obesity due to increased appetite) Increased risk of diabetes & heart problems Increased risk for depression & substance abuse
REM reboundWhen sleep is abruptly reduced, as is often the case for people switching between day and night shift, there are very marked effects. These include intense fatigue, being irritable, and being intellectually inefficient. The following night an interesting thing happens – there is an increase in REM sleep to compensate for the loss. This is called REM rebound. When volunteers have reduced sleep over a longer period of time they tend to fall more quickly into REM sleep and reduce the amount of Non REM sleep between their dreams. When sleep is abruptly reduced there is no time to adopt this new pattern.
Activities
1. Make a list of the ways that sleep deprivation affects you in class. You may even be experiencing these symptoms right now!
2. Ethics alert! How do you think the researchers kept rats awake for up to 4 weeks? Do you think this experiment is morally justified?
3. What happens to rats who are deprived of sleep after 2 weeks? What happens after 4 weeks?4. When humans are deprived of sleep gradually what are the consequences?5. What happens to humans if sleep is abruptly reduced in a shorter period of time?6. Describe the phenomena of REM rebound in your own words.
14

Human Case Studies of Sleep Deprivation
1. Peter Tripp
Peter Tripp was a Top 40 radio personality from the mid-1950s, whose career peaked with his 1959 record breaking 201 hour wakeathon (working on the radio non-stop without sleep to benefit the March of the Dimes). For much of the stunt, he sat in a glass booth in Times Square. After a few days he began to hallucinate, and for the last 66 hours the observing scientists and doctors gave him drugs to help him stay awake. He was broadcasting in New York City at the time. Tripp suffered psychologically, after the stunt, he began to think he was an imposter of himself, and kept that thought for some time.
His career soon suffered a massive downturn when he was involved in a scandal of 1960. Like several other disc jockeys he had been playing particular records in return for gifts from record companies. Indicted only weeks after his stunt, it emerged that he had accepted $36,050 in bribes. Despite his claims of innocence, he was found guilty on a charge of commercial bribery, receiving a $500 fine and a six-month suspended sentence.
Tripp suffered significantly both physically and cognitively during his period of wakefulness. His wife reported that he never fully recovered following the event and his personality changed permanently. This case study is evidence which supports restoration theory – without sleep we will suffer physically and mentally as we are not given the opportunity to restore.
2. Randy Gardner
Randy Gardner is the holder of the record for the scientifically documented longest period sleep deprivation without use of stimulants of any kind. In 1964, Gardner, a 17-year-old high school student in San Diego, California stayed awake for 264.4 hours (11 days 24 minutes). Gardner's record attempt was monitored by Stanford sleep researcher Dr William Dement, and a log was kept by two classmates from Point Loma High.
Gardner's experiment is often used to demonstrate that extreme sleep deprivation has little effect, other than the mood changes associated with tiredness. For example, researcher William Dement stated that on the tenth day of the experiment, Gardner had been, among other things, able to beat Dement at pinball. However, there were reported serious cognitive and behavioural changes. These included moodiness, problems with concentration and short term memory, paranoia and hallucinations. On the eleventh day, when he was asked to subtract seven repeatedly, starting with 100, he stopped at 65. When asked why he had stopped, he replied that he had forgotten what he was doing.
On his final day, Gardner presided over a press conference where he spoke without slurring or stumbling his words and in general appeared to be in excellent health.
Gardner slept 14 hours and 40 minutes, awoke naturally around 8:40 p.m., and stayed awake until about 7:30 p.m. the next day, when he slept an additional ten and a half hours. Gardner appeared to fully recover from his loss of sleep, with follow up sleep recordings taken one, six, and ten weeks after the fact showing no significant differences. No long term psychological or physical effects have been observed.
This case study does not support restoration theory – Gardner suffered very few physical side effects from his period of sleep deprivation and returned to normal following a period of sleep.
15

Evolutionary Theory of Sleep
EcologyEnergy has to be obtained by feeding but this behaviour puts the animal at risk of predation. Sleep keeps an animal unobtrusive when other behaviour is not possible. It reduces energy output and risk.
The Indus river dolphin lives in fast-flowing freshwater with a high load due to mountain run-off. Prolonged sleep would be impossible as this mammal would drown or be struck by floating debris. Instead the dolphin sleeps for seconds at a time throughout the whole day. The Bottlenose dolphin sleeps with only one hemisphere of the brain at a time for stretches of 2 hours, alternating throughout a 12 hour night.
Energy ConservationEvolutionary theory suggests that periods of activity and inactivity evolved as a means of conserving energy. According to this theory, all species have adapted to sleep during periods of time when wakefulness would be the most hazardous.
Support for this theory comes from comparative research of different animal species. Animals that have few natural predators, such as bears and lions, often sleep between 12 to 15 hours each day. On the other hand, animals that have many natural predators have only short periods of sleep, usually getting no more than 4 or 5 hours of sleep each day. Cattle which have many natural predators sleep very little. Predators tend to sleep more than their prey species but this is a consequence of a high energy diet of proteins and fats rather than cellulose.
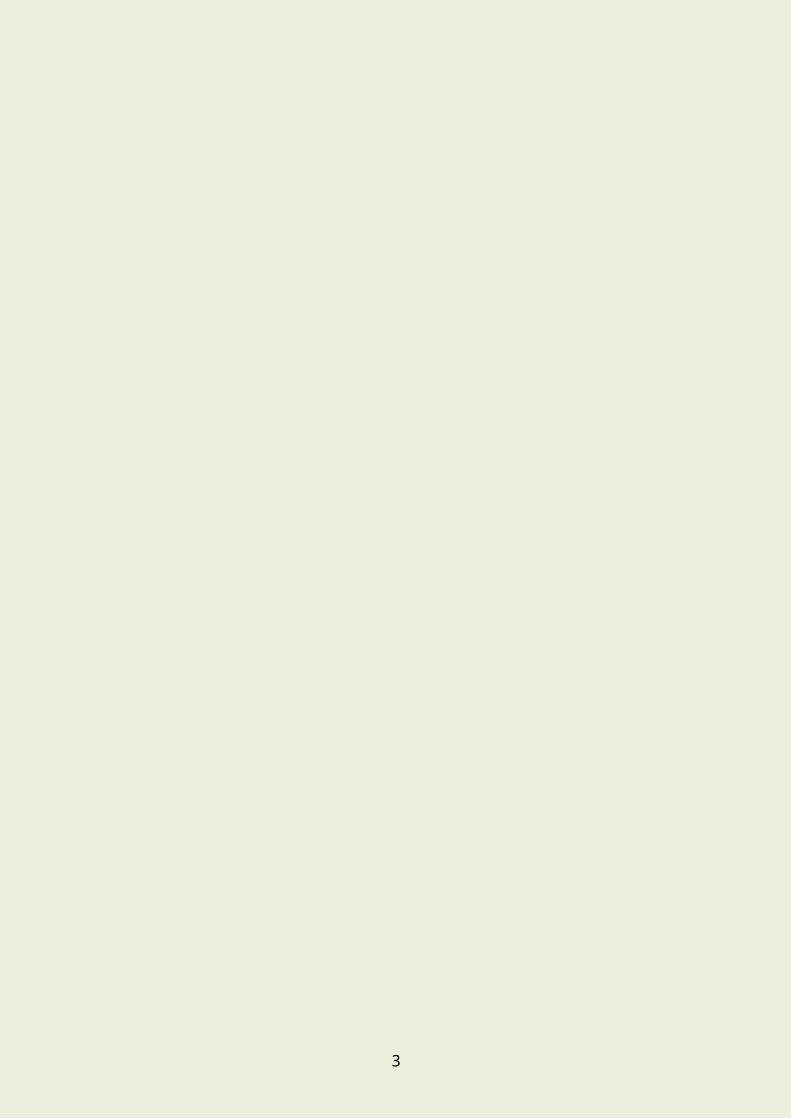
PhysiologyTotal sleep time per day correlates with body size, decreasing as the land mammal increases in size. But metabolic rate also decreases as size increases due to surface area:volume ratio. So sleep could be a strategy to save energy for animals that must spend their waking time feeding.
Shrews must eat three or four times their body weight every day due to their small size and subsequent heat energy loss, yet they remain
asleep for 12 hours. During this time their heart, breathing and metabolic rates can be reduced to save energy. In smaller mammals sleep may be important for conserving resources as well as keeping them safe from predators.
The sloth is relatively large and not the most active of animals, and should not need much sleep, yet it sleeps for around 20 hours a day; this goes against the body size correlation and restoration ideas.
L
R
16

The Activation Synthesis Theory of Dreaming
Hobson & McCarley (1988) developed the activation synthesis theory of dreaming. This theory states that dreams are produced by random stimuli from the pons. The forebrain, the "thinking" part of the brain, receives these stimuli and then makes up stories to make sense of them. These stories are what we call dreams.
According to the activation-synthesis theory, dreams are merely the brain's reaction to random biological processes that occur during sleep.
Various parts of the brain - in particular the pons, part of the brain stem - continue to function and produce stimuli during sleep and REM sleep in particular. The brain then takes these internal stimuli and attempts to make some sort of sense of them. To do this it uses other random stimuli and memories, especially those easily accessible in the short-term memory.
Random BrainwavesFor example, the randomly produced stimuli might resemble those produced when running. The sleeper's mind could then interpret those stimuli as a dream of running. If, in addition, they had earlier that day been startled by a cat then the brain might latch on to that memory and produce a dream of being chased by a lion. The brain produces a random dream with no deep or hidden meanings or purpose.
As the pons continues to fire random stimuli at the forebrain, the brain constantly attempts to interpret them. This is why dreams sometimes shift so suddenly in content. The forebrain is attempting to respond to totally new random stimuli and needs to build a completely new situational model to incorporate them.
The activation-synthesis hypothesis has the advantage that it renders dreams meaningless and removes any need to understand or interpret them. Some would argue that this is also its biggest disadvantage.
Summary of the Biological Theories
Due to the fact that sleep duration and patterning seems to depend on different factors, it is unlikely that any single biological explanation could account for all the functions of sleep and dreams. While each theory has support, there is still no clear-cut single theory of why we sleep. Sleeping impacts many biological processes, so it is very possible that sleep occurs for many reasons and purposes. It is possible to use each of these theories to explain it.
The Cognitive Approach to Sleep & Dreams
Activities
1. According to the Activation Synthesis Theory, how are dreams produced?2. Are dreams meaningful according to this theory?3. Summarise the theory using the following key words : pons, REM, brain4. Why do dreams suddenly shift in content?5. What is the biggest advantage and disadvantage of this theory?
17

Computer AnalogyThe cognitive approach focusses on the role of sleep in memory and thinking. According to this viewpoint, the mind is a processor of information and sleep largely exists in order to facilitate this processing. During sleep, the mind can clean up files, pruning out unnecessary items and strengthening the link between memories.
Stickgold (2009) has investigated the processes by which memories develop during sleep. According to his research, sleep can be of benefit to every type of memory, but he suggests that those that have a medium (rather than strong or weak) memory trace gain the biggest benefit.
Sometimes a nap is just as good as an overnight sleep when it comes to consolidating learning through sleep. Seehagen et al (2015) found that when babies are learning a new action, those who had taken a nap showed a better recall of the skill than those who had not.
Walker et al (2003) used a finger-tapping task to study the role of sleep in memories. They found that sleep helps memories to be reliably encoded but that recalling an item the following day reactivates the memory, allowing a skill (such as playing a musical instrument) to be refined.
SchemasA schema is a set of ideas, or a pattern of thought about a particular concept or situation. The key idea is that information is not stored separately, but is linked together with other relevant information. We may have a schema for a school building for example, which will be drawn from our direct experience of school buildings, as well as buildings that we have seen or read about. The result is a concept that includes a typical image or average features.
Schemas play a role when it comes to jokes or stories. If someone tells a joke which begins “a man walked into a bar…” this deliberately activates the schemas for a typical man and a typical bar. Of course, each person will have slightly different schemas for both of these things – because everyone has different experiences, everyone’s schemas will be different. However, it is very likely that your schemas will be similar to those of other people with a similar upbringing, and someone from a different culture from yourself will have very different schemas.
Sleep SchemasThe cognitive approach looks at dreams in terms of normal thought processes such as schemas. According to Domhoff (2011), a dream is what happens when the mind does not have any other task. He draws comparisons between the dream and waking experiences, such as daydreams and fantasies, saying that they are very similar in content and occur when the mind is not set a particular task to do. From this point of view, the mind’s usual processes of schemas, beliefs and emotions will play a large role in dream content. Therefore, this view studies dreams using knowledge of waking thought processes as a start point.
The cognitive approach to dreaming would predict links between what we think about during the day and what appears in our dreams, and is partly supported by evidence that dreams usually have a story that makes sense, rather than being a random mixture of memories.
Irrational Thoughts & BeliefsThe traditional view of the human mind was that it was rational. Although Freud recognised that irrational thought processes can affect us, he considered these to be childlike unconscious forces and regarded the ego as the rational aspect of the mind.
18

Later cognitive psychologists have identified several ways in which human thought processes are biased or irrational. One basis for this is that we are guided by beliefs about the world, and that these beliefs may at times be wrong and harmful. Ellis (2003) argued that a lot of anxiety can arise from distorted beliefs such as:
Personalisation – a tendency to relate all events to oneself. For example, if someone doesn’t talk to you in the corridor, personalisation would be thinking “she must be in a bad mood with me” rather than for example “she must be busy and distracted”.
Overgeneralisation – taking one thing and applying it to many or all situations. For example, after failing a test a student may overgeneralise and think “I’m useless at everything”.
Selective abstraction – tendency to focus on one small part of an even. For example, after a date that went well overall, the person may focus on one thing that went wrong (e.g. maybe they tripped over and felt clumsy) and ignore all of the positive events, therefore remembering it as having been a really bad evening.
Humans don’t actually work everything out like a computer, but instead rely on simplistic assumptions. These help the mind to save on limited mental resources such as attention. Essentially, people’s behaviour is not always rational, but is instead often guided by intuition.
Beck's cognitive triad, also known as the negative triad, is an irrational and pessimistic view of the three key elements of a person's belief system present in depression. It was proposed by Aaron Beck in 1976.
(i) negative view of myself (I am a failure)(ii) negative view of my situation (It is a disaster and my fault)(iii) negative view of the future (It is never going to change)
As a result of these views, we exaggerate the negatives in our lives and do not recognise the positives. This negative view of ourselves can affect the content of our dreams; according to approach views of ourselves and learning from that day will be the focus of dreams.
Evaluation The approach is supported by a large body of experimental findings showing that thought processes are not always logical and can be distorted. However, much of the research is based in the laboratory. In particular, research into the key cognitive areas of memory and perception has tended to be very artificial.
The approach assumes that thought processes cause people to have negative feelings and behaviours, but thoughts may be the result rather than the cause of conditions such as stress.
Research has tended to ignore the underlying brain processes involved. This is changing, however, as brain scanning technology improves.
Information Consolidation Theory of Sleep
19

You may have heard of this theory, which suggests that the function of sleep is to process information that has been acquired during the day, so we are better prepared for the day to come.
There is also compelling evidence that a function of sleep may be to support the formation of long-term memory. The idea is that memories are temporarily stored in short-term memory (in a part of the brain called the hippocampus), then gradually get transferred to a long-term memory store, or are forgotten. It is during sleep that this transfer from short-term to long-term memory happens, specifically deep (nREM) sleep.
The implications of this are that without good quality sleep, we would be unable to function properly during the day. If you think about it, we are our memories - they form our consciousness. Without the memory consolidation function that sleep provides, we would not form long-term memories, which would affect our sense of self. Support for this idea stems from a number of sleep deprivation studies demonstrating that a lack of sleep has a serious impact on the ability to recall and remember information.
Reverse Learning Theory of Sleep
The reverse learning theory says that as we learn and grow, connections are made in our neocortex in a semi-random way. As the number of connections increases, the network becomes less and less efficient. If there were no mechanism to control the number of connections, "parasitic" memories - memories that combine parts of real memories and are falsely associated with many different inputs - would develop eventually. Crick and Mitchison predicted that if this were to happen, people might develop bizarre thoughts (from mixed up memories), hallucinations (from memories being associated with the wrong inputs) or obsessions (from the same connections being made over and over).
According to the reverse learning theory, rapid eye movement (REM) sleep, the sleep stage that is associated with dreaming, prevents this from happening. During REM sleep, the neocortex's major connections to the external world are shut off. The brain stem then sends random stimuli to the neocortex. Crick and Mitchison hypothesized that this would cause some of the connections in the cortex to weaken, which would eliminate some of the thoughts and random associations that aren't useful to keep. They commented on the fact that dreams are often bizarre and illogical, like the expected outputs of parasitic memories.
Adaptive memories: things that will be useful for us to retain
Parasitic memories: useless or harmful memories that waste resources
20

Reorganisational Theory of Dreaming
Crick and Mitchison (1986) developed the Reorganisational theory of dreams. They famously wrote that “we dream in order to forget”.
They devised a theory that stated that the main function of dreams is reorganisation, in order to improve memory storage. The theory is based on the concept of reverse learning, meaning that learning can be undone during REM sleep. They believed that dreams are just a side effect of de-cluttering process that takes place in the brain – the cortex becomes overloaded with information during the day, an dthat during REM sleep, unwanted memories are deleted in order to improve organisation and make space.
Adaptive memories: things that will be useful for us to retainParasitic memories: useless or harmful memories that waste resources
They feel that the brain benefits from reverse learning of parasitic memories and that this is the purpose of REM sleep. Therefore, the theory states that sleep is for cognitive reorganisation. As these unconnected memories and ideas are activated, a random selection of thoughts and memories form into a dream.
Research EvidenceTo support their theory, Crick and Mitchison refer to other species that lack REM sleep – the echidna and two species of dolphin. These animals also have larger brains than might be expected for their overall body size. The researchers conclude that the ‘pruning’ of memories during REM sleep allows the brain to be smaller and more efficient in other species.
The researchers have also run neural network computer models of learning. In these, they have found that memories are easily overloaded but that this can be reduced using reverse learning.
EvaluationA strength of the reorganizational theory is that it gives a clear theory about why REM sleep could be important. By making memory more efficient, Crick and Mitchison argue that better use is made of the available space in the brain.
The spiny anteater is a primitive egg laying mammal who has no REM sleep, but does have a huge enlarged frontal context. Crick and Mitchison claim this is to store unnecessary memories which humans dispose of in REM sleep.
However, a major weakness of this theory is that it is based on computer models of memory, and lack research support on human participants. Numerous studies have shown that rather than destroying memories, sleep is beneficial to memory.
This theory also does not explain why dreams have a narrative (storyline) – our dreams appear to make sense the majority of the time. This doesn’t seem to fit well with the idea that random memories are being activated and destroyed.
21
Problem Solving Theory of Dreaming
Ever had a bad day? The idea of starting fresh every morning with a sunny outlook has some modern scientific backing. According to Cartwright’s theory (1984), dreamers sort through and accept emotions associated with yesterday's misfortunes. While researchers such as Crick and Mitchison dismissed dreams as a disorganized scrap pile of recent experiences, Cartwright conducted studies linking dreaming to the emotional state of waking life.
One of Cartwright's studies concluded that a good night's sleep can cause the dreamer to wake up on the right side of the bed. Upon arousal, Cartwright's study subjects who began dreaming earlier than others in their sleep cycle dreamed for longer time periods, woke up able to remember dreams and demonstrated a better mood. Adversely, Cartwright found that subjects who reported hardly any dreams felt even worse in the morning.
She demonstrated dreams as actual treatment to reach remission. She determined that the content of dreams was a product of the dreamer’s waking emotional state and that working through those dreams was therapeutic. As the study concluded, there were certain exceptions.
Evidence to Support Problem Solving TheoryBarrett 1993 studied students who were instructed to solve a problem. Over a week a panel of independent judges found 50% dreamt a solution.
Stickgold (2000) found Tetris players dreamt solutions to problems connected to the game.
Cartwright (1984) found couples separating had dreams relating to their waking coping strategies
Stress and Anxiety Can Interfere With Sleep
Seven out of ten adults in the United States say they experience stress or anxiety daily, and most say it interferes at least moderately with their lives. About one-third report persistent stress or excessive anxiety daily or that they have had an anxiety or panic attack. Seven out of ten of those adults say they have trouble sleeping.
These are among the findings of the 2007 Stress & Anxiety Disorders Survey, a report examining the effects of anxiety disorders and everyday stress and anxiety on sleep. The survey was commissioned by the Anxiety Disorders Association of America (ADAA).
Stress and Sleep Problems
The majority of adults with a stress-induced sleep problem experience it at least once per week, and more than half experience it at least several times a week. Three-fourths of adults whose sleep is affected by stress or anxiety say that their sleep problems have also increased their stress and anxiety: 54 percent say that stress or anxiety increased their anxiety about falling asleep at night, and 52 percent of men and 42 percent of women reported it affected their ability to remain focused the next day.
22

Key Research into Sleep
Dement & Kleitman (1957)“The relation of eye movements during sleep to dream activity: an objective method for the study of dreams”
AimAserinsky and Kleitman found a relationship between rapid eye movement (REM) during sleep and reports of dreaming. Dement and Kleitman aimed to test:
Whether more dreaming occurs during REM sleep than non REM sleep Whether there is a positive correlation between the objective length of time spent in REM and the
subjective duration of reported dreaming Whether there is any relationship between the pattern of rapid eye movements and the content of the
dream.
This was a laboratory experiment with a small group of volunteers (7 males & 2 females). Participants were invited to the lab in the evening to monitor physiological changes during sleep. They were asked to perform normal duties during the day but asked to avoid caffeine. Participants were measured during sleep using PSG means, i.e. EEG, EOG etc. They were woken at various times and had to report on their dreaming. Dreaming only counted if a fairly detailed and coherent dream was reported.
Study oneSubjects were awoken during either REM or non-REM sleep either deliberately during REM and non-REM periods or randomly when they had been told they would be awoken during periods of REM sleep or at the whim of the experimenter. Participants had to record their responses rather than answer experimenter questions directly in order to avoid bias.
Study twoSubjects were awoken either 5 or 15 minutes after REM sleep began and were asked to decide whether the duration of their dream was closer to 5 or 15 minutes. The length of the dream, measured in terms of the number of words in their dream narratives, was correlated to the duration of REM sleep before awakening.
Study threeSubjects were woken as soon as one of four patterns of eye movement had occurred for 1 minute, and were asked exactly what they had dreamt.
Mainly vertical eye movements Mainly horizontal eye movements Both vertical and horizontal eye movements Very little or no eye movement
23

ResultsStudy oneRegardless of how participants were woken, more dreams were reported in REM than non-REM sleep. When they recalled dreams from non–REM sleep it was most often close to the end of REM.
Study twoParticipants were correct in matching the duration of their dream to length of time they had shown REM sleep. All showed a significant positive correlation between the length of their dream narratives and duration of sleep.
Study threeThere was a very strong association between the patterns of REMs and the content of dream reports e.g. the vertical REM periods were associated with dreams of looking up and down at cliff faces, ladders and basketball nets.
Evaluation- Dreams may be recalled more easily in REM than NREM sleep because the latter is a deeper stage of
sleep - perhaps dreams occur in deeper sleep, but are more difficult to recall from it.
- The study used a limited sample with more men, therefore showed a lack of generalisability.
- Lab experiment so there was low ecological validity. The participants may not have experienced their average sleep – performing the experiment as a field experiment would allow for higher ecological validity.
- Ethical issues – waking people from their sleep is considered as unethical by the BPS.
+ The research provides support for the idea that dreams can be studied in an objective way. This then opens up areas of research for the effect of environmental stimuli on dreaming.
Activities:
1. Outline the study conducted by Dement and Kleitman in your own words (note that you will need to write the conclusion!).
2. What measures were taken by the researchers to ensure bias did not influence their participants/results. Why did they do this?
3. What can you say about the sample of participants used?
4. The experiment conducted was a lab experiment. Evaluate this method and suggest how this study could be improved in it’s methodology.
5. Outline the main strengths and weaknesses of the study.
6. Suggest one further strength and one further weakness not mentioned above.
24

The Psychoanalytic Approach to Dreams
Freud postulated that dreams are the symbolic expression of frustrated desires that had been relegated to the unconscious mind. He used dream interpretation in the form of psychoanalysis to uncover these desires.
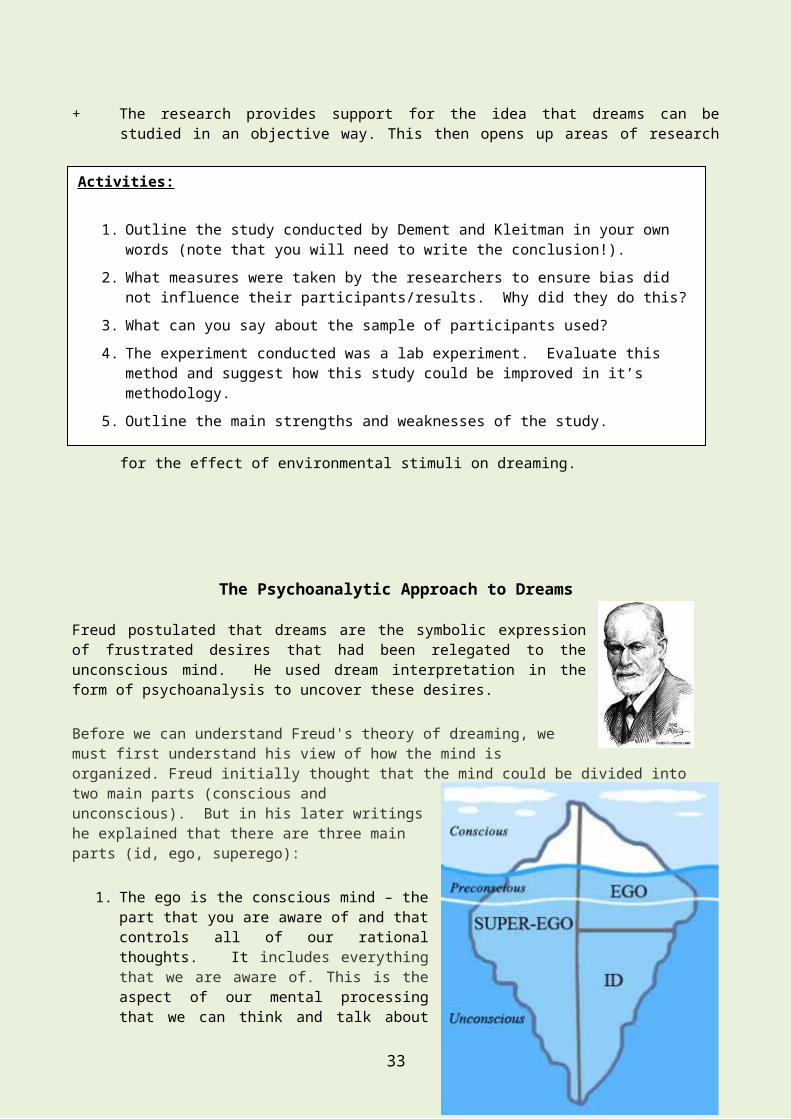
Before we can understand Freud's theory of dreaming, we must first understand his view of how the mind is organized. Freud initially thought that the mind could be divided into two main parts (conscious and unconscious). But in his later writings he explained that there are three main parts (id, ego, superego):
1. The ego is the conscious mind – the part that you are aware of and that controls all of our rational thoughts. It includes everything that we are aware of. This is the aspect of our mental processing that we can think and talk about rationally. A part of this includes our memory, which is not always part of consciousness but can be retrieved easily at any time and brought into our awareness. Freud called this ordinary memory the preconscious.
2. The superego is partly conscious and partly unconscious. It is our awareness of society’s rules, and therefore provides us with a moral sense of right and wrong. If we do things that our superego does not approve of, we get feelings of guilt.
3. The id is the unconscious mind. It is the first to develop in childhood. It is a reservoir of feelings, thoughts, urges, and memories that outside of our conscious awareness. Most of the contents of the unconscious are unacceptable or unpleasant, such as feelings of pain, anxiety, or conflict. According to Freud, the unconscious continues to influence our behaviour and experience, even when we are not aware of it doing so. These feelings, wishes and desires are in the unconscious mind and, according to Freud, would drive us to madness if we were aware of them!
Psychological problems can arise from conflicts between the conscious and unconscious. The rational ego may be urging a person to do one thing, but the irrational id is prompting them to do something different. Like an iceberg, the largest and most powerful part of the mind – the unconscious – was thought to be beneath the surface.
Id, Ego, & Superego in Relation to DreamsFreud saw the process of sleep as motivated – the mind desires to withdraw from the external world and go into a foetus-like state without troubles and worries. In this view, dreams are seen as a problematic interruption.
The psychoanalytic approach states that during sleep the id becomes dominant, and the id’s main motivation is pleasure; dreams reveal our unconscious wishes and fantasies. Freud believed that dreams involved wish fulfilment – we dream about what we want – especially about wishes that have been denied in real life.
Psychoanalysts believe that only some thoughts are truly inaccessible. There are others that we may be unaware of at a particular moment but can become conscious if we make the effort under the right
Activities1. Explain Freud’s iceberg analogy. What happens within each part of the mind?
25

conditions – our preconscious thoughts. Most memories about ourselves and our lives are, therefore, preconscious, as are memories of our dreams.
Psycho-Sexual Stages of DevelopmentFreud developed a controversial theory of how people’s minds develop through childhood. He thought that just as adults get physical pleasure from sex, children get pleasure from their bodies too, but from different body parts. He thought that a baby derives pleasure from its mouth (being fed) and called the associated
stage of development the oral stage. He also thought that toddlers get pleasure from controlling their bladder and bowel movements when going to the toilet/potty. He called this the anal stage.
This theory was not just about explaining behaviour during breast-feeding or toilet training – Freud thought that these stages had an important on your later personality. He explained that some people develop a fixation in these stages, leading to effects on their personality later
in life. Fixation might result from getting too little stimulation during these stages, or from being harshly punished, such as a child being strictly told off for having an accident during toilet training. The idea of people having an ‘anal personality’ derives from this idea – an anally retentive personality is fussy and strict, with an obsession with neatness. Someone with ‘oral personality’ may habitually bite their nails, smoke or overeat.
Perhaps more important still was Freud’s view of what happened next. Inspired by a dream he had about his own mother, Freud stated that boys at around the age of five move into the phallic stage, and develop the Oedipus complex, where they become romantically attached to their mother as an idealised role model of the opposite sex. The boy then feels guilt and fears being punished by his father. Freud’s case study of Little Hans is a key example of this stage from his research. Hans was seen as an example of the Oedipus complex.
A similar theory was developed which applies to girls – the Electra complex. This is the idea that the child experiences a process of falling in love with her father.
Freud said that this stage is resolved when the child appeases the same-sex parent by copying their behaviour, and therefore, at this stage, the boy starts to behave in a more traditionally masculine way and girls adopt traditionally feminine behaviours, such as the clothes that they choose to wear and that the activities that they are interested in.
According to Freud, the experiences we have during our childhood shapes our personalities. The experiences that we endure throughout the stages of development will have a direct impact upon the adult that you become.
Psycho-Sexual Stages & DreamingFreud thought that dreams contain a series of symbols, with the true meaning of the dream hidden from the conscious mind. In particular, anything disturbing or embarrassing can be hidden by the unconscious mind using a symbolic image. These symbols may be based on the psychosexual obsessions of the person’s psychological stage of development. For example, Little Hans dreamed about his penis during the phallic stage.
Activities1. Explain Freud’s iceberg analogy. What happens within each part of the mind?
26

Defence MechanismsFreud believed that the ego tries to defend itself by distorting reality. According to this approach, a lot of problematic or disturbed behaviour may be caused by defence mechanisms that the mind uses. Freud believed that some uncomfortable thoughts are a threat to the ego, so they are repressed – pushed out of the conscious mind and into the unconscious. This concept of repression is one of the most important defence mechanisms.
In a famous case, Freud’s patient, Anna O, suffered from paralysis on her right side and she felt sick when eating or drinking. Freud believed that her discomfort with drinking stemmed from a repressed memory of a dog drinking from her water glass. Freud claimed that when the repressed memory was made conscious through therapy, the problem was solved.
Sometimes thoughts and memories are thought to have been repressed, meaning that they have apparently been forgotten, but in reality have been pushed out of the ego and into the id because they are too painful or disturbing.
As well as repression, there are a further five defence mechanisms that you should be aware of:
Regression Regression means acting in a more child-like way. This links to Freud’s theory of psychosexual development – comfort is found in a more childlike state rather than the threatening and conflict-filled present. Examples could be sucking your thumb/biting your nails or chewing on things when anxious, having a childish tantrum or just curling up in your bedroom like a young child might do.
Denial This is when people distort reality, typically by stating that something is less of a problem than it is. They may ignore the risks of behaviour such as smoking or unprotected sex, or fool themselves into believing that their behaviour is normal or harmless.
Displacement This is where it would cause anxiety or simply be impossible to direct our emotions towards their true target, so instead we begin to focus the same emotion on another, more accessible target. Examples could be feeling very angry with a strict parent but being too afraid to say so, and so bullying another child instead. Little Hans was thought to have displaced his fear of his father onto horses. Romantic attraction can also be displaced.
Projection This is where we claim that our feelings belong to someone else. Have you ever heard someone say “I think my friend is worried about her exams” or claiming that a friend is attracted to someone? Projection could include negative feelings about ourselves. “You think I’m stupid, don’t you?”
Reaction formation
This is when someone’s behaviour is the opposite of their true feelings. For example, if someone is attracted to another person, they may be rude and hurtful instead of showing affection. Similarly, sexual desires may be warded off by exaggerated disgust towards sexuality. The behaviour is as far as possible from their true feelings, so that the ego does not have to consciously accept the true feelings that cause anxiety.
Dreaming
27

According to Freud, there are two functions of dreams:
1. To allow the expression of primitive urges e.g. sex and aggression 2. To use disguised images (symbols) to protect the sleeper from becoming aware of their latent
thoughts.
Freud believed that the content of dreams is related to wish fulfilment and suggested that dreams have two types of content: manifest content and latent content. The manifest content is the actual literal subject matter of the dream, while the latent content is the underlying meaning of these symbols. The latent content of a dream is the hidden psychological meaning of the dream.
Manifest Content Latent ContentSchool Learning or being judgedA storm Emotional turmoilTeeth falling out Worries or lack of controlPregnancy New aspects of the self
The latent content has to be disguised in symbols as it would it would be threatening to our sense of self if expressed directly from the id. Dreaming is therefore an ego defence mechanism.
Freud answered that symbols appear in dreams because the referents for which the symbols are surrogates are distasteful to the censor. The dream work can smuggle unacceptable things in to a dream by transforming them into innocuous (harmless) symbols. So for example we might dream of climbing a tree instead of masturbating because climbing trees (the symbol) is condoned and masturbating (the referent) is condemned. In short, symbols are disguises for referents.
Understanding a dream involves a process of interpretation of the manifest content in order to understand the latent content, and therefore, the true meaning. In addition, Freud thought that several processes occur that distort the true meaning of the dream, making the content harder to understand. Two key processes include:
Condensation – several ideas or symbols get merged together Secondary elaboration – the dreamer’s own interpretation or things that they add when telling the
dream. This makes it harder for an analyst to recognise the latent content. Displacement - disguises the emotional meaning of the latent content by confusing the important
and insignificant parts.
The Interpretation of DreamsThe psychoanalytic approach is known for the case study method, which for studies of sleep could involve interviews and dream diaries used to record individual patients’ experiences. One of the best examples of this is Freud’s case study of Little Hans, in which the interpretation of Hans’ dreams was crucial.
In the early days of psychoanalysis, Freud used the technique of dream analysis, believing dreams reveal unconscious thoughts and motivations. As time went on, Freud found free association to be a more reliable technique. This involves letting the patients speak in an uninterrupted stream of ideas, with one idea leading to the next. Freud felt that this allowed ideas from the unconscious to be revealed. Free association also aimed to strengthen the ego and help patients to develop a clearer idea of reality, and to make the pressure from the superego more humane and less focussed on punishment and guilt. During sessions, the therapist would stay relatively quiet and take notes while the client did most of the talking. Freud’s preference was for patients to lie on a couch, not looking at the therapist.
28

However, Jung (1964) disagreed with Freud’s method of interpreting dreams. He said that dream symbols are unique to the individual and they cannot have a general meaning. He also stated that dreams should only be interpreted based on what actually appears in the dream, and not translated by the therapist – so for example, he would not say that a dream about giraffes was actually a dream about your parents.
Problems with Freud’s Theory of Dreaming
1. Freud’s theory of symbols-as-disguises is difficult to prove when one night a person has a symbolic dream and the next night they may have an explicit sexual dream. Why are wishes sometimes concealed and sometimes they are not? Freud has no answer to this.
2. Many people have a real talent for dream interpretation although they may have little or no information about Freudian symbolism. Why would we bother to deceive ourselves by dreaming in symbols when dreams can be translated so readily by the dreamer themselves? Again Freud had no plausible answer.
3. People have been using symbolism in their speech for centuries using slang, many of which are sexual in character. How can these symbols be effective as disguises in dreams when they are used in waking life?
4. It assumes that the mind during sleep is capable of performing exceedingly complex operations.
If one were seeing a therapist, it can be said that that individual is experiencing or has experienced some level of stress. This level of distress may influence the way in which they re-tell their dreams.
Dreams are subjective; they are heavily influenced by feelings and emotions. This will inevitably have an impact on the way in which the dreamer describes their dream. Dreams are impossible to study in an objective way through the psychoanalytical approach. Dream interpretation cannot be scientifically tested.
As dreams are an ego defence mechanism, will the patient (unconsciously) ego defend in analysis and only report what is acceptable? – selective and reconstructive memory may be used to ensure their descriptions of their dream are socially acceptable.
Psychoanalytic Research into DreamsFreud’s Case Study of Little Hans (1909)
29

AimFreud wanted to provide evidence for his controversial Oedipus complex. When he was approached by a friend, Herr Graf, whose son suffered from a severe phobia of horses, Freud decided to see if the boy’s behaviour fitted his theory.
MethodFreud’s study was a case study, although it was unusual compared to modern case studies in that he did not study the patient, “Little Hans”, directly, but instead exchanged letters with Herr Graf, discussing the boy’s behaviour, and in particular, his phobia of horses.
FindingsHans had been frightened by seeing a horse collapsing in the street, and had developed a strong phobia of horses (horses were common on the streets of Vienna at this time). He was anxious about the birth of his baby sister Hanna, and apparently, made a connection between her birth and a loaded cart pulled by a horse. Freud was very interested to hear about Hans’s dreams and fantasies, because he thought that these were evidence of unconscious processes. Hans had three key dreams:
In one, he dreamed that he was married to his mother and they had their own family. This was interpreted by Freud as showing Hans’s romantic desire for his mother.
In another dream, a crumpled giraffe was being squashed by a large giraffe – Freud thought giraffes represented Hans’ parents, and that this dream showed Hans’s fear and hostility towards his father.
In a third, a plumber came to the house and removed Hans’s penis, replacing it with a larger one. Freud said that this showed Hans’s desire to be a grown up man and marry his mother, as well as linking to the penis obsession of the phallic stage of development.
He also had certain fantasies and dreams about urinating. He was caught playing with his penis and his mother threatened to have the doctor cut it off! This provoked some anxiety.
EvaluationFreud saw the issues as being evidence for his Oedipus complex, but it is possible that he and Hans’s father distorted the evidence to fit the theory. It is hard to generalise from one patient in a case study – in this case, Hans’s issues do not prove that all boys fear their fathers.
There are difficulties with Freud’s evidence. Hans’ father, who provided Freud with most of his data, was already familiar with the Oedipus complex and interpreted the case in the light of this. It is therefore possible that he supplied Hans with clues that led to his fantasies of marriage etc.
If Hans did have a fully-fledged Oedipus complex, it shows that it exists not how common it is. Freud believed his complex to be universal.
A limitation of the case study method is that it cannot be generalised as it only applies to one person/small group of people.
Freud often based his research on a very limited sample.
Evaluation of the Psychoanalytic Approach to Sleep & Dreams
30

The concept of the unconscious mind and that idea that we may be unaware of reasons behind some of our motivations has returned to popularity. However, many of Freud’s theories of the mind are controversial, and even 100 years on, there is a lack of research evidence to support them. Psychoanalytic theory as a whole is too vague and broad to be testable, and can therefore be called unscientific.
A strength of this approach is its impact in terms of popular understanding of dreams. It has had a major effect on society, in particular in terms of the idea that dreams have hidden meanings.
However, psychoanalysts do not all agree on how to interpret dreams. In particular, Freud and Jung took different approaches. Another obvious challenge for Freud’s idea of wish fulfilment is that many dreams are unpleasant! The approach struggles to give a satisfactory explanation of nightmares.
In general, this approach to sleep and dreams relies too heavily on case studies such as the case of Little Hans. The findings of such studies are hard to generalise to other people.
31

Sleep Disorders
There are four categories of sleep disorders:
1. Circadian rhythm disorders – a circadian rhythm is a body rhythm which occurs once in a 24 hour period e.g. sleep-wake cycle. A normal sleep pattern would be 5 cycles of the of the sleep stages. If the sleep-wake cycle is affected then it disrupts our body clock.
2. Insomnia - where a person cannot get to sleep or stay asleep.3. Hypersomnia - where an individual is sleepy all of the time.4. Parasomnias – when the person is asleep (during non-REM sleep) e.g. sleep-
walking, nightmares, sleep terrors. Children are more likely to sleep walk than adults. Also these are more likely for males. Let’s explore some of these in more detail.
Circadian Rhythm Sleep Disorders
Circadian rhythm sleep disorders all involve a problem in the timing of when a person sleeps and is awake. The human body has a master circadian clock in a control centre of the brain known as the suprachiasmatic nucleus (SCN). This internal clock regulates the timing of such body rhythms as temperature and hormone levels.
The primary circadian rhythm that this body clock controls is the sleep-wake cycle. The circadian clock functions in a cycle that lasts a little longer than 24 hours. The circadian clock is “set” primarily by visual cues of light and darkness that are communicated along a pathway from the eyes to the SCN. This keeps the clock synchronized to the 24-hour day.
Other time cues, known as zeitgebers, also can influence the clock’s timing. These cues include meal and exercise schedules. Circadian rhythms and their sensitivity to time cues may change as a person ages. Each circadian rhythm sleep disorder involves one of these problems: you have a hard time initiating sleep, you struggle to maintain sleep, waking up frequently during the night, you tend to wake up too early and are unable to go back to sleep, your sleep is nonrestorative or of poor quality.
Jet lag disorder: Every day, millions of travellers struggle against one of the most common sleep disorders — jet lag. For years, jet lag was considered merely a state of mind. Now, studies have shown that the condition actually results from an imbalance in our body's natural "biological clock" caused by traveling to different time zones.
Jet lag occurs when long travel by airplane quickly puts a person in another time zone. In this new location the person must sleep and wake at times that are misaligned with his or her body clock. The severity of the problem increases with the number of time zones that are crossed. The body tends to have more trouble adjusting to eastward travel than to west-ward travel. Jet lag affects all age groups. However, in the elderly, symptoms may be more pronounced and the rate of recovery may be more prolonged than in younger adults. Sleep deprivation, prolonged uncomfortable sitting positions, air quality and pressure, stress and excessive caffeine and alcohol use may increase the severity of insomnia and impaired alertness and function associated with trans meridian travel. Jet lag is a temporary condition with symptoms that begin approximately one to two days after air travel across at least two time zones. Exposure to light at inappropriate times may prolong the time of adjustment by shifting the circadian rhythms in the opposite direction.
When traveling to a new time zone, our circadian rhythms are slow to adjust and remain on their original biological schedule for several days. This results in our bodies telling us it is time to sleep, when it's actually the middle of the afternoon, or it makes us want to stay awake when it is late at night.
32
Shift Work Sleep Disorder (SWSD)SWSD is a sleep disorder that affects people who frequently rotate shifts or work at night. About 20% of the US workforce is involved in some form of shift work. Schedules of these people go against the body's natural circadian rhythm, and individuals have difficulty adjusting to the different sleep and wake schedule. SWSD consists of a constant or recurrent pattern of sleep interruption that results in difficulty sleeping or excessive sleepiness. This disorder is common in people who work non-traditional hours, usually between 10:00 p.m. and 6:00 a.m.
The most common symptoms of SWSD are difficulty sleeping and excessive sleepiness. Other symptoms associated with SWSD can include difficulty concentrating, headaches or lack of energy. Not every shift worker suffers from SWSD. However, if you are a shift worker and experience any of these symptoms, you should talk to your doctor.
Consequences of SWSD include increased accidents, increased work-related errors, increased sick leave, and increased irritability or mood problems.
Shift workers must be willing to make sleep a priority. People who work shifts other than a 9:00a.m. to 5:00p.m. routine might have to prepare for sleep even though it might be daylight outside. Minimize exposure to light on your way home from work if you are on the night shift to keep morning sunlight from activating your internal "daytime clock." Follow bedtime rituals and try to keep a regular sleep schedule—even on weekends. Go to sleep as soon as possible after work. It is important to get at least 7 to 8 hours of sleep every day.
Some general guidelines for decreasing the effects of shift work sleep disorder (SWSD)
Decrease the number of night shifts worked in a row. Shift workers working the night shift sleep less than day workers and become progressively more sleep-deprived over several days. You are more likely to recover from sleep deprivation if you can limit your number of third shifts to five or less, with days off in between.
Avoid extended work hours. Avoid working prolonged shifts and putting in excessive overtime. Make sure you have time to sleep and participate in family and social activities.
Avoid long commutes, which can take time away from sleeping. Avoid frequently rotating shifts. It is more difficult to deal with rotating shifts than it
is to work the same shift for a longer period of time. Get enough sleep on your days off. Practice good sleep hygiene by planning and
arranging a sleep schedule and by avoiding caffeine, alcohol, and nicotine. Do not start a night shift with sleep deprivation.
Plan a nap before or during the night shift. Naps can improve alertness in night shift workers.
Appropriate light exposure during the early part of the shift can improve alertness during the shift.
Accidents Caused by Sleep Deprivation from Shift Work
Chernobyl - When the nuclear power plant in Ukraine exploded, creating what some have described as the world’s worst nuclear disaster, the engineers involved had been working for 13 hours or more. Two plant workers died that night. Nearly 240 people were originally diagnosed with radiation poisoning, and 134 cases were later confirmed. The number of deaths attributed to the explosion over the next 15 years proved difficult to quantify.
The Challenger Explosion - The space shuttle exploded just seconds after its January 1986 launch, killing all seven crew members. According to a 1988 report, certain managers involved in the launch had only slept two hours before arriving to work at 1 a.m. that morning. The Presidential Commission on the accident admitted the danger of this deprivation in its June 1986 report, writing, “The willingness of NASA employees in general to
33

work excessive hours, while admirable, raises serious questions when it jeopardizes job performance, particularly when critical management decisions are at stake.”
Circadian Rhythm Sleep Disorder TreatmentsBiological Treatments:
Light TherapyLight therapy can help someone “re-set” a clock that is off. Regular sleep patterns help to keep the clock set at the new time. Light therapy is only part of a treatment plan that should be guided by a doctor who is familiar with sleep disorders. Light therapy is used to expose your eyes to intense but safe amounts of light for a specific and regular length of time. In many places, sunlight is not available at the proper time to be used as treatment. Artificial light may be used to affect the body clock in the same way that sunlight does.
Melatonin Supplements For adults, a medication called Circadin is sometimes used to help relieve the symptoms of jet lag. It contains a naturally occurring hormone called melatonin, which helps to regulate the sleep cycle. Circadin is usually only recommended for three weeks at first. However, these supplements are not available in the UK.
Cognitive Treatments:
Cognitive treatments focus on sleep habits and your environment to try and ensure a good night’s sleep. For the treatment circadian rhythm sleep disorders, a cognitive approach would suggest techniques such as eating meals at regular times and exercise. Eating meals at the correct time according to the new time zone will help your body clock to adjust to the new time zone. Natural light and excise will also help to entrain your body clock.
On a long trip, don’t turn in until it’s bedtime in the new time zone. For the first day or two, spend as much time outdoors as possible to let daylight reset your internal clock.
Drink plenty of fluids, but not caffeine or alcohol. Caffeine and alcohol promote dehydration, which worsens the physical symptoms of jet lag. They can also disturb sleep.
34

Exposure to Bright Light and Darkness to Treat Physiologic Maladaptation to Night Work
Name: Czeisler et al (1990)
Aim: to identify the conditions that ensure rapid entraining of the circadian pacemaker - suprachiasmatic nucleus (SCN).
Sample: eight healthy men aged 22 to 29. They had no medical, psychiatric or sleep disorders as determined by their medical histories, physical examinations, chest radiographs, electrocardiograms, biochemical screening tests, and psychological screening questionnaires. None had worked regularly at night on a permanent or rotating night shift within the preceding year and none had travelled to another time zone during the previous 6 weeks. They were not taking any medications and were instructed to abstain from alcohol and caffeine during the study. Urinary screening verified that they were drug free at the time of the study.
Method: a lab experiment in which eight young healthy males were subjected to night-shift work conditions. The control tests were under ordinary room light at night (150 lux) and daylight in transit to home where they slept. Those in the treatment condition were exposed to bright light at night (around 10,000 lux) and blacked-out dark conditions on return home to sleep during the day. Physiological and behavioural assessments were made across 7 days.
Results: men under the treatments were sleepier during the day and slept 7.7 hrs compared to controls of 5.7 hrs. Alertness and performance indices improved during the night shift for the bright-dark treatment.
Conclusion: The control group failed to adapt to an inversion of the daily routine even after a week. However the bright-dark condition induced a complete adaptation to night work. So the circadian pacemaker (SCN) can be shifted using bright-dark conditions.
Meaning: The ability to adjust the circadian phase and improve the sleep of night-shift workers could have important implications for both industrial productivity and safety.
Evaluation + This had good control of conditions in a lab experiment when most prior research
has been field experiment.+ Multiple physiological and behavioural assessments were used to provide robust
findings that were in agreement with each other.- However the study used a very small sample that does not generalise to the
whole working population.Activities
1. Outline the research by Czeisler et al (1990). Describe the aim, method, procedure, results.
2. Evaluate the study in terms of design, method, sample, procedure, and ethics. 3. What extraneous variables did these researchers control in their study, in terms
of participants?4. What extraneous variables did they control in the environment?
35

Insomnia 1 in 10 adults may have persistent insomnia affecting 3 or more nights in 7 for more than 3 months. Typical insomniacs remain active right up to bedtime involved with tasks of the day like work, dinner and email. They often have lights on in the room in which they sleep. Insomnia can also be due to natural and artificial influences such as the hot flushes of menopause, medication, caffeine and worry. Insomnia can lead to daytime fatigue and impaired performance.
Psychologists believe Insomnia may be caused by another disorder (secondary) or a disorder in its own right (primary). Primary Insomnia are cases where insomnia occurs on its own, with no known causes, for more than a month. The individual may be stressed or depressed but psychological states are not the main problem. It may be developed from bad sleep habits (staying up late, well lit room) but insomnia is the only problem resulting from these habits. Sometimes insomnia, which had an identifiable cause which has now disappeared, continues due to the expectation of sleep difficulty.
The most severe case of insomnia is idiopathic insomnia which begins in early childhood and is effectively lifelong, in severest cases it is not affected by anxiety or arousal however can be associated with high levels of depression.
Primary insomnia is thought to be caused by a malfunction of our sleep control systems or anxiety or Obsessive Compulsive Disorder (OCD).
Secondary Insomnia is where there is a single, underlying medical, psychiatric disorder or environmental cause. Insomnia is a characteristic symptom disorder i.e. it is secondary. Morin et al (1999) estimated 40% of patients seeking treatment for insomnia have an associated psychiatric disorder. E.g.
Psychological disorders; depression, anxiety states. Medical conditions; heart disease, Parkinson’s, asthma. Drugs; stimulants like amphetamines, alcohol. Phase delay syndrome (circadian rhythm disorder from Shift Work) Parasomnias; sleep apnoea, sleepwalking. Environmental causes like too much caffeine.
Treatments for Insomnia:
Biological Treatments: Drugs are only used in secondary insomnia cases to treat depression or anxiety; antidepressants or anti-anxiety drugs such as benzodiazepines. Sleeping pills may increase sleep time but evidence shows they reduce sleep quality, disrupting the normal ultradian pattern of REM and NREM sleep. And when the drugs are stopped increased insomnia can result.
Cognitive Treatments: Cognitive therapy (CBT) helps people with insomnia identify and correct inappropriate thoughts and beliefs that may contribute to insomnia. Cognitive therapy can give people the proper information about sleep norms, age-related sleep changes, reasonable sleep goals, and the influence of naps and exercise.
Stimulus control (SC) is a practice in which the bedroom is reserved for sleep and sex. SC derives from the idea that insomnia may be caused by bedroom associations unrelated to those uses, such as stressful situations, or TV watching. Therefore, the bedroom should be reserved for sleep, sex, and dressing only.
Activities
1. Outline the research by Czeisler et al (1990). Describe the aim, method, procedure, results.
2. Evaluate the study in terms of design, method, sample, procedure, and ethics. 3. What extraneous variables did these researchers control in their study, in terms
of participants?4. What extraneous variables did they control in the environment?
36

Psychological stressors such as exams, deadlines, or job stress may interfere with sleep. It is beneficial for people to develop some kind of pre-sleep ritual to break the connection between stress and bedtime. Some people find it helpful to make a list of all the stressors of the day, along with a plan to deal with them. In addition, periods of relaxation (meditating or taking a hot bath) can help a person relax and get to sleep
Other Sleep Disorders
NarcolepsyIndividuals with narcolepsy cannot control when they fall asleep. Their sleep-waking cycle and SCN appear disturbed by either genetic, neurochemical or organic problems.
ParasomniasAny activity that occurs whilst the person is asleep that is not related to sleeping. Sleepwalking and nightmares are the most well-known. However acting out dreams is now being documented. In 2012 Becky Mason drove 5 miles to work in pyjamas on a Saturday night and crashed her car after being turned away by a security man as she wasn’t due in till Monday morning. Although she was 3 times over the alcohol limit she was cleared of drink-driving. Expert opinion given to the court was that she had and a family history of parasomnia and was asleep until the crash occurred, hence “not responsible”.
Parasomniac activity occurs at fringes of waking and REM sleep and so seems very real. They are more likely when sleep is disrupted by stress, shift work, alcohol, etc. It may account for some of the genuinely believed reports of astral projection and alien abduction.
Sleep WalkingSleep walking is an example of a parasomnia, an event occurring during sleep that does not result in severe insomnia or daytime sleepiness. It occurs during NREM sleep and is related to night terrors which occur during NREM sleep. Activities carried out during sleep are routine but can be quite complicated such as making a cup of tea. Sleep walking is not a conscious activity and a person will have no memory of the events that occurred during sleep walking.
Hublin et al (1997) found that the disorder is most common in childhood, as children have more short wave sleep. It affects about 20% of children and 3% of adults. In severe cases it can have considerable effects on a person’s life and may be a risk of injury. It is only classified as a sleep disorder when it becomes distressing to the individual.
Plazzi et al (2005) found that various factors appear to increase the likelihood of SW. E.g. sleep deprivation, alcohol, having a fever, stress. Hormonal changes during puberty and menstruation can also be triggers.
37

Sleep apnoea Sleep apnoea is the inability to breathe during sleep commonly caused by obesity, enlarged tonsils or throat and middle ear infections. Without breathing, carbon dioxide levels in the blood increase. This triggers the brain to wake up and breathe again, so the individual has regularly interrupted sleep. Obstructive Apnoea is more common and related to snoring. Whilst treatable in adults, sleep apnoea is a possible cause of Sudden Infant Death Syndrome (Cot Death). Breathing and pulse functions are now included with EEG measurement in standard polysomnography.
Obstructive Sleep Apnoea (OSA) –The upper airways are obstructed and breathing is inefficient. It is due to a narrowing of the airways, enlargement of the tissue at the back of the mouth or enlargement of the tonsils. OSA is highly correlated with obesity, typically patients are middle aged and overweight. It affects 4% men and 2% women.
Central Sleep Apnoea (CSA) – There are no problems with upper airways, CSA is linked to heart problems and blood supply to the brain resulting in malfunctions in the brain’s control of respiration and cardiac function. It results in several episodes of breathing failure in the night associated with a chocking sensation. It can lead to insomnia and daytime sleepiness.
Surgery can be used for OSA to widen upper airways, whilst weight loss is also effective. A night cap can also be used. Treatment of CSA is limited but drugs can help the underlying condition.
Activity
In groups, choose one category of disorder to research (circadian rhythm disorders, insomnia, hypersomnia or parasomnia).
You must produce a presentation on the category, giving information about at least two disorders from this category.
Your presentation must consider both CBT and drug treatments for each disorder you talk about.
The more distinctive you make it – the more easily they will remember it.
Each group has 5 mins to explain your sleep disorder to another group.
38

Activity
In groups, choose one category of disorder to research (circadian rhythm disorders, insomnia, hypersomnia or parasomnia).
You must produce a presentation on the category, giving information about at least two disorders from this category.
Your presentation must consider both CBT and drug treatments for each disorder you talk about.
The more distinctive you make it – the more easily they will remember it.
Each group has 5 mins to explain your sleep disorder to another group.
39