the pocketbook: pharmacoeconomic issues related to intravenous immunoglobulin therapy
TRANSCRIPT

The Pocketbook: Pharmacoeconomic Issues Related toIntravenous Immunoglobulin Therapy
Parthiv J. Mahadevia, M.D., M.P.H.
Two analyses were conducted to compare the cost-effectiveness of differentintravenous immunoglobulin (IGIV) formulations: IGIV purified by caprylateprecipitation and chromatography (IGIV-C) and IGIV manufactured by anolder solvent-detergent method (IGIV-S/D). The results indicated that IGIV-Cis associated with cost savings for patients with primary immunodeficiency oridiopathic (immune) thrombocytopenic purpura (ITP). With primaryimmunodeficiency, the largest cost driver was hospitalizations, whereas withITP, it was ancillary product use and, more specifically, additional IGIVtherapy. Although differences were noted between the two IGIV formulations,the long-term cost consequences of administering these IGIV products areunclear. Further work is necessary to determine whether the results of theseanalyses can be generalized beyond these particular patients and to evaluatethe effects on long-term health care costs.Key Words: intravenous immunoglobulin, IGIV-C, IGIV-S/D, primaryimmunodeficiency, idiopathic thrombocytopenic purpura, immunethrombocytopenic purpura, ITP, health care costs.(Pharmacotherapy 2005;25(11 Pt 2):94S–100S)
The ever-rising cost of health care is increasingthe demand for product value—assurance that agiven product truly improves patient well-beingat an appropriate price. Polyvalent intravenousimmunoglobulins (IGIVs) may be consideredcommodity products by many purchasers,leading to product selection based on price alone.However, this practice assumes that the productshave identical efficacy, tolerability, and safety,which may not be a valid assumption. Clinicaldifferences in products could affect resource useand costs, which must be considered whenchoosing an IGIV. Pharmacoeconomics is thecomprehensive study of the costs and benefits ofdrug or biologic therapies.
When new drugs or biologics enter the market,they may be better than, worse than, or nodifferent from another product and may costmore, less, or the same. A product that has thesame or a worse outcome at a similar or higher
cost is not likely to succeed in the marketplace,whereas one with a similar or better outcome atthe same or lower cost is likely to becomecompetitive. Unfortunately, the situation is rarelyso clear. Most new products have betteroutcomes at a higher cost; the questionpurchasers need to consider is whether theproduct is worth the increased cost.
Two separate economic, double-blindcomparisons of an IGIV purified by caprylateprecipitation and chromatography (IGIV-C,Gamunex; Talecris Biotherapeutics, Clayton, NC)and an IGIV preparation manufactured by anolder solvent-detergent method (IGIV-S/D,Gamimune N 10%; Bayer Biologicals, Clayton,NC) were performed. The objective of bothstudies was to evaluate the cost-effectiveness ofIGIV-C, defined as the cost of each eventavoided.
In the first study, which examined patientswith primary immunodeficiency, the principaloutcome measure was the number of validatedinfections (e.g., pneumonia, sinusitis). Analysisdetermined the cost of each validated infection
From MEDTAP International, Inc., Bethesda, Maryland.Address reprint requests to Parthiv J. Mahadevia, M.D.,
M.P.H., Amgen, Inc., Columbia Square, 555 13th StreetNorthwest, Suite 600 West, Washington, DC 20004-1109.

PHARMACOECONOMIC ISSUES RELATED TO IGIV THERAPY Mahadevia
avoided. The second study involved patientswith idiopathic (immune) thrombocytopenicpurpura (ITP); the primary end point was asustained platelet response. In these patients,economic analysis determined the cost of eachsustained platelet response.
Whether differences in the manufacture ofthese two IGIVs produce tangible differences inresource use or costs for patients with ITP isunclear. Because efficacy and costs can beseparate and independent of each other, weexamined the resource use and costs incurredduring two clinical trials of 87 patients receivingIGIV-C and 85 receiving IGIV-S/D. A briefoverview of the methods and results of theseanalyses is presented.
Methods
Examination of Costs
We examined costs from a broad societalperspective. Productivity or indirect costs wererecorded for the primary immunodeficiency trialbut not the ITP trial. Specific costs examined inthe primary immunodeficiency trial were asfollows, with unit costs measured in 2003 U.S.dollars:
• Hospitalizations (obtained from patient diarycards and adverse-event case report forms)
• Prescription drugs• Physician and emergency department visits• Productivity costs (measured as days missed
at school or work, obtained from patientdiary cards)
Specific costs examined in the ITP trial (in2003 dollars) were as follows:
• Splenectomy-related hospitalizations• All other hospitalizations• Prescription drugs• Ancillary products• Diagnostic tests
Acquisition costs of the two IGIV productsused in the study (IGIV-C and IGIV-S/D) wereconsidered the same; thus, no incremental costdifferences were noted based on price alone.Costs for each patient were calculated in a three-stage process: medical resources used and/or lostproductivity during the episode of care werecategorized for each patient, a standard unit costwas assigned to each type of resource, and thequantity of each resource used by a patient wasmultiplied by the cost of that resource.
Assignment of Costs
Physician and emergency department visitswere monetized using Current ProceduralTerminology coding.1 Because the patient diariesin the primary immunodeficiency study did notdistinguish between physician and emergencydepartment visits, a 50:50 distribution of eachwas assumed. In the ITP study, unit costs fordiagnostic procedures (peripheral blood smearsand bone marrow aspirations) were determinedusing national Medicare databases.
Incident drugs were valued using 95% of theaverage wholesale price listed in the 2003 DrugTopics Red Book.2 Costs were computed for allincident drugs with complete dosage, treatmentduration, and drug information. For incidentdrugs with incomplete information, the cost wasimputed with the average cost of documentedprescriptions within the same drug class.
The cost of hospital admissions wasdetermined using the Healthcare Cost andUtilization Project (HCUP) database, a nationalinpatient database.3 Using data from the clinicaltrial, the reason for each hospitalization wasidentified and assigned a code from theInternational Classification of Diseases, NinthRevision (ICD-9). An average daily charge wascomputed for the associated ICD-9 code.Charges were converted to costs using thestandard HCUP cost:charge ratio of 0.56(national estimate according to the HCUPdatabase).
The value of each day missed from school orwork as recorded in patient diaries from theprimary immunodeficiency study wasdetermined by multiplying the median hourlywage in the United States of all non–farmworkers (obtained from the Bureau of LaborStatistics) by 8 hours of lost productivity. Thisapproach assumes that all study patients whowork or one caregiver for each patient whoattends school will miss 8 hours of work. It alsoassumes that lost productivity will not bereplaced later.
Statistical Analysis
Pharmacoeconomic data are not amenable tostandard statistical tests, in part because not allpatients incur all types of expenses. Therefore, atwo-part multivariate model was used forinferential analysis.4 Briefly, this method uses aprobit model to determine the probability ofhaving a nonzero cost for each study group toaccount for zero costs (e.g., hospitalization of
95S

Supplement to PHARMACOTHERAPY Volume 25, Number 11, 2005
patients who were never hospitalized). Thismethod also uses a generalized linear model toexamine differences among those who used agiven resource. It allows incorporation of allpatient data that are nonnormal and have abimodal cost distribution (zero mass peak andnonzero peak).
All analyses were performed for an intent-to-treat study sample. All costs for hospitalizationsand adverse events were included in thecalculations regardless of causality, which is theU.S. Food and Drug Administration standard.
Results
Primary Immunodeficiency Disease
Patients with primary immunodeficiencytypically require lifelong periodic replacementtherapy with IGIV to prevent infection. Thestandard of care for these patients consists ofIGIV infusions every 3–4 weeks, generally atdoses of 300–600 mg/kg5; the annual cost/patientis high.6
A randomized, double-blind, head-to-headclinical trial compared the efficacy and safety ofIGIV-C and IGIV-S/D.7 This study compared theproportion of patients with validated andclinically defined infections (pneumonia,sinusitis, and acute exacerbation of chronicsinusitis), time to first infection, and annualinfection rates. The study involved 172 patientsenrolled at 25 medical centers in the UnitedStates and Canada from 1999–2000. All studypatients had a confirmed diagnosis of primaryimmunodeficiency as defined by World HealthOrganization criteria. These criteria include, butare not limited to, congenital agammaglobu-linemia or hypogammaglobulinemia (including
X-linked and autosomal forms), commonvariable immunodeficiency, severe combinedimmunodeficiency, and Wiskott-Aldrichsyndrome. The patients were followed for 9months from the day of their first IGIV infusion.Demographic differences among the studypatients were not statistically significant.
The results demonstrated that IGIV-C wasassociated with a reduction in the percentage ofpatients with at least one validatedsinopulmonary infection (12% of patientsreceiving IGIV-C, 23% of those receiving IGIV-S/D). The annual validated infection rate was0.18 in the IGIV-C group compared with 0.43 inthe IGIV-S/D group (p=0.023).
To understand the economic impact of usingIGIV products that are manufactured differently,we recently reported an examination of theincremental cost-effectiveness of IGIV-C versusIGIV-S/D in patients with primaryimmunodeficiency.8 Using clinical trial casereport forms, patient diaries, or the trial drugdatabase, we identified the number of physicianand emergency department visits, dosage andquantity of incident drugs, number of daysmissed at school or work, and number ofhospitalizations. Given the high morbidity andcosts associated with sinopulmonary infectionscommonly associated with primaryimmunodeficiency, choosing a cost-effectivetreatment strategy was necessary to maximize thevalue of competing treatment strategies.
Costs for components of care are presented inTable 1. Total outpatient costs for the 87 patientswith primary immunodeficiency who werereceiving IGIV-C were $17,370, versus $20,422for the 85 patients receiving IGIV-S/D, with a costdifference of approximately $3000. This
96S
Table 1. Costs for Patients with Primary Immunodeficiency in the Two Treatment Groups
Cost ($)a
IGIV-C Group IGIV-S/D Group DifferenceCategory (n=87) (n=85) ($)Outpatient 17,370 20,422 -3052Prescriptions 100,379 123,975 -23,596
Validated infections 1793 4957 -3164Nonvalidated infections 40,342 46,238 -5896Related to adverse events 888 510 378Other drugs 57,356 72,270 -14,914
Productivity 37,031 35,488 1543Hospitalizations 104,160 182,892 -78,732IGIV-C = intravenous immunoglobulin purified by caprylate precipitation and chromatography; IGIV-S/D= intravenous immunoglobulin manufactured by a solvent-detergent method.aIn 2003 U.S. dollars.

PHARMACOECONOMIC ISSUES RELATED TO IGIV THERAPY Mahadevia
difference is partially attributable to the lowerresource use for physician and emergencydepartment visits in the IGIV-C–treated patients,who had 26 fewer visits than the IGIV-S/D–treated patients.
For concomitant prescription costs, the totaldifference between the groups was approximately$24,000. When the total cost is categorized bysubgroup, the IGIV-C treatment group incurredapproximately $3000 less in prescription drugcosts related to validated infections (occurring 2wks from the point of a validated infection),approximately $6000 less in drug costs related tononvalidated infections, and nearly $15,000 lessin all other drug costs. Drugs related to adverseevents (prescribed on the same day the adverseevent occurred) resulted in a $378 differencebetween the two treatment groups. The IGIV-Cgroup reported 240 missed days at school orwork (productivity losses) compared with 230reported in the IGIV-S/D group. Productivitycosts/patient were similar for both groups.
Of all cost categories considered,hospitalizations were the major source of costdifferences among patients with primaryimmunodeficiency in the IGIV-C group. Thedifference was approximately $79,000 betweenthe two treatment groups. Of note, the IGIV-Cgroup had eight fewer hospitalizations than theIGIV-S/D group.
In a multivariate analysis, annual meancosts/patient were significantly lower in the IGIV-C group than the IGIV-S/D group (Table 2). Astatistically significant reduction was found inaverage cost/patient between those in the IGIV-Cand IGIV–S/D groups for prescription drugs(-$302, 95% confidence interval [CI] -$598 to-$6), hospitalizations (-$1454, 95% CI -$1828to -$1080), and total costs (-$1304, 95% CI -$1867to -$742). Costs associated with productivity andphysician visits were similar for both groups andwere not statistically significant.
Some assumptions were made at the outset ofthis trial. For example, in examiningproductivity costs, we assumed that a day missedfrom school or work would cost 8 hours/daymultiplied by the median hourly wage for aworker. Also, because physician and emergencydepartment visits were not recorded separatelybut were a pooled outcome, we assumed a 50:50distribution of both in our base case analysis. Weperformed a sensitivity analysis in which severalof the cost-determination methods were changedto determine the robustness of the findings. Wechanged the ratio of physician:emergency
department visits from 50:50 to 80:20 in favor ofphysician visits, determined the cost ofprescriptions using 80% rather than 95% of theaverage wholesale price, reduced 8 hours of workmissed to 4 hours, and included onlyhospitalizations that were possibly or probablyrelated to the study disease rather than allhospitalizations. Thus, the average patient costdifferences between the study groups remainedstatistically significant in favor of the IGIV-Ctreatment group. For all assumption changesmade simultaneously, the average cost savings forthe IGIV-C–treated patients was lower butremained statistically significant (D $796, 95% CI-$556 to -$1036).
In summary, the total cost savings over 9months for patients with primaryimmunodeficiency treated with IGIV-C wasapproximately $104,000. Assuming equivalentacquisition costs, the cost savings with IGIV-Cwas approximately $1300/patient. An earlierstudy estimated that the costs of primaryimmunodeficiency were$17,000–$34,000/patient/year.6 Based on thiscost, and extrapolating the 9-month$1300/patient/year savings determined in thisanalysis, IGIV-C therapy could save $1700, or5–10% of costs/patient/year compared with IGIV-S/D therapy.8 Thus, IGIV-C could be considereda product with better outcomes and the same orlower costs, or with lower costs and the same orbetter outcomes. These results strongly suggestthat manufacturing processes can result inmeaningful clinical and economic differences.
Idiopathic (Immune) Thrombocytopenic Purpura
97S
Table 2. Cost Differences/Patient with PrimaryImmunodeficiency
Cost Difference BetweenIGIV-C and IGIV-S/D 95% CI
Category Groups ($)a ($)Physician and -34 -70 to 3emergencyroom visits
Prescriptions -302b -598 to -6Productivity -8 -60 to 45Hospitalizations -1454b -1828 to -1080Total costs -1304b -1867 to -742IGIV-C = intravenous immunoglobulin purified by caprylateprecipitation and chromatography; IGIV-S/D = intravenousimmunoglobulin manufactured by a solvent-detergent method; CI =confidence interval.aIn 2003 U.S. dollars.bp<0.05.From reference 8.

Supplement to PHARMACOTHERAPY Volume 25, Number 11, 2005
Idiopathic (immune) thrombocytopenicpurpura is an autoimmune disorder marked bythrombocytopenia and, frequently, bleedingepisodes. This disorder, which affects bothchildren and adults, is a cause of significantmorbidity and mortality.9 The estimated annualincidence is 100 cases/1 million persons,10 andpredicted 5-year mortality rates from bleeding inthe most severe cases range from 2.2% forpatients younger than 40 years to 47.8% for thoseolder than 60 years.11 Failure to treat ITPadequately can lead to consumption of costlyresources requiring hospitalization (e.g., forsplenectomy) to treat low platelet count andultimately prevent bleeding.
A recent study of IGIV-C in patients with ITPdemonstrated efficacy and safety (noninferiority)compared with IGIV-S/D.12 This multicenter,prospective, randomized, double-blind, parallel-group, noninferiority trial involved 97 pediatricand adult patients with acute and chronic ITP.The primary efficacy outcome was the proportionof patients achieving a platelet response (plateletcount ≥ 50 x 103/mm3) by day 7 after completingthe first dose of IGIV.
A secondary outcome was sustained plateletresponse for at least 7 days. Patients werefollowed for 6 months after randomization.Baseline data (age, ITP treatment duration,platelet counts, previous treatment) werecomparable between the IGIV-C and IGIV-S/Dgroups. Findings showed that the averageplatelet response gain was 90% in the IGIV-Cgroup versus 83% in the IGIV-S/D group; thedifference was not statistically significant. TheIGIV-C group also had a slightly higherproportion of patients with sustained platelet
response counts (74% vs 62%), although thedifference was not statistically significant.Compared with IGIV-S/D, fewer patients treatedwith IGIV-C required postemergencycorticosteroid therapy (47% vs 24%, p=0.02).Also, fewer cases of splenectomy occurred in theIGIV-C group (6% vs 13%, p=NS).
In our study, estimated total costs for the 6-month episode of care were calculated byassigning standard unit costs to counts ofmedical resources used by patients in the clinicaltrial. The primary outcome in the costconsequence analysis was the incrementalcost/patient in the IGIV-C and IGIV-S/D groups.
Costs for components of care in our study arepresented in Table 3. The IGIV-C treatmentgroup incurred lower costs for diagnosticprocedures (e.g., peripheral blood smears andbone marrow aspirations) and total prescriptions(approximately $1200 and $27,000, respectively).Blood smears were performed for 12 IGIV-C– andnine IGIV-S/D–treated patients; bone marrowaspirations were performed for only two IGIV-C–and six IGIV-S/D–treated patients. This resultedin slightly higher costs for peripheral bloodsmears in the IGIV-C group ($267) versus theIGIV-S/D group ($219), but in much higher costsfor bone marrow aspirations in the IGIV-S/Dgroup ($1883) versus the IGIV-C group ($628).
Ancillary product use accounted for the largestcost difference, accounting for over $168,000more in costs in the IGIV-SD group, representing76% of the total cost difference between the twotreatment groups. Additional IGIV treatmentaccounted for the largest portion of total cost inboth groups, representing 50% of total cost in theIGIV-C group and 59% in the IGIV-S/D group.
98S
Table 3. Costs for Patients with Idiopathic (immune) Thrombocytopenic Purpura in theTwo Treatment Groups
Cost ($)a
IGIV-C Group IGIV-S/D Group DifferenceCategory (n=45) (n=47) ($)Diagnostic tests 895 2101 -1207Prescriptions 40,465 67,405 -26,941Ancillary products 212,207 380,343 -168,137
Blood components 1783 2493 -711Immunoglobulins 206,220 369,443 -163,223Rho(D) immune globulin 4203 8407 -4203
Hospitalizations 169,165 195,038 -25,873Splenectomy 19,857 62,052 -42,196Other hospitalizations 149,308 132,986 16,322
IGIV-C = intravenous immunoglobulin purified by caprylate precipitation and chromatography; IGIV-S/D= intravenous immunoglobulin manufactured by a solvent-detergent method.aIn 2003 U.S. dollars.
PHARMACOECONOMIC ISSUES RELATED TO IGIV THERAPY Mahadevia
Although the study patients were randomized toreceive a set amount of IGIV product initially, theproviders ultimately determined whether andhow much additional IGIV therapy was required.Patients in the IGIV-C group received 48additional infusions during the follow-up period,whereas the IGIV-S/D group received 88additional infusions. Hospitalization costs alsowere lower in the IGIV-C group, totaling$169,165, a difference of nearly $26,000. Mostof this difference was due to fewer splenectomy-related hospitalizations.
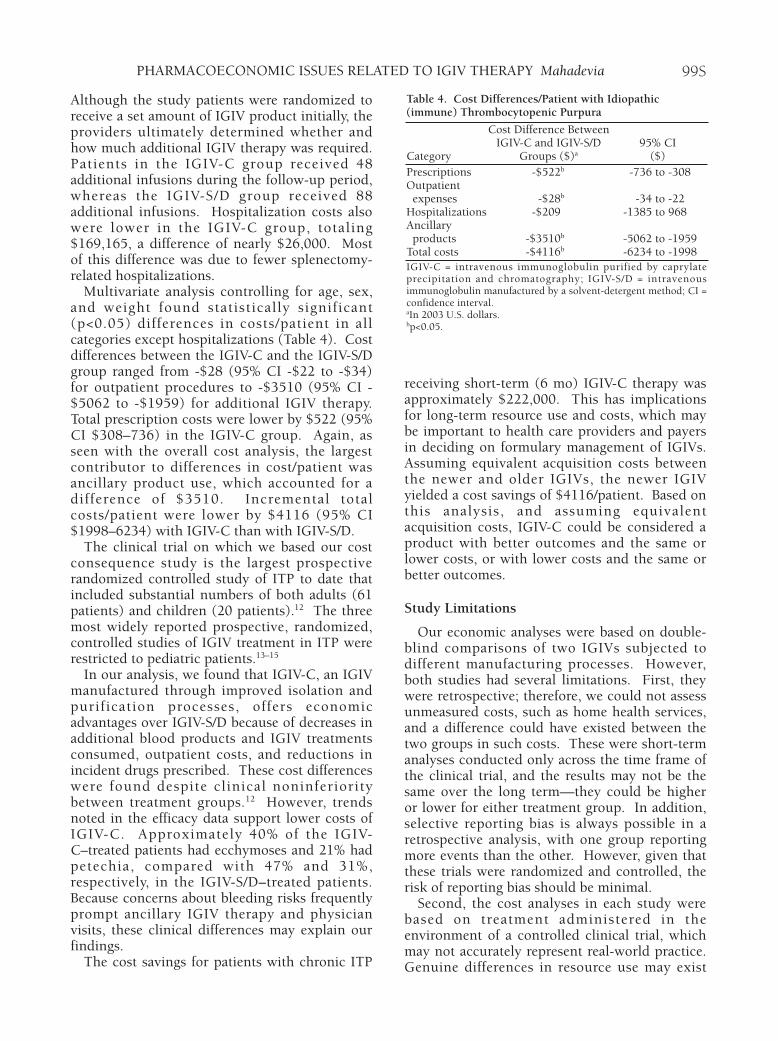
Multivariate analysis controlling for age, sex,and weight found statistically significant(p<0.05) differences in costs/patient in allcategories except hospitalizations (Table 4). Costdifferences between the IGIV-C and the IGIV-S/Dgroup ranged from -$28 (95% CI -$22 to -$34)for outpatient procedures to -$3510 (95% CI -$5062 to -$1959) for additional IGIV therapy.Total prescription costs were lower by $522 (95%CI $308–736) in the IGIV-C group. Again, asseen with the overall cost analysis, the largestcontributor to differences in cost/patient wasancillary product use, which accounted for adifference of $3510. Incremental totalcosts/patient were lower by $4116 (95% CI$1998–6234) with IGIV-C than with IGIV-S/D.
The clinical trial on which we based our costconsequence study is the largest prospectiverandomized controlled study of ITP to date thatincluded substantial numbers of both adults (61patients) and children (20 patients).12 The threemost widely reported prospective, randomized,controlled studies of IGIV treatment in ITP wererestricted to pediatric patients.13–15
In our analysis, we found that IGIV-C, an IGIVmanufactured through improved isolation andpurification processes, offers economicadvantages over IGIV-S/D because of decreases inadditional blood products and IGIV treatmentsconsumed, outpatient costs, and reductions inincident drugs prescribed. These cost differenceswere found despite clinical noninferioritybetween treatment groups.12 However, trendsnoted in the efficacy data support lower costs ofIGIV-C. Approximately 40% of the IGIV-C–treated patients had ecchymoses and 21% hadpetechia, compared with 47% and 31%,respectively, in the IGIV-S/D–treated patients.Because concerns about bleeding risks frequentlyprompt ancillary IGIV therapy and physicianvisits, these clinical differences may explain ourfindings.
The cost savings for patients with chronic ITP
receiving short-term (6 mo) IGIV-C therapy wasapproximately $222,000. This has implicationsfor long-term resource use and costs, which maybe important to health care providers and payersin deciding on formulary management of IGIVs.Assuming equivalent acquisition costs betweenthe newer and older IGIVs, the newer IGIVyielded a cost savings of $4116/patient. Based onthis analysis, and assuming equivalentacquisition costs, IGIV-C could be considered aproduct with better outcomes and the same orlower costs, or with lower costs and the same orbetter outcomes.
Study Limitations
Our economic analyses were based on double-blind comparisons of two IGIVs subjected todifferent manufacturing processes. However,both studies had several limitations. First, theywere retrospective; therefore, we could not assessunmeasured costs, such as home health services,and a difference could have existed between thetwo groups in such costs. These were short-termanalyses conducted only across the time frame ofthe clinical trial, and the results may not be thesame over the long term—they could be higheror lower for either treatment group. In addition,selective reporting bias is always possible in aretrospective analysis, with one group reportingmore events than the other. However, given thatthese trials were randomized and controlled, therisk of reporting bias should be minimal.
Second, the cost analyses in each study werebased on treatment administered in theenvironment of a controlled clinical trial, whichmay not accurately represent real-world practice.Genuine differences in resource use may exist
99S
Table 4. Cost Differences/Patient with Idiopathic(immune) Thrombocytopenic Purpura
Cost Difference BetweenIGIV-C and IGIV-S/D 95% CI
Category Groups ($)a ($)Prescriptions -$522b -736 to -308Outpatientexpenses -$28b -34 to -22
Hospitalizations -$209 -1385 to 968Ancillaryproducts -$3510b -5062 to -1959
Total costs -$4116b -6234 to -1998IGIV-C = intravenous immunoglobulin purified by caprylateprecipitation and chromatography; IGIV-S/D = intravenousimmunoglobulin manufactured by a solvent-detergent method; CI =confidence interval.aIn 2003 U.S. dollars.bp<0.05.

Supplement to PHARMACOTHERAPY Volume 25, Number 11, 2005
between a clinical trial setting and routinepractice. For example, a protocol-drivenphysician visit could lead to additional drugprescription, leading to overstatement of absolutecosts/group. We attempted to reduce thislimitation by including only resource use thatwas not protocol driven but was actuallyprescribed by investigators in a discretionary,case-by-case manner for each patient.
Finally, the patients recruited for these trialsmay not represent the primary immunodeficiencyand ITP patient populations on a larger scale.These limitations may limit generalizability of thestudy results.
Conclusion
The analyses presented suggest that themethod described can be used to compare thecost-effectiveness of two different IGIVformulations—IGIV-C and IGIV-S/D—fortreatment of particular conditions. We foundthat IGIV-C is associated with cost savings forpatients with primary immunodeficiency or ITP.With primary immunodeficiency, the largest costdriver is hospitalizations, whereas with ITP it isancillary product use—more specifically,additional IGIV therapy. Although differenceswere noted between the two IGIV treatmentsover the short term, it remains unclear what thelong-term cost consequences are of administeringthese IGIVs. Further work is necessary todetermine whether the results can be generalizedbeyond these particular patients and to evaluatethe effects on long-term health care costs.
Acknowledgments
I would like to thank Dan Kunaprayoon, B.S., B.A.,Anne Rentz, M.S.P.H., John Strell, B.S., Erwin Gelfand,M.D., and Ron Sacher, M.D., for their contributions tothis research.
References1. Anonymous. 2003 current procedural terminology data files.
Chicago, IL: American Medical Association, 2003.2. Cohen HE, ed. Drug topics red book. Montvale, NJ: Thomson
PDR, 2003.3. Agency for Healthcare Research and Quality. Health care
utilization project: nationwide inpatient sample. 9-1-200.Washington, DC: Agency for Healthcare Research and Quality,2003.
4. Blough DK, Madden CW, Hornbrook MC. Modeling risk usinggeneralized linear models. J Health Econ 1999;18:153–71.
5. Knapp MJ, Colburn PA. Clinical uses of intravenous immuneglobulin. Clin Pharm 1990;9:509–29.
6. Stadtmauer G, Cunningham-Rundles C. Outcome analysis andcost assessment in immunologic disorders. JAMA1997;278:2018–23.
7. Roifman CM, Schroeder H, Berger M, et al. Comparison of theefficacy of IGIV-C, 10% (caprylate/chromatography) and IGIV-SD, 10% as replacement therapy in primary immune deficiency:a randomized double-blind trial. Int Immunopharmacol2003;3:1325–33.
8. Mahadevia PJ, Strell J, Kunaprayoon D, Gelfand E. Costsavings from intravenous immunoglobulin manufactured fromchromatography/caprylate (IGIV-C) in persons with primaryhumoral immunodeficiency disorder. Value Health2005;8:488–94.
9. Simpson KN, Coughlin CM, Eron J, et al . Idiopathicthrombocytopenic purpura: treatment patterns and an analysisof cost associated with intravenous immunoglobulin and anti-Dtherapy. Semin Hematol 1998;35(suppl 1):58–64.
10. Cines D, Blanchette VS. Immune thrombocytopenic purpura.N Engl J Med 2002;346:995–1008.
11. Cohen YC, Djulbegovic B, Shamai-Lubovitz O, et al. Thebleeding risk and natural history of idiopathicthrombocytopenic purpura in patients with persistent lowplatelet counts. Arch Intern Med 2000;160:1630–8.
12. Bussel JB, Eldor A, Kelton JG, et al. IGIV-C, a novelintravenous immunoglobulin: evaluation of safety, efficacy,mechanisms of action, and impact on quality of life. ThrombHaemost 2004;91:771–8.
13. Blanchette V, Imbach P, Andrew M, et al. Randomised trial ofintravenous immunoglobulin G, intravenous anti-D, and oralprednisone in childhood acute immune thrombocytopenicpurpura. Lancet 1994;344:703–7.
14. Blanchette VS, Luke B, Andrew M, et al. A prospective,randomized trial of high-dose intravenous immune globulin Gtherapy, oral prednisone therapy, and no therapy in childhoodacute immune thrombocytopenic purpura. J Pediatr1993;123:989–95.
15. Imbach P, Wagner HP, Berchtold W, et al. Intravenousimmunoglobulin versus oral corticosteroids in acute immunethrombocytopenic purpura in childhood. Lancet 1985;2:464–8.
100S