the nature of cardiac and pulmonary dyspnea
TRANSCRIPT

The Lewis A. Conner Memorial Lecture
The Nature of Cardiac and of Pulmonary DyspneaBy DICKINSON W. RICHARDS, JR., M.D.
Dyspnea has many characteristics, differing from one clinical state to another. In pulmonary dis-eases the immediate cause is usually a disproportion between actual ventilation (breathing require-ment) and breathing capacity. The hyperventilation of organic pulmonary disease is often mis-takenly diagnosed as psychoneurosis. In early cardiac dyspnea, muscular fatigue associated withinadequate cardiac output may be a factor. True pulmonary congestion becomes important inmore advanced left ventricular failure.
D R. Lewis Atterbury Conner, for whomthis lectureship is named, died on Dec.4, 1950, at the age of 84. A man of
outstanding achievement and broad interests,he was throughout his long life primarily aclinician and a teacher of medicine. He was amaster in the art and science of physical diag-nosis, and was among those who hold firm tothe belief that new advances should supportand add to our simpler forms of knowledge,rather than replace them; that in the analysisand treatment of disease, laboratory findings,whatever their nature, should be our servantsand not our masters.
In dealing with clinical situations generallyone can well argue for an approach that is andremains comprehensive and inclusive, not ex-clusive or partial. As Whitehead' has so power-fully argued, the unit of reality is not a name,or a definition, or a formula, or even a theory.It is an event, a whole event, an experience.In clinical medicine the event is the patient.
Delivered at the Scientific sessions of the Twenty-fifth Annual Meeting of the American Heart As-sociation, Cleveland, Ohio, April 18, 1952.
From the Department of Medicine, College ofPhysicians and Surgeons, Columbia University, andthe First Medical and Chest Divisions, BellevueHospital, New York, N. Y.
These investigations were supported in part by a
research grant (PHS Grant H-833) from the NationalHeart Institute of the National Institutes of Health,Public Health Service; and in part by a researchgrant from the Life Insurance 1Iedical Research
Fund.
15
Nowhere in medicine, perhaps, does the pa-tient, whole and entire, so much need to beconsidered as in the field of respiration. Breath-ing is truly a strange phenomenon of life,caught midway between the conscious and theunconscious, and peculiarly sensitive to both.Dyspnea, the major symptom of disordered
breathing, which is the subject of this lecture,deserves, therefore, at the very start of ourdiscussion, some orientation as to its intrinsicnature, and we come, even upon the most cas-ual examination, to a realization that this isactually very different from one clinical stateto another.There is, for example, the dyspnea of the
athlete, the mountain climber, a powerful mus-cular effort that becomes a part of the ex-hilaration of utmost physical effort. Very dif-ferent is the dyspnea of asthma, the hardgasping, the combination of panic and exhaus-tion that oppresses the man whose airways areclosing down; or the even more agonizing slowsuffocation of the man with a tracheal tumor.Still different is the dyspnea of the cardiac,breathlessness compounded with profound ex-haustion, sometimes also with cardiac pain,anxiety, and fear. Thus, in addition to differ-ences in dyspnea itself, there are not infre-quently adjuvant bodily disturbances, such asmuscular fatigue or pain, that are uncon-sciously included, both by patient and doctor,in the symptom. In my further discussion, Ishall endeavor to keep before us an awarenessof these important distinctions.
Physiologically, dyspnea is defined as breath-Circulation, Volume VII, January, 1953
by guest on January 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

NATURE OF CARDIAC AND OF PULMONARY DYSPNEA
ing associated with effort or distress, includinghere both subjective breathlessness and the ob-jective evidences of labored breathing. As asimple description of the process, Cournandand J2 suggested, a number of years ago,the statement that dyspnea occurs wheneverthe individual's actual ventilation cannot eas-ily be provided by his breathing capacity-astatement not greatly different from that byMeans3 a decade earlier. This is obviously anoversimplification, but it applies well to severalforms of dyspnea, especially those occurringin chronic pulmonary disease. It also bringsforward three of the main features to bestudied: breathing capacity, an anatomic andmechanical function; breathing effort, also amechanical function; and ventilation or respir-atory drive producing actual ventilation,largely a physicochemical or neurogenic func-tion.
This simple statement of factors, or influ-ences, producing dyspnea is set forth in thechart in figure 1, and this will form the planof this presentation. Referring very briefly to
MAJOR INFLUENCES PRODUCING THE DISPNEIC STATE
Breat~ing Mechanics Resoiratory Drive
Reduced Increased IncreasedVentilatory Ventilatory Respiratory
Capacity Work Stimulus
Restrcted Labored Increased (hyperpnic)Breathing Breathing Breathing
D Y S N E A
Adjuvant Influences(Chest Pain, Muscular Exhaustion, Psychic Effects, etc.)
FIG. 1.
one or two basic methods of physiologic study,I will review a number of forms of clinicaldyspnea, moving from the simple to the more
complex. As certain types of pulmonary dysp-nea are simplest, or seem to me to be so, Iwill discuss these first, and cardiac dyspnealast.
First as to the breathing capacity, or maxi-mum breathing capacity itself. For many years
the familiar vital capacity was considered tobe an adequate measure of this function, butit became apparent after a time that this didnot record speed of respiration and thus gave a
poor correlation with ventilatory capacity in
such conditions as obstructed or retardedbreathing. The simplest method of includingthe time factor is to have the subject's maxi-mum voluntary effort measured, as for ex-ample, by a tracing recorded on a moving drumto produce the familiar spirogram.4 The detailsof the spirogram, in quiet and maximumbreathing, and in normal and abnormal sub-jects, are well known and do not require spe-cial review.The maximum breathing capacity has in
fact been used as an index of pulmonary func-tion or of dyspnea, just as vital capacity for-merly was; and simplified indices have beendeveloped which give a measure of speed andvolume of ventilation. The recent air velocityindex of Gaensler5 is a modification of this, anextension of the earlier method of Gaubatz.6This, however, leaves out of consideration theamount that the individual actually does ven-tilate under the given conditions of rest orstress, whether hyper- or hypoventilation.There have also been indices of actual ventila-tion only, with no regard for ventilatory capac-ity. Among the best known of these is the so-called ventilatory equivalent of Anthony7 andKnipping,8 the amount of ventilation neededper liter of oxygen consumption, a factor ob-viously increasing as hyperventilation in-creases.We have found, however, as might be ex-
pected, that ventilatory sufficiency, or insuffi-ciency or dyspnea, is better evaluated by con-sidering both factors, breathing capacity andactual ventilation. We have therefore used thebreathing reserve (Knipping9), which is the maxi-mum breathing capacity minus the actual ven-tilation, or the reserve of ventilation still avail-able at any moment. This difference, expressedas a percentage of the maximum breathingcapacity, was found by Cournand and myself2to define quite well the appearance of dyspnea,in various normal and abnormal subjects, whenit reached a value below about 70 per cent or65 per cent. Wright'0 has a somewhat similardyspnea index which is the actual ventilationdivided by the maximum breathing capacity.These two are of course only approximate meas-ures of the entire process. The factors of rateof breathing and effort of breathing in thedyspneic state are not included. I will refer tothese later.
16
by guest on January 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

DICKINSON W. RICHARDS, JR.
The mechanical factors that may limit maxi-mum breathing capacity are of course many:deformities of the chest cage, defects in themusculature involved in respiration, pleuralthickening, hydrothorax, loss of pulmonaryelasticity and expansibility through fibrosis orother intrinsic pulmonary disease, and otherfactors.The many patients in this category can be
illustrated by the first case, that of a woman of40 with widespread fibrotic pulmonary tuber-culosis, who had also had a partial left thora-coplasty. She became dyspneic on moderateexertion, the dyspnea subsiding promptly whenshe stopped and rested. Figure 2 shows a ven-tilatory tracing from each lung obtained by
BRONCHOSP/ROME TRICTRACINGS
___ LEFT LUNG _
FIG. 2. Bronchospirometry. Patient A. S. Tracingsindicate pulmonary ventilation, and oxygen con-
sumption (upward slope of curve), from each lung.
bronchospirometry, and indicates a marked de-crease in ventilatory capacity as well as oxygen
consumption of the left lung. Table 1 gives herover-all respiratory function. As you will see,
her difficulty is simply that of restricted breath-ing mechanics. Inelastic lungs have shrunk hervital capacity and reduced her maximumbreathing capacity to one-half the estimatednormal for an individual of her size and age.
Her actual ventilation, in rest and exercise,and her blood aeration are practically withinthe limits of normal. She is dyspneic on exer-
tion solely because of restricted ventilatorycapacity.
This is probably the most benign form ofdyspnea, at least in its moderate stages. Withsymptoms appearing only on considerable exer-tion, many are unaware of any limitation intheir physical capacity. As Wright"1 has shown,many individuals with uncomplicated second-stage silicosis are in this category, so long as thesilicosis is not complicated by emphysema.
In the majority of the more serious forms ofdiffuse pulmonary disease with functional dis-ability, however, there is usually disturbancealso in the third of the major influences onrespiratory activity as given in our initial dia-gram, namely, respiratory drive or stimulus.As to actual pulmonary ventilation, hyper-
or hypoventilation in clinical conditions, there
TABLE 1 -Chronic Pulmonary Tuberculosis(Patient A. S. Female, Age, 40 years)
Vital capacity,cc.Maximum breathing capacity,L./min..
Pulmonary ventilation, L./min./sq.m.B.S.
Rest.After 1 minute exercise.
Arterial oxygen saturation, percent
Observed
1175
52
3.413.1
Rest ......................... 94After 1 minute exercise .......... 91
NormalControl
3480
97
3.211.9
9696
have been many general statements, but notmuch careful analysis. Even some modern text-books, for example, still give out the generaldictum that patients in chronic cardiac failuretypically hyperventilate while patients withchronic pulmonary failure do not. We havebeen gathering data in both groups over a
number of years, and can say categoricallythat no statement could be further from thetruth than that.
But, in order to understand the cause andnature of a patient's actual ventilatory per-formance, one should know several things: (1)the efficiency or inefficiency of the alveolar airexchange; (2) the effectiveness of aeration ofthe blood; (3) the effectiveness of transport ofthese gases, these chemical stimuli, to the re-
spiratory centers by the circulation; and (4)
:
17
by guest on January 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

NATURE OF CARDIAC AND OF PULMONARY DYSPNEA
how these influences, and others as well, com-bine to produce the final respiratory stimulus.
1. The distribution of inhaled tidal air toperfused alveolar spaces may be somewhat un-equal even in normal subjects, and is oftenmarkedly so in many forms of pulmonary dis-ease. Some air spaces are greatly overventi-lated, others underventilated. There is ventila-tion of regions having no blood perfusion. Inthe terms of respiratory physiology, the inef-fectual or dead space component of ventilationis usually increased in diffuse chronic pulmo-nary disease." Thus to provide for adequaterespiratory gas exchange total ventilation mustalso increase. Here respiratory rate is often ofprime importance, the patient with rapid shal-
TABLE 2.-Behavior of Arterial Chemical Agents inVarious Types of Hyperpnea
(from Gray, J. S. Pulmonary Ventilation)
Max. Vent. Changes in ArterialCondition L./min.P02, PC02 pH
Anoxia ............... 12 _ - +C02 Inhalation ....... 70 + +Metabolic Acidosis 35 + - -
Moderate Exercise .....50±.50 4tSevere Exercise....'. 120 - -
low breathing ventilating chiefly his pulmo-nary airways, with little effective aeration ofalveolar spaces.
2. As distribution of inhaled air deterioratesfurther, alveolar air stagnates in some parts,where active blood perfusion continues, andaeration of the blood becomes inadequate here,even in the presence of total pulmonary hyper-ventilation. Arterial anoxia then ensues. Witha thickened or edematous alveolocapillarymembrane, the tendency to anoxia is in-creased."3The elimination of carbon dioxide by the
lungs differs from that of oxygen in that withsufficient hyperventilation of perfused and wellventilated spaces, the stagnation in poorly ven-
tilated spaces can often be compensated andblood carbon dioxide levels remain normal.When there is carbon dioxide retention inchronic pulmonary disease, this usually indi-
cates an inadequate respiratory stimulus.' Iwill return to this point later.
3. If there is retarded blood flow, venousanoxia and hypercapnia are increased in thetissues, including the tissues of the respiratorycenters, and this may increase the respiratorystimulus.
4. We have just remarked that with ineffec-tual alveolar ventilation, total ventilation"must be increased" to provide normal gasexchange. This teleologic statement, of course,explains nothing, and requires mechanistic sup-port. How is such hyperventilation broughtabout? What are the active respiratory stim-uli? This question brings us into the midst of acontroversy that has been tossed about amongphysiologists for well over half a century. Inhis great book on Blood: A Study in GeneralPhysiology, published 24 years ago, L. J. Hen-dersonl5 concluded that there was not one re-spiratory stimulus, but many. This point ofview has been taken up again recently byJ. S. Gray,16 who has developed a number ofquantitative relations, on the basis of publisheddata. He demonstrates that low oxygen ten-sion, or partial pressure, in the blood, highcarbon dioxide tension, and increased bloodacidity are all positive stimuli to the respira-tory center. Depending upon the level of eachin a given physiologic situation, these supple-ment or inhibit one another, and the net re-spiratory stimulus is the algebraic sum of all.Thus Gray finds that pure anoxia of markeddegree is a powerful respiratory stimulus, butthe usual hyperventilation in anoxia promptlylowers carbon dioxide partial pressure andraises pH and so the net effect is small. On theother hand, anoxia in the presence of normalor high carbon dioxide tension and low pHshould cause, and does cause, very markedhyperventilation. Table 2, taken from Gray'smonograph, shows how these three stimuli mayinteract in various clinical conditions associ-ated with hyperpnea. In muscular exercise,the three stimuli are inadequate to explaintotal ventilation, and Gray postulates a fourth,as yet not identified.Given a certain total respiratory stimulus,
the actual manner in which ventilation is car-
18
by guest on January 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

DICKINSON W. RICHARDS, JR.
ried out rapid and shallow, slow and deep,regular or irregular is conditioned, as Hess,Fleisch,'7 and others pointed out years ago, bythe patient's anatomic limitations and bycountless proprioceptive and other reflexesstreaming in from all parts of the breathingmechanism. All breathing is thus reflexly stim-ulated and conditioned, just as all breathingis also chemically stimulated.
Finally, over and above the chemical andreflex influences, the final ventilatory perform-ance is influenced, more or less, by conscious orsubconscious psychic influences.
30 times in one minute, and measured ventila-tion at rest, during exercise, and for five min-utes during recovery. This gives a fairly con-sistent increase in oxygen consumption, anindex of the amount of additional work done,although the total "oxygen debt" may not becompletely paid by the end of the five-minuterecovery period.'The next clinical case will illustrate the man-
ner in which, in the course of severe, progress-ing pulmonary fibrosis, a restricted ventila-tory capacity, combined with a hyperactiverespiratory center, greatly aggravates the pa-tient's clinical dyspnea. The patient was a man
TABLE 3.-Cardiopulmonary Function inAdvanced Silicosis
(Patient, M. C., Male Age, 66 years)
Observed | Normal
Vital capacity, cc.................Maximum breathing capacity, L./
min.............................Ventilation, L./min./sq.m.B.S.....
Rest............................1 minute exercise...............1st minute recovery.............
Arterial oxygen saturation, percentRest............................Exercise ........................
Arterial CO2 tension, mm.HgRest............................
FIG. 3. Patient M. C. Advanced silicosis.
One further point on methods of study. Tomeasure dyspnea, except in advanced states,the individual has to be put under some sort ofstress. One simple technic has been the breath-holding time; but variations in conscious effortfrom patient to patient render this unreliable.The most direct and generally satisfactory isan exercise test. A continued mild-to-moderateexertion, such as walking on a treadmill, whichprovides a physiologic steady state, over sev-
eral minutes' time, is best. As a simple index ofpulmonary function, however, a single step testof brief duration is often adequate. In most ofour clinical studies we have used a single step,
of 66 with advanced silicosis, complaining ofsevere dyspnea on mild exertion. Figure 3 showsthe x-ray of his chest, and table 3 a summary
of the findings on physiologic study. The pa-
tient has a moderately reduced vital capacityand maximum breathing capacity, but a strik-ing thing also is his marked hyperventilation,both at rest and in the mild standard exercise(30 steps in one minute), ventilation beingalmost twice that of a normal subject. Hisdyspnea is easily explained, since the reducedbreathing capacity and high actual ventilationleave him with a much reduced breathing re-
serve.
But why should he hyperventilate? He hasan increased pulmonary dead space that is,he ventilates unperfused alveolar spaces but
2210
64
5.123.022.0
9597
34
3800
88
3.911.214.5
9696
40
19
by guest on January 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

NATURE OF CARDIAC AND OF PULMONARY DYSPNEA
even so the ventilation of perfused alveolarspaces is such that he keeps his blood carbondioxide level, his carbon dioxide tension, wellbelow normal (34 mm. Hg compared withthe normal 40 mm. Hg). Arterial oxygen satura-tion is normal, at rest and in exercise. Therewas no evidence of cardiac insufficiency here.Catheterization showed that cardiac outputwas normal; there was only a mild pulmonaryarterial hypertension and no increase of sys-temic venous pressure.
Figure 4 shows the same phenomenon, amoderate hyperventilation compared with nor-mal values in a group of 14 patients with un-complicated pulmonary fibrosis, at rest, in exer-cise, and during five minutes' recovery.
2o0
0.~
-Q
c
b0
ac
/5
/0
5
Uncomplhcoaed Pu/m. Fibrosis25 Cases
Res Ex, / 2 3 4 5- - M'nufes of Recovery -
|F1G. 4. Pulmonary ventilation, at rest, exercise,and recovery, in 25 cases of pulmonary fibrosis (solidline) compared with normal subjects (dotted line).
Is this hyperventilation functional, a sortof hysterical dyspnea? Such is always conceiv-able, but there is, by and large, nothing elseto support such an explanation in this largegroup of chronic advanced cases of diffuse pul-monary fibrosis.
Is it reflex dyspnea? In the sense that thepatient does overbreathe to the extent of keep-ing his blood carbon dioxide at an arterialtension of 34 mm. Hg, which is well belownormal, one may well argue that the Hering-Breuer impulses or other reflex mechanism are
exaggerated in this case. We do not have acomplete and satisfactory explanation here, but
there is some evidence to suggest that if wecould add up correctly all the basic chemicalstimuli, after the manner of Gray, we mightcome out with a sufficient chemical explana-tion. One fact of importance is that with low-ered carbon dioxide tension, a respiratorycenter does become more sensitive. Another isthat in this type of case, in spite of practicallynormal blood oxygen values and apparentlynormal circulatory performance, the adminis-tration of oxygen often definitely lowers pul-monary ventilation. This has been known formany years. It suggests that there may be herea significant anoxic respiratory stimulus, inspite of apparently normal arterial oxygen sat-uration.But the question of the functional or psychic
aspect of clinical dyspnea is a most importantone, both in pulmonary and cardiac dyspnea,and frequently difficult of analysis. I am notspeaking of the true respiratory neuroses; theseare relatively simple, either the compulsionneurosis, the repeated sighing respirations, orthe attacks of hysterical dyspnea in the typicalanxiety state. The difficult problem is that ofthe patient with some pulmonary disease, andmuch dyspnea and hyperpnea.An interesting group in this category is that
studied during the war by Galdston, Luet-scher, and their collaborators'8 following acutephosgene poisoning. These cases presentedmany interesting details; one of the strikingfeatures being the frequent persistence of thesymptom of dyspnea long after the patient'sx-ray had completely cleared, physical exam-ination was normal, and pulmonary functionmeasurements had returned nearly to normal,also.
I shall present one of their cases briefly: awoman of 43 with a past history includingconsiderable nervous and emotional instability.She suffered moderately severe exposure tophosgene, with development of pulmonaryedema and acute respiratory insufficiency, re-quiring pressure-oxygen therapy and othermeasures for several days. X-ray and physicalsigns then improved steadily, but for severalmonths thereafter, her nervous symptoms wereaggravated, and she suffered from exertionaldyspnea and, in addition, from independent
20
by guest on January 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

DICKINSON W. RICHARDS, JR.
episodes of breathlessness coming on withoutapparent cause.The measurements of her pulmonary func-
tion several months after the phosgene ex-posure, when x-ray and physical signs werenormal, consisted of a normal vital capacity,maximum breathing capacity that was some-what reduced, some hyperventilation at restand on exertion. Arterial oxygen saturationwas essentially normal. Thus with the milddegree of these deviations from normal, it wouldseem that the functional factor here was animportant one. On the other hand, the patternof respiration was not dissimilar from that ofthe cases of unquestioned pulmonary fibrosisjust considered. Are we entirely sure that thispatient may not have had mild recurrences ofpulmonary edema, giving symptoms, but sub-clinical to x-ray and physical signs?
There is no doubt that anxiety may play apart in the dyspnea of these patients, and themore so the more they become pulmonary crip-ples; and this mental state needs study andcare. On the other hand, we are seeing more andmore of these patients whose physical diseasehas been either undetected or else disregarded,and who are considered to be mental casesonly. Surely there is no more bitter punish-ment that a doctor can inflict upon a patientthan a mistaken diagnosis of psychoneurosis.With no treatment, understanding or even sym-pathy for his underlying condition, he is oftendriven, by doctor, friends, and family alike,into activities which he cannot endure. Physi-cally sick and exhausted, he can get no honesthearing, his perplexity deepens into depression,only to have himself further stigmatized as ahopeless neurotic. Our pulmonary clinics areincreasingly populated by the victims of theseblunderings of our psychosomatic enthusiasts.At all events, it would seem wise in cases
like this not to brand the patient too freely aspsychoneurotic; or at least to judge the specialmanifestations of neurosis on their own meritsonly; but in cases where there is or has beenrespiratory disease or injury, to treat the hyper-ventilation syndrome as primarily a responseto organic disease.A few comments now on dyspnea in the group
of chronic pulmonary diseases known as dif-
fusion insufficiencies. By diffusion insufficiency,I mean that group of diseases, to which Ham-man and Rich'9 first called attention in thiscountry, including beryllium granulomatosis,Boeck's sarcoid, scleroderma of the lung andother conditions in which the important patho-logic lesion is the creation by the disease proc-ess of an alveolar-capillary block causing im-paired diffusion of oxygen into the pulmonaryblood. The symptoms are marked dyspnea,hyperpnea and tachycardia, cyanosis after exer-cise, cough, often febrile episodes, clubbing offingers and toes. Hyperventilation is so marked
20
ti.
I-
-1C
.0
-Z4
Alveolar- Capillary Block25 Cases
/5 F
/0 F
5
,Q11
1111
11
1111
6
Q,CL
ao
ResI Ex. / 2 3 4 5--Minufes of Recovery---
FIG. 5. Pulmonary ventilation in 25 cases ofdiffusion insufficiency (alveolar-capillary block),compared with normal subjects.
in these cases that they too have not infre-quently been diagnosed as psychoneurosis.
Physiologically, these cases are characterizedby a symmetric reduction in lung volumes dueto their diffuse fibrosis, a remarkable mainte-nance of maximum breathing capacity, arterialoxygen saturation little reduced at rest butmarkedly decreased in exercise, carbon dioxidelevels somewhat low in milder cases but essen-tially normal in the more advanced.'3The extent of their hyperventilation is shown
in figure 5, and this sufficiently explains theurgent and continuous dyspnea which is thedominant symptom of this disease. On theGray hypothesis, with a normal or nearly nor-mal carbon dioxide pressure and an unimpededanoxic stimulus, the chemical basis for hyperp-
21
by guest on January 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

NATURE OF CARDIAC AND OF PULMONARY DYSPNEA
nea is perhaps adequate but there may wellbe other factors. There is, for example, thequestion whether there may not be a cardio-circulatory element as well, a retarded circula-tion increasing the stimulus in the respiratorycenter. We have measured cardiac output insome of these cases and it appears to be ade-quate both in rest and in exercise, except latein the disease. A further evidence of the sig-nificance of anoxia in diffusion insufficiency isthe striking relief which is obtained, with sharpreduction in ventilation, through adequate oxy-gen therapy.
I have given but little attention thus far tothe second of the categories of ventilatory me-
TABLE 4. Forms of Pulmonary Dysfunction CausingDyspnea in Chronic Obstructive Emphysema
I. Factors Decreasing Breathing Capacity, andIncreasing Ventilatory EffortNarrowing of Air PassagesInelasticity of Pulmonary TissueHyperinflation of Lungs and ChestSpasm and Asynergy of Respiratory Muscles
II. Factors Increasing Respiratory StimulusEnlarged Intrapulmonary Volume, and PoorDistribution of Inhaled Air
Impaired Alveolar-Capillary DiffusionAnoxiaHypercapniaDecreased Arterial pH
chanics concerned in dyspnea, namely, the ef-fort or work involved in the breathing process.Is the effort per breath increased in these cases
of diffuse pulmonary fibrosis? We have no goodinformation on this point. We do know thatthe air passages are not obstructed, but it maywvell be that the loss of elasticity in pulmonarytissues provides an added burden to respiratoryeffort. However this may be, this factor be-comes a very potent contributing cause ofdyspnea in the next and final group of pul-monary diseases to be considered, namely, pul-monary emphysema.
It would be difficult to construct, scarcelyeven to imagine, a type of disease in whichthere occurred simultaneously more differentkinds of pulmonary dysfunction than are foundin advanced pulmonary emphysema. Corre-spondingly, a great deal has been learned about
pulmonary and cardiopulmonary functionthrough continued studies, in a number ofclinics in this country and abroad, on this dis-ease or group of diseases.
Table 4 summarizes the more important ofthese dysfunctions. The basic change morpho-logically is usually a combination of obstruc-tion of air passages, loss of intrinsic elasticity,and trophic change in pulmonary tissue. Theselead early to the assumption of the chronicallymaintained state of hyperinflation of the chest,since thus air passages are wider, and intra-pleural pressure can again be negative or neu-tral. But hyperinflation with elevated anteriorchest and lowered diaphragm is most unfavor-able for ventilatory activity. The whole mus-cular framework in emphysema becomes spas-tic and asynergic.21 All these factors increasegreatly the actual work or effort per breath.This was well demonstrated by Christie20 someyears ago in his measurements of intrapleuralpressure, in relation to breathing, in normaland emphysematous subjects, in which heshowed that inspiration and expiration inemphysema were associated with wide swingsof pleural pressure above and below zero level,indicating an inelastic lung and greatly in-creased effort in providing its ventilation.
Intrapulmonary air exchange in emphysemais greatly compromised. Maximum breathingcapacity is reduced, due chiefly to expiratoryretardation. Hyperinflation, with increasedresidual air, means relative ineffectiveness oftidal air aerating the lung spaces, but muchmore important is the uneven distribution ofmixing within the lung itself, some parts beinghyperventilated, others greatly hypoventi-lated.12 22 The former leads to hyperpnea, thelatter to anoxia and eventually to carbon di-oxide retention. Finally, the attenuated pulmo-nary capillaries and often a progressively de-veloping pulmonary arteriosclerosis lead topulmonary arterial hypertension and eventuallyright heart failure.
Clinically, the progress of emphysema canbe considered as falling into four classes.22 Atfirst there is decreased maximum breathingcapacity, some hyperpnea, with therefore exer-tional dyspnea as a major symptom, but nor-mal a-ration of the blood. When pulmonary
22
by guest on January 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

DICKINSON W. RICHARDS, JR.
ventilation deteriorates further, there is inade-quate oxygenation of arterial blood, especiallyin exercise. Still further insufficiency bringsinadequate carbon dioxide elimination by thelungs, and carbon dioxide levels in blood andtissues rise, along with more advanced anoxia.With the rising anoxia and carbon dioxide
/5/4/3/2
t' 1/
1/0R'9
87
-i6: 5.1 4
32
/5/4/3/2
.4 //E /0-- 9
76
;2 4
r.2
65 on- 0 NORMAL0- GROUP I
Reds Ex. / 2 3 4 5Minutes of Recovery
in rest and exercise of the four stages of em-physema are charted. Anoxia is of course nowfurther increased, and the vicious cycle becomesin fact complete.Thus in the most advanced emphysema, us-
ually the cases with cor pulmonale in failure,the patients, while dyspneic, are sometimes
/5
Is
/4 O-/ NOMA
*,[ 1
{a / 75 Or ---- NORMALj2 GROUP 3
/5/4/3/2
/09876543
/
o ---O NORMAL
*- GROUP 2
Rest Ex / 2 3 4 5Minutes of Recovery
Rest Lx. / 2 3 4 5*Minutes of Recoveryv
0.--O NORMAL*-* GROUP 4
Rest Ex. / 2 3 4 5Mintwes of Recovery
FIG. 6. Pulmonary ventilation in rest, exercise, and recovery in patients with advancing degrees ofchronic pulmonary emphysema. (Reprinted from Medicine 28: 201, 1949.)
levels, and falling blood pH, one would expectthat the final stage would be associated withexcessive hyperventilation and dyspnea, butat this point another change has occurred. Thechronic hypercapnia, the increased carbon di-oxide, actually deadens the respiratory center,and its insensitivity results in a failure of venti-latory volume even to reach normal values.This is shown in figure 6, where the ventilation
not urgently so, in spite of profound anoxia.It is in this state that the use of morphine isespecially hazardous, and oxygen therapy, byremoving the anoxic stimulus to respiration,induces ventilatory stagnation, with excessivecarbon dioxide retention and carbon dioxidenarcosis.With the above principles in mind, it is not
surprising that the present-day treatment of
23
by guest on January 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

NATURE OF CARDIAC AND OF PULMONARY DYSPNE.IA
emphysema has shifted from the mere adminiis-tration of cough mixtures, sedation and oxygen,to a vigorous effort to open the air passages,and ventilate the lungs by mechanical aids,corrective exercises, and artificial respirators.To those of you primarily interested in heart
disease, this excursion into pulmonary physi-ology has been a long introduction. But I be-lieve that the nature of cardiac dyspnea can beclarified by comparison with these simpler pul-monary forms.While the principles explaining the causes
of dyspnea in heart failure have not changed
20[
/5
/0
RHD - /7 CasesI-
<DT Q.
K
x.
5[
quately, oxygen thus could not be conveyed totissues, and carbon dioxide from tissues, insufficient quantity.23 Relatively retarded bloodflow, increasing anoxia and acidity in the re-spiratory center would induce hyperpnea; andthe prolongation of the hyperpneic state duringthe recovery period, so characteristic a featureof cardiac dyspnea, was explained by the slowrestoration of tissues to their metabolic rest-ing state.A more specific pulmonary component of
congestive heart failure was postulated some60 years ago by von Basch24 the stiffening ofthe lungs that would be expected to occur withpulmonary vascular congestion and this re-
I/O
/00
90
80
70
60
so
40
30
\G -
-- _ o
*0
00
0
00
0
0
0* 0
0
A
A
/0 20 30 40 50 60 70
0
Resi Ex. / 2 3 4 5- - Minufes of Recovery -
FIG. 7. Pulmonary ventilation in 17 cases ofambulatory rheumatic heart disease, with limitedcardiac reserve.
greatly since, let us say, the publication ofHarrison's Failure of the Circulation in 1935,23much has been added in the way of evidence: bycardiac catheterization, by new methods ofpulmonary study, and quite recently by someof the physiologic results of mitral valvesurgery.
Obviously the basic defect in heart failureas compared with pulmonary failure, is inade-quate performance of heart and circulation,rather than inadequate performance of thelungs. Ever since it was known that the cardiacpatient could not increase his oxygen consump-tion, his oxygen intake, in exercise as much asa normal subject, it was assumed that this wasbecause cardiac output failed to increase ade-
MEAN PULMONARY ARTERIAL PRESSURE,mm.Hg., AT REST
FIG. 8. Maximum breathing capacity and meanpulmonary arterial pressures at rest in 15 rheumaticcardiac patients (dots) and two patients with em-physema (triangles).
ceived much emphasis when Peabody25 dem-onstrated the decrease in vital capacity andventilatory capacity with advanced congestivefailure.
Cardiac catheterization studies have nowamply confirmed both hypotheses: the failureof normal increase in cardiac output in exer-cise, and the early abnormal rise in pulmonaryarterial pressures in exercising cardiac sub-jects.26
There has recently arisen also something of acontroversy on the nature of cardiac failure,whether the failure of cardiac output is all-important, or whether the congestive state assuch, "pressure failure," so to speak, may itselfplay a dominant part in the symptomatology.Some evidence which I shall now present
suggests that there may be differences in rela-
24
by guest on January 29, 2018http://circ.ahajournals.org/
Dow
nloaded from
DICKINSON W. RICHARDS, JR.
tive importance of these factors as one movesfrom the milder degrees of heart failure to themore severe. Specifically, the effects of retardedblood flow appear to be dominant early infailure, the evidences of pulmonary congestionbecoming more important when failure is ad-vanced.
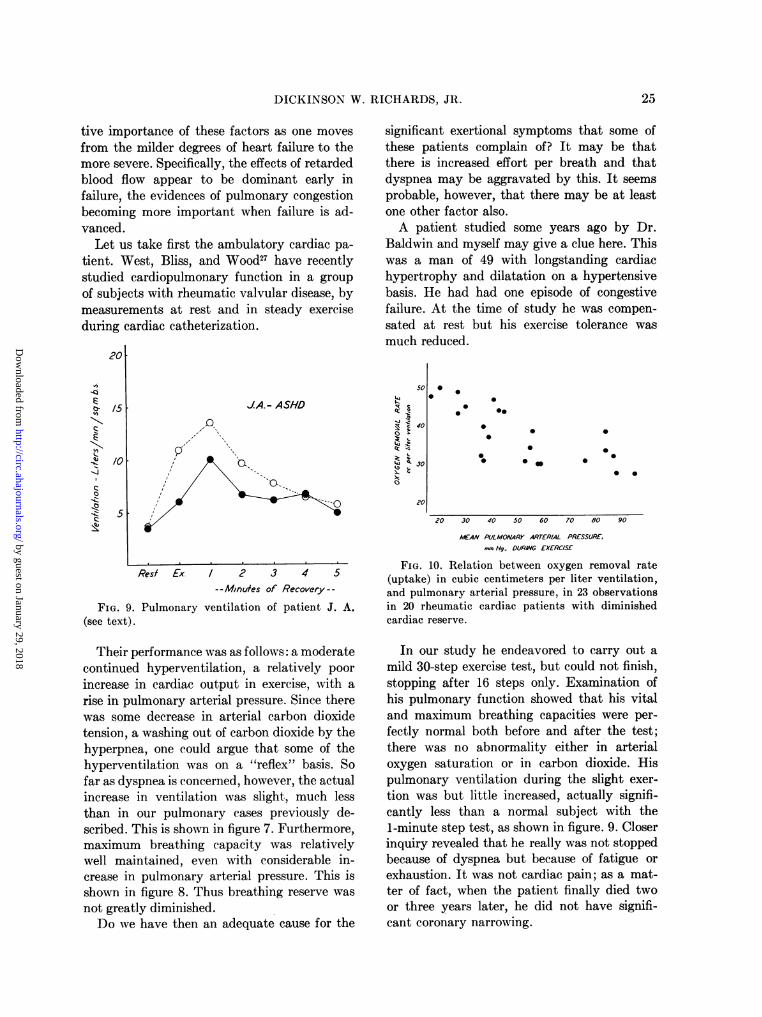
Let us take first the ambulatory cardiac pa-tient. West, Bliss, and Wood27 have recentlystudied cardiopulmonary function in a groupof subjects with rheumatic valvular disease, bymeasurements at rest and in steady exerciseduring cardiac catheterization.
20
--0
c
"N~
c
-,z030b
/5 JA.- ASHD
p,/0 [
5
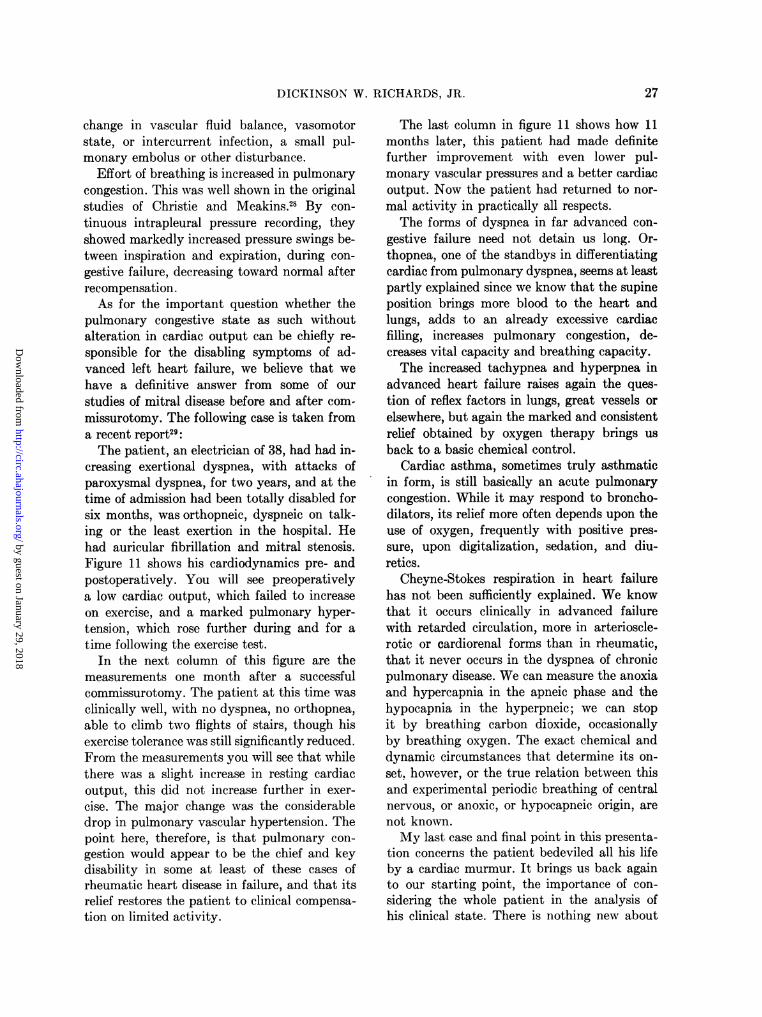
significant exertional symptoms that some ofthese patients complain of? It may be thatthere is increased effort per breath and thatdyspnea may be aggravated by this. It seemsprobable, however, that there may be at leastone other factor also.A patient studied some years ago by Dr.
Baldwin and myself may give a clue here. Thiswas a man of 49 with longstanding cardiachypertrophy and dilatation on a hypertensivebasis. He had had one episode of congestivefailure. At the time of study he was compen-sated at rest but his exercise tolerance wasmuch reduced.
so
z0
0i Q.il C 4
oc01o.
,*0
00* 0
0
00
00*
4
20 30 40 50 60
00
0
* 0
- - - - ^ - 70 60 90
Res Ex. / 2- - Minufes
FIG. 9. Pulmonary ventilation(see text).
3 4 5of Recovery--
of patient J. A.
dECAN PULMONARY ARTERIAL PRESSURE.mmyHg.. DURWG EXERCISE
FIG. 10. Relation between oxygen removal rate(uptake) in cubic centimeters per liter ventilation,and pulmonary arterial pressure, in 23 observationsin 20 rheumatic cardiac patients with diminishedcardiac reserve.
Their performance was as follows: a moderatecontinued hyperventilation, a relatively poor
increase in cardiac output in exercise, with a
rise in pulmonary arterial pressure. Since therewas some decrease in arterial carbon dioxidetension, a washing out of carbon dioxide by thehyperpnea, one could argue that some of thehyperventilation was on a "reflex" basis. Sofar as dyspnea is concerned, however, the actualincrease in ventilation was slight, much lessthan in our pulmonary cases previously de-scribed. This is shown in figure 7. Furthermore,maximum breathing capacity was relativelywell maintained, even with considerable in-crease in pulmonary arterial pressure. This isshown in figure 8. Thus breathing reserve was
not greatly diminished.Do we have then an adequate cause for the
In our study he endeavored to carry out amild 30-step exercise test, but could not finish,stopping after 16 steps only. Examination ofhis pulmonary function showed that his vitaland maximum breathing capacities were per-fectly normal both before and after the test;there was no abnormality either in arterialoxygen saturation or in carbon dioxide. Hispulmonary ventilation during the slight exer-tion was but little increased, actually signifi-cantly less than a normal subject with the1-minute step test, as shown in figure. 9. Closerinquiry revealed that he really was not stoppedbecause of dyspnea but because of fatigue orexhaustion. It was not cardiac pain; as a mat-ter of fact, when the patient finally died twoor three years later, he did not have signifi-cant coronary narrowing.
25
70 OO 90
by guest on January 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

NATURE OF CARDIAC AND OF PULMONARY DYSPNEA
What was the cause of this muscular exhaus-tion? We have found it, as have others, to bea prominent symptom in some of our cases ofadvanced mitral disease admitted for surgery,
and here it seems to be associated with very
low and fixed cardiac output. These patientsnotice it more acutely if they suddenly becomefree of the symptom after successful commis-surotomy. May it not be, therefore, that inade-quate blood flow manifests itself by this symp-
J. C. RHEUMATIC HEART DISEASE
concentration is used in these spot charts, inpreference to actual volumes of pulmonaryventilation, since it indicates the degree ofventilation or hyperventilation per unit of oxy-
gen absorbed, and therfore permits comparisonof values in individual subjects with differentoxygen intakes.The relation with cardiac output in exercise
is even more striking: there appears to be onlya moderate increase in ventilation (decreased
EH. MS. AF.
CL.D
j---,
0o cCO Z_ > -Vo
a 4
I-cc
cc
(9
Or
D
0n0n
0.(LI0
0
0
o
CI.
3.0
2.5
2.0
7080
5040
0
0
6 0
450
40
2 0V 0
W 20120
Z 0
:o
SV. + %
11¢S.V.
-0A + S.V.
S.v. + 7 % Ci.50 c.i .X
0~~~~~~~~~~~~~~~~~~~~~25.
NORMALI OF M2UOCONTROL MNUTIES OF MINUTES OF MINUTES OF MINUTES Of CONTROL MINUTES OF MNUTESAT REST EXERCISE. RECOVERY EXERCISE RECOVERY EXERCISE RECOVERY
PnW- nPorPTIVF' MO. POnRT-nPFRATIVF MOS. POST-OPERATIVE
FIG. 11. Patient J. C. before and after mitral commissurotomy. Lower three graphs indicate intra-
vascular and intracardiac pressures: pulmonary artery, end-diastolic in right ventricle, and brachialartery.
tom of fatigue, which has been mixed with,and yet is really separate from, the symptom ofdyspnea itself? Perhaps by a more exact andcareful clinical history, clinicians will be ableto identify this fatigue or exhaustion factor,as well as by complex laboratory tests.As the state of left ventricular failure ad-
vances, we find corresponding changes both inpulmonary and in cardiac measurements. Fig-ure 10 from West, Bliss, and Wood27 shows howthe oxygen concentration in expired air, whichis essentially the reciprocal of pulmonary ven-
tilation, decreases with rising pulmonarycongestive hypertension. Expired air oxygen
oxygen per cent) until cardiac output hasdropped to a really low value, below which thedegree of hyperpnea is markedly aggravated,presumably associated with hypoxia of brainand tissues. This is due in large part to retardedblood flow, though we are finding a fair numberof cases in which the acute pulmonary conges-tion of exercise is associated with some arterialanoxia, with therefore a further anoxic respira-tory stimulus. One wonders whether an abruptshift of this kind, in pressure or output, or
both, may not be the trigger that sets off an
attack of paroxysmal dyspnea or cardiacasthma, this in turn induced by some small
26
-Y,Mnt- UMtnAI||V C Mu. u |- rn
by guest on January 29, 2018http://circ.ahajournals.org/
Dow
nloaded from
DICKINSON W. RICHARDS, JR.
change in vascular fluid balance, vasomotorstate, or intercurrent infection, a small pul-monary embolus or other disturbance.
Effort of breathing is increased in pulmonarycongestion. This was well shown in the originalstudies of Christie and Meakins.28 By con-
tinuous intrapleural pressure recording, theyshowed markedly increased pressure swings be-tween inspiration and expiration, during con-
gestive failure, decreasing toward normal afterrecompensation.As for the important question whether the
pulmonary congestive state as such withoutalteration in cardiac output can be chiefly re-
sponsible for the disabling symptoms of ad-vanced left heart failure, we believe that we
have a definitive answer from some of our
studies of mitral disease before and after com-
missurotomy. The following case is taken froma recent report29:The patient, an electrician of 38, had had in-
creasing exertional dyspnea, with attacks ofparoxysmal dyspnea, for two years, and at thetime of admission had been totally disabled forsix months, was orthopneic, dyspneic on talk-ing or the least exertion in the hospital. Hehad auricular fibrillation and mitral stenosis.Figure 11 shows his cardiodynamics pre- andpostoperatively. You will see preoperativelya low cardiac output, which failed to increaseon exercise, and a marked pulmonary hyper-tension, which rose further during and for a
time following the exercise test.In the next column of this figure are the
measurements one month after a successfulcommissurotomy. The patient at this time was
clinically well, with no dyspnea, no orthopnea,able to climb two flights of stairs, though hisexercise tolerance was still significantly reduced.From the measurements you will see that whilethere was a slight increase in resting cardiacoutput, this did not increase further in exer-
cise. The major change was the considerabledrop in pulmonary vascular hypertension. Thepoint here, therefore, is that pulmonary con-
gestion would appear to be the chief and keydisability in some at least of these cases ofrheumatic heart disease in failure, and that itsrelief restores the patient to clinical compensa-
tion on limited activity.
The last column in figure 11 shows how 11months later, this patient had made definitefurther improvement with even lower pul-monary vascular pressures and a better cardiacoutput. Now the patient had returned to nor-mal activity in practically all respects.The forms of dyspnea in far advanced con-
gestive failure need not detain us long. Or-thopnea, one of the standbys in differentiatingcardiac from pulmonary dyspnea, seems at leastpartly explained since we know that the supineposition brings more blood to the heart andlungs, adds to an already excessive cardiacfilling, increases pulmonary congestion, de-creases vital capacity and breathing capacity.The increased tachypnea and hyperpnea in
advanced heart failure raises again the ques-tion of reflex factors in lungs, great vessels orelsewhere, but again the marked and consistentrelief obtained by oxygen therapy brings usback to a basic chemical control.
Cardiac asthma, sometimes truly asthmaticin form, is still basically an acute pulmonarycongestion. While it may respond to broncho-dilators, its relief more often depends upon theuse of oxygen, frequently with positive pres-sure, upon digitalization, sedation, and diu-retics.
Cheyne-Stokes respiration in heart failurehas not been sufficiently explained. We knowthat it occurs clinically in advanced failurewith retarded circulation, more in arterioscle-rotic or cardiorenal forms than in rheumatic,that it never occurs in the dyspnea of chronicpulmonary disease. We can measure the anoxiaand hypercapnia in the apneic phase and thehypocapnia in the hyperpneic; we can stopit by breathing carbon dioxide, occasionallyby breathing oxygen. The exact chemical anddynamic circumstances that determine its on-set, however, or the true relation between thisand experimental periodic breathing of centralnervous, or anoxic, or hypocapneic origin, arenot known.My last case and final point in this presenta-
tion concerns the patient bedeviled all his lifeby a cardiac murmur. It brings us back againto our starting point, the importance of con-sidering the whole patient in the analysis ofhis clinical state. There is nothing new about
27
by guest on January 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

NATURE OF CARDIAC AND OF PULMONARY DYSPINEA
this. Dr. Conner's fine paper 20 years ago onthe psychic factors in cardiac disorders30pointed the way. Various recent writers havereferred to "iatrogenic" heart disease, an ex-cellent term. We have encountered some fla-grant examples, as others doubtless have also, inexamining cases referred for cardiac surgery.They are individuals with a story of severeexertional dyspnea who have been found tohave entirely normal cardiac and pulmonaryfunction, both at rest and on the standardexercise test. Going back to the patient again,we have found that having had a cardiac mur-
W.G. RHD. EH. MS. MI. NSR. IA.
QO . C.I.
i ° 4.0
< F 3.0
U 4
Lic<icc 70I m
On
Li
W
(I)OnLI
0
0
0Ja]
3 0
-X a: 2 0
_J < 0
* 0
z _io
> 5
a crCC(
150_
ccO
I W o o
a: <m 50
S.v 4
-90 +4
...0
0
467 1012 1314NORMAL CONTROL 4 OF MINUTES OF
AT REST E X ERCISE RECOVERY
FIG. 12. Patient W. G. Dynamics of circulation.
mur all his life, the patient has not been allowedexertion to the point of even normal breathless-ness. He has suffered not from dyspnea, butthe fear of dyspnea. Figure 12 shows the meas-
urements on one such patient in rest and exer-
cise. Perhaps as great satisfaction as we havehad in our physiologic studies has been thedemonstration to these patients that they needno severe restriction, but can lead essentiallynormal lives.
It may seem inconsistent that I am arguingfor more emphasis on the psychogenic factorin cardiac dyspnea, and less in pulmonarydyspnea. My impression may be mistaken, but
it has been, in fact, that the diagnosis ofneurosis is made rather too often in chronicpulmonary disease and perhaps not oftenenough in rheumatic heart disease with a valvu-lar murmur but no failure.
In summary, I should like to stress the fol-lowing:
1. Dyspnea, or distressed breathing, is a verydifferent entity from one disease to another,and its special qualities in each deserve bothphysiologic and clinical analysis.
2. In general, it can be thought of as a balancebetween breathing capacity and breathing ef-fort, on the one hand, and on the other, theactual ventilation produced by the existingrespiratory stimulus.
3. The multiple or summation theory ofrespiratory stimulus has made a significantcontribution to our understanding of dyspnea.
4. Hyperventilation is common both to pul-monary and to cardiac dyspnea, often morepronounced in the former.
5. One should be cautious in explaining dysp-nea on a functional or neurotic basis whenorganic pulmonary disease is present.
6. In cardiac dyspnea, the factor of muscularexhaustion, due to reduced blood flow, may besignificant.
7. Pulmonary hypertension and congestionmay be the chief element producing symptomsin advanced left-sided congestive failure.
8. In general, the dyspnea of mild cardiacfailure appears to be due chiefly to inadequatecardiac output; that of advanced congestivefailure to pulmonary congestion.
9. "Iatrogenic" heart disease still occurs;that is, the patient with a cardiac murmurwhose physical activity is needlessly restricted.
SUMARIo ESPA OL
Disnea tiene muchas caracteristicas que di-fieren de un estado clinico a otro. En enfer-medades pulmonares la causa inmediata esusualmente una desproporcion entre la venti-laci6n actual y la capacidad respiratoria. Lahiperventilacion de enfermedad pulmonar or-ganica es frecuentemente confundida con psico-neurosis. En disnea cardiaca temprana, cansan-cio muscular con una produccion total cardiacainsuficiente puede que sea un factor. Conges-
28
by guest on January 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

DICKINSON W. RICHARDS, JR.
tion pulmonar es un factor importante en casos
mas avanzados de decompensacion del ventri-culo izquierdo.
REFERENCES
WHITEHEAD, A. N.: Science and the ModernWorld. New York, Macmillan, 1925.
2 COURNAND, A., AND RICHARDS, D. W., JR.: Pul-monary insufficiency. Discussion of a physi-ological classification and presentation of clinicaltests. Am. Rev. Tuberc. 44: 26, 1941.
'MEANS, J. H.: Dyspnea. Medicine 3: 309, 1924.4HERMANNSEN, J.: Untersuchungen ueber die maxi-
male Ventilations-groesse (Atemgrenzwert).Ztschr. ges. exper. Med. 90: 130, 1933.
5 GAENSLER, E. A.: Air velocity index, a numericalexpression of the functionally effective portionof ventilation. Am. Rev. Tuberc. 62: 17, 1950.
6SCHMIDT, W., AND GAUBATZ, E.: SpirometrischeFunktionspruefungen von Herz und Kreislauf,in Kollapstherapie der Lungentuberkulose.Leipzig, Thieme, 1938.
7 ANTHONY, A. J.: Funktionspruefung der Atmung.Leipzig, Barth, 1937.
8 KNIPPING, H. W., AND MONCRIEFF, A.: Theventilation equivalent for oxygen. Quart. J.Med. 1:17, 1932.
9 -: Dyspnoe. Beitr. Klin. Tuberk. 82: 133, 1933.10WRIGHT, G. W., AND FILLEY, G. F.: Pulmonary
fibrosis and respiratory function. Am. J. Med.10: 642, 1951.
-: Industrial pulmonary diseases and capacity forwork. Occup. Med. 2: 546, 1946.
12 SONNE, C.: Respiratory air exchange in the lungsunder normal and pathological conditions. Actamed. scandinav., Suppl. 59: 348, 1934.
13 BALDWIN, E. DEF., COURNAND, A., AND RICHARDS,D. W., JR.: Pulmonary insufficiency. II. Astudy of 39 cases of pulmonary fibrosis. Medi-cine 28: 1, 1949.
4aMEAKINS, J. C., AND DAVIES, H. W.: Respiratoryfunction in disease. London, 1925.
14b Scott, R. W.: Observations on the pathologicphysiology of chronic pulmonary emphysema.Arch. Int. Med. 26: 544, 1920.
15HENDERSON, L. J.: Blood: a Study in GeneralPhysiology. New Haven, Yale University Press,1928.
16GRAY, J. S.: Pulmonary Ventilation and Its Phys-iological Regulation. Springfield, Ill. Thomas,1950.
17 HESS, W. R.: Die Regulierung der Atmung. Leip-
zig, Thieme, 1931. Fleisch, A.: Neuere Ergeb-nisse ueber Methodik und proprioceptive Steu-erung der Atmungsbewegungen. Ergebn. Phys-iol. 36: 249, 1934. Christie, R. V.: Dyspnoea,a Review. Quart. J. Med. 7: 422, 1938.
18 GALDSTON, M., LUETSCHER, J. A., JR., LONG-COPE, W. T., AND BALLICH, N. L.: A study of theresidual effects of phosgene poisoning in humansubjects. I. After acute poisoning. J. Clin.Investigation 26: 145, 1947.
19HAMMAN, L., AND RICH, A. R.: Acute diffuseinterstitial fibrosis of the lungs. Bull. JohnsHopkins Hosp. 74: 177, 1944.
20 CHRISTIE, R. V.: The elastic properties of theemphysematous lung and their clinical signifi-cance. J. Clin. Investigation 13: 295, 1934.
21 COURNAND, A., BROCK, H. J., RAPPAPORT, I., ANDRICHARDS, D. W., JR.: Disturbance of action ofrespiratory muscles as a contributing cause ofdyspnea. Arch. Int. Med. 57: 1, 1936.
22 BALDWIN, E. DEF., COURNAND, A., AND RICHARDS,D. W., JR.: Pulmonary insufficiency. III. Astudy of 122 cases of chronic pulmonary em-physema. Medicine 28: 201, 1949.
23 HARRISON, T. R.: Failure of the Circulation.Baltimore, Williams & Wilkins, 1935.
24 VON BASCH, S. S. K.: Die cardiale Dyspnoe unddas cardiale Asthma. Klin. Zeit. und Streits-fragen, 1887. P. 82.
25PEABODY, F. WV.: Cardiac dyspnea. Harvey Lec-tures 12: 248, 1916.
21 HICKAM, J. B., AND CARGILL, WV. H.: The effect ofexercise on cardiac output and pulmonary ar-terial pressure in normal persons and in patientswith cardiovascular disease and pulmonary em-physema. J. Clin. Investigation 27: 10, 1948.
27 WEST, J. R., BLISS, H. A., AND WOOD, J. C.: Tobe published.
28 CHRISTIE, R. V., AND MEAKINS, J. C.: The in-trapleural pressure in congestive heart failureand its clinical significance. J. Clin. Investiga-tion 13: 323, 1934.
29 RICHARDS, D. W., JR., HARVEY, R. M., FERRER,M. I., WEST, J. R., CATHCART, R. T., ANDCOURNAND, A.: The influence of mitral valvulardisease of rheumatic origin upon the dynamicsof the circulation, with special reference toindications for surgery. First World Congressof Cardiology, 1950. Tome III, p. 190, Paris,1952.
30 CONNER, L. A.: Psychic factors in cardiac dis-orders. J. A. NI. A. 94: 447, 1930.
29
by guest on January 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

DICKINSON W. RICHARDS, JR.Dyspnea
The Lewis A. Conner Memorial Lecture: The Nature of Cardiac and of Pulmonary
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1953 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.7.1.15
1953;7:15-29Circulation.
http://circ.ahajournals.org/content/7/1/15the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document.
Permissions and Rights Question and Answer Further information about this process is available in therequested is located, click Request Permissions in the middle column of the Web page under Services.the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright Clearance Center, notCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on January 29, 2018http://circ.ahajournals.org/
Dow
nloaded from