the icare rebound tonometer: comparisons with goldmann tonometry, and influence of central corneal...
TRANSCRIPT

Original Article
The iCare rebound tonometer: comparisons withGoldmann tonometry, and influence of centralcorneal thicknessceo_2109 687..691
Ali Poostchi MBChB,1,2 Robert Mitchell MBChB,1 Simon Nicholas MBChB,1,2 Gordon Purdie BSc3 andAnthony Wells FRANZCO1,2
1Department of Ophthalmology, Wellington Hospital, 2Capital Eye Specialists, and 3Department of Public Health, Wellington School ofMedicine, Wellington, New Zealand
ABSTRACT
Purpose: To assess agreement between the iCarerebound tonometer and Goldmann tonometry andto assess the influence of central corneal thick-ness and the value of scleral rebound tonometerreadings.
Methods: Prospective single-centre cross-sectionalstudy comparing iCare rebound tonometer (RT)intraocular pressure (IOP) readings taken fromcorneal and scleral locations to Goldmann applana-tion tonometer (GAT) readings in 100 subjectsattending ophthalmology clinics.
Results: There was a significant difference betweenRT and GAT, with RT tending to overestimate IOP.The mean difference between RT and GAT measure-ments was 3.36 mmHg. The mean differencebetween the log of RT and the log of GAT measure-ments was 0.2356, a ratio of 1.27 (P < 0.0001). Aformula derived from a linear regression analysissuggested that a 10% increase in CCT increased theRT IOP reading by 9.9%. Scleral RT readings showedno relationship to GAT readings.
Conclusions: The rebound tonometer cannot replacethe Goldmann tonometer in the office setting giventhe wide limits of agreement between the twodevices. Corneal rebound tonometer readings areinfluenced by CCT whereas scleral rebound tonom-eter readings are of no value.
Key words: Goldmann tonometry, iCare reboundtonometer, intraocular pressure.
INTRODUCTION
Accurate determination of intraocular pressure (IOP)is vital in the investigation of glaucoma and isclassically measured using Goldmann applanationtonometer (GAT).1 This device is seen as the goldstandard and infers IOP from the force required toflatten a predetermined area of central cornea. Unsur-prisingly, it is known to be affected by changes incentral corneal thickness (CCT), structure andcurvature.2 It further requires a slit-lamp set up,topical anaesthesia and an experienced examiner. Bycontrast, the iCare rebound tonometer (RT) is por-table, does not require anaesthesia and can be reli-ably used with little experience.3,4 It uses theprinciple of rebound tonometry whereby a magne-tized steel probe with a rounded plastic tip isbounced off the cornea and creates an electricalinduction current as it returns to the machine. Thiscurrent is used to calculate the deceleration of probeon the cornea from which is derived the IOP.5
Scleral measurements of IOP may be desirable incases of corneal pathology or where the patient isaverse to corneal measurements. Recently, two otherportable tonometers have been introduced. TheTGDc01’PRA’ (Ryazan State Instrument-Making)and the Proview Phosphene Tonometer both deter-mine IOP through transpalpebral measurementsinvolving the sclera. There may also be role inassessing the biomechanical response of the scleral
� Correspondence: Dr Simon Nicholas, 10 Catherine Cres, Paparangi, Wellington, New Zealand. Email: [email protected]
Received 1 April 2009; accepted 30 June 2009.
Clinical and Experimental Ophthalmology 2009; 37: 687–691 doi: 10.1111/j.1442-9071.2009.02109.x
© 2009 The AuthorsJournal compilation © 2009 Royal Australian and New Zealand College of Ophthalmologists
shell. This study was designed to assess the agree-ment between the Goldmann and iCare tonometers,the effect of CCT and reliability of scleral reboundtonometry measurements.
METHODS
One hundred patients without corneal disease wererecruited from Ophthalmology clinics at WellingtonPublic Hospital. One eye of each patient was ran-domly selected for sampling. An experienced exam-iner measured IOP twice in the selected eye usingthe GAT first and then the RT. RT measurementsconsisted of six consecutive readings. The primaryset of measurements was taken from the centralcornea. A second set was taken from the inferiorsclera, approximately 4 mm from the limbus withthe patients gaze directed superiorly. RT readingswere repeated if the machine indicated that the stan-dard deviation of readings was greater than normal.All IOP measurements for each subject were con-ducted within a 5 min period by the same experi-enced examiner. The tonometers used were regularlycalibrated according to manufacturer’s instructions.After the IOP measurements had been taken, thesame examiner measured the CCT using a Pachmatepachymeter (DGH technology, Exton, PA, USA).
The study adhered to the tenets of the Declarationof Helsinki and was approved by our local ethicscommittee.
Intermethod agreement was assessed using themethod described by Bland and Altman.6,7
Coefficients of repeatability and limits of agree-ment were used to assess intra- and inter-methodvariation. Linear regression was used to evaluate theinfluence of corneal thickness on tonometry. Pearsoncorrelation coefficients were determined and differ-ences compared with a paired t-test. As the measure-ments were more consistent with a log-normal thana normal distribution, these analyses were made onthe log-transformed measurement. The level of sig-nificance for each test was set at P < 0.05. All statis-tical analysis was performed using Microsoft Excel2002 (Microsoft Corporation, USA) and SAS (SASInstitute Inc., Cary, NC, USA).
RESULTS
One hundred patients were included in this study,57 male and 43 female, with a mean age of 54 years(range 9–84). There were 53 right eyes and 47 lefteyes tested.
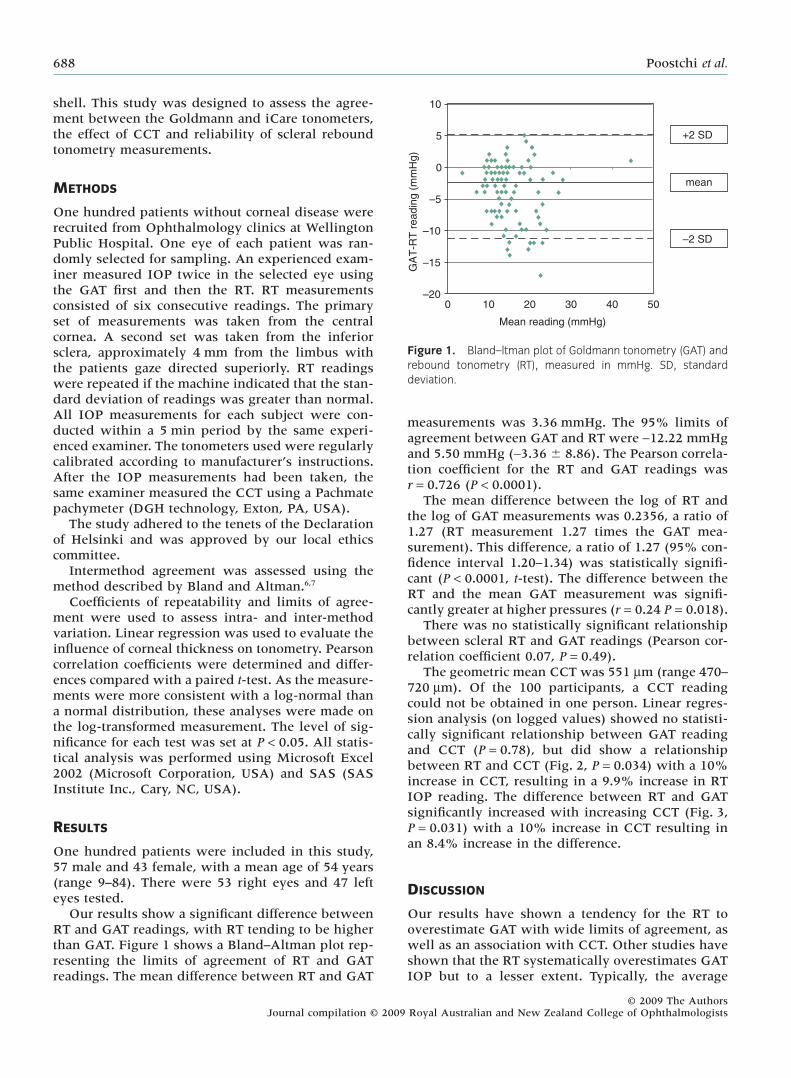
Our results show a significant difference betweenRT and GAT readings, with RT tending to be higherthan GAT. Figure 1 shows a Bland–Altman plot rep-resenting the limits of agreement of RT and GATreadings. The mean difference between RT and GAT
measurements was 3.36 mmHg. The 95% limits ofagreement between GAT and RT were -12.22 mmHgand 5.50 mmHg (-3.36 � 8.86). The Pearson correla-tion coefficient for the RT and GAT readings wasr = 0.726 (P < 0.0001).
The mean difference between the log of RT andthe log of GAT measurements was 0.2356, a ratio of1.27 (RT measurement 1.27 times the GAT mea-surement). This difference, a ratio of 1.27 (95% con-fidence interval 1.20–1.34) was statistically signifi-cant (P < 0.0001, t-test). The difference between theRT and the mean GAT measurement was signifi-cantly greater at higher pressures (r = 0.24 P = 0.018).
There was no statistically significant relationshipbetween scleral RT and GAT readings (Pearson cor-relation coefficient 0.07, P = 0.49).
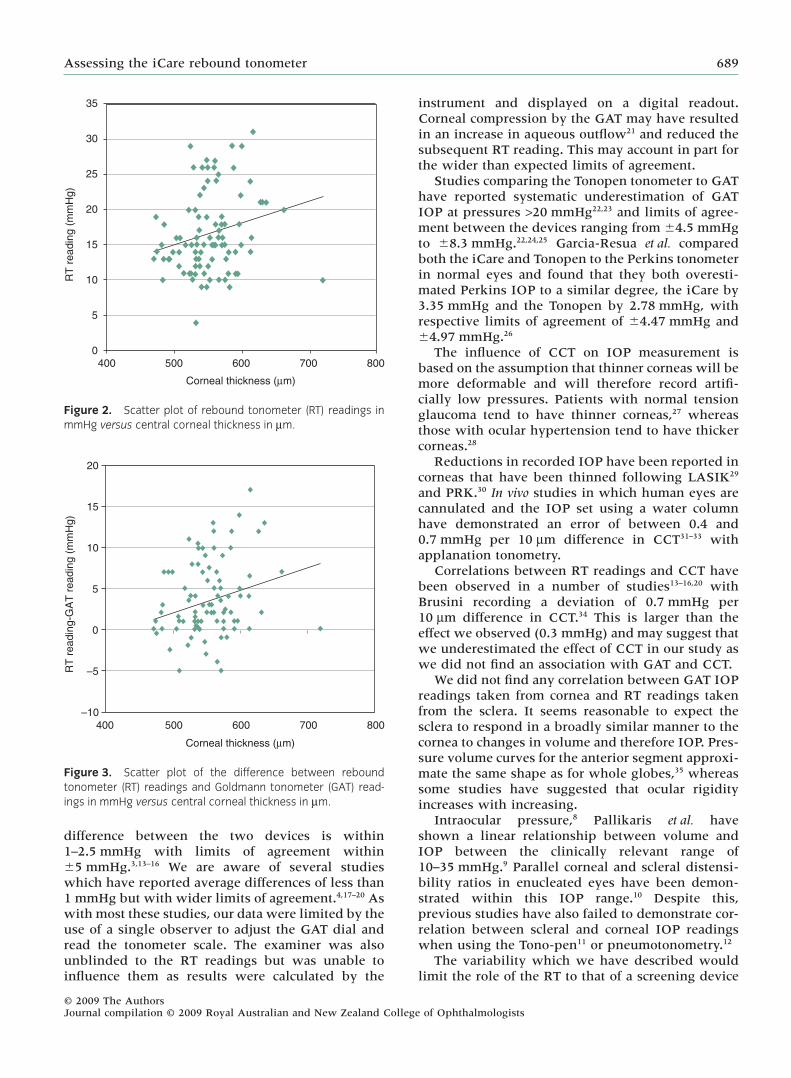
The geometric mean CCT was 551 mm (range 470–720 mm). Of the 100 participants, a CCT readingcould not be obtained in one person. Linear regres-sion analysis (on logged values) showed no statisti-cally significant relationship between GAT readingand CCT (P = 0.78), but did show a relationshipbetween RT and CCT (Fig. 2, P = 0.034) with a 10%increase in CCT, resulting in a 9.9% increase in RTIOP reading. The difference between RT and GATsignificantly increased with increasing CCT (Fig. 3,P = 0.031) with a 10% increase in CCT resulting inan 8.4% increase in the difference.
DISCUSSION
Our results have shown a tendency for the RT tooverestimate GAT with wide limits of agreement, aswell as an association with CCT. Other studies haveshown that the RT systematically overestimates GATIOP but to a lesser extent. Typically, the average
10
5
0
–5
–10
–15
–200 10 20 30 40 50
Mean reading (mmHg)
GA
T-R
T r
ea
din
g (
mm
Hg
)
+2 SD
–2 SD
mean
Figure 1. Bland–ltman plot of Goldmann tonometry (GAT) andrebound tonometry (RT), measured in mmHg. SD, standarddeviation.
688 Poostchi et al.
© 2009 The AuthorsJournal compilation © 2009 Royal Australian and New Zealand College of Ophthalmologists
difference between the two devices is within1–2.5 mmHg with limits of agreement within�5 mmHg.3,13–16 We are aware of several studieswhich have reported average differences of less than1 mmHg but with wider limits of agreement.4,17–20 Aswith most these studies, our data were limited by theuse of a single observer to adjust the GAT dial andread the tonometer scale. The examiner was alsounblinded to the RT readings but was unable toinfluence them as results were calculated by the
instrument and displayed on a digital readout.Corneal compression by the GAT may have resultedin an increase in aqueous outflow21 and reduced thesubsequent RT reading. This may account in part forthe wider than expected limits of agreement.
Studies comparing the Tonopen tonometer to GAThave reported systematic underestimation of GATIOP at pressures >20 mmHg22,23 and limits of agree-ment between the devices ranging from �4.5 mmHgto �8.3 mmHg.22,24,25 Garcia-Resua et al. comparedboth the iCare and Tonopen to the Perkins tonometerin normal eyes and found that they both overesti-mated Perkins IOP to a similar degree, the iCare by3.35 mmHg and the Tonopen by 2.78 mmHg, withrespective limits of agreement of �4.47 mmHg and�4.97 mmHg.26
The influence of CCT on IOP measurement isbased on the assumption that thinner corneas will bemore deformable and will therefore record artifi-cially low pressures. Patients with normal tensionglaucoma tend to have thinner corneas,27 whereasthose with ocular hypertension tend to have thickercorneas.28
Reductions in recorded IOP have been reported incorneas that have been thinned following LASIK29
and PRK.30 In vivo studies in which human eyes arecannulated and the IOP set using a water columnhave demonstrated an error of between 0.4 and0.7 mmHg per 10 mm difference in CCT31–33 withapplanation tonometry.
Correlations between RT readings and CCT havebeen observed in a number of studies13–16,20 withBrusini recording a deviation of 0.7 mmHg per10 mm difference in CCT.34 This is larger than theeffect we observed (0.3 mmHg) and may suggest thatwe underestimated the effect of CCT in our study aswe did not find an association with GAT and CCT.
We did not find any correlation between GAT IOPreadings taken from cornea and RT readings takenfrom the sclera. It seems reasonable to expect thesclera to respond in a broadly similar manner to thecornea to changes in volume and therefore IOP. Pres-sure volume curves for the anterior segment approxi-mate the same shape as for whole globes,35 whereassome studies have suggested that ocular rigidityincreases with increasing.
Intraocular pressure,8 Pallikaris et al. haveshown a linear relationship between volume andIOP between the clinically relevant range of10–35 mmHg.9 Parallel corneal and scleral distensi-bility ratios in enucleated eyes have been demon-strated within this IOP range.10 Despite this,previous studies have also failed to demonstrate cor-relation between scleral and corneal IOP readingswhen using the Tono-pen11 or pneumotonometry.12
The variability which we have described wouldlimit the role of the RT to that of a screening device
35
30
25
20
15
10
5
0400 500 600 700 800
Corneal thickness (μm)
RT
readin
g (
mm
Hg)
Figure 2. Scatter plot of rebound tonometer (RT) readings inmmHg versus central corneal thickness in mm.
Corneal thickness (μm)
RT
readin
g-G
AT
readin
g (
mm
Hg)
20
15
10
5
0
–5
–10
400 500 600 700 800
Figure 3. Scatter plot of the difference between reboundtonometer (RT) readings and Goldmann tonometer (GAT) read-ings in mmHg versus central corneal thickness in mm.
Assessing the iCare rebound tonometer 689
© 2009 The AuthorsJournal compilation © 2009 Royal Australian and New Zealand College of Ophthalmologists

and even then it should be used in combination withpachymetry or measures of corneal biomechanics.Other authors have indicated that it compares wellwith the Tonopen and its portability, ease of use andtolerability may make it useful in paediatric andelderly populations. Scleral measurements using theRT appear to be of no value.
ACKNOWLEDGEMENTS
We would like to acknowledge the support of theCapital Vision Research Trust and of Designs forVision (DFV, New Zealand).
REFERENCES
1. Kass MA. Standardizing the measurement of intraocu-lar pressure for clinical research. Guidelines from theEye Care Technology forum. Ophthalmology 1996; 103:183–5.
2. Whitacre MM, Stein R. Sources of error with use ofGoldmann-type tonometers. Surv Ophthalmol 1993; 38:1–30.
3. Detry-Morel M, Jamart J, Detry MB et al. Clinicalevaluation of the dynamic rebound tonometer ICare.J Fr Ophtalmol 2006; 29: 1119–27.
4. Abraham LM, Epasinghe NC, Selva D, Casson R. Com-parison of the ICare((R)) rebound tonometer withthe Goldmann applanation tonometer by experi-enced and inexperienced tonometrists. Eye 2008; 22:503–6.
5. Kontiola AI, Goldblum D, Mittag T, Danias J. Theinduction/impact tonometer: a new instrument tomeasure intraocular pressure in the rat. Exp Eye Res2000; 73: 781–5.
6. Bland JM, Altman DG. Statistical methods for assess-ing agreement between two methods of clinicalmeasurement. Lancet 1986; 1: 307–10.
7. Bland JM, Altman DG. Agreement between methodsof measurement with multiple observations perindividual. J Biopharm Stat 2007; 17: 571–82.
8. Silver DM, Geyer O. Pressure-volume relation for theliving human eye. Curr Eye Res 2000; 20: 115–20.
9. Pallikaris IG, Kymionis GD, Ginis HS, Kounis GA,Tsilimbaris MK. Ocular rigidity in living human eyes.Invest Ophthalmol Vis Sci 2005; 46: 409–14.
10. Richards RD, Tittel PG. Corneal and scleral distensi-bility ratio on enucleated human eyes. Invest OphthalmolVis Sci 1973; 12: 836–9.
11. Kolin T, Wedemeyer LL, Kolin E, Braun Y. Compari-son of scleral and corneal Tono-Pen readings. J AAPOS2003; 7: 291–2.
12. Breitfeller JM, Krohn DL. Limbal pneumatonometry.Am J Ophthalmol 1980; 89: 344–52.
13. Iliev ME, Goldblum D, Katsoulis K, Amstutz C, FruehB. Comparison of rebound tonometry with Goldmannapplanation tonometry and correlation with cen-tral corneal thickness. Br J Ophthalmol 2006; 90:833–5.
14. Nakamura M, Darhad U, Tatsumi Y et al. Agreement ofrebound tonometer in measuring intraocular pressurewith three types of applanation tonometers. Am J Oph-thalmol 2006; 142: 332–4.
15. Fernandes P, Diaz-Rey JA, Queiros A, Gonzalez-Meijome JM, Jorge J. Comparison of the ICarerebound tonometer with the Goldmann tonometer in anormal population. Ophthalmic Physiol Opt 2005; 25:436–40.
16. Martinez-de-la-Casa JM, Garcia-Feijoo J, Castillo A,Garcia-Sanchez J. Reproducibility and clinical evalu-ation of rebound tonometry. Invest Ophthalmol Vis Sci2005; 46: 4578–80.
17. Davies LN, Bartlett H, Mallen EA, Wolffsohn JS. Clini-cal evaluation of rebound tonometer. Acta OphthalmolScand 2006; 84: 206–9.
18. Van der Jagt LH, Jansonius NM. Three portabletonometers, the TGDc-01, the ICARE and the TonopenXL, compared with each other and with Goldmannapplanation tonometry. Ophthalmic Physiol Opt 2005; 25:429–35.
19. Schreiber W, Vorwerk CK, Langenbucher A, Behrens-Baumann W, Viestenz A. A comparison of reboundtonometry (ICare) with TonoPenXL and Goldmannapplanation tonometry. Ophthalmologe 2007; 104: 299–304.
20. Pakrou N, Gray T, Mills R, Landers J, Craig J. Clinicalcomparison of the Icare tonometer and Goldmannapplanation tonometry. J Glaucoma 2008; 17: 43–7.
21. Krakau CE, Wilke K. On repeated tonometry. Acta Oph-thalmol (Copenh) 1971; 49: 658–71.
22. Iester M, Mermoud A, Achache F, Roy S. NewTonopen XL: comparison with the Goldmanntonometer. Eye 2001; 15: 52–8.
23. Horowitz GS, Byles J, Lee J, D’Este C. Comparison ofthe Tono-Pen and Goldmann tonometer for measuringintraocular pressure in patients with glaucoma. ClinExperiment Ophthalmol 2004; 32: 584–9.
24. Bafa M, Lambrinakis I, Dayan M, Birch M. Clinicalcomparison of the measurement of the IOP with theocular blood flow tonometer, the Tonopen XL and theGoldmann applanation tonometer. Acta OphthalmolScand 2001; 79: 15–8.
25. Midelfart A, Wigers A. Clinical comparison of theProTon and Tono-Pen tonometers with the Goldmannapplanation tonometer. Br J Ophthalmol 1994; 78: 895–8.
26. Garcia-Resua C, Gonzalez-Meijome JM, Gilino J,Yebra-Pimentel E. Accuracy of the new Icare reboundtonometer vs other portable tonometers in healthyeyes. Optom Vis Sci 2006; 83: 102–7.
27. Shah S, Chatterjee A, Mathai M et al. Relationshipbetween corneal thickness and measured intraocularpressure in a general ophthalmology clinic. Ophthal-mology 1999; 106: 2154–60.
28. Herndon LW, Choudhri SA, Cox T, Damji KF, ShieldsMB, Allingham RR. Central corneal thickness innormal, glaucomatous, and ocular hypertensive eyes.Arch Ophthalmol 1997; 115: 1137–41.
29. Emara B, Probst LE, Tingey DP, Kennedy DW, WillmsLJ, Machat J. Correlation of intraocular pressure and
690 Poostchi et al.
© 2009 The AuthorsJournal compilation © 2009 Royal Australian and New Zealand College of Ophthalmologists

central corneal thickness in normal myopic eyes andafter laser in situ keratomileusis. J Cataract Refract Surg1998; 24: 1320–5.
30. Schipper I, Senn P, Oyo-Szerenyi K, Peter R. Centraland peripheral pressure measurements with the Gold-mann tonometer and Tono-Pen after photorefractivekeratectomy for myopia. J Cataract Refract Surg 2000; 26:929–33.
31. Ehlers N, Bramsen T, Sperling S. Applanation tonom-etry and central corneal thickness. Acta Ophthalmol(Copenh) 1975; 53: 34–43.
32. Kohlhaas M, Boehm AG, Spoerl E, Pursten A, GreinHJ, Pillunat LE. Effect of central corneal thickness,
corneal curvature, and axial length on applanationtonometry. Arch Ophthalmol 2006; 124: 471–6.
33. Whitacre MM, Stein RA, Hassanein K. The effect ofcorneal thickness on applanation tonometry. Am J Oph-thalmol 1993; 115: 592–6.
34. Brusini P, Salvetat ML, Zeppieri M, Tosoni C, Parisi L.Comparison of ICare tonometer with Goldmannapplanation tonometer in glaucoma patients.J Glaucoma 2006; 15: 213–17.
35. Browning AC, Bhan A, Rotchford AP, Shah S, Dua HS.The effect of corneal thickness on intraocular pressuremeasurement in patients with corneal pathology. Br JOphthalmol 2004; 88: 1395–9.
Assessing the iCare rebound tonometer 691
© 2009 The AuthorsJournal compilation © 2009 Royal Australian and New Zealand College of Ophthalmologists