glaukoma br5 13 - aeon astron humphrey field analyzer ii 745 (carl zeiss, meditec, dublin, ca, usa)....
TRANSCRIPT


��������
224
240
246
251
259
267
272
CONTENTS
B U L G A R I A N F O R U M
G L A U C O M AEdition of the ãNational Academy GlaucomaÓ Foundation, Sofia, Bulgaria
SURGICAL TREATMENT1. Ex-PRESS¨ and OlogenTM - single step implantation of two implants with a different mechanism of actionin glaucoma surgery
B. Anguelov
PSEUDOEXFOLIATION SYNDROME
2. Systemic diseases in pseudoexfoliation syndrome
G. Hollo, P. Kothy
GLAUCOMA - PATHOGENESIS3. Production of cyclooxsygense-1 and -2 in human heal-thy and glaucomatous eyes and role of prostaglandin E
2
B. Anguelov, B. Mihaylova
DIAGNOSTICS4. Cross-impact degree and characteristics of the mor-pho functional correlation between primary open-angle glaucoma and age-related macular dege ne-ration
Avdeev R.V., Alexandrov A.S., Basinsky A.S., BlyumE.A., Brezhnev A.Yu., Volkov E.N., Galimova A.B.,Gaponko O.V., Garkavenko V.V., Getmanova A.M.,Gorodnichy V.V., Gusarevitch A.A., Diordiychuk S.V., Dorofeev D.A., Zavadsky P.Ch., Zvereva O.G.,Karimov U.P., Kulik A.V., Kuroyedov A.V., LaninS.N., Lovpache Dzh.N., Loskutov I.A., MolchanovaE.V., Onufrichuk O.N., Ogorodnikova V.Yu., PetrovS.Yu., Rozhko Yu.I., Sidenko T.A.
5. New system for stage determination of thestructural changes in primary open-angle glaucomabased on morphometric analysis of the optic diskperformed by Heidelberg Retina Tomograph II(version 3.1.2)
B. Anguelov, A. Toshev
6. Use of nuclear magnetic resonance in cases ofadvanced glaucoma
B. Gagova, K. Stoyanova, N. Dakov, B. Anguelov
CLINICAL GENETICS7. Changes in anterior eye segment in childrenwith glaucoma attending some common hereditarydiseasesA. Popova
���� ��� ���1. Ex-PRESS¨ � OlogenTM - e��������� ��������� ����� �������� � ��� ��!�� ��"����#� �� ��$����� �%��&'������ "��&� %���. ������
*�+��/�0���4+� �����52. Systemische Krankheiten im Pseudoexfoliationssyndrom
G. Hollo, P. Kothy
���/�5� - *�4� �6�
3. *���&'7�� �� 7�'���'��%�����-1 � -2 � ������ �%��&'���� !���8'� �!� � ���� �� ������%������ E
2
�. ������, �. �� ���
�� ���4/�4. � ������� �������%� ������� � "���' �����-��'�" ���9�9&�'7�����:�;" ����������8���$��<�& �����!��$ ��'�;��&%��:��$ %��&'���$ � ��'&��������9��$
���� �.�., ����� ���� �.�., � ������� �.�.,���� �.�., ������ �.�., ����� �.�., � ���� �.�., � ������ �.�., � ��� ���� �.�., ��!� �� �.., �������"�� �.�., �#� ���" �.�., $������-"#� �.�., $���%�� $.�., & ����� '.(., &��� �.�., ) ���� *.�., )#��� �.�., )#����� �.�.,+ ��� �.�., +�� "� $�.�., +���#!� /.�.,��" �� �.�., ��#%���"#� �.�., ���������� �.�., '�!�� �.�., ����� �./., ������� 0.�.
5. ���� ������� �� ���������� ������ �� ���&'-�&����� ��������� ��� �#���!�� ��'����#%#���%��&'��� =������a �� ���9������!�� ������ �����'� �� ��������� ���� ���#�8�� � ��$���=��%������� ����%��9 II (������ 3.1.2)
�. ������, �. 0�8�
6. +#���<����� �� ������������ � ������-��%��-��� �������� ��� ��&!�� � ���������� %��&'���
�. � �� , ). �!�9�� , �. $ ��, �. ������
/����� �4/�7. *������ � ������� �!�� ��%���� ��� ��7�� %��&'��� �#�#�����>� ��'�� �������������=>� ��=���������. '���
Õ Õ Õ Õ
��+� ���/4��:
$�:. �-� ��!�� ������, �.�./������ �� �9�������%��, 5�
�5@�� ã���'��������'�Ó, ��9��, @#�%����
Assoc. Prof. Botio Anguelov, MD, PhDDepartment of Ophthalmology, Medical University
ãAlexandrovskaÓ Hospital, Sofia, Bulgaria
EDITOR-IN-CHIEF:
���/J���� /�� Q: EDITORIAL BOARD:
'��%. �-� ����9 (������� , �.�., �.�.�./������ �� �������%��, 5�
�5@�� ã���'��������'�Ó, ��9��, @#�%����
'��%. �-� � ;�� <o��, �.�., �.�.�./������ �� �9�������%��
������������'� =����7� ã�������$�Ó@&����>�, ��%����
'��%. �-� ���� /���/������ �� �9�������%��
������������'� =����7�, @���, V��$7����
$�:. �-� � �; � =�����, �.�.�!�� '����'�, ������������'� ����7���'� 7���#� �W=����
�W=����, ��������
'��%. �-� >�!�� 0��#?��, �.�.����������� ã���������Ó, @����7� A�E*�
/������ �� �9�������%�����&�, #�7��
'��%. �-� ����� ��@� )#�����, �.�., �.�.�.2-�� J�������� ������ =����7� ã5�����'�Ó
/������ �� �9�������%���#�<���� ����7���'� &����������, 5��'��, �&���
$�:. �-� '�� (�, �.�./������ �� �9�������%��
��7������� &�����������'� =����7����%��&�
$-� 0���� J � #� ��&'���� ��'���
/������ �� '����!�� �������&'�������'� &����������
V��$7����
'��%. �-� ��!���� �!����, �.�./������ �� �9�������%��
����������� ����%� �� /����������� /��&��, ������
'��%. �-� ��;@�! *�����;�!�� 7���#� ãV���$Ó
��&'���� 7���#� ã������#�Ó/���9����$�'� &����������, ��� ���%�, /���9�����, ��Z
'��%. �-� 0 �#� $ � J���#� �� �!�� ��&'� ã�-� ���<����� *�����Ó
�����&� �� ����7���'� ��&'��W ���"�, ����
$-� ��!�� <���� ��&'���� ��'���, @����7� ã����Ó
+����, �������
'��%. �-� J���� �� ���, �.�. ��&'���� 7���#� ã��� ���=��%Ó
5���7���'� 7���#� ãV�=�Ó4�� ��8����, �����
$-� � �#�� =���, �.�.�����&� ã���'���Ó, ��������, 0������
�!�� �����&�, ����������� �� [<�� 0������, 4����,0������, ��Z
$-� ���9� =�!�� �����=&�%, 0���7��
$-� ����� � $ ��/������ �� �9�������%��, 5�
�5@�� ã���'��������'�Ó, ��9��, @#�%����
Prof. Sylvia Cherninkova, MD, PhD, DSciDepartment of Neurology, Medical University
ãAlexandrovskaÓ Hospital, Sofia, Bulgaria
Prof. Gabor Hollo, MD, PhD, DSciDepartment of Ophthalmology
Semmelweis UniversityBudapest, Hungary
Prof. Milko Iliev, MDDepartment of Ophthalmology
University of Bern, Inselspital, Bern, Switzerland
Assoc. Prof. Barbara Cvenkel, MD, PhDEye Clinic, University Medical Centre Ljubljana
Ljubljana, Slovenia
Prof. Fotis Topouzis, MD, PhDAristotle University, AHEPA Hospital
Department of OphthalmologyThessaloniki, Greece
Prof. Alexander Kuroyedov, MD, PhD, DSciMandryka 2nd Central Clinical Hospital
Department of OphthalmologyRussian State Medical University, Moscow, Russia
Assoc. Prof. Paul Chew, MD, PhDDepartment of Ophthalmology
National University HospitalSingapore
Tarek Shaarawy, MDGlaucoma sector
Department of Clinical NeurosciencesUniversity of Geneva
Switzerland
Prof. Antonio Martlnez, MD, PhDDepartment of Ophthalmology
University of Santiago de CompostelaLa Coruna, Spain
Prof. Robert Weinreb, MDShiley Eye Center
Hamilton Glaucoma CenterUniversity of California, San Diego, California, USA
Prof. Tanuj Dada, MDDr Rajendra Prasad Centre for Ophthalmic Sciences
All India Institute of Medical SciencesNew Delhi, India
Anton Hommer, MDGlaucoma Unit, Hera Hospital
Vienna, Austria
Prof. Shlomo Melamed, MD, PhDThe Sam Rothberg Glaucoma Center
Sheba Medical CenterTel Hashomer, Israel
Radouil Tzekov, MD, PhDvvThe Roskamp Institute, Sarasota, FloridaUSF Eye Institute, Tampa, Florida, USA
Boriana Tzvetkova, MD Strasbourg, France
Nikolai Dakov, MD Department of Ophthalmology, Medical University
ãAlexandrovskaÓ Hospital, Sofia, Bulgaria
~
ÕÕ
Contact information: e-mail: [email protected]
Õ Õ

224 2013, ТОМ 3, Брой 5
ХИРУРГИЧНО ЛЕЧЕНИЕ / SURGICAL TREATMENT
IntroductionLowering the intraocular pressure (IOP) to the individual
target levels remains the only way proved to be effective in controlling the structural and functional progression of the glaucoma disease. In the large number of cases performing antiglaucoma surgery is an invasive, but most effective meansof reducing the IOP.
Trabeculectomy remains the „gold standard” in surgical treatment of most types of glaucoma [43]. The long-term experience with this procedure shows that it leads to IOP drop in the larger percentage of the patients [9, 28, 32]. The
main disadvantage of trabeculectomy is the relatively high risk of developing some serious intraoperative, early and latepostoperative complications [11, 18, 44, 41, 42]. Many of themare due to the fact that during trabeculectomy a new pathway for aqueous out� �w is created. The application of anti� brotic agents considerably improves the hypotensive effect of trabeculectomy, but it also increases the risk of developing somecomplications [16, 18, 19, 30]. The basic problem, particularly tothe long-term hypotensive effect, is the pathological changesin the � ltering bleb zone [16]. Episcleral � brosis, � brosis andbleb encapsulation, dysmorphic � ltering bleb can compromise
Ex-PRESS® and OlogenTM - single step implantation of two implants with a different mechanism
of action in glaucoma surgeryB. Anguelov
Department of Ophthalmology, Medical University „Alexandrovska” Hospital, So� a
AbstractPurpose: To perform a single step surgical implantation of two implants with a different mechanism of action - Ex-PRESS® and OlogenTM in advanced glaucoma patients indicated for surgical treatment. To follow-up and assess thepostoperative results.Materials and Methods: Single step implantation of two different implants - Ex-PRESS® (P-50 model) and subconjunctival biodegradable implant OlogenTM (12.0 mm in diameter and 1.0 mm in height) was performed in 15 eyes (12 patients). Five patients (6 eyes) are with pseudoexfoliative glaucoma and seven patients (9 eyes) are withprimary open-angle glaucoma. In some of the cases, another surgical treatment for glaucoma and/or cataract wasperformed prior the intervention performed by us. In all eyes the drug therapy failed to reach the target intraocular pressure (IOP).The Ex-PRESS® implant was placed under a triangular scleral � ap. The scleral � ap was � xated with 1 to 3 single sutures.The OlogenTM was placed under the tenon and conjunctiva in the area of the scleral � ap. Viscoelastic substance and/or maintainer were used to maintain the anterior chamber. During two interventions neither maintainer nor viscoelasticsubstance was used. �enon and conjunctiva were sutured with 10-0.Results: IOP drop and discontinuing of the drug therapy were achieved in 14 of the treated 15 eyes during the follow-up. Mean preoperative IOP was 25.94±11.11 mmHg. Mean postoperative IOP at the last follow-up visit was 12±3.06mmHg. Mean IOP drop from the baseline was 13.93±10.58 mmHg (�<0.05) �r ~53.0%. (high standard deviationwas due to the large variance of preoperative IOPs). Higher, statistically signi� cant IOP drop was observed inpseudoexfoliation glaucoma patients compared to the IOP drop in the primary open-angle glaucoma patients (�<0.05).Four eyes (3 patients) had a needle revision of the � ltering bleb during the follow-up. One combined hypotensive drughas been started in one of these eyes.Conclusion: Postoperative results show that our new surgical approach of single step surgical implantation of twoimplants with different mechanism of action Ex-PRESS® and OlogenTM could be an alternative to trabeculectomy (withor without the use of antimetabolites). Patients’ selection is also essential for the postoperative outcome. The fact that all the described patients are dif� cult for management cases of advanced glaucoma, medically treated for long period of time, and some of them surgically, de� nitely has impact on the post-op results and should be taken into account.Following up more operated patients for a longer period of time is needed.Key words: glaucoma, glaucoma implants, Ex-PRESS®, OlogenTM.

2252013, Vol. 3, Issue 5
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
to a varying degree the outcome of the performed surgical intervention. Restriction of the aqueous humor out� ow throughthe newly created pathway leads to IOP elevation above thetarget values.
The main idea of the newly developed interventions, surgical techniques and implants in glaucoma surgery, is to establish an effective and maximally safe procedure, which would be an alternative to the traditional � ltration surgery. Improving thelong-term hypotensive effect and reducing the complications(intraoperative, early and late postoperative) is the key goal.
Ex-PRESS® Glaucoma Filtration Device (Alcon Laboratories®
Inc., Fort Worth, TX) is a miniature, non-valved, tube shaped, drainage system made of stainless steel. It providescommunication between the anterior chamber and intrascleral space and creates a new pathway for aqueous out� ow, whichleads to reduction of the IOP [17]. The design of the Ex- PRESS®
implant is of great signi� cance for the very good results [3, 20, 25, 37]. There are different modi� cations of the implant, but theP-model is most widely used.
OlogenTM (Aeon Astron Corp., Netherlands) is a biodegrad-able collagen matrix implant comprised of 90% atelocollagentype I and 10% glycosaminoglycans. It has a porous structure with pore size ranges between 10~300 �m. According to differ-ent data, it degrades for a period of 90 to 180 days [8, 12, 48]. The OlogenTM is available in different forms and sizes and apart from glaucoma surgery it is used in the operative managementof strabismus and pterygium. The basic idea in the develop-ment and application of the OlogenTM in glaucoma surgery is the reduction and postponement of the � brous processes in the� ltering area. As a result the IOP lowering effect of the operation is being improved and stabilized and the complications due to usage of antimetabolites are being reduced [6, 34, 39].
PurposeTo perform a single step surgical implantation of two
implants with different mechanism of action - Ex-PRESS® and ®
OlogenTM in advanced glaucoma patients indicated for surgical treatment. To follow-up and assess the postoperative results.
Material and MethodsFifteen eyes (12 patients) with different types of advanced,
medically uncontrolled glaucoma are presented - 6 eyes (5 patients) with pseudoexfoliative glaucoma and 9 eyes (7 patients) with primary open-angle glaucoma. In some of the cases, another surgical treatment for glaucoma and/or cataract was performed prior the intervention performed by us. In alleyes the drug therapy failed to reach the target IOP.
Patients underwent routine ophthalmological examination,as well as ultrasound pachymetry (Ocuscan RxP, Alcon), optical coherence tomography (RTVue-100, Optovue), Heidelbergretinal tomography (HRT II, Soft. ver. 3.1.2., HeidelbergEngineering GmbH), standard automated perimetry performedwith Humphrey Field Analyzer II 745 (Carl Zeiss, Meditec,Dublin, CA, USA). All IOP measurements were made with a Goldmann tonometer.
Single step implantation of two different implants - Ex-PRESS® (P-50 model) and subconjunctival biodegradable®
implant OlogenTM (12.0 mm in diameter and 1.0 mm in height)was performed in all eyes. All the surgeries were carried outby one surgeon. All the patients signed an Informed consentform. Retrobulbar anesthesia was used. To maintain the anterior chamber a viscoelastic substance and/or maintainer were used.During two interventions neither maintainer nor viscoelasticsubstance was used. The conjunctival � ap was fornix based.Cauterization of the scleral vessels was not performed. A triangular scleral � ap was separated with 1/3 to 1/2 thickness of that of the sclera. Paracentesis of the anterior chamber in the blue-grey zone was made with 25 G needle. Through theformed channel the Ex-PRESS® implant was inserted by a®
special delivery system (EDS). The scleral � ap was � xed, with1 to 3 single 10-0 absorbable sutures. In the area of the scleral� ap, the OlogenTM was folded and placed under the tenon andconjunctiva. Conjunctiva and tenon were sutured with 10-0.
Case - I� 56-year-old male with pseudoexfoliative glaucoma had
been instilling three hypotensive medications on the left eyefor 4 months. On the � rst examination the best corrected visualacuity (BCVA) was 20/20 on the right eye and 20/25 on the lefteye. The IOP was 14 mmHg of the right eye and 23 mmHg of the left eye. Central corneal thickness (CCT) was: OD - 565 �m(- 1) and OS -562 �m (- 1). The slit lamp examination revealedsigni� cant deposits of pseudoexfoliative material on the anterior lens capsule. Ophthalmoscopy showed 0.2 Cup/Disc ratio (C/D)of the right eye and 0.9 C/D with nasal displacement of theblood vessels of the optic nerve head (ONH) of the left eye. Gonioscopy proved open anterior chamber angle of both eyes- Shaffer III degree.
Optical coherence tomography (OCT), Heidelbergretinal tomography (HRT), standard automated perimetryperformed with Humphrey � eld analyzer (HFA) revealed typicalglaucomatous structural and functional changes on the left eye(Fig. 1).
Single step implantation of Ex-PRESS® and Ologen TM wasperformed on the left eye. The main stages of the surgery aredemonstrated on Figure 2. Pre-op the IOP of the left eye was 25mmHg. The surgery was performed according to the describedtechnique, but without using an anterior chamber maintainer or viscoelastic material. The scleral � ap was � xated with only onesuture on the top of the � ap triangle.
One day post-op the IOP of the treated eye was 10 mmHg.Twenty months post-op the IOP of the treated eye was 11mmHg. On Table 1 the IOPs measured at the follow-up visits arepresented. Anterior segment photos of the treated eye after thespeci� ed period of time post-op, are demonstrated on Figure 3.Figure 4 and Figure 5 present the ultrasound biomicroscopy onthe second and the third month after the surgery.
During the 20 months follow-up period, neither additionalIOP lowering interventions were performed nor antiglaucomadrops were instilled on the operated eye.

226 2013, ТОМ 3, Брой 5
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
Fig. 2. Case - I. Some stages of the surgery - single step implantation of two different implants - Ex-PRESS® and OlogenTM .
Fig. 1. Case - I. HRT, OCT, HFA results.

2272013, Vol. 3, Issue 5
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
Case - II� 58-year-old female with pseudoexfoliative glaucoma
that was diagnosed 2 months ago had been instilling three hypotensive medications on the left eye. On the � rst examination the BCVA was 20/20 of the right eye and 20/20 of the left eye. The IOP was 14 mmHg of the right eye and 21 mmHg of the
Table 1. Case - I. IOP at the follow-up visits.
Post-op period 24 h 18 days
30 days
60 days
120days
6 months
8 months
9 months
14months
15 months
20 months
IOP of the operated left eye (mmHg) 10 11 11 9 11 9 10 8 10 11 11
Fig. 5. Case - I. Ultrasound biomicroscopy (performed by St. Dokov) on the third month after surgery.
Fig. 3. Case - I. Treated left eye after the speci� ed period of time post-op.
Fig. 4. Case - I. Ultrasound biomicroscopy (performed by St. Dokov) on the second month after surgery.
18 days post-op 60 days post-op 6 months post-op
left eye. CCT was: OD - 528 �m (+ 1) and OS - 531 �m (+1). The slit lamp examination showed deposits of pseudoexfoliativematerial on the pupillary margin of the iris and on the anterior lens capsule. During ophthalmoscopy we observed 0.5 C/D of the right eye and 0.9 C/D with nasal displacement of the blood vessels of the ONH of the left eye. Open anterior chamber angle
228 2013, ТОМ 3, Брой 5
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
was gonioscopically proved of both eyes - Shaffer III degree. OCT, HRT and computer perimetry revealed glaucomatous structural and functional changes on the left eye.
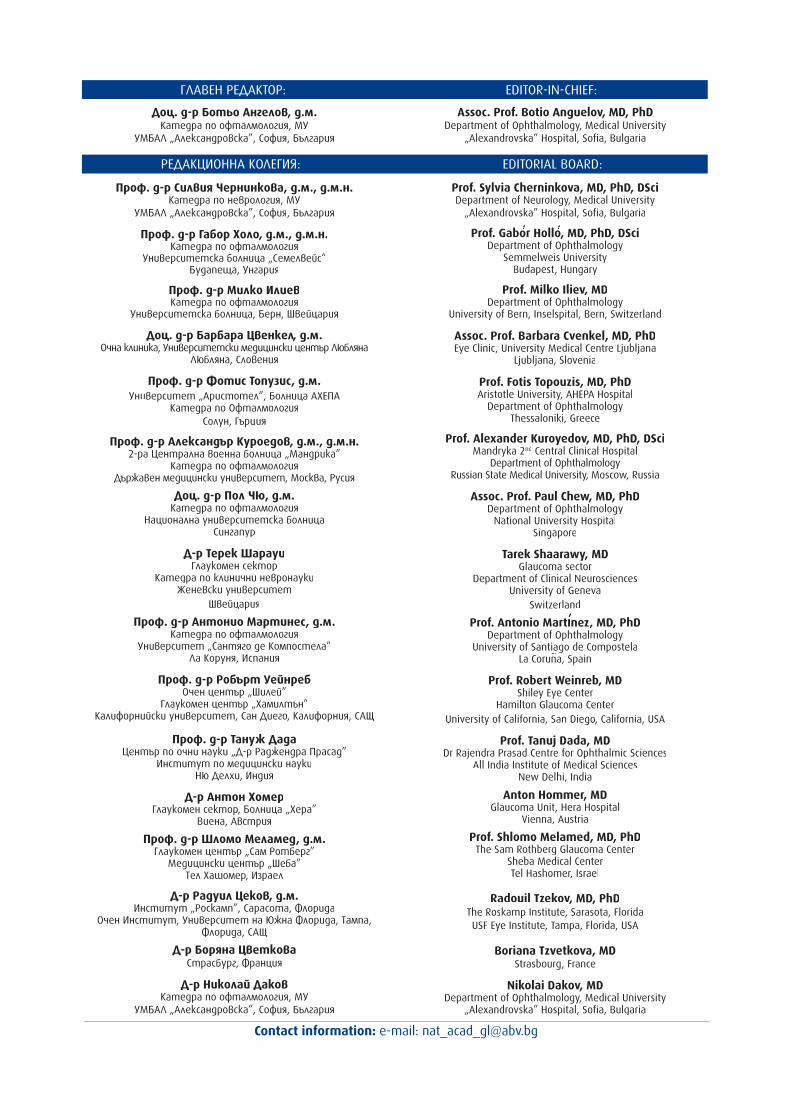
Single step implantation of Ex-PRESS® and Ologen® TM was performed on the left eye. Pre-op the IOP of the left eye was 24 mmHg. One day post-op the IOP of the treated eye was 10mmHg. 20 days post-op the IOP was 11 mmHg. Ultrasound biomicroscopy was performed and the two implants as well asthe � ltering bleb were visualized (Fig. 6). Figure 7 shows thetreated eye after the speci� ed period of time post-op. Nineteen months post-op the IOP was 11 mmHg. On Table 2 are presentedthe IOP of the operated eye measured at the follow-up visits.
During the 19 months follow-up, neither additional IOP lowering interventions were performed nor antiglaucoma drugs were instilled.
Case - III� 80-year-old male with a 5 year history of primary
open-angle glaucoma had been instilling three hypotensive medications on the left eye. Six years ago he lost functionalvision on his right eye, which is currently with corneal leucoma
Fig. 7. Case - II. Treated left eye after the speci� ed period of time post-op.
Table 2. Case - II. IOP at the follow-up visits.
Post-op period 24 hours 20 days 90 days 6 months 8 months 9 months 15 months 19 months
IOP of the treated left eye (mmHg) 10 11 13 12 11 11 12 11
and with a therapeutic lens. The left eye underwent cataractextraction and posterior chamber IOL implantation two years ago. On the � rst examination performed by us the BCVA was20/30 of the left eye, while the right eye had no light perception - Ø. The IOP of the left eye was 19 mmHg. CCT was: OS -563 �m (-1). The slit lamp examination of the left eye showeda deep anterior chamber, and the intraocular lens was insidethe capsular bag. There were vitreal � bers reaching posterior surface of the cornea and deforming the pupillary margin of theiris. Deep cupping 0.9 C/D was observed on the left eye withnasal displacement of the blood vessels. Gonioscopy proved anopen anterior chamber angle - Shaffer III degree. OCT, HRT andcomputer perimetry revealed advanced glaucomatous structuraland functional changes on the left eye.
Single step implantation of Ex-PRESS® and Ologen™ was®
performed on the left eye. Pre-op the IOP of the left eye was 20 mmHg. The surgery was performed according to the describedtechnique. As stated, the patient had vitreal � bers touching theposterior surface of the cornea and deforming the pupillarymargin of the iris, which we removed during the surgery. The scleral � ap was � xed with one suture on the top of the triangle.
Fig. 6. Case - II. Ultrasound biomicroscopy (performed by St. Dokov) 20 days after surgery.
20 days post-op 19 months post-op
2292013, Vol. 3, Issue 5
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
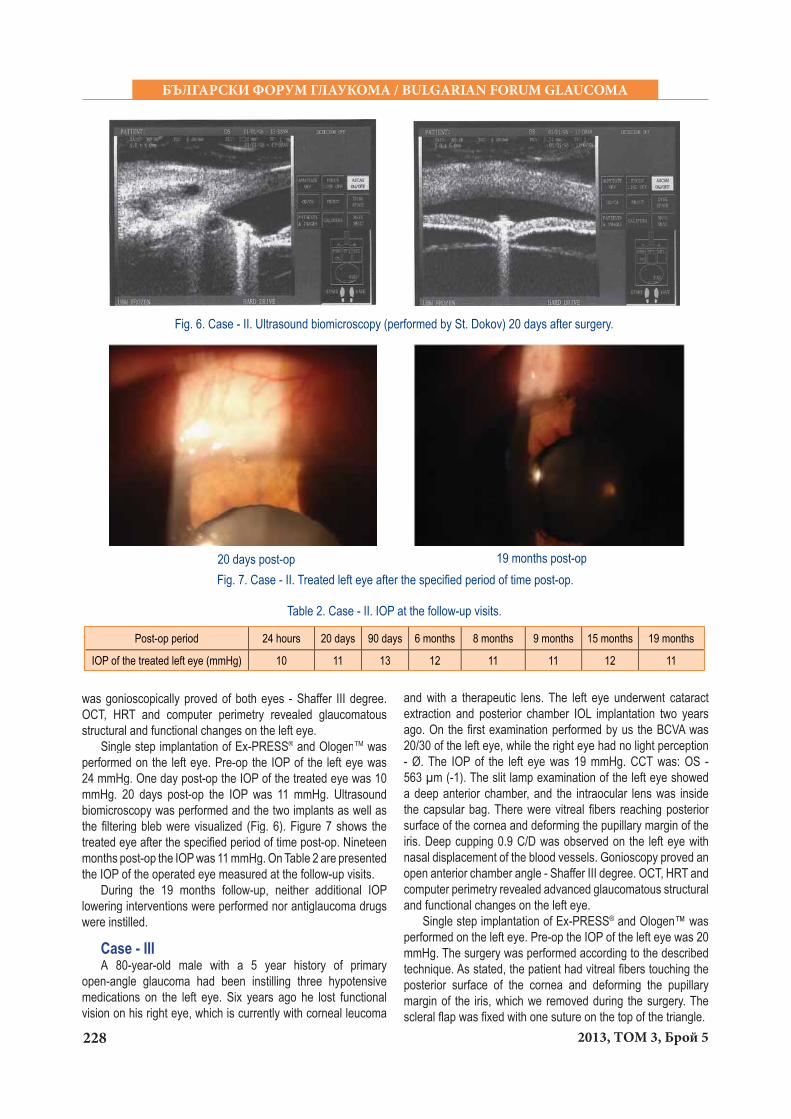
One day post-op the IOP on the treated eye was 10 mmHg. On Table 3 the IOPs of the operated eye measured at the follow-up visits are presented. Figure 8 shows the treated eye after thespeci� ed period of time post-op.
Needle revision of an encapsulated � ltering bleb on the operated eye was performed. During the 17 months follow-up no IOP lowering medications were used.
Case - IV / Case - V� 71-year-old male with 3 years history of pseudoexfoliative
glaucoma. He had been instilling three hypotensive medications on both eyes. On the � rst examination the BCVA was 20/20 of the right eye and PLC (presence of light perception) of the left
Post-op period 24 hours 5 days
7 days
40 days
50 days
60 days
3 months
6months
8 months
12months
17months
IOP of the treated left eye (mmHg) 10 7 8 15 15 7 12 16 14 11 16
17 months post-opFig. 8. Case - III. Treated left eye after the speci� ed period of time post-op.
Table 3. Case - III. IOP at the follow-up visits.
eye. The IOP was 20 mmHg of the right eye and 39 mmHg of the left eye. CCT was: OD - 523 �m (+ 1) and OS - 545 �m (0).
The slit lamp examination revealed deposits of pseudoexfoliative material on the anterior lens capsule onboth eyes. There was a slight corneal oedema on the left eye,atrophic iris, and cataract. Ophthalmoscopy showed 0.6 C/D of the right eye and 0.9 C/D of the left eye with nasal displacementof the blood vessels of the ONH and peripapillary atrophy in both eyes. Gonioscopy proved an open anterior chamber angleon both eyes - Shaffer III degree. OCT, HRT and the computer perimetry revealed glaucomatous structural and functionalchanges of both eyes, more advanced in the left one.
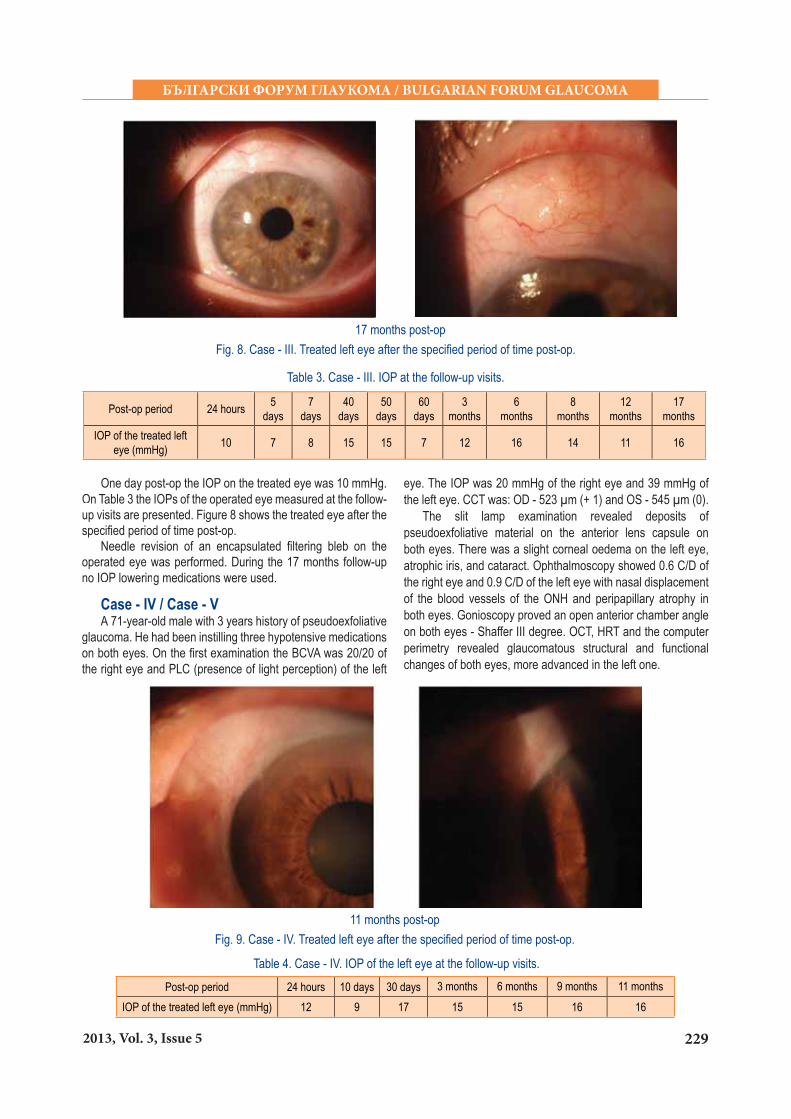
11 months post-opFig. 9. Case - IV. Treated left eye after the speci� ed period of time post-op.
Post-op period 24 hours 10 days 30 days 3 months 6 months 9 months 11 monthsIOP of the treated left eye (mmHg) 12 9 17 15 15 16 16
Table 4. Case - IV. IOP of the left eye at the follow-up visits.

230 2013, ТОМ 3, Брой 5
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
Table 5. Case - V. IOP of the right eye at the follow-up visits.
3 months post-opFig. 10. Case - V. Treated right eye after the speci� ed period of time post-op.
Post-op period 24 hours 7 days 30 days 2 months 3 months
IOP of the treated right eye (mmHg) 11 11 16 15 14
Single step implantation of Ex-PRESS® and Ologen® TM was performed on both eyes. The left eye (Case IV) was operated� rst. The intervention on the right eye (Case V) was performed9 months later. The surgeries were performed according to thedescribed technique. Pre-op the IOP of the left eye was 62mmHg and 20 mmHg of the right eye.
One day post-op the IOP of the left eye was 12 mmHg. Elevenmonths after the surgery the IOP was 16 mmHg. Figure 9 showsthe treated eye after the speci� ed period of time post-op. On Table4 the IOPs measured at the follow-up visits are presented.
One day post-op the IOP of the right eye was 11 mmHg.Three months after the surgery the IOP was 14 mmHg. Figure 10 shows the treated eye after the speci� ed period of time post-op. On Table 5 the IOPs measured at the follow-up visits arepresented.
All IOP lowering medications that had been administeredon both eyes were discontinued after the surgeries. During the 11 months follow-up of the left eye and 3 months follow-up of the right eye, neither additional IOP lowering interventions wereperformed nor antiglaucoma drops were instilled.
Case - VI� 57-year-old male with eight years history of primary open-
angle glaucoma. During this period, he had been instilling 2 or 3 hypotensive medications on both eyes. On the � rst examination,the patient was instilling 3 hypotensive medications. Since 2011 the vision of the right eye has been getting worse. Trabeculectomy was performed on the left eye.
On the � rst examination the BCVA was PLC of the right eye and 20/50 of the left eye. The IOP was 45 mmHg of the
Fig. 11. Case - VI. Treated left eye after the speci� ed period of time post-op.
Table 6. Case - VI. IOP at the follow-up visits.
Post-op period 24 hours 10 days 30 days 40 days 3 months 6 months 8 months
IOP of the treated left eye (mmHg) 17 17 30 20 16 16 18
40 days post-op 3 months post-op

2312013, Vol. 3, Issue 5
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
right eye and 24 mmHg of the left eye. CCT was: OD - 502 �m (+ 4) and OS - 483 �m (+ 5). The slit lamp examination showed: OD - shallow anterior chamber, iris - bombe, pupillary marginwas in contact with the anterior lens capsule, mature cataract,pigment on the anterior lens capsule, phacodonesis, pupil - no light reaction; OS - encapsulated bleb, iris with basal iridectomy,partial posterior synechia, lens - cortical cataract, pigment onthe anterior lens capsule. Fundus of the right eye could not beobserved due to the mature cataract. Ophthalmoscopy of theleft eye showed 0.8 C/D with nasal displacement of the blood vessels of the ONH and peripapillary atrophy. Gonioscopyproved an open anterior chamber angle in the left eye - Shaffer III degree. Anterior chamber angle of the right eye was Shaffer II degree.
Trabeculectomy with OlogenTM was performed � rst on the right eye. After a month, we performed a single-step implantationof �x-PRESS® and Ologen® TM on the left eye. Pre-op the IOP of the right eye was 25 mmHg. One day post-op the IOP of the treated eye was 17 mmHg. Eight months post-op the IOP was 18 mmHg. Figure 11 shows the treated eye after the speci� ed period of time post-op. On Table 6 the IOPs measured at thefollow-up visits are presented.
During the � rst 6 months post-op, no antiglaucoma drops were instilled on the operated eye. Tendency of bleb encapsulation was observed. Bleb needling was performedseveral times. Cataract extraction and IOL implantation was carried out in the left eye. Due to IOP elevation above the target values, after the follow-up visit at the six month we prescribedto the patient a � x-combination IOP lowering drug to instill on the left eye.
Case - VII� 64-year-old female with primary open-angle glaucoma
that was diagnosed 2 years ago had been instilling three hypotensive medications on both eyes. On the � rst examinationthe BCVA was 20/20 of the right eye and 20/20 of the left eye.
The IOP was 14 mmHg of the right eye and 16 mmHg of the left eye. CCT was: OD - 506 �m (+ 3) and OS - 512 �m (+ 3).The slit lamp examination showed initial cataract on both eyesand no other pathological changes. During ophthalmoscopywe observed 0.5 C/D on the right eye and 0.8 C/D with nasaldisplacement of the blood vessels of the ONH of the left eye. Gonioscopy proved open anterior chamber angle of both eyes -Shaffer III degree. OCT, HRT and computer perimetry revealedglaucomatous structural and functional changes of both eyes,more advanced in the left one.
Single step implantation of Ex-PRESS® and Ologen® TM was performed on the left eye. Pre-op the IOP of the left eye was 20 mmHg. The surgery was performed according to the describedtechnique.
One day post-op the IOP of the treated eye was 11 mmHg. Seven months after the surgery the IOP was 8 mmHg. Figure12 shows the treated eye after the speci� ed period of time post-op. On Table 7 the IOPs measured at the follow-up visits are presented.
All IOP lowering medications that had been administeredon the left eye were discontinued after the surgery. During the 7months follow-up, neither additional IOP lowering interventionswere performed nor antiglaucoma drops were instilled.
Case -VIII / Case - IX� 60-year-old female with 2 years history of primary open-
angle glaucoma. She had been instilling two hypotensivemedications on both eyes. On the � rst examination the BCVA was 20/20 of the right eye and 20/25 of the left eye. The IOP was 24 mmHg of the right eye and 20 mmHg of the left eye. CCT was: OD - 502 �m (+ 4) and OS - 512 �m (+3).
The slit lamp examination revealed cataract in both eyes.Ophthalmoscopy showed 0.9 C/D of the right eye and 0.7 C/Dof the left eye with nasal displacement of the blood vessels of the ONH and peripapillary atrophy of both eyes. Gonioscopyproved an open anterior chamber angle in both eyes - Shaffer
Fig. 12. Case - VII. Treated left eye 7 months post-op.
Table 7. Case - VII. IOP at the follow-up visits.
Post-op period 24 hours 7 days 30 days 2 months 3 months 7 months
IOP of the treated left eye (mmHg) 11 9 8 10 10 8
232 2013, ТОМ 3, Брой 5
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
III degree. OCT, HRT and the computer perimetry revealed glaucomatous structural and functional changes of both eyes, more advanced in the right one.
Single step implantation of Ex-PRESS® and Ologen™ was ®
performed on both eyes. The right eye (Case VIII) was operated� rst. The intervention on the left eye (Case IX) was performed 5 months later. The surgeries were performed according to the described technique. Pre-op the IOP of the right eye was 26 mmHg and 20 mmHg of the left eye.
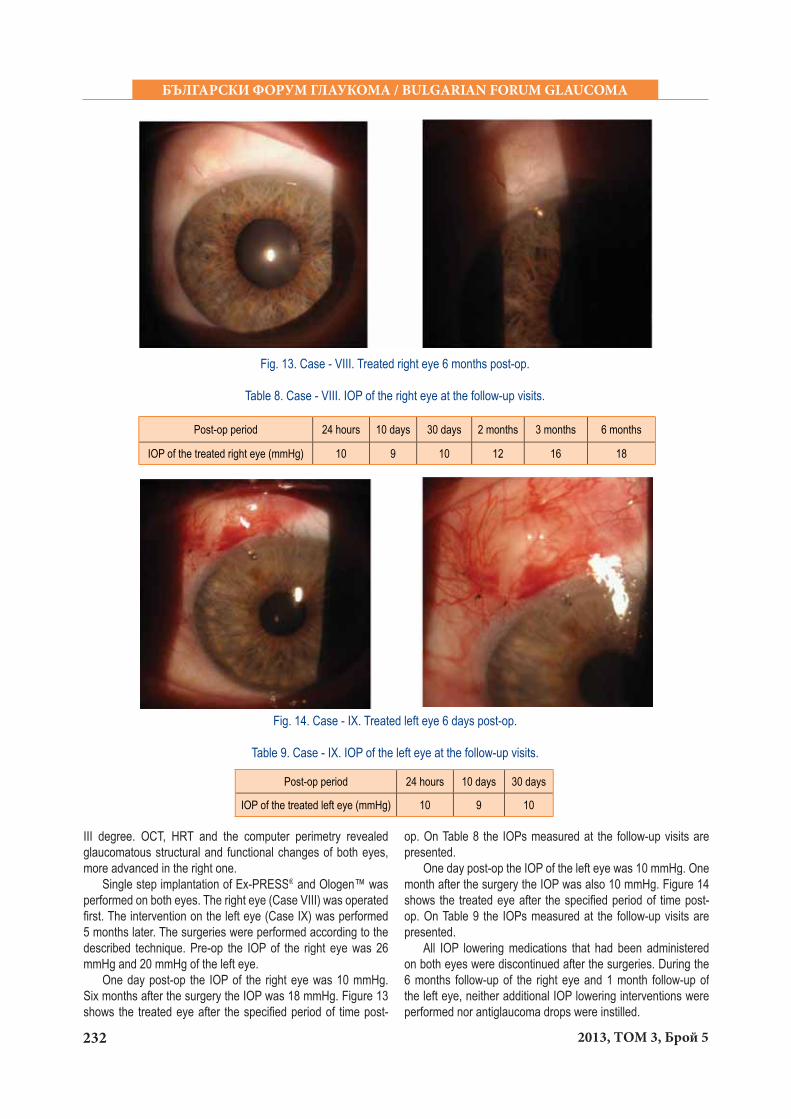
One day post-op the IOP of the right eye was 10 mmHg. Six months after the surgery the IOP was 18 mmHg. Figure 13shows the treated eye after the speci� ed period of time post-
Fig. 13. Case - VIII. Treated right eye 6 months post-op.
Table 8. Case - VIII. IOP of the right eye at the follow-up visits.
Post-op period 24 hours 10 days 30 days 2 months 3 months 6 months
IOP of the treated right eye (mmHg) 10 9 10 12 16 18
op. On Table 8 the IOPs measured at the follow-up visits arepresented.
One day post-op the IOP of the left eye was 10 mmHg. Onemonth after the surgery the IOP was also 10 mmHg. Figure 14shows the treated eye after the speci� ed period of time post-op. On Table 9 the IOPs measured at the follow-up visits arepresented.
All IOP lowering medications that had been administeredon both eyes were discontinued after the surgeries. During the6 months follow-up of the right eye and 1 month follow-up of the left eye, neither additional IOP lowering interventions wereperformed nor antiglaucoma drops were instilled.
Fig. 14. Case - IX. Treated left eye 6 days post-op.
Table 9. Case - IX. IOP of the left eye at the follow-up visits.
Post-op period 24 hours 10 days 30 days
IOP of the treated left eye (mmHg) 10 9 10
2332013, Vol. 3, Issue 5
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
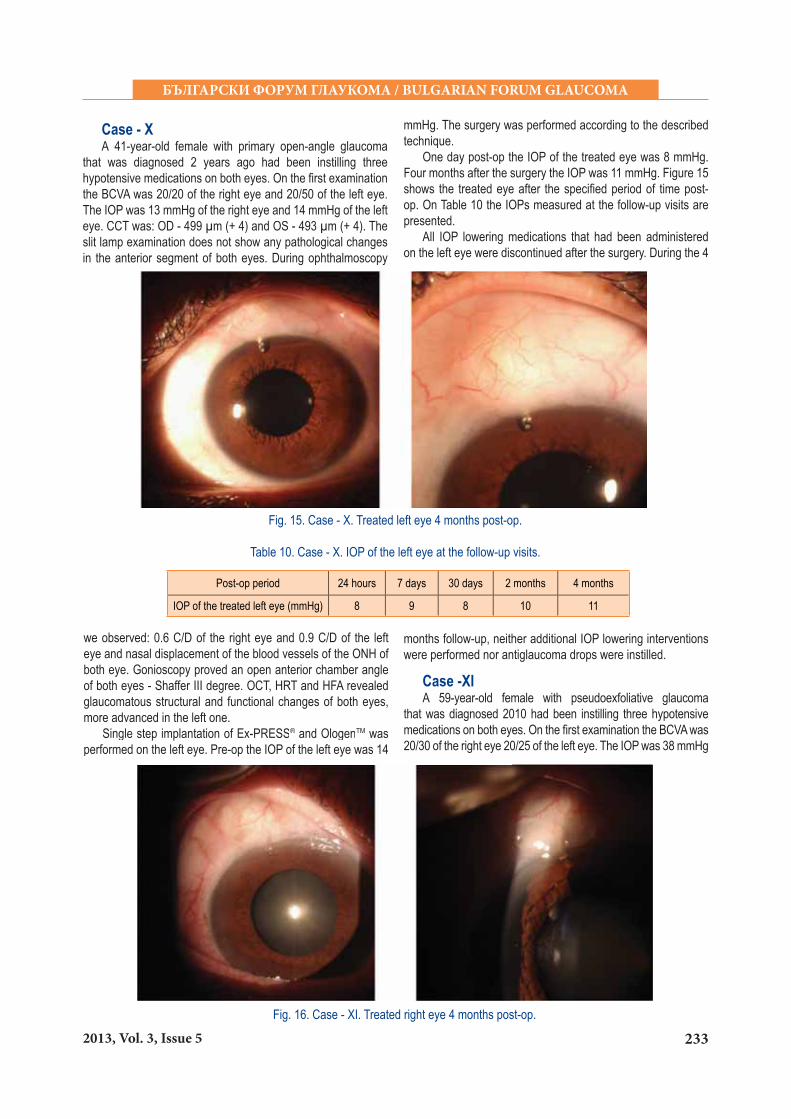
Case - X� 41-year-old female with primary open-angle glaucoma
that was diagnosed 2 years ago had been instilling three hypotensive medications on both eyes. On the � rst examinationthe BCVA was 20/20 of the right eye and 20/50 of the left eye. The IOP was 13 mmHg of the right eye and 14 mmHg of the left eye. CCT was: OD - 499 �m (+ 4) and OS - 493 �m (+ 4). The slit lamp examination does not show any pathological changes in the anterior segment of both eyes. During ophthalmoscopy
Fig. 15. Case - X. Treated left eye 4 months post-op.
Table 10. Case - X. IOP of the left eye at the follow-up visits.
Post-op period 24 hours 7 days 30 days 2 months 4 months
IOP of the treated left eye (mmHg) 8 9 8 10 11
we observed: 0.6 C/D of the right eye and 0.9 C/D of the lefteye and nasal displacement of the blood vessels of the ONH of both eye. Gonioscopy proved an open anterior chamber angleof both eyes - Shaffer III degree. OCT, HRT and HFA revealedglaucomatous structural and functional changes of both eyes,more advanced in the left one.
Single step implantation of Ex-PRESS® and Ologen® TM was performed on the left eye. Pre-op the IOP of the left eye was 14
mmHg. The surgery was performed according to the describedtechnique.
One day post-op the IOP of the treated eye was 8 mmHg. Four months after the surgery the IOP was 11 mmHg. Figure 15shows the treated eye after the speci� ed period of time post-op. On Table 10 the IOPs measured at the follow-up visits are presented.
All IOP lowering medications that had been administeredon the left eye were discontinued after the surgery. During the 4
months follow-up, neither additional IOP lowering interventionswere performed nor antiglaucoma drops were instilled.
Case -XI� 59-year-old female with pseudoexfoliative glaucoma
that was diagnosed 2010 had been instilling three hypotensivemedications on both eyes. On the � rst examination the BCVA was20/30 of the right eye 20/25 of the left eye. The IOP was 38 mmHg
Fig. 16. Case - XI. Treated right eye 4 months post-op.

234 2013, ТОМ 3, Брой 5
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
of the right eye and 14 mmHg of the left eye. CCT was: OD - 506 �m (+ 3) and OS - 510 �m (+ 3). The slit lamp examination showed deposits of pseudoexfoliative material on the anterior lens capsule of both eyes. During ophthalmoscopy we observed 0.9 C/D on the right eye and 0.4 C/D of the left eye with nasal displacement of the blood vessels of the ONH of both eyes. Gonioscopy proved an open anterior chamber angle in both eyes - Shaffer III - IV degree. OCT, HRT and the computer perimetry revealed glaucomatous structural and functional changes.
Single step implantation of Ex- PRESS® and Ologen® TM was performed on the right eye. Pre-op the IOP of the right eye was 40 mmHg. The surgery was performed according to the described technique.
One day post-op the IOP on the treated eye was 9 mmHg.Four months after the surgery the IOP was 10 mmHg. Figure 16 shows the treated eye after the speci� ed period of time post-op. On Table 11 the IOPs measured at the follow-up visits are presented.
All IOP lowering medications that had been administered on the right eye were discontinued after the surgery. During the 4 months follow-up, neither additional IOP lowering interventions were performed nor antiglaucoma drops were instilled.
Case - XII / Case - XIII� 78 - year-old male with 20 years history of primary open-
angle glaucoma. He had been instilling three hypotensive medications on both eyes. On the � rst examination the BCVA was 20/100 on the right eye and 20/400 on the left eye. The IOP was 26 mmHg of the right eye and 15 mmHg of the left eye.
Post-op period 24 hours 10 days 30 days 2 months 3 months
IOP of the treated right eye (mmHg) 11 10 12 23 14
Table 12. Case - XII. IOP of the right eye at the follow-up visits.
CCT was: OD - 499 �m (+ 4) and OS - 516 �m (+ 2). Cataractextraction with IOL implantattion was performed on both eyes -right eye (year 1997) and left eye (year 1994).
The slit lamp examination revealed a deformed pupillary margin of the iris of both eyes. The IOL in each eye was inside the capsular bag. Ophthalmoscopy showed 0.8 - 0.9 C/D of the right eye and 0.9 C/D of the left eye with nasal displacement of the blood vessels of the ONH and peripapillary atrophy of both eyes. Gonioscopy proved an open anterior chamber angle in both eyes - Shaffer III - IV degree. OCT, HRT and the computer perimetry revealed glaucomatous structural and functionalchanges of both eyes.
Single step implantation of Ex-PRESS® and Ologen™ was ®
performed on both eyes. The right eye was operated � rst. The intervention on the left eye was performed 1 month later. Thesurgeries were performed according to the described technique. Pre-op the IOP of the right eye was 23 mmHg and 20 mmHg of the left eye.
One day post-op the IOP of the right eye was 11 mmHg.Three months after the surgery the IOP was 14 mmHg. Figure 17 shows the treated eye after the speci� ed period of time post-op. On Table 12 the IOPs measured at the follow-up visits are presented.
One day post-op the IOP of the left eye was 11 mmHg. Twomonths after the surgery the IOP was also 14 mmHg. Figure 18 shows the treated eye after the speci� ed period of time post-op. On Table 13 the IOPs measured at the follow-up visits are presented.
Fig. 17. Case - XII. Treated right eye 3 months post-op.
Table 11. Case - XI. IOP of the right eye at the follow-up visits.
Post-op period 24 hours 14 days 40 days 3 months 4 months
IOP of the treated right eye (mmHg) 9 9 10 10 10

2352013, Vol. 3, Issue 5
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
Fig. 18. Case - XIII. Treated left eye 2 months post-op.
Table 13. Case - XIII. IOP of the left eye at the follow-up visits.
Post-op period 24 hours 10 days 30 days 2 months
IOP of the treated left eye (mmHg) 11 10 18 14
Needle revision of an encapsulated � ltering bleb wasperformed on both eyes. All IOP lowering medications were dis-continued after the operations.
Case - XIV� 70-year-old male with pseudoexfoliative glaucoma
that was diagnosed 2012 had been instilling two hypotensive medications on both eyes. On the � rst examination the BCVA was PPLC (presence of light perception and projection) of theright eye and 20/50 of the left eye. The IOP was 29 mmHg of theright eye and 13 mmHg of the left eye. CCT was: OD - 492 �m
(+ 4) and OS - 491 �m (+ 4). The slit lamp examination showed: deposits of pseudoexfoliative material on the anterior lens ffcapsule of both eyes, cataract in both eyes (more advanced in the right eye). During ophthalmoscopy we observed: 0.8 - 0.9 C/D on the right eye and 0.5 C/D on the left eye with nasal displacement of the blood vessels of the ONH of both eyes. Gonioscopy proved an open anterior chamber angle in both eyes - Shaffer III - IV degree. OCT, HRT and the computer perimetry revealed glaucomatous structural and functionalchanges in both eyes, more advanced in the right eye.
Fig. 19. Case - XIV. Treated right eye 1 month post-op.
Table 14. Case - XIV. IOP of the right eye at the follow-up visits.
Post-op period 24 hours 10 days 30 days
IOP of the treated right eye (mmHg) 8 9 9

236 2013, ТОМ 3, Брой 5
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
Single step implantation of Ex-PRESS® and Ologen™ was ®
performed on the right eye. Pre-op the IOP of the right eye was 28 mmHg. The surgery was performed according to the described technique.
One day post-op the IOP on the treated eye was 8 mmHg.One month after the surgery the IOP was 9 mmHg. Figure 19shows the treated eye after the speci� ed period of time post-op. On Table 14 the IOPs measured at the follow-up visits are presented.
All IOP lowering medications that had been administered on the right eye were discontinued after the surgery. During the 1 month follow-up, neither additional IOP lowering interventions were performed nor antiglaucoma drops were instilled.
Case - XV� 74-year-old female was diagnosed with primary open-
angle glaucoma recently. She had been instilling two hypotensivemedications on both eyes. The BCVA was 20/20 of the right eyeand 20/20 of the left eye. The IOP varied between 14 mmHgand 17 mmHg of the right eye and 15 and 18 mmHg of the
Table 15. Case - XV. IOP of the left eye at the follow-up visits.
Post-op period 24 hours 10 days 30 days
IOP of the treated left eye (mmHg) 9 11 10
Fig. 20. Case - XV. Treated left eye 1 month post-op.
left eye. CCT was: OD - 502 �m (+ 4) and OS - 496 �m (+ 4). The slit lamp examination showed initial cataract on both eyesand no other pathological changes. During ophthalmoscopy we observed: vertically elongated cup shape of the ONH of both eyes, 0.7 C/D of the right eye and 0.8 C/D of the left eye, withnasal displacement of the blood vessels of the ONH of the both eyes. Gonioscopy proved an open anterior chamber angle in both eyes - Shaffer III degree. OCT, HRT and automatedperimetry revealed glaucomatous structural and functional changes on both eyes.
Single step implantation of Ex-PRESS® and Ologen™ was ®
performed on the left eye. Pre-op the IOP of the left eye was 18 mmHg. The surgery was performed according to the described technique.
One day post-op the IOP on the treated eye was 9 mmHg.One month after the surgery the IOP was 10 mmHg. Figure 20shows the treated left eye after the speci� ed period of time post-op. On Table 15 the IOPs measured at the follow-up visits are presented.
All IOP lowering medications that had been administeredon the left eye were discontinued after the surgery. During the1 month follow-up, neither additional IOP lowering interventionswere performed nor antiglaucoma drops were instilled.
ResultsIOP drop and discontinuing of the drug therapy was
achieved in 14 of the treated 15 eyes during the follow-up(between 1 month and 20 months). Mean preoperative IOP was25.94±11.11 mmHg. Mean postoperative IOP at the last follow-up visit was 12±3.06 mmHg. Mean IOP drop from the baselinewas 13.93±10.58 mmHg (�<0.05) �r ~53.0%. (high standarddeviation was due to the large variance of preoperative IOPs).Higher, statistically signi� cant IOP drop was observed inpseudoexfoliation glaucoma patients compared to the IOP drop
in the primary open-angle glaucoma patients (�<0.05).During the follow-up, 4 eyes (3 patients) underwent needle
revision of the � ltering bleb. One combined hypotensive drughas been started in one of these eyes.
DiscussionDevelopment and introduction of a variety of new implants,
surgery techniques or modifying the established ones is essential for the progress of glaucoma surgery.
There are many studies exploring the effectiveness andcomplication rates after Ex-PRESS® implantation. A great®
amount of data is collected about Ex-PRESS® application as®
an alternative to trabeculectomy [1, 24, 31, 35]. Unlike thetrabeculectomy while implanting Ex-PRESS®, two of the eye

2372013, Vol. 3, Issue 5
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
traumatizing steps - sclerectomy and iridectomy are avoided. Due to this fact the rate of intra- and postoperative complicationis lower, and the procedure is less invasive and easier to perform [24, 35, 45]. The innovative and practical design of the Ex-PRESS® glaucoma � ltration device is another advantage of ®
the implant [3].Different researches show that the implant is suitable
especially for patients who underwent previous unsuccessful� ltration surgery [24, 29, 33, 35]. Based on a one year follow-up of 100 eyes (100 patients) Lankaranian et al., sum up that Ex-PRESS® implantation in patients with previous unsuccessful ®
� ltration surgery or cataract extraction is an effective and safe procedure for IOP control [29]. For a long period of time the effect on IOP after Ex-PRESS® surgery is similar to those after ®
trabeculectomy [33, 35, 45]. The rate of the most frequent intraoperative and early postoperative complications is lower with Ex-PRESS® [10, 15, 31, 33, 35, 37, 45, 46]. Dahan et al., ®
follow a group of patients with glaucoma on both eyes where a trabeculectomy is performed on one of the eyes and an Ex-PRESS® implant is inserted on the other eye [15]. Results ®
proved that both interventions had similar IOP lowering effectbut the eyes with Ex-PRESS® implant had less complications, ®
additional postoperative procedures and a signi� cant reductionof antiglaucoma medications. According to Kuroyedov et al., Ex-PRESS® implantation is safe and with a long-term hypotensive ®
effect for advanced glaucoma cases [26]. The implant application leads to reduction of antiglaucoma medications aswell as lowering the cost of treatment [13, 15, 25].
The long-term success of � ltration surgery is based not only upon the used surgical technique but also on the individual postoperative shaping of the � ltration bleb. Subconjuctival � brosis leads to a decreased effect and it is one of the leading factors for the failure of the � ltration surgery. To minimize thesubconjuctival � brosis in the bleb area antimetabolites like Mitomycin C, 5- Fluorouracil etc., have been used for years. Their usage improves the success of trabeculectomy, but also increases the risk of some early and late post-op complications [11, 16, 18, 19, 23, 27, 30]. Histological research of the � ltration bleb after trabeculectomy with antimetabolites shows damages in the conjunctival epithelium, interruption of the basal membrane, hypocellular conjunctiva and subconjunctival tissue.As a result of the thinning of the avascular conjuctival layers its protective mechanism is reduced and the risk of infection of the bleb and endophthalmitis is increased [4, 27, 36].
In order to reduce and delay the � brosis in the bleb areabiodegradable collagen matrix implant Ologen™ is developed and widely applied. The use of collagen-glycosaminoglycan co-polymer leads to reorganization of the regenerating myo� broblasts and � broblasts and improves the secretion of extracellular matrix (collagen), and in this way the cicatrix formation is reduced [21, 22, 47]. The porous structure of the Ologen™ optimizes aqueous out� ow through the bleb by physiological regeneration of the extracellular matrix and the formed reservoir system [21, 22, 47, 48]. The interaction between the tissue and the collagenous matrix leads to a formation of a stable bleb structure.
Research results show that, Ologen™ is appliedsuccessfully in patients with different glaucoma types,including refractory ones [7]. Trabeculectomy with Ologen™leads to a similar hypotensive effect. There are less post-op complications, and it is an effective and safer adequatealternative to trabeculectomy with MMC [14, 39]. Ologen™ is also used for phacotrabeculectomy in patients with cataract andprimary open-angle glaucoma [4]. It is also applied for surgicaltreatment of complications and tissue repairing after glaucomadraining devices tube exposure (�hmed glaucoma valve Baerveldt) [38]. The � rst results of the surgical revision withOlogenTM implantation in eyes with glaucoma and �x-PRESS®
that we perform are very good [2].The main idea of our surgical technique is that by a single step
implantation of two implants with different mechanisms of action(Ex-PRESS® and Ologen® TM) not only is the hypotensive effectof the intervention improved, but also the risk of some typicalfor � ltration surgery (with or without the use of antimetabolites) serious inra- and postoperative complications is reduced. The two implants are inserted in a single step intervention in order to reduce the risk of possible complications after two separatesurgeries, especially those related to the morphology and the� brous processes in the � ltration bleb area.
The maneuver of folding the Ologen™ implant wasperformed in order to ensure a maximum space between sclera,conjunctiva and tenon. In this way a wider and higher space and greater volume in the bleb zone would be formed, so the risk of cicatrization in it would be reduced.
By performing a single step implantation of two implants withdifferent mechanism of action we achieve several main goals:
- Improving the aqueous out� ow- IOP lowering and discontinuing of the drug therapy- Modulating the wound healing process (by using
OlogenTM) and reducing the risk of excessive cicatrization in� ltration area.
- By OlogenTM implantation we avoid antimetabolitesapplication and in this way we avoid the typical complicationsrelated to their usage.
Our � rst results of the single step implantation of two implants with different mechanisms of action (Ex- PRESS® and Ologen® TM)in 4 eyes (4 patients) were already published [5]. This was a � rst publication in the open literature describing a procedure of this kind - single step implantation of Ex- PRESS® and Ologen® TM Inthe open literature, we found that insertion of two, but identical implants (iStent) in the same eye was described [40].
The presence of complications like encapsulating of thebleb and ranging IOP values in some of the patients is due to thefact that they are dif� cult for management cases of advancedglaucoma. It is imminent that some additional interventions beneeded, aiming at consolidation or improvement of postoperativeresults. Namely for this reason patient selection is essential for the post-op outcome. The fact that all the described patientsare dif� cult for management cases of advanced glaucoma,medically treated for long period of time, and some of themsurgically, de� nitely has impact on the post-op results andshould be taken into account.

238 2013, ТОМ 3, Брой 5
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
ConclusionPostoperative results show that the surgical approach we
suggest - single step implantation of two implants with different mechanism of action - Ex-PRESS® and Ologen® TM - could bean adequate alternative to trabeculectomy (with or without the use of antimetabolites). Patients’ selection is essential for the post-op outcome. In order to identify the effectiveness andcomplication rates of this surgical procedure, a follow-up of larger number of patients for a longer period of time is needed.
References:1. Ahmed K. Ex-PRESS® Mini glaucoma shunt: techniques and pearls. ®
Clinical & surgical ophthalmology 2008; 26(9):306-10.2. Anguelov B. Clinical cases of surgical revision with OlogenTM
implantation in eyes with glaucoma and �x-PRESS® implant. Bul F®
Glaucoma 2013; 3(4):172-83.3. Anguelov B. Design and application of Ex-PRESS® Filtration Device ®
in modern glaucoma surgical treatment. Bul F Glaucoma 2012; 2(1):11-5.
4. Anguelov B. Phacotrabeculectomy with absorbable suture of thescleral � ap and subconjunctival biodegradable collagen matriximplant (OlogenTM) in eyes with a cataract and primary open-angleglaucoma. Ref Bul Ophthalmol 2009; 6:17-26.
5. Anguelov B. Surgical treatment of some types of advanced glaucomawith a single step implantation of two different implants - Ex-PRESS®
and OlogenTM. Bul F Glaucoma 2012; 2(4):4-17.6. Anguelov B. Trabeculectomy with absorbable suture of the scleral
� ap and subconjunctival biodegradable collagen matrix implant (OlogenTM) in primary open-angle glaucoma Ref Bul Ophthalmol2010; 1:21-8.
7. Anguelov B. Trabeculectomy with absorbable suture of the scleral � apand subconjunctival biodegradable collagen matrix implant (OlogenTM)in refractory glaucoma. Ref Bul Ophthalmol 2009; 5:23-30.
8. Aptel F, Dumas S, Denis P. Ultrasound biomicroscopy and optical coherence tomography imaging of � ltering blebs after deep sclerectomy with new collagen implant. Eur J Ophthalmol 2009; 19:223-30.
9. Beckers HJ, Kinders KC, Webers CA. Five-year results of trabeculectomy with mitomycin C. Graefes Arch Clin Exp Ophthalmol 2003 Feb; 241(2):106-10.
10. Beltran-Agullo L, Trope GE, Jin Y, Wagschal LD, Jinapriya D, BuysYM. Comparison of visual recovery following ex-press versustrabeculectomy: Results of a Prospective Randomized Controlled Trial. J Glaucoma 2013 Jun 25. [Epub ahead of print]
11. Bindish R, Condon GP, Schlosser JD, D’Antonio, Lauer KB, Lehrer R. Ef� cacy and safety of mitomycin-C in primary trabeculectomy: � ve-year follow-up. Ophthalmology 2002; 109:1336-41.
12. Boey PY, Narayanaswamy A, Zheng C, Perera SA, Htoon HM, Tun TA, Seah SK, Wong TT, Aung T. Imaging of blebs after phacotrabeculectomy with OlogenTM collagen matrix implants. Br J Ophthalmol 2011 Mar; 95(3):340-4.
13. Cantor LB, Katz LJ, Cheng SW, Chen E, Tong KB, Peabody JW. Economic evaluation of medication, laser trabeculoplasty and � lteringsurgeries in treating patients with glaucoma in the U.S. Curr Med ResOpin 2008; 24(10):2905-18.
14. Cillino S, Di Pace F, Cillino G, Casuccio A. Biodegradable collagenmatrix implant vs mitomycin-C as an adjuvant in trabeculectomy:a 24-month, randomized clinical trial. Eye (Lond) 2011 Dec; 25(12):1598-606.
15. Dahan E, Ben Simon GJ, Lafuma A. Comparison of trabeculectomy and Ex-PRESS® implantation in fellow eyes of the same patient: a ®
prospective, randomised study. Eye (Lond) 2012 May; 26(5):703-10.16. DeBry PW, Perkins TW, Heatley G, Kaufman P, Brumback LC.
Incidence of late-onset bleb-related complications following trabeculectomy with mitomycin. Arch Ophthalmol 2002; 120:297-300.
17. Estermann S, Yuttitham K, Chen JA, Lee OT, Stamper RL.Comparative In Vitro Flow Study of 3 Different Ex-PRESS® Miniature®
Glaucoma Device Models. J Glaucoma. 2012 Jan 20. [Epub ahead of print].
18. Gedde SJ, Herndon LW, Brandt JD, Budenz DL, Feuer WJ, SchiffmanJC. Surgical complications in the Tube Versus Trabeculectomy studyduring the � rst year of follow-up. Am J Ophthalmol 2007; 143:23-31.
19. Green� eld DS, Suñer IJ, Miller MP, Kangas TA, Palmberg PF, FlynnHW Jr. Endophthalmitis after � ltering surgery with mitomycin. ArchOphthalmol 1996; 114:943-9.
20. Hendrick AM, Kahook MY. Ex-PRESS mini glaucoma shunt: surgicaltechnique and review of clinical experience. Expert Rev Med Devices2008 Nov; 5(6):673-7.
21. Hsu W-C, Ritch R, Krupin T, Chen HS-L. Tissue bioengineeringfor surgical bleb defects: an animal study. Graefes Arch Clin ExpOphthalmol 2008; 246:709-17.
22. Hsu WC, Spilker MH, Yannas IV, Rubin PA. Inhibition of conjunctivalscarring and contraction by a porous collagen-glycosaminoglycanimplant. Invest Ophthalmol Vis Sci 2000 Aug; 41(9):2404-11.
23. Hu CY, Matsuo H, Tomita G, Suzuki Y, Araie M, Shirato S, TanakaS. Clinical characteristics and leakage of functioning blebs after trabeculectomy with mitomycin-C in primary glaucoma patients. Ophthalmology. 2003 Feb; 110(2):345-52.
24. Jong L, Lafuma A, Aguadé AS, Berdeaux G. Five-year extension of aclinical trial comparing the Ex-PRESS® glaucoma � ltration device and®
trabeculectomy in primary open-angle glaucoma. Clin Ophthalmol. 2011; 5:527-33.
25. Kaplan-Messas A, Traverso C, Glovinsky Y et al. The Ex-PRESS®
miniature glaucoma implant: intermidiate results of prospective multi-center study. Invest Ophthalmol Vis Sci 2002; 542:52.
26. Kuroyedov A, Ogorodnikova V. A long-term period of observation of patients with advanced glaucoma after implantation of Ex-PRESS®
glaucoma � ltration device. Bul F Glaucoma 2012; 2(2):15-21.27. Lama PJ, Fechtner RD. Anti� brotics and wound healing in glaucoma
surgery. Surv Ophthalmol. 2003 May-Jun; 48(3):314-46.28. Landers J, Martin K, Sarkies N, Bourne R, Watson P. A twenty-
year follow-up study of trabeculectomy: risk factors and outcomes.Ophthalmology 2012 Apr; 119(4):694-702. Epub 2011 Dec 23.
29. Lankaranian D, Razeghinejad MR, Prasad A, Fakhraie G, Freitas DJ, Ichhpujani P, Moster MR. Intermediate-term results of the Ex-PRESS® miniature glaucoma implant under a scleral � ap in previously®
operated eyes. Clin Experiment Ophthalmol 2011 Jul; 39(5):421-8.30. Law SK, Nguyen AM, Coleman AL, Caprioli J. Severe loss of
central vision in patients with advanced glaucoma undergoingtrabeculectomy. Arch Ophthalmol 2007; 125:1044-55.
31. Long LA. The Ex-PRESS® glaucoma shunt versus trabeculectomy®
in open-angle glaucoma: a prospective randomized study. Adv Ther March 2009; 26(3):336-45.
32. Lusthaus JA, Kubay O, Karim R, Wechsler D, Booth F. Primarytrabeculectomy with mitomycin C: safety and ef� cacy at 2 years. ClinExperiment Ophthalmol 2010 Dec; 38(9):831-8.
33. Maris P.J., Smith M.E., Netland P.A. Clinical outcomes with theEx-PRESS® miniature glaucoma implant. Invest Ophthalmol Vis Sci ®
2005;46.34. Papaconstantinou D, Georgalas I, Karmiris E, Diagourtas A,
Koutsandrea C, Ladas I, Apostolopoulos M, Georgopoulos G.Trabeculectomy with OlogenTM versus trabeculectomy for thetreatment of glaucoma: a pilot study. Acta Ophthalmol 2010; 88:80-5.
35. Peter J, Maris G, Ishida K, Netland A. Comparison of trabeculectomywith Ex-PRESS® miniature glaucoma device implanted under scleral®
� ap. J Glaucoma 2007; 16:14-9.36. Poulsen EJ, Allingham RR. Characteristics and risk factors of
infections after glaucoma � ltering surgery. J Glaucoma. 2000 Dec;9(6):438-43.
37. Reinthal EK, Rohrbach JM, Grisanti S. Glaucoma drainage implants.Klin Monbl Augenheilkd Jan 2010; 227(1):49-55.
38. Rosentreter A, Schild AM, Dinslage S, Dietlein TS. Biodegradableimplant for tissue repair after glaucoma drainage device surgery. JGlaucoma. 2012 Feb; 21(2):76-8.

2392013, Vol. 3, Issue 5
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
39. Rosentreter A, Schild AM, Jordan JF, Krieglstein GK, Dietlein TS. A prospective randomised trial of trabeculectomy using mitomycin C vsan OlogenTM implant in open angle glaucoma. Eye 2010; 24:1449-57.
40. Scharioth BG, Craven R. Trabecular bypass surgery. Glaucomasurgery, 2010; 1:304-7.
41. Soltau JB, Rothman RF, Budenz DL, Green� eld DS, Feuer W,Liebmann JM, Ritch R. Risk factors for glaucoma � ltering blebinfections. Arch Ophthalmol 2000; 118:338-42.
42. Song A, Scott IU, Flynn HWJr, Budenz DL. Delayed-onset blebassociated endophthalmitis: clinical features and visual acuityoutcomes. Ophthalmology 2002; 109:985-91.
43. Terminology and guidelines for glaucoma. 3rd edition Europeanglaucoma society 2008.
44. Tham CC, Lai JS, Poon AS et al. Results of trabeculectomy with
adjunctive intraoperative mitomycin C in Chinese patients with glaucoma. Ophthalmic Surg lasers Imaging 2006; 37:33-41.
45. Wamsley S, Moster MR, Rai S, Alvim HS, Fontanarosa J. Results of the use of the Ex-PRESS® miniature glaucoma implant in technically®
challenging, advanced glaucoma cases: a clinical pilot study. Am JOphthalmol Dec 2004; 138(6):1049-51.
46. Wang W, Zhou M, Huang W, Zhang X. Ex-PRESS® implantation®
versus trabeculectomy in uncontrolled glaucoma: a meta-analysis.PLoS One. 2013 May 31; 8(5):e63591.
47. Young MJ, Borrás T, Walter M, Ritch R. Tissue bioengineering:potential applications to glaucoma. Arch Ophthalmol 2005 Dec;123(12):1725-31.
48. Zelefsky JR, Hsu WC, Ritch R. Biodegradable collagen matrix implantfor trabeculectomy. Expert Rev Ophthalmol 2008; 3:613-7.