the hepatic vasculature: case presentation - ucsf cme m. crawford, m.d., ph.d. ... intraabdominal...
TRANSCRIPT

The Hepatic Vasculature:Missed Lesions, Missed Diagnoses
James M. Crawford, M.D., Ph.D.Department of Pathology and Laboratory Medicine
North Shore-Long Island Jewish Health System
•••
• •
•
••
•
••• • • •
♦
Case presentation73 yo female
-h/o hypertension, GE reflux
-Elective EGD for abd pain, nausea, distention, bloating, constipation x months-No abnormalities identified on esophagogastroduodenoscopy-Video capsule placed without complications
-6h later: returned for download of video capsule-Complained of epigastric pain, chest and back. Admitted for further eval.-Cardiac enzymes negative-CT: multiple foci of sub-diaphragmatic free air lateral to esophagus
-Presumed diagnosis of esophageal perforation-CT follow-up at 2 days: ‘perforation improving’
-5th day of admission: syncopal episode, thought due to dehydration (was NPO)
-6th day of admission: Hct declined from 29.6 to 11.9; Hb from 11.1 to 4.2 g/dl-transferred to MICU, treated for dehydration and hypotension (no blood given)-cardiac arrest, unable to be resuscitated
Case 3 Case 3

Case 3
Case presentation (Cont’d)Autopsy findings:-2 liters free blood in abdomen-Subcapsular hepatic hematoma (10.0 x 8.0 cm), left lobe of liver
-ruptured capsule-Left hepatic artery dissection, communicating with subcapsular hematoma
-rupture of left hepatic artery, into dissection-Main hepatic artery, right hepatic artery: dissection, without rupture
Hepatic Vascular LesionsClinical History: often not suspected
Pathology Examination (gross and microscopic): - may be missed- if seen, may be misinterpreted- if correctly diagnosed, may be completely change course
of clinical management
Hepatic Vascular LesionsTwo angles on hepatic vascular disease:
- Histopathologic examination of percutaneous liver biopsies
- Examination of explanted liver
- Post-mortem examination
Generally not an issue in partial hepatectomy resections
NOTE: Transplant pathology and nodular lesions are not covered in this presentation

Vascular Pathology of the Liver:a conceptual framework
Inflow: Hepatic ArteryPortal VeinPresinusoidal
Sinusoidal: CirrhosisOther
Outflow: Hepatic VenousOutflow Obstruction
Ca: 1550
Liver Vasculature: Basic facts
Normal Liver: 1200-1400 g = 2.5% of body weight
Blood Flow: 25% of cardiac output2/3 via portal vein1/3 via hepatic artery
Portal vascular tree: 17 to 20 orders of dichotomous branchesPortal vein blood enters parenchyma directly via “septal venules”Hepatic arterial blood supplies: bile ducts, capsule, vasa vasorum
enters parenchyma as post-capillary blood in portal blooddirect arteriolar supply of parenchyma is negligible in humans
Hepatic venous tree: fewer ramifications than portal treedrains into: right, middle, and left hepatic veins
Liver Vasculature: “third inflow”- Cholecystic veins through the gallbladder bed*- Extrahepatic parabiliary venous system- Extragastric paraumbilical venous system through falciform ligament
Implications: - Apparent “pseudolesions” on CT perfusion studies,
which are, in fact, artefact of differential blood flow- May rarely create local metabolic changes, e.g. differential steatosis
Yoshimitsu et al, Radiographics 2001; 21: S81-S96
*

PortalVein
Bile HepaticDuct Artery
The perfect Portal Tract
Approximately 11 portal tracts/biopsy (range: 3-23) = 6 per cm (14G)62% contain a portal vein, 91% a hepatic artery, and 93% a bile ductBUT: 2.3 bile ducts, 2.6 hepatic arteries, and 0.7 portal veins per PT
Crawford AR et al., Hepatology 1998; 28: 323-331
Liver TransplantationOther: Systemic vascular disease
Intraabdominal inflammationulcerative colitis, peritonitisintra-arterial chemotherapyendoscopic injection of sclerosing agents
Hepatic Artery Thrombosis
Cholangitis Infarction
Hepatic artery occlusion in the liver transplant: infarction of the biliary tree
Parenchymalinfarction
Hilarinfarction

Hepatic Artery Thrombosis
Polyarteritis Nodosa
Systemic Vascular Disease:Polyarteritis nodosaRheumatologic disorders with vasculitisSystemic amyloidosisHyaline arteriosclerosis
Portal Vein Obstruction
Portal vein thrombosis:Surgical complications, traumaIntrabdominal sepsis, phlebitisHepatocellular carcinomaMalignancy in pancreas, hepatic hilumThrombogenic disorders, Pancreatitis(can occur in setting of cirrhosis)
acute thrombosis of portal vein
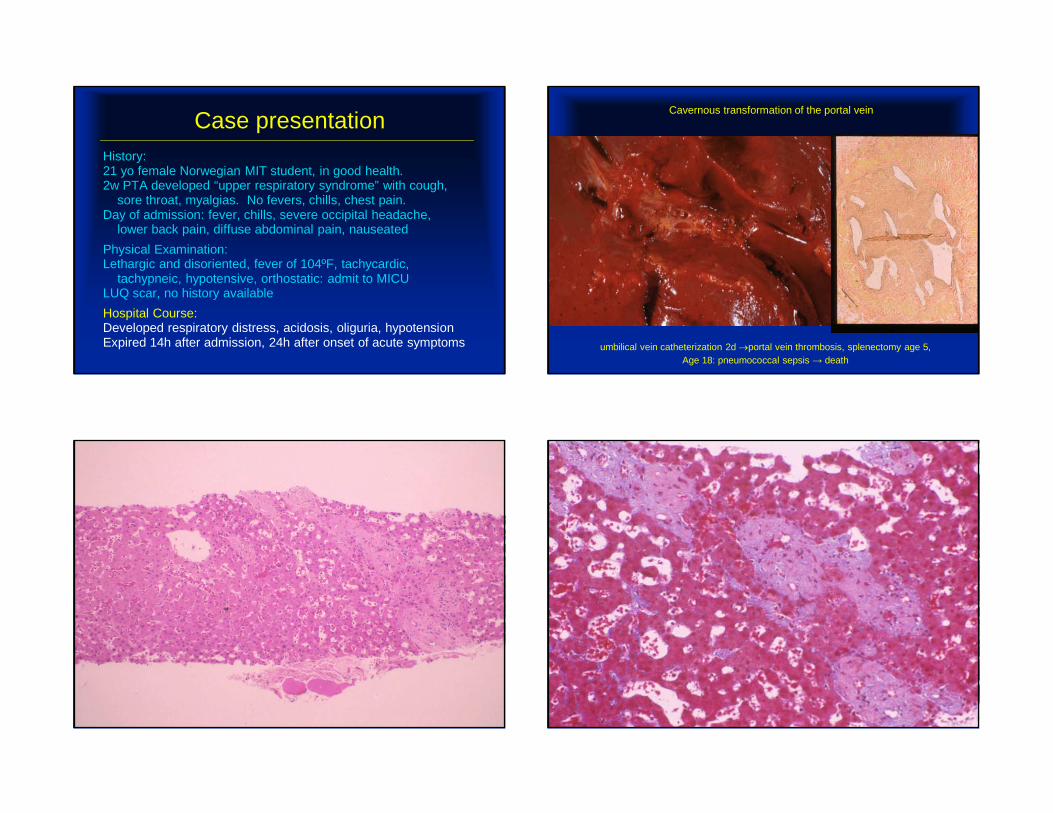
Case presentationHistory:21 yo female Norwegian MIT student, in good health.2w PTA developed “upper respiratory syndrome” with cough,
sore throat, myalgias. No fevers, chills, chest pain.Day of admission: fever, chills, severe occipital headache,
lower back pain, diffuse abdominal pain, nauseated
Physical Examination:Lethargic and disoriented, fever of 104ºF, tachycardic,
tachypneic, hypotensive, orthostatic: admit to MICULUQ scar, no history available
Case presentationHistory:21 yo female Norwegian MIT student, in good health.2w PTA developed “upper respiratory syndrome” with cough,
sore throat, myalgias. No fevers, chills, chest pain.Day of admission: fever, chills, severe occipital headache,
lower back pain, diffuse abdominal pain, nauseated
Physical Examination:Lethargic and disoriented, fever of 104ºF, tachycardic,
tachypneic, hypotensive, orthostatic: admit to MICULUQ scar, no history available
Hospital Course:Developed respiratory distress, acidosis, oliguria, hypotensionExpired 14h after admission, 24h after onset of acute symptoms
Cavernous transformation of the portal vein
umbilical vein catheterization 2d →portal vein thrombosis, splenectomy age 5, Age 18: pneumococcal sepsis → death

Hepatoportal Sclerosis:Dense sclerosis of portal tractsObliteration of portal vein radiclesNo fibrous septa or cirrhosisIdiopathic vs. smoldering inflammation
arsenic, myeloproliferative syndromes, peritonitisazathioprine, cyclophosphamide, methotrexate
Presinusoidal Obstruction(Non-cirrhotic portal hypertension) Case presentation
58 year old white male-endstage liver disease, “cryptogenic cirrhosis”-endstage renal disease, secondary to hypertension and diabetes mellitus
Liver/kidney transplant performed
Case 2 Case 2

Case 2 Case 2
Case 2 Case 2

Case 2 Case 2
Case 2 Case 2

Case 2 Case 2
Case 2 Case 2

Case 2 Case 2
Case presentationFinal Diagnosis:-Consistent with partially reversed cirrhosis-suspect etiology = non-alcoholic fatty liver disease
Fiel I, Thung S, Prodromos H, et al. HPS. Am J Surg Path 2007; 31: 607-614
Incomplete Septal Cirrhosis

Reversal of Cirrhosis
Treated hemochromatosis
Hepatocellular carcinoma in “reversed cirrhosis”Blumberg RS, Gastroenterology 1988; 95:1399-1402
1957: initial diagnosis, age 37
1985: phlebotomy x 28 years, age 65
Reversal of Cirrhosis
Treated hemochromatosisTreated autoimmune hepatitis, Wilson’s?Treated viral hepatitis?
NOTE: vascular lesion remains →“non-cirrhotic” portal hypertension
1957: initial diagnosis, age 37
1985: phlebotomy x 28 years, age 65 Hepatocellular carcinoma in “reversed cirrhosis”Blumberg RS, Gastroenterology 1988; 95:1399-1402
Incomplete Septal Cirrhosis:No substantive portal tract fibrosisFibrous septa (complete bridging and incomplete): no cirrhosis
note: approximation of portal tracts and terminal hepatic veinsDe novo parenchymal fibrosing injury vs. partially resorbed cirrhosis
Hepatoportal Sclerosis:Dense portal tract fibrosis, obliteration of portal vein radiclesNo significant parenchymal fibrosisDe novo portal fibrosing injury vs. partially resorbed cirrhosis
Non-cirrhotic portal hypertensionde novo injury vs. reversal of cirrhosis
Wanless IR et al., Arch Pathol Lab Med 2000; 124: 1599-1607
Case 2

Incomplete Septal Cirrhosis ???
Presinusoidal Obstruction
Nodular Regenerative Hyperplasia:No fibrosis at allNodules throughout the liverSmoldering vascular injuryCompensatory hyperplasia
Rheumatologic conditions, BMTx, Solid organ TxDiagnosis very difficult on liver biopsy
(AASLD Post-graduate Course 1987)
(Non-cirrhotic portal hypertension)
Incomplete Septal Cirrhosis:No substantive portal tract fibrosisFibrous septa (complete bridging and incomplete): no cirrhosis
note: approximation of portal tracts and terminal hepatic veinsDe novo parenchymal fibrosing injury vs. partially resorbed cirrhosis
Hepatoportal Sclerosis:Dense portal tract fibrosis, obliteration of portal vein radiclesNo significant parenchymal fibrosisDe novo portal fibrosing injury vs. partially resorbed cirrhosis
Nodular Regenerative Hyperplasia:No fibrosis of portal tracts or parenchymaRegenerative nodules with intervening parenchymal atrophyDe novo smoldering vascular injury vs. partially resorbed cirrhosis
Non-cirrhotic portal hypertensionde novo injury vs. reversal of cirrhosis
Wanless IR et al., Arch Pathol Lab Med 2000; 124: 1599-1607

Sinusoidal Obstruction
Cirrhosis: causes of portal hypertensionIncreased sinusoidal resistancePortal-to-arterial shuntsFast vascular channels, arteriolar resistance
Crawford JM, in MacSween 4th Edition, 2002, Fig. 13.1

Crawford JM, in MacSween 4th Edition, 2002, Fig. 13.4: based on Wanless IR, Hepatology 1995; 21: 1238-1247
Imaging studies: thrombosis of larger portal veins: 17% of liversOkuda K, et al., Gastroenterology 1985; 89: 279-286
Autopsy: thrombosis of larger portal veins: 39% of liversobliteration of small hepatic veins: 74% of livers
Hou & McFadzean, J Pathol Bact 1965; 89: 473-480
Liver TX: obliterative lesions of portal veins: 36% of liversrelatively uniform distribution
obliterative lesions of hepatic veins: 70% of liversnon-uniform distribution
solitary portal vein obliteration → regional variation in nodule sizedual obliteration → confluent fibrosis and parenchymal extinction
Wanless IR et al., Hepatology 1995; 21: 1238-1247
Role of vascular thrombosis in development of cirrhosis
Sinusoidal DisordersAlcoholic Cirrhosis

Sinusoidal Spread of Cancer
Amyloid
Kappa Lambda

Sinusoidal Obstruction
Sickle Cell Disease: intravascular sickling
Sickle Cell Disease
Sinusoidal Obstruction
Sickle Cell Disease: intravascular sickling
Infiltrative malignancy: intravascular tumorbreast, lung, leukemia, melanoma
Amyloidosis, Congenital Syphilis
Ecclampsia: intravascular coagulation
Sickle Cell Disease Metastatic Malignant Melanoma
Sinusoidal Obstruction: DIC in Ecclampsia Ecclampsia

??? Congenital Syphilis
Venous Outflow Obstruction
Centrilobular congestionright heart failure: congestion only
Centrilobular hemorrhagic necrosis:congestion + forward flow ischemia“nutmeg liver”
Centrilobular hemorrhagic necrosis

Venous Outflow Obstruction
“Cardiac Cirrhosis” = Cardiac SclerosisChronic right sided heart failure only: veno-centric fibrosis onlyChronic right sided heart failure + hepatic vein thrombosis: rapid fibrosis
Cardiac sclerosis
Venous Outflow Obstruction
Hepatic vein thrombosis = Budd-Chiari Syndrome:Major hepatic veins, Hypercoagulable statesMyeloproliferative disorders: polycythemia veraCoagulative disorders: antiphospholipid syndromeIntra-abdominal cancers: HCCHormonal: pregnancy, oral contraceptives (+ other)
Obliterative hepatocavopathy(inferior vena cava thrombosis)
Idiopathic / coagulation disorders; associated with infections (in Nepal)
The IVC thrombosis resolves, leaving incomplete membranous web in IVC near hepatic vein orifices
Not to be confused with normal ‘eustachian valve’ in IVC

Sinusoidal Obstruction Syndrome
Veno-occlusive DiseaseTerminal hepatic veins, irregular distributionBM Tx; hypercoagulable statespyrrolizidine alkaloids (still)hepatic toxicity, endothelial damage, occlusion
Vascular Diseases of the LiverConclusion
Consideration of vascular disease is critical in differential diagnosisof virtually every hepatic pathology
Hepatic artery compromise:non-transplant setting: usually a smoldering subclinical processtransplantation setting: severe, usually leads to loss of organ
Portal vein compromise:large vessel: dramatic, may be life-threateningsmall vessel: subclinical, may give rise to pre-sinusoidal hypertension
Sinusoidal obstruction:Cirrhosis: sinusoids, small portal veins, small hepatic veinsAssortment of infiltrative disorders
Hepatic venous outflow obstruction:Large vessel: Budd-Chiari syndrome - acute, sub-acuteSmall vessel: Veno-occlusive disease (sinusoidal obstruction syndrome)