testosterone - laboratoire dr. collard: root be · pdf fileblood levels of testosterone were...
TRANSCRIPT

1

2
Testosterone -deficient
Testosterone -
sufficient
Poor beard & moustache
Small wrinkles
Hypotonic
face muscles
Small wrinkles
Dry eyes
Pale face
Dry, thin hair
The importance of Testosterone
3
Low
Testosterone -deficient
Testosterone –
excessive

4
TESTOSTERONE ENANTHATE 100 mg injections in
aging men & effects on serum lipoproteins
Figure : effects of 3 month of 100 mg testosterone enanthate injections (1
x/week) or placebo injections in 13 healthy men aged 57-76 years old
(Tenover JS, J Clin Endocrinol Metab, 1992, 75: 1092-1098)
0
50
100
150
200baselineTotal
chole-
sterol
(mg/dl)
placebo
testo
0
40
80
120
LDL
cholesterol
199 203
177 128 132
113
placebo
testo
(mg/dl)

5
Testosterone
=> Serum
Total cholesterol

6
TESTOSTERONE ENANTHATE 100 mg injections
in aging men & effects on serum lipoproteins
Figure: effects of 3 month of 100 mg testosterone
enanthate injections (1 x/week) or placebo
injections in 13 healthy men aged 57-76 years old
(Tenover JS, J Clin Endocrinol Metab, 1992, 75: 1092-1098)
0
15
30
45
baselineHDL
(mg/dl)
placebotesto
0
25
50
75
100
125
Triglycerids
(mg/dl)49
4644 112
123
105
placebo
testo

7
Total Cholesterol
American Heart association

8
Serum cholesterol
1 mmol/l = 39 mg/dl (38,647 mg/dl)
3 mmol/l= 115 mg/dl
5 mmol/l = 193 mg/dl
8 mmol/l = 308 mg/dl

9
Men with serum cholesterol => life expectancy
0
3
6
9
+ 3,8 yrs
Men with low serum cholesterol
(less than 200 mg/dl)
Increase
in life span
n = 92.488 men
(18-39 yrs)
+ 8,7 yrs
Figure: Data from 3 studies:
Chicago Heart Association project (n= 11,017 men (18-39 yrs) followed in 1967-1973;
Peoples Gas Company Study (n= 1266 men (25-39 yrs) followed in 1959-1963;
Multiple risk Factor Intervention Trial (n= 62,205 men (35-39 yrs) evaluated in 1973-1975.
A constant, progressive, solid & independent exists between serum cholesterol & long
term risk of coronary disease & cardiovascular mortality versus men with low cholesterol.
Stamler J, Daviglius ML, Garside DB, et al. Relationship of baseline serum cholesterol levels in 3 large cohorts of
younger men to long-term coronary, cardiovascular, & all-cause mortality & longevity. JAMA 2000; 284: 311-318

10
Testosterone
=> Serum
HDL cholesterol

11
HDL Cholesterol
American Heart association

12
Men with serum HDL cholesterol
=> all-cause mortality
0
0,5
1
All-cause
Mortality
(Relative
risk)
Serum HDL Cholesterol
p < 0.05
Figure: A high HDL cholesterol is a sign. protector against all-cause
mortality, & near sign. protector against cardiovasc. dis. mortality.
Okamura T, ….,Ueshima H;The inverse relationship between serum high-density lipoprotein cholesterol level and all-
cause mortality in a 9.6-year follow-up study in the Japanese general population. Atherosclerosis. 2006
Jan;184(1):143-50 JShiga Un.apan
n = 7175 Japanese residents ; 9.6 yrs of foloow-up
(1.04 (40
mg/dl)-1.55
mmol/L
(59.61),
p < 0.05
0.63
(0.41-
0.94)
0.73
(0.41-
0.94)
Men
-27 % -37 %
very high HDL-C category (>
or = 1.82 mmol/L = 70 mg/dl),
1
Women

13

14
LDL Cholesterol
with age
HDL Cholesterol
with age
in men
Atherogenic ratio
LDL/HDL Cholesterol
with age
Men
Women
LDL
HDL
LDL/HDL

15
0
10
20
30
40
50
"good" HDL cholesterol "bad" VLDL cholesterolBlood cholesterol levels (mg/dl)
men with
low testosterone
Figure : The blood HDL cholesterol level increases and the level of the VLDL cholesterol declines proportionately to the increase of testosterone in the blood.
247 men of middle age participated in this study. The extreme values of blood levels of testosterone were for the three groups respectively 780-5330, 6.420-7.610 and 9.370-16.500 pg/ml.
(Gutai J et al, AM J Cardiol, 1981, 48 : 897-902)
men with
average testosterone
men with
high testosterone
TESTOSTERONE &
BLOOD CHOLESTEROL
VLDL
HDL

16
the higher the plasma testosterone :
- the higher the HDL cholesterol (+ 12 % for the highest quartile) (in 391 men aged 30-79 years)( 1,2,3)
- the the VLDL cholesterol (1, 3)
- the the triglycerids (3)
the higher the plasma DHT :
the higher the HDL cholesterol (4) (in coronary heart disease patients)(1) Khaw KIT et al, Arterioscler Thromb, 1991, 11(3): 489-94 for study in 391 men aged 30-79 yrs
(2) Freedman DS et al, Arterioscler Thrombos, 1991, 11(2): 307-15 for study in 4.062 men
(3)Gutai I et al, Am J Cardiology, 1981, 48: 897-902 (4) Hämäläinen E et al, Atheroscdlerosis, 1987, 67: 155-62
Plasma Testosterone => Serum Lipids

17
Oral testosterone undecanoate (Andriol®) in men with
coronary heart disease :
- E2/testo : testo, E2 =
- sign. total cholesterol, TG, HDL =
- apolipoproteins A & B =
(Wu S et al, Chim Med Sci J, 1992, 7(3): 137-41)
Injectable testosterone esters (Sustanon®)
(Wu S et al, Chin Med Sci J, 1993, 8(4): 207-9)
in coronary heart patients (60-75 years) :
- thromboxane A-2 => constrictory peptide
- prostaglandins 2 =>dilatatory peptide
peptides that have dilatatory & constrictory effects on the coronary arteries
Testosterone therapy =< Cardiovascular blood parameters
18
0
0,2
0,4
0,6
0,8
1
1,2
1,4
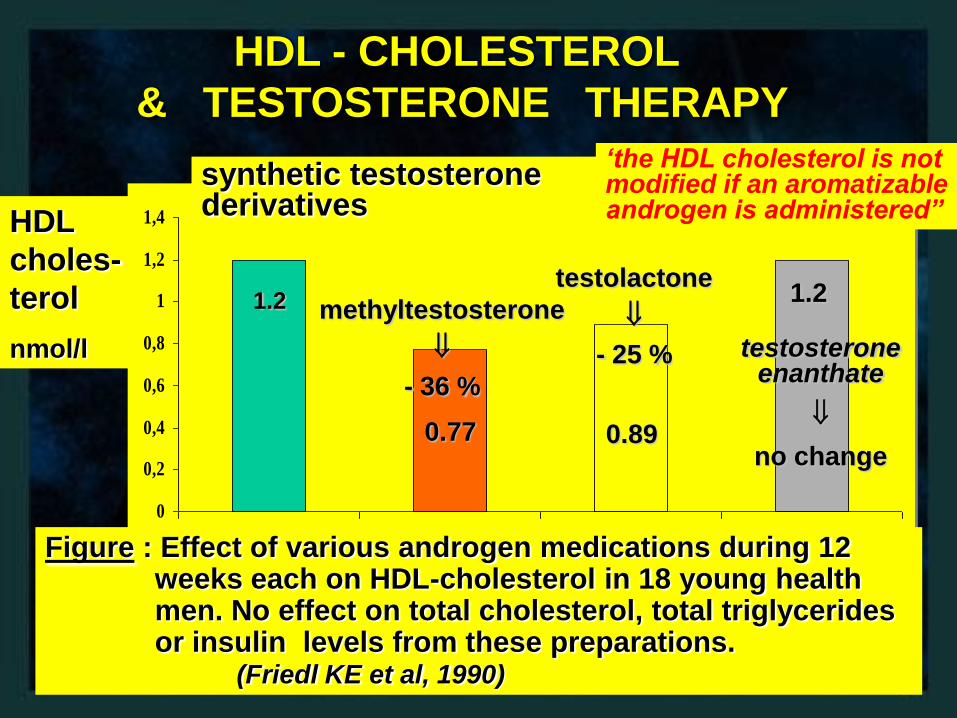
HDL - CHOLESTEROL
& TESTOSTERONE THERAPY
HDL
choles-
terol
nmol/l
Figure : Effect of various androgen medications during 12 weeks each on HDL-cholesterol in 18 young health men. No effect on total cholesterol, total triglycerides or insulin levels from these preparations.
(Friedl KE et al, 1990)
1.2
0.77 0.89
1.2
synthetic testosterone derivatives
‘the HDL cholesterol is not modified if an aromatizable androgen is administered”
methyltestosterone
- 36 %
testolactone
- 25 % testosterone enanthate
no change

19
Testosterone
=>
Serum
Triglycerides

20
Serum Testo => correlated negatively w/ Serum Triglycerides & Lipoprotein a
0
50
100
150Serum
levels
(% versus
healthy
controls)
Men + low testosterone (< 270 ng/ml)
Figure: Low plasma T level may be arisk factor for coronary heart
disease, which may relate to the changes of plasma lipoproteins.
Zhao S, Li X, Wang Z. Plasma levels of lipids, lipoproteins and apolipoproteins affected by endogenous testosterone.
Hunan Yi Ke Da Xue Xue Bao. 1998;23(3):299-301 Hunan Medical University, Changsha
n = 201subjects, among them 102 patients + coronary heart disease & 99 healthy subjects
+34 %
- 14 %
100 %
Lipoprotein aTriglyce-
rides
25 vs
17 g/L1.47 vs
1.10
mmol/
L
HDL-
cholesterol
p < 0.05 for all
HDL 3-
chole-
sterol
Men + normal
testosterone
> 270 ng/ml
1.31 vs
1.44
mmol/L
0.88 vs
1.02
mmol/L
+ 47 %
-11 %

21
Triglycerides
American Heart association

22
Men with serum triglycerides
=> risk of ischemic heart disease
0
1
2
3Ischemic
heart
disease
(Relative
risk)
Serum Triglycerides
p = 0.5
Figure: Men belonging to the highest tertile of serum triglycerides
have an increased risk of developping ischemic heart disease (8 yrs of follow-up, initially aged: 53 - 74 yrs, 229 on 2906 developped the disease).
Jeppesen J, et al. Triglyceride concentration and ischemic heart disease: an eight-year
follow-up in the Copenhagen Male Study. Circulation 1998; 97 (11): 1029-36
n = 2906
white men
Lowest
tertile
p < 0.001
2.2
(1.4 - 3.4)
1.5
(1.0-2.3)
Middle
tertile
+ 50 %
+ 120 %
Highest
tertile
1

23
Testosterone =>
Lipoprotein a

24
Lipoprotein aSerum lipoproteine a
=> should be
< 24 mg/dl (Cheng 2001)
or < 30 mgdl (Koda 1999)
Cheng SW, Ting AC. Lipoprotein (a) level and mortality in patients with critical lower limb ischaemia.
Eur J Vasc Endovasc Surg. 2001 Aug;22(2):124-9. Department of Surgery, The University of Hong Kong Medical Centre, Hong Kong, China.
Koda Y, Nishi S, Suzuki M, Hirasawa Y. Lipoprotein(a) is a predictor for cardiovascular mortality of
hemodialysis patients. Kidney Int Suppl. 1999 Jul;71:S251-3. Kidney Center of Shinraku-en Hospital,
Niigata University, School of Medicine, Japan. [email protected]

25
Men, not women, with lipoprotein a
=> mortality
0
1
2
Relative Risk
(adjsuted for age, sex,; other risk
factors such as total & HDL cholest.,
iglycerides; carotid-wall thickness;
smokin or little effect)g status; tdiabetes
or not,& systolic & diastolic ypertension
had no or little effect)
Serum Lipoprotein a in men
p < 0.05
Figure: Similar analyses for women,which also included adjustment
for estrogen use or nonuse, revealed no suchrelation.
Ariyo AA, Thach C, Tracy R; Cardiovascular Health Study Investigators. Lp(a) lipoprotein, vascular disease, and
mortality in the elderly. N Engl J Med. 2003 Nov 27;349(22):2108-15. Dallas, TX 75212, USA
n =5888 community-dwelling older
adults (65 years of age or older) in
the United States,2375 women and
1597 men
Lowest
quintile
p < 0.05
2.54
(1.59-
4.08)
1.76
(1.31-
2.36)
+ 76 %
2.5 x
1
Highest qukntiles
All-cause
Mortality
Vasc. events
Mortality
3.00
(1.59-
5.65)
Stroke
Risk
p < 0.05
3 x
26
• What is Lp-a? = a lipoprotein particle found in the bloodstream. The structure of the Lp-a particle is very similar to an LDL particle linked to a plasminogen molecule. Plasminogen is involved in dissolving blood clots. The function of Lp(a) is unknown.
• How is Lp-a related to atherosclerosis?
• Lp-a is a marker for the development of atherosclerotic vascular disease. Individuals with elevated Lp-a are definitely at an elevated risk of developing atherosclerosis. Whether Lp-a is directly involved in the atherogenic process has not been determined. The concentration of Lp-a is race specific.
• How is Lp-a treated ? Treatments of Lp-a are very few. Nicotinic acid (vit. B3) has been shown to lower concentration of Lp-a to a small degree as well as estrogen supplementation.
Lipoprotein a - Lp(a) – part 1
Preventive Cardiology website- Victoria

27
Serum Testo => correlated negatively w/ Serum Triglycerides & Lipoprotein a
0
50
100
150Serum
levels
(% versus
healthy
controls)
Men + low testosterone (< 270 ng/ml)
Figure: Low plasma T level may be arisk factor for coronary heart
disease, which may relate to the changes of plasma lipoproteins.
Zhao S, Li X, Wang Z. Plasma levels of lipids, lipoproteins and apolipoproteins affected by endogenous testosterone.
Hunan Yi Ke Da Xue Xue Bao. 1998;23(3):299-301 Hunan Medical University, Changsha
n = 201subjects, among them 102 patients + coronary heart disease & 99 healthy subjects
+34 %
- 14 %
100 %
Lipoprotein aTriglyce-
rides
25 vs
17 g/L1.47 vs
1.10
mmol/
L
HDL-
cholesterol
p < 0.05 for all
HDL 3-
chole-
sterol
Men + normal
testosterone
> 270 ng/ml
1.31 vs
1.44
mmol/L
0.88 vs
1.02
mmol/L
+ 47 %
-11 %

28
Serum testo => neg assoc. w/ Lp-a
Serum testosterone: Lipoprotein a
Patients-Controls Reference
an inverse correlation between T & Lp(a) (r=-0.24, P=0.04).
108 postmenop. women (age 62+/-7 yrs)
Kaczmarek A, Int J Cardiol. 2003 Jan;87(1):53-7
a negative assoc. between serum Total testo & serum TG level & Lp-a (r=-0.163,P<0.05)
201 subjects, among them 102patients with CHD and 99 healthy subjects
Int J Cardiol. 1998 Jan 31;63(2):161-4
No difference in homocysteine
47 p. (5 men; 38 yrs) + SH & 50 controls (4 men; 34 yrs )
Aldasouqi S, Endocr Pract. 2004 Sep-Oct;10(5):399-403, Saudi Arabia
S. higher homocysteine => T4 => reduced hom.
33 women + SH, 25 control women
Sengul E, Endocr Res. 2004 Aug;30(3):351-9 Kocaeli Un., Izmit, Turkey.

29
Chemical castration => reduced or
increases Lp-a!Serum testosterone Patients-Controls Reference
GnRH analog triptorelin => sign. increased serum Lp-a from 278 to 377U/l (P=0.004)
10 healthy men + serum testo reversibly suppressed
for 5 weeks
Kaczmarek A, Int J Cardiol. 2003 Jan;87(1):53-7
Suppression of testosterone => sign. increased serum Lp-afrom 5.5 to 8.5 mg/dL
12 healthy young men + during 3 weeks daily s.c. inj. of Cetrorelix, a GnRH antagonist
von Eckardstein A, J Clin Endocrinol Metab. 1997 Oct;82(10):3367-72
GnRH analog buserelin
=> reduced serum Lp-a
by - 48%
elderly males +
prostate cancer
Arrer E, J Clin Endocrinol Metab. 1996 Jul;81(7):2508-11. Austrai
Finasteride => increases Lp-a, but reduces DHT
13 men + benign prostate hyperplasia
+ finasteride;
15 controls
Denti L, Atherosclerosis. 2000 Sep;152(1):159-66.

30
Serum testo => no assoc. w/ Lp-aSerum testosterone: Lipoprotein a
Patients-Controls Reference
No correlation w/ Lp-a, nor CRP 715 healthy middle-aged men
Van Pottelbergh I, Atherosclerosis. 2003;166(1):95-102
No changes in Lp-a in the study population as a whole, but a 17.6% (p < 0.05) reduction in the subjects + high pre-treatmentLp(a) (> 20 mg/dL).
62 healthy obese patients (21 men aged 32 +/- 9.6years and 41 women aged 37 +/- 14.6 years
Nutr Metab Cardiovasc Dis. 2001 Jun;11(3):153-7
Lp(a) concentrations were not
related to all hormonal & clinical
parameters ; Lp(a), did not
change sign. after treatment
22 + idiopathic
hypogonadotropic
hypogonadism & 9 +
Klinefelter's syndrome
Ozata M, J Clin
Endocrinol Metab.
1996 Sep;81(9):3372-8
no assoc. between sex hormones
& Lp(a) levels, incl. Testo &
DHEAs
33 women + SH, 25 control women
Haffner SM,
Arterioscler Thromb.
1994 Jan;14(1):19-24
Lipoprotein(a) levels increased by similar amounts in both(testosterone treated, 3 mg/dL; placebo treated, 4 mg/dL; P = 1.0).
108 healthy men > 65 years +serum testons >1 SD below the mean for young men
Snyder PJ, Am J Med. 2001 Sep;111(4):255-60.

31
Testo => reduces Lipoprotein a
0
50
100
150Serum
Lipoprotein
a
(% versus
healthy
controls)
Normal men
Figure: testosterone reduces Lp(a) in men primarily by anandrogenic
effect and not by its conversion to estradiol.Publication
Study 2: Zmunda JM, Thompson PD, Dickenson R, Bausserman LL. Testosterone decreases lipoprotein(a) in men. Am J
Cardiol. 1996 Jun 1;77(14):1244-7.
187 vs
140 mg/L
- 28 %
100 %
Study 1 (n = 33 )
Prior
treatment
- 25 %
Testo enanthate
(IM 200 mg/wk
after 16 weeks)Testo
Study 1: Anderson RA, Wallace EM, Wu FC. Effect of testosterone enanthate on serum lipoproteins in man. Contraception.
Testo +
testoslactone
(aromatase
inhibitor)
Study 2
- 37%

32
Testo therapy => no effect on Lp-atestosterone => lipoprotein
A
N = participants Reference
Short 16 wks transd.
testo => no change of
Lp-a, nor CRP
Postmenop .women
+transd.estrogen for at least 8
weeks + 2 mg.d of transd.
testo
Davies SR,
Menopause.
2006;13(1):37-45
Australia
Non sign. reduction of
Lp-a with testosterone.
50 women + surgical
menopause + oral 2 mg of E2
valerate + 40 mg of Testo
undecanoate or placebo for
24 wks
Floter A,
Maturitas. 2004
20;47(2):123-9
Sweden
Lo dose testo => no
differences in Lp-a
22 women + severe PMS
(39.6 yrs) + subcut. T
implants (100 mg/6 months)
for at least 2 yrs
Buckler HM, Clin
Endocrinol (Oxf).
1998
Aug;49(2):173-8
Testo => no effect on
Serum Lp(a)
22 + idiopathic
hypogonadotropic
hypogonadism & 9 +
Klinefelter's syndrome
Ozata M, J Clin
Endocrinol Metab.
1996
Sep;81(9):3372-8

33
The End