technologies for anatomical and geometric … · corneal and anterior segment imaging techniques...
TRANSCRIPT
Seminars in Ophthalmology, Early Online, 1–10, 2013
! Informa Healthcare USA, Inc.
ISSN: 0882-0538 print / 1744-5205 online
DOI: 10.3109/08820538.2013.835844
REVIEW ARTICLE
Technologies for Anatomical and GeometricCharacterization of the Corneal Structure and
Anterior Segment: A Review
David P. Pinero1,2,3Q3
1Department of Ophthalmology (Oftalmar), Medimar International Hospital, Alicante, Spain, 2Foundation forthe Visual Quality (FUNCAVIS), Fundacion para la Calidad Visual, Alicante, Spain, and 3Department of
Optics, Pharmacology and Anatomy, University of Alicante, Alicante, Spain
ABSTRACT
Corneal and anterior segment imaging techniques have become a crucial tool in the clinical practice ofophthalmology, with a great variety of applications, such as corneal curvature and pachymetric analysis,detection of ectatic corneal conditions, anatomical study of the anterior prior to phakic intraocular lensimplantation, or densitometric analysis of the crystalline lens. From the Placido-based systems that allow only acharacterization of the geometry of the anterior corneal surface to the Scheimpflug photography-based systemsthat provide a characterization of the cornea, anterior chamber, and crystalline lens, there is a great variety ofdevices with the capability of analyzing different anatomical parameters with very high precision. To date,Scheimpflug photography-based systems are the devices providing the more complete analysis of the anteriorsegment in a non-invasive way. More developments are required in anterior segment imaging technologies inorder to improve the analysis of the crystalline lens structure as well as the ocular structures behind the iris in anon-invasive way when the pupil is not dilated.
Keywords: Corneal topography, optical coherence tomography, orbscan, scheimpflug photography,ultrasonography
INTRODUCTION
The anatomical and geometric characterizations of thecorneal structure and anterior segment have become acrucial analysis in the clinical practice of ophthalmol-ogy for anterior segment specialists. Due to themultiple applications of the analysis of the cornealand anterior segment structures in ophthalmologyand their relevance for optimizing corneal andintraocular refractive surgery procedures, differentimaging techniques have been developed rapidly inthe last few years, mainly because of recent advancesin refractive surgery.1–11 All of these imagingtechniques provide a specific type of analysis,with some limitations and advantages over theremaining techniques developed. Specifically, the
great majority of imaging devices provide a more orless precise and accurate analysis of a specificanatomical and geometric parameter or parameters,with few instruments attempting to provide anintegral analysis and evaluation of the anteriorsegment, including curvature, asphericity, and thick-ness analysis of cornea and crystalline lens as well asthe measurement of the dimensions of the anteriorsegment space.
The purpose of the present review is to provide ageneral overview of the available technologies for theanatomical and geometric characterization of thecorneal structure and/or anterior segment, showingthe advantages and disadvantages of each of them aswell as the scientific evidence of their precision andclinical applicability.
Correspondence: Dr. David P. Pinero, Oftalmar, Department of Ophthalmology, Medimar International Hospital, Avda. Denia, 78, 03016Alicante, Spain. E-mail: [email protected]
Received 29 March 2013; accepted 7 August 2013; published online 2 2 2
1
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
CORNEAL TOPOGRAPHY
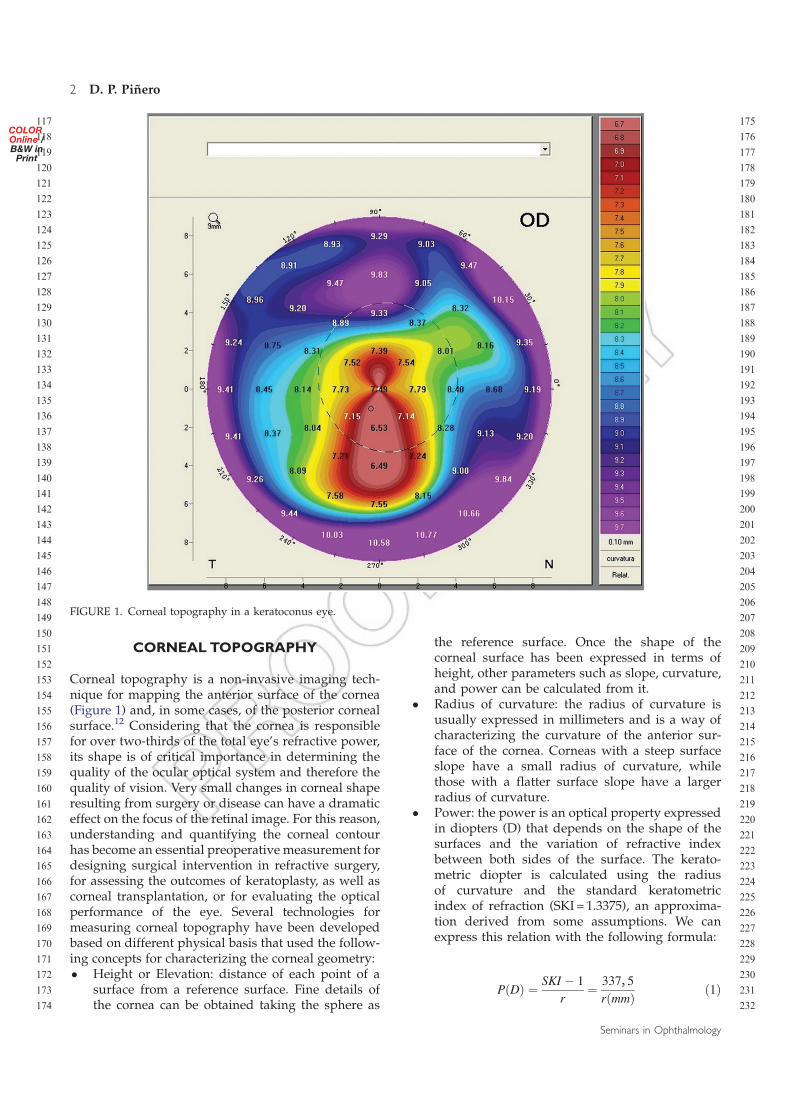
Corneal topography is a non-invasive imaging tech-nique for mapping the anterior surface of the cornea(Figure 1) and, in some cases, of the posterior cornealsurface.12 Considering that the cornea is responsiblefor over two-thirds of the total eye’s refractive power,its shape is of critical importance in determining thequality of the ocular optical system and therefore thequality of vision. Very small changes in corneal shaperesulting from surgery or disease can have a dramaticeffect on the focus of the retinal image. For this reason,understanding and quantifying the corneal contourhas become an essential preoperative measurement fordesigning surgical intervention in refractive surgery,for assessing the outcomes of keratoplasty, as well ascorneal transplantation, or for evaluating the opticalperformance of the eye. Several technologies formeasuring corneal topography have been developedbased on different physical basis that used the follow-ing concepts for characterizing the corneal geometry:� Height or Elevation: distance of each point of a
surface from a reference surface. Fine details ofthe cornea can be obtained taking the sphere as
the reference surface. Once the shape of thecorneal surface has been expressed in terms ofheight, other parameters such as slope, curvature,and power can be calculated from it.
� Radius of curvature: the radius of curvature isusually expressed in millimeters and is a way ofcharacterizing the curvature of the anterior sur-face of the cornea. Corneas with a steep surfaceslope have a small radius of curvature, whilethose with a flatter surface slope have a largerradius of curvature.
� Power: the power is an optical property expressedin diopters (D) that depends on the shape of thesurfaces and the variation of refractive indexbetween both sides of the surface. The kerato-metric diopter is calculated using the radiusof curvature and the standard keratometricindex of refraction (SKI = 1.3375), an approxima-tion derived from some assumptions. We canexpress this relation with the following formula:
PðDÞ ¼SKI ÿ 1
r¼
337, 5
rðmmÞð1Þ
FIGURE 1. Corneal topography in a keratoconus eye.
2 D. P. Pinero
Seminars in Ophthalmology
117
118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232

This concept is a simplification ignoring the factthat the refracting surface is air-tear interface, and itdoes not account for the oblique incidence of incom-ing light in the corneal periphery. As a result, itmiscalculates a true corneal refractive index of 1.376to 1.3375 to correct for some of these factors. That iswhy these diopters more correctly are termed kerato-metric diopters to distinguish them from the dioptersexpressing more precisely the true refractive power ata certain corneal point.
The evolution of the quantitative assessment of theanterior corneal curvature has been progressive andits range of measurement has been extended fromfour points a few millimeters apart measured bykeratometers to a grid of thousands of points coveringalmost the entire cornea, measured by computerizedcorneal topography.
Keratometer
The keratometer uses the ability of the anteriorcorneal surface to behave as a convex mirror. TheHelmholtz keratometer projects four points onto thecornea, creating a reflected image, which can beanalyzed and converted to corneal radius data usingan equation that considers distance from mire tocornea, image, and mire size. Although keratometersare still used commonly in clinical practice, they haveimportant limitations:� They perform measurements of the central 3mm,
accounting only for 6% of the corneal surface.� They assume that the cornea has a perfect
spherocylindrical shape, which is not true.� Information from the periphery is not provided.� They give no information about the central zone
inside the four points measured.
Placido-Based Systems
The patient is positioned sitting down and facing abowl containing the projected pattern, which isfocused on the anterior surface of the patient’scornea. The pattern reflected off from the cornea isanalyzed by a computer that provides data about thegeometric configuration of the cornea in differentkinds of numerical and graphical formats (Figure 2).Some of the errors that examiners can make using aPlacido-based system are the following: focusingerrors, alignment and fixation errors (that couldinduce wrong levels of astigmatisms), wrong calcula-tion of the position of the center from the small centralrings, and increased inaccuracy toward the peripherydue to the lack of accuracy of the preceding points.We can conclude that critical points for a precisemeasurement are accurate alignment, centering andfocusing. These issues depend on the ability of the
examiner to take a good measurement. It is essentialfor obtaining a good exam that the tear film forms asmooth layer over the irregular corneal epithelium.Tear film break-up causes mistracking of the miresand artifacts in the corneal map that appear asirregularity areas or false irregular astigmatism. Forexample, a dry patch could be associated with an areaof focal flattening in the corneal map. In order toavoid disturbing the tear film, corneal topographyshould be performed before giving dilating drops andtaking intraocular pressures.
In spite of being the most widely used, the Placido-based systems present some limitations13,14:� The central circle is dark and therefore no real
information from this central area is obtained.� They are designed to capture information along
meridians radially, not providing direct informa-tion of the corneal geometry circumferentially
� Approximations based on specific algorithms areused which are not very appropriate when highlyirregular corneas are analyzed. Specifically, errorsgreater than 4D may occur in very steep or flatcorneas, keratoconus with local steepening, sharptransition zones after uncomplicated refractivesurgeries, diffusely irregular surfaces after pene-trating keratoplasty, and complex surfaces afterdecentered ablations in refractive surgery orcentral islands.
Scanning-Slit Systems
In the slit-scan systems, a slit is projected sequentiallyonto the cornea at different angles. This is the basisused by the Orbscan II corneal topography systemfrom Bausch & Lomb (Figure 3). A high-resolutionvideo camera captures 40 light slits projected onto thecornea. The diffuse reflection is obtained from the
FIGURE 2. Placido rings image.
Corneal Structure and Anterior SegmentQ1 3
! 2013 Informa Healthcare USA, Inc.
233
234
235
236
237
238
239
240
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284
285
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
301
302
303
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
338
339
340
341
342
343
344
345
346
347
348

cornea, iris, and lens. By triangulation, data isobtained from the anterior and posterior surfaces ofthe cornea and from other structures. These issuespermit this instrument to calculate anterior chamberdepth or full pachymetry of the cornea.12 In addition,this device provides data of the elevation and curva-ture of the posterior corneal surface.
The measurement with this device is significantlydependent on many factors, such as movement of thepatient’s eye, stability of tear film, ability of patients tokeep the eyes wide open, corneal transparency, andthe presence of corneal abnormalities. One of the mainlimitations of this scanning-slit system is the longertime of image acquisition in comparison with anyof the other commercially available instruments.In addition, there are some controversies about thevalidity of some measurements of the posteriorcorneal surface provided by the Orbscan system,especially after some types of keratorefractive surgicalprocedures.15 There are numerous scientific studiesshowing the poor reliability of some measurements ofthe posterior corneal surface provided by the Orbscansystem15–19 and articles reporting the error of under-estimation of the corneal pachymetry after laser-assisted in-situ keratomileusis, which is assumed tobe related to inaccurate detection and location of theposterior corneal surface.20–25
Scheimpflug Photography-Based Systems
Scheimpflug imaging is based on the Scheimpflugprinciple, which occurs when a planar subject is notparallel to the image plane. In this scenario, an obliquetangent can be drawn from the image, object, and lensplanes, and the point of intersection is theScheimpflug intersection, where the image is in bestfocus.26 The Pentacam from Oculus is one of the mostrecognized systems based on this principle.Specifically, this system uses a rotating Scheimpflugcamera to obtain 50 Scheimpflug images of theanterior segment in less than two seconds. Each
image has 500 true elevation points for a totalof 25,000 true elevation points for the surface ofthe cornea (Figure 4). Advantages of the Pentacaminclude the following: (1) high resolution analysisof the entire cornea, including the center of thecornea; (2) ability to measure corneas with accur-acy with severe irregularities, such as keratoconus,which may not be amenable to Placido imaging;and (3) ability to calculate pachymetry from limbus tolimbus.
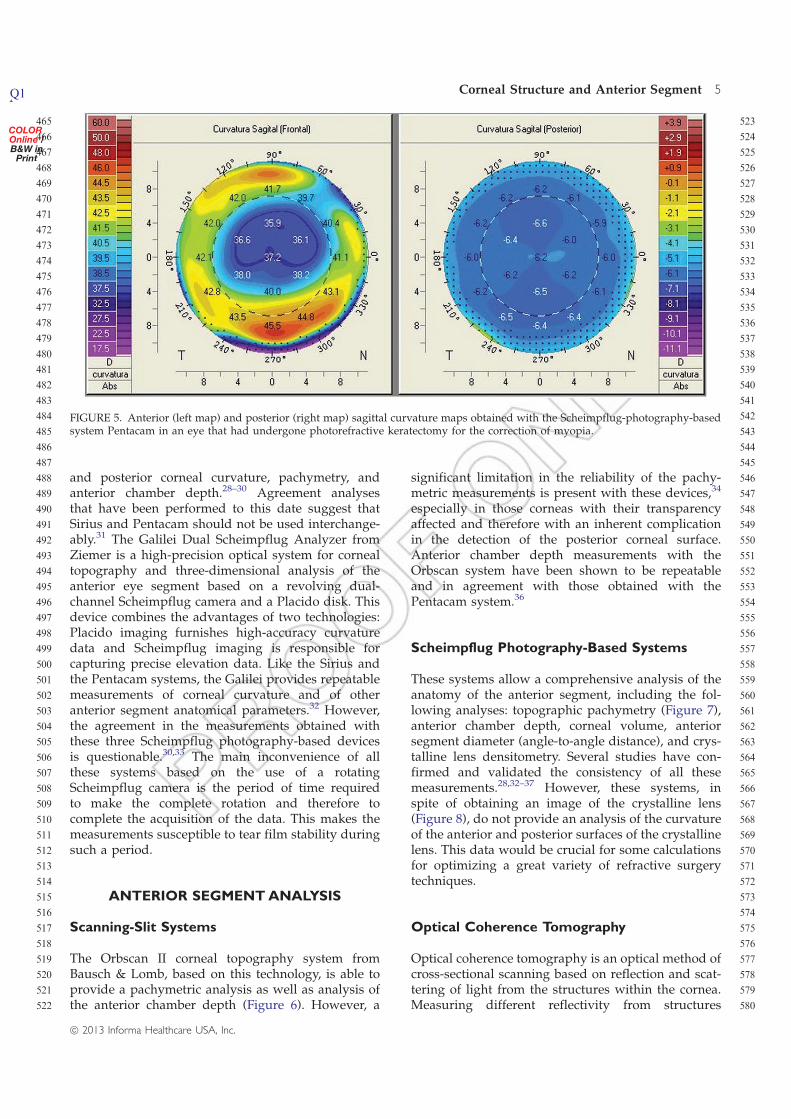
The Pentacam system allows the study of boththe anterior and posterior corneal surfaces and pro-vides more repeatable and reproducible anterior andposterior measurements (Figure 5) of cornealpower than scanning-slit technology. Kawamoritaet al.27 reported 0.19 of agreement for within-raterconsecutive measurements of posterior corneal powermeasurements of diopter (D) with a Scheimpflug-based system and 0.96 D with a scanning-slit systemand for between-rater measurements, of 0.56 D and1.58 D, respectively.
Other systems based on Scheimpflug photographyhave been developed and released commercially, suchas the Sirius or Galilei systems. The Sirius system(CSO, Florence, Italy) is a topography device whichuses the principles of Scheimpflug photography andenables the acquisition and processing of 25 radialsections of the cornea and anterior chamber in veryfew seconds. The combination between two mono-chromatic 360�-rotating Scheimpflug cameras and aPlacido disk allows a full analysis of the cornea andanterior segment, providing tangential and axialcurvature data of anterior and posterior cornealsurfaces, and the global refractive power of thecornea, as well as a biometric estimation of variousstructures, and a corneal wavefront map with ananalysis of visual quality and corneal pachymetrymaps. Specifically, this system allows a measurementof 35,632 points for the anterior corneal surface and30,000 for the posterior corneal surface on high-resolution mode in 1–2 seconds.28 This device hasbeen shown to provide in normal and even inkeratoconus eyes consistent measurements of anterior
FIGURE 3. Scanning-slit system Orbscan II (Bausch & Lomb).
FIGURE 4. Scheimpflug image of the anterior segmentobtained with the Pentacam system (Oculus).
4 D. P. Pinero
Seminars in Ophthalmology
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
412
413
414
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
459
460
461
462
463
464
and posterior corneal curvature, pachymetry, andanterior chamber depth.28–30 Agreement analysesthat have been performed to this date suggest thatSirius and Pentacam should not be used interchange-ably.31 The Galilei Dual Scheimpflug Analyzer fromZiemer is a high-precision optical system for cornealtopography and three-dimensional analysis of theanterior eye segment based on a revolving dual-channel Scheimpflug camera and a Placido disk. Thisdevice combines the advantages of two technologies:Placido imaging furnishes high-accuracy curvaturedata and Scheimpflug imaging is responsible forcapturing precise elevation data. Like the Sirius andthe Pentacam systems, the Galilei provides repeatablemeasurements of corneal curvature and of otheranterior segment anatomical parameters.32 However,the agreement in the measurements obtained withthese three Scheimpflug photography-based devicesis questionable.30,33 The main inconvenience of allthese systems based on the use of a rotatingScheimpflug camera is the period of time requiredto make the complete rotation and therefore tocomplete the acquisition of the data. This makes themeasurements susceptible to tear film stability duringsuch a period.
ANTERIOR SEGMENTANALYSIS
Scanning-Slit Systems
The Orbscan II corneal topography system fromBausch & Lomb, based on this technology, is able toprovide a pachymetric analysis as well as analysis ofthe anterior chamber depth (Figure 6). However, a
significant limitation in the reliability of the pachy-metric measurements is present with these devices,34
especially in those corneas with their transparencyaffected and therefore with an inherent complicationin the detection of the posterior corneal surface.Anterior chamber depth measurements with theOrbscan system have been shown to be repeatableand in agreement with those obtained with thePentacam system.36
Scheimpflug Photography-Based Systems
These systems allow a comprehensive analysis of theanatomy of the anterior segment, including the fol-lowing analyses: topographic pachymetry (Figure 7),anterior chamber depth, corneal volume, anteriorsegment diameter (angle-to-angle distance), and crys-talline lens densitometry. Several studies have con-firmed and validated the consistency of all thesemeasurements.28,32–37 However, these systems, inspite of obtaining an image of the crystalline lens(Figure 8), do not provide an analysis of the curvatureof the anterior and posterior surfaces of the crystallinelens. This data would be crucial for some calculationsfor optimizing a great variety of refractive surgerytechniques.
Optical Coherence Tomography
Optical coherence tomography is an optical method ofcross-sectional scanning based on reflection and scat-tering of light from the structures within the cornea.Measuring different reflectivity from structures
FIGURE 5. Anterior (left map) and posterior (right map) sagittal curvature maps obtained with the Scheimpflug-photography-basedsystem Pentacam in an eye that had undergone photorefractive keratectomy for the correction of myopia.
Corneal Structure and Anterior SegmentQ1 5
! 2013 Informa Healthcare USA, Inc.
465
466
467
468
469
470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
529
530
531
532
533
534
535
536
537
538
539
540
541
542
543
544
545
546
547
548
549
550
551
552
553
554
555
556
557
558
559
560
561
562
563
564
565
566
567
568
569
570
571
572
573
574
575
576
577
578
579
580

within the cornea by a method of optical interferom-etry produces the cross-section image of the corneaand other anterior segment structures.38 In opticalinterferometry, the light source is split into thereference and measurement beams. The measurementbeam is reflected from ocular structures and interactswith the reference light reflected from the referencemirror, a phenomenon called interference. The coher-ent or positive interference characterized by anincreased resulting signal is measured by the inter-ferometer and, subsequently, the position of thereflecting structure of the eye can be determined.38
In this way, the structures of the anterior segment canbe visualized with a high degree of resolution (cur-rently 18 microns axial and 60 microns transverse)(Figure 9). This allows imaging of fine structures suchas LASIK flaps, Schlemm canal, and lenticles fromlamellar keratoplasty surgery to be easily obtained.
The systems based on this technology have thefollowing two main advantages: the measuring pro-cedure is fast and easy for the examiner and patient,and no corneal touch or specific interphase is neededfor measuring. They provide a more comfortableprocedure of measurement for the patient. All anteriorsegment structures in front of the iris and posteriorsegment structures visible through the pupillary
aperture can be analyzed precisely with this technol-ogy.39 Several applications have been described forthese devices, including analysis of corneal path-ology,40 corneal refractive surgery changes,41 theposition of phakic intraocular lenses42 (Figure 10),the configuration of the iridocorneal angle area, andchanges in the central part of the lens during accom-modation.43 However, AS-OCT has an importantlimitation: it cannot detect structures behind the iris.Therefore, it is not possible to estimate the sulcus-to-sulcus distance or to analyze the areas of the crystal-line lens not visible through the iris. In addition, thedevice cannot analyze any object behind any opaquestructure. It should also be mentioned that this type ofdevice does not provide measurements of the cornealcurvature, only an anatomical analysis of the anteriorsegment.
Very High-Frequency Ultrasonography
Ultrasonic systems allow visualization of anteriorsegment structures, even in the presence of opticalopacities. In general, the resolution and depth ofpenetration are affected by transducer frequency. Thetraditional ultrasonography of the whole eye uses a
FIGURE 6. Anterior segment analysis provided by the scanning-slit system Orbscan II (Bausch & Lomb). The maps represent theanterior corneal elevation (top left), the posterior corneal elevation (top right), the anterior tangential curvature (down left) andpachymetry (down right). Additional anatomical data are listed in the central column of the screen.
6 D. P. Pinero
Seminars in Ophthalmology
581
582
583
584
585
586
587
588
589
590
591
592
593
594
595
596
597
598
599
600
601
602
603
604
605
606
607
608
609
610
611
612
613
614
615
616
617
618
619
620
621
622
623
624
625
626
627
628
629
630
631
632
633
634
635
636
637
638
639
640
641
642
643
644
645
646
647
648
649
650
651
652
653
654
655
656
657
658
659
660
661
662
663
664
665
666
667
668
669
670
671
672
673
674
675
676
677
678
679
680
681
682
683
684
685
686
687
688
689
690
691
692
693
694
695
696

10MHz transducer with approximately 150 mm reso-lution. Higher frequency of a 50MHz transducerincreases the tissue resolution to 50 mm but only at theexpense of decreasing tissue penetration depth of4–5mm, sufficient to image the anterior segment(Figure 11). Scanning of the cornea is possible with a100MHz transducer that increases the tissue reso-lution to less than 20 mm.
Different applications have been described for thisophthalmic technology; these include intraoculartumours analysis,44 determination of the position ofa phakic intraocular lens,45 planning for refractivesurgery retreatment,46 microkeratome cut analysis inLASIK,47 study of intraocular pathology,48 and
FIGURE 7. Comprehensive pachymetric analysis provided by the Scheimpflug-photography-based system Pentacam.
FIGURE 8. Crystalline analysis by Scheimpflug imaging in acase of posterior lenticonus.
FIGURE 9. Image of the anterior segment obtained with the Visante OCT system (Zeiss).
Corneal Structure and Anterior SegmentQ1 7
! 2013 Informa Healthcare USA, Inc.
697
698
699
700
701
702
703
704
705
706
707
708
709
710
711
712
713
714
715
716
717
718
719
720
721
722
723
724
725
726
727
728
729
730
731
732
733
734
735
736
737
738
739
740
741
742
743
744
745
746
747
748
749
750
751
752
753
754
755
756
757
758
759
760
761
762
763
764
765
766
767
768
769
770
771
772
773
774
775
776
777
778
779
780
781
782
783
784
785
786
787
788
789
790
791
792
793
794
795
796
797
798
799
800
801
802
803
804
805
806
807
808
809
810
811
812

analysis of some posterior segment structures.49
As resolution normally improves with frequency,VHF waves are used for most anterior segmentimaging, providing an axial resolution of less than40 mm.50 A main advantage of this technology is itsaccuracy and repeatability.51 The problems arise fromthe measuring procedure. Most ultrasound imagingdevices require physical contact between the corneaand the probe, which can be uncomfortable for somepatients. As example, the Artemis 2 system (ArcScan)ultrasound device does not require cornea–probecontact; rather, an interface eye transducer of salineis used as the acoustic coupling medium between thecornea and probe. However, the position of the headis uncomfortable for patients and the procedurerequires a very experienced examiner. It should alsobe mentioned that this type of device does not providemeasurements of the corneal curvature, only ananatomical analysis of the anterior segment.
CONCLUSIONS
The analysis of the anterior segment is a very usefulprocedure, especially in the field of refractive surgery,allowing a better planning of the surgery, a morecomprehensive follow-up, and a better understandingof some postoperative complications. In summary,there are a few main clinical applications of theanterior segment imaging technology:� Corneal curvature and pachymetric analysis to
evaluate the possibility of performing with safety
keratorefractive surgery with excimer laser in aspecific case.
� Detection of ectatic corneal conditions, especiallyin the most incipient stages, in order to avoid theperformance of laser refractive surgery in suchcases and to analyze and prevent the progressionof this type of corneal disease.
� Accurate planning of enhancements or retreat-ments of corneal refractive surgery procedures.
� Analysis of the anatomical outcomes of thedifferent techniques of corneal transplantation.
� Anatomical study of the anterior segment toperform a precise and accurate planning of theimplantation of phakic intraocular lenses for thecorrection of moderate to high ametropia.
� In-vivo evaluation of the real position of ananterior and even posterior segment phakicintraocular lens and the interaction with theadjacent ocular structures.
� Densitometric analysis of the crystalline lens tocontrol and evaluate its transparency and theneed for cataract surgery.
� Precise control and monitoring of corneal andanterior segment pathological conditions.
� Analysis of the iridocorneal angle configuration inglaucoma patients.
There is a great variety of technologies availableallowing the clinician to perform a characterization ofdifferent anterior segment structures. Each technologyhas different features and is useful for a specific taskin the analysis of the anterior segment and cornea.From the Placido-based systems that allow only acharacterization of the geometry of the anteriorcorneal surface to the Scheimpflug photography-based systems that provide a characterization of thecornea, anterior chamber, and crystalline lens, there isa variety of devices with the capability of analyzingdifferent anatomical parameters with very high pre-cision. It is important to know the capabilities andlimitations of each technology for performing anoptimized use of it. Scheimpflug photography-basedsystems are to date the devices providing the morecomplete analysis of the anterior segment in a non-invasive way, allowing the characterization of the
FIGURE 10. Visualization of the position of a posterior chamberpIOL (Phakic Refractive Lens, PRL, Zeiss) to the anteriorsurface of the crystalline lens by means of spectral-domainAS-OCT.
FIGURE 11. Analysis of the cornea by means of a very high-frequency ultrasonographer with a transducer of 50MHz.
8 D. P. Pinero
Seminars in Ophthalmology
813
814
815
816
817
818
819
820
821
822
823
824
825
826
827
828
829
830
831
832
833
834
835
836
837
838
839
840
841
842
843
844
845
846
847
848
849
850
851
852
853
854
855
856
857
858
859
860
861
862
863
864
865
866
867
868
869
870
871
872
873
874
875
876
877
878
879
880
881
882
883
884
885
886
887
888
889
890
891
892
893
894
895
896
897
898
899
900
901
902
903
904
905
906
907
908
909
910
911
912
913
914
915
916
917
918
919
920
921
922
923
924
925
926
927
928
geometry of anterior and posterior corneal surfaces,the anterior chamber depth and pachymetric distri-bution, and the densitometry and thickness of thecrystalline lens. However, there is no system provid-ing a characterization of the geometry of the twocorneal surfaces of the crystalline lens. More devel-opments are required in anterior segment imagingtechnologies in order to improve the analysis of thecrystalline lens structure as well as the ocular struc-tures behind the iris when the pupil is not dilated.
DECLARATION OF INTEREST
The authors report no conflicts of interest. The authorsalone are responsible for the content and writing ofthe paper.Q2
REFERENCES
1. Reinstein DZ, Gobbe M, Archer TJ. Anterior segmentbiometry: A study and review of resolution and repeat-ability data. J Refract Surg 2012;28(7):509–520.
2. Mireskandari K, Tehrani NN, Vandenhoven C, Ali A.Anterior segment imaging in pediatric ophthalmology.J Cataract Refract Surg 2011;37(12):2201–2210.
3. Hahn P, Migacz J, O’Connell R, et al. The use ofoptical coherence tomography in intraoperative ophthal-mic imaging. Ophthalmic Surg Lasers Imaging 2011;42(Suppl):S85–S94.
4. Wang J, Abou Shousha M, Perez VL, et al. Ultra-highresolution optical coherence tomography for imaging theanterior segment of the eye. Ophthalmic Surg Lasers Imaging2011;42(Suppl):S15–S27.
5. Dada T, Gadia R, Sharma A, et al. Ultrasound biomicro-scopy in glaucoma. Surv Ophthalmol 2011;56(5):433–450.
6. Bianciotto C, Shields CL, Guzman JM, et al. Assessment ofanterior segment tumors with ultrasound biomicroscopyversus anterior segment optical coherence tomography in200 cases. Ophthalmology 2011;118(7):1297–1302.
7. Oliveira CM, Ribeiro C, Franco S. Corneal imagingwith slit-scanning and Scheimpflug imaging techniques.Clin Exp Optom 2011;94(1):33–42.
8. Kiernan DF, Mieler WF, Hariprasad SM. Spectral-domainoptical coherence tomography: A comparison of modernhigh-resolution retinal imaging systems. Am J Ophthalmol2010;149(1):18–31.
9. Jancevski M, Foster CS. Anterior segment optical coher-ence tomography. Semin Ophthalmol 2010;25(5–6):317–323.
10. Salomao MQ, Esposito A, Dupps Jr WJ. Advances inanterior segment imaging and analysis. Curr OpinOphthalmol 2009;20(4):324–332.
11. Dorairaj S, Liebmann JM, Ritch R. Quantitative evaluationof anterior segment parameters in the era of imaging. TransAm Ophthalmol Soc 2007;105:99–108; discussion 108–10.
12. Arnalich F, Pinero D, Alio JL. Fundamentals in cornealtopography. In: Mastering the Techniques of LASIK,EPILASIK and LASEK (Techniques and Technologies) (GargA, Alio JL, Pajic B, Mehta CK, Eds.); New Delhi: JaypeeBrothers Medical Publishers Ltd., 2007.
13. Rand R, Howland H, Applegate R. Mathematical model ofa Placido disk keratometer and its implications for recov-ery of corneal topography. Optom Vis Sci 1997;74:926–930.
14. Applegate R. Comment: Inherent error in corneal topog-raphy/Roberts. J Refract Corneal Surg 1994;10:113–114.
15. Maldonado MJ, Nieto JC, Diez-Cuenca M, Pinero DP.Repeatability and reproducibility of posterior cornealcurvature measurements by combined scanning-slit andplacido-disc topography after LASIK. Ophthalmology 2006;113:1918–1926.
16. Cheng AC, Rao SK, Lam DS. Accuracy of Orbscan II in theassessment of posterior curvature in patients with myopicLASIK. J Refract Surg 2007;23:677–680.
17. Ueda T, Nawa Y, Masuda K, et al. Posterior corneal surfacechanges after hyperopic laser in situ keratomileusis.J Cataract Refract Surg 2005;31:2084–2087.
18. Nawa Y, Masuda K, Ueda T, et al. Evaluation of apparentectasia of the posterior surface of the cornea afterkeratorefractive surgery. J Cataract Refract Surg 2005;31:571–573.
19. Grzybowski DM, Roberts CJ, Mahmoud AM, Chang Jr JS.Model for nonectatic increase in posterior corneal elevationafter ablative procedures. J Cataract Refract Surg 2005;31:72–81.
20. Nilforoushan MR, Speaker M, Marmor M, et al.Comparative evaluation of refractive surgery candidateswith Placido topography, Orbscan II, Pentacam, andwavefront analysis. J Cataract Refract Surg 2008;34:623–631.
21. Nishimura R, Negishi K, Saiki M, et al. No forward shiftingof posterior corneal surface in eyes undergoing LASIK.Ophthalmology 2007;114:1104–1110.
22. Chakrabarti HS, Craig JP, Brahma A, et al. Comparison ofcorneal thickness measurements using ultrasound andOrbscan slit-scanning topography in normal and post-LASIK eyes. J Cataract Refract Surg 2001;27:1823–1828.
23. Iskander NG, Anderson Penno E, Peters NT, et al.Accuracy of Orbscan pachymetry measurements andDHG ultrasound pachymetry in primary laser in situkeratomileusis and LASIK enhancement procedures.J Cataract Refract Surg 2001;27:681–685.
24. Giessler S, Duncker GI. Orbscan pachymetry after LASIK isnot reliable. J Refract Surg 2001;17:385–387.
25. Prisant O, Calderon N, Chastang P, et al. Reliability ofpachymetric measurements using orbscan after excimerrefractive surgery. Ophthalmology 2003;110:511–515.
26. Swartz T, Marten L, Wang M. Measuring the cornea: thelatest developments in corneal topography. Curr OpinOphthalmol 2007;18:325–333.
27. Kawamorita T, Uozato H, Kamiya K, et al. Repeatability,reproducibility, and agreement characteristics of rotatingScheimpflug photography and scanning slit corneal top-ography for corneal power measurement. J Cataract RefractSurg 2009;35:127–133.
28. Montalban R, Pinero DP, Javaloy J, Alio JL. Intrasubjectrepeatability of corneal morphology measurementsobtained with a new Scheimpflug photography-basedsystem. J Cataract Refract Surg 2012;38:971–977.
29. Savini G, Barboni P, Carbonelli M, Hoffer KJ. Accuracy ofcorneal power measurements by a new Scheimpflugcamera combined with Placido-disk corneal topographyfor intraocular lens power calculation in unoperated eyes.J Cataract Refract Surg 2012;38:787–792.
30. Bedei A, Appolloni I, Madesani A, et al. Repeatability andagreement of 2 Scheimpflug analyzers in measuring thecentral corneal thickness and anterior chamber angle,volume, and depth. Eur J Ophthalmol 2012;22(Suppl7):S29–S32.
31. Nasser CK, Singer R, Barkana Y, et al. Repeatability of theSirius imaging system and agreement with the PentacamHR. J Refract Surg 2012;28:493–497.
32. Savini G, Carbonelli M, Barboni P, Hoffer KJ. Repeatabilityof automatic measurements performed by a dual
Corneal Structure and Anterior SegmentQ1 9
! 2013 Informa Healthcare USA, Inc.
929
930
931
932
933
934
935
936
937
938
939
940
941
942
943
944
945
946
947
948
949
950
951
952
953
954
955
956
957
958
959
960
961
962
963
964
965
966
967
968
969
970
971
972
973
974
975
976
977
978
979
980
981
982
983
984
985
986
987
988
989
990
991
992
993
994
995
996
997
998
999
1000
1001
1002
1003
1004
1005
1006
1007
1008
1009
1010
1011
1012
1013
1014
1015
1016
1017
1018
1019
1020
1021
1022
1023
1024
1025
1026
1027
1028
1029
1030
1031
1032
1033
1034
1035
1036
1037
1038
1039
1040
1041
1042
1043
1044
Scheimpflug analyzer in unoperated and post-refractivesurgery eyes. J Cataract Refract Surg 2011;37:302–309.
33. Salouti R, Nowroozzadeh MH, Zamani M, et al.Comparison of anterior and posterior elevation mapmeasurements between 2 Scheimpflug imaging systems.J Cataract Refract Surg 2009;35:856–862.
34. Gonzalez-Meijome JM, Cervino A, Yebra-Pimentel E,Parafita MA. Central and peripheral corneal thicknessmeasurement with Orbscan II and topographicalultrasound pachymetry. J Cataract Refract Surg 2003;29:125–132.
35. Boscia F, La Tegola MG, Alessio G, Sborgia C. Accuracy ofOrbscan optical pachymetry in corneas with haze.J Cataract Refract Surg 2002;28:253–258.
36. Lackner B, Schmidinger G, Skorpik C. Validity andrepeatability of anterior chamber depth measurementswith Pentacam and Orbscan. Optom Vis Sci 2005;82:858–861.
37. Milla M, Pinero DP, Amparo F, Alio JL. Pachymetricmeasurements with a new Scheimpflug photography-based system: Intraobserver repeatability and agreementwith optical coherence tomography pachymetry. J CataractRefract Surg 2011;37:310–316.
38. Radhakrishnan S, Rollins AM, Roth JE, et al. Real-timeoptical coherence tomography of the anterior segment at1310 nm. Arch Ophthalmol 2001;119:1179–1185.
39. Muller M, Dahmen G, Porksen E, et al. Anterior chamberangle measurement with optical coherence tomography:Intraobserver and interobserver variability. J CataractRefract Surg 2006;32:1803–1808.
40. Aslanides IM, Reinstein DZ, Silverman RH, et al. High-frequency ultrasound spectral parameter imaging of anter-ior corneal scars. CLAO J 1995;21:268–272.
41. Avila M, Li Y, Song JC, Huang D. High-speedoptical coherence tomography for management after laserin situ keratomileusis. J Cataract Refract Surg 2006;32:1836–1842.
42. Baikoff G, Lutun E, Wei J, Ferraz C. Contact between3 phakic intraocular lens models and the crystalline
lens: an anterior chamber optical coherence tomographystudy. J Cataract Refract Surg 2004;30:2007–2012.
43. Baikoff G, Lutun E, Ferraz C, Wei J. Static and dynamicanalysis of the anterior segment with optical coherencetomography. J Cataract Refract Surg 2004;30:1843–1850.
44. Char DH, Kundert G, Bove R, Crawford JB. 20MHz highfrequency ultrasound assessment of scleral and intraocularconjunctival squamous cell carcinoma. Br J Ophthalmol2002;86:632–635.
45. Garcıa-Feijoo J, Hernandez-Matamoros JL, Castillo-GomezA, et al. High-frequency ultrasound biomicroscopy ofsilicone posterior chamber phakic intraocular lens forhyperopia. J Cataract Refract Surg 2003;29:1940–1946.
46. Reinstein DZ, Couch DG, Archer T. Direct residual stromalthickness measurement for assessing suitability for LASIKenhancement by Artemis 3D very high-frequency digitalultrasound arc scanning. J Cataract Refract Surg 2006;32:1884–1888.
47. Reinstein DZ, Silverman RH, Sutton HFS, Coleman DJ.Very high-frequency ultrasound corneal analysis identifiesanatomic correlates of optical complications of lamellarrefractive surgery: Anatomic diagnosis in lamellar surgery.Ophthalmology 1999;106:474–482.
48. Silverman RH, Rondeau MJ, Lizzi FL, Coleman DJ. Three-dimensional high-frequency ultrasonic parameter imagingof anterior segment pathology. Ophthalmology 1995;102:837–843.
49. Coleman DJ, Silverman RH, Chabi A, et al. High-resolutionultrasonic imaging of the posterior segment. Ophthalmology2004;111:1344–1351.
50. Reinstein DZ, Archer TJ, Silverman RH, Coleman DJ.Accuracy, repeatability, and reproducibility of Artemisvery high-frequency digital ultrasound arc-scan lateraldimension measurements. J Cataract Refract Surg 2006;32:1799–1802.
51. Pinero DP, Plaza AB, Alio JL. Anterior segment biometrywith 2 imaging technologies: Very-high-frequency ultra-sound scanning versus optical coherence tomography.J Cataract Refract Surg 2008;34:95–102.
10 D. P. Pinero
Seminars in Ophthalmology
1045
1046
1047
1048
1049
1050
1051
1052
1053
1054
1055
1056
1057
1058
1059
1060
1061
1062
1063
1064
1065
1066
1067
1068
1069
1070
1071
1072
1073
1074
1075
1076
1077
1078
1079
1080
1081
1082
1083
1084
1085
1086
1087
1088
1089
1090
1091
1092
1093
1094
1095
1096
1097
1098
1099
1100
1101
1102
1103
1104
1105
1106
1107
1108
1109
1110
1111
1112
1113
1114
1115
1116
1117
1118
1119
1120
1121
1122
1123
1124
1125
1126
1127
1128
1129
1130
1131
1132
1133
1134
1135
1136
1137
1138
1139
1140
1141
1142
1143
1144
1145
1146
1147
1148
1149
1150
1151
1152
1153
1154
1155
1156
1157
1158
1159
1160