technical considerations in the surgical treatment of colon and rectal cancer
TRANSCRIPT

Seminars in Surgical Oncology 10:200-207 (1994)
Technical Considerations in the Surgical Treatment of Colon and Rectal Cancer
__-
S C O T A. FENGLER, MD. AND RUSSELL K. PEARL, MD
From the Division of Colon and Rectal Surgery, Cook County Hospital (S.A.F., R.K.P.) and Department of Clinical Surgery, University of lllinois College of Medicine (R.K.P.),
Chicago, lllinois
Surgery is the primary mode of therapy for colorectal cancer. Ad- vances beyond exteriorization began to appear at the end of the nine- teenth century. The antibiotic era brought on more advances. Dogma abounds with respect to the technical aspects of surgery for colon and rectal cancer and few randomized, prospective trials have been done to evaluate the importance of these techniques. Firmly established are the techniques of resection of lymphatic drainage of tumors, en bloc resec- tion of invaded structures, and obtaining at least 2 cm margins of rectal cancers. Radical lymph node dissection, luminal ligation, oophorec- tomy, and the “No-Touch Technique” are discussed. Despite the paucity of irrefutable scientific data to support many of the described surgical techniques, differences in outcome between surgeons suggest that technique is important. There is great need for randomized, pro- spective trials to evaluate the multitude of techniques described for the surgical treatment of COlOreCtal cancer. Q 1994 Wiley-Liss. Inc.
KEY WORDS: colorectal carcinoma, recurrence, surgery, technique
HISTORY Before the beginning of this century the history of
surgical treatment of cancer of colon and rectum was essentially the treatment of cancer of the rectum. In the preanesthetic era, Jacques Lisfranc of Paris was the first to perform a planned operation for rectal cancer. This was first performed in 1826, and several years later, of nine patients reported, six survived and were reportedly continent. The rectum was excised perineally, an approach that dominated surgery for the remainder of the nineteenth century. In 1896, H.W. Allingham of St. Mark’s Hospital described the procedure in detail [l]. Only mobile tumors located posteriorly in the rectum were judged suitable for re- section. A circular incision was made at the anal verge and extended posteriorly to the tip of the coccyx. An intraluminal incision was then made circularly in the rectum proximal to the tumor, about 10 to 12 cm from the anal verge. Circular mobilization outside the rectal wall then enabled the surgeon to excise the rectal tumor. Ligation of blood vessels was not described, and the wound was packed open. No further down-
ward mobilization of the proximal rectum was per- formed, and the wound was allowed to granulate. A surprising number of these patients survived (mortal- ity in most series was less than 20%), and many sur- geons also stated that their patients maintained fecal continence. Allingham said this operation took him about 10 min to perform. Many modifications of this procedure were described throughout the nineteenth century, the most enduring being the posterior ap- proach described by Kraske [2].
Although many patients survived the perineal ap- proach for excision for rectal cancer, the vast majority ultimately died from recurrent cancer. This motivated Miles [3] to study the patterns of spread of rectal can- cer. The data he gathered were obtained by noting the position of metastases during the performance of an operation, by pathologic examination of operative specimens. by observing the site of recurrence after operative treatment, and by studying the autopsy find-
Address reprint requests to Scott A . Fengler, MD, Division o f Colon and Rectal Surgery, Cook County Hospital, 1835 W. Harri- son, Chicago, IL 60612.
0 1994 Wiley-Liss, Inc.
Surgical Technique for Colorectal Cancer 201
ings of patients dying of advanced and inoperable carcinomas of the rectum. Miles concluded that cancer of the rectum spread predominantly through the lym- phatics draining the rectum and that this spread would occur in three directions. The first was the zone of upward spread. This comprises lymphatics and nodes lying along the superior hemorrhoidal vessels that lie in the mesorectum and the base of the mesentery of the sigmoid. The second is the zone of lateral spread. This consisted of the lymphatics running in the lateral liga- ments between the pelvic peritoneum and the levator muscle, Ultimately ending in the internal iliac nodes in the pelvic side wall. The third is the zone of downward spread. This included the lymphatics traversing the sphincter muscle, the perianal skin, and ischiorectal fat, ultimately draining into the inguinal nodes . Based on these observations he advocated extensive removal of the entire rectum and related structures by a com- bined abdominoperineal approach as the best treat- ment for all cases of rectal cancer, including proximal rectal cancer.
The superior hemorrhoidal artery was ligated at the junction of the left colic artery and the entire mesorec- tum removed. This operation was first described in 1908 before either intravenous fluids or banked blood were available. Not surprisingly, operative mortality was very high, in excess of 50%, but in patients that survived the operation, prolonged survival from rectal cancer was the rule. In the same year, Moynihan [4] described more proximal ligation of the inferior mes- enteric artery made at its junction with the aorta to resect the greatest number of lymph nodes en bloc with the tumor in the rectum.
Subsequent study of the modes of spread of rectal cancer in operative specimens in the 1930s confirmed Miles’ observation that upward spread was a frequent mode of dissemination. However, evidence of lateral or downward spread could not be demonstrated [2]. Nev- ertheless, Miles’ contribution remains the most signifi- cant advance in the treatment of colorectal cancer.
PLANNING THE OPERATION Planning the surgical approach to colon and rectal
cancer is important as patient education and counsel- ing, positioning on the operating room table, and po- tential use of neoadjuvant therapy all depend on it. Unfortunately, pretherapeutic staging, one of the keys to selecting the appropriate surgical approach in colon and rectal cancer, is inaccurate. Some success has been achieved in pretherapeutic staging in rectal cancer with endorectal ultrasound. Endorectal ultrasound does have limitations however in distinguishing be- tween benign and malignant lymph nodes [5,6]. Fur- ther research and refinement of pretherapeutic staging
of rectal cancer would be of great benefit as the surgi- cal options vary from the minimally invasive (local excision, fulguration, or radiotherapy) to radical and irreversible (proctectomy and permanent colostomy).
Pretherapeutic staging of colon cancer is limited by the intraabdominal location of the colon and by lack of accurate modalities in staging. The value of pre- therapeutic staging of colon cancer is also felt to be somewhat less critical in that many patients benefit from palliative resections.
LIMITS OF EXCISION The extent of resection of colorectal cancer is best
defined by the combination of our knowledge of the biology of colorectal cancer and properly controlled clinical studies that demonstrate the effectiveness of a procedure in preventing recurrent cancer. Although much is known about the biology of colorectal cancer, almost every study related to surgical technique has been poorly constructed, comparing patients selected nonrandomly either to no controls at all or historical controls, thus making the results of these studies im- possible to interpret.
In spite of this deficiency, little controversy exists about the extent of resection for carcinomas of the cecum, hepatic flexure, transverse colon, splenic flex- ure, or descending colon. The extent of resection and level of vascular ligation are described in Table I. Some surgeons feel, however, that less radical resections are warranted for their lower morbidity and mortality [7]. The remainder of this section concentrates on lesions about which the most difficult decisions must be made regarding the extent of resection and about which the greatest controversies exist-carcinomas of the recto- sigmoid and rectum. In planning a resection for tumors at this level, decisions must be made about the following factors: the distal margin, the proximal margin, the lateral margin, whether to resect to distal mesorectum, what to do about adherent, adjacent organs, and whether to perform an oophorectomy.
DISTAL MARGIN The distal margin of resection is determined by
three factors: (1) the likelihood of downward lym- phatic spread, (2) intramural spread of the carcinoma, and ( 3 ) the adequacy of the blood supply to the distal colon for anastomosis after appropriate vascular liga- tion. To ensure resection of all metastatic disease in distal or downward lymphatic channels and nodes, Miles performed an abdominoperineal resection of the rectum and anus for carcinomas located as high as 10 to 20 cm from the dentate line. Yet investigators in the 1930s demonstrated that both downward and lateral spread were unlikely in surgically curable cancers of

202 Fengler and Pearl
TABLE I. Radical Resection for Colorectal Cancer
Location of tumor
Cecum Ileocolic, right colic Right hemicolectomy Ileotransverse colostomy Ascending colon Ileocolic. right colic Right hemicolectomy Ileotransverse colostomy Hepatic flexure Ileocolic. right colic, middle Extended right hemicolectomy Ileodescending colostomy
Transverse colon Ileo-, right. middle, and Subtotal colectomy Ileosigmoidostomy
Splenic flexure Ileo-, right, middle, and Subtotal colectomy Ileosigmoidostomy
Descending colon Inferior mesenteric Left hemicolectomy Transverse coloproctostomy Sigmoid colon Inferior mesenteric Left hemicolectomy Transverse coloproctostomy Rectosigmoid, upper rectum Inferior mesenteric Rectosigmoidectomy Descending coloproctostomy Lower rectum Inferior mesenteric, (superior Restorative proctectomy Coloanal anastomosis (or
Anal canal Superior rectal Proctectomy (or nonsurgical None
Extent of resection Anastomosis -~ ~ _______ Level of vascular ligation _ _ _ ~ -__
colic
ascending left colic
ascending left colic
rectal) colostomy)
therapy)
the rectum [2]. From that work came the justification for low anterior resection for carcinomas of the upper rectum and distal sigmoid.
DISTAL MESORECTUM Numerous studies have demonstrated the safety of
low anterior resection, with 5-year survival rates that usually exceed those for carcinomas of the distal rec- tum requiring abdominoperineal resection [8]. Yet there is the curious anomaly of patients that have low anterior resection having a higher tumor recurrence rate in the pelvis than patients having ab- dominoperineal resection, despite their improved sur- vival, a finding that has been supported in a number of series. One possible explanation for this can be seen in the work of Heald and co-workers [9,10] regarding the importance of the distal mesorectum in rectal cancer surgery. They have demonstrated that lymph nodes a short distance distal to the primary tumor may con- tain metastatic deposits (Fig. I ) . In the performance of an anterior resection, the angularity of the incision in the mesorectum is such that the lymph nodes are often left in situ. By carefully resecting the entire distal mes- orectum down to the levator diaphragm, Heald and his colleagues have lowered the local tumor recurrence rate in the pelvis to 3.2%, the lowest figure ever re- ported in a series of this size. If this finding is sup- ported by other investigators, then localized down- ward lymphatic spread as originally proposed by Miles may in fact be of some importance in the biol- ogy of colorectal cancer. Another potential anatomic explanation is that the nodes described by Heald may in fact have been the epicolic nodes draining the por- tion of the rectum containing the tumor. The angle of the rectum in the pelvis is such that during an anterior resection the epicolic nodes would normally be left in situ, although these are the lymph nodes most likely to
contain metastatic disease. If the distal mesorectum is resected in all rectal and distal sigmoid carcinomas, the blood supply to the distal margin of resection will arise only through the wall of the rectum above the levators. In that instance the amount of rectum that can be left above the levators is severely limited by the adequacy of its blood supply, and therefore no more than 3 to 4 cm of rectum above the levators could be safely used for anastomosis. In this way the location of the distal margin of resection is determined by the adequacy of the blood supply to that margin.
INTRAMURAL SPREAD Traditionally the margin distal to the primary
tumor has been determined by the likelihood of the intramural spread of the tumor. Grinnell [l I ] reported that although intramural spread of colorectal cancer may happen through submucosal lymphatics or peri- rectal fat, submucosal spread rarely exceeds 4 cm, even in the most unfavorable cases [ I 11. Therefore he rec- ommended a margin of at least 5 cm of grossly normal bowel during resection for colorectal cancer. More recent studies suggest that in well-differentiated le- sions a distal margin of 2 cm may be quite adequate because 98% of such lesions spread less than 2 cm. This rather small difference of 3 cm is of critical impor- tance for carcinomas located in the mid rectum. In patients with tumors at this level, this difference often determines the choice of anterior resection or ab- dominoperineal resection with permanent colostomy.
Although the resection of the rectum to be 2 cm distal to the tumor has been demonstrated safe in clinical studies, as measured both by local tumor re- currence and 5-year survival, its success in the hands of the average practitioner depends on two things. First, the adequacy and accuracy of preoperative bi- opsy are essential. Histologic features frequently vary

Surgical Technique for Colorectal Cancer 203
Fig. 1. Epicolic lymph nodes in the posterior mesorectum may be left in the pelvis in a low anterior resection if overcompensation is not made for the curve of the pelvis and if the whole mesorectum is not resected en bloc with the tumor-bearing rectosigmoid. (From Nelson RL: Prob Gen Surg 4:93, 1987, [36] with permission of J.B. Lippincott Co.)
within a single tumor, and multiple preoperative biop- sies are required. Second, accurately locating the distal margin of the tumor in a small pelvis is difficult during operation. Frequently, when a resected specimen is opened, a margin that was thought to be 5 cm is actually somewhat less. An unacceptable surgical error would be to aim for a point 2 cm distal to the primary tumor and find upon opening the resected specimen that the distal margin of resection includes tumor-bearing tissue on gross visual inspection. Sub- mucosal injection of a small volume of methylene blue through a proctoscope at the distal margin of the tumor may be helpful, although this is generally used for soft, difficult to feel villous adenomas located more proximally in the rectum, since direct viewing of the injection site is difficult deep in the pelvis [12].
PROXIMAL MARGIN The proximal margin of resection is determined by
the level of vascular ligation. In discussing cancers of
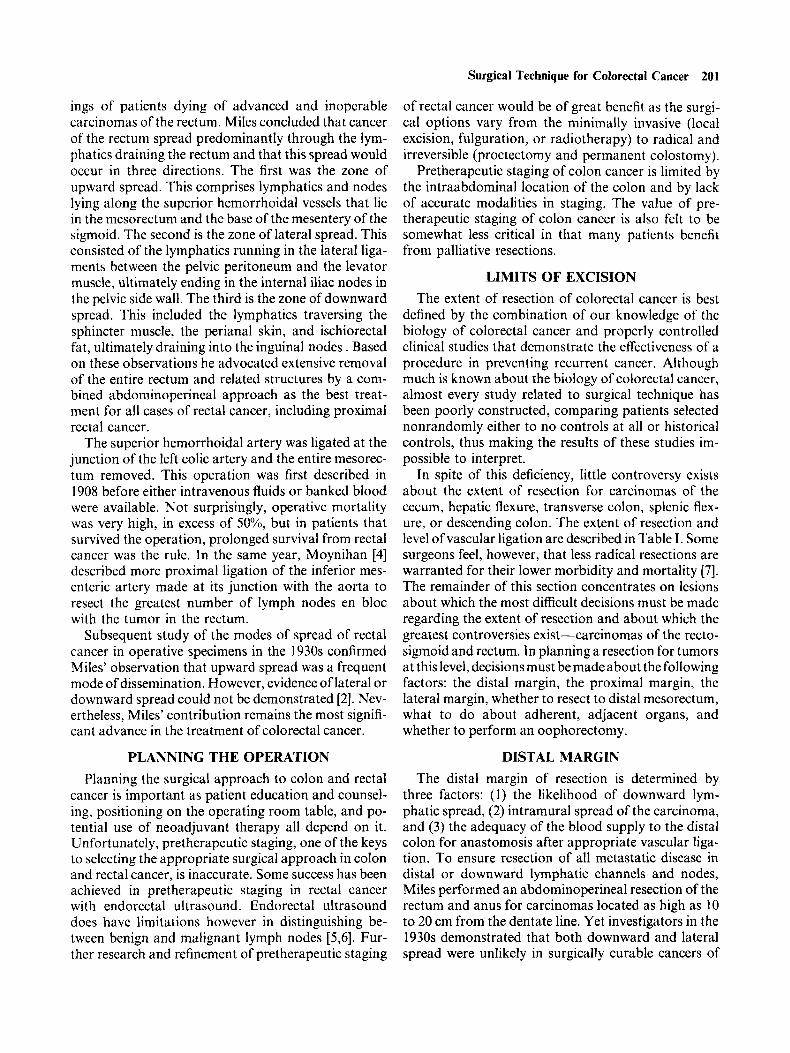
the mid- or upper rectum, once again, to do the most extended form of left hemicolectomy, the inferior mes- enteric artery must be ligated flush with the aorta and the inferior mesenteric vein must be ligated at the lateral duodenojejunal fossa; this obtains the greatest number of lymph nodes en bloc with the resected spec- imen. This also allows for complete mobilization of the left half of the colon to accomplish a tension-free colorectal or coloanal anastomosis [ 131. In addition. it is how a “no-touch’’ resection of the left colon is initi- ated [14] (Figs. 2 and 3).
Patients with an apical lymph node that contains metastatic cancer have a poor prognosis. Grinnell [ 131 reported a small series of patients having high liga- tions of the inferior mesenteric artery in whom proxi- mal lymph node metastasis were found in 10.6%. None of this latter group of patients survived 5 years. In a review of 1,370 patients from S t . Mark’s Hospital in London, ligation of the inferior mesenteric artery at its origin from the aorta was compared with ligation distal to the origin of the left colic artery. In this report survival advantage was demonstrated with a higher level of arterial ligation (Fig. 3). All Dukes’ classifica- tions of colorectal cancer showed equivalent survival rates except for individuals whose highest lymph node contained metastatic cancer (C2 lesions in their modi- fication of the Dukes system). Patients with C2 lesions having the higher ligation had a worse prognosis (pre- sumably because more nodes were positive). The study was not done prospectively. Instead its design de- pended on the surgical practice of different consultant surgeons at St. Mark’s Hospital, who habitually li- gated the inferior mesenteric artery either flush with the aorta or distal to the left colic artery [ 151. There should be no biologic advantage to separate higher venous ligation, as the predominant pattern of lym- phatic spread is along the arterial supply. As men- tioned above, the higher venous ligation increases the mobility of the left colon for tension-free anastomoses and also facilitates the “no-touch technique.” There- fore it would seem that patients with lesions of the middle and upper rectum may have preservation of the left colic artery and the descending colon without alteration in prognosis.
LATERAL MARGIN In 1979, Enker and associates [16] reported 260 pa-
tients, a few of whom had extended lateral pelvic wall lymph node resections en bloc with their primary rec- tosigmoid cancers. Although Enker et al. stated that the improved survival in these patients was caused by the extended lymph node dissection in the pelvic wall, no criteria for selection of those patients were men- tioned nor was any group of patients presented to
204 Fengler and Pearl
Fig. 2. Technique of high vascular ligation before mobilization of the left colon (“No-Touch Technique”). An incision is made in the lateral duodenal-jejunal fossa exposing and dividing the inferior mesenteric vein. A finger swept medially in this incision beneath the duodenum will hook the inferior mesenteric artery as i t leaves the aorta. well away from the ureter. (From Abcarian H, Pearl RK: Dis Colon Rectum, 34:l 138. 1991 [14], with permission of Williams and Wilkins.)
whom they could have been compared. The lateral pelvic wall lymph node dissection had been reported 20 years earlier by Stearns and Deddish [17]. They found that the extended resection not only did not improve 5-year survival when compared retrospec- tively with standard low anterior or abdominoperineal resections, but also there was a large increase in trans- fusion requirements intraoperatively and a 67% inci- dence of operative genitourinary complications post- operatively. It was Stearns and Deddish’s recommendation at that time, as well as Goligher’s [2] and more recently the St. Mark’s group, that this pro- cedure be abandoned [ 181.
On the other hand, Quirke and colleagues examined whole-mount sections of entire operative specimens by transverse slicing of resected rectal cancers from 52 patients. They found tumor spread to the lateral mar- gins in 14 patients (27%), and 12 of these developed local recurrence. They concluded that lateral spread
and inadequate surgical excision are direct causes of pelvic recurrence [ 191.
Hojo and associates [20] reviewed results of 437 nonrandomized patients undergoing curative resec- tion of rectal carcinoma (262 Miles operations and 175 sphincter-saving procedures). One hundred and ninety-two patients had extended ileopelvic lym- phadenectomy, and 245 had conventional lym- phadenectomy. The extended resection took 30 min longer to perform and was associated with 400 ml greater blood loss. However, operative mortality was not significantly different. The 5-year survival of pa- tients with extended versus conventional lym- phadenectomy was 88% versus 74% in Dukes’ B and 61% versus 41% in Dukes’ C lesions (P < 0.05). Local recurrence rates for extended versus conventional re- sections were 0% versus 5.20/0 for Dukes’ A, 6.20/0 ver- sus 21.8‘1/0 for Dukes’ B, and 23.6% versus 32.9% for Dukes’ C lesions (P < 0.05). This procedure was as-

Surgical Technique for Colorectal Cancer 205
Fig. 3 Should the inferior mesenteric artery (IMA) be ligated at its origin or below the takeoff of the left colic artery (LCA)? Al- though more lymph nodes are removed with higher ligation, retro- spective studies have not demonstrated improved survival using this technique (see Pezim [15]). This is one of many facts of colon cancer surgery that has never been subjected to a study. the design of which might adequately provide an answer for this question. SRA, superior rectal artery. (From Nelson RL: Prob Gen Surg 4:97, 1987 [36]. with permission of J.B. Lippincott, Co.)
sociated with a high risk of genitourinary complica- tions. Loss of bladder-fullness sensation was seen in 39.4% of the extended resection group versus 8.8% of the conventional excision group, and the incidence of sexual impotence also was twice as high (76% versus 37.5%).
ADHERENT ADJACENT STRUCTURES Resection of contiguous organs adherent to colo-
rectal cancer is imperative if local control and curative resection are to be accomplished. Separation of adher- ent organs and division of benign-looking adhesions is to be condemned. Also, local invasion to adjacent organs does not necessarily mean a dismal prognosis [21]. Additional reports have demonstrated that by using multiple organ resections, an almost 10% in- crease in resectability and 6% higher cure rates may be achieved with very little increase in morbidity [22,23]. In a review of 52 patients reoperated for so-called “unresectable” colorectal cancers, Neuman and Stearns [24] found that resection for cure was possible
in 32 patients and palliative resection in 8 others, and the 5-year survival in these patients was 36%.
OOPHORECTOMY It is free dissemination of tumor cells within the
peritoneal cavity that causes ovarian metastases. The ovaries have been found to be a particularly fertile site of implantation of tumor cells. The incidence of occult metastatic colorectal carcinoma in ovaries of all women receiving surgery for colorectal cancer has been reported to be 70/0 with the highest incidence in Dukes’ C lesions. Barr and co-workers [25] reported 17 patients who had presumably curative resections. They found metastatic disease to the ovaries in eight patients. Ovarian metastases were found in 7.4% of the patients reported by McKeigan and Ferguson [26]. However, in this study the incidence of ovarian metas- tases in premenopausal women was alarmingly high (25%). Based on these data the Ferguson group con- cluded that the high incidence of ovarian metastases (and the higher cure rates among women with micro- scopic metastases found at prophylactic oophorec- tomy) warrants oophorectomy in all women with colorectal cancer regardless of their age. Oophorec- tomy has the additional advantage of providing pro- phylaxis against primary ovarian carcinoma for that 4% to 6% of women in whom this disease ultimately develops.
Yet, in general, few 5-year survivors have been re- ported among patients with metastases in the ovary: that is, the procedure when performed may have been superfluous. However, another favorable report is that of Morrow and Enker [27], who reported 63 pa- tients in whom ovarian metastases appeared after the primary colonic resection. When it was technically fea- sible to resect all gross disease in the pelvis, the mean survival time in this group was 48 months with two 5-year survivors. In patients in whom the disease could not be resected, the mean survival time was only 9.6 months. This study implies that staged resection of clinically apparent ovarian metastases is feasible and may provide at least as good an opportunity as simul- taneous oophorectomy to lengthen survival time and possibly to obtain a cure.
“NO-TOUCH TECHNIQUE” Several operative techniques have been developed
to prevent the intraoperative spread of colorectal can- cer. First of these is the “no-touch technique” first reported by J. Peyton Barnes [28] in 1952. He de- scribed division of the ileum and transverse colon with an anastomosis before mobilization of a cecal carci- noma. Cole and colleagues [29,30] demonstrated via- ble tumor cells in the peripheral venous blood of pa-

206 Fengler and Pearl
tients having intraoperative manipulation of their colorectal cancer. They recommended therefore that the arterial and venous supply to the tumor be ligated before tumor mobilization. However, subsequent studies by other investigators could not confirm that the incidence of malignant cells was increased in the peripheral circulation during operative manipulation of the tumor, nor could follow-up studies of patients at the University of Illinois correlate ultimate survival with the incidence of malignant cells being detected in the peripheral circulation [3 11.
The first clinical series of patients using the “no- touch technique” was reported by Turnbull et al. [32]. That study was marred, however, by the additional variable of a much different extent of resection in his patients when compared with the historical control population being treated by his colleagues at the Cleveland Clinic [32]. Wiggers and co-workers [33] reported the first study of surgical technique in colo- rectal cancer with true randomization of patients to the treatment arms, which were “no-touch technique” versus conventional resection. They studied 236 pa- tients with curative resections and presented 5-year follow-up. The time to appearance of liver metastases was less and the number of liver metastases was more in the conventional arm, although a significant differ- ence in 5-year survival was not achieved in this study population (3 1.1% disease-related deaths in the con- ventional arm, 24.7% disease-related deaths with the no-touch technique) [33]. This report is extremely im- portant because it demonstrates the feasibility of per- forming prospective, randomized studies of surgical technique in colorectal cancer surgery.
The technique of vascular ligation and division before tumor mobilization is shown in Figure 2 [14]. For right colon lesions the mesentery of the colon and terminal ileum can be opened for high division of the ileocolic artery and vein, though care must be taken not to injure the duodenum, right ureter, and superior mesenteric arterial trunk. Many surgeons would feel more comfortable mobilizing the right colon to pro- tect these structures before ligation of the ileocolic vessels. More proof of a survival advantage of the “no-touch technique” may need to be demonstrated to compensate for this potential risk of intraoperative injury.
LUMINAL LIGATION McGrew and colleagues [30] also found malignant
cells within the lumen of the colon after operative manipulation of a colonic tumor. It was their conten- tion that viable tumor cells might implant in the anas- tomotic line and be the explanation for suture line recurrence in colorectal cancer. It was therefore rec-
ommended that the lumen of the colon be occluded proximal and distal to the primary tumor by ligating the colon externally with cotton tapes (Cole tapes) [34] before operative manipulation and mobilization of the tumor. This procedure was found useful in historical comparison studies of suture line recurrence rates from various institutions. An alternative viewpoint well supported by recent data is that apparent suture line recurrence is caused by inadequate resection of the distal mesorectum [lo]. In the area where luminal liga- tion would be most needed, i.e., for tumors of the mid- and upper rectum, distal ligation before mobilization is very difficult to perform.
SUMMARY If the concept of radical surgery were to be taken to
its extreme limits for carcinomas of the mid-rectum, the inferior mesenteric artery would be ligated flush with the aorta, the inferior mesenteric vein would be ligated at the duodenojejunal fossa, the internal iliac lymph nodes would be resected with possible ligation of the hypogastric blood vessels, and paraaortic lymph nodes would be removed. As much as a 10 cm margin distal to the primary tumor would need to be obtained along with all the distal mesorectum, the ovaries, en bloc resection of adherent adjacent structures, and, more often than not, resection of the remainder of the abdominal colon, thus requiring low ileoproctostomy. The clinical results would frequently be intractable diarrhea, problems with fecal continence, a 67% inci- dence of genitourinary complications and impotence, without a proven survival advantage for these tech- niques when compared with more limited resection. A less radical resection would avoid most of these com- plica tions.
Yet it has been shown that variations in surgical technique are the most important determinants of can- cer recurrence. Many of the techniques described may be critical to patient survival from colorectal cancer. There is the implication of survival advantage for each of them. However, with the exception of the Dutch study of “no-touch technique,” the appropriate stud- ies to determine the efficacy of these techniques has simply never been done.
Cancer of the colon and rectum is the second most common cause of cancer death in the United States. Despite a decline in incidence and mortality since its peak in 1985 [ 3 5 ] more work is needed to determine what factors are responsible for this improvement. Primary and secondary prevention should not be over- looked, but evidence indicates that surgical technique may also be a major influence in the recent changes in incidence and mortality of colorectal cancer. There continues to be great need for randomized, prospec-

Surgical Technique for Colorectal Cancer 207
tive studies of sufficient quality to evaluate the effects of surgical technique in the treatment of colon and rectal cancer.
REFERENCES 1. Allingham HW: Cancer of the rectum: Its etiology, symptoms,
varieties, and treatment. In Gant SG (ed): “Diseases of the Rectum, Anus, and Contiguous Textures.” Philadelphia: FA Davis, 1896, 29 1-307.
2. Goligher JC: Incidence and pathology of carcinoma of the colon and rectum. In Goligher JC (ed): “Surgery of the Colon, Rectum, and Anus.” London: Balliere Tindall, 1975,481-518.
3. Miles WE: A method of performing abdominoperineal resec- tion for carcinoma of the rectum and of the terminal portion of the pelvic colon. Lancet 2:1812-1813, 1908.
4. Moynihan BGA: Cancer of the sigmoid flexure and rectum. Surg Gynecol Obstet 6:463-466, 1908.
5. Jochem RJ, Reading CC, Dozois RR, et al: Endorectal ul- trasonographic staging of rectal carcinoma. Mayo Clin Proc
6. Roubein LD. David C, DuBrow R, et al: Endoscopic ul- trasonography in staging rectal cancer. Am J Gastro 85:1391- 1394, 1990.
7. Busuttil RW, Foglia RP, Longmire WP: Treatment of carci- noma of the sigmoid colon and upper rectum. A comparison of local segmental resection and left hemicolectomy. Arch Surg
8. Williams NS: The rationale of preservation of the anal sphinc- ter in patients with low rectal cancer. Br J Surg 71:575-581, 1984.
9. Heald RJ. Husband EM, Ryall RDH: The mesorectum in rectal cancer surgery: The clue to pelvic recurrence? Br J Surg
10. Heald RJ. Ryall RDH: Recurrence and survival after total mesorectal excision for rectal cancer. Lancet 1 :1479-1482. 1986.
1 I . Grinnell RS: Distal intramucosal spread of carcinoma of the rectum and rectosigmoid. Surg Gynecol Obstet 99:421-430, 1954.
12. Nicosia JF, Abcarian H: The localization of rectosigmoidal tumors or biopsy sites by methylene blue marking. Dis Colon Rectum 20:231-235, 1977.
13. Grinnell RS: Results of ligation of inferior mesenteric artery at the aorta in resection of carcinoma of the descending and sigmoid colon and rectum. Surg Gynecol Obstet 121:1031- 1035. 1965.
14. Abcarian H, Pearl RK: A simple technique for high ligation of the inferior mesenteric artery and vein. Dis Colon Rectum 34:1138, 1991.
15. Pezim ME. Nichols RJ: Survival after high or low ligation of the inferior mesenteric artery during curative surgery for rectal cancer. Ann Surg 200:729-733, 1984.
16. Enker WE, Laffler UT, Block GE: Enhanced survival of pa- tients with colon and rectal cancer is based upon wide ana- tomic resection. Ann Surg 190:350-354, 1979.
65: 1571-1577, 1990.
112:920-923, 1977.
691613-616, 1982.
17. Stearns MW, Deddish MR: Five-year results of abdominal lymph node dissection for carcinoma of rectum. Dis Colon Rectum 2: 1 69-1 72, 1959.
18. Glass RE, Richie JK, Thompson HR, et al: The results of surgical treatment of cancer of the rectum by radical resection and extended abdominoiliac lymphadenectomy. Br J Surg 71:
19. Quirke P. Dixon MF, Dundey P, et al: Local recurrence of rectal adenocarcinoma due to inadequate surgical resection: Histopathological study of lateral tumor spread and surgical excision. Lancet 2:996-998, 1986.
20. Hojo K, Sawada T, Moriya Y: An analysis of survival and voiding: Sexual function after wide ileopelvic lymphadenec- tomy in patients with carcinoma of rectum compared with conventional lymphadenectomy. Dis Colon Rectum 32: 118 .- 133, 1989.
21. McGlone TP, Bernie WA, Elliot DW: Survival following ex- tended operations for extracolonic invasion by colon cancer. Arch Surg 117:595-599, 1982.
22. Prohaska JV, Nelson S. Evans SO: Radical surgery in ad- vanced carcinoma of intra-abdominal organs. Arch Surg 73:
23. Polk HL: Extended resection for selected adenocarcinoma of the large bowel. Ann Surg 1975:892-896, 1979,.
24. Neuman HK, Stearns MW: Re-exploration for “unresectable“ colonic carcinoma. Dis Colon Rectum 18576-580. 1973.
25. Barr SS, Valiente MA, Bacon HE: Rationale for bilateral oo- phorectomy concomitant with resection for carcinoma of the rectum and colon. Dis Colon Rectum 5:450-452. 1962.
26. McKeigan JM, Ferguson JA: Prophylactic oophorectomy and colorectal cancer in premenopausal patients. Dis Colon Rec- tum 22:401-405, 1979.
27. Morrow M, Enker WE: Late ovarian metastases in carcinoma of the colon and rectum. Arch Surg 119:1385-1388, 1984.
28. Barnes JP: Physiologic resection of the right colon. Surg Gyne- col Obstet 94:723-726. 1952.
29. Cole WH, Packard D, Southwick HW: Cancer of the colon and special reference to prevention of recurrence. JAMA 155: 1549- 1553, 1954.
30. McGrew EA, Lars JP. Cole WH: Free malignant cells in rela- tion to recurrence of cancer of the colon. JAMA 154:1251- 1254, 1954.
31. Roberts S. Jonasson 0, Long L, et al: Clinical significance of cancer cells in the circulating blood: two- to five-year survival. Ann Surg 154:362-371, 1961.
32. Turnbull RB, Kyle K, Wilson FR, et al: Cancer of the colon: The influence of the no-touch isolation technique in survival rate. Ann Surg 166420-427, 1967.
33. Wiggers T, Jeekel J, Arends JW, et al: No-touch isolation technique in colon cancer: A controlled prospective trial. Br J Surg 75:409-415, 1988.
34. Cole WH, Roberts SS, Graham AL: Carcinoma of the colon. Arch Surg 91:547-557, 1965.
35. DeCosse JJ, Tsioulias GJ, Jacobson JS: Colorectal cancer: Detection, treatment, and rehabilitation. CA 44( 1):27-4?. 1994.
599-601, 1985.
671-681, 1956.
36. Nelson RL: Prob Gen Surg 4:93-102, 1987.