syphilis gebre k. tseggay, md february 13, 2006. syphilis introduction caused by treponema pallidum....
TRANSCRIPT

SYPHILIS
Gebre K. Tseggay, MD
February 13, 2006

SYPHILISINTRODUCTION
• Caused by Treponema pallidum.• Transmission: sexual; maternal-fetal, and rarely
by other means. • Primary and secondary syphilis in the US
dropped by ~ 90 %t from 1990 to 2000, the number of cases have gone up since then.
• A dramatic increase in cases in men from 2000 to 2002 reflected syphilis in MSM.
• Syphilis increases the risk of both transmitting and getting infected with HIV.
• Do HIV testing in all patients with syphilis.





STAGES OF SYPHILIS
1. Primary2. Secondary3. Latent
• Early latent • Late latent
4. Late or tertiary • May involve any organ, but main parts are:
– Neurosyphilis– Cardiovascular syphilis– Late benign (gumma)
PRIMARY SYPHILIS(The Chancre)
• Incubation period 9-90 days, usually ~21 days. • Develops at site of contact/inoculation.• Classically: single, painless, clean-based, indurated
ulcer, with firm, raised borders. Atypical presentations may occur.
• Mostly anogenital, but may occur at any site (tongue, pharynx, lips, fingers, nipples, etc...)
• Non-tender regional adenopathy • Very infectious.• May be darkfield positive but serologically negative. • Untreated, heals in several weeks, leaving a faint scar.




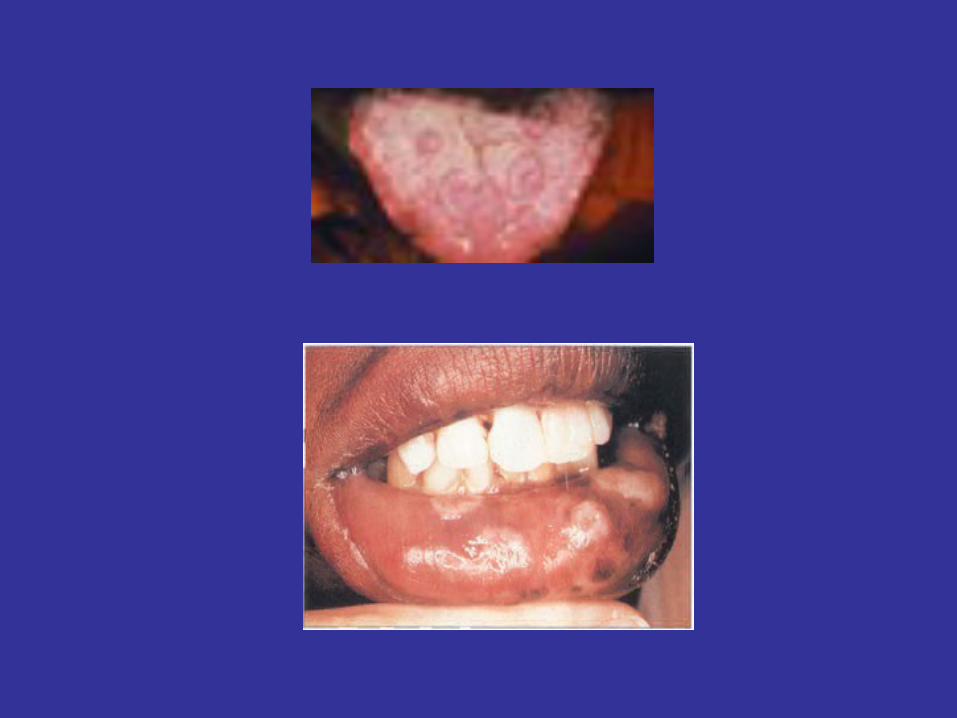
“Kissing chancres”


Oral chancres in primary syphilis

SECONDARY SYPHILIS
• Seen 6 wks to 6 mos after primary chancre• Usually w diffuse non-pruritic, indurated rash, including
palms & soles.• May also cause:
– Fever, malaise, headache, sore throat, myalgia, arthralgia, generalized lymphadenopathy
– Hepatitis (10%)– Renal: an immune complex type of nephropathy with
transient nephrotic syndrome– Iritis or an anterior uveitis– Bone: periostitis– CSF pleocytosis in 10 - 30% (but, symptomatic
meningitis is seen in <1%)

SECONDARY SYPHILIS(Cont.)
• The skin rash:– Diffuse,– often with a superficial scale (papulosquamous). – May leave residual pigmentation or depigmentation.
• Condylomata Lata:– Formed by coalescence of large, pale, flat-topped papules.– Occur in warm, moist areas such as the perineum.– Highly infectious.
• Mucosal lesions: ~ 30% of secondary syphilis patients develop mucous patch
(slightly raised, oval area covered by a grayish white membrane, with a pink base that does not bleed).
– Highly infectious


Condylomata lata

Alopecia areata

SECONDARY SYPHILIS Differential diagnosis
• The rash may be confused with– Pityriasis rosea (usually has a herald patch and lesions seen along lines
of skin cleavage)
– Drug eruptions– Acute febrile exanthems– Psoriasis– Lichen planus – Scabies
• The mucous patch may be confused with oral thrush. • Malaise, sore throat, generalized adenopathy, hepatitis,
& rash may be confused with infectious mononucleosis. • Fortunately, the serologic tests for syphilis are positive in 99% of
secondary syphilis pts.

RECURRENT SYPHILITIC SKIN LESIONS
• Seen in 20-30% of pts, after resolution of primary or secondary syphilis.
• Recurrent lesions are usually fewer & more firmly indurated than initial lesions
• Are infectious (like those in primary & sec. syphilis)

Lesions of syphilis resolve without treatment although person remains infected
LATENT SYPHILIS
Positive syphilis serology without clinical signs of syphilis (& has normal CSF). – It begins with the end of secondary syphilis and may
last for a lifetime.– Pt may or may not have a h/o primary or secondary
syphilis. – Diseases known to cause occasional false-positive
nontreponemal test reactions for syphilis, such as systemic lupus erythematosus (SLE), and congenital syphilis must be excluded before the diagnosis of latent syphilis can be made.
• Is divided into early and late latency.
LATENT SYPHILIS (cont.)
1. Early latent:– The first year after the resolution of primary or
secondary lesions, or– A reactive serologic test for syphilis in an
asymptomatic individual who has had a negative serologic test within the preceding year.
– Infectious.
2. Late latent:– Usually not infectious, except for the pregnant
woman, who may transmit infection to her fetus.

World War II Poster: Both of These Men Had Syphilis
•1/3 of untreated pts will proceed to tertiary syphilis

LATE SYPHILIS‘Tertiary Syphilis’
• Is the destructive stage of the disease.• Lesions develop in skin, bone, & visceral organs (any organ).• The main types are:
– Late benign (gummatous) – Cardiovascular & – Neurosyphilis
• Can be crippling and life threatening• Blindness, deafness, deformity, lack of coordination, paralysis,
dementia may occur• It is usually very slowly progressive, barring certain neurologic
syndromes which may develop suddenly due to endarteritis and thrombosis in the CNS
• Late syphilis is noninfectious.


NEUROSYPHILIS
• Divided into 5 groups, which may overlap:– Asymptomatic neurosyphilis – Syphilitic meningitis – Meningovascular syphilis– General paresis– Tabes dorsalis

ASYMPTOMATIC NEUROSYPHILIS
• Dx: CSF abnormalities, such as pleocytosis, protein elevation, or a reactive VDRL in the absence of signs and symptoms of neurologic disease.
• Some untreated secondary syphilis pts have an abnormal CSF test result

SYPHILITIC MENINGITIS
• ‘Aseptic meningitis’• Usually within the first year of infection, but mwithin the first year of infection, but may occur at
any time after the primary stage. • CSF shows:
– Lymphocytic pleocytosis – Elevated protein and usually normal glucose concentrations– VDRL test is usually reactive.
• It can mimic tuberculous or fungal meningitis or aseptic meningitis of various causes.
• Often involves the base of the brain and may result in unilateral or bilateral cranial nerve palsies.
• Without treatment, syphilitic meningitis usually resolves, like the other manifestations of early syphilis.

MENINGOVASCULAR SYPHILIS
• Usually occurs 5 to 10 years after the initial infection. More common in men.
• Caused by cerebrovascular thrombosis and infarction due to syphilitic endarteritis and perivascular inflammation. Often with associated aseptic meningitis.
• Consider when young pt with a history of syphilis has a CVA without other causes for CVA. – But, most CVAs even in patients with a reactive serologic test for
syphilis are not caused by this.

GENERAL PARESIS• Chronic meningoencephalitis resulting in gradually progressive loss of cortical
function.• Occurs 10 to 20 years after the initial infection. • Pathologically, there is a perivascular and meningeal chronic inflammatory
reaction with thickening of the meninges, granular ependymitis, degeneration of the cortical parenchyma, and abundant spirochetes in the tissues.
• With effective penicillin therapy, this disease has become much less common; • In the US, first admissions to mental hospitals because of syphilitic psychosis
declined from 7694 in 1940 to 154 in 1968, the last year for which definite figures are available.
• Physical signs are primarily those of the altered mental status. Cranial nerve palsies are uncommon. Optic atrophy is rare. The complete Argyll Robertson pupil is also uncommon, but irregular or otherwise abnormal pupils are not infrequent. Peripheral reflexes are often somewhat increased.
• CSF is almost always abnormal, with lymphocytic pleocytosis and increased protein. Serum & CSF VDRL is usually reactive.
• Responds well to penicillin therapy if administered early. As many as 1/3 of treated patients may develop progressive neurologic decline in later years.

TABES DORSALIS • Occurs 20-30 years after the initial infection.• It is uncommon. (The survey of newly diagnosed late syphilis cases
in Denmark between 1961 and 1970 showed that ~ 11% of pts with late syphilis and 40% of those with clinical neurosyphilis had evidence of tabes dorsalis). More common in whites and in men.
• It’s a slowly progressive, degenerative disease involving the posterior columns and posterior roots of the spinal cord.
• Results in progressive loss of peripheral reflexes, impairment of vibration and position sense, and progressive ataxia.
• Sudden and severe painful crises are a characteristic:– Usually involve the lower extremities but may occur at any site. – Severe, sharp abdominal pains may lead to exploratory surgery. – Attacks may be triggered by exposure to cold or other stresses or may
arise with no obvious precipitating cause. • Bladder incontinence & impotence are common. • Chronic destructive changes of the large joints of the affected limbs
may be seen in advanced cases (i.e., Charcot's joints).

TABES DORSALIS (CONT.)
• Optic atrophy is seen in 20% of cases. • Typical cases present with: lightning pains, ataxia, Argyll
Robertson pupils, absent deep tendon reflexes, and loss of posterior column function. Atypical cases are difficult to diagnose.
• Serum VDRL may be non-reactive in 30 - 40%, CSF-VDRL may be non-reactive in 10-20%, serum FTA-ABS is almost always reactive.
• Penicillin may arrest progression but does not reverse the symptoms. Carbamazepine in doses of 400 to 800 mg/day may effectively treat the lightning pains.

CARDIOVASCULAR SYPHILIS• May not manifest clinically until 20-30 years after
infection, but usually begins within 5-10 years after initial infection.
• Primarily aortic insufficiency and aortic aneurysm of the ascending aorta. Other large arteries may sometimes be involved, and rarely the coronary ostia may be involved.
• Caused by obliterative endarteritis of the vasa vasorum with resultant damage to the intima & media of the great vessels, causing dilatation of the ascending aorta and eventually results in stretching of the ring of the aortic valve, producing aortic insufficiency. The valve cusps remain normal.
• Asymptomatic aortitis is best diagnosed by visualizing linear calcifications in the wall of the ascending aorta.
• More common in men than in women and possibly in blacks than in whites.

LATE BENIGN SYPHILIS (THE GUMMA)
• The gumma was the most common complication of late syphilis in the Oslo Study of untreated patients (1891 to 1951); rare in the penicillin era.
• Usually develop 1-10 years after infection and may involve any part of the body.
• Gummas may be single or multiple. Start as a superficial nodule or as a deeper lesion that breaks down to form punched-out ulcers. They are ordinarily indolent, slowly progressive, and indurated granulomata, with central healing with an atrophic scar surrounded by hyperpigmented borders.
• Cutaneous gummas may be confused with skin lesions of TB, sarcoidosis, leprosy, and deep fungal infections (but, gumma is the only such lesion to heal dramatically with penicillin therapy). Gumma can also be papulosquamous type mimicking psoriasis.
• T. pallidum is ordinarily not demonstrable by silver stain but can sometimes be recovered by inoculation of rabbits.
• May be destructive, but responds rapidly to treatment, thus, is relatively benign.

LATE BENIGN SYPHILIS (Gumma) (Cont.)
• May also involve deep visceral organs, particularly the respiratory tract, gastrointestinal tract, bones, larynx, lung, liver,
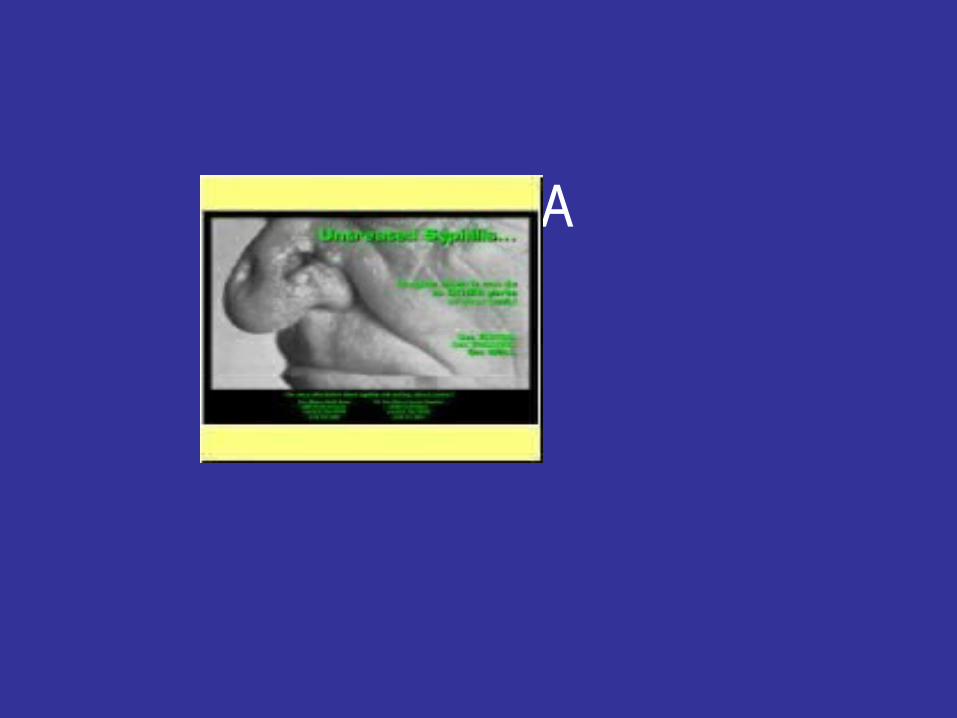
• In earlier centuries, gummas of the nose and palate commonly resulted in septal perforations and disfiguring facial lesions.
• Bone involvement may cause a characteristic symptom of nocturnal bone pain. – Radiologic abnormalities, when present, include
periostitis, and lytic or sclerotic, destructive osteitis.
GUMMA

Late syphilis - serpiginous gummata of forearm

Late syphilis - ulcerating gumma

CLINICAL MANIFESTATION IN SUMMARY

TESTS FOR SYPHILIS
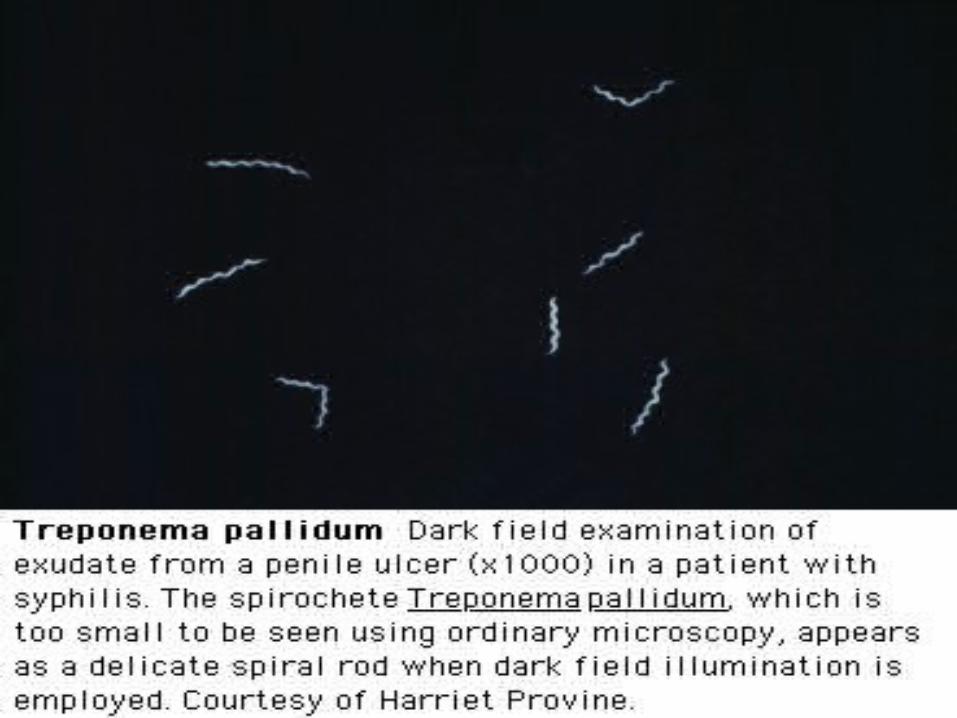
• Dark field Microscopy
• VDRL, RPR
• FTA-ABS, MHA-TP
• Direct Fluorescent Antibody (DFA)



NONTREPONEMAL SEROLOGIC TESTSIMPORTANT POINTS
• VDRL and RPR: tests of choice for screening and monitoring response to tx.
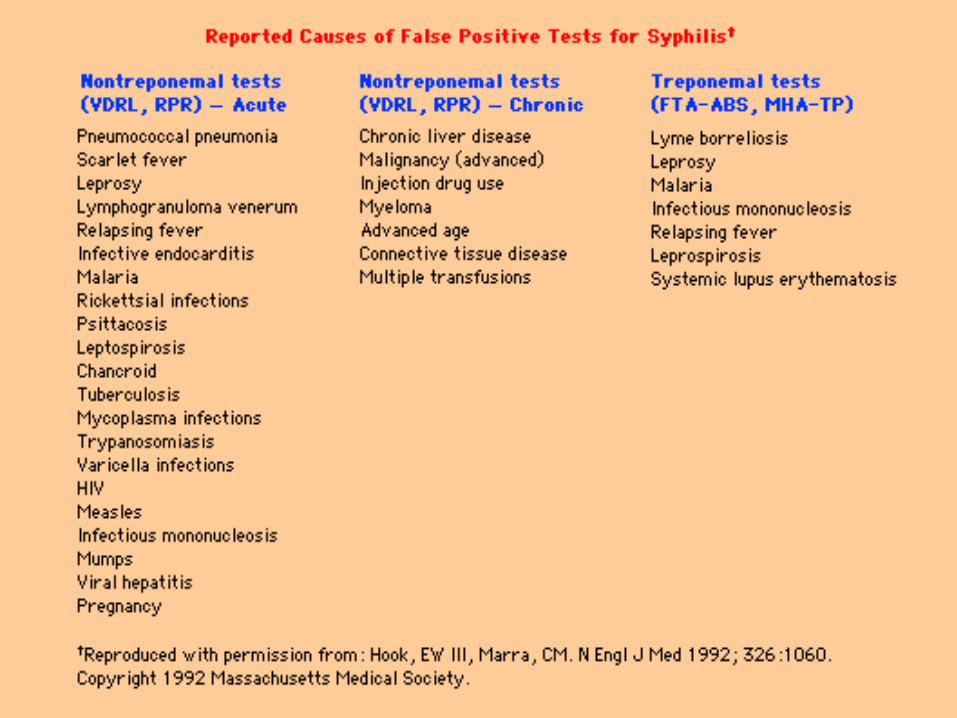
• Nonspecific; must be confirmed by treponemal test. False-positives usually have a titer of < 1:8.
• VDRL and RPR titers are not interchangeable (RPR titer is often slightly higher than VDRL titer).
• A nonreactive VDRL test does not exclude primary syphilis. • VDRL is positive for 99% of patients with secondary syphilis.• Consider the PROZONE PHENOMENON. Patients with very high
titers of antibody may have a “negative’ VDRL; dilution of the serum results in conversion of a negative test to a positive test result.
• VDRL reactivity tends to diminish in later stages of the disease• VDRL titers of treated patients may turn negative with time or may
remain low-normal for long time, “serofast.”

TREPONEMAL TESTS
FTA-ABS• Used as a confirmatory tests. • Sensitivity and specificity high.
– 85% of patients with primary syphilis are reactive– 99% with secondary syphilis– > 95% with late syphilis (It may be the only test with a positive result for
patients with cardiovascular or neurologic syphilis). • Remains reactive for lifein most, despite adequate therapy. Only 15-
25 % of those treated for primay syphilis may turn negative by 2-3 yrs.• False positive in other treponemal diseases (pinta, yaws..) and other
spirochete diseases (Lyme, leptospirosis…)
MHA-TP test (microhemagglutination assay for T. pallidum; agglutination of RBCs to which T. pallidum antigens have been fixed is the basis).


Primary, Secondary, Early LatentSyphilis
Recommended regimen
-Benzathine Penicillin G, 2.4 million units IMPenicillin Allergy*
-Doxycycline 100 mg twice daily x 14 days or
-Ceftriaxone 1 gm IM/IV daily x 8-10 days (limited studies) or
-Azithromycin 2 gm single oral dose (preliminary data)
*Use in HIV-infection has not been studied
*Azithromycin Rx Failures reported --- San Francisco, CA 2002--2003
Primary/Secondary Syphilis Response to Treatment
• No definitive criteria for cure or failure are established
• Re-examine clinically and serologically at 6 and 12 months
• Consider treatment failure if signs/symptoms persist or sustained 4x increase in nontreponemal test
• In treatment-failure cases, do: HIV test, CSF analysis; administer benzathine pcn weekly x 3 wks
• Additional therapy not warranted in instances when titers don’t decline despite nl CSF and repeat therapy
Primary/Secondary SyphilisResponse to Therapy in HIV Infection
• Most respond appropriately to benzathine penicillin 2.4 million units IM
• Some experts recommend CSF exam before therapy and additional Rx (wkly benz pen IM x 3)
• Clinical/serologic evaluation at 3, 6, 9, 12, 24 mo; some perform CSF exam at 6 mo
• Rx/serologic failure (6-12 mo after Rx): CSF exam, retreat w. benz penicillin 2.4 mu wkly x 3

SyphilisLatent Syphilis
Recommended regimen
Benzathine penicillin G 2.4 million units IM at one week intervals x 3 doses
Penicillin allergy*Doxycycline 100 mg orally twice daily x 28 days
orTetracycline 500 mg orally four times daily x 28d
*Note: Duration of therapy 28 days;
Close clinical and serologic follow-up;
Data to support alternatives to pcn are limited

Latent SyphilisManagement Considerations
• Clinical evaluation for tertiary disease (aorititis, gumma, iritis)
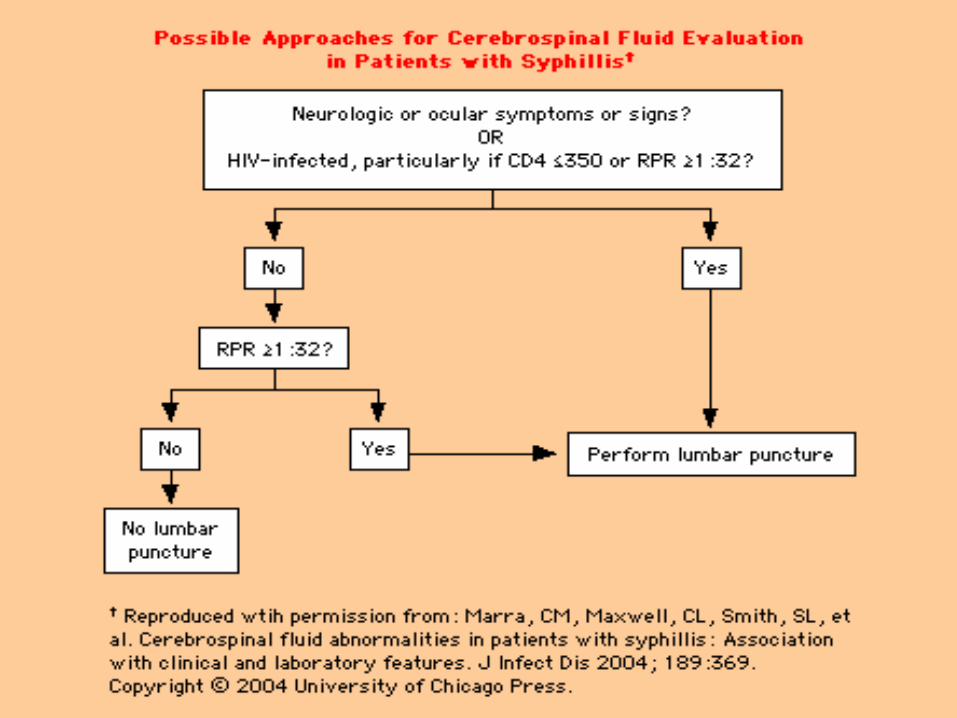
• LP should be done in pts w: neurologic or ophthalmic signs/sx, active tertiary disease, tx failure, HIV infection
• Some experts recommend CSF exam in those with nontreponemal titer of >1:32
• An interval of 10-14 days between benz pen doses may be acceptable before restarting treatment course in nonpregnant patients

Latent SyphilisResponse to Treatment
• Limited data available to guide evaluation
• Repeat RPR(VDRL) at 6, 12, 24 months
• Perform CSF exam & re-treat for latent syphilis, if:
– 4x increase in titer,
– initial nontreponemal titer >1:32 fails to decline 12-24 mo after tx, or
– signs/sx

Latent SyphilisResponse to Therapy in HIV Infection
• CSF exam before treatment
• If Normal CSF exam: benzathine penicillin 2.4 million units IM wkly x 3 weeks
• Clinical/serologic evaluation at 6, 12, 18, 24 months
• Repeat CSF exam and treatment:– if there is development of sx or 4x titer rise.
– if nontreponemal titer does not decline in 12-24 months

NeurosyphilisRecommended regimen
Aqueous crystalline penicillin G, 18-24 million units administered 3-4 million units IV every 4 hours for 10-14 days
Alternative regimen
Procaine penicillin 2.4 million units IM daily plus probenecid 500 mg orally four times daily for 10-14 days
Some experts administer benzathine penicillin 2.4 million units IM wkly x 3 after completion of these regimens to provide comparable duration of treatment with latent syphilis

NeurosyphilisPenicillin Allergy
• Ceftriaxone 2 gm daily IM/IV for 10-14 days
• Consideration of cross-reactivity
• Pregnant patients should undergo penicillin desensitization
• Other regimens have not been evaluated

NeurosyphilisResponse to Treatment
• Initial CSF pleocytosis--repeat CSF exam every 6 months until cell count normal
• CSF VDRL and protein decline slowly
• Consider re-treatment if cell count has not decreased by 6 months or if CSF is not normal by 2 years

SyphilisTreatment in Pregnancy
• Screen for syphilis at first prenatal visit;
• Repeat RPR third trimester/delivery for those at high risk or high prevalence areas
• Treat for the appropriate stage of syphilis
• Some experts recommend additional benzathine penicillin 2.4 mu IM after the initial dose for primary, secondary, or early latent syphilis
• Management and counseling may be facilitated by sonographic fetal evaluation for congenital syphilis in the second half of pregnancy

Recommended Follow-up
after Treatment of Syphilis Primary and Secondary Syphilis • VDRL or RPR at 6 and 12 months • Fourfold drop in titers generally expected after 6 months Latent Syphilis • VDRL or RPR at 6, 12 and 24 months • a titer of > 1:32 should fall 4-fold within 12-24 months Pregnancy • VDRL or RPR in the third trimester and at delivery, monthly if at high
risk of reinfection or area of high prevalence of syphilis. Response should be the same as for non-pregnant persons.
HIV infection • VDRL or RPR at 3, 6, 19, 12 and 24 months for primary and
secondary syphilis, and 6, 12, 18 and 24 months for latent syphilis. • Expect a fourfold decrease within 6 to 12 months for primary and
secondary syphilis, and within 12 to 24 months for latent syphilis

SyphilisManagement of Sex Partners
• Rx presumptively: Exposure to primary, secondary, or early latent within 90 days (even
if serology neg)
• Rx presumptively if serology not available: Exposure to primary, secondary, or early latent > 90 days
• Exposure to latent syphilis who have high nontreponemal titers > 1:32, consider presumptive tx for early syphilis

Jarisch-Herxheimer reaction• Manifestations: general malaise, fever, headache, sweating, rigors,
or a temporary exacerbation of the syphilitic lesions.• Usually seen w early syphilis, especially secondary syphilis.• Seen within 6 to 12 h of initial treatment. • Usually subsides within 24 h and poses no danger but may produce
anxiety. • However, patients with general paresis or a high CSF cell count are
likely to develop serious disorders, such as seizures or strokes. • It may be confused with allergy to antibiotics.• May indicate coexistent syphilis in patients treated for other
conditions with antibiotics active against syphilis• This reaction should be explained to the patient before
treatment.
EPIDEMIOLOGIC INVESTIGATION AND TREATMENT
• Report all patients with syphilis to public health authorities.
• Careful interview by qualified persons of all patients with early syphilis (<1 year) should be done, to determine the nature of their recent sex contacts.
• Treat sexual contacts of patients with early syphilis even if the contacts are clinically and serologically normal on examination.
• In general, preventive treatment is given to all sexual contacts of the past 90 days (although nearly all cases of syphilis in contacts develop within 60 days of exposure).

Inadvertent Use of Bicillin® C-R to Treat Syphilis Infection --- Los Angeles, California,
1999--2004MMWR??? March 11, 2005 / 54(09);217-219
• In March 2004, the Los Angeles County Department of Health Services (LACDHS) was notified that a large nonprofit clinic serving the gay and lesbian community in Los Angeles used a nonrecommended preparation of penicillin to treat syphilis patients during January 1999--March 2004.
• The clinic had inadvertently used Bicillin® C-R, a mixture of 1.2 million units (MU) benzathine penicillin G (BPG) and 1.2 MU procaine penicillin G, rather than Bicillin® L-A, a preparation that contains the 2.4 MU BPG per dose recommended by CDC .
• Bicillin L-A is recommended for treating syphilis and upper respiratory tract infections caused by susceptible streptococci .
• Bicillin C-R is indicated for streptococcal infections of the skin and respiratory tract; however, its efficacy in treating syphilis is unknown.
• The inadvertent use of Bicillin C-R, which contains only half the recommended dose of BPG for syphilis, was discovered after a patient treated for syphilis read the product insert, which stated that the medication was not indicated for treatment of syphilis

"He who knows syphilis, knows medicine"
Sir William Osler

nice little limerick on syphilis:
There was a young man from Back Bay Who thought syphilis just went away. He believed that a chancre Was only a canker That healed in a week and a day. But now he has "acne vulgaris" -- (Or whatever they call it in Paris); On his skin it has spread From his feet to his head, And his friends want to know where his hair isThere's more to his terrible plight:His pupils won't close in the light His heart is cavorting, His wife is aborting, And he squints through his gun-barrel sight. Arthralgia cuts into his slumber; His aorta's in need of a plumber; But now he has tabes, And saber-shinned babies, While of gummas he has quite a number. He's been treated in every known way, But his spirochetes grow day by day; He's developed paresis, Has long talks with Jesus,And thinks he's the Queen of the May.




Congenital Syphilis• Congenital syphilis is transmitted in utero after the first 16 weeks of
pregnancy, therefore it is usually not a cause of abortion during the first trimester.
• The infected child born later in a family usually has less severe syphilis. • Again, it has been divided according to the arbitrary dividing line of two
years into early and late types.• Early Congenital • The features are similar to secondary syphilis. Usually it occurs 2-8 weeks
after birth, presenting with failure to thrive, muco-cutaneous lesions (condylomata lata), generalized lymphadenopathy, nasal snuffles and skin rash.
• Late Congenital • The onset usually occurs at or near puberty. Well-known stigmata include
nerve deafness, interstitial keratitis, Hutchison's teeth (Hutchison's triad), rhagades around mouth, clutton's joint, osteitis & chondritis (saddle nose, frontal bossing, sabre tibia) and perforated palate.

CONGENITAL SYPHILIS• Late congenital syphilis is defined as congenital syphilis of more
than 2 years' duration. The disease may remain latent with no manifestation of late damage. Cardiovascular alterations have not been observed in patients with congenital syphilis. Neurologic manifestations are common, and there may be eighth cranial nerve deafness and interstitial keratitis. The latter occurs in more than 10% of patients but may not be apparent until the 10th year of life or later. Periostitis may result in prominent frontal bones, depression of the bridge of the nose (i.e., saddle nose), poor development of the maxilla, and anterior bowing of the tibias (i.e., saber shins). There may be late-onset arthritis of the knees (i.e., Clutton's joints). The permanent dentition may show characteristic abnormalities known as Hutchinson's teeth; the upper central incisors are widely spaced, centrally notched, and tapered in the manner of a screwdriver. The molars may show multiple, poorly developed cusps (i.e., mulberry molars). Some of the late manifestations such as interstitial keratitis and Clutton's joints may be caused by hypersensitivity responses and are benefited by corticosteroids in some cases.

Congenital Syphilis Infants with Seroreactive Mothers
• Nontreponemal test on infant serum
• Examination (nonimmune hydrops, jaundice, HSM, rhinitis, rash)
• Pathologic exam of placenta or umbilical cord (fluorescent antitreponemal antibody)
• Darkfield or DFA of suspicious lesions or body fluids

Congenital Syphilis Proven/highly probable disease
• Abnormal physical exam consistent with congenital syphilis
• Nontreponemal titer 4X > maternal titer or + DFA or darkfield
• Evaluation: CSF exam, CBC; other tests as clinically indicated--long bone films, LFTs, cranial US, eye exam, auditory brain stem response

Congenital SyphilisProven/highly probable disease
Aqueous crystalline penicillin G 100,000-150,000 units/kg/day, administered as 50,000 units/kg/dose IV q 12 hours during the first 7 days and thereafter q 8 hours for 10 days
or
Procaine penicillin G 50,000 units/kg/dose IM in a single daily dose for 10 days

Congenital Syphilis Normal exam/RPR < 4X maternal titer
• Mother inadequately treated;
• treated with nonpenicillin regimen;
• received tx < 4 wks before delivery; or
• mother has early syphilis with serologic response
Evaluation: CSF analysis, CBC/plt, long bone x-ray

Congenital SyphilisNormal Exam/RPR < 4X maternal titer
Aqueous penicillin G 100,000-150,000 units/kg/day as 50,000 units/kg/dose IV every 12 hours for first 7 d then q 8 hours for total of 10 d
or
Procaine penicillin G 50,000 units/kg/dose IM in single daily dose for 10 d
or
Benzathine penicillin G 50,000 units/kg/dose IM in single dose

Congenital Syphilis Normal exam/RPR < 4X maternal titer
• Mother treated appropriately > 4 wks before delivery; maternal RPR titers decreased 4X; no relapse or reinfection
• No evaluation required
• Benzathine pcn G 50,000 units/kg/dose IM

Congenital Syphilis Normal exam/RPR < 4X maternal titer
• Mother received adequate tx before pregnancy; maternal RPR remained low and stable during pregnancy and delivery
• No evaluation necessary
• No treatment required; some specialists would tx with single dose of benz pen G

Congenital SyphilisSubsequent Evaluation
• Clinical/serologic evaluation q 2-3 mo
• RPR should decline by 3 mo, nonreactive at 6 mo
• Stable or increasing titers after 6-12 mo--CSF analysis/parenteral pcn X 10 d
• Reactive treponemal/RPR after 18 mo re-evaluate and treat for congenital syphilis

Congenital SyphilisOlder Infants and Children
• Review records and maternal serology- congenital vs acquired
• Evaluation- CSF analysis, CBC/pts; +/- long bone films, auditory brain stem response
• Treatment- Aqueous pcn G 50,000 units/kg q 4-6 hours for 10 days

Syphilis-HIV Interactions• Syphilis, like other genital ulcer diseases, is associated with a three-fold to
five-fold increased risk for HIV acquisition. Presumably, genital ulcers act as portals of entry through which HIV may more readily infect exposed individuals.
• In individuals with HIV infection who acquire syphilis, the natural history of the infection may be modified. HIV-infected syphilis patients are somewhat more likely to present with secondary syphilis than are non-HIV-infected patients. HIV-infected, secondary syphilis patients are more likely to have coexistent chancres than are HIV-negative, secondary syphilis patients, suggesting that the healing of chancres is delayed or the appearance of secondary manifestations is accelerated in the presence of HIV co-infection.
• Neurosyphilis may be more common in patients with HIV infection; however, no large or carefully controlled studies document this association. In HIV-infected syphilis patients in whom therapy fails, neurosyphilis may be a more common presenting feature than in patients without HIV infection.
• Failure of treatment using currently recommended regimens for syphilis therapy is more common in patients with coexistent HIV infection. The magnitude of this increase, however, is small, and as a result, alternate treatment regimens are not recommended.
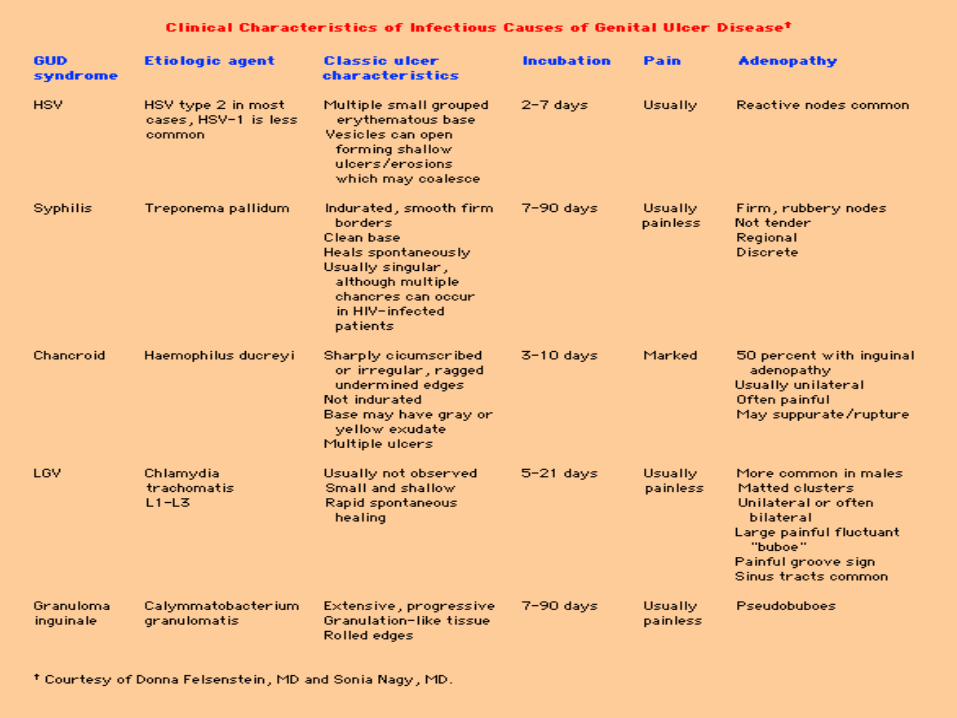

Differential diagnosis of a genital ulcer
• Genital herpes: usually multiple, painful, superficial, and if seen early, vesicular. Atypical presentations may be indistinguishable from a syphilitic chancre.
• Chancroid: usually painful, often multiple, frequently exudative, non-indurated.
• Lymphogranuloma venereum: a small, papular lesion associated with a regional adenopathy.
• Other conditions: granuloma inguinale, drug eruptions, carcinoma, superficial fungal infections, traumatic lesions, lichen planus.






Untreated Syphilis(The Oslo and Tuskegee studies)
The course of untreated syphilis was studied • retrospectively in a group of nearly 2000 patients with primary or secondary
disease diagnosed clinically (the Oslo Study, 1891–1951) and • prospectively in 431 African-American men with seropositive latent syphilis of 3
years' duration (the notorious Tuskegee Study, 1932–1972).
In the Oslo Study:• 24% of patients developed relapsing secondary lesions within 4 years, • 28% eventually developed one or more manifestations of tertiary syphilis.
– Cardiovascular syphilis, including aortitis, was detected in 10% of patients, none of whom had been infected before age 15;
– 7% of patients developed symptomatic neurosyphilis, and – 16% developed benign tertiary syphilis (gummas of the skin, mucous
membranes, and skeleton). – Syphilis was the primary cause of death in 15% of men and 8% of women. – Cardiovascular syphilis was documented in 35% of men and 22% of women
who eventually came to autopsy.– In general, serious late complications were nearly twice as common among
men as among women.

Untreated Syphilis (The Oslo and Tuskegee studies)
The Tuskegee Study showed that:• Death rate among untreated African-American men with syphilis (25 to 50 years
old) was 17% higher than that among uninfected subjects• 30% of all deaths were attributable to cardiovascular or CNS syphilis. By far the
most important factor in increased mortality was cardiovascular syphilis. Anatomic evidence of aortitis was found in 40 to 60% of autopsied subjects with syphilis (vs. 15% of control subjects), whereas CNS syphilis was found in only 4%.
• Rates of hypertension were also higher among the infected subjects. • The ethical issues eventually raised by this study (begun in the preantibiotic era
but continuing into the early 1970s) had a major influence on the development of current guidelines for human medical experimentation, and the history of the study may still contribute to a reluctance of some African Americans to participate as subjects in clinical research.
These two studies both showed that:• About 1/3 of patients with untreated syphilis develop clinical or pathologic evidence of
tertiary syphilis, • About 1/4 die as a direct result of tertiary syphilis, • There is additional excess mortality not directly attributable to tertiary syphilis.

The Tuskegee Syphilis Study1932-1972
• 600 low-income African-American males, 400 infected with syphilis are monitored for 40 years.
• Even though a proven cure (penicillin) became available in the 1950s, the study continues until 1972 with participants denied treatment.
• Perhaps as many as 100 died of syphilis during the study (Allen, 1978).