surgery promotes the development of...
TRANSCRIPT
Surgery promotes the development of endometriosis
Xishi Liu Shanghai OB/GYN Hospital
Fudan University Shanghai, China

Surgery
• Surgery is now a well accepted treatment modality
• Surgery is an effective treatment for – Cancer – Endometriosis
• Women tend to receive more surgeries – Gynecological operations – Plastic surgeries – Lipo suction
The downside of surgery
• A trauma • Carries its own risk of mortality and
morbidity • Risk of complications • Blood loss, transfusion, hypothermia, and
certain anesthesia can impact negatively on – Cell-mediated immunity – Thus promoting metastasis
• Laparotomy induces more stress hormones than laparoscopy (Muzii et al. 1996)
Documented risk of surgery • Breast augmentation surgery increases the
risk of – stomach (SIR = 2.65) – cervix (SIR = 3.18) – vulva (SIR = 2.51) – brain (SIR = 2.16) – leukemia (SIR = 2.19) (Brinton et al. 2001)
• Hysterectomy increases the risk of renal cancer (OR=1.8 (1.3—2.5)) (Gago-Dominguez et al. 1999)
• Surgical stress promotes metastasis (Sood et al. 2012)
Does surgery increase the risk of developing endometriosis?
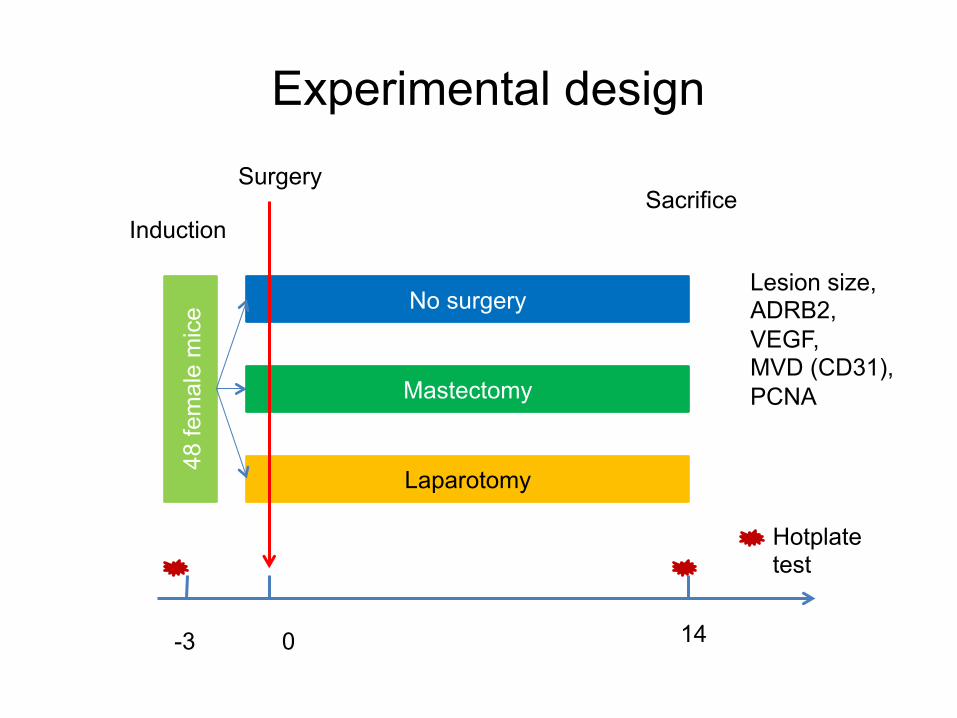
48 fe
mal
e m
ice
-3 0 14
Induction Sacrifice
Laparotomy
Mastectomy
No surgery Lesion size, ADRB2, VEGF, MVD (CD31), PCNA
Surgery
Hotplate test
Experimental design

Control Mastectomy Laparotomy
0.05
0.10
0.15
A: Lesion weight by groups
Group
Tota
l les
ion
wei
ght (
g)
**

C
C
-5 0 5 10 15
510
1520
B: Kinetics of mean hotplate latency
Time since surgery(Day)
Hot
plat
e la
tenc
y (s
ec)
M
M
L
L
CML
ControlMastectomyLaparotomyNS
*Induction
Surgery
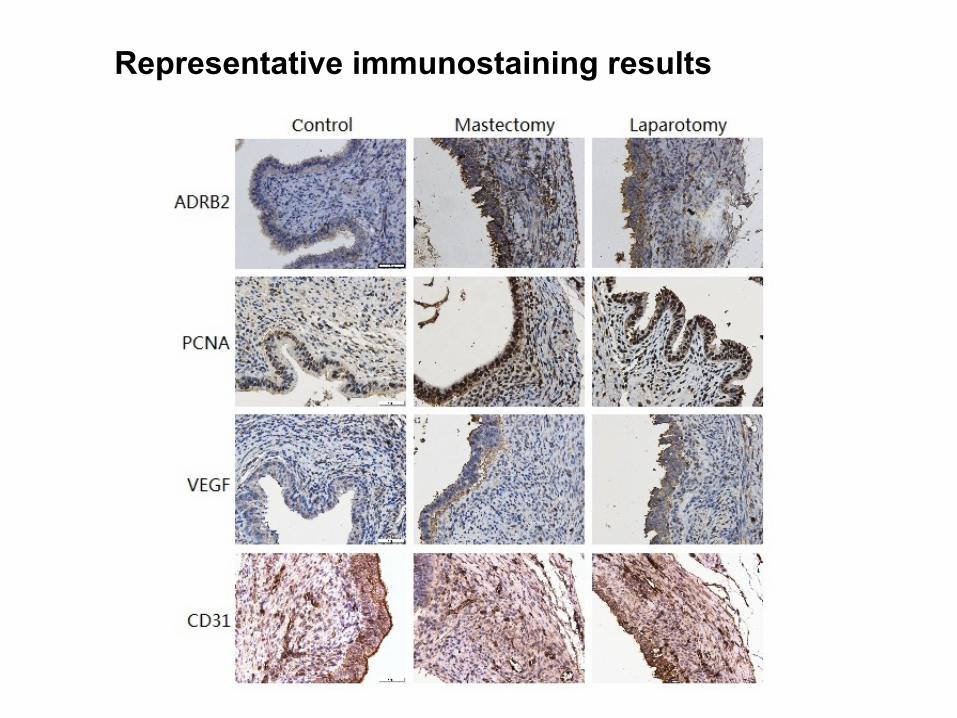
Representative immunostaining results

Control Mastectomy Laparotomy
0.00
0.10
0.20
0.30
A: ADRB2
Group
Stai
ning
leve
l
*****

Control Mastectomy Laparotomy
0.2
0.3
0.4
0.5
0.6
B: PCNA
Group
Stai
ning
leve
l
****
Control Mastectomy Laparotomy
0.10
0.15
0.20
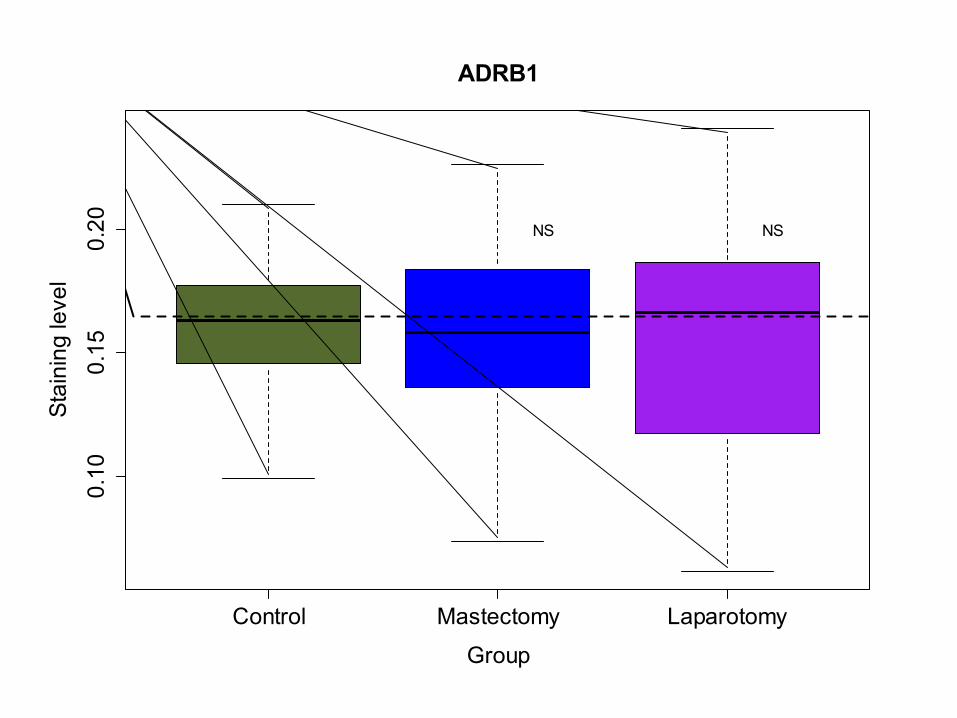
ADRB1
Group
Stai
ning
leve
l
**
***
NS NS
Control Mastectomy Laparotomy
0.10
0.15
0.20
0.25
0.30
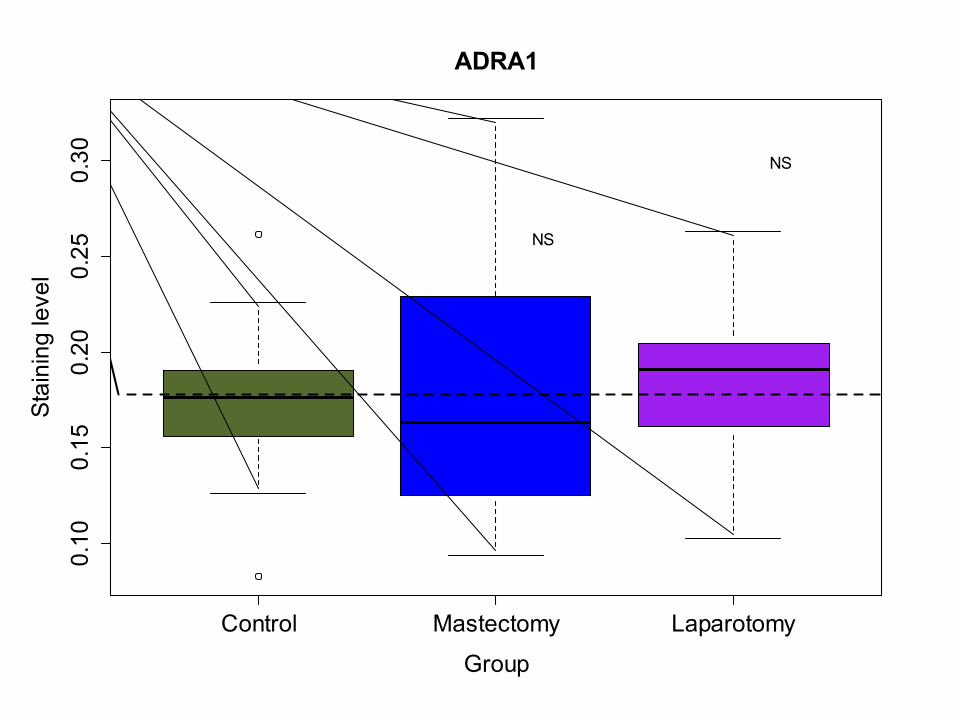
ADRA1
Group
Stai
ning
leve
l
NS
NS
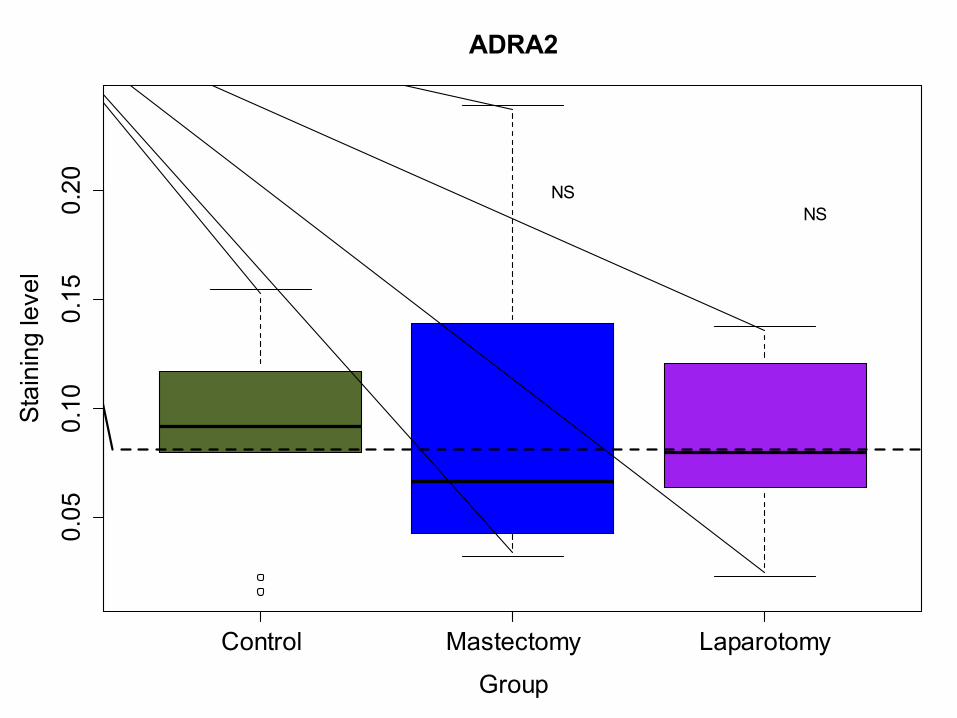
Control Mastectomy Laparotomy
0.05
0.10
0.15
0.20
ADRA2
Group
Stai
ning
leve
l
NSNS

Is intervention possible?

-7 .. -3 -2 -1 0 1 … 7 … 10 … 14
Induction
Laparotomy + Propranolol
Mastectomy + Propranolol
Propranolol
Laparotomy + PBS
Mastectomy + PBS
PBS
Surgery Sacrifice
The effect of surgery on the development of endometriosis
Day
60 f
emal
e B
lb/C
mic
e
Lesion size IHC: ADRB2, VEGF, MVD (CD31), PCNA
Hotplate test, bodyweight Randomization
Alzet pumps implanted

PBS Mast+PBS Lap+PBS Pro Mast+Pro Lap+Pro
18
19
20
21
22
23
24
A: Baseline bodyweight
Group
Bodyw
eig
ht
(g)
p=0.89
PBS Mast+PBS Lap+PBS Pro Mast+Pro Lap+Pro
18
19
20
21
22
23
24
B: Bodyweight 2w post induction
Group
Bodyw
eig
ht
(g)
p=0.24
PBS Mast+PBS Lap+PBS Pro Mast+Pro Lap+Pro
18
19
20
21
22
23
24
C: Bodyweight 2w after treatment
Group
Bodyw
eig
ht
(g)
p=0.01
PBS Mast+PBS Lap+PBS Pro Mast+Pro Lap+Pro
-2-1
01
23
45
D: Change in Bodyweight post induction
Group
Change
p=0.01
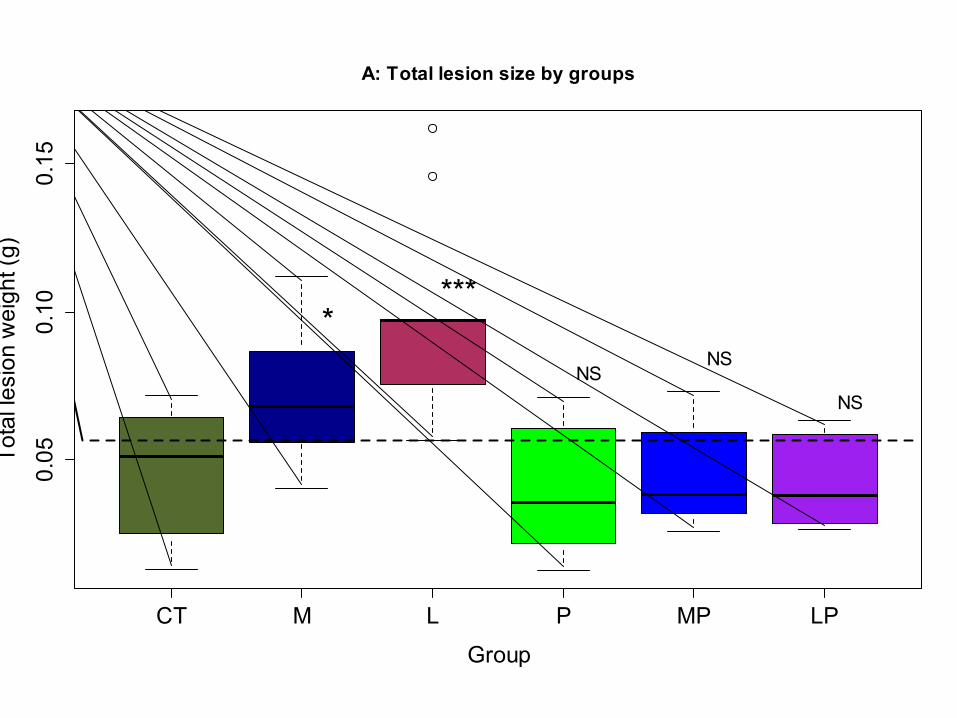
CT M L P MP LP
0.05
0.10
0.15
A: Total lesion size by groups
Group
Tota
l les
ion
wei
ght (
g)
****
NSNS
NS
CC
C
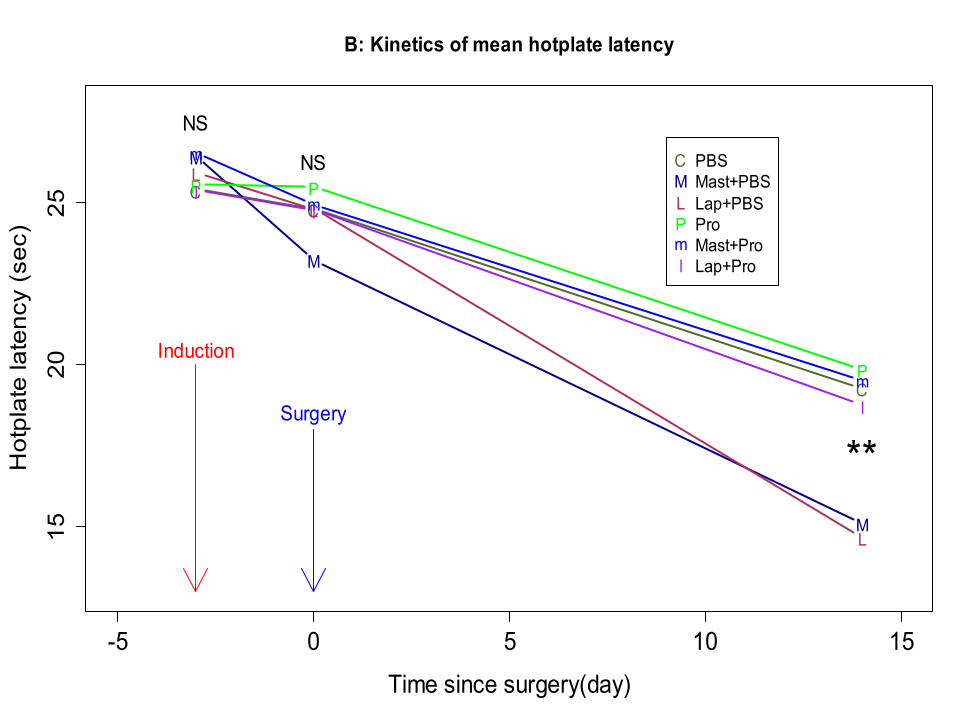
-5 0 5 10 15
1520
25B: Kinetics of mean hotplate latency
Time since surgery(day)
Hot
plat
e la
tenc
y (s
ec)
M
M
M
L
L
L
P P
P
m
m
m
ll
l
CMLPml
PBSMast+PBSLap+PBSProMast+ProLap+Pro
Induction
Surgery
NS
NS
**
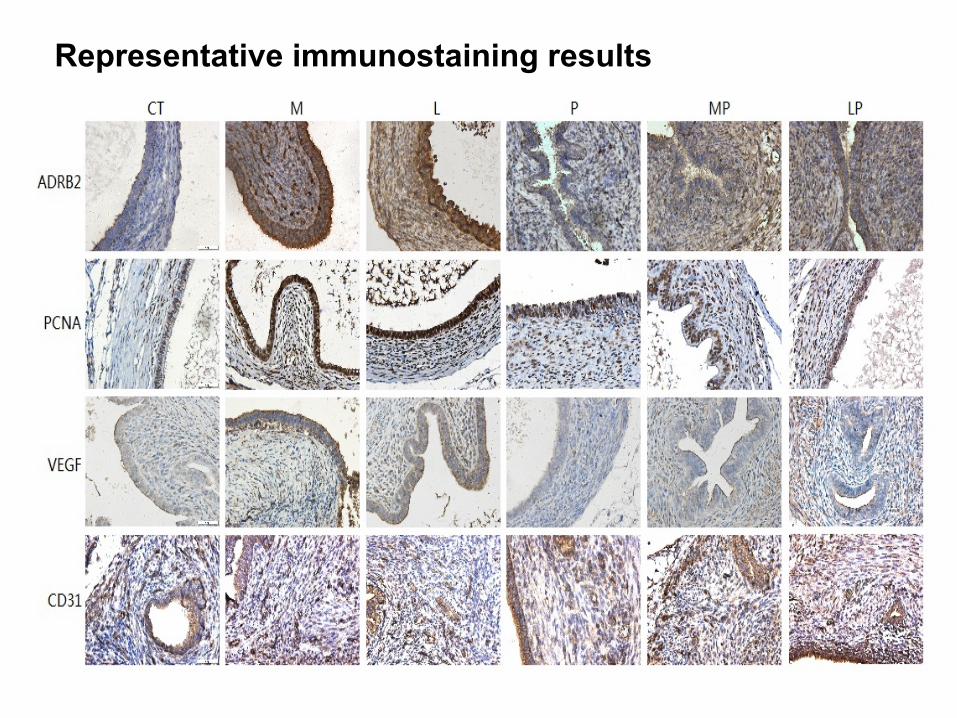
Representative immunostaining results
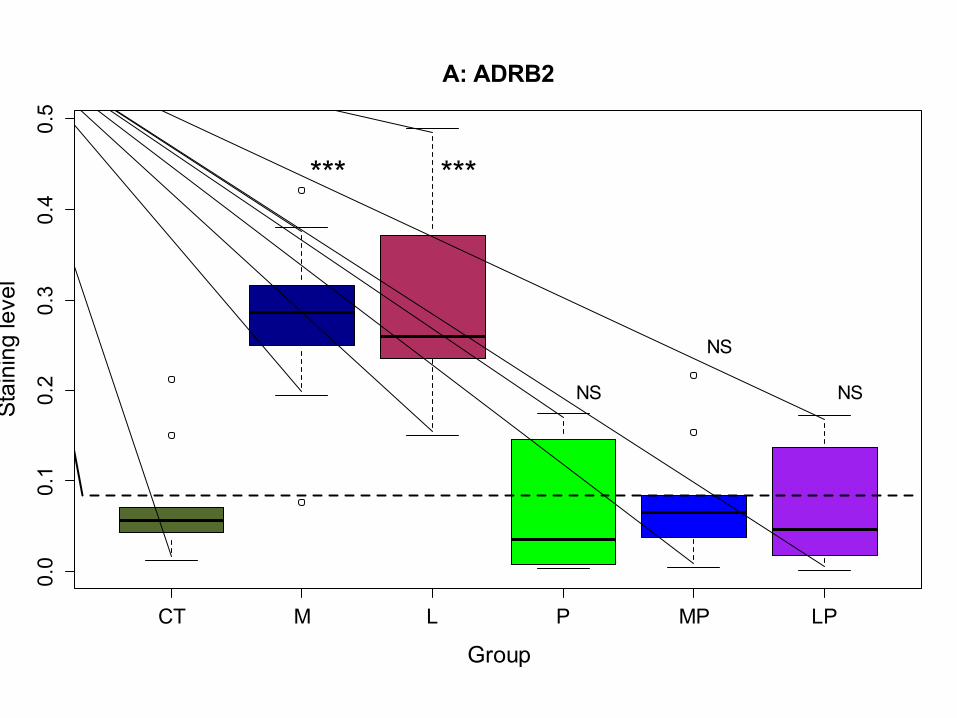
CT M L P MP LP
0.0
0.1
0.2
0.3
0.4
0.5
A: ADRB2
Group
Stai
ning
leve
l
*** ***
NS
NS
NS
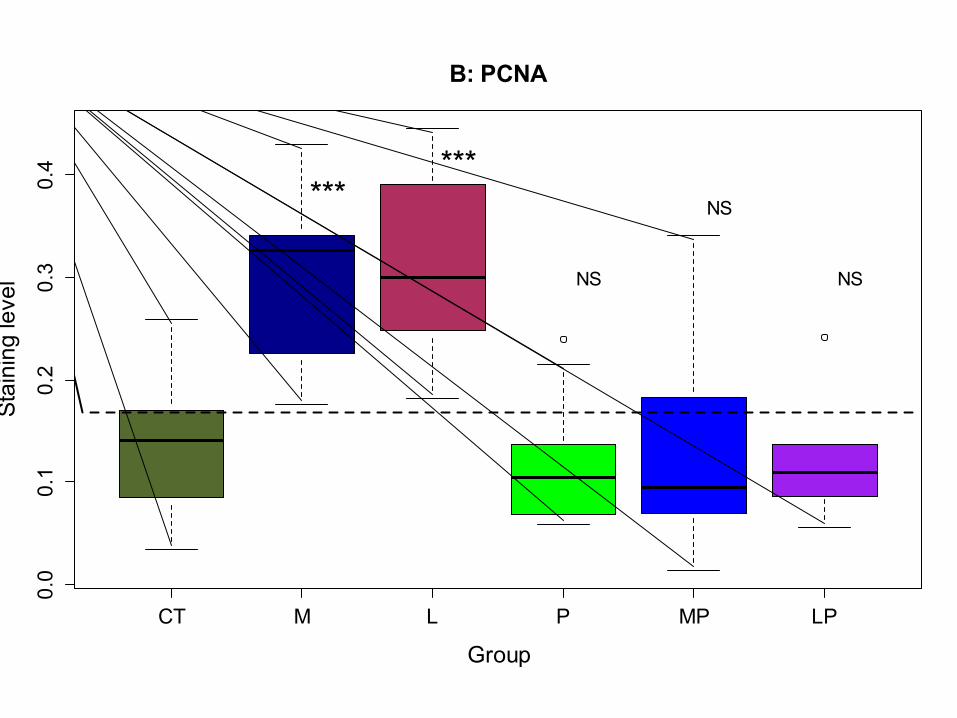
CT M L P MP LP
0.0
0.1
0.2
0.3
0.4
B: PCNA
Group
Stai
ning
leve
l
******
NS
NS
NS

CT M L P MP LP
0.00
0.05
0.10
0.15
C: VEGF
Group
Stai
ning
leve
l
*NS
NS
NS
NS
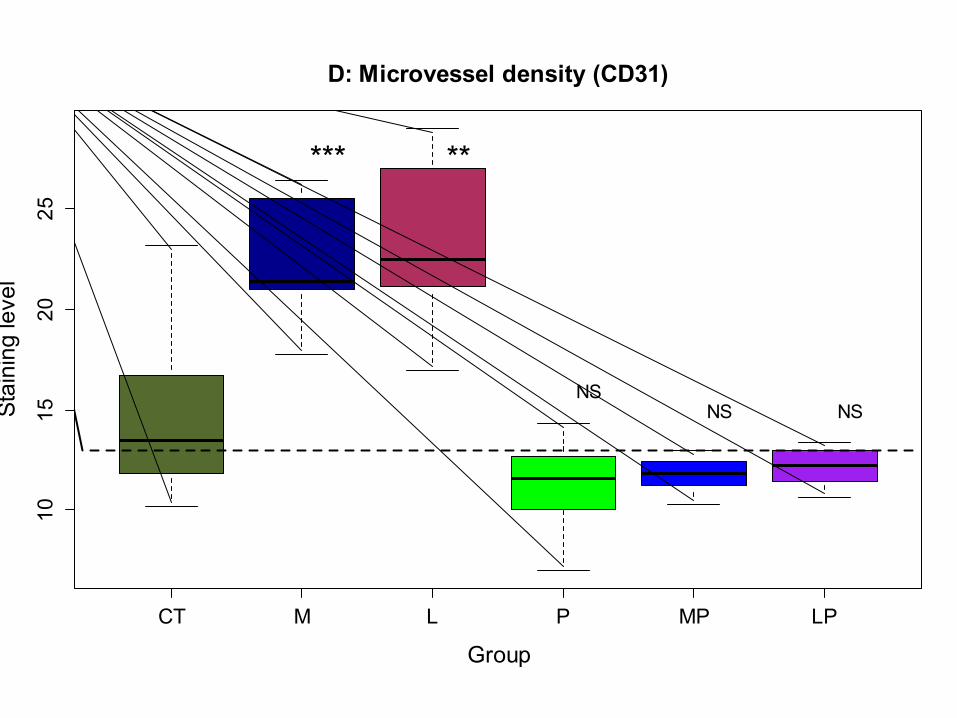
CT M L P MP LP
1015
2025
D: Microvessel density (CD31)
Group
Stai
ning
leve
l
*** **
NSNS NS

CT M L P MP LP
0.05
0.10
0.15
0.20
0.25
F: ADRA1
Group
Stai
ning
leve
l
NS NS NS NS NS

CT M L P MP LP
0.05
0.10
0.15
0.20
0.25
G: ADRA2
Group
Stai
ning
leve
l
NS NS NS NS NS

How about humans?
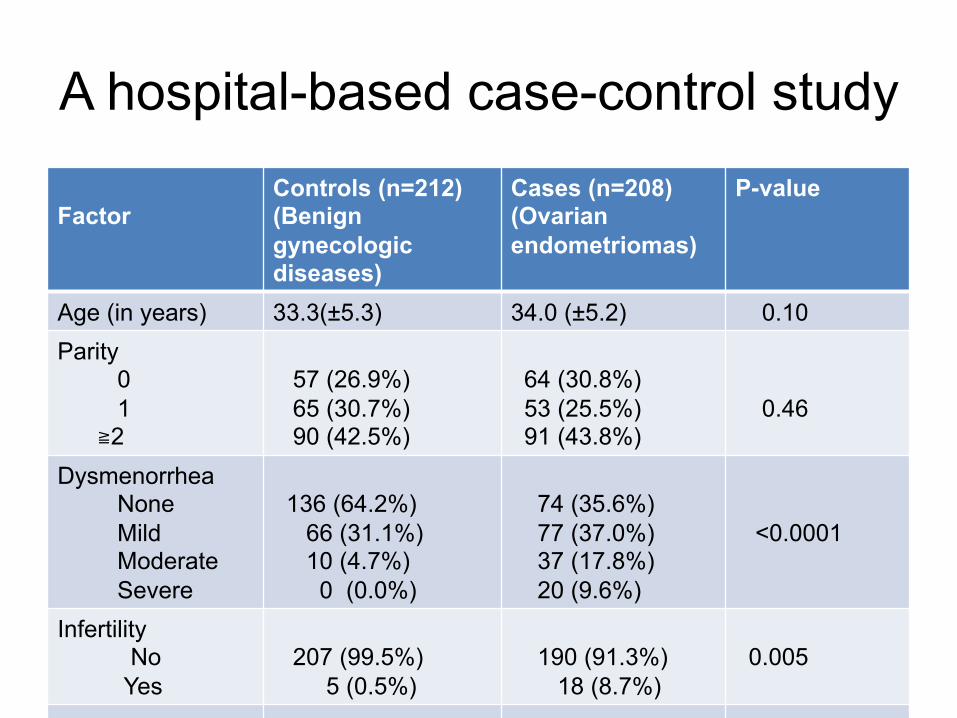
A hospital-based case-control study Factor
Controls (n=212) (Benign gynecologic diseases)
Cases (n=208) (Ovarian endometriomas)
P-value
Age (in years) 33.3(±5.3) 34.0 (±5.2) 0.10 Parity 0 1 ≧2
57 (26.9%) 65 (30.7%) 90 (42.5%)
64 (30.8%) 53 (25.5%) 91 (43.8%)
0.46
Dysmenorrhea None Mild Moderate Severe
136 (64.2%) 66 (31.1%) 10 (4.7%) 0 (0.0%)
74 (35.6%) 77 (37.0%) 37 (17.8%) 20 (9.6%)
<0.0001
Infertility No Yes
207 (99.5%) 5 (0.5%)
190 (91.3%) 18 (8.7%)
0.005
Information collected
• Demographic information – Education, marital status, occupation, OC use,
smoking status, • Reproductive history
– Gravidity, # of abortions, # of C-sections • Surgical history
– # of abdominal surgeries, # of laparoscopic surgeries,
– # of other surgeries – Total # of surgeries

Most interesting result Controls (n=212) Cases (n=208) P-value
Abdominal surgery (Post-menarche) None Once Twice
208 (98.1%) 4 (1.9%) 0 (0.0%)
197 (94.7%) 10 (4.8%) 1 (0.5%)
0.081
Crude OR=2.90 (0.84—12.89) Multivariate logistic regression indicates that OR=3.40 (1.08—10.70)
Post-menarche surgery is a risk factor for the development of endometriosis

Conclusions
• Surgery accelerates the development of endometriosis in mouse – Likely through ADRB2-mediated angiogenesis
and proliferation • Open abdominal surgery is associated
with increased risk of developing endometriosis in humans (OR=3.4 (1.08—10.70))
• β-blockade seems to be effective in abolishing the promoting effect of surgery