statement of medical necessity (smn) - genentech biooncology access solutions smn, genentech...
TRANSCRIPT

BY COMPLETING THIS FORM, I am requesting services on behalf of the patient, which may include benefits investigation, help navigating the prior authorization (PA) process and appeals support.
Insurance Information Step 2:
No Insurance
Primary insurance name:
Phone: ( ) - Subscriber name:
Subscriber/Policy ID #:
Group #:
ORAL PRODUCTS Refer Patient to Co-pay Assistance GATCF† Patient Assistance
Required field (*) ACS/062315/0110(3) 11/17
Last name*: First name*: DOB*: / / Gender: M F
Street*: City*: State*: ZIP*:
Home phone: ( ) - Work/cell: ( ) - OK to contact patient for additional information? Yes No
Patient preferred language:
Alternate contact name: Relationship: Alternate phone: ( ) -
Patient InformationStep 1:
Statement of Medical Necessity (SMN)SUBMIT SMN AND PAN FORMS ONLYPhone: (888) 249-4918 Fax: (877) 313-2659
Genentech-Access.com/BioOncology
Prescriber InformationStep 3:
Last name*: First name*:
Practice name*:
Street*: Suite #: City*: State*: ZIP*:
Prescriber tax ID #: Prescriber NPI‡ #: Group NPI #:
Office contact: Office contact phone: ( ) - Fax: ( ) -
To the highest level of specificity, provide:
Primary diagnosis code*: Has treatment started? Yes No
Date of treatment: / /
Secondary diagnosis code:
PHARMACY AND SHIPPING INFORMATION
Specialty pharmacy Yes No
Preferred specialty pharmacy:
Onsite pharmacy Yes No
Onsite pharmacy:
Ship to: Patient Practice Other:
Diagnosis CodeStep 4:
*Required field. Genentech BioOncology Access Solutions cannot process your SMN unless these fields are completed. †Genentech® Access to Care Foundation. ‡ National Provider Identifier. 1/3
Indicate the patient’s therapy*: ALECENSA® (alectinib) COTELLIC® (cobimetinib) Erivedge® (vismodegib) Tarceva® (erlotinib) ZELBORAF® (vemurafenib)
Secondary insurance name:
Phone: ( ) - Subscriber name:
Subscriber/Policy ID #:
Group #:

Sign and date here, then fax to (877) 313-2659 Prescriber’s Signature*: Date*: / /
(Original signature required. This form cannot be processed without a prescriber’s signature.)
*Required field. Genentech BioOncology® Access Solutions cannot process your SMN unless these fields are completed.
REMINDER: This form cannot be processed without a prescriber’s signature and date, as well as a signed and dated PAN form.
2/3
Unresectable/metastatic melanoma?* Yes No Other Confirmed positive for BRAF V600E?* Yes No
ZELBORAF prescription 960 mg twice a day Other: Dispense: -month supply Refill times
For ZELBORAF® (vemurafenib) patients:
PHYSICIAN CERTIFICATION: By signing below, I certify: (a) the above therapy is medically necessary, (b) I received the authorization to release the information above and other protected health information (as defined by the Health Insurance Portability and Accountability Act of 1996 [HIPAA]) to Genentech, Inc., Genentech Access Solutions, the contracted dispensing pharmacy, or other contractors for the purpose of requesting reimbursement support, assisting in initiating or continuing therapy and/or the evaluation of the patient’s eligibility for GATCF, as a break in treatment would negatively impact the patient’s therapeutic outcome and (c) I will not attempt to seek reimbursement for free product provided to the patient. I request Genentech Access Solutions convey to the pharmacy chosen by the above-named patient the prescription described herein.I agree to comply with the Genentech, Inc. program guidelines and understand that GATCF, at its sole discretion, reserves the right to modify or discontinue the program at any time and to verify the accuracy of the information submitted. I further understand that Genentech will provide vial replacement in a configuration that will create the least wastage. If applying for GATCF, I certify that (a) this patient has no medical insurance coverage or otherwise meets the financial criteria for the prescribed therapy, and is not eligible for other product financial support programs, and (b) the therapy identified above will not be used in a clinical trial. Note: Prescribers in all states must follow applicable law for a valid prescription and who is considered an authorized prescriber. For prescribers in states with official prescription form requirements, such as New York, please submit prescriptions on an official state prescription blank along with this form.Unapproved Use Warning: Please read the FDA-approved label for Genentech products before prescribing. If the indication for which you are prescribing a Genentech product is not listed in the FDA-approved label, you are prescribing the medication for an “unapproved” use, meaning that the FDA has not approved the efficacy, dosage amount or safety of this medication when used for such a use. Nevertheless, GATCF will consider providing the medication for your patient with this admonition, based upon your medical order, within program requirements.
Sign and Date FormStep 6:
Prescription Information for PatientStep 5:
Required field (*)
Last name*: First name*: DOB*: / /
For ALECENSA® (alectinib) patients:
Metastatic non-small cell lung cancer (NSCLC)?* Yes NoConfirmed positive for anaplastic lymphoma kinase (ALK)?* Yes No
ALECENSA prescription 600 mg twice daily Other: Dispense: -month supply Refill times
ALECENSA SureStart® free starter supply 600 mg twice daily Dispense: 1-month supply Refill times
For Tarceva® (erlotinib) patients:
Treatment of patients with metastatic non-small cell lung cancer (NSCLC) whose tumors have epidermal growth factor receptor (EGFR) exon 19 deletions or exon 21 (L858R) substitution mutations?* Yes No Advanced pancreatic cancer and have not received chemotherapy?* Yes No
Tarceva prescription 150 mg daily 100 mg daily Other: mg daily Dispense: -month supply Refill times
For COTELLIC® (cobimetinib) patients:
Unresectable/metastatic melanoma?* Yes No Used in combination with ZELBORAF® (vemurafenib)?* Yes No (If yes, complete ZELBORAF section below.)Confirmed positive for: BRAF V600E?* Yes No BRAF V600K?* Yes No
COTELLIC prescription 60 mg daily for 21 consecutive days on, followed by a 7-day rest period Other: Dispense: -month supply Refill times
Metastatic basal cell carcinoma?* Yes NoLocally advanced basal cell carcinoma recurred following surgery, or not a candidate for surgery, and not a candidate for radiation?* Yes No
Erivedge prescription 150 mg daily Other: Dispense: -month supply Refill times
For Erivedge® (vismodegib) patients:
Tarceva SureStart® free starter supply 150 mg daily 100 mg dailyDispense: 15-day supply Refill times
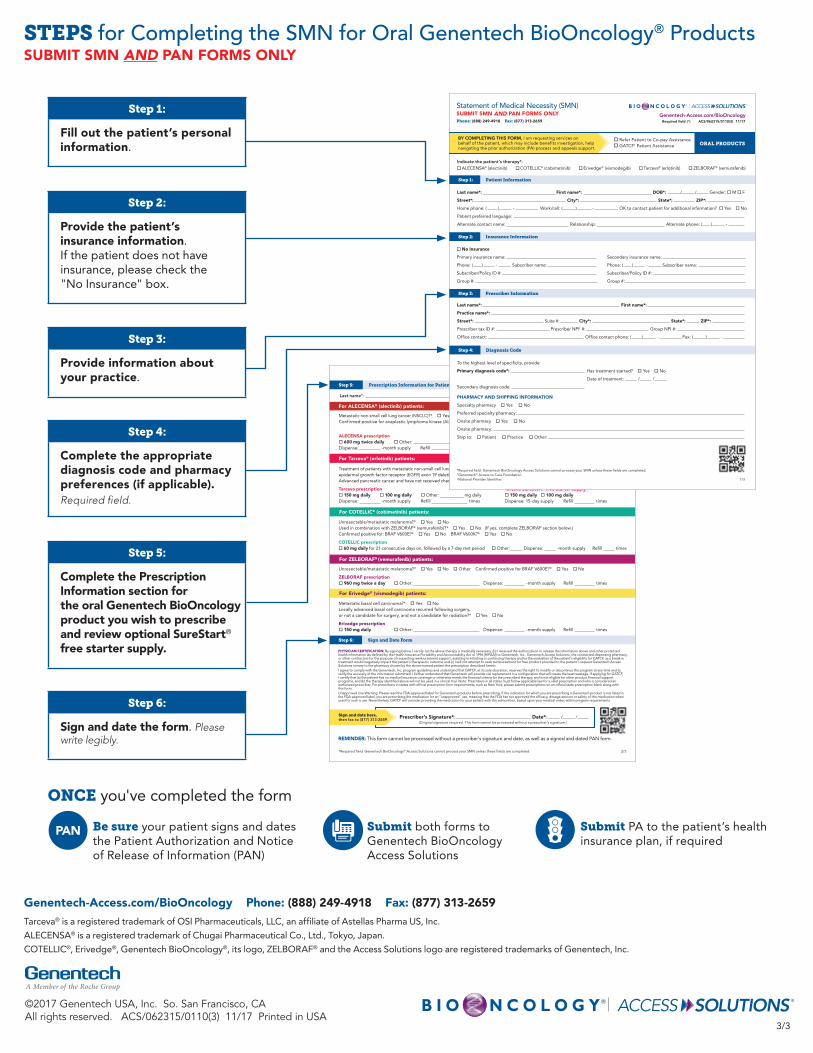
ONCE you've completed the form
Be sure your patient signs and dates the Patient Authorization and Notice of Release of Information (PAN)
Submit both forms to Genentech BioOncology Access Solutions
Submit PA to the patient’s health insurance plan, if required
Sign and date here, then fax to (877) 313-2659 Prescriber’s Signature*: Date*: / /
(Original signature required. This form cannot be processed without a prescriber’s signature.)
*Required field. Genentech BioOncology® Access Solutions cannot process your SMN unless these fields are completed.
REMINDER: This form cannot be processed without a prescriber’s signature and date, as well as a signed and dated PAN form.
2/3
Unresectable/metastatic melanoma?* Yes No Other Confirmed positive for BRAF V600E?* Yes No
ZELBORAF prescription 960 mg twice a day Other: Dispense: -month supply Refill times
For ZELBORAF® (vemurafenib) patients:
PHYSICIAN CERTIFICATION: By signing below, I certify: (a) the above therapy is medically necessary, (b) I received the authorization to release the information above and other protected health information (as defined by the Health Insurance Portability and Accountability Act of 1996 [HIPAA]) to Genentech, Inc., Genentech Access Solutions, the contracted dispensing pharmacy, or other contractors for the purpose of requesting reimbursement support, assisting in initiating or continuing therapy and/or the evaluation of the patient’s eligibility for GATCF, as a break in treatment would negatively impact the patient’s therapeutic outcome and (c) I will not attempt to seek reimbursement for free product provided to the patient. I request Genentech Access Solutions convey to the pharmacy chosen by the above-named patient the prescription described herein.I agree to comply with the Genentech, Inc. program guidelines and understand that GATCF, at its sole discretion, reserves the right to modify or discontinue the program at any time and to verify the accuracy of the information submitted. I further understand that Genentech will provide vial replacement in a configuration that will create the least wastage. If applying for GATCF, I certify that (a) this patient has no medical insurance coverage or otherwise meets the financial criteria for the prescribed therapy, and is not eligible for other product financial support programs, and (b) the therapy identified above will not be used in a clinical trial. Note: Prescribers in all states must follow applicable law for a valid prescription and who is considered an authorized prescriber. For prescribers in states with official prescription form requirements, such as New York, please submit prescriptions on an official state prescription blank along with this form.Unapproved Use Warning: Please read the FDA-approved label for Genentech products before prescribing. If the indication for which you are prescribing a Genentech product is not listed in the FDA-approved label, you are prescribing the medication for an “unapproved” use, meaning that the FDA has not approved the efficacy, dosage amount or safety of this medication when used for such a use. Nevertheless, GATCF will consider providing the medication for your patient with this admonition, based upon your medical order, within program requirements.
Sign and Date FormStep 6:
Prescription Information for PatientStep 5:
Required field (*)
Last name*: First name*: DOB*: / /
For ALECENSA® (alectinib) patients:
Metastatic non-small cell lung cancer (NSCLC)?* Yes NoConfirmed positive for anaplastic lymphoma kinase (ALK)?* Yes No
ALECENSA prescription 600 mg twice daily Other: Dispense: -month supply Refill times
ALECENSA SureStart® free starter supply 600 mg twice daily Dispense: 1-month supply Refill times
For Tarceva® (erlotinib) patients:
Treatment of patients with metastatic non-small cell lung cancer (NSCLC) whose tumors have epidermal growth factor receptor (EGFR) exon 19 deletions or exon 21 (L858R) substitution mutations?* Yes No Advanced pancreatic cancer and have not received chemotherapy?* Yes No
Tarceva prescription 150 mg daily 100 mg daily Other: mg daily Dispense: -month supply Refill times
For COTELLIC® (cobimetinib) patients:
Unresectable/metastatic melanoma?* Yes No Used in combination with ZELBORAF® (vemurafenib)?* Yes No (If yes, complete ZELBORAF section below.)Confirmed positive for: BRAF V600E?* Yes No BRAF V600K?* Yes No
COTELLIC prescription 60 mg daily for 21 consecutive days on, followed by a 7-day rest period Other: Dispense: -month supply Refill times
Metastatic basal cell carcinoma?* Yes NoLocally advanced basal cell carcinoma recurred following surgery, or not a candidate for surgery, and not a candidate for radiation?* Yes No
Erivedge prescription 150 mg daily Other: Dispense: -month supply Refill times
For Erivedge® (vismodegib) patients:
Tarceva SureStart® free starter supply 150 mg daily 100 mg dailyDispense: 15-day supply Refill times
STEPS for Completing the SMN for Oral Genentech BioOncology® ProductsSUBMIT SMN AND PAN FORMS ONLY
3/3
Genentech-Access.com/BioOncology Phone: (888) 249-4918 Fax: (877) 313-2659Tarceva® is a registered trademark of OSI Pharmaceuticals, LLC, an affiliate of Astellas Pharma US, Inc.
ALECENSA® is a registered trademark of Chugai Pharmaceutical Co., Ltd., Tokyo, Japan.
COTELLIC®, Erivedge®, Genentech BioOncology®, its logo, ZELBORAF® and the Access Solutions logo are registered trademarks of Genentech, Inc.
©2017 Genentech USA, Inc. So. San Francisco, CA All rights reserved. ACS/062315/0110(3) 11/17 Printed in USA
Step 1:
Fill out the patient’s personal information.
Step 2:
Provide the patient’s insurance information. If the patient does not have insurance, please check the "No Insurance" box.
Step 4:
Complete the appropriate diagnosis code and pharmacy preferences (if applicable). Required field.
Step 3:
Provide information about your practice.
Step 5:
Complete the Prescription Information section for the oral Genentech BioOncology product you wish to prescribe and review optional SureStart® free starter supply.
Step 6:
Sign and date the form. Please write legibly.
BY COMPLETING THIS FORM, I am requesting services on behalf of the patient, which may include benefits investigation, help navigating the prior authorization (PA) process and appeals support.
Insurance Information Step 2:
No Insurance
Primary insurance name:
Phone: ( ) - Subscriber name:
Subscriber/Policy ID #:
Group #:
ORAL PRODUCTS Refer Patient to Co-pay Assistance GATCF† Patient Assistance
Required field (*) ACS/062315/0110(3) 11/17
Last name*: First name*: DOB*: / / Gender: M F
Street*: City*: State*: ZIP*:
Home phone: ( ) - Work/cell: ( ) - OK to contact patient for additional information? Yes No
Patient preferred language:
Alternate contact name: Relationship: Alternate phone: ( ) -
Patient InformationStep 1:
Statement of Medical Necessity (SMN)SUBMIT SMN AND PAN FORMS ONLYPhone: (888) 249-4918 Fax: (877) 313-2659
Genentech-Access.com/BioOncology
Prescriber InformationStep 3:
Last name*: First name*:
Practice name*:
Street*: Suite #: City*: State*: ZIP*:
Prescriber tax ID #: Prescriber NPI‡ #: Group NPI #:
Office contact: Office contact phone: ( ) - Fax: ( ) -
To the highest level of specificity, provide:
Primary diagnosis code*: Has treatment started? Yes No
Date of treatment: / /
Secondary diagnosis code:
PHARMACY AND SHIPPING INFORMATION
Specialty pharmacy Yes No
Preferred specialty pharmacy:
Onsite pharmacy Yes No
Onsite pharmacy:
Ship to: Patient Practice Other:
Diagnosis CodeStep 4:
*Required field. Genentech BioOncology Access Solutions cannot process your SMN unless these fields are completed. †Genentech® Access to Care Foundation. ‡ National Provider Identifier. 1/3
Indicate the patient’s therapy*: ALECENSA® (alectinib) COTELLIC® (cobimetinib) Erivedge® (vismodegib) Tarceva® (erlotinib) ZELBORAF® (vemurafenib)
Secondary insurance name:
Phone: ( ) - Subscriber name:
Subscriber/Policy ID #:
Group #: