should we admit these patients to the icu? triage ... 9/02_sepsis in... · should we admit these...
TRANSCRIPT

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
Should we admit these patients to the ICU? Triage, boundaries and outcomes
Filomena Faria| [email protected]
Serviço de Cuidados Intensivos, IPO Porto FG EPE
1

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
Topics:
#1 Introduction;
#2 Epidemiology;
#3 Triage;
#4 Boundaries;
#5 Outcomes;
#6 Take home message.
2

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
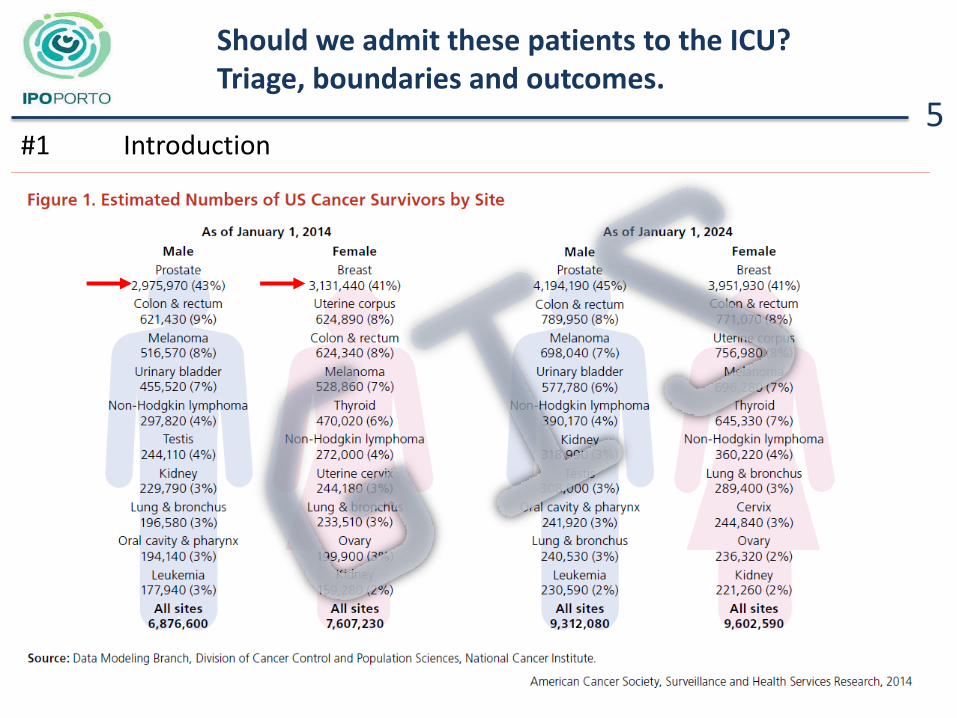
#1 Introduction
→ It is common belief that “cancer patients in the Intensive Care Unit (ICU) have a bad outcome”.
→More patients are admitted in the ICU, due to previous complications (co-morbidities) or chemotherapy /radiotherapy/surgery side effects.
→ Lack of solid prognostic factors -empirical clinical decisions.
→ Cancer patients are a very heterogeneous population.
3
Cancer Facts & Figures 2011: American Cancer Society.

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
→ IPO Porto’s ICU - April, 1995 / 2015;
→ Oncological disease change of paradigm:
- Acute disease (tumoral lysis syndrome, airway obstruction), needing of a multidisciplinary approach;
- Acute on chronic disease;
- Sub-clinical sequel of cancer treatment (chemo brain).
All need a multidisciplinary approach
#1 Introduction 4
Should we admit these patients to the ICU? Triage, boundaries and outcomes.
#1 Introduction 5

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
6 #2 Epidemiology
→ Infection is an important complication in cancer patients … there is no national estimate on the magnitude of this problem.
→ 16.4 cases / 1000 people with cancer/ year;
→ The in-hospital mortality for cancer patients with severe sepsis was 37,8% (relative risk , 2.77);
→ Overall, severe sepsis is associated with 8.5% of all cancer deaths at a cost of $3.4 billion per year.
→ Severe Sepsis is a common, deadly, and costly complication in
cancer patients.

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
7
Septic LOS APACHE SAPS ICU Hospital
Patients days II II survival survival
Nº mean mean mean
Hematological 175 11 26 59 45.7% 45.1%
(Nº Patients) (80) (79)
Solid Tumours 461 11 25 56 71.8% 67,6
(Nº Patients) (331) (312)
Without Tumours 2 8 36 68 50,0% 50,0%
(Nº Patients) (1) (1)
→ Should we admit these patients to the ICU? Yes… of course. → 2010 – 2015: 1710 ICU admissions and 638 of them due to sépsis.
#2 Epidemiology

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
8
Septic
SV IV NIV IV
Patients + NIV
Hematological 175 22 99 11 43 ICU survival 100,0% 33,3% 90,9% 34,9%
(Nº Patients) (22) (33) (10) (15) Hospital survival 100,0% 28,3% 90,9% 34,9%
(Nº Patients) (22) (28) (10) (15) Solid Tumours 461 49 338 24 50
ICU survival 95,9% 68,9% 79,2% 64,0% (Nº Patients) (47) (233) (19) (32)
Hospital survival 93,9% 64,2% 70,8% 64,0% (Nº Patients) (46) (217) (17) (32)
Without Tumours 2 0 2 0 0 ICU survival 50,0%
(Nº Patients) (1) Hospital survival 50,0%
(Nº Patients) (1)
→ Survival and ventilation: Invasive Ventilation/Non Invasive Ventilation

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
#3 Triage
9

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
10 #3 Triage
Should we admit these patients to the ICU? Triage, boundaries and outcomes.
11 #3 Triage
Should we admit these patients to the ICU? Triage, boundaries and outcomes.
12
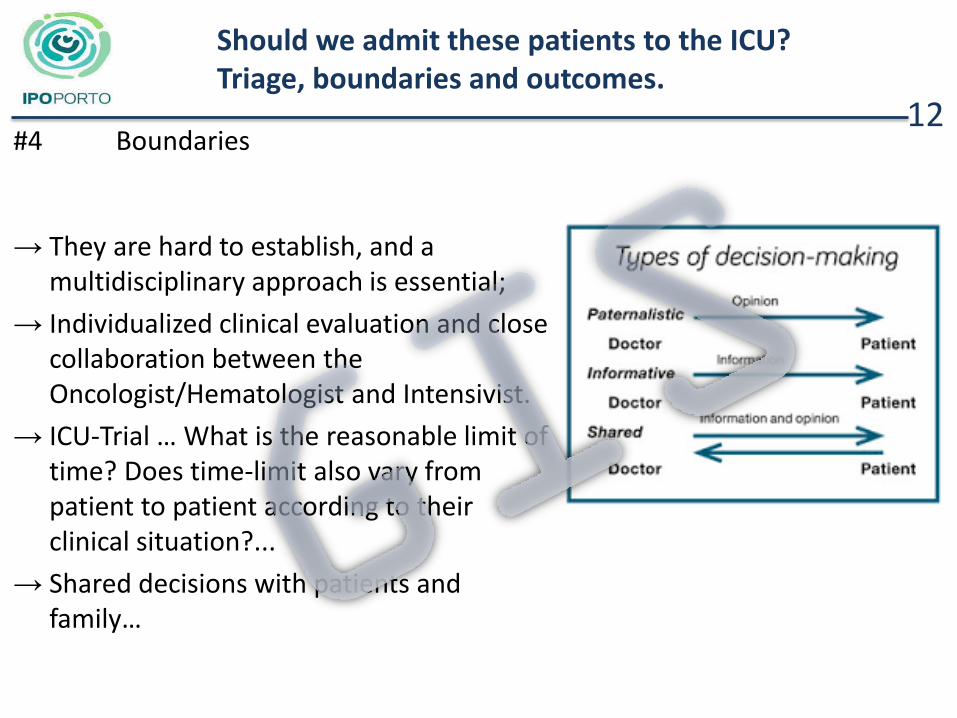
→ They are hard to establish, and a multidisciplinary approach is essential;
→ Individualized clinical evaluation and close collaboration between the Oncologist/Hematologist and Intensivist.
→ ICU-Trial … What is the reasonable limit of time? Does time-limit also vary from patient to patient according to their clinical situation?...
→ Shared decisions with patients and family…
#4 Boundaries

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
13 #4 Boundaries – Clinical case 1
→ Male, 69 years old, ECOG 0 with retroperitoneal high degree stage III liposarcoma (pT2bN0M0), underwent surgery and radiotherapy that ended seven months ago (patient had refused chemotherapy).
→ Admited twenty-four hours before due to urinary sepsis, anuric and acidemia;
→ US: left hydronephrosis, with peri-renal fluid; ascites and liver with
space occupying lesions (liver mts?); → Oncologist suggested ICU-Trial (re-evaluation after 3 days). → Clinical situation discussed with the family.

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
14 #4 Boundaries – Clinical case 1
→ Admission: Urinary septic shock
- Broad-spectrum antibiotherapy, invasive ventilation, vasopressor support and dialysis.
- Left kidney nefrostomy with
drainage of bleary urine.
- Ascites drainage (hematic, no malignant cells)…
- Liver biopsy.

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
15 #4 Boundaries – Clinical case 1
→ Good clinical evolution, with the suspension of vasopressors and extubation after 72 hours;
→ Discharged from the ICU on the fifth day, but still in need of dialysis.. → Liver biopsy: hepatic infiltration by adenocarcinome (unknown primary
– Digestive?) → UEndoscopy: no evidence of lesions.
→ Died on the fifteenth day of admission with palliative care.

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
16 #4 Boundaries – Clinical case 2
→ Male, 25 years old, with ALL-T on the 1st cycle of chemotherapy.
→ Prolonged hospital inpatient, with multiple complications from CT: - Severe cachexy (loss of 20 Kg since admission). - Vincristine dysautonomy. - Mucositis and colitis, with multiple episodes of low digestive
hemorrhage, leading to the need of a left colectomy extended to the transverse colon and a right derivative colostomy.

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
17 #4 Bondaries – Clinical case 2
→ Admission: Sepsis following nosocomial pneumonia, Klebsiella Pneumoniae, after the 47th day of CT.
₋ Broad-spectrum antibiotherapy; ₋ Mechanical invasive ventilation; ₋ Multiple episodes of low digestive
hemorrhage, through the colostomy;
₋ Colonoscopy with placement of hemostatic endoclips, with the confirmation of flat ulcers of the colic mucosa.

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
18 #4 Bondaries – Clinical case 2
→ Clinical evolution was slow, but good.
→ Extubated on the 8th day, to non-invasive ventilation.
→ Discharged from the ICU on the 15th day.
→ Discharged from the hospital after 2 months.
→ Later restarted chemotherapy.
→ Colostomy closed after a year.
→ 2 years follow-up: ECOG 0, active life.
Should we admit these patients to the ICU? Triage, boundaries and outcomes.
19
→Male, 62 years-old, with primary mielofibrosis, on the 6th month after Allo-HSCT;
→ Digestive GVHD with histological confirmation: Imunosuppressors with prednisolone, mofetil mycophenolate and cyclosporine;
→ Iatrogenic diabetes.
→ Admission to Hospital: hyperthermia, alterations of conscience state and right hemiparesis;
#4 Boundaries – Clinical Case 3

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
20
→ Admission: CNS Sepsis.
- Starts broad-spectrum antibiotherapy.
- Invasive mechanical ventilation.
- Brain CT.
- LP (bleary liquid with LDH of 54 U/L, Glicose of 4,1 mmol/L, Proteins 2961,8 mg/L, Chlorides of 124 mmol/L; nucleated elements 247/ mmc com predominio de PMN).
- Brain MRI (encephalitis)
# Boundaries – Clinical Case 3

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
21
→ Good clinical evolution, with antibiotic de-escalation on the 4th day (Listeria monocytogenes meningoencephalitis)
→ Extubated on the 9th day;
→ Discharged from the ICU on the 10th day.
→ Discharged from the hospital on the 65th day.
→ 18 months follow-up: ECOG 1, program of physiotherapy.
#4 Boundaries – Clinical Case 3

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
22 #5 Outcomes
Should we admit these patients to the ICU? Triage, boundaries and outcomes.
#5 Outcomes 23

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
24 #5 Outcomes

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
25 #5 Outcomes
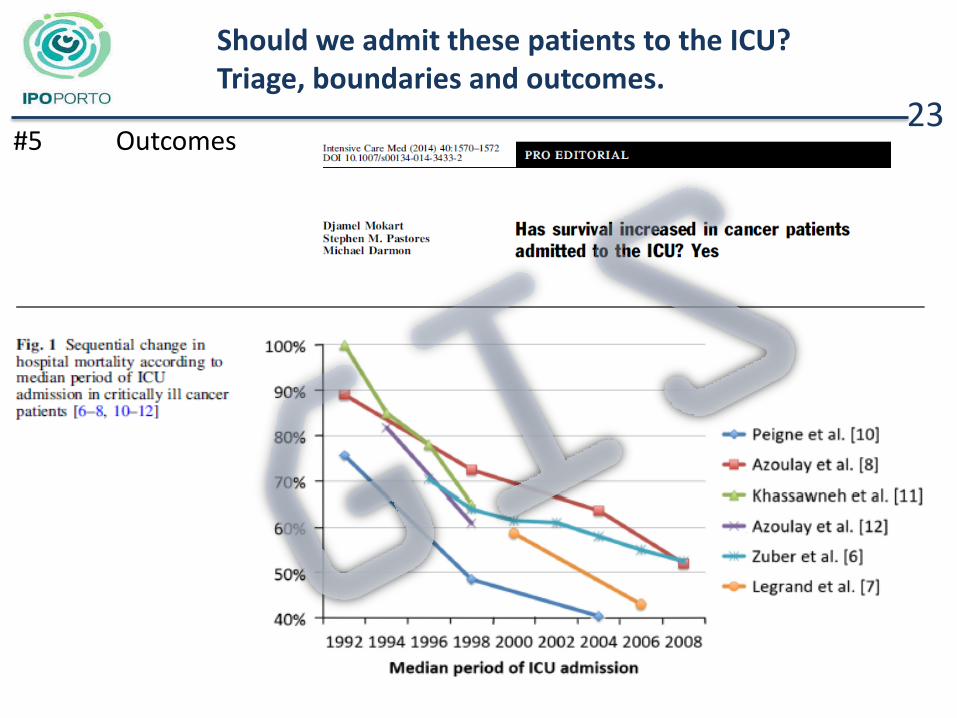
→ Advances in oncology have led to a dramatic reduction in mortality rates;
→More complex and intensive cytotoxic and immunosuppressive regimens, in addition to major surgical procedures in patients who would have previously received palliative care, are being done.
→ Poorer performance status, sepsis, mechanical ventilation, use of vasopressors, increased the risk of both ICU and in-hospital mortality.

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
26 #5 Outcomes
→ The impact of cancer stage has been inconsistently associated with mortality.
→ Research is needed to describe whether cancer patients are likely to receive planned anti-cancer therapy after discharge from ICU.
→ Primary research is still needed to describe outcomes in cancer patients with sufficient case mix and treatments details to be of prognostic value to clinicians.
Should we admit these patients to the ICU? Triage, boundaries and outcomes.
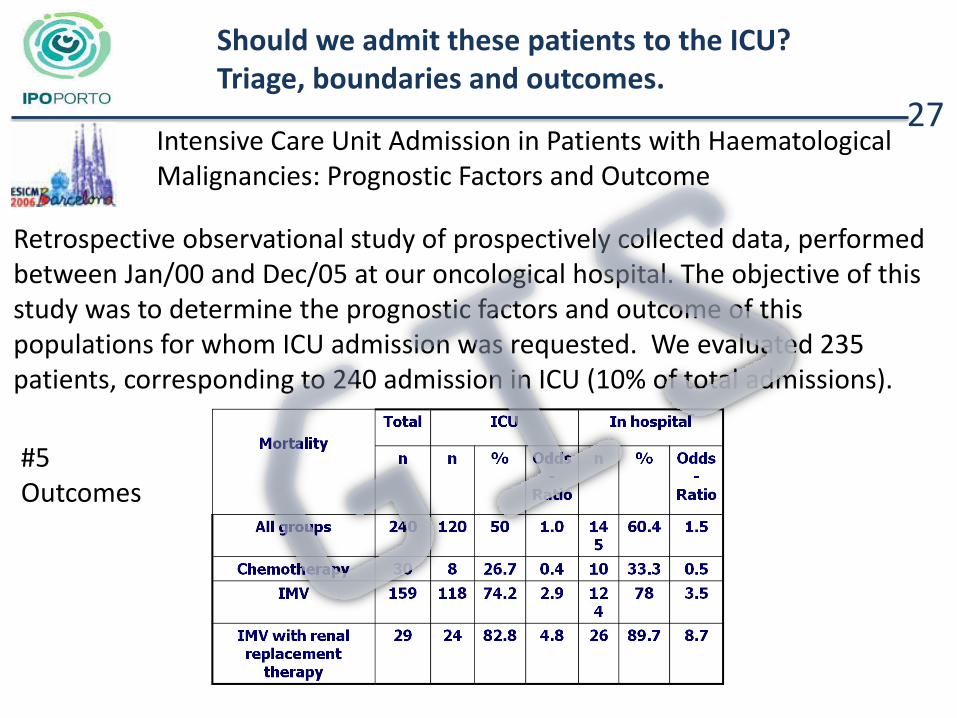
Retrospective observational study of prospectively collected data, performed between Jan/00 and Dec/05 at our oncological hospital. The objective of this study was to determine the prognostic factors and outcome of this populations for whom ICU admission was requested. We evaluated 235 patients, corresponding to 240 admission in ICU (10% of total admissions).
Intensive Care Unit Admission in Patients with Haematological Malignancies: Prognostic Factors and Outcome
27
#5 Outcomes
Should we admit these patients to the ICU? Triage, boundaries and outcomes.
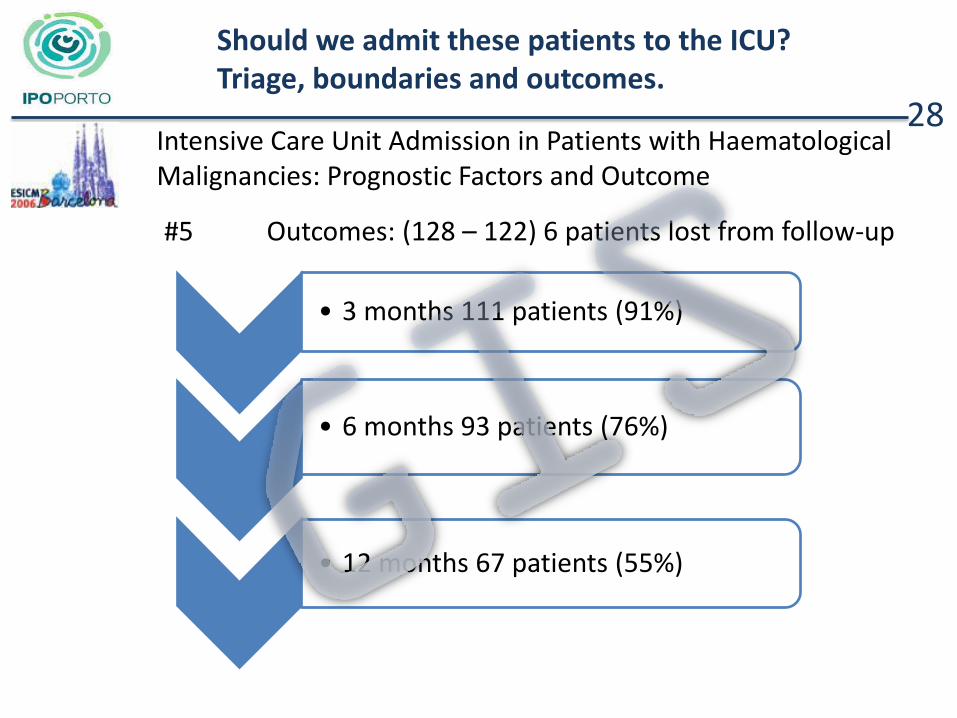
#5 Outcomes: (128 – 122) 6 patients lost from follow-up
Intensive Care Unit Admission in Patients with Haematological Malignancies: Prognostic Factors and Outcome
28
• 3 months 111 patients (91%)
• 6 months 93 patients (76%)
• 12 months 67 patients (55%)

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
Patients with severe sepsis and solid tumours
29
→ Objective is evaluate the outcome and prognostic factors in a group of patients with severe sepsis and solid tumours.
→ 91.4% of patients required mechanical ventilation, 42% vasopressors, and kidney replacement therapy in 4%.
→ Decisions to forgo (withhold or withdrawn) life-sustaining
therapies were taken in 19% patients.
→ In the patients with the intention to treat the ICU and hospital survival rates were 76.5% and 56.3 %.
→ Survival rate at 3, 6 and 12 months were 97%, 81% and 45% respectively.
#5 Outcomes

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
→ The challenge facing ICU physicians is to identify which cancer patients are likely to benefit from ICU care.
→ Specialized skills by Intensivists and
close collaboration between the Intensivists and Oncologists/Hematologists, will improve the outcome.
→ Individual decisions, must consider the
patient’s will, co-morbidities and cancer prognosis.
→ ICU Trial… Time evaluation… Clinical
criteria…
30 #6 Take home messages

Should we admit these patients to the ICU? Triage, boundaries and outcomes.
31