should integrase inhibitors be your first choice when starting hiv therapy- expert faculty debate...
TRANSCRIPT
Joseph J. Eron, Jr., MDUniversity of North CarolinaChapel Hill, North Carolina
Daniel R. Kuritzkes, MDBrigham and Women’s HospitalHarvard Medical SchoolBoston, Massachusetts
Should Integrase Inhibitors Be Your First Choice When Starting HIV Therapy? Expert Faculty Debate the Evidence
This activity is supported by an educational grant from ViiV
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
About These Slides
Users are encouraged to use these slides in their own noncommercial presentations, but we ask that content and attribution not be changed. Users are asked to honor this intent
These slides may not be published or posted online without permission from Clinical Care Options (email [email protected])
DisclaimerThe materials published on the Clinical Care Options Web site reflect the views of the authors of the CCO material, not those of Clinical Care Options, LLC, the CME providers, or the companies providing educational grants. The materials may discuss uses and dosages for therapeutic products that have not been approved by the United States Food and Drug Administration. A qualified healthcare professional should be consulted before using any therapeutic product discussed. Readers should verify all information and data before treating patients or using any therapies described in these materials.
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Program Director
Joseph J. Eron, Jr., MD Professor of Medicine and EpidemiologyUniversity of North Carolina School of MedicineDirector, AIDS Clinical Trials UnitUniversity of North CarolinaChapel Hill, North Carolina
Faculty
Daniel R. Kuritzkes, MDChief, Division of Infectious DiseasesBrigham and Women’s HospitalProfessor of MedicineHarvard Medical SchoolBoston, Massachusetts
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Additional Faculty Contributing to Content
Eric S. Daar, MDChief, Division of HIV MedicineHarbor-UCLA Medical CenterProfessor of MedicineDavid Geffen School of Medicine at UCLALos Angeles, California
Sally Hodder, MDDirector, Clinical Translation Science InstituteProfessor of MedicineWest Virginia UniversityMorgantown, West Virginia
Kathleen E. Squires, MDW. Paul and Ida H. Havens Professor of Infectious DiseasesDirector, Division of Infectious DiseasesSidney Kimmel Medical College of Thomas Jefferson UniversityPhiladelphia, Pennsylvania
Introduction to the Use of Integrase Inhibitor–Based
Regimens in First-line Therapy
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
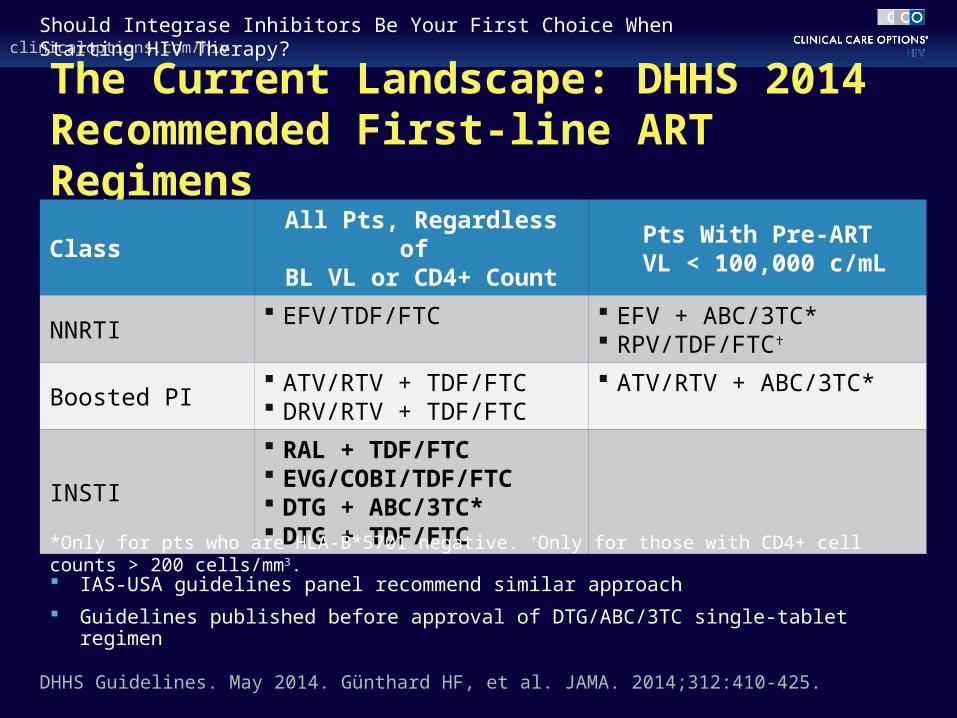
The Current Landscape: DHHS 2014 Recommended First-line ART Regimens
IAS-USA guidelines panel recommend similar approach
Guidelines published before approval of DTG/ABC/3TC single-tablet regimen
DHHS Guidelines. May 2014. Günthard HF, et al. JAMA. 2014;312:410-425.
ClassAll Pts, Regardless of BL VL or CD4+ Count
Pts With Pre-ART VL < 100,000 c/mL
NNRTI EFV/TDF/FTC EFV + ABC/3TC*
RPV/TDF/FTC
Boosted PI ATV/RTV + TDF/FTC DRV/RTV + TDF/FTC
ATV/RTV + ABC/3TC*
INSTI
RAL + TDF/FTC EVG/COBI/TDF/FTC DTG + ABC/3TC* DTG + TDF/FTC
*Only for pts who are HLA-B*5701 negative. Only for those with CD4+ cell counts > 200 cells/mm3.

Daniel R. Kuritzkes, MDChief, Division of Infectious DiseasesBrigham and Women’s HospitalProfessor of MedicineHarvard Medical SchoolBoston, Massachusetts
Current Evidence on Integrase Inhibitors in First-line Therapy

Raltegravir
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
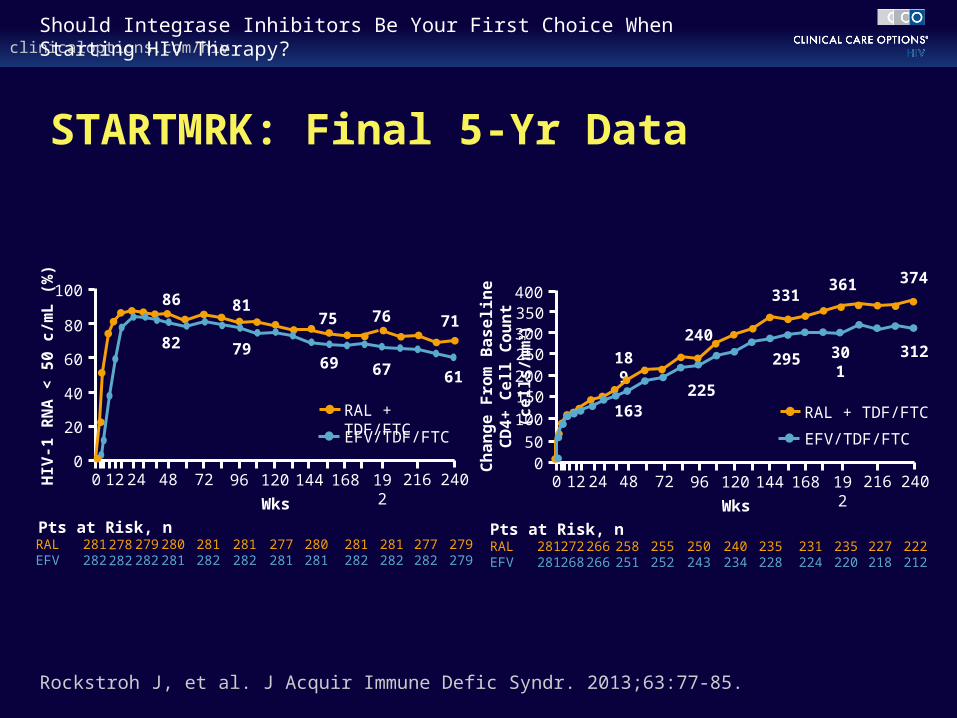
STARTMRK: Final 5-Yr Data
Rockstroh J, et al. J Acquir Immune Defic Syndr. 2013;63:77-85.
281282
100
80
60
40
20
0 HIV
-1 R
NA
< 5
0 c
/mL
(%
)
0 48 72 96 120 144
Wks
RALEFV
Pts at Risk, n281282
278282
280281
281282
277281
280281
86
82
81
79
75
69
281282
192
76
67
24012 216
71
61
277282
279279
24
279282
168
281282
RAL + TDF/FTC
EFV/TDF/FTC
250243
400
300
200
100
500 C
ha
ng
e F
rom
Ba
se
lin
e
CD
4+
Ce
ll C
ou
nt
(ce
lls
/mm
3)
0 48 72 96 120 144
Wks
RALEFV
Pts at Risk, n281281
272268
258251
255252
240234
235228
189
163
240
225
331
295
235220
192
361
301
24012 216
374
312
227218
222212
24
266266
168
231224
RAL + TDF/FTC
EFV/TDF/FTC
350
250
150
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
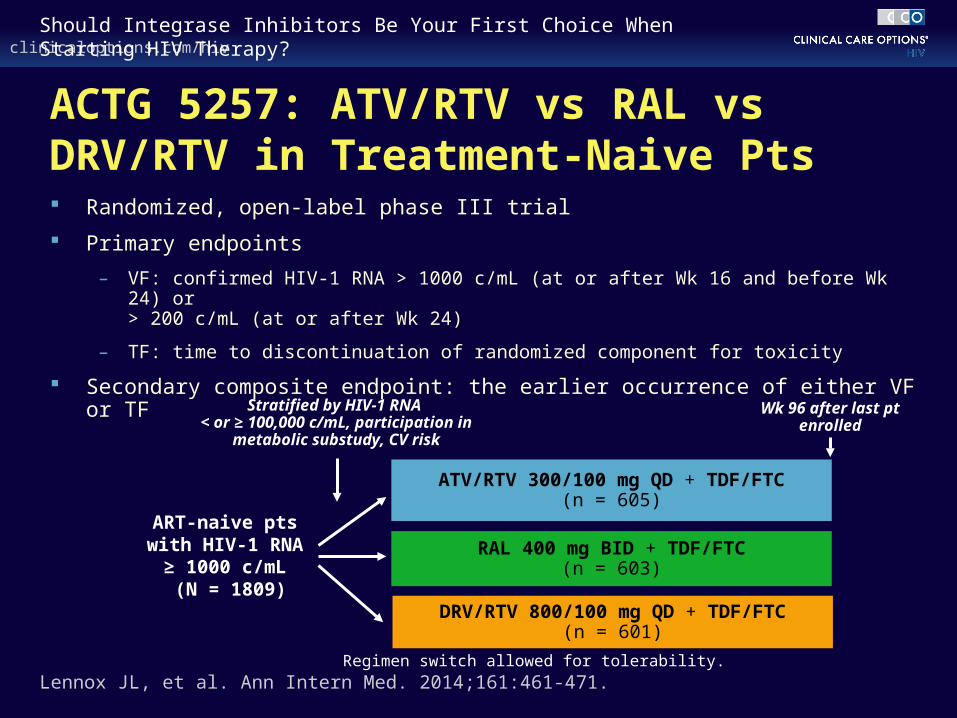
ACTG 5257: ATV/RTV vs RAL vs DRV/RTV in Treatment-Naive Pts Randomized, open-label phase III trial
Primary endpoints
– VF: confirmed HIV-1 RNA > 1000 c/mL (at or after Wk 16 and before Wk 24) or > 200 c/mL (at or after Wk 24)
– TF: time to discontinuation of randomized component for toxicity
Secondary composite endpoint: the earlier occurrence of either VF or TF
Lennox JL, et al. Ann Intern Med. 2014;161:461-471.
ART-naive pts with HIV-1 RNA
≥ 1000 c/mL (N = 1809)
ATV/RTV 300/100 mg QD + TDF/FTC(n = 605)
RAL 400 mg BID + TDF/FTC(n = 603)
Stratified by HIV-1 RNA < or ≥ 100,000 c/mL, participation in
metabolic substudy, CV risk
DRV/RTV 800/100 mg QD + TDF/FTC(n = 601)
Wk 96 after last pt enrolled
Regimen switch allowed for tolerability.

clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
ACTG 5257: Cumulative Incidence of Virologic Failure at Wk 96
Lennox JL, et al. Ann Intern Med. 2014;161:461-471.
Difference in 96-Wk Cumulative Incidence (97.5% CI)
-20 0-10 10 20
ATV/RTV vs RAL3.4% (-0.7% to 7.4%)
DRV/RTV vs RAL5.6% (1.3% to 9.9%)
ATV/RTV vs DRV/RTV-2.2% (-6.7% to 2.3%)
1.00
0.75
0.50
0.25
0
Cu
mu
lati
ve I
nci
den
ce
0
Wks Since Study Entry
24 48 64 80 96 112 128 144
ATV/RTVRALDRV/RTV
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Favors RAL
Favors DRV/RTV
Lennox JL, et al. Ann Intern Med. 2014;161:461-471.
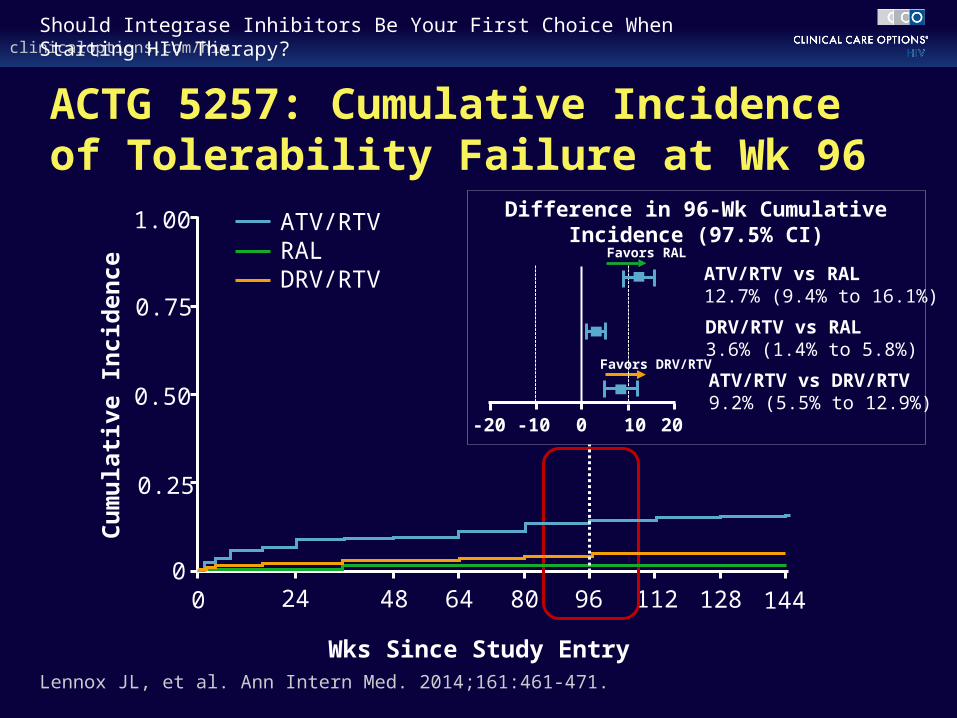
ACTG 5257: Cumulative Incidence of Tolerability Failure at Wk 96
Difference in 96-Wk Cumulative Incidence (97.5% CI)
-20 0-10 10 20
ATV/RTV vs RAL12.7% (9.4% to 16.1%)
DRV/RTV vs RAL3.6% (1.4% to 5.8%)
ATV/RTV vs DRV/RTV9.2% (5.5% to 12.9%)
1.00
0.75
0.50
0.25
0
Cu
mu
lati
ve I
nci
den
ce
0
Wks Since Study Entry
24 48 64 80 96 112 128 144
ATV/RTVRALDRV/RTV
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Difference in 96-Wk Cumulative Incidence (97.5% CI)
Favors RAL
Favors RAL
Favors DRV/RTV
Lennox JL, et al. Ann Intern Med. 2014;161:461-471.
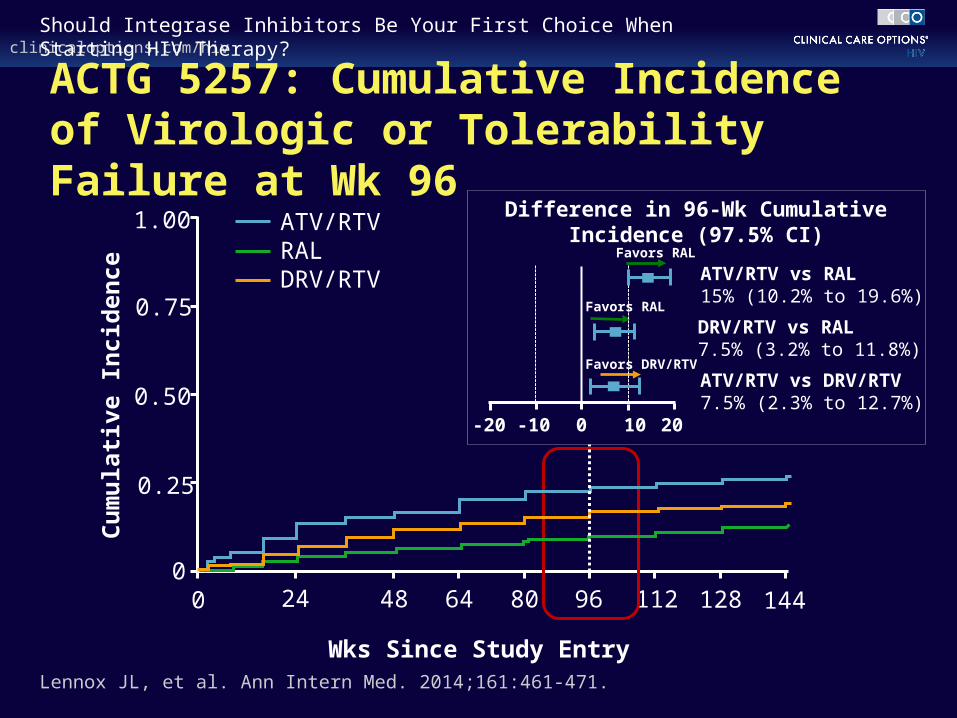
ACTG 5257: Cumulative Incidence of Virologic or Tolerability Failure at Wk 96
-20 0-10 10 20
ATV/RTV vs RAL15% (10.2% to 19.6%)
DRV/RTV vs RAL7.5% (3.2% to 11.8%)
ATV/RTV vs DRV/RTV7.5% (2.3% to 12.7%)
1.00
0.75
0.50
0.25
0
Cu
mu
lati
ve I
nci
den
ce
0
Wks Since Study Entry
24 48 64 80 96 112 128 144
ATV/RTVRALDRV/RTV
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
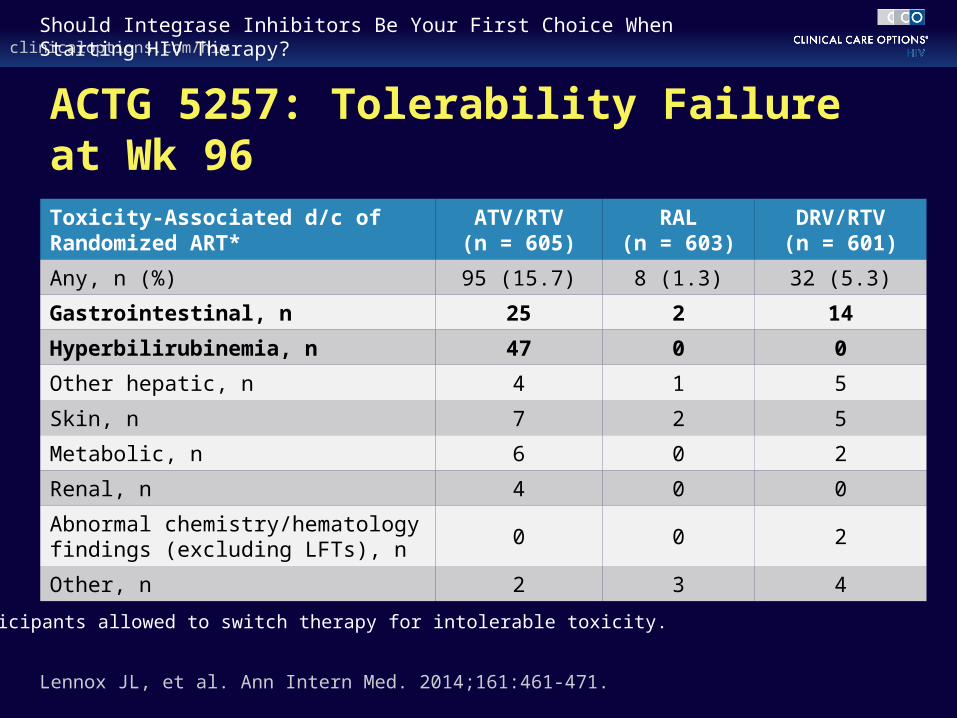
ACTG 5257: Tolerability Failure at Wk 96
Lennox JL, et al. Ann Intern Med. 2014;161:461-471.
Toxicity-Associated d/c of Randomized ART*
ATV/RTV(n = 605)
RAL(n = 603)
DRV/RTV(n = 601)
Any, n (%) 95 (15.7) 8 (1.3) 32 (5.3)
Gastrointestinal, n 25 2 14
Hyperbilirubinemia, n 47 0 0
Other hepatic, n 4 1 5
Skin, n 7 2 5
Metabolic, n 6 0 2
Renal, n 4 0 0
Abnormal chemistry/hematology findings (excluding LFTs), n
0 0 2
Other, n 2 3 4
*Participants allowed to switch therapy for intolerable toxicity.
Elvitegravir
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
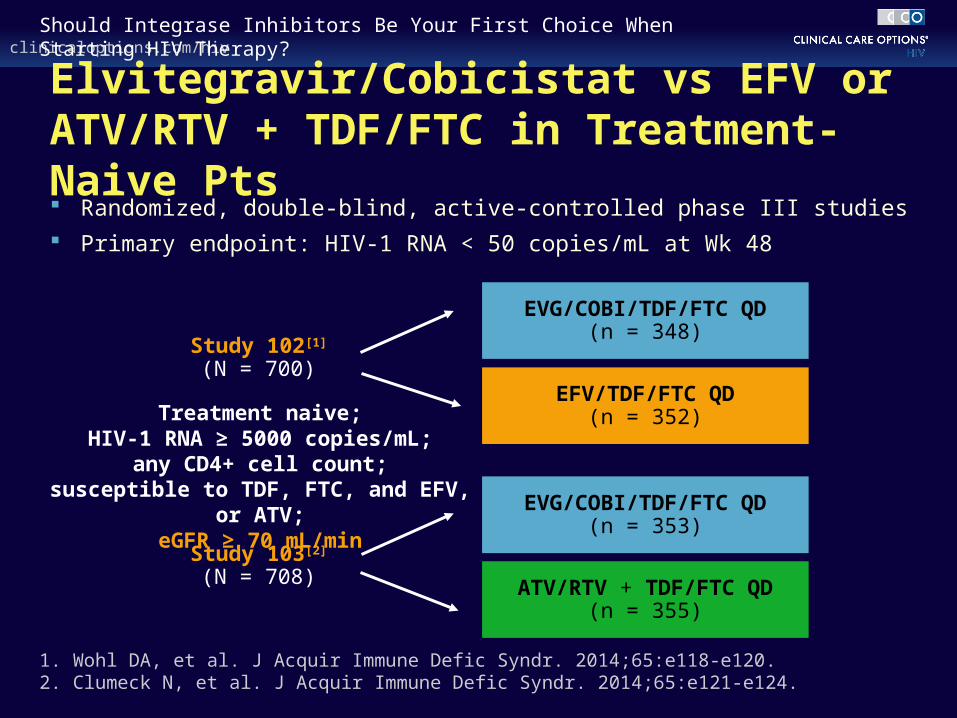
Elvitegravir/Cobicistat vs EFV or ATV/RTV + TDF/FTC in Treatment-Naive Pts Randomized, double-blind, active-controlled phase III studies
Primary endpoint: HIV-1 RNA < 50 copies/mL at Wk 48
1. Wohl DA, et al. J Acquir Immune Defic Syndr. 2014;65:e118-e120. 2. Clumeck N, et al. J Acquir Immune Defic Syndr. 2014;65:e121-e124.
Treatment naive;HIV-1 RNA ≥ 5000 copies/mL;
any CD4+ cell count;susceptible to TDF, FTC, and EFV, or
ATV;eGFR ≥ 70 mL/min
Study 102[1]
(N = 700)
Study 103[2]
(N = 708)
EVG/COBI/TDF/FTC QD(n = 348)
EFV/TDF/FTC QD(n = 352)
EVG/COBI/TDF/FTC QD(n = 353)
ATV/RTV + TDF/FTC QD(n = 355)
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
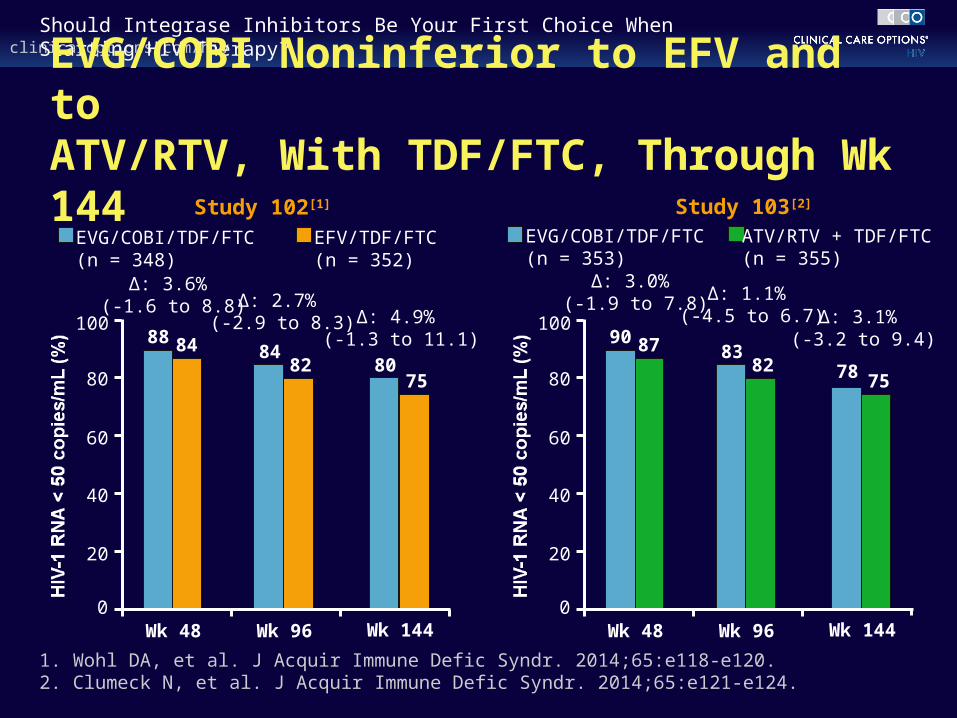
EVG/COBI Noninferior to EFV and to ATV/RTV, With TDF/FTC, Through Wk 144
Wk 48 Wk 144
EVG/COBI/TDF/FTC (n = 348)
EFV/TDF/FTC (n = 352)
8075
0
20
40
60
80
10088 84
Δ: 3.6% (-1.6 to 8.8)
Δ: 4.9% (-1.3 to 11.1)
8482
Wk 96
Δ: 2.7% (-2.9 to 8.3)
EVG/COBI/TDF/FTC (n = 353)
ATV/RTV + TDF/FTC (n = 355)
Δ: 3.0% (-1.9 to 7.8) Δ: 1.1%
(-4.5 to 6.7)
Wk 48 Wk 144
78 75
0
20
40
60
80
10090 87
Δ: 3.1% (-3.2 to 9.4)
8382
Wk 96
Study 102[1] Study 103[2]
1. Wohl DA, et al. J Acquir Immune Defic Syndr. 2014;65:e118-e120. 2. Clumeck N, et al. J Acquir Immune Defic Syndr. 2014;65:e121-e124.
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Studies 102 and 103: Common Adverse Events Study 102[1]
– More CNS effects, rash observed with EFV vs EVG/COBI
– More nausea with EVG/COBI vs EFV
Study 103[2]
– More ocular icterus observed with ATV/RTV vs EVG/COBI
– Common adverse events of EVG/COBI included nausea and diarrhea; frequency similar to that observed with ATV/RTV
1. Sax P, et al. Lancet. 2012;379:2439-2448. 2. DeJesus E, et al. Lancet. 2012;379:2429-2438.

clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Studies 102 and 103: Change in Serum Creatinine Through Wk 48
1. Sax P, et al. Lancet. 2012;379:2439-2448. 2. DeJesus E, et al. Lancet. 2012;379:2429-2438.
Study 102[1] Study 103[2]
Ch
ang
e F
rom
Bas
elin
e in
S
eru
m C
reat
inin
e (µ
mo
l/L
)
20
15
10
5
0
-5
-100 2 4 8 12 16 24 32 40 48
EVG/COBI/TDF/FTCEFV/TDF/FTC
Ser
um
Cre
atin
ine
Co
nce
ntr
ati
on
Ch
an
ge
(µm
ol/
L) 20
15
10
5
0
-5
-100 2 4 8 12 16 24 32 40 48
EVG/COBI/TDF/FTCATV/RTV + TDF/FTC
Wks Wks

Dolutegravir
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
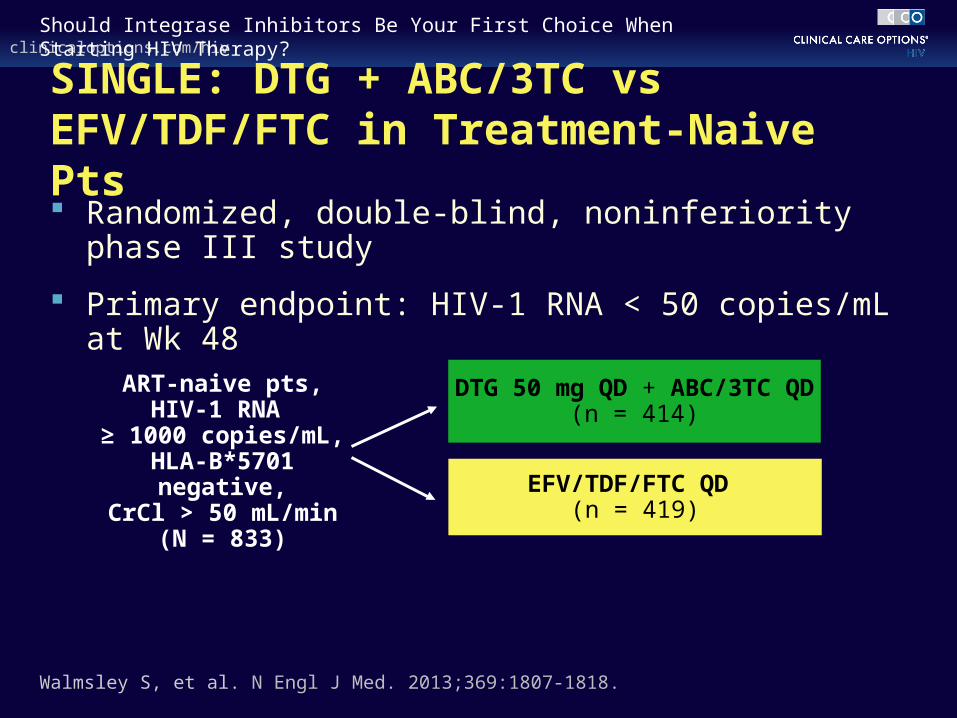
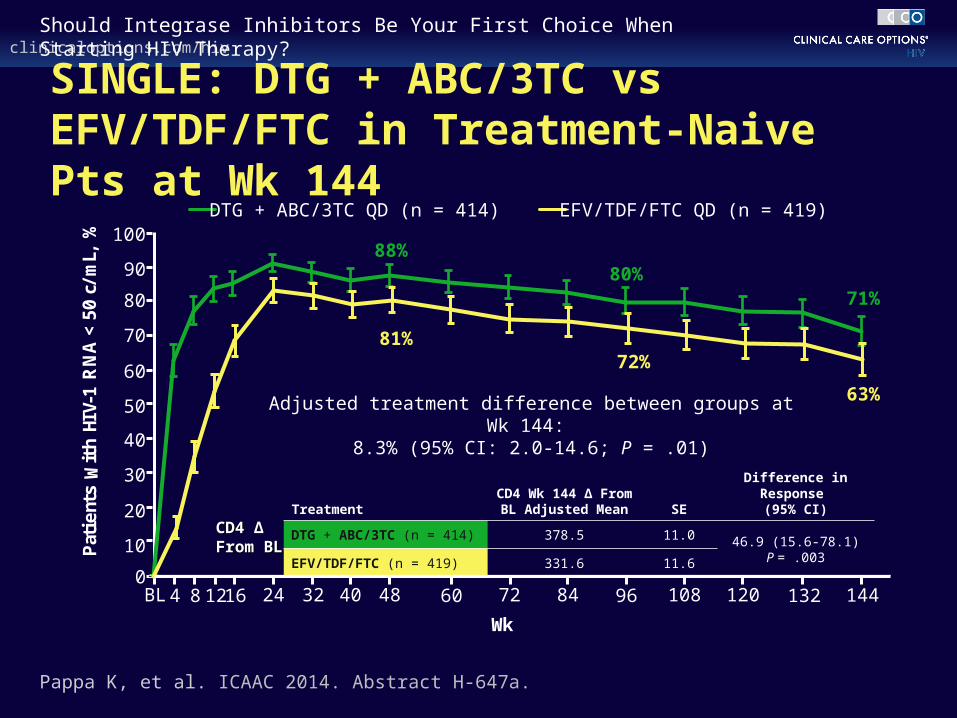
SINGLE: DTG + ABC/3TC vs EFV/TDF/FTC in Treatment-Naive Pts Randomized, double-blind, noninferiority phase III study
Primary endpoint: HIV-1 RNA < 50 copies/mL at Wk 48
ART-naive pts,HIV-1 RNA
≥ 1000 copies/mL,HLA-B*5701 negative,
CrCl > 50 mL/min(N = 833)
DTG 50 mg QD + ABC/3TC QD(n = 414)
EFV/TDF/FTC QD (n = 419)
Walmsley S, et al. N Engl J Med. 2013;369:1807-1818.
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Wk
71%
63%
80%
72%81%
88%
TreatmentCD4 Wk 144 ∆ From BL
Adjusted Mean SEDifference in Response
(95% CI)
DTG + ABC/3TC (n = 414) 378.5 11.0 46.9 (15.6-78.1)P = .003EFV/TDF/FTC (n = 419) 331.6 11.6
BL 4 8 1216 24 32 40 14448 60 72 84 96 108 120 132
Adjusted treatment difference between groups at Wk 144: 8.3% (95% CI: 2.0-14.6; P = .01)
CD4 ∆ CD4 ∆ From BLFrom BL
Pappa K, et al. ICAAC 2014. Abstract H-647a.
SINGLE: DTG + ABC/3TC vs EFV/TDF/FTC in Treatment-Naive Pts at Wk 144
Pat
ients
With H
IV-1
RN
A <
50 c
/mL,
% DTG + ABC/3TC QD (n = 414) EFV/TDF/FTC QD (n = 419)
100
90
80
70
60
50
40
30
20
10
0
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
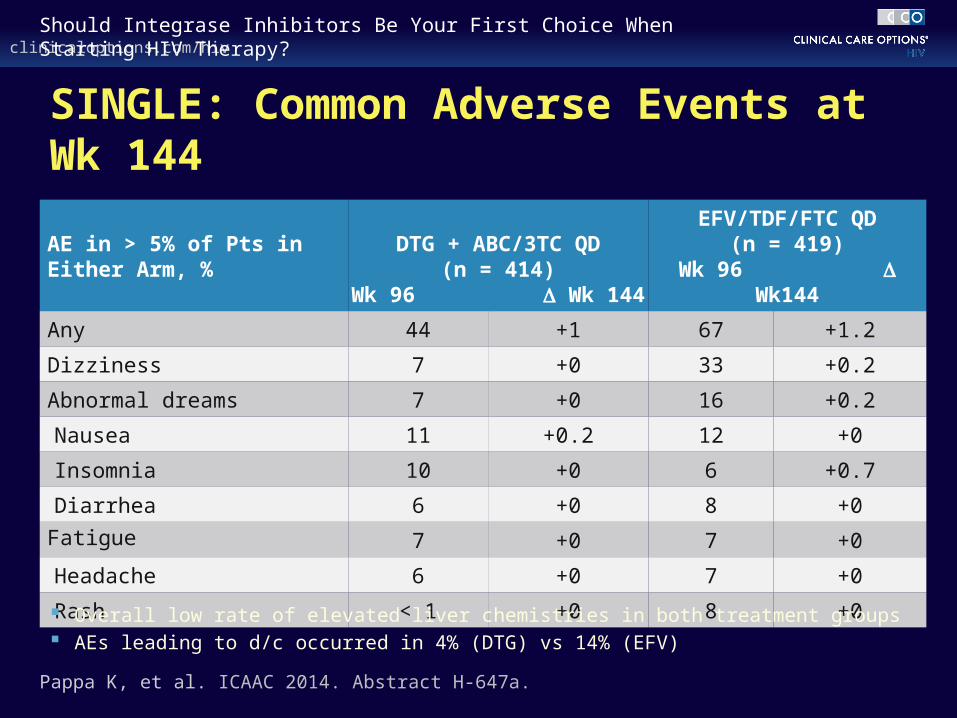
AE in > 5% of Pts in Either Arm, %
DTG + ABC/3TC QD(n = 414)
Wk 96 Wk 144
EFV/TDF/FTC QD(n = 419)
Wk 96 Wk144
Any 44 +1 67 +1.2
Dizziness 7 +0 33 +0.2
Abnormal dreams 7 +0 16 +0.2
Nausea 11 +0.2 12 +0
Insomnia 10 +0 6 +0.7
Diarrhea 6 +0 8 +0
Fatigue 7 +0 7 +0
Headache 6 +0 7 +0
Rash < 1 +0 8 +0
Pappa K, et al. ICAAC 2014. Abstract H-647a.
SINGLE: Common Adverse Events at Wk 144
Overall low rate of elevated liver chemistries in both treatment groups AEs leading to d/c occurred in 4% (DTG) vs 14% (EFV)

clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
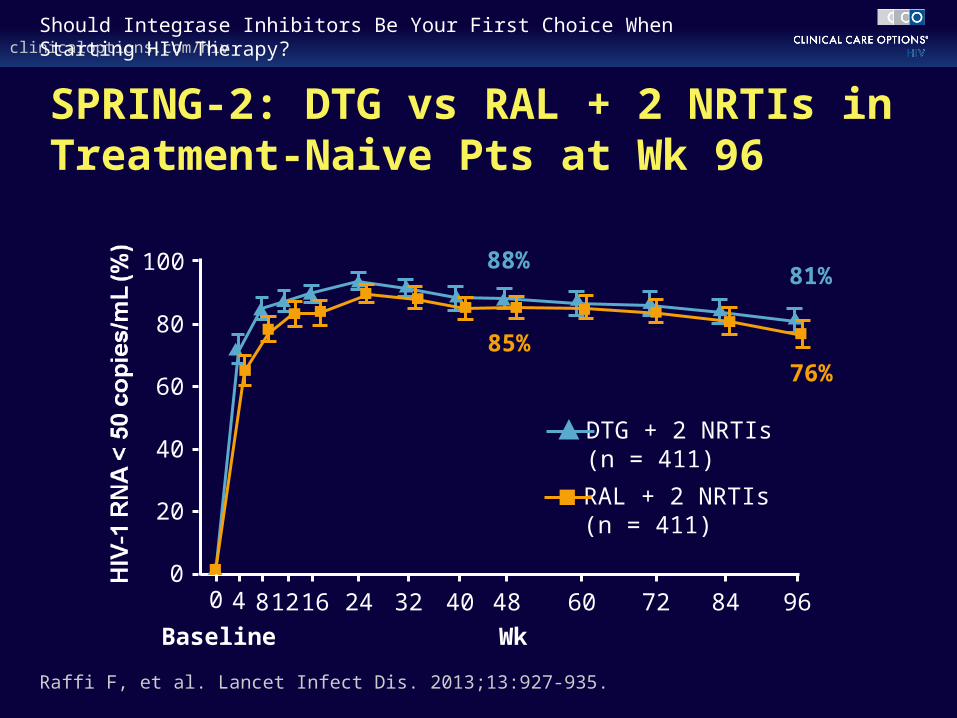
SPRING-2: DTG + NRTIs vs RAL + NRTIs in Treatment-Naive Pts Randomized, double-blind, noninferiority phase III study Primary endpoint: HIV-1 RNA < 50 copies/mL at Wk 48
ART-naive pts,HIV-1 RNA
≥ 1000 copies/mL(N = 822)
DTG 50 mg QD + 2 NRTIs*(n = 411)
RAL 400 mg BID + 2 NRTIs*(n = 411)
*Investigator-selected NRTI backbone: either TDF/FTC or ABC/3TC.
Raffi F, et al. Lancet. 2013;381:735-743.
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
SPRING-2: DTG vs RAL + 2 NRTIs in Treatment-Naive Pts at Wk 96
Raffi F, et al. Lancet Infect Dis. 2013;13:927-935.
DTG + 2 NRTIs (n = 411)
RAL + 2 NRTIs (n = 411)
81%
76%
100
80
60
40
20
0
Baseline Wk
4 8 16 24 32 48 60 72 968440120
88%
85%

clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
SPRING-2: Change in Creatinine
Raffi F, et al. Lancet Infect Dis. 2013;13:927-935.
40
30
20
10
0
-20
-10
Wk
4 8 16 24 32 48 60 72 968440120
DTG + 2 NRTIs (n = 411)
RAL + 2 NRTIs (n = 411)
Dolutegravir n = Raltegravir n =
401403
397400
393391
389388
390387
384375
371354
374354
364355
358348
351338
342327
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
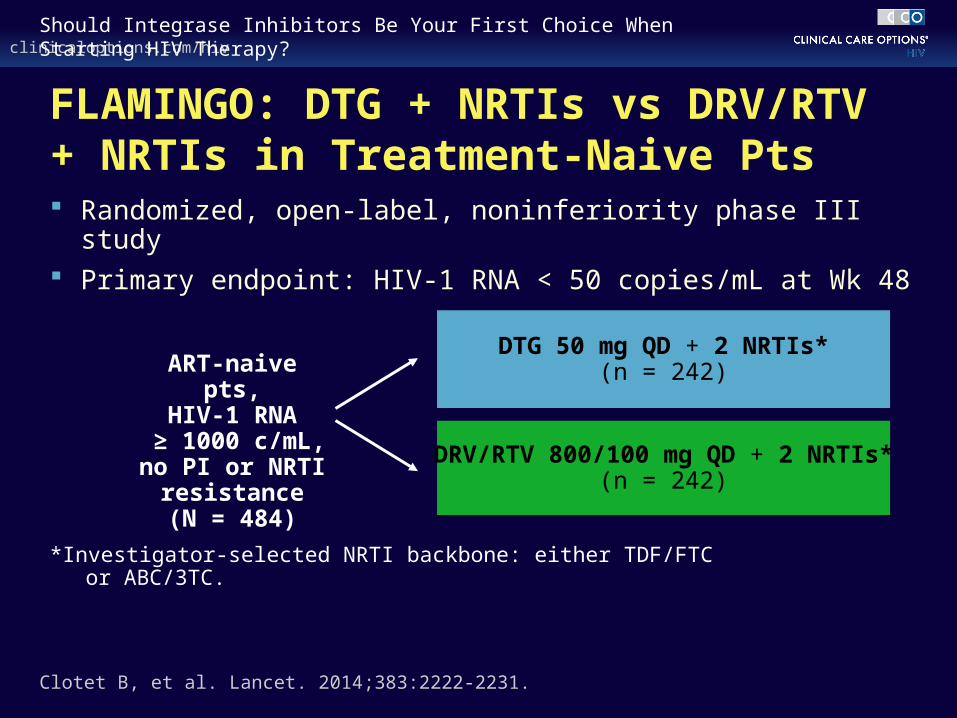
FLAMINGO: DTG + NRTIs vs DRV/RTV+ NRTIs in Treatment-Naive Pts Randomized, open-label, noninferiority phase III study Primary endpoint: HIV-1 RNA < 50 copies/mL at Wk 48
*Investigator-selected NRTI backbone: either TDF/FTC or ABC/3TC.
DTG 50 mg QD + 2 NRTIs*(n = 242)
DRV/RTV 800/100 mg QD + 2 NRTIs*(n = 242)
ART-naive pts,HIV-1 RNA
≥ 1000 c/mL,no PI or NRTI
resistance(N = 484)
Clotet B, et al. Lancet. 2014;383:2222-2231.
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
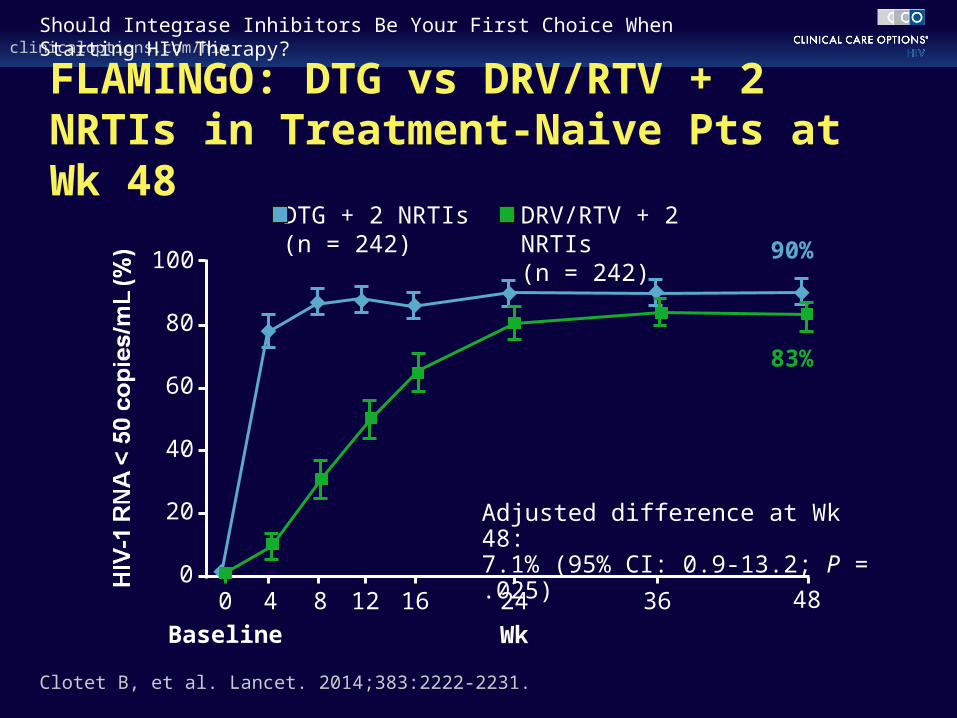
FLAMINGO: DTG vs DRV/RTV + 2 NRTIs in Treatment-Naive Pts at Wk 48
Clotet B, et al. Lancet. 2014;383:2222-2231.
DTG + 2 NRTIs (n = 242)
DRV/RTV + 2 NRTIs
(n = 242)90%
83%
100
80
60
40
20
0
Baseline Wk
Adjusted difference at Wk 48:7.1% (95% CI: 0.9-13.2; P = .025)
4 8 12 16 24 36 480
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
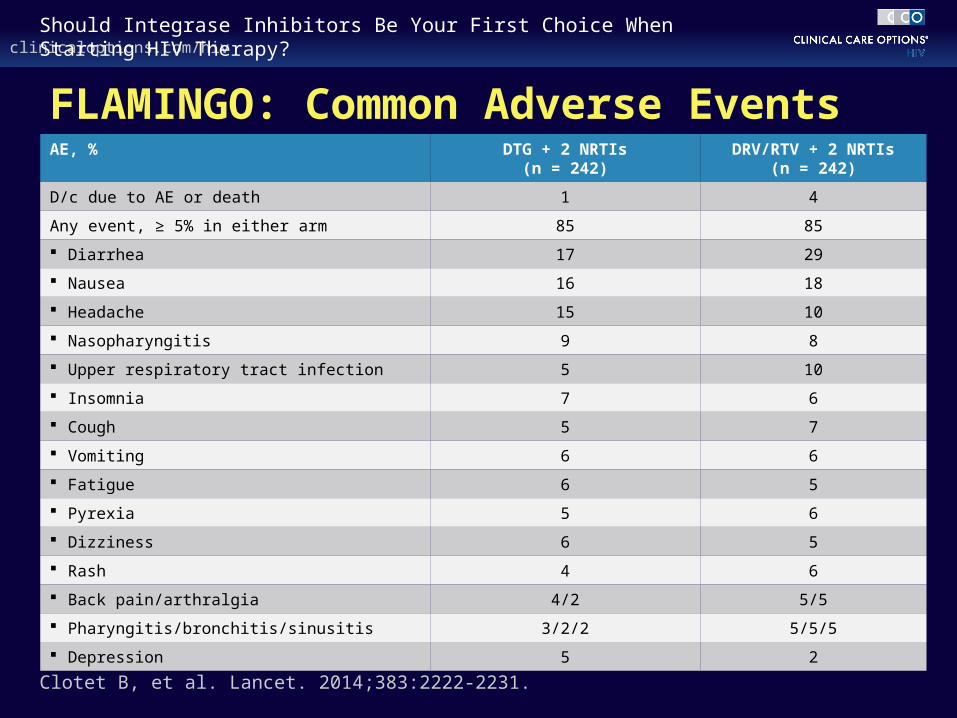
FLAMINGO: Common Adverse EventsAE, % DTG + 2 NRTIs
(n = 242)DRV/RTV + 2 NRTIs
(n = 242)
D/c due to AE or death 1 4
Any event, ≥ 5% in either arm 85 85
Diarrhea 17 29
Nausea 16 18
Headache 15 10
Nasopharyngitis 9 8
Upper respiratory tract infection 5 10
Insomnia 7 6
Cough 5 7
Vomiting 6 6
Fatigue 6 5
Pyrexia 5 6
Dizziness 6 5
Rash 4 6
Back pain/arthralgia 4/2 5/5
Pharyngitis/bronchitis/sinusitis 3/2/2 5/5/5
Depression 5 2
Clotet B, et al. Lancet. 2014;383:2222-2231.

Use in Clinical Practice
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
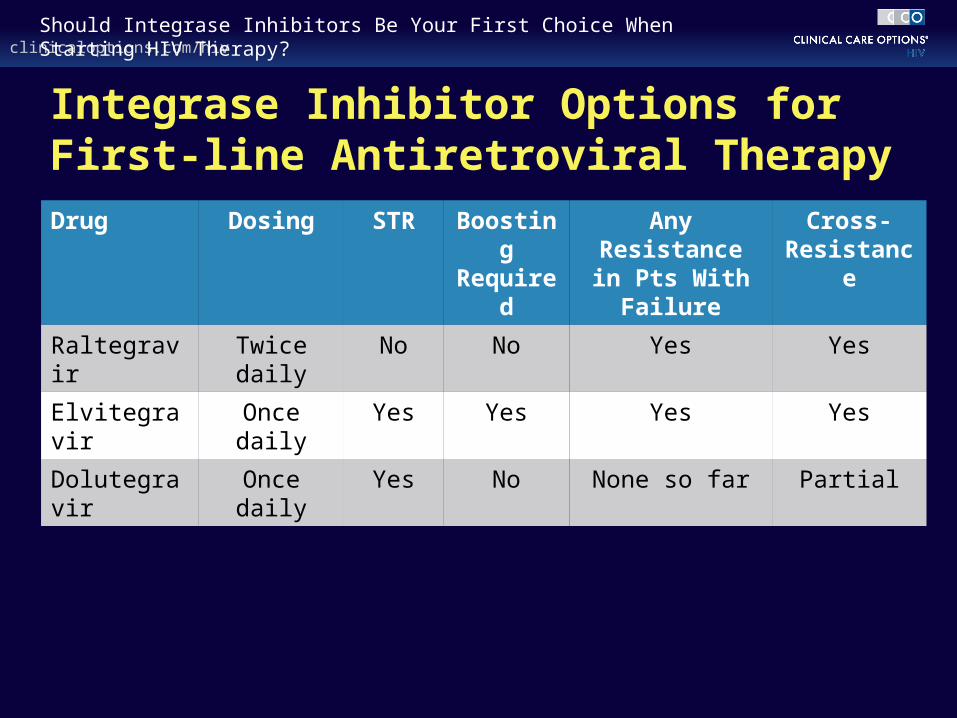
Integrase Inhibitor Options for First-line Antiretroviral TherapyDrug Dosing STR Boosting
RequiredAny Resistance
in Pts With Failure
Cross- Resistance
Raltegravir Twice daily No No Yes Yes
Elvitegravir Once daily Yes Yes Yes Yes
Dolutegravir Once daily Yes No None so far Partial
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
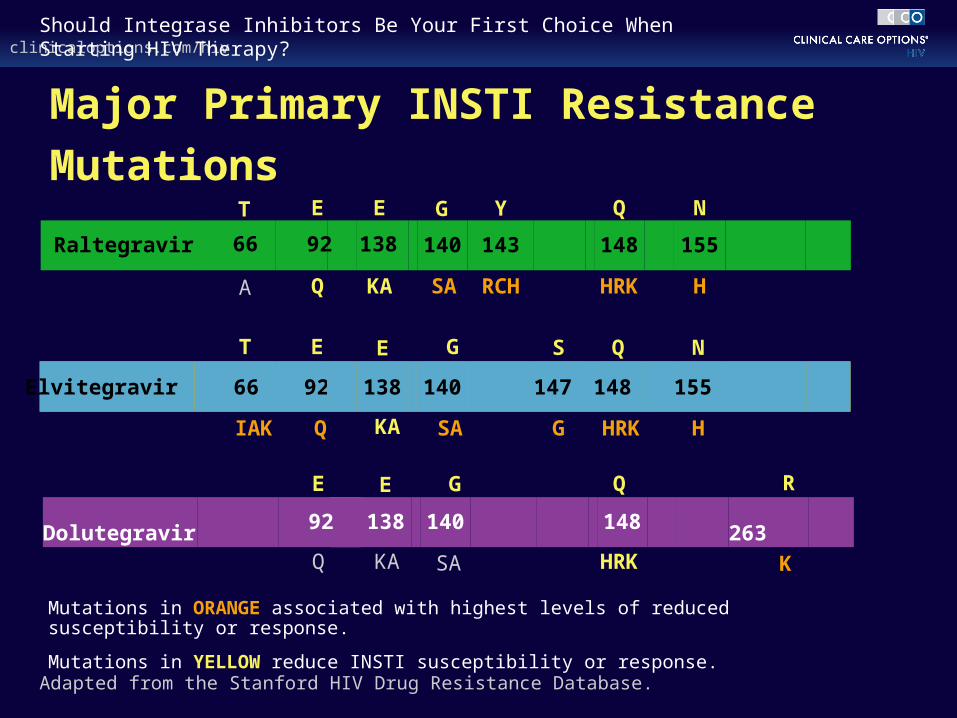
Major Primary INSTI Resistance Mutations
HSA
G
HRK
NQ
G
S
Q
E
IAK
T
Adapted from the Stanford HIV Drug Resistance Database.
H
N
RCH
Y
KA
E
HRK
Q
Q
E
SA
HRK
Q
Q
E
G
E
KA
T
A
E
KA
G
SA
R
K
Mutations in ORANGE associated with highest levels of reduced susceptibility or response.
Mutations in YELLOW reduce INSTI susceptibility or response.
15597 14814792 155140 1481479266 138Elvitegravir
155143140 14892 13866 Raltegravir
263140 14813892 Dolutegravir
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
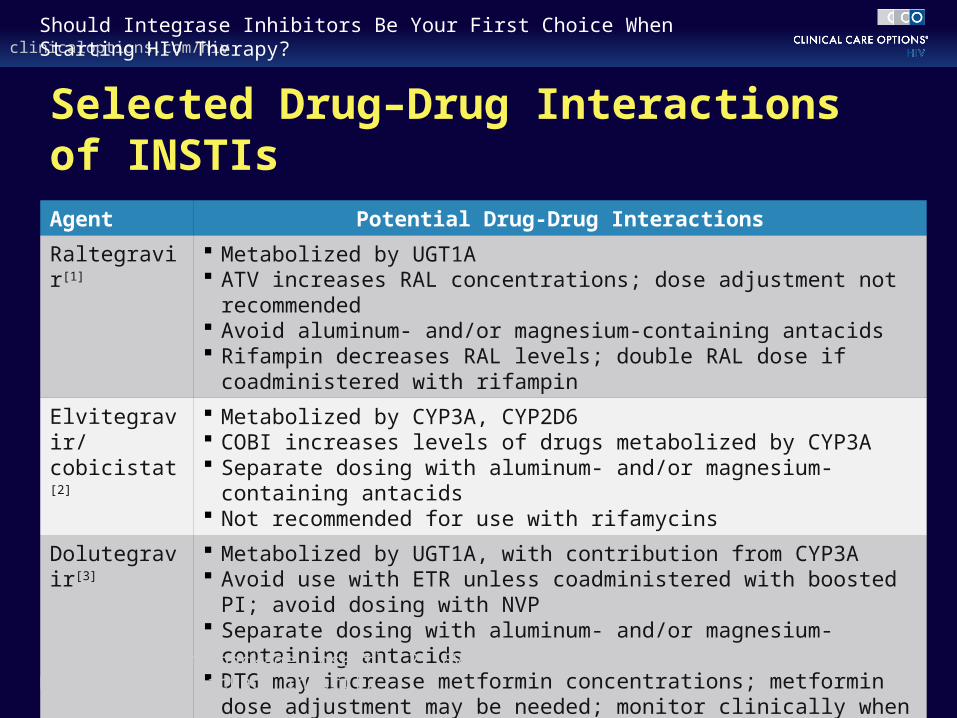
Selected Drug–Drug Interactions of INSTIs
Agent Potential Drug-Drug Interactions
Raltegravir[1] Metabolized by UGT1A ATV increases RAL concentrations; dose adjustment not recommended Avoid aluminum- and/or magnesium-containing antacids Rifampin decreases RAL levels; double RAL dose if coadministered with
rifampin
Elvitegravir/cobicistat[2]
Metabolized by CYP3A, CYP2D6 COBI increases levels of drugs metabolized by CYP3A Separate dosing with aluminum- and/or magnesium-containing antacids Not recommended for use with rifamycins
Dolutegravir[3] Metabolized by UGT1A, with contribution from CYP3A Avoid use with ETR unless coadministered with boosted PI; avoid dosing
with NVP Separate dosing with aluminum- and/or magnesium-containing antacids DTG may increase metformin concentrations; metformin dose adjustment
may be needed; monitor clinically when starting or stopping DTG
1. Raltegravir [package insert]. 2. EVG/COBI/TDF/FTC [package insert]. 3. Dolutegravir [package insert].
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Current DHHS and IAS-USA Guidelines: Recommended INSTIs for First-line ART RAL + TDF/FTC
EVG/COBI/TDF/FTC
– Only for pts with pretreatment CrCl ≥ 70 mL/min[1,2]
DTG + TDF/FTC
DTG + ABC/3TC*
– Only for pts who are HLA-B*5701 negative[1,2]
1. DHHS Guidelines. May 2014. 2. Günthard H, et al. JAMA. 2014;312:410-425.
*Guidelines predate availability of single-tablet regimen.

Ongoing Development
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Recent and Anticipated Developments in the INSTI Field DTG/ABC/3TC single-tablet regimen
EVG/COBI/TAF/FTC single-tablet regimen
DTG/RPV single-tablet regimen
RAL/3TC once-daily coformulation
Cabotegravir (S/GSK1265744)
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Summary
INSTI-based regimens have demonstrated at least noninferior efficacy vs regimens containing boosted PIs or NNRTIs in treatment-naive pts
– INSTIs generally well tolerated
– Some INSTIs have low resistance barrier (RAL, EVG)
– No emergent resistance to date with first-line DTG failure
INSTI-based regimens are among preferred options for first-line ART
Once-daily INSTI-based STRs are available (EVG, DTG)
– More anticipated in future

Joseph J. Eron, Jr., MD Professor of Medicine and EpidemiologyUniversity of North Carolina School of MedicineDirector, AIDS Clinical Trials UnitUniversity of North CarolinaChapel Hill, North Carolina
Panel Discussion: Are Integrase Inhibitors the New Gold Standard for First-line Antiretroviral Therapy?

Panel Discussion
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Key Questions for Debate
When selecting a first-line regimen, should INSTI-based options be the “default” choice?
For which pts, if any, might there not be an appropriate first-line INSTI-based regimen?
In the absence of head-to-head first-line trials, what considerations related to efficacy and safety should influence the choice between available INSTI-based regimens?
How do considerations such as availability of coformulations, dosing frequency, drug–drug interactions, and so on, affect the decision-making process for individual pts?
Case 1: A 24-Yr-Old Male Recently Diagnosed HIV Positive
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Case 1: 24-Yr-Old Male Recently Diagnosed HIV Positive 24-yr-old black MSM recently diagnosed HIV positive
HIV-1 RNA: 187,000 c/mL; CD4+ count: 448 cells/mm3
HIV genotype: WT, HBV immune, HCV Ab negative; CrCl: 120 mL/min; AST/ALT normal; HLA-B*5701 negative
No significant past medical history, no medications, occasional alcohol and marijuana use, sexually active with 1 steady HIV-negative partner
Has attended several clinic visits and is interested in starting HIV therapy; prefers to take as few pills as possible but wants what you think is best
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Summary of Panel Discussion
Many options are available for initial therapy
Most pts opt for a single-tablet regimen over a multitablet regimen, given the choice
– Simpler dosing, fewer copays
A variety of single-tablet regimens would be appropriate choices for the case pt
– He is young and healthy and has no comedications or comorbidities
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Summary of Panel Discussion
Efavirenz/TDF/FTC: extensive clinical experience with this agent, but CNS adverse events may persist
Rilpivirine/TDF/FTC: not recommended for this pt due to HIV-1 RNA > 100,000 copies/mL
Dolutegravir/ABC/3TC: data are supportive of this option, including in pts with high HIV-1 RNA
Elvitegravir/COBI/TDF/FTC: also a popular choice as it is well tolerated and trials have demonstrated noninferior efficacy vs PI-based or NNRTI-based therapy
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Panel Discussion
What if the pt were a woman with HIV-1 RNA 87,000 c/mL who is considering pregnancy in the near future
– Would this change your approach?
24-yr-old black woman recently diagnosed HIV positive HIV-1 RNA: 87,000 c/mL; CD4+ count: 448 cells/mm3
HIV GT: WT, HBV immune, HCV Ab-; CrCl: 120 mL/min; AST/ALT normal; HLA-B*5701- No comedications, occasional alcohol/marijuana use, steady HIV-negative partner Starting HIV therapy, prefers few pills as possible
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Summary of Panel Discussion
Important to discuss risk and assess the pt’s knowledge and plans
Most data on ART in pregnancy concerns boosted PIs, particularly ATV/RTV, LPV/RTV
– Most NRTI data with ZDV/3TC, increasingly with TDF/FTC
Panel believed most women choose not to take an STR when presented with these data
Panel would not choose an EFV-based regimen for a woman planning pregnancy; however, therapy should not be switched if a woman receiving EFV-based therapy becomes pregnant
Other STRs could be considered for this pt, although data on their use in pregnancy are lacking
Data from women receiving ART in pregnancy should be added to the Antiretroviral Pregnancy Registry (www.apregistry.com)
Case 2: A 28-Yr-Old Male With Advanced HIV Infection
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Case 2: 28-Yr-Old Male With Advanced HIV Infection 28-yr-old HIV-infected MSM, previously refused ART, now
referred to you for specialist care
HIV-1 RNA: 78,300 c/mL; CD4+ count: 70 cells/mm3
HIV GT: WT RT/pro; HBV Ag+; HBV DNA: 34 million IU/mL, HCV neg; ALT: 78 IU/L; Cr: 0.8 mg/dL (70.7 µmol/L); CBC: normal
Physical exam reveals woody edema of right leg with some discoloration at the ankle, no palpable adenopathy; subsequent biopsy shows KS
Binges on alcohol; denies other drug use or sexual activity
He will try ART if you recommend it
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Summary of Panel Discussion
Nonadherence is a concern in this pt
Some panelists would choose a boosted PI due to low risk of resistance at failure
DTG + TDF/FTC may be another option, as it is well tolerated and convenient, and available data suggest risk of resistance at failure is also very low
RAL-based therapy may be a good choice for coadministration with chemotherapy due to lack of drug–drug interactions
RPV-based therapy is not recommended for this pt due to CD4+ cell count < 200 cells/mm3
Use of Integrase Inhibitorsin Primary NNRTI Resistance
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Case 3: 68-Yr-Old Female With Primary NNRTI Resistance 68-yr-old black woman recently diagnosed HIV positive
Ready to begin ART following several clinic visits
HIV-1 RNA: 215,600 c/mL; CD4+ count: 350 cells/mm3
Believes she acquired HIV from her husband who died 8 or 9 yrs ago
HTN well controlled on diuretic; UA: 1+ protein; CrCl: 50 mL/min; US shows slightly enlarged kidneys with no obstruction; nonsmoker, no alcohol use
Anti-HBs positive; HCV Ab negative; ALT: 37 IU/L, HLA-B*5701 negative
HIV RT/pro genotype detects K103N, no other mutations
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Summary of Panel Discussion
The pt likely acquired HIV from her husband at least 8 or 9 yrs ago; therefore, integrase resistance is unlikely
Most panelists do not routinely order integrase genotypes
– May be more likely to do so in recently infected pts, particularly those with transmitted resistance
A combined genotype test is available that assesses RT, protease, and integrase genes
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Summary of Panel Discussion
Renal biopsy may be considered to assess whether the pt’s renal dysfunction is related to HIV infection
ABC/3TC or daily TDF/FTC may be reasonable options with careful monitoring
– ABC/3TC may be less active if M184V is present as a minority species that was not detected on genotyping
Panelists would not choose ZDV/3TC or a regimen that did not include 2 NRTIs

clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Summary of Panel Discussion
Rilpivirine is not recommended due to HIV-1 RNA > 100,000 copies/mL
Atazanavir/ritonavir is associated with renal dysfunction and may not be the best choice for this pt
Darunavir/ritonavir could be used, but simpler regimens are available
Elvitegravir/cobicistat is not recommended for pts with creatinine clearance < 70 mL/min
Dolutegravir or raltegravir are both options for this pt
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
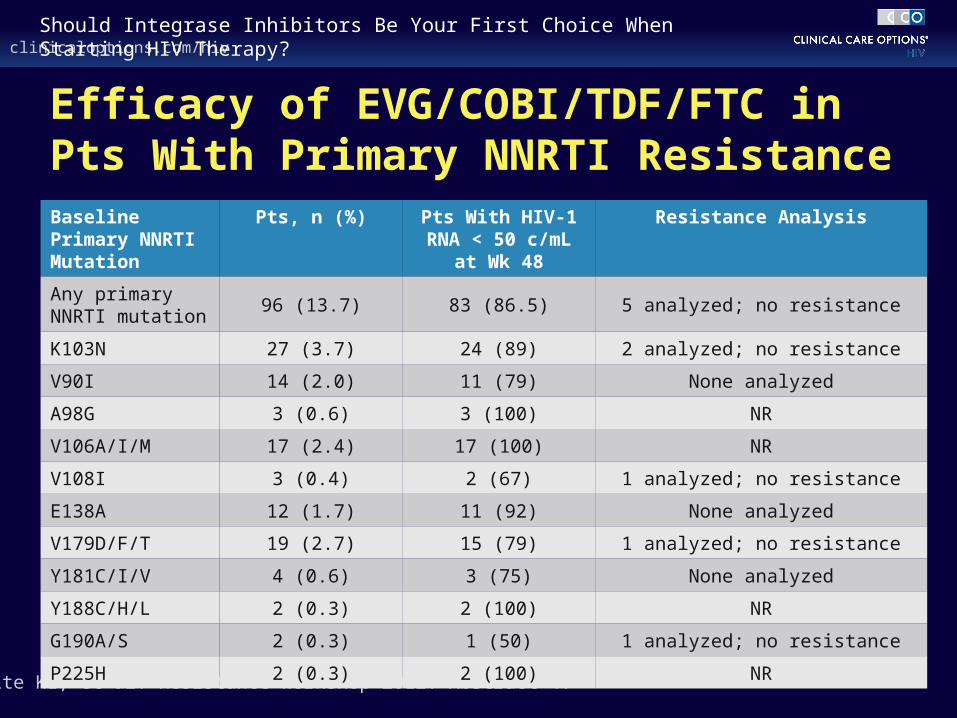
Efficacy of EVG/COBI/TDF/FTC in Pts With Primary NNRTI Resistance
White KL, et al. Resistance Workshop 2012. Abstract 4.
Baseline Primary NNRTI Mutation
Pts, n (%) Pts With HIV-1 RNA < 50 c/mL at Wk 48
Resistance Analysis
Any primary NNRTI mutation
96 (13.7) 83 (86.5) 5 analyzed; no resistance
K103N 27 (3.7) 24 (89) 2 analyzed; no resistance
V90I 14 (2.0) 11 (79) None analyzed
A98G 3 (0.6) 3 (100) NR
V106A/I/M 17 (2.4) 17 (100) NR
V108I 3 (0.4) 2 (67) 1 analyzed; no resistance
E138A 12 (1.7) 11 (92) None analyzed
V179D/F/T 19 (2.7) 15 (79) 1 analyzed; no resistance
Y181C/I/V 4 (0.6) 3 (75) None analyzed
Y188C/H/L 2 (0.3) 2 (100) NR
G190A/S 2 (0.3) 1 (50) 1 analyzed; no resistance
P225H 2 (0.3) 2 (100) NR
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Summary of Panel Discussion
Dolutegravir/ABC/3TC is available as a fixed-dose combination and was a popular choice for this pt
– However, data on the activity of dolutegravir-based therapy in pts with primary NNRTI resistance are lacking
Data on the use of darunavir/ritonavir with ABC/3TC are limited
Rilpivirine and atazanavir/ritonavir remain unsuitable
Raltegravir has been studied with ABC/3TC and may be considered in this pt
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
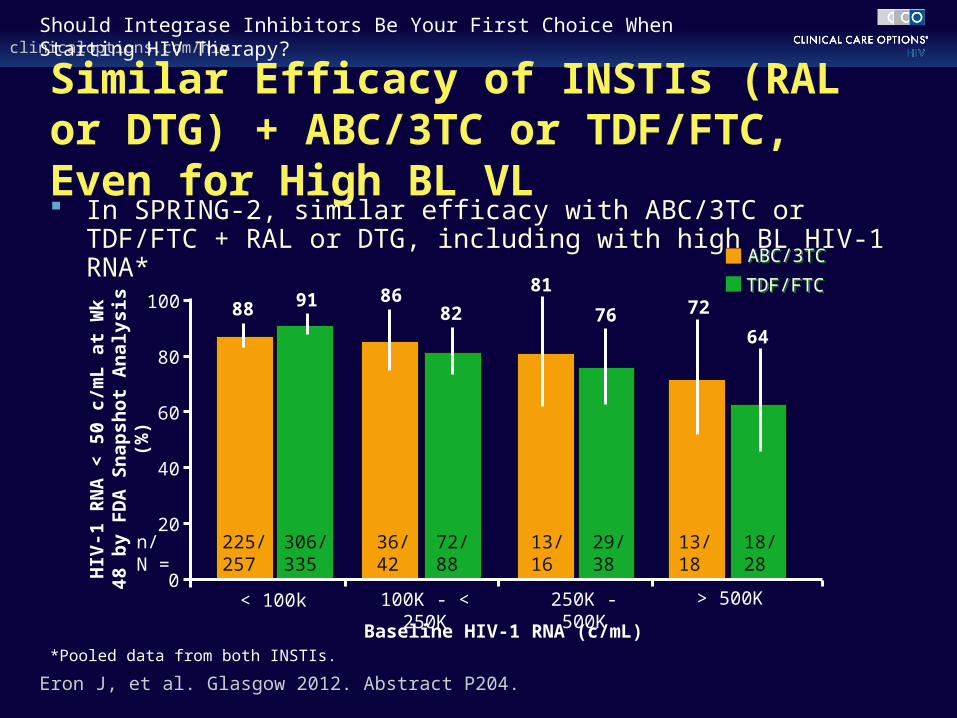
Similar Efficacy of INSTIs (RAL or DTG) + ABC/3TC or TDF/FTC, Even for High BL VL In SPRING-2, similar efficacy with ABC/3TC or TDF/FTC + RAL or
DTG, including with high BL HIV-1 RNA*
Eron J, et al. Glasgow 2012. Abstract P204.
< 100k 100K - < 250K 250K - 500K > 500K0
20
40
60
80
100
HIV
-1 R
NA
< 5
0 c/
mL
at
Wk
48
by
FD
A S
nap
sho
t A
nal
ysis
(%
)
86
n/N =
88
225/257
91
306/335
36/42
82
72/88
81
13/16
76
29/38
72
13/18
64
18/28
Baseline HIV-1 RNA (c/mL)
TDF/FTCTDF/FTC
ABC/3TCABC/3TC
*Pooled data from both INSTIs.
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Panel Discussion
What if the pt had CVD and renal disease?
– Modification: DM on metformin, PTCA with stent for an RCA lesion 2 yrs ago, no chest pain on β-blocker and atorvastatin, CrCl: 30 mL/min with 3+ microalbuminuria
Would you use a regimen sparing 2 NRTIs? If so, which one?
68-yr-old female recently diagnosed HIV positive HIV-1 RNA: 215,600 c/mL; CD4+ count: 350 cells/mm3
HTN controlled on therapy, DM on metformin, PTCA with stent, β-blocker and atorvastatin, CrCl: 30 mL/min
Anti-HBs+; HCV Ab-; ALT: 37 IU/L; HLA-B*5701- HIV RT/pro genotype: K103N, no integrase resistance
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Summary of Panel Discussion
Some panelists would still consider a regimen containing 2 NRTIs for this pt, though perhaps utilizing tenofovir/FTC dosed every other day
NRTI-sparing or NRTI-limiting regimens could be another option
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
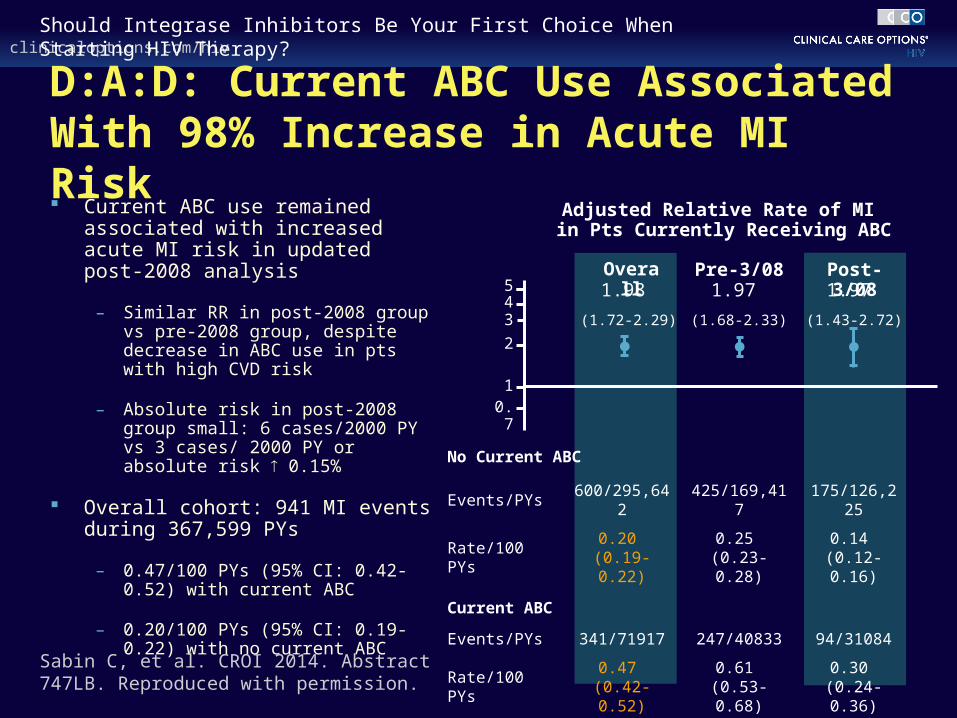
D:A:D: Current ABC Use Associated With 98% Increase in Acute MI Risk Current ABC use remained
associated with increased acute MI risk in updated post-2008 analysis
– Similar RR in post-2008 group vs pre-2008 group, despite decrease in ABC use in pts with high CVD risk
– Absolute risk in post-2008 group small: 6 cases/2000 PY vs 3 cases/ 2000 PY or absolute risk 0.15%
Overall cohort: 941 MI events during 367,599 PYs
– 0.47/100 PYs (95% CI: 0.42-0.52) with current ABC
– 0.20/100 PYs (95% CI: 0.19-0.22) with no current ABC
No Current ABC
Events/PYs 600/295,642 425/169,417 175/126,225
Rate/100 PYs0.20
(0.19-0.22)0.25
(0.23-0.28)0.14
(0.12-0.16)
Current ABC
Events/PYs 341/71917 247/40833 94/31084
Rate/100 PYs0.47
(0.42-0.52)0.61
(0.53-0.68)0.30
(0.24-0.36)Sabin C, et al. CROI 2014. Abstract 747LB. Reproduced with permission.
543
2
10.7
Overall Pre-3/08 Post-3/08
Adjusted Relative Rate of MI in Pts Currently Receiving ABC
1.98
(1.72-2.29)
1.97
(1.68-2.33)
1.97
(1.43-2.72)
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
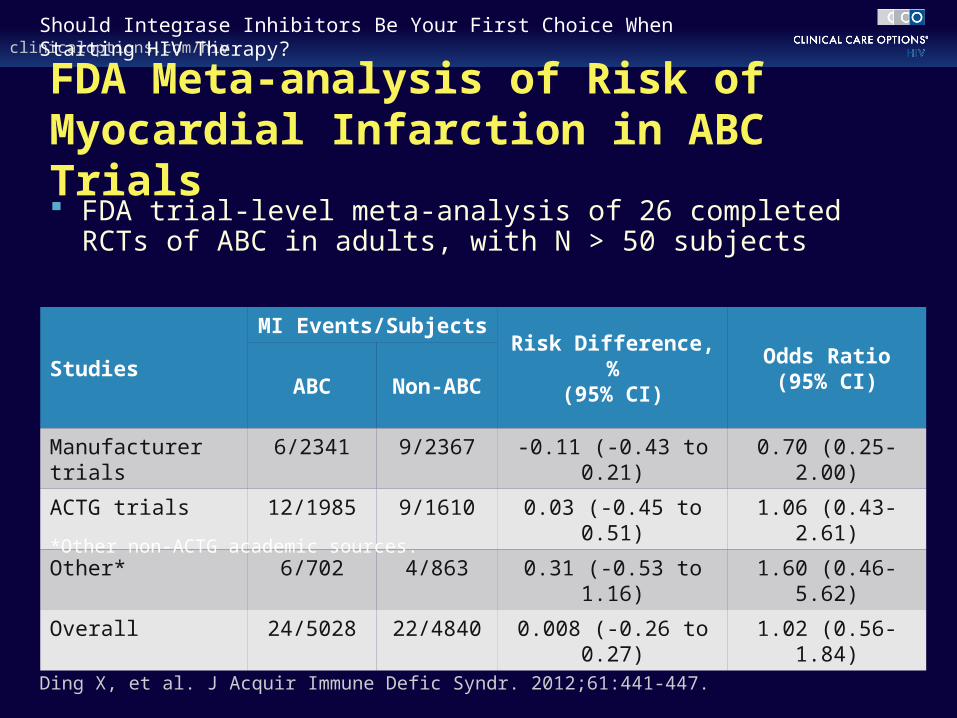
FDA Meta-analysis of Risk of Myocardial Infarction in ABC Trials FDA trial-level meta-analysis of 26 completed RCTs of
ABC in adults, with N > 50 subjects
Studies
MI Events/SubjectsRisk Difference, %
(95% CI)Odds Ratio
(95% CI)ABC Non-ABC
Manufacturer trials 6/2341 9/2367 -0.11 (-0.43 to 0.21) 0.70 (0.25-2.00)
ACTG trials 12/1985 9/1610 0.03 (-0.45 to 0.51) 1.06 (0.43-2.61)
Other* 6/702 4/863 0.31 (-0.53 to 1.16) 1.60 (0.46-5.62)
Overall 24/5028 22/4840 0.008 (-0.26 to 0.27) 1.02 (0.56-1.84)
Ding X, et al. J Acquir Immune Defic Syndr. 2012;61:441-447.
*Other non-ACTG academic sources.
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Summary of Panel Discussion
Darunavir/RTV plus raltegravir was noninferior to darunavir/RTV plus TDF/FTC in NEAT
– NRTI-sparing regimen appeared less efficacious at high HIV-1 RNA, although the difference between regimens was not statistically significant
Darunavir/RTV plus maraviroc was inferior to darunavir/RTV plus TDF/FTC in MODERN
Lopinavir/RTV plus raltegravir was comparable to lopinavir/RTV plus TDF/FTC in PROGRESS; although this was a small study
Lopinavir/RTV plus 3TC was comparable to lopinavir/RTV plus 2 NRTIs in GARDEL, including in pts with high HIV-1 RNA
Most panelists opted for darunavir/RTV plus dolutegravir plus 3TC; although this is an untested regimen
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
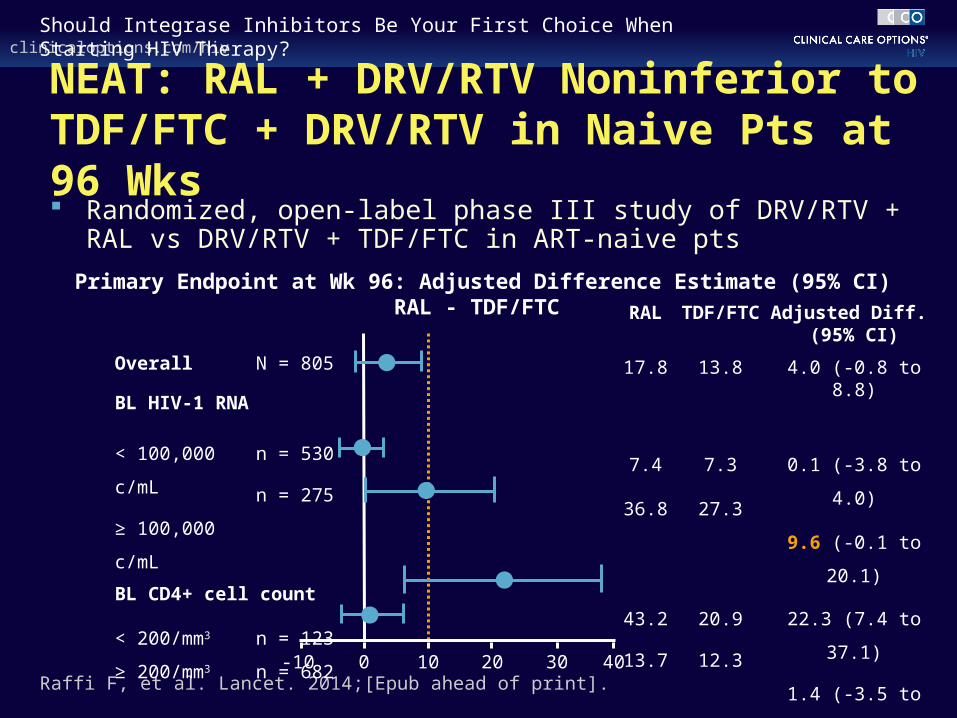
NEAT: RAL + DRV/RTV Noninferior to TDF/FTC + DRV/RTV in Naive Pts at 96 Wks Randomized, open-label phase III study of DRV/RTV + RAL vs
DRV/RTV + TDF/FTC in ART-naive pts
Raffi F, et al. Lancet. 2014;[Epub ahead of print].
Overall N = 805
BL HIV-1 RNA
< 100,000 c/mL
≥ 100,000 c/mL
n = 530
n = 275
BL CD4+ cell count
< 200/mm3
≥ 200/mm3
n = 123
n = 682
Primary Endpoint at Wk 96: Adjusted Difference Estimate (95% CI) RAL - TDF/FTC
RAL TDF/FTC Adjusted Diff. (95% CI)
17.8 13.8 4.0 (-0.8 to 8.8)
7.4
36.8
7.3
27.3
0.1 (-3.8 to 4.0)
9.6 (-0.1 to 20.1)
43.2
13.7
20.9
12.3
22.3 (7.4 to 37.1)
1.4 (-3.5 to 6.3)
-10 0 10 20 4030
Use of Integrase Inhibitorsin HIV/HCV Coinfection
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
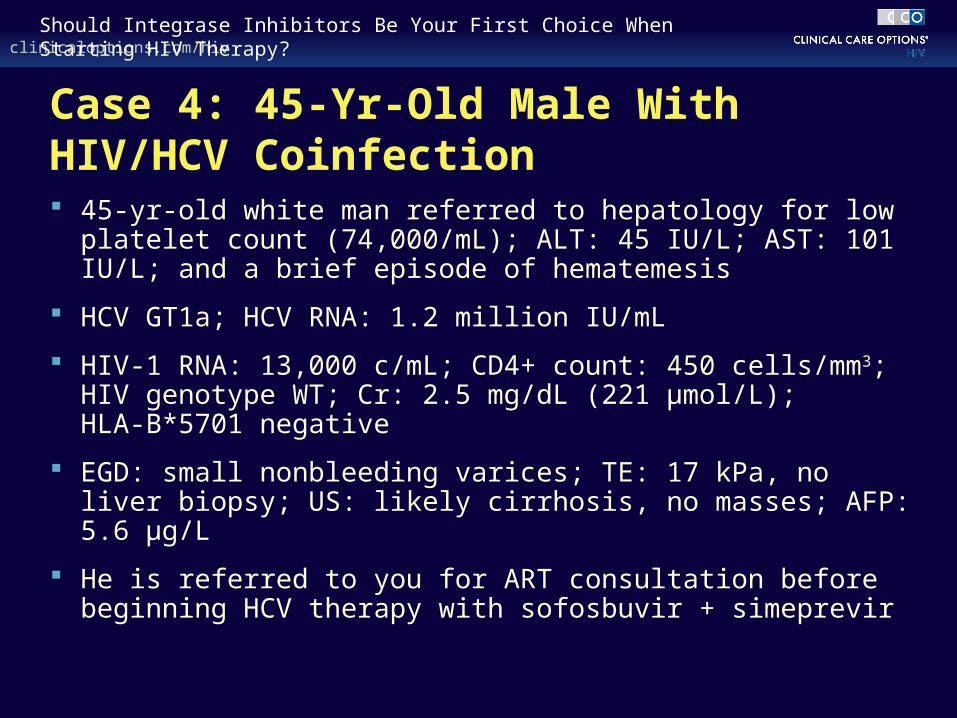
Case 4: 45-Yr-Old Male With HIV/HCV Coinfection 45-yr-old white man referred to hepatology for low platelet
count (74,000/mL); ALT: 45 IU/L; AST: 101 IU/L; and a brief episode of hematemesis
HCV GT1a; HCV RNA: 1.2 million IU/mL
HIV-1 RNA: 13,000 c/mL; CD4+ count: 450 cells/mm3; HIV genotype WT; Cr: 2.5 mg/dL (221 µmol/L); HLA-B*5701 negative
EGD: small nonbleeding varices; TE: 17 kPa, no liver biopsy; US: likely cirrhosis, no masses; AFP: 5.6 μg/L
He is referred to you for ART consultation before beginning HCV therapy with sofosbuvir + simeprevir
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Summary of Panel Discussion
There was no consensus among panelists about the best approach for this pt
– HIV therapy could be deferred until HCV therapy is completed, given the relatively short duration of the latter
– HCV therapy could be initiated soon after initiation of HIV therapy, once the pt is tolerating ART
Panelists would not defer HIV therapy in pts with low CD4+ cell counts
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Summary of Panel Discussion
Efavirenz, atazanavir/ritonavir, and darunavir/ritonavir should not be coadministered with simeprevir
Rilpivirine is an option for this pt, although this agent is more commonly used with TDF/FTC than with ABC/3TC
Most panelists opted for dolutegravir or raltegravir
– Raltegravir can be administered with simeprevir; requires twice-daily dosing but switch to simpler HIV therapy may be possible following completion of HCV therapy
– Dolutegravir can be administered with ABC/3TC as a fixed-dose combination, although estimated CrCl would require close monitoring in this pt to assess 3TC dosing
clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
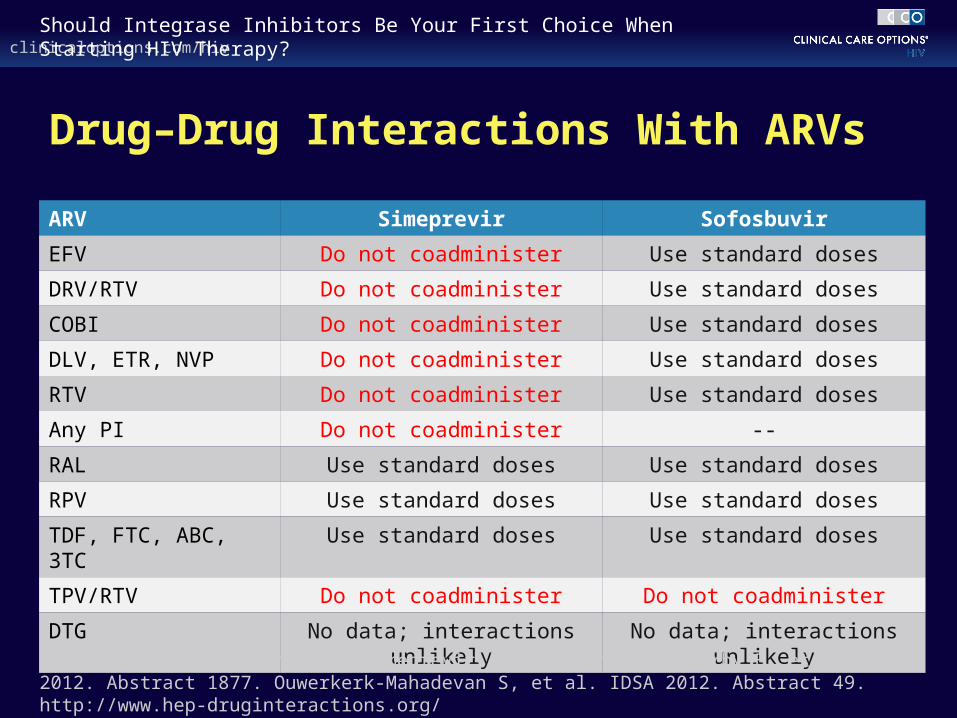
Drug–Drug Interactions With ARVs
ARV Simeprevir Sofosbuvir
EFV Do not coadminister Use standard doses
DRV/RTV Do not coadminister Use standard doses
COBI Do not coadminister Use standard doses
DLV, ETR, NVP Do not coadminister Use standard doses
RTV Do not coadminister Use standard doses
Any PI Do not coadminister --
RAL Use standard doses Use standard doses
RPV Use standard doses Use standard doses
TDF, FTC, ABC, 3TC Use standard doses Use standard doses
TPV/RTV Do not coadminister Do not coadminister
DTG No data; interactions unlikely No data; interactions unlikely
Sofosbuvir [package insert]. Simeprevir [package insert]. Kirby B, et al. AASLD 2012. Abstract 1877. Ouwerkerk-Mahadevan S, et al. IDSA 2012. Abstract 49. http://www.hep-druginteractions.org/

clinicaloptions.com/hivShould Integrase Inhibitors Be Your First Choice When Starting HIV Therapy?
Summary
When selecting a first-line regimen, each of the INSTI-based options can be considered
For most pts, at least 1 INSTI-based regimen is likely to be an option
Issues such as single-tablet options, choice of NRTI backbone, drug–drug interactions, tolerability, and once- vs twice-daily dosing should influence choice between available INSTI-based regimens
Go Online for More CCO Coverage of INSTI-Based Therapy
ClinicalThought™ commentaries by expert faculty focusing on the practical application of new data, guidelines and regulatory developments
Interactive Virtual Presentation featuring streaming narration of these slides and case studies illustrating the use of integrase inhibitors across the treatment spectrum by expert faculty John J. Eron, Jr., MD and Daniel R. Kuritzkes, MD
clinicaloptions.com/firstchoice