integrase inhibitors clinical...
TRANSCRIPT

INTEGRASE
INHIBITORS CLINICAL
CONSIDERATIONSBabafemi Taiwo, MBBS
Gene Stollerman Professor of Medicine
Chief, Division of Infectious Diseases
Northwestern University
Chicago
US

Disclosure
• Dr. Taiwo has served as a paid consultant to ViiV
Healthcare, GlaxoSmithKline, Gilead, and Merck

Rocky Road → New Horizon

First line ART regimens target
HIV enzymes:
Reverse Transcriptase (3)
Integrase (4)
Protease (6)
Source:
AIDS Info

Integrase Inhibitors
• Raltegravir (3 pills daily for full regimen)
• Elvitegravir/cobicistat (has booster)
• Dolutegravir (dual combinations, three-drug STR, or
other combinations)
• Bictegravir (oral co-formulation with FTC/TAF)
• Cabotegravir (IM long-acting, oral)

SHOULD EVERY PERSON
WITH HIV BE ON AN
INTEGRASE INHIBITOR?Naïve, suppressed and failing patients

7
Registrational Treatment-Naive Clinical Trials: Cross-Study Comparison*
HIV RNA <50 c/mL at Week 48
66686868686969707071
73767676777878
808282838484
868788
90
0 10 20 30 40 50 60 70 80 90 100
NRTI backbone
FTC/TDF
3TC/ABC qd
3TC+ABC bid
3TC/ZDV
3TC+TDF
% of Patients with HIV-1 RNA <50 copies/mL at Week 48
*This slide depicts data from multiple studies published from 2004-2012. Not all regimens have been compared head-to-head in a clinical trial
STARTMRK RAL (n=281)8
CASTLE ATV+RTV (n=440)6
ABT 730 LPV/r qd (n=333)5
CASTLE LPV/r (n=443)6
GS 934 EFV (n=243)4
MERIT ES EFV (n=303)3
KLEAN LPV/r (n=444)14
ECHO/THRIVE EFV (n=546)10
ABT 730 LPV/r bid (n=331)5
GS-102 QUAD (n=348)11
GS-103 QUAD (n=353)12
GS-103 ATV+RTV (n=355)12
GS-102 Atripla (n=352)11
MERIT ES MVC (n=311)3
ARTEMIS DRV+RTV (n=343)7
ECHO/THRIVE RPV (n=550)10
GS-903 EFV (n=299)9
STARTMRK EFV (n=282)8
GS 934 EFV (n=244)4
ARTEMIS LPV/r (n=346)7
KLEAN FPV/r (n=434)14
CNA 30024 EFV (n=324)13
CNA 30024 EFV (n=325)13
SOLO FPV/r (n=322)2
SOLO NFV (n=327)2
CNA 30021 EFV (n=386)1
CNA 30021 EFV (n=384)1

Era of Integrase Inhibitors
90%87%
82% 82%83%81%
71%69%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
FLAMINGO WAVES ARIA DAWNING
Viro
log
ica
lly s
up
resse
d p
atie
nts
(%
)
DTG DRV/r
(n=243
)
(n=245
)
DTG ATZ/r
(n=248
)
(n=247
)
DTG LPV/r
(n=257
)
(n=215
)
2 31 4
1. Clotet B, et al. Lancet 2014;383:2222−31; 2. Squires K, et al. Lancet HIV 2016;3:e410−20; 3. Orrell C, et al. Lancet 2017;S2352-3018:30095-4; 4 . Llibre JM, et
al. 24th CROI. Seattle, 2017. Abstract 44LB.
• Clinical trials favoring INSTI over boosted PI
EVG/c ATZ/r
(n=289
)
(n=286
)
SINGLE STUDY:
DTG superior to
EFV
bPI: drug
interactions
and
comorbidities
RESISTANCE
ADVANTAGE

BIC/FTC/TAF vs DTG-Containing Regimens
• No resistance for any regimen components detected for either group
1. Gallant J, et al. Lancet. 2017;[Epub ahead of print]. 2. Sax PE, et al. Lancet. 2017;[Epub ahead of
print].
GS-1489: Wk 48 Virologic
Efficacy[1]
GS-1490: Wk 48 Virologic
Efficacy[2]
Pts
(%
)
Pts
(%
)
100
80
60
40
20
0HIV-1 RNA
< 50 c/mL
HIV-1 RNA
≥ 50 c/mL
No Virologic
Data
BIC/FTC/TAF (n = 314)
DTG/ABC/3TC (n = 315)
92 93
1 3 7 4
100
80
60
40
20
0HIV-1 RNA
< 50 c/mL
HIV-1 RNA
≥ 50 c/mL
No Virologic
Data
BIC/FTC/TAF
DTG + FTC/TAF
8993
4 16
0
99> 99
1 <
1
60
PP1°
Treatment difference: -
0.6%
(95% CI: -4.8% to 3.6%) Treatment difference (1°):
-3.5%
(95% CI: -7.9% to 1.0%)

Transmitted resistance by drug class in US (CDC data)

Are Baseline Resistance Genotypes Still
Needed?• Modeling analysis of clinical benefit and cost-
effectiveness of baseline genotype vs no genotype if
starting a DTG plus dual NRTI regimen
• Results
• Baseline genotype provides minimal projected impact on survival (<
1 day)
• Not cost-effective – $420,000/quality-adjusted life year gained
• Only beneficial under extreme parameters – e.g., < 50% viral
suppression in the setting of transmitted NRTI resistance
• Limitation: Modeling analysis; does not take into account
starting with or switching to two-drug regimens
Hyle E, et al. Clinical Infectious Diseases
2019.

International first line guidelines
EACS
(2018)1
DHHS
(2018)2,3
IAS–USA
(2018)4
WHO
(2018)6
NRTI
backbone
TAF/FTC
TDF/FTC
ABC/3TC*
TAF/FTC
TDF/FTC
ABC/3TC*
TAF/FTC
ABC/3TC*
2 NRTIs†
NNRTI RPV* – – -
INSTI BIC
DTG
RAL
BIC
RAL
DTG
DTG
BIC
DTG‡
PI DRV/c or /r – – –
BIC, bictegravir; c, cobicistat; DRV, darunavir; DTG, dolutegravir;; EVG, elvitegravir; FTC, emtricitabine;; r, ritonavir; RAL, raltegravir; RPV, rilpivirine; TAF, tenofovir
alafenamide fumarate; TDF, tenofovir disoproxil fumarate. *Use recommended only if baseline viral load <100,000 copies/mL.†Optimised backbone should be used.‡ Women and adolescent girls of childbearing potential with consistent and reliable contraception and who are fully informed of the benefits and risks can use DTG
1. EACS. Available from: http://www.eacsociety.org/guidelines/eacs-guidelines/eacs-guidelines.html. 2. DHHS. Available from: https://aidsinfo.nih.gov/guidelines/html/1/adult-
and-adolescent-arv/0. 3. DHSS. Available from: https://aidsinfo.nih.gov/news/2044/adult-arv-panel-classifies-bic-taf-ftc-as-recommended-initial-regimen-for-hiv. 4. Saag MS et al.
JAMA 2018;320:379-396. 5.. All URLs accessed July 2018.
Recommended and preferred regimens-

SHOULD EVERY PERSON
WITH HIV BE ON AN
INTEGRASE INHIBITOR?NAIVES- A LOT OF PATIENTS CONSIDERING THE
GUIDELINES AND THE NEW DTG/3TC APPROACH

Switching to a New 3-drug Regimen
Works
VL < 50
BTG
TAF
FTC
DTG
ABC
3TC
DTG
TAF
FTC
DRV/c
TAF
FTC
Pros Cons
There is an integrase
inhibitor combination
to address almost any
concern

Pre-existing NRTI ResistanceStudy 380-4030
*20 participants stratified to categories 1 or 2 based on investigator-suspected NRTI resistance (19 participants category 2, and 1 participant category 1); †Includes K65R/E/N, or ≥3 TAMs that include M41L or L210W, or T69 insertions; ‡Includes only M184V/I mutations confirmed by genotype.
Catego
ry
NRTI Mutation,
n (%)
Stratificatio
n at
randomizati
on*
n=565
Final
analysis
n=565
B/F/TAF
n=284
DTG +
F/TAF
n=281
1K65R/E/N or ≥3
TAMs† 15 (3) 30 (5) 16 (6) 14 (5)
2 Any other pattern 63 (11) 108 (19) 55 (19) 53 (19)
3No NRTI
mutation487 (86) 427 (76) 213 (75) 214 (76)
M184V/I‡ ± other
mutations
(from category 1 or 2)
29 (5) 81 (14) 47 (17) 34 (12)
M184V/I‡ only 12 (2) 21 (4) 15 (5) 6 (2)
♦ For more details on the resistance mutations in study 380-4030, see poster MOPEB241
15

<1
93
61
91
8
0
20
40
60
80
100
HIV-1 RNA
<50 c/mL
HIV-1 RNA
≥50 c/mL
No Virologic
Data
1
284
3
281
265
284
256
281
22
281
18
284
Virologic Outcome at Week 48Study 380-4030
• Switching to B/F/TAF was noninferior to remaining on DTG + F/TAF
• No participant with pre-existing NRTI resistance had HIV-1 RNA ≥50 c/mL in either group
CI, confidence interval. 16
Treatment Difference in % Participants With HIV-1 RNA
≥50 c/mL (95.001% CI)
-… 1.0
-0.7
-4 -2 0 2 4
Favors
B/F/TAF
Favors
DTG + F/TAFDTG+ F/TAF
(n=281)
B/F/TAF (n=284)
Virologic Outcome by FDA
Snapshot
Pa
rtic
ipa
nts
, %
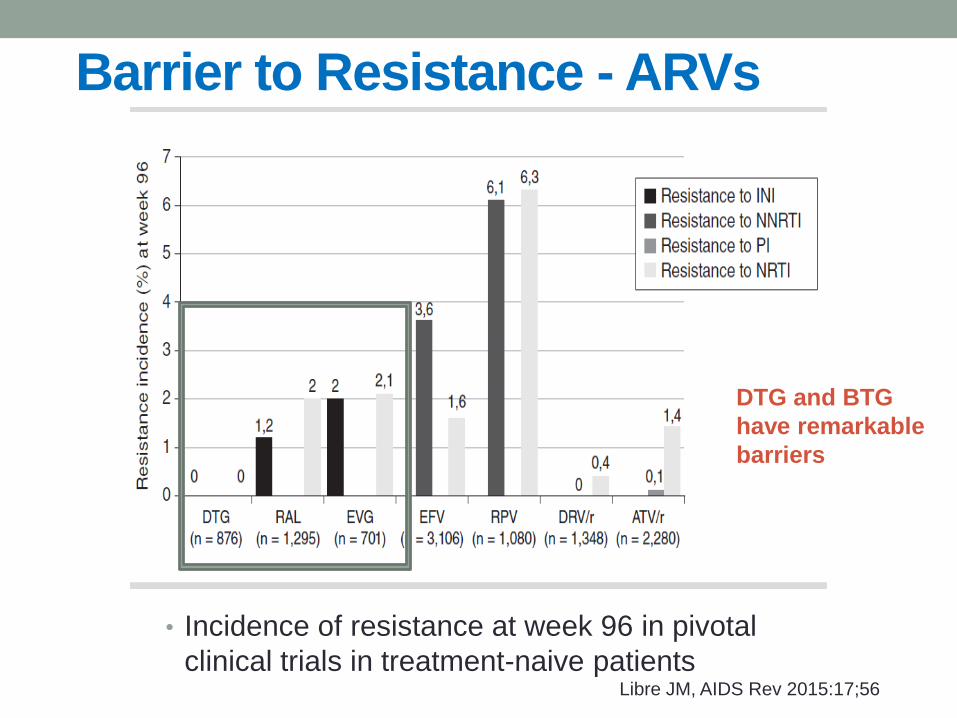
Barrier to Resistance - ARVs
• Incidence of resistance at week 96 in pivotal
clinical trials in treatment-naive patientsLibre JM, AIDS Rev 2015:17;56
DTG and BTG
have remarkable
barriers
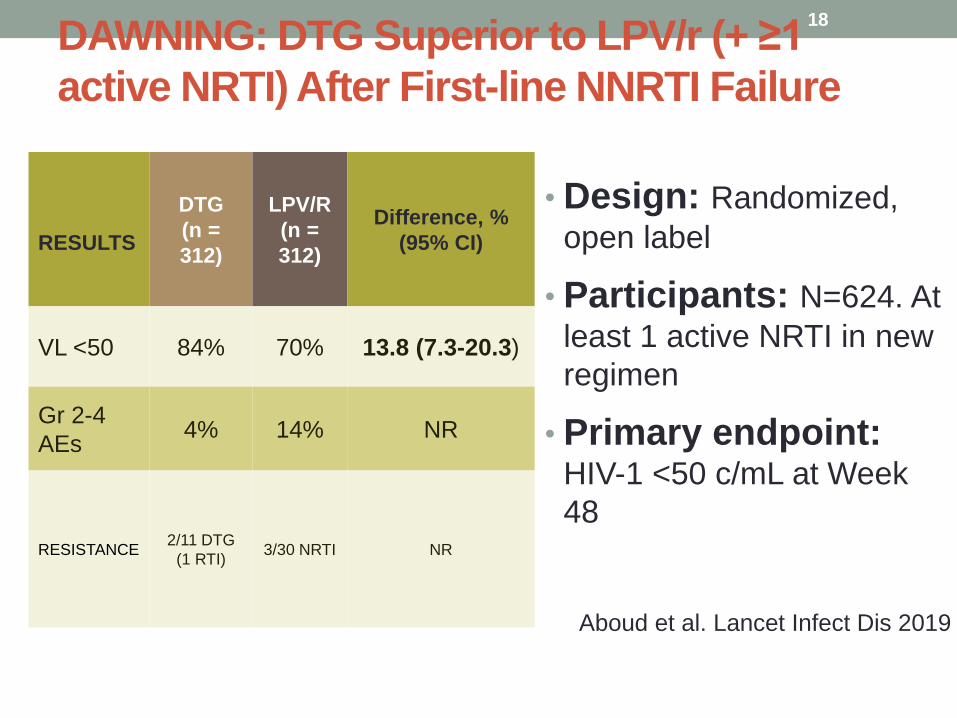
DAWNING: DTG Superior to LPV/r (+ ≥1
active NRTI) After First-line NNRTI Failure
• Design: Randomized,
open label
• Participants: N=624. At
least 1 active NRTI in new
regimen
• Primary endpoint: HIV-1 <50 c/mL at Week
48
18
Aboud et al. Lancet Infect Dis 2019
RESULTS
DTG
(n =
312)
LPV/R
(n =
312)
Difference, %
(95% CI)
VL <50 84% 70% 13.8 (7.3-20.3)
Gr 2-4
AEs4% 14% NR
RESISTANCE2/11 DTG
(1 RTI)3/30 NRTI NR

DOLUTEGRAVIR AFTER INTEGRASE INHIBITOR
FAILURE
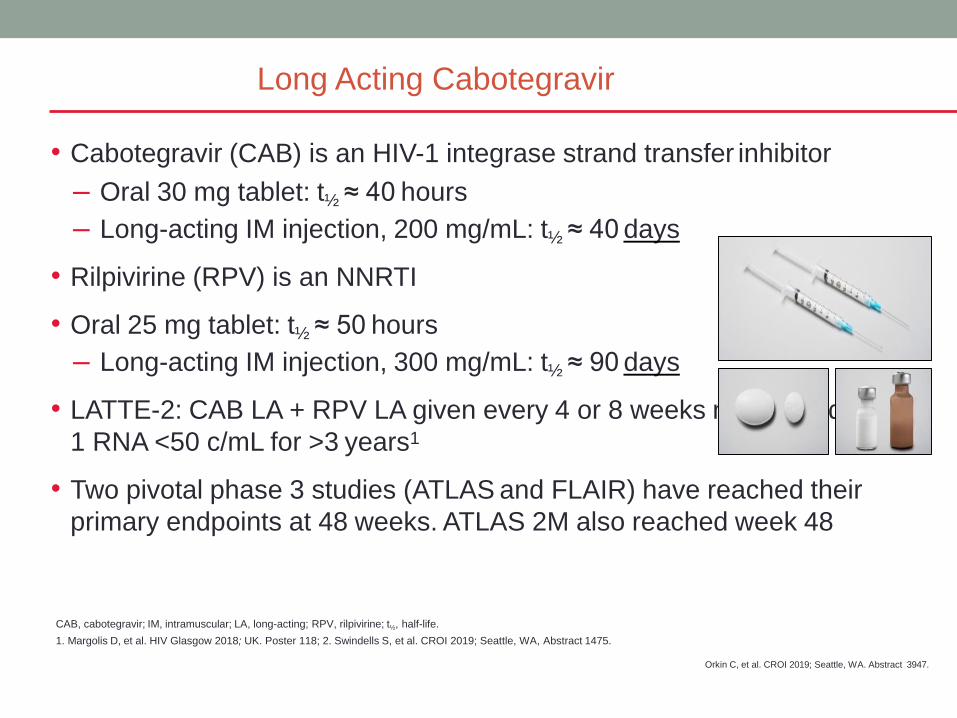
• Cabotegravir (CAB) is an HIV-1 integrase strand transfer inhibitor
– Oral 30 mg tablet: t½ ≈ 40 hours
– Long-acting IM injection, 200 mg/mL: t½ ≈ 40 days
• Rilpivirine (RPV) is an NNRTI
• Oral 25 mg tablet: t½ ≈ 50 hours
– Long-acting IM injection, 300 mg/mL: t½ ≈ 90 days
• LATTE-2: CAB LA + RPV LA given every 4 or 8 weeks maintained HIV-
1 RNA <50 c/mL for >3 years1
• Two pivotal phase 3 studies (ATLAS and FLAIR) have reached their
primary endpoints at 48 weeks. ATLAS 2M also reached week 48
Long Acting Cabotegravir
Orkin C, et al. CROI 2019; Seattle, WA. Abstract 3947.
CAB, cabotegravir; IM, intramuscular; LA, long-acting; RPV, rilpivirine; t½, half-life.
1. Margolis D, et al. HIV Glasgow 2018; UK. Poster 118; 2. Swindells S, et al. CROI 2019; Seattle, WA, Abstract 1475.
Conference on Retroviruses and Opportunistic Infections;

SHOULD EVERYONE BE ON
AN INTEGRASE INHIBITOR?TREATMENT EXPERIENCED PATIENTS- A LOT OF
PATIENTS CAN, PARTICULARLY DTG OR BTG; AND
NOW WITH DTG/3TC AND DTG/RPV

Integrase inhibitors: a host of benefits
• Avoid Boosting
• Excellent resistance barrier with DTG and BTG
• Limited drug interactions
• No food restrictions
• New concepts (DTG/RPV, DTG/3TC, CAB LA + LA RPV)
• Special populations
• Pregnancy (RAL)
• TB (DTG) . NOT BTG
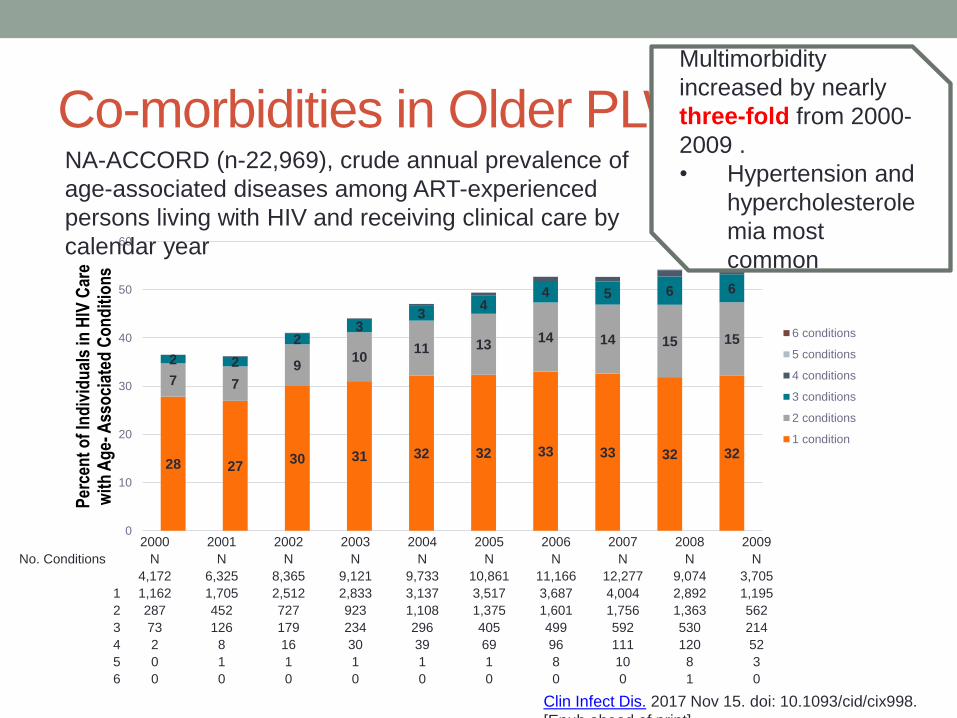
Co-morbidities in Older PLWHIV
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
No. Conditions N N N N N N N N N N
4,172 6,325 8,365 9,121 9,733 10,861 11,166 12,277 9,074 3,705
1 1,162 1,705 2,512 2,833 3,137 3,517 3,687 4,004 2,892 1,195
2 287 452 727 923 1,108 1,375 1,601 1,756 1,363 562
3 73 126 179 234 296 405 499 592 530 214
4 2 8 16 30 39 69 96 111 120 52
5 0 1 1 1 1 1 8 10 8 3
6 0 0 0 0 0 0 0 0 1 0
28 2730 31 32 32 33 33 32 32
7 7
910
11 1314 14 15 15
2 2
23
34
4 5 6 6
0
10
20
30
40
50
60
Per
cen
t o
f In
div
idu
als
in H
IV C
are
wit
h A
ge-
Ass
oci
ated
Co
nd
itio
ns
6 conditions
5 conditions
4 conditions
3 conditions
2 conditions
1 condition
NA-ACCORD (n-22,969), crude annual prevalence of
age-associated diseases among ART-experienced
persons living with HIV and receiving clinical care by
calendar year
Clin Infect Dis. 2017 Nov 15. doi: 10.1093/cid/cix998.
[Epub ahead of print]
Multimorbidity
increased by nearly
three-fold from 2000-
2009 .
• Hypertension and
hypercholesterole
mia most
common

Weight Gain and INSTIs: Data From
CROI 2019
Positive Association
• NA-ACCORD, initial
therapy
(N = 24,001)[1]
• ACTG A5001, A5322
switch cohort (N =
691)[2]
• Women’s Interagency
HIV Study, switch
cohort (N = 1118)[3]
No Association
• TRIO retrospective
switch cohort (N =
3468)[4]
• HPTN 077 cohort of
HIV-uninfected people
receiving cabotegravir
(N = 199)[5]
1. Bourgi. CROI 2019. Abstr 670. 2. Lake. CROI 2019. Abstr 669. 3. Kerchberger. CROI 2019 Abstr 672.4. McComsey. CROI 2019. Abstr 671. 5. Landovitz. CROI 2019. Abstr 34.
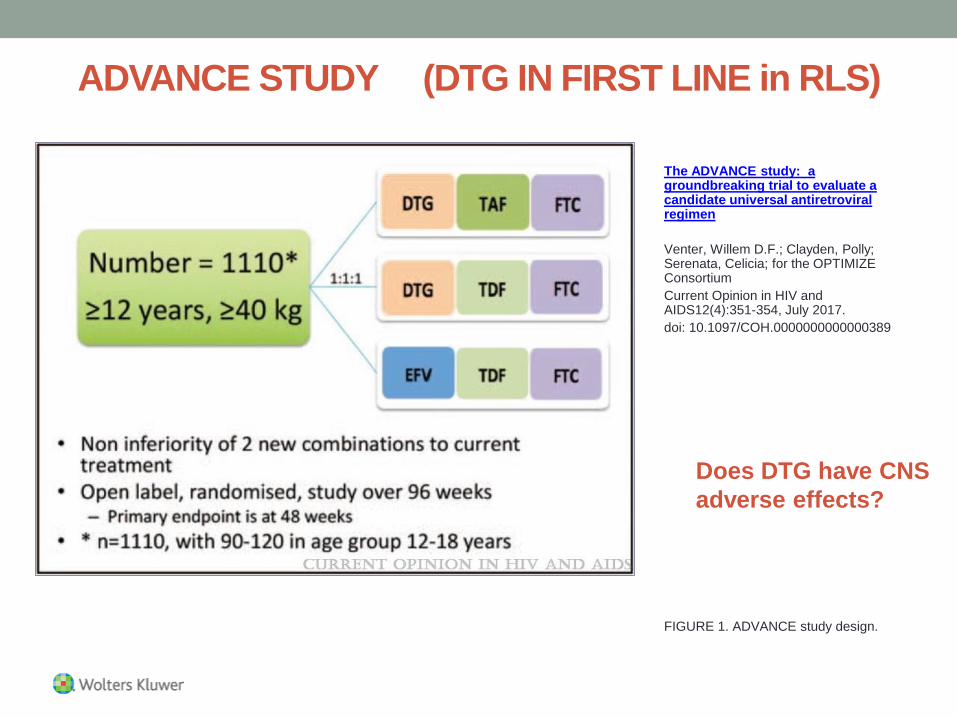
ADVANCE STUDY (DTG IN FIRST LINE in RLS)
FIGURE 1. ADVANCE study design.
Copyright © 2017 Wolters Kluwer Health, Inc. All rights reserved. 25
The ADVANCE study: a groundbreaking trial to evaluate a candidate universal antiretroviral regimen
Venter, Willem D.F.; Clayden, Polly; Serenata, Celicia; for the OPTIMIZE Consortium
Current Opinion in HIV and AIDS12(4):351-354, July 2017.
doi: 10.1097/COH.0000000000000389
Does DTG have CNS
adverse effects?

ADVANCE Study: Changes in Weight
Dolutegravir-Based Regimen at Week 96
Dolutegravir
+F/TAF
(n=351)
Dolutegrav
ir
+ F/TDF
(n=351)
Efavirenz/F/
TDF
(n=351)
Mean weight change (kg)
Overall
Men
Women
+8*†
+5*
+10*‡
+5*
+4*
+5*
+2
+1
+3
≥10% change in body weight (%) 25*† 13* 11
Treatment-emergent obesity (BMI ≥30
kg/m2; %)
19*† 8* 4
*P<0.001 versus efavirenz/F/TDF; †P<0.01 versus dolutegravir + F/TAF, and ‡P<0.001 versus dolutegravir + F/TDF.
Hill A, et al. J Int AIDS Soc. 2019;22(suppl 5):92. Abstract MOAX0102LB.Venter WF, et al. N Engl J Med. 2019;July 24, 2019. [Epub ahead of print].

?BICTEGRAVIR/FTC/TAF

CONCLUSION
• ART is in the integrase inhibitor era
• DTG and BTG provide options across the ART continuum
• Newer approaches include dual ART (DTG/3TC,
DTG/RPV) and CAB LA regimens
• New association with weight gain needs further
investigation to quantify risk, isolate risk factors, and
understand consequences

Conclusion