renal 4 2017 october 30, 2017 nrosci/biosci i070 renal...
TRANSCRIPT

Renal42017 October30,2017
1
NROSCI/BIOSCII070
RenalPhysiology4
Todaywewillfocusontheregulationoftheosmolalityoftheblood(andbodyfluids).NotethatlasttimewediscussedhowADHreleaseissensitivetochangesinpOsm,andADHcanrapidlyadjustwaterexcretiontomaintainanormalplasmaosmolality.However,indoingso,ADHwouldalsoalterbodyfluidvolume.[slide1]Thus,thereneedstobeamechanismtoindependentlyregulateexcretionofosmoles,ifbodyfluidvolumeweretobemaintained.Notethattotalfluidvolumeisnotascriticalaparameterasosmolality(why?)andthereforedoesnotneedtoberegulatedasrapidlyorsensitively.ThisiscertainlyreflectedinthedifferentsensitivitiesofADHsecretionforchangesinvolumeandosmolality.
Interstitialfluidis~300mOsm/L(actuallyalittleless,~290).ThisismadeupprimarilyofNa+andthenegatively-chargedionsassociatedwithit.PlasmaNa+istypicallyaround140-145mOsm/L(or140-145mEq/L,sinceforamonovalentionosm=Eq).Na+andtheassociatedanionsaccountforgreaterthan90%ofECFosmolality.
Thecontrolofplasmaosmolality(pOsm),whichistheninequilibriumwithinterstitialfluidosmolality,isdonebyregulatinghowmuchwaterthereistodiluteorconcentratethesolutes.Therearetwomajormechanismstoaccomplishthis:controlofwaterloss(relativetosolute)bythekidneysandcontrolofwaterintake(thirst).Osmolalityisregulatedbyalteringwaterintakeandexcretionrelativetothenumberofosmoles(whichisprimarilyNa+).Howeverthenumberofosmolesinthebodyisalsoacriticalcomponentofthisregulation.AndsinceNa+isthemajorosmole,let’sconsidertheregulationofNa+excretion.
Slide2:

Renal42017 October30,2017
2
[simplifiedversion–slide3]Na+isfreelyfilteredintheglomerulusandthenreabsorbedbyactivetransportinmostsegmentsofthetubulesystem.(Whichsegmentsdon'ttransportNa+?)Aswithwater,~2/3oftheNa+isreabsorbedintheproximaltubule(indeed,it’stheNa+that’scausingthereabsorptionofwater),andthisisaccomplishedlargelybyprimaryactivetransport(i.e.,theNa-K-ATPase)atthebasolateralmembraneandvariousprocessesontheapicalmembrane,includingsecondaryactivetransportofothersolutes(e.g.,glucose,aminoacids)[slide4].Anadditional25-30%oftheNa+isreabsorbedintheascendinglimboftheLoopofHenle(slide5),andherethemaintransporterontheapicalmembraneistheNa-K-2Cltransporter.However,theregulatedportionofreabsorptionoccursdistaltotheloopofHenle,inthecollectingduct.Beforewetalkaboutthat,afewothercommentsonthenon-regulatedprocessesofNa+reabsorption.[slides6,7,8]ThecontrolofNa+reabsorptionisprimarilyunderthecontrolofasinglehormone,aldosterone.[slide9]Aldosteroneisasteroidhormonereleasedfromtheadrenalcortex.AldosteroneactsonthecorticalcollectingductstopromoteNa+reabsorption(activetransport).Intheabsenceofaldosterone,approximately2%ofthefilteredloadofNa+isexcretedintheurine.(Thismaynotsoundlikealot,butgiventhatthefilteredloadofNa+is~25,OOOmillimoles/day,2%representsalotofNa+.)Incontrast,inthepresenceofhighconcentrationsofaldosterone,essentiallyallNa+isreabsorbed.Therefore,~98%ofthefilteredloadofNa+isreabsorbedinanon-regulatedmanner,whereastheexcretionof~2%ofthefilteredloadishighlyregulated.HowdoesaldosteroneincreaseNa+reabsorption?[slide10]AldosteronecausesthesynthesisofnewNa+,K+-ATPasemoleculesthatgetinsertedintothebasolateralmembraneinthecorticalcollectingducts.Inaddition,aldosteronestimulatestheinsertionofNachannelsintotheluminalmembrane.(Itisinterestingtonotethataldosteronealsohasasimilareffectintheintestines,whichactstopromoteNa+absorptionfromthediet.)Thisactionofaldosterone,likemostactionsofsteroidhormones,ismediatedviaanactiononthegenome,tocauseincreasedtranscription,increasedmRNA,andincreasedsynthesisoftheseproteinsinvolvedinNatransport.NotethatNaK-ATPaseexpressionintheproximaltubuleisnotregulatedbyaldosterone.
[slides11-15providesomeadditionalcomplexitytothis,andaddinsomeofthemorerapideffectsofaldosteroneonregulationofthesetransporters.]

Renal42017 October30,2017
3
So,aldosteronecontrolsthereabsorptionofNa+.[slide16]Thisleadstothequestionofwhatcontrolsthereleaseofaldosterone.Theprimarystimulusforaldosteronesecretionisangiotensinactingonthealdosterone-releasingcellsoftheadrenalcortex.(K+alsoactsdirectlytoincreasealdosteronerelease;we'llcomebacktothis.)Therenin-angiotensinsystem[slide17]:Reninisreleasedfromthejuxtaglomerularcells,whichlieadjacenttothemaculadensa.Reninisanenzymethat,inblood,causesthesynthesisofangiotensin1fromangiotensinogen(alsocalledreninsubstrate).Angiotensinogen,whichissynthesizedintheliver,istypicallypresentinrelativelyhighconcentration,sotheproductionofangiotensin1isdependentupontheamountofcirculatingrenin.Angiotensin1isthenconvertedtoangiotensinII(theactivehormone)byangiotensinconvertingenzyme,whichislocalizedinpulmonarycapillaries.(Whatitthesignificanceofsuchlocalization?)AngiotensinIIhasalargenumberofactionsinadditiontostimulatingaldosteronesecretion,allofwhichacttomaintainbloodpressureandplasmavolumeandosmolality.So,angiotensinIIhasabunchofactions,whichpromptsthequestionofwhatinitiatesthis.Whatisthestimulusforreninsecretion.[slide18]Thereare3primarystimuliforrenninrelease:sympatheticinnervationofthejuxtaglomerularcells(beta-adrenergicreceptorstimulatedreninsecretion),themaculadensa,andintrarenalbaroreceptors(theJGcellsthemselvesarestretch-sensitive;lessstretch,whichreflectslowerrenalperfusionpressure,stimulatesreninsecretion)

Renal42017 October30,2017
4
Onemorethingabouttherenin-angiotensinsystemwhilewearetalkingaboutit:inrecentyearsthewholesystemhasgottenwaymorecomplex(slide19).Nowinadditiontotheclassicangiotensinsystem,thereisACE2generatingAng1-7;thereisareceptorforreninitself,andmore….[TheonlypointIwanttomakehereisthatthisisanactiveareaofresearch,withnewtwistsandturns.]Inadditiontoaldosterone,otherhormonesinfluenceNa+reabsorption.[slide20]AngiotensinIIappearstoactdirectlyontheproximaltubuletopromoteNa+reabsorption,asdoessympatheticinnervationofthekidney.Atrialnatriuretichormone,releasedfromtherightatriuminresponsetostretchpromotesNa+excretion.AtrialnatriuretichormonedecreasesNareabsorption,andalsoincreasesGFR(whichpromotesNaexcretion).[Anaside:Recentdataalsoindicatethatoxytocin,releasedfromtheposteriorpituitaryinresponsetoincreasedosmolality,isalsonatriuretic(atleastinsomespecies)Thoughoxytocinmayalsoincreasereninsection(atleastinsomespecies)sotheeffectsofoxytocinmightbequitecomplicated.].Also,sympatheticinnervationofproximaltubulepromotesNareabsorption.Notethatwehavementioned3thingsthatsympatheticinnervationofthekidneysinfluence:reninsecretion,Nareabsorption,andrenalbloodflow[slide21].These3effectsofsympatheticinputtothekidneyaredifferentiallysensitivetorenalnerveactivityandaremediatedbydifferenttypesofadrenergicreceptors.Briefcommentonsaltappetiteandcontributionofsaltintaketosodiumbalance.(slide22)Briefcommentonsalt,bloodpressure,andabriefcommentondietarysaltanddietarysaltrecommendations.(slides23,24,25)Slide26:aniceflowchartforyoutoworkthrough.
Renal42017 October30,2017
5
WhataboutK+?K+doesnotcontributesubstantiallytoosmolality;itsextracellularfluidconcentrationisquitelow(~4.2mEq/L).However,theextracellularfluidlevelofK+mustbemaintainedwithinnarrowlimitsfornormalfunctionofcells[slide27],especiallyexcitablecells.K+isfreelyfilteredintheglomerulusandlargelyreabsorbed.[slide28,29]Regulationoccursbysecretionatthelevelofthecorticalcollectingducts.Thisregulationisprimarilybyaldosterone.RememberthatonestimulusforaldosteronereleaseisadirectactionofincreasedextracellularK+levelonthealdosterone-releasing:cells.AldosteroneincreasesNa/K-ATPaseinthecollectingducts,whichwouldpromoteK+secretion.[slide30]
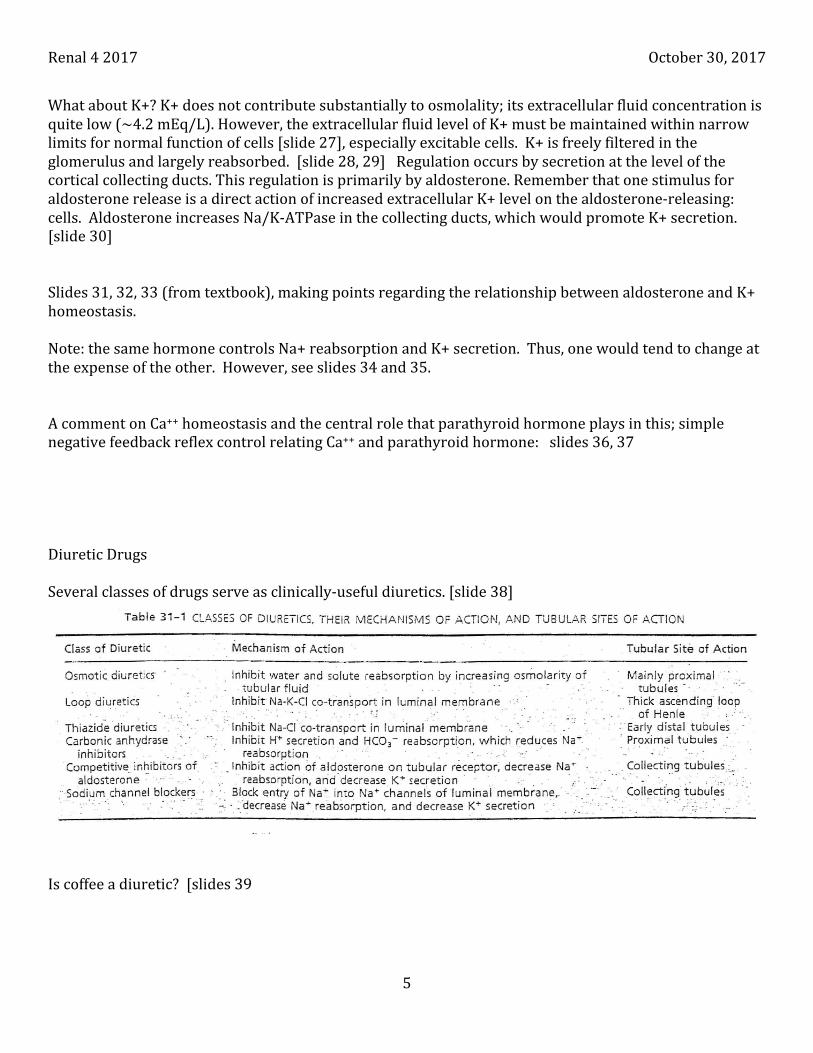
Slides31,32,33(fromtextbook),makingpointsregardingtherelationshipbetweenaldosteroneandK+homeostasis.Note:thesamehormonecontrolsNa+reabsorptionandK+secretion.Thus,onewouldtendtochangeattheexpenseoftheother.However,seeslides34and35.AcommentonCa++homeostasisandthecentralrolethatparathyroidhormoneplaysinthis;simplenegativefeedbackreflexcontrolrelatingCa++andparathyroidhormone:slides36,37DiureticDrugsSeveralclassesofdrugsserveasclinically-usefuldiuretics.[slide38]
Iscoffeeadiuretic?[slides39

Renal42017 October30,2017
6
Theroleofthekidneyinlong-termpHregulation.InthecollectingtubuleH+reabsorptionorsecretion(andtheoppositewithbicarbonate)isalteredinresponsetoplasmaH+(slides44-45).Giventhehighconcentrationofbicarbonateintheplasma,thefilteredloadofbicarbonateislargeandthevastmajorityis“reabsorbed”intheproximaltubule.Thewordreabsorbedwasplacedinquotations,becauseasillustratedinslides46and46itisnottheactualbicarbonatemoleculesinthetubulefluidthataretransportedintotheperitubularcapillaries.Recentlyrenalnervedenervationhasreceivedconsiderableattentionasatreatmentforhypertension[slides48-54].Doesitwork?Yes,no,yes…Why?RenalDialysis[slides55-56]

Renal42017 October30,2017
7