relationship between ventricular ectopic beat...
TRANSCRIPT

PVC FREQUENCY AND HEART RATE/Winkle
pendent of the carotid baroreflex. Phenylephrine andnitroglycerin affect venous compliance and venous re-turn to the heart, in addition to their effects on theperipheral arterial tree. Neck suction or pressure maychange venous return from the head or may influenceaortic baroreceptors in a direction opposed to the pre-sumed effect on carotid baroreceptors. When the ob-tained results from different studies using differentmeasurement techniques are discrepant, and when, asin our study, the obtained results in the same subjectsvary with the measurement technique, these operation-al definitions of baroreflex sensitivity become mean-ingless. We therefore caution clinical investigatorsagainst drawing inferences about overall baroreflexfunction on the basis of a single measurementtechnique.
AcknowledgmentThe authors gratefully acknowledge the assistance of Joan Folio,
R.N., and Bert Chidakel in conducting this study.
References1. Kezdi P: Baroreceptors and Hypertension. New York, Pergamon,
19672. Bristow JD, Honour AJ, Pickering GW, Sleight P, Smyth HS:
Diminished baroreflex sensitivity in high blood pressure. Circula-tion 39: 48, 1969
3. Takeshita A, Tanaka S, Kuraiwa A, Nakamura M: Reduced baro-receptor sensitivity in borderline hypertension. Circulation 51:738, 1975
4. Korner PI, Tonkin AM, Uther JB: Valsalva constrictor and heartrate reflexes in subjects with essential hypertension with normalblood pressure. Clin Exp Pharmacol Physiol 6: 97, 1979
5. Pickering TG, Sleight P: Quantitative index of baroreflex activityin normal and hypertensive subjects using Valsalva's manoeuvre.Br Heart J 31: 392, 1969
6. Bevegard S, Castenfors J, Danielson M: Carotid baroreceptorfunction in hypertensive patients. Scand J Clin Lab Invest 37: 495,1977
7. Mancia G, Ludbrook J, Ferrari A, Gregorini L, Zanchetti A: Baro-receptor reflexes in human hypertension. Circ Res 43: 170, 1978
8. Mancia G, Ferrari A, Gregorini L, Parati G, Ferrari MC, Pomi-dossi G, Zanchetti A: Control of blood pressure by carotid sinusbaroreceptors in human beings. Am J Cardiol 44: 895, 1979
9. Ludbrook J, Mancia G, Zanchetti A: Does the baroreceptor-heartrate reflex indicate the capacity of the arterial baroreceptors tocontrol blood pressure? Clin Exp Pharmacol Physiol 7: 499, 1980
10. Eckberg DL, Cavanaugh MS, Mark AL, Abboud FM: A simplifiedneck suction device for activation of carotid baroreceptors. J LabClin Med 85: 167, 1975
11. Zanchetti A, Mancia G, Malliani A: Alterations of cardiovascularreflexes in hypertension. Clin Exp Hypertension 2: 451, 1980
12. Mancia G, Ferrari A, Gregorini L, Bianchini C, Terzoli L, LeonettiG, Zanchetti A: Methyldopa and neural control of circulation inessential hypertension. Am J Cardiol 45: 1237, 1980
The Relationship Between Ventricular EctopicBeat Frequency and Heart Rate
ROGER A. WINKLE, M.D.
SUMMARY We examined the relationship between the frequency of premature ventricle complexes(PVCs) and underlying heart rate in 24 patients with frequent PVCs using 24-hour ambulatory ECGrecordings. Plots of PVC frequency vs heart rate were made at 1-beat/min intervals for all heart rates thatwere recorded for at least 5 minutes of the 24 hours. Heart rates during 24 hours ranged from 56 + 10.0 to102.2 ± 15.4 beats/min. Twenty-three of the 24 patients had a distinct relationship between PVC frequencyand heart rate. Patterns included an approximate log-linear increase in PVCs at higher heart rates in 12patients, a log-linear decrease (overdrive suppression) in one patient, flat curves in three patients, and a
complex relationship (e.g., more PVCs at low rates and suppression at high rates) in seven patients.Patterns were reproducible in 21 of the 24 patients on repeat ambulatory ECG monitorings done 1 day to 2months later. We conclude that most patients with frequent PVCs have a characteristic relationship betweenPVC frequency and heart rate over the range of heart rates achieved during routine daily activity. The mostfrequent relationship is a marked increase in PVC frequency with increasing heart rate. These observationsmay in part explain such phenomena as "spontaneous" variability of PVC frequency, sleep suppression ofPVCs and suppression of PVCs by f3-blocking drugs.
A DIRECT RELATIONSHIP between ventricular ec-topic beat frequency and heart rate has been reported inanimal studies.' 2 Similarly, most clinicians have ob-served patients in whom ventricular arrhythmias seemrelated to underlying heart rate. Examples are the
From the Cardiology Division, Stanford University Medical Center,Stanford, California.
Address for correspondence: Roger A. Winkle, M.D., CardiologyDivision, Stanford University Medical Center, Stanford, California94305.
Received August 11, 1981; revision accepted December 7, 1981.Circulation 66, No. 2, 1982.
emergence of ventricular escape beats in patients withsinus bradycardia or complete atrioventricular blockand exercise-induced or overdrive suppression of ven-tricular arrhythmias. These observations are usuallymade over short recording periods and at heart rateshigher or lower than those achieved during most ordi-nary daily activities. The present study is a report ofthe relationship between the occurrence of ventricularectopic beats and underlying heart rate in a group ofambulatory patients with frequent ventricular ectopicbeats. The analysis of long periods of ECG recordingsusing computer techniques allowed us to uncover rela-
439
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL 66, N) 2, AUGUST 1982
tionships between frequency of premature ventricularcomplexes (PVCs) and heart rate that are not readilyappreciated in many patients by examining the datafrom standard ECG strips.
MethodsTwenty-four-hour, two-channel ambulatory ECG
recordings were analyzed from 24 patients at StanfordMedical Center. Patients were randomly selected fromthose with frequent chronic ventricular ectopic beatsreferred for participation in antiarrhythmic drug proto-cols. To be included in this report, patients had to havemore than one PVC per minute averaged over 24 hourson an initial ambulatory ECG recording and to have asecond 24-hour ECG monitoring available for analy-sis. Both recordings were done after discontinuing allantiarrhythmic drugs for at least 5 half-lives.
Ambulatory ECG analysis was performed using theStanford computerized system.3' This system pro-vides identification of all PVCs recorded on a 24-hourrecording. Each beat is classified as supraventricularor ventricular in origin. Ventricular ectopic beats arethose with wide QRS complexes and no preceding Pwave. The accuracy of ventricular ectopic beat countsare verified by selecting random minutes during eachrecording and by selecting a representative sampling ofminutes containing arrhythmias. During these selectedminutes, beat-by-beat annotation of each QRS com-plex is obtained. All digitized ECG data are stored on arandom access disc or on magnetic tape for easy re-trieval and review of data. Fortran programming per-mits easy implementation of new data analysisalgorithms.We generated tabular and graphic information con-
cerning the frequency of ventricular ectopic beats as afunction of heart rate. In this algorithm, the averageheart rate is established for each minute during the 24hours by averaging all RR intervals during each min-ute. The number of PVCs is also tabulated for eachminute. The number of minutes at each heart rate (in 1-beat/min increments) is determined, as well as the totalnumber of PVCs in these minutes. The number ofPVCs per 15 minutes is calculated for each heart rateaccording to the formula (number of PVCs in all min-utes at a given heart rate/the number of minutes at agiven heart rate) x 15. The number of PVCs per 15minutes can be thought of as the number of PVCs thatoccur for each 15 minutes spent at any given heart rate.Heart rates recorded for less than 5 minutes of the 24hours were not analyzed. Patients with interpolatedPVCs were excluded from analysis because theywould have an artifactual increase in heart rate at highPVC frequencies. Data were plotted as the log of thenumber of PVCs per 15 minutes as a function of heartrate. The graphs were inspected visually to estimatethe relationship between PVC frequency and heart ratefor each patient. The second 24-hour ambulatory ECGmonitoring was compared with the initial recording todetermine if patterns were reproducible over time.
ResultsPatients
Twenty-four ambulatory ECG recordings from 24patients (18 males and six females, average age 60.3± 10.5 years, range 36-76 years) were studied. Thir-teen patients had coronary artery disease, eight ofwhom had a previous myocardial infarction and six ofwhom had previous coronary bypass grafting. Threepatients each had atypical chest pain and primary myo-cardial disease, two had apparently normal hearts andone patient each had mitral valve prolapse, sleep apneasyndrome and paroxysmal, nonsustained ventriculartachycardia.
PVC Frequency and Minimum and Maximum Heart RatesThe median PVC frequency on the initial ambula-
tory ECG recordings was 8672 per 24 hours (range1499-60,477 per 24 hours). The lowest heart rate re-corded for at least 5 minutes during the 24-hour record-ing was 56.2 ± 10.0 beats/min (range 37-72 beats/min) and the highest heart rate recorded for at least 5minutes was 102.2 ± 15.4 beats/min (range 61-122beats/min). On the second ambulatory ECG recording,the median number of PVCs was 10,976 per 24 hours(range of 3029-50,307 per 24 hours), and low andhigh heart rates were not significantly different fromthe initial recording, averaging 58.8 ± 8.8 beats/min(range 40-80 beats/min) and 100.0 ± 12.0 beats/min(range 68-121 beats/min).
Relationship Between PVC Frequency and Heart RateTwenty-three of the 24 patients showed a distinct
relationship between PVC frequency and heart rate.While there were almost as many patterns of this rela-tionship as there were patients, the relationships wereclassified into broad categories. Twelve patientsshowed a positive correlation between PVC frequencyand heart rate (fig. 1-3). The slopes of this relationshipvaried from only slightly to markedly positive. Somesubjects with a positive slope showed a tendency to-ward slight flattening of the curves at higher heart rates(fig. 3). Seven patients showed a complex relationshipbetween PVC frequency and heart rate. Overall, mostsubjects with complex patterns tended to have morePVCs at higher heart rates. Some of these patients hadreproducible dips or notches in their relationships andothers had an increasing PVC frequency at lower heartrates, a flat relationship at intermediate heart rates andoverdrive suppression (a negative correlation betweenPVC frequency and heart rate) at the highest heart ratesachieved (fig. 4). Three patients showed a relativelyflat curve at all heart rates, indicating equal numbers ofPVCs at each heart rate. One patient had a predomi-nantly negative pattern, showing fewer PVCs at higherheart rates (fig. 5). Only one subject had no apparentrelationship between PVC frequency and heart rate.There was no correlation between type of underlyingheart disease and pattern of the relationship betweenPVC frequency and heart rate.
CIRCULATION440
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

PVC FREQUENCY AND HEART RATE/Winkle
3/27/80 4/11/80
w
ziL0U1)
C;CL
1U
J1- E,~1:-_
40 60 80 100 120 40 60 80 100 120HEART RATE HEART RATE
FIGURE 1. (left) The relationship between frequency ofpremature ventricular complexes (PVCs) and heart rate in a 52-year-oldfemale with mitral valve prolapse. Each point represents the number ofPVCs every 15 minutes spent at each heart rate (in I -beatlminincrements) recordedfor at least 5 minutes during the 24-hour recording. The PVCfrequency is plotted on a logarithmic scale, andthere is a striking and linear increase in PVCfrequencies as heart rate increases from just below 70 beats/min to approximately 120beatslmin. (right) The same data in this patient approximately 2 weeks later. The two graphs are very similar.
Reproducibility
Repeat ambulatory ECG monitorings were carriedout 1 day to 2 months after the initial recording (figs.1-5). Of the 23 patients showing a relationship be-tween PVC frequency and heart rate on the initial re-cording, 21 showed reproducibility of this pattern onthe repeat monitoring. In a qualitative sense, this re-producibility was judged excellent in 11 patients, goodin five patients and fair in five patients. Reproducibil-ity did not seem to be a function of number of daysbetween recordings. The graphic pattern was repro-ducible, but in some patients, the PVC frequency-heart rate curve shifted slightly upward or downwardor to the right or left from one recording to the next.
DiscussionThis study shows a remarkable correlation between
ventricular ectopic beat frequency and underlyingheart rate in patients with frequent PVCs. The majorityof patients have a relationship between PVC frequencyand heart rate that is characteristic for that patient and
is reproducible over time. Heart rate-dependent ven-tricular ectopy has been described in dogs after acutecoronary artery ligation. Chadda et al.2 showed moreventricular ectopic beats at rapid and slow heart ratesand could demonstrate an "optimal antiarrhythmicheart rate. " Han et al. I also found that the heart rate isan important determinant of PVC frequency in dogssubjected to ischemic, physiologic or electrical stress.Data in man on this subject are limited. Zipes andKnoebell reported two subjects with recent myocardialinfarction in whom atropine-induced tachycardia wasassociated with an increase in ventricular ectopy. Mostclinicians have seen patients in whom ventricularectopy was either induced or suppressed by exercise.Although such patients are known to exist, one of themore remarkable findings in our study was that a highpercentage of patients with frequent PVCs had definiteand reproducible relationships between PVC frequen-cy and underlying heart rate. This observation wasclearly related to the availability of computer analysisof 24-hour electrocardiographic strips that enabled de-tection of subtle or complex relationships between
w
I-z
tL
b0.
441
I100(
10C
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

VoCL 66, No 2. AUGUST 1982
10/15/80
1000
cowI-z
10100T-coU)0C
1C
1000
c)w
z
,, 100I-C)
a.
10
11/10/80
40 60
HEART RATE HEART RATEFIGURE 2. Relationship between frequency ofpremature ventricular complexes (PVCs) and heart rate for a 60-yxear-old male with coronary artery disease. The positive correlation between PVCfrequency and underlying heartrate was reproducible over 3'1 weeks.
PVC frequency and heart rate. These relationshipswere detected even though no attempt was made toevaluate the relationship between PVC frequency andheart rate for each PVC morphology. Some of thecomplex patterns may have resolved into the sum of anumber of simpler relationships if such a separationhad been made. The heart rates achieved during theseambulatory ECG monitorings are considerably belowthose achieved during a routine exercise treadmill test.Some of our patients with a positive relationship be-
3/20/80
w
X-
z2
I-CO
100
tween PVC frequency and heart rate might have shownoverdrive suppression had they achieved heart ratesduring everyday activity similar to those during exer-cise testing.
Potential MechanismsThese observations do not permit statements about
the mechanism of the observed relationship betweenPVC frequency and heart rate, or that they are causeand effect. However, one may speculate on the reasons
4/21/80
C')w
z
C')b0-cn)
1000°
I_ I_
10 4 60 I8 -640 60 80 100
HEART RATE HEART RATEFIGURE 3. The relationship betweenfrequency ofpremature ventricular complexes (PVCs) and heart rate in a 62-year-old male withno evidence of organic heart disease. PVC frequency increased with heart rate, and the PVC curve tended to flatten at heart ratesgreater than 60-70 beatslmin. The pattern is reproducible over a period of approximatelv I month.
I
IeX -.a B ---7-
CIRCULATION442-
vO
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
PVC FREQUENCY AND HEART RATE/Winkle43
2/28/80
1000
40 60 80 100 120
HEART RATE
cowI-z
LOT-
U)b
140 60 80 100 120
HEART RATE
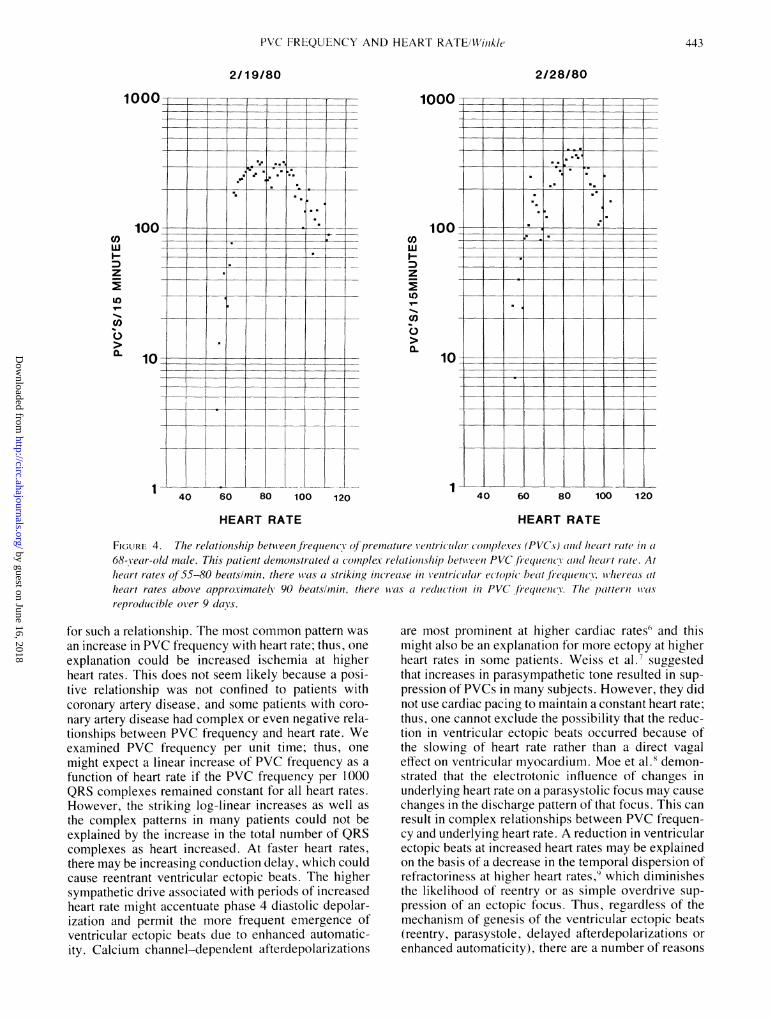
FIGURE 4. The relationtship between frequencY of premature ventricular comnplcexes (PVCs) and/ hieart i-tate in68-year-old mnale. This patient demonistrated complex relaItioIislip lbetween PVC,frequencC( vX(811( heart ratei. Atleart rates of 55-80 beatslmin, there was a strikinlg increase in ventricular ectopic bheat frequency, whereas at
hieart rates above (ipproximatelh 90 beatsl/min, there ivas ta reductltionl in PVC firequencY. The 1)attern-1wasreproducible over 9 days.
for such a relationship. The most common pattern was
an increase in PVC frequency with heart rate; thus, one
explanation could be increased ischemia at higherheart rates. This does not seem likely because a posi-tive relationship was not confined to patients withcoronary artery disease, and some patients with coro-
nary artery disease had complex or even negative rela-tionships between PVC frequency and heart rate. Weexamined PVC frequency per unit time; thus, one
might expect a linear increase of PVC frequency as a
function of heart rate if the PVC frequency per 1000QRS complexes remained constant for all heart rates.However, the striking log-linear increases as well as
the complex patterns in many patients could not beexplained by the increase in the total number of QRScomplexes as heart increased. At faster heart rates,there may be increasing conduction delay, which couldcause reentrant ventricular ectopic beats. The highersympathetic drive associated with periods of increasedheart rate might accentuate phase 4 diastolic depolar-ization and permit the more frequent emergence ofventricular ectopic beats due to enhanced automatic-ity. Calcium channel-dependent afterdepolarizations
are most prominent at higher cardiac rates'3 and thismight also be an explanation for more ectopy at higherheart rates in some patients. Weiss et al.7 suggestedthat increases in parasympathetic tone resulted in sup-
pression of PVCs in many subjects. However, they didnot use cardiac pacing to maintain a constant heart rate;thus, one cannot exclude the possibility that the reduc-tion in ventricular ectopic beats occurred because ofthe slowing of heart rate rather than a direct vagaleffect on ventricular myocardium. Moe et al.8 demon-strated that the electrotonic influence of changes inunderlying heart rate on a parasystolic focus may cause
changes in the discharge pattern of that focus. This can
result in complex relationships between PVC frequen-cy and underlying heart rate. A reduction in ventricularectopic beats at increased heart rates may be explainedon the basis of a decrease in the temporal dispersion ofrefractoriness at higher heart rates,9 which diminishesthe likelihood of reentry or as simple overdrive sup-
pression of an ectopic focus. Thus, regardless of themechanism of genesis of the ventricular ectopic beats(reentry, parasystole, delayed afterdepolarizations or
enhanced automaticity), there are a number of reasons
2/19/80
c)wI-z
I')
U)
0-
1
443
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

Voil 66. No 2. Avi(rs-r 1982
4/21/81
1000-
100
CO)
>a-
10
I_z
IL)T-
CO0a.
4/24/81
50 70 90 ll1HEART RATE
l0 130 50 70 90 110 130
HEART RATE
FIGURE 5. Relationship between frequencc ofpremature ventric ular (Yompleses (PVCs) and ieart r(lte in 36-Year-old male with coronary arterv disease. The overall pattern of decreasing PVC frequency with increasingheart rate in the range of58-100 beatslmin is uSnusual and is noted in only ti miniority of subjects: this patienit wasthe only one in the present study showing this pattern. Such patients often have increases in ventricular ectopicbeats during sleep and exacerbation of ventricular ectopic beats when givenfl-blocking dr-ugs. There is a smliallnotch in this patient's curve near a heart rate qf 70 beatslmin. While the patternis on each recording date (resimilar, thev are not identical. The recording on the left showts 100 PVC.s per 15 mi/luwtes at a hiert ratite oJ'60 beattslmin, whereas the recording dotne 3 daxs later at the same heart rate show.s aI PVCfrequency' o'fapproximnately 200per 15 minutes.
to anticipate that a relationship should exist betweenheart rate and PVC frequency.
Implications for Spontaneous Variationof Ventricular Ectopic Beats
The relationships between PVC frequency and heartrate described in this study might account for a part ofthe spontaneous variability in PVC frequencies pre-viously reported.'0 " Although we did not examinethis issue directly, several patients' graphic outputs ofPVC frequency and heart rate over time clearly sug-gested that this is the case: What appears to be sponta-neous variation in PVC frequency over time couldclearly be shown to be associated with changes inunderlying heart rate (fig. 6). However, the findings inthe present report can only partially account for thespontaneous variation in ventricular ectopic beats. Al-though the overall pattern of the relationship betweenPVC frequency and heart rate were reproducible fromone recording to the next in most of our patients, in
some instances the curves were shifted slightly upwardor downward or to the right or left, suggesting aninfluence of the autonomic nervous system or otherfactors. Because the vertical axis in our graphic out-puts is a logarithmic scale, slight shifts in the curveupward or downward results in striking differences inventricular ectopic beat frequency even if heart rate isheld constant from one 24-hour period to the next.
Implications for Sleep Suppressionof Ventricular Ectopic BeatsMany subjects with ventricular ectopic beats have
fewer arrhythmias during sleep.'- '3 Although in-creases in parasympathetic tone have been postulatedto account for these changes, for many patients sleepsuppression or enhancement of ventricular ectopicbeats may merely be an extension of the relationshipbetween PVC frequency and heart rate that occurs alsowhile that subject is awake (fig. 6). Pickering et al.,'4who studied the sleep suppression of PVCs in 12 pa-
444 CIRCULATION
-
L
+t-
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

PVC FREQUENCY AND HEART RATE/Winkle
3 7 11tPM 3 7 11AM
FiloURE 6. The relation.ship betweeni "spontaneous variation offrequenxy premature ventricular complexes(PVCs) and changes in heart rate. These data are,from a 62-year-old male with coronary arterv disease. Thispatient's PVC frequency vs heart rate plot vvIs similar to that ofthe patienit shown in figure 1, i.e., a steep, log-
lintear increase in PVCJfrequencv at inc reasing heart rates. The parallel changes in heart rate and PVCfrequencXsluggest that the changes in PVC frequency are niot spontaneous, but are due to changes in heart rate. At nightthere i.s a marked reduction of PVC frequenc-y that might be termed ''sleep'' suppression. Howvever, there is a
similar falIl in PVCfrequency at 11 a. m. to 1 p. m. when the patient is awake but has a slows heart rate similar to
that during sleep.
tients, concluded that the nocturnal decrease correlatedmore closely with a change in heart rate than with levelof arousal. During wakefulness, similar changes inPVCs could be produced by administering propranololor phenylephrine.
Implications for Studying Antiarrhythmic DrugsComputer analysis of ambulatory ECG recordings
as described in this study may provide new techniquesof assessing and potentially predicting response toantiarrhythmic drugs. The findings that the majority ofsubjects have an increase in PVC frequency as a func-tion of heart rate during 24-hour ambulatory ECG re-
cordings may in part explain the findings that the ma-
jority of patients have a reduction in ventricular ectopicbeats when treated with /3-blocking agents.' h Thedocumentation of fewer PVCs at higher heart ratesmight help to identify patients whose arrhythmias
would be worsened by /3-blocking drugs or might besuppressed by overdrive pacing. The evaluation ofPVC frequency as a function of heart rate may providea new and powerful tool for understanding the mecha-nism of action of and predicting response to antiar-rhythmic agents.
AcknowledgmentThe authors thank Dr. John Fitzerald and Debbie Bragg-Remschel for
developing the computer program used in this study. Inez Rodriguez for
analyzing the FCG recordings. and Glenda Rhodes for secretarialassistance.
References1. Han DeTraglia J, Millet D. Moe GK: Incidence of ectopic beats
as a function of basic rate in the ventricle. Am Heart J 72: 632,1966
2. Chadda KD. Banka VS, Helfant RH: Rate dependent ventricularectopia following acute coronary occlusion: the concept of an opti-
wI-
'C
100
50
1000
co i
1I
11 AM
445
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

446 CIRCULATION
mal antiarrhythmic heart rate. Circulation 49: 654, 19743. Bragg-Remschel DA, Harrison DC: A computerized two channel
ambulatory arrhythmia analysis system. In Computers in Cardiolo-gy. IEEE 80 CHI 606-3. Williamsburg, Virginia. October 22-24,1980, pp 197-200
4. Fitzgerald JW, Winkle RA, Alderman EL, Harrison DC: Comput-er analyzed ambulatory electrocardiograms for predicting and eval-uating responses to antiarrhythmic agents. In Computers in Cardi-ology, IEEE Proceedings. Rotterdam, The Netherlands. October1975, pp 151-154
5. Zipes DP, Knoebel SB: Rapid-dependent ventricular ectopy: ad-verse responses to atropine-induced rate increase. Chest 62: 255,1972
6. Wit AL, Rosen MR: Cellular electrophysiology of cardiac arrhyth-mias. Part I. Arrhythmias caused by abnormal impulse generation.Mod Concepts Cardiovasc Dis 50: 1, 1981
7. Weiss T, Lattin GM, Engelman K: Vagally mediated suppression
of premature ventricular contractions in man. Am Heart J 89: 700.1975
8. Moe GK, Jalife J, Mueller WJ, Moe B: A mathematical model ofparasystole and its application to clinical arrhythmias. Circulation56: 968, 1977
9. Han J, Millet D, Chizzonitti B, Moe GK: Temporal dispersion ofrecovery of excitability in atrium and ventricle as a function of
VOL 66. No 2, AUGUST 1982
heart rate. Am Heart J 71: 481, 196610. Winkle RA: Antiarrhythmic drug effect mimicked by spontaneous
variability of ventricular ectopy. Circulation 57: 1116, 197811. Morganroth J, Michelson EL, Horowitz LN, Josephson ME, Pearl-
man AS, Dunkman WB: Limitations of routine long-term electro-cardiographic monitoring to assess ventricular ectopic frequency.Circulation 58: 408, 1978
12. Lown B, Tykocinski M, Garfein A, Brooks P: Sleep and ventricu-lar premature beats. Circulation 48: 691, 1973
13. Winkle RA: Circadian variations in ventricular ectopic activity. InManagement of Ventricular Tachycardia Role of Mexilitine,edited by Sand0e E, Julian DG, Bell JW. Amsterdam, ExcerptaMedica, 1978, pp 165-169
14. Pickering TG. Johnston J. Honour AJ: Comparison of the effects ofsleep, exercise and autonomic drugs on ventricular extrasystoles,using ambulatory monitoring of electrocardiogram and electroen-cephalogram. Am J Med 65: 575, 1978
15. Winkle RA, Gradman AH, Fitzgerald JW: Antiarrhythmic drugeffect assessed from ventricular arrhythmia reduction in the ambu-latory electrocardiogram and treadmill test: comparison of propran-olol, procainamide and quinidine. Am J Cardiol 42: 473, 1978
16. Woosley RL, Kornhauser D, Smith R, Reele S, Higgins SB, NiesAS, Shand DG, Oates JA: Suppression of chronic ventricular ar-rhythmias with propranolol. Circulation 60: 819, 1979
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
R A WinkleThe relationship between ventricular ectopic beat frequency and heart rate.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1982 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.66.2.439
1982;66:439-446Circulation.
http://circ.ahajournals.org/content/66/2/439the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from