reducing sepsis mortality - · pdf filecontinuous quality improvement the principal diagnosis...
TRANSCRIPT
Reducing Sepsis Mortality
Kathy Lopez-Bushneil, William S. Demaray, and Cathy jaco
I nfection at any body site canlead to sepsis, a primary bloodstream infection. Sepsis caused
over 34,800 deaths in 2007, andremains the leading cause of deathin noncardiac intensive care units(Xu, Dochanek, Murchy, & Tejada-Vera, 2010). Mortality rates due tosepsis have remained unchanged forthe last several decades, rangingfrom 23% to 43% (Durthaler, Ernst,& Johnston, 2009). The cost of sepsisin the United States is over $400 bil-lion annually (Vodovotz & Billiar,2013; World Health Organization,2011).
Literature ReviewSepsis is the leading cause of death
in hospitalized patients and has sub-stantial impact on health careresources. Sepsis is difficult to identifybecause the signs and symptoms areoften subtle, and they mirror thesigns and symptoms of other condi-tions (Gaieski, Edwards, KaUan, &Carr, 2013). About 1.6 million peopleare treated in U.S. hospitals annuallyfor sepsis, and this number has morethan doubled in recent years (Powell,Khare, Courtney & Feinglass, 2010).A thorough literature review on theeffect of protocols on sepsis outcomeswas conducted using CINAHL,Cochrane Database of SystematicReviews, PubMed, National GuidelineClearinghouse, ISI Web of Know-ledge, and Ebsco Discovery Servicefor 2009-2013.
The use of standardized order setsfor the management of sepsis shouldbe recommended strongly for betterperformance in treatment. Standardorder sets use serum lactate valuesbecause of the relationship to organdysfunction in sepsis (Mikkelsen et
Sepsis is the leading cause of death in hospitalized patients and hassubstantial impact on health care resources. An evidence-basedproject reduced mortality rates associated with sepsis through useof a nursing sepsis protocol.
al., 2009). Miller and colleagues(2013) found using standard ordersets for sepsis reduced mortality for4,329 adult patients in intensive careunits (ICU) from 21.7% to 9.7% in 6years (2004-2010). As the standardorder set compliance increased, amarked reduction in hospital mor-tality occurred. Similar findings werenoted in older adults when the useof standardized order sets for sepsiswas associated with reduced mortali-ty and reduced length of staybecause of improved initial appropri-ate therapy (Heppner et al., 2012).
The majority of cases of sepsis areidentified in ICUs and emergencyrooms; however, management ofpatients on medical-surgical units candecrease mortality and costs becausenurses will identify symptoms andinitiate the sepsis bundle early(Daniels, Nutbeam, McNamara, &Galvin, 2011). Signs and sjmiptomsof sepsis include fever, chills, alteredwhite blood count, increased C-reac-tive protein, tachycardia, altered skinperfusion, and reduced urine output.Because symptoms of sepsis may berecognized late and treated inappro-
priately, nurses must learn to identifyand report them promptly in anycare setting (Vincent et al., 2002).
ImprovementNeeds/Group Oversight
To reduce mortality rates, sepsismust be identified and treated asearly as possible. The SurvivingSepsis Campaign (SSC), which wasformed in 2002 to reduce sepsis by25% in 5 years, published evidence-based guidelines for the treatment ofpatients with sepsis and septic shock(Durthaler et al., 2009). These guide-lines provide 17 recommendations;the three most frequently used wereprompt ordering of cultures, admin-istration of broad-spectrum antibi-otics, and deep vein thrombosis pro-phylaxis. Deterioration of laboratoryvalues is the most common clue tosevere sepsis (Durthaler et al., 2009).
In 2008, leaders of the Universityof New Mexico Hospital (UNMH)reported 21.7% of patient deathswere related to sepsis, with one-thirdof these deaths reported by the inter-nal medicine service. Sepsis was also
Kathy Lopez-Bushnell, EdD, MPH, MSN, APRN, is Director of Nursing Research, University ofNew Mexico Hospitals, Albuquerque, NM.
William S. Demaray, RT, is Respiratory Therapist, University of New Mexico Hospitals,Albuquerque, NM.
Cathy Jaco, IVISN, RN, is Director of Quality Resources, Great River Health System, Burlington,lA.
MEDSURG isrxjns iisro. ¡anuary-February 2014 • Vol. 23/No. 7
Continuous Quality Improvement
the principal diagnosis in 33% ofpatients who died in 2007 at UNMH.Nurses worked with the internalmedicine physicians, memhers ofthe quality outcomes department,and the Rapid Response Team (RRT)in developing a sepsis protocol forpiloting on two medical-surgicalunits. Nurses also developed thescreening tool for sepsis. Members ofthis interdisciplinary group calledthemselves the Sepsis MortalityImprovement Team (SMITe), andtheir goal was to reduce the numberof mortalities due to sepsis on thegeneral units.
CQI ModelThe Institute for Healthcare Im-
provement (IHI) Model used for thisprogram included setting aims,forming teams, establishing meas-ures, and selecting and testingchanges. The process included Plan-Do-Study-Act (PDSA), engaging phy-sicians in the improvement and exe-cution, improving capacity andcapability, and engaging staff inimprovement and quality improve-ment. The Severe Sepsis Bundle (IHI,2013) was revised in June 2013 toinclude the 3-hour resuscitation andthe 6-hour septic shock bundles. The3-hour bundle includes measuringlactate levels, obtaining blood cul-tures, administering broad-spectrumantibiotics, and infusing crystalloidfor hypotension or lactate increases.The 6-hour bundle includes measur-ing central venous pressure and cen-tral venous oxygen, and remeasuringlactate if initial values were elevated.The project hospital is part of theSSC. In this article, findings of thework of the multidisciplinary teamand the decreased sepsis-relatedmortality are described (D'Angelo,Doefler, Parmentier, & Jacobsen,2013).
Quality Indicators and DataCollection
To reach the goal of reducing sep-sis-related mortality, members of theSMITe realized laboratory and hemo-dynamic variables were needed torecognize patients with systemicinflammatory response syndrome
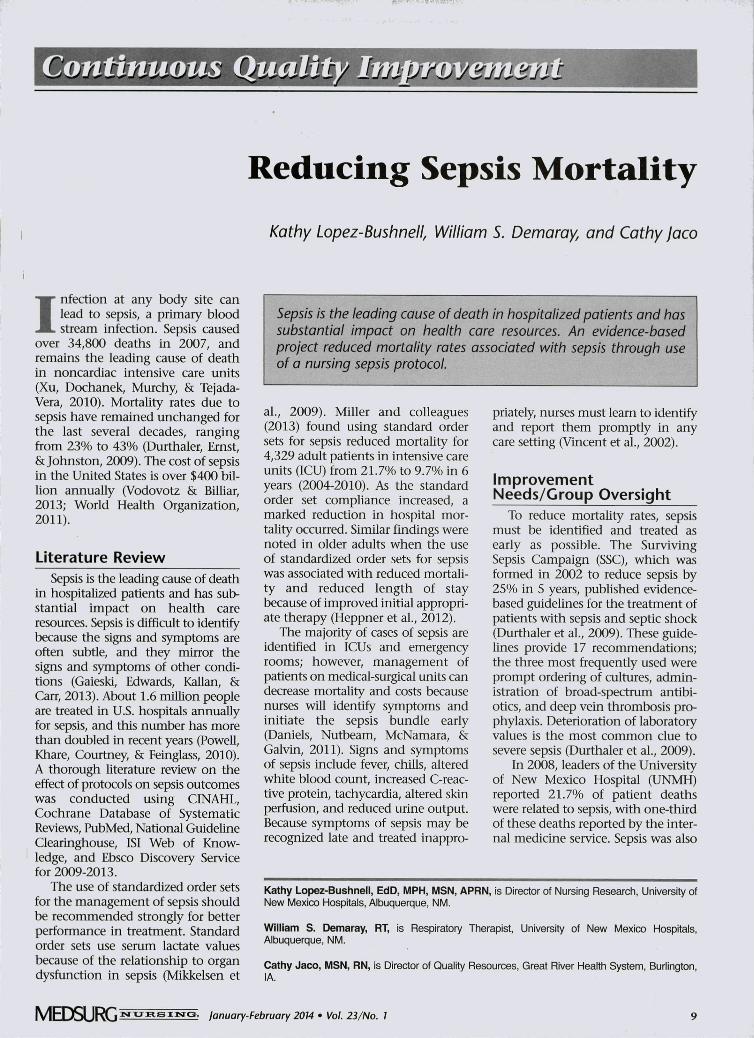
FIGURE 1.Sepsis Screening Tool Performed Twice Daily
InstructionsUse this tooi to screen patients for sepsis on the floors, in the ICU, or ED.
Sections A, B, C: Unit RN complete Sections D, E: RRT/ICU/ED staff complete
Date: / / Time: RN Initials:.D Sepsis Order Set initiated within last 24 hours - STOP screening - Reassess at
next shift
A. INFECTION (Does the patient have a documented, or do you suspect infection?)
D Suspected/documented infection: D No infection
B. SIRS Criteria - Assess for two or more of the following (check all that apply):D Temp s 38 C or s 36 C D Resp rate a 20 or PaC02 s 32D HR s 90 D WBC a 12K or s 4K or a 10% bands
D Less than two of above. STOP screening - Reassess at next shift.
C. SEPSISIf you checked the box that an infection is present in Part A and at least two boxesin Part B, patient has screened positive for sepsis:1. Draw lactate.2. Notify the MD - request orders to initiate
Labs drawn @Lactate results @
Sepsis Order Set.D Sepsis Order Set NOT initiated, per physician. STOP screening - Reassess at
next shiftReason:D Sepsis Order Set initiated (preprinted order set is required) - Continue to Step 3
3. Notify the RRT, 555-1234, to follow patient if order set initiated or if lactate isabnormal (>2)
Time: RRT/ICU/ED Initials:.
D. ORGAN DYSFUNCTIOND No organ dysfunction -Patient on the D YELLOW PATHWAY D GREEN PATHWAYD Acutely altered mental status D Platelet count <100,000D SBP < 90 or MAP < 65 mmHg D Billirubin >2 mg/dl, AST >90, ALT >90D SpO2 < 90% on room air D Lactate >4 mol/L
or supplemental O^D Creatinine > 2 mg/dl or urine output < 0.5 ml/kg/hr for > 2 hours
E. SEVERE SEPSIS - RED PATHWAYIf at least one box checked in section D, patient has screened positive forSEVERE SEPSIS.D Contact MD to continue severe sepsis resuscitation bundle.D Severe sepsis bundle not implemented per physician. Reason:
* Remind MD to document in chart the reason for not initiating order set.
Patient Label
(SIRS) in response to infection andassociated with acute organ dysfunc-tion at the earliest possible stage.Differentiating them from patientswith sepsis, severe sepsis, or septicshock was also critical. The UNMHRapid Response Team would assess.
monitor, and target patients formore aggressive treatment and ap-propriate nursing care. The methodused by the SMITe was innovativeand different from other nationalprograms because pilots were begunon medical-surgical units rather than
10 ¡anuary-February 2014 • Vol. 23/No. 1 M E D S U R G
Mobility/Activity Circles: A Quality Improvement Effort to Reduce Falls
in intensive care and emergency set-tings. Medical-surgical units werechosen because nurses in those areasare the primary responders to deteri-oration. The sepsis bundle comprisesbasic care elements that can be deliv-ered in these areas as well as morecomplex tasks requiring critical care.The most effective interventions -rapid delivery of fluids and adminis-tration of intravenous antibioticswithin 1 hour - can reduce mortalityby 30%-50% (Daniels et al., 2011;Vincent et al, 2002).
A nursing unit director wasapproached by an internal medicinephysician to initiate this evidence-based sepsis project in collaborationwith other nursing unit leaders. Thenurse unit directors, physicianchampion, and quality consultantselected and reviewed the literatureand adopted the evidence for earlyrecognition of sepsis. Recognizingthe significance of the sepsis diagno-sis for the medicine units as well asthe impact on mortality for the hos-pital, nurses on two units volun-teered to participate in this qualityinitiative through their shared gover-nance councils. Nurses on the unitswere introduced to the SurvivingSepsis Guidelines developed by theEuropean Society of Critical CareMedicine and the Society of CriticalCare Medicine (Durthaler et al.,2009), with the goal of improvingsepsis diagnosis, management, andsurvival of affected patients. Thenurses took a 4-hour continuingeducation course titled "SurvivingCritical Care Medicine." Members ofthe interdisciplinary team developedadditional inservlce training oppor-tunities for direct-care nursing staffconcerning initial resuscitation,screening for sepsis, and perform-ance improvement, diagnosis, andantimicrobial therapy. An intranetsite was developed to display dataand provide additional educationalmaterials.
Recognizing the importance ofrapid continuous improvement cy-cles, nurses on the units participatedin testing the tools and makingmodifications, using one patient at atime. The tools were tested and mod-ified based on review by two nursesor a nurse and physician who identi-
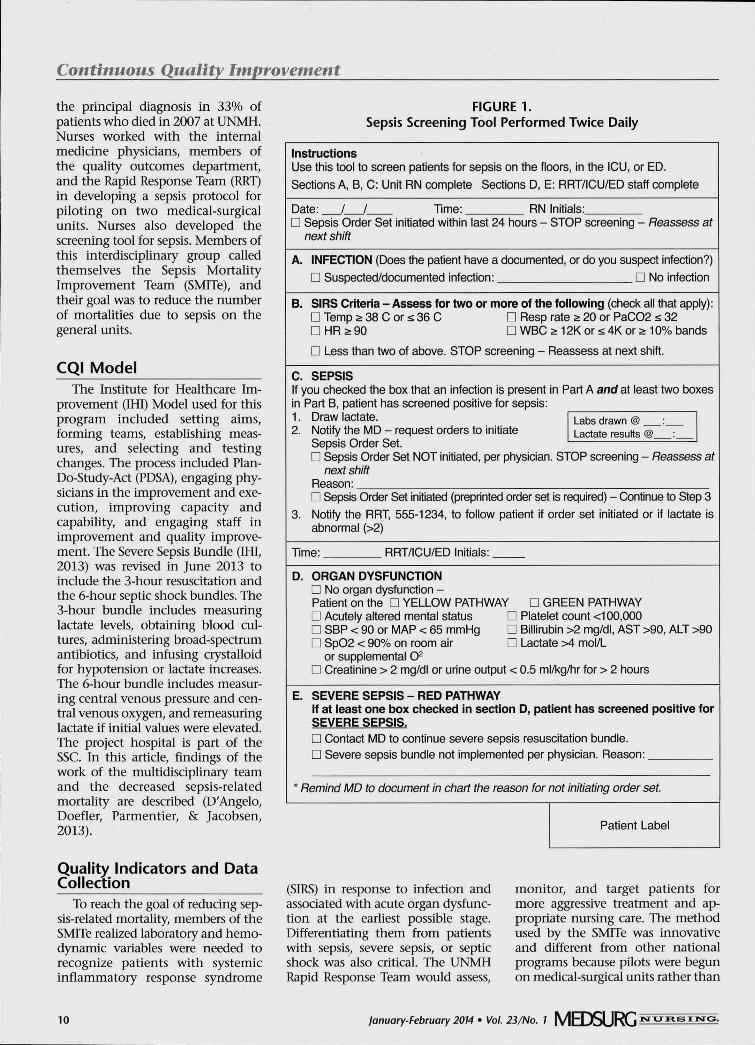
FIGURE 2.Verbal Order Telephone Scripts
Nurse Call Script: Positive Sepsis ScreenIf you fiave a positive screen, draw lactate, then use this script to contact physician.
"Dr. , this is (your name). I'm the nurse taking care of (patient name) in Room .
"I've just completed a sepsis screening of the patient, and I suspect the patient mayhave an infection (state location of infection) and meets the SIRS criteria of (list thetwo or more criteria met on the screening tool). Per protocol, I have already drawna lactate.
'The next step in the Sepsis Protocol is to initiate the Sepsis Powerplan. The SepsisPowerplan is required.
"The order set begins with drawing a bundle of lab tests, if they haven't been drawnwithin the last 12 hours, and includes lactate, chem 10, bilirubin, sputum and urinecultures, AST, ALT, and CBC with diff, and INR. I will also draw blood cultures if theyhave not been done within fhe last 6 hours.
"The patient is already on (name of antibiotic). Would you like to continue or modi-fy?" or "The patient is not on antibiotics. Would you like to start a regimen now?"
"The patient is currently receivingincrease the tluids, or change the fluids?"
IVFs. Would you like to give a bolus,
If the sepsis protocol is not initiated by the physician, ask for the reason he/shewould like recorded on the screening tool for not initiating the orders. If the lactateresults come back abnormal, call the physician with the results and ask to initiatethe protocol. Call the RRT to follow patient
If sepsis orders are initiated, notify RRT to come to floor to complete an assessmentto check for organ dysfunction.
fied signs and symptoms of sepsis inpatients and then recommendedsteps for initiation of the sepsis bun-dle. The tool was modified until thecorrelation between reviewers was0.8 or higher. Feedback helpedensure measurable outcomes andavoid unnecessary steps. Each rapidimprovement cycle involved datecollection and feedback to nurses soappropriate changes could be madeto the process. Direct-care nurses,physicians, and other team membersreviewed each cycle and discussedthe process, care, and outcomes.Without the input of direct-carenurses, the project would not havesucceeded in the early stages.
As an outcome of this process, theSMITe developed several tools toassist staff in the diagnosis and treat-ment of patients with sepsis. Toolsincluded:• A sepsis screening tool that
allows nurses to review sepsis-related symptoms.
• Outlined steps (bundle) thenurse must take in caring forpatient with suspected sepsis.
• An electronic sepsis order set.• Verbal order telephone scripts to
support communication betweenthe physician and nurse.
• Complete protocol.All patients on medical-surgical
units now are screened each shift,serum lactate is drawn for positivescreens, and blood cultures are takenprior to initial antibiotic administra-tion. Antibiotics are administeredwithin 1 hour of order initiation,and fluids are administered for allpatients on the Red Pathway. TheRed Pathway allows the identifica-tion of patients who have positiveblood cultures and abnormal serumlactates. Serum lactate is used as amarker for a positive screen becauseit is associated with mortality(Mikkelsen et al., 2009). The tools toassist staff in the diagnosis and treat-ment of patients with sepsis were put
MEDSURG isrunsiisro. January-February 2014 • Vol. 23/No. 1 11
Continuous Quality Improvement
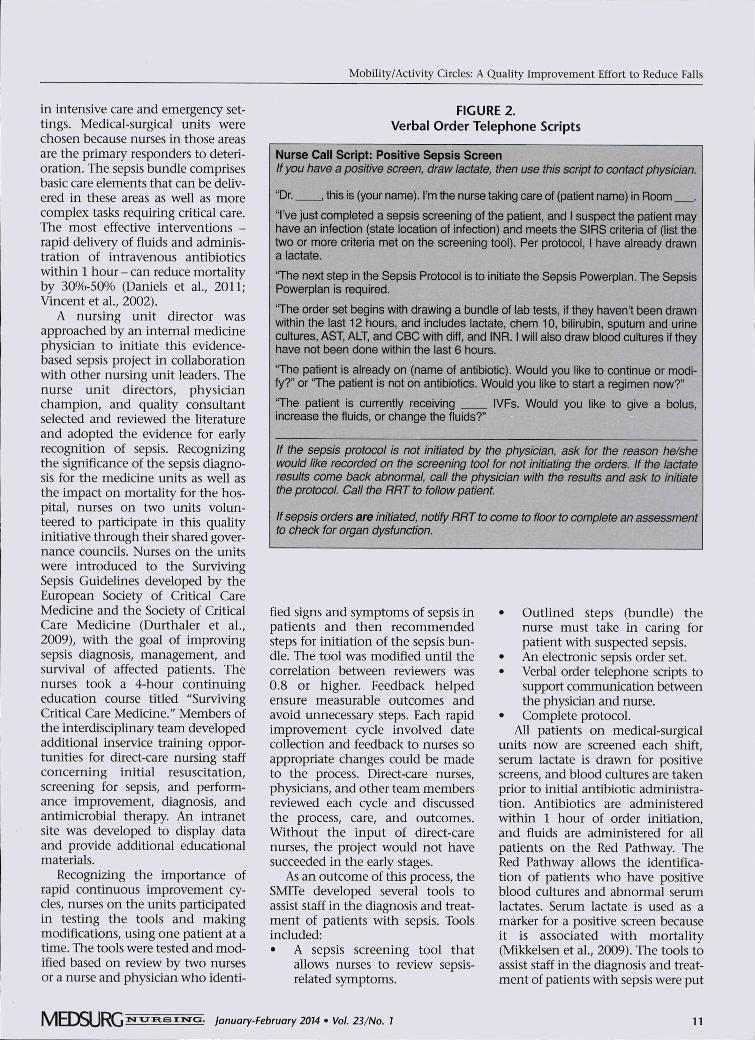
FIGURE 3.Complete Sepsis Protocol
Sepsis Bundle: Early Goal-Directed Therapy Guideline
SIRS CriteriaAssess for two or more of the following:1. Temp a 38 C or s 36 C2. HRa903. Resp rate a 20 or PaC02 s 324. WBC a 12K, or s4K or a 10% bands
Early Recognition6-Hour Goals
SEPSIS
1. NURSE: Notify MD & RRT of positive sepsis screen.2, MD: Confirm sepsis diagnosis and initiate Sepsis Order Set or doc-
ument reason for NOT initiating Sepsis Order Set.
CHECK LACTATE, LAB RESULTS, AND BLOOD PRESSURE
1. Lactate < 2 and2. Normotensive and3. No evidence of acute
organ dysfunction
1. Lactate >4 or2. SBP < 90 or3. Decrease in SBP > 30 mmHg
1, Normotensive and2, Lactate 2-4 or aoute organ dysfunction
SEVERE SEPSIS
Confirm culture drawn.Give appropriate antibiotics.Reassess lactate q8 hours x 1(repeat as needed).Repeat labs: reassess for signs/symptoms of organ dysfunctioiq day x 2 days.
1, Give 20 ml/kg IVF bolus2. Assess for CVP need
Responsive ;
4,
Unresponsive
SEPTIC SHOCK
Confirm cultures drawnand antibiotics given.Aggressive IVFs,Recheck lactate q 4 hours x 3;reassess.Consider transfer to SAC forcloser monitoring.Repeat labs; reassess forsigns/symptoms of organdysfunction q day x 2 days.
1, Notify ICU,2, If in ED, take patient to Resus Room,3, Broad-spectrum antibiotics, supplemental 02, large bore IV, Foley, labs, cultures, assess for source control4, Place arterial line and central line and initiate EGDT/Sepsis Order Set,
step 1 :CVP
GOAL
CVP 8-12
IF
<8t• -
THEN
Give NS/LF bolus. Repeat until CVP 8-12.Then continue to monitor CVP.No action needed - Continue to Step 2
Step 2SBP/MAP
SBP 90-140CVP 8-12
MÄF'<65or-SBP<90
Arterial line, pressors, andConsider baseline oortisol and steroids.
Goals Achieved
No
Recheck laotate q 8 hours x 3. : ;Reassess Steps 1 -2 andConsider mechanical ventilation and sedation.
12 January-February 2014 • Vol. 23/No. 1 M E D S U R G
Continuons Quality Improvetnent
on the UNMH intranet and havebecome the standard of practice forall medical-surgical units at UNMH(see Figures 1-3). Understanding theimportance of quick recognition anddiagnosis, members of the SMITealso developed a Sepsis Lab Bag thatcontains all blood tubes required forsepsis diagnosis.
The SMITe continues to meetmonthly and review the efficacy ofthe existing protocol for continuousimprovement. Outcomes includereduced mortality and morbidity ofpatients with sepsis at UNMH.
Evaluation and Action PlanData are collected through chart
abstractions and reviewed by mem-bers of the SMITe. Results are present-ed monthly to the department ofinternal medicine and annually tothe hospital leadership via the quali-ty committee. This information alsois available to unit directors on theproject's web page to share with staff.During the first 2 years after initia-tion of the SMITe iniriative, 225 adultpatients screened positive for sepsis;less than 112 deaths occurred, repre-senfing a 50% decrease in mortality.
Results and LimitationsThrough the use of the protocol,
and tools developed by the SMITeand staff educators, nurses are able torecognize patients with sepsis, orderlaboratory tests, and initiate treat-ment. Daily patient reports are heldbetween the RRT and the unit direc-tor to support rapid bed placementand initiation of the sepsis protocol.This process led to early identifica-tion of patient deterioration andprompt management using appro-priate skills. Nurses had a key role inidenrifying patients with sepsis orseptic shock and providing appropri-ate treatment. Their knowledgeabout sepsis and nursing guidelinesprovided a format for systematicassessment and management.
Between March 2008 and April2009, 225 patients screened positivefor sepsis and 22 (10%) were trans-ferred to a higher level of care as aresult. Twenty-one patients weretransferred from one of the medical-
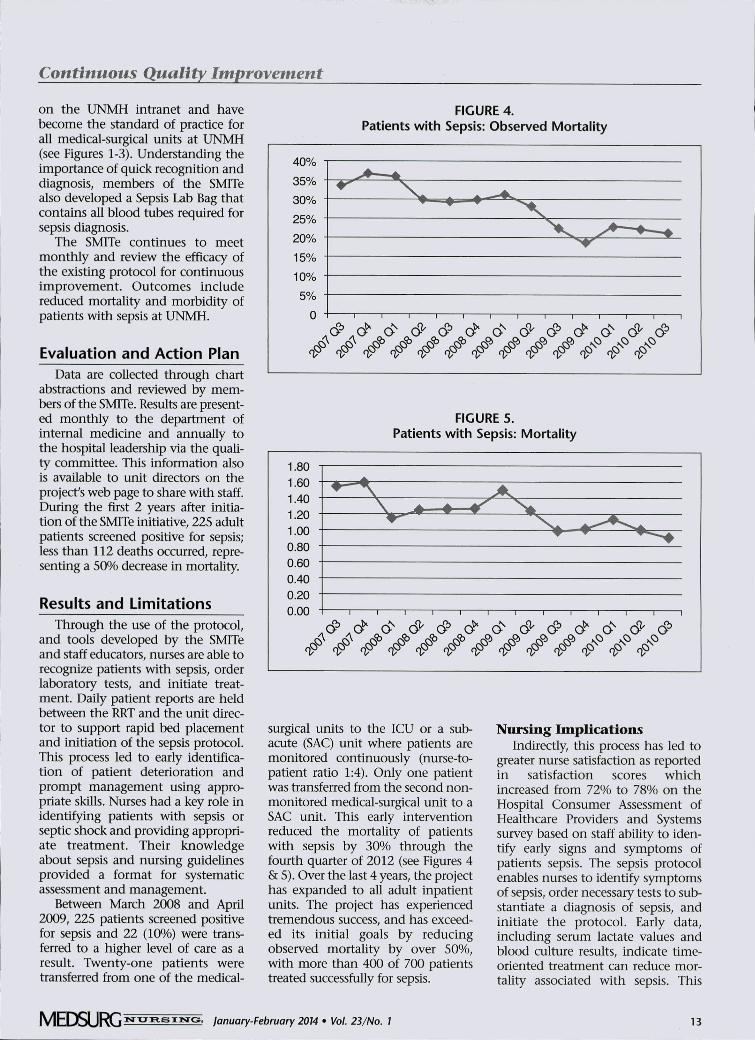
FIGURE 4.Patients with Sepsis: Observed Mortality
40%
35%
30%
25%
20%
15%
10%
5%
0 1 1 1 1 1 1 1 r ~\ 1 1 1
r<^ rO^ rQ>
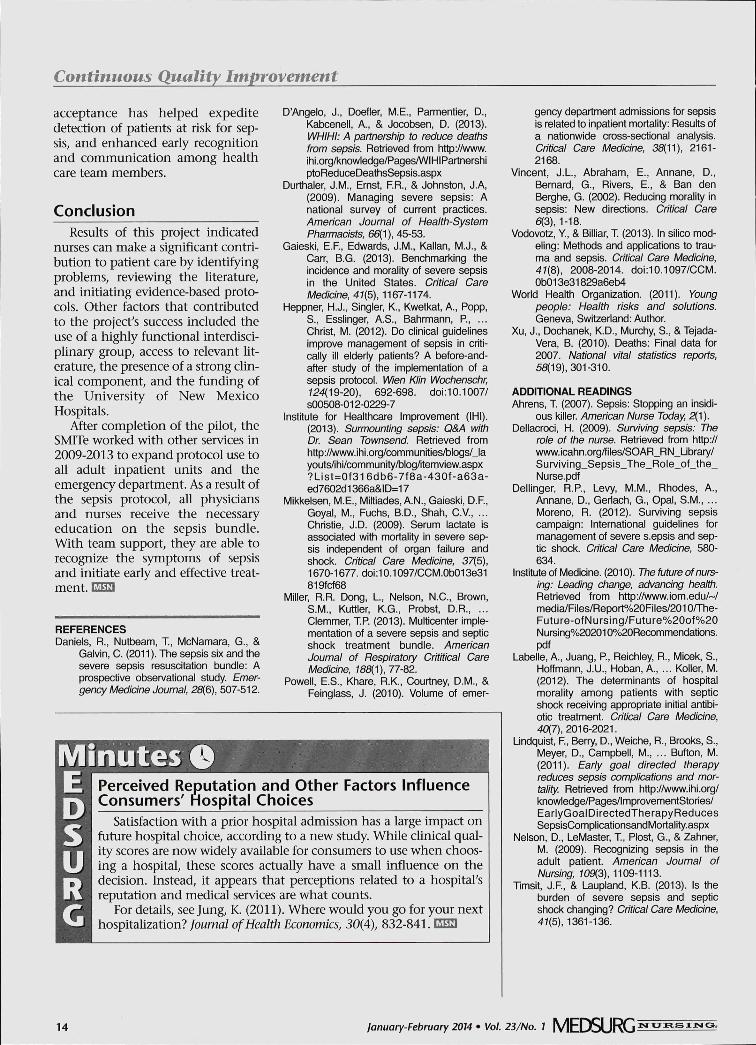
FIGURE 5.Patients with Sepsis: Mortality
surgical units to the ICU or a sub-acute (SAC) unit where patients aremonitored continuously (nurse-to-patient ratio 1:4). Only one patientwas transferred from the second non-monitored medical-surgical unit to aSAC unit. This early interventionreduced the mortality of patientswith sepsis by 30% through thefourth quarter of 2012 (see Figures 4& 5). Over the last 4 years, the projecthas expanded to all adult inpatientunits. The project has experiencedtremendous success, and has exceed-ed its initial goals by reducingobserved mortality by over 50%,with more than 400 of 700 patientstreated successfully for sepsis.
Nursing ImplicationsIndirectly, this process has led to
greater nurse satisfaction as reportedin satisfaction scores whichincreased from 72% to 78% on theHospital Consumer Assessment ofHealthcare Providers and Systemssurvey based on staff ability to iden-tify early signs and symptoms ofpatients sepsis. The sepsis protocolenables nurses to identify symptomsof sepsis, order necessary tests to sub-stantiate a diagnosis of sepsis, andinitiate the protocol. Early data,including serum lactate values andblood culture results, indicate time-oriented treatment can reduce mor-tality associated with sepsis. This
MEDSURG January-February 2014 • Vol. 23/No. I 13
Continuous Quality Improvement
acceptance has helped expeditedetection of patients at risk for sep-sis, and enhanced early recognitionand communication among healthcare team members.
ConclusionResults of this project indicated
nurses can make a significant contri-bution to patient care by identifyingproblems, reviewing the literature,and initiating evidence-based proto-cols. Other factors that contributedto the project's success included theuse of a highly functional interdisci-plinary group, access to relevant lit-erature, the presence of a strong clin-ical component, and the funding ofthe University of New MexicoHospitals.
After completion of the pilot, theSMITe worked with other services in2009-2013 to expand protocol use toall adult inpatient units and theemergency department. As a result ofthe sepsis protocol, all physiciansand nurses receive the necessaryeducation on the sepsis bundle.With team support, they are able torecognize the sjnnptoms of sepsisand initiate early and effective treat-ment.
REFERENCESDaniels, R., Nutbeam, T., McNamara, G., &
Galvin, C. (2011). The sepsis six and thesevere sepsis resuscitation bundle: Aprospective observational study. Emer-gency Medicine Journal, 28{6), 507-512.
D'Angelo, J., Doefler, M.E., Parmentier, D.,Kabcenell, A., & Jocobsen, D. (2013).WHIHI: A partnership to reduce deathsfrom sepsis. Retrieved from http://www.ihi.org/l<nowledge/Pages/WIHIPartnershiptoReduceDeathsSepsis.aspx
Durthaler, J.M., Ernst, F.R., & Johnston, J.A,(2009). Managing severe sepsis: Anational survey of current practices.American Journal of Health-SystemPharmacists, 66(1 ), 45-53.
Gaieski, E.F., Edwards, J.M., Kalian, M.J., &Carr, B.G. (2013). Benchmarking theincidence and morality of severe sepsisin the United States. Critical CareMedicine, 41{5), 1167-1174.
Heppner, H.J., Singler, K., Kwetkat, A., Popp,S., Esslinger, A.S., Bahrmann, P., ...Christ, M. (2012). Do clinical guidelinesimprove management of sepsis in criti-cally ill elderly patients? A before-and-after study of the implementation of asepsis protocol. Wien Klin Wochenschr,Í24(19-2O), 692-698. doi:10.1007/S00508-012-0229-7
Institute for Healthcare Improvement (IHI).(2013). Surmounting sepsis: Q&A withDr. Sean Townsend. Retrieved fromhttp://www.ihi.org/communities/blogs/_layouts/ihi/community/blog/itemview.aspx?List=0f316db6-7f8a-430f-a63a-ed7602d1366a&ID=17
Mikkelsen, M.E., Miltiades, A.N., Gaieski, D.R,Goyal, M., Fuchs, B.D., Shah, C.V., ...Christie, J.D. (2009). Serum lactate isassociated with mortality in severe sep-sis independent of organ failure andshock. Critical Care Medicine, 37(5),1670-1677. doi:10.1097/CCM.0b013e31819fcf68
Miller, R.R. Dong, L, Nelson, N.C., Brown,S.M., Kuttler, K.G., Probst, D.RClemmer, TP. (2013). Multicenter imple-mentation of a severe sepsis and septicshock treatment bundle. AmericanJournal of Respiratory Crititical CareMedicine, iSS(1), 77-82.
Powell, E.S., Khare, R.K., Courtney, D.M., &Feinglass, J. (2010). Volume of emer-
MinutesllPerceived Reputation and Other Factors InfluenceConsumers' Hospital Choices
Satisfaction with a prior hospital admission has a large impact onfuture hospital choice, according to a new study. While clinical qual-ity scores are now widely available for consumers to use when choos-ing a hospital, these scores actually have a small influence on thedecision. Instead, it appears that perceptions related to a hospital'sreputation and medical services are what counts.
For details, see Jung, K. (2011). Where would you go for your nexthospitalization? foumal of Health Economics, 30(4), 832-841. EMU
gency department admissions for sepsisis related to inpatient mortality: Results ofa nationwide cross-sectional analysis.Critical Care Medicine, 3S(11), 2161-2168.
Vincent, J.L., Abraham, E., Annane, D.,Bernard, G., Rivers, E., & Ban denBerghe, G. (2002). Reducing morality insepsis: New directions. Critical Care6(3), 1-18.
Vodovotz, Y, & Billiar, T (2013). In silico mod-eling: Methods and applications to trau-ma and sepsis. Critical Care Medicine,41{8), 2008-2014. doi:10.1097/CCM.0b013e31829a6eb4
World Health Organization. (2011). Youngpeople: Health risks and solutions.Geneva, Switzerland: Author.
Xu, J., Dochanek, K.D., Murchy, S., & Tejada-Vera, B. (2010). Deaths: Final data for2007. National vital statistics reports,55(19), 301-310.
ADDiTiONAL READINGSAhrens, T (2007). Sepsis: Stopping an insidi-
ous killer. American Nurse Today, 2(1).Dellacroci, H. (2009). Surviving sepsis: The
role of the nurse. Retrieved from http://www.icahn.org/files/SOAR_RN_Ubrary/Surviving_Sepsis_The_Role_of_the_Nurse.pdf
Dellinger, R.P., Levy, M.M., Rhodes, A.,Annane, D., Gerlach, G., Opal, S.M., ...Moreno, R. (2012). Surviving sepsiscampaign: International guidelines formanagement of severe s.epsis and sep-tic shock. Critical Care Medicine, 580-634.
Institute of Medicine. (2010). The future of nurs-ing: Leading change, advancing health.Retrieved from http://www.iom.edu/~/media/Files/Report%20Files/2010/The-Future-ofNursing/Future%20of%20Nursing%202010%20Recommendations.pdf
Labelle, A., Juang, P., Reichley R., Micek, S.,Hoffmann, J.U., Hoban, A., ... Koller, M.(2012). The determinants of hospitalmorality among patients with septicshock receiving appropriate initial antibi-otic treatment. Critical Care Medicine,40(7), 2016-2021.
Lindquist, F, Berry, D., Weiche, R., Brooks, S.,Meyer, D., Campbell, M., ... Button, M.(2011). Early goal directed therapyreduces sepsis complications and mor-tality. Retrieved from http://www.ihi.org/knowledge/Pages/lmprovementStories/EarlyGoalDirectedTherapy ReducesSepsisCompllcationsandMortality.aspx
Nelson, D., LeMaster, T, Plost, G., & Zahner,M. (2009). Recognizing sepsis in theadult patient. American Journal ofNursing, 109(3), 1109-1113.
Tlmsit, J.F, & Laupland, K.B. (2013). Is theburden of severe sepsis and septicshock changing? Critical Care Medicine,41(5), 1361-136.
14 January-February 2014 • Vol. 23/No. 1 M E D S U R G

Copyright of MEDSURG Nursing is the property of Jannetti Publications, Inc. and its contentmay not be copied or emailed to multiple sites or posted to a listserv without the copyrightholder's express written permission. However, users may print, download, or email articles forindividual use.