recurrent seizures due to pancreatic insulinoma - japi.org · recurrent seizures due to pancreatic...
TRANSCRIPT

Journal of The Association of Physicians of India ■ Vol. 64 ■ June 201686
Recurrent Seizures Due to Pancreatic InsulinomaAnjali Rajadhyaksha1, Archana Sonawale2, Ashwin Chichkhede3, Abhishek Zanwar4
AbstractWe present the case of a 70 year old man who was admitted with history of generalized tonic clonic seizures on and off since 6 years in spite of being on regular therapy with anticonvulsants. Patient was found to have hypoglycemia and was evaluated for same. He was diagnosed to have endogenous hyperinsulinemia due to pancreatic insulinoma. Patient underwent enucleation of tumor and was relieved of his symptoms.
1Professor, 2Associate Professor, 3Registrar, 4Specialty Medical Officer, Department of Medicine, Seth GS Medical College and KEM Hospital, Mumbai, MaharashtraReceived; 06.02.2015; Accepted: 22.08.2015
Introduction
Recurrent seizures can often arise due to under ly ing metabo l i c
disturbance. Herein, we report a case of insulinomia presenting with recurrent seizures due to hypoglycemic spells.
Case Report
A 70 year old man presented with generalized tonic clonic seizures since 6 years. He had history of dizziness and sweating prior to the convulsion which would occur mainly in mornings and before meals. On enquiry, patient reported relief from symptoms after meals. He has been started on Phenytoin (100 mg thrice daily) tds by a private physician. He had stopped phenytoin on his own and continued to have seizures. Patient had no history of diabetes mellitus, no significant medical or surgical illness in past and no family history of similar illness and denied addiction. On examination patient was well built (BMI-29.9) higher mental functions were normal, pulse was 80/min, BP was 130/80 mm of Hg. Systemic examination was within normal limits. His complete blood count, liver profile, creatinine and electrolytes were normal. However, his random blood sugar
was 28 mg/dl. CT-brain and EEG was normal. In view of patient’s blood sugar level of 28 mg/dl, we decided to find cause of hypoglycemia. His serum insulin level was 6.83 μIU/L and C-peptide level was 2.1 ng/ml during the seizure episode. The HbA1c was found to be <4 gm%. In the hospial, he needed regular infusion of dextrose for hypoglycemia prevention. CT abdomen triple phase contrast demonstrated a 1.7 cm enhancing mass at head-neck j u n c t i o n o f p a n c r e a s ( F i g u r e 1 ) . Contrast-enhanced USG abdomen was performed to augment the CT findings and it showed an ill-defined 9 mm × 7 mm hypoechoic nodule at head-neck junction of pancreas. In lieu of these findings, patient was diagnosed to have pancreat ic insul inoma with h y p o g l y c e m i c s e i z u r e s . F u r t h e r w o r k - u p f o r m u l t i p l e e n d o c r i n e neoplasia was negative. Serum AFP and PSA level were a lso normal . Patient underwent enucleation of the pancreatic nodule. An intra pancreatic
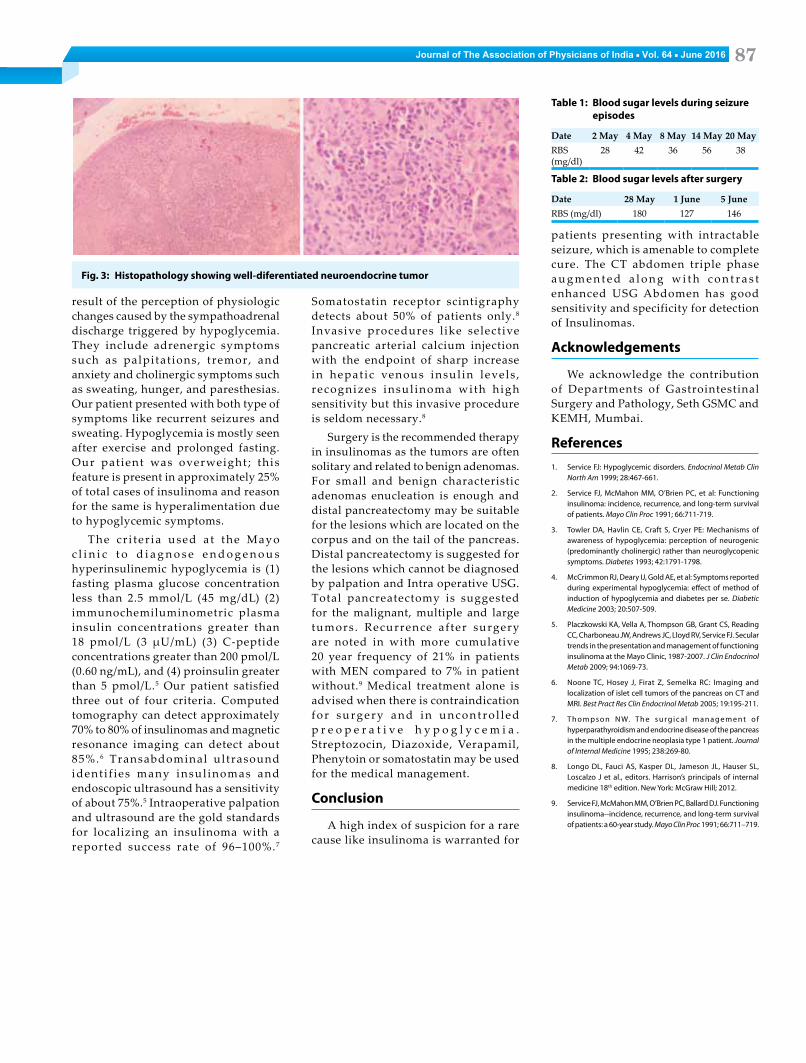
mass measuring 2.5 cm × 2 cm (Figure 2) was removed and patient became asymptomatic and seizure free after that Tables 1 and 2 show pre and post-operative blood sugars. Histopathology report showed a well circumscribed mass composed of cell arranged in nets and sheets. Cells contained round nuclei and eosinophilic cytoplasm without any nuclear atypia or mitotic activity. Focal presence of papillae were seen. Mass was surrounded by fibrous condensation. Above Findings suggest ive of wel l d i f ferent ia ted neuroendocrine tumor (Figure 3).
Discussion
Insulinomas are the most common cause of hypoglycemia related to endogenous hyper insul inemia in adults.1 It is a rare neuroendocrine pancreat i c tumor . The es t imated incidence is one case per 2,50,000 p a t i e n t - y e a r s . 2 M e d i a n a g e a t presentation is 5th decade in sporadic cases and 3 rd decade in mul t ip le endocrine neoplasia syndrome. It is typically sporadic, solitary and less than 2 cm in diameter. Ninety percent or more of all insulinomas are benign. Fewer than 5% of insulinomas are larger than 3 cm. Larger tumors are more likely to be malignant.
Hypoglycemia is clinically evident by Whipple’s triad (symptoms consistent with hypoglycemia, a low plasma glucose concentration, and relief of those symptoms when the plasma glucose concentration is raised). Our patient had typical triad. Symptoms of hypoglycemia can be divided into two categories, neuroglycopenic and neurogenic (autonomic) symptoms.3,4 N e u r o g l y c o p e n i c s y m p t o m s a r e the direct result of CNS neuronal glucose deprivation. They include b e h a v i o r a l c h a n g e s , c o n f u s i o n , fatigue or weakness, visual changes, seizure, loss of consciousness, and, if hypoglycemia is severe and prolonged, death. Neurogenic symptoms are the
Fig. 1: CT abdomen showing a 1.7 cm enhancing mass at head-neck junction of pancreas (arrow)
Fig. 2: Excised intra-pancreatic mass measuring 2.5 cm × 2 cm
Journal of The Association of Physicians of India ■ Vol. 64 ■ June 2016 87
Fig. 3: Histopathology showing well-diferentiated neuroendocrine tumor
result of the perception of physiologic changes caused by the sympathoadrenal discharge triggered by hypoglycemia. They include adrenergic symptoms such as palpitat ions, tremor, and anxiety and cholinergic symptoms such as sweating, hunger, and paresthesias. Our patient presented with both type of symptoms like recurrent seizures and sweating. Hypoglycemia is mostly seen after exercise and prolonged fasting. Our pat ient was overweight ; this feature is present in approximately 25% of total cases of insulinoma and reason for the same is hyperalimentation due to hypoglycemic symptoms.
The cr i ter ia used a t the Mayo c l i n i c t o d i a g n o s e e n d o g e n o u s hyperinsulinemic hypoglycemia is (1) fasting plasma glucose concentration less than 2.5 mmol/L (45 mg/dL) (2) immunochemiluminometric plasma insulin concentrations greater than 18 pmol/L (3 μU/mL) (3) C-peptide concentrations greater than 200 pmol/L (0.60 ng/mL), and (4) proinsulin greater than 5 pmol/L.5 Our patient satisfied three out of four criteria. Computed tomography can detect approximately 70% to 80% of insulinomas and magnetic resonance imaging can detect about 85%. 6 Transabdominal ultrasound ident i f ies many insul inomas and endoscopic ultrasound has a sensitivity of about 75%.5 Intraoperative palpation and ultrasound are the gold standards for localizing an insulinoma with a reported success rate of 96–100%.7
Somatostatin receptor scintigraphy detects about 50% of patients only.8 Invasive procedures l ike selective pancreatic arterial calcium injection with the endpoint of sharp increase in hepat ic venous insul in levels , recognizes insul inoma with h igh sensitivity but this invasive procedure is seldom necessary.8
Surgery is the recommended therapy in insulinomas as the tumors are often solitary and related to benign adenomas. For small and benign characteristic adenomas enucleation is enough and distal pancreatectomy may be suitable for the lesions which are located on the corpus and on the tail of the pancreas. Distal pancreatectomy is suggested for the lesions which cannot be diagnosed by palpation and Intra operative USG. Total pancreatectomy is suggested for the malignant, multiple and large tumors . Recurrence af ter surgery are noted in with more cumulative 20 year frequency of 21% in patients with MEN compared to 7% in patient without.9 Medical treatment alone is advised when there is contraindication for surgery and in uncont ro l l ed p r e o p e r a t i v e h y p o g l y c e m i a . Streptozocin, Diazoxide, Verapamil, Phenytoin or somatostatin may be used for the medical management.
Conclusion
A high index of suspicion for a rare cause like insulinoma is warranted for
Table 1: Blood sugar levels during seizure episodes
Date 2 May 4 May 8 May 14 May 20 MayRBS (mg/dl)
28 42 36 56 38
Table 2: Blood sugar levels after surgery
Date 28 May 1 June 5 JuneRBS (mg/dl) 180 127 146
patients presenting with intractable seizure, which is amenable to complete cure. The CT abdomen triple phase a u g m e n t e d a l o n g w i t h c o n t r a s t enhanced USG Abdomen has good sensitivity and specificity for detection of Insulinomas.
Acknowledgements
We acknowledge the contribution of Departments of Gastrointestinal Surgery and Pathology, Seth GSMC and KEMH, Mumbai.
References1. Service FJ: Hypoglycemic disorders. Endocrinol Metab Clin
North Am 1999; 28:467-661.
2. Service FJ, McMahon MM, O’Brien PC, et al: Functioning insulinoma: incidence, recurrence, and long-term survival of patients. Mayo Clin Proc 1991; 66:711-719.
3. Towler DA, Havlin CE, Craft S, Cryer PE: Mechanisms of awareness of hypoglycemia: perception of neurogenic (predominantly cholinergic) rather than neuroglycopenic symptoms. Diabetes 1993; 42:1791-1798.
4. McCrimmon RJ, Deary IJ, Gold AE, et al: Symptoms reported during experimental hypoglycemia: effect of method of induction of hypoglycemia and diabetes per se. Diabetic Medicine 2003; 20:507-509.
5. Placzkowski KA, Vella A, Thompson GB, Grant CS, Reading CC, Charboneau JW, Andrews JC, Lloyd RV, Service FJ. Secular trends in the presentation and management of functioning insulinoma at the Mayo Clinic, 1987-2007. J Clin Endocrinol Metab 2009; 94:1069-73.
6. Noone TC, Hosey J, Firat Z, Semelka RC: Imaging and localization of islet cell tumors of the pancreas on CT and MRI. Best Pract Res Clin Endocrinol Metab 2005; 19:195-211.
7. T h o m p s o n N W. T h e s u r g i c a l m a n a g e m e n t o f hyperparathyroidism and endocrine disease of the pancreas in the multiple endocrine neoplasia type 1 patient. Journal of Internal Medicine 1995; 238:269-80.
8. Longo DL, Fauci AS, Kasper DL, Jameson JL, Hauser SL, Loscalzo J et al., editors. Harrison’s principals of internal medicine 18th edition. New York: McGraw Hill; 2012.
9. Service FJ, McMahon MM, O’Brien PC, Ballard DJ. Functioning insulinoma--incidence, recurrence, and long-term survival of patients: a 60-year study. Mayo Clin Proc 1991; 66:711–719.