pup biologic warfare
TRANSCRIPT

L 11 Epidemics and Emerging Infections 1
Epidemics and Emerging Infections
Hospital Preparedness for Emergencies

Wars of the Future: Biological Warfare and Chemical
Weapons
Teodoro Herbosa MD FPCS Department of Emergency Medicine
College of Medicine University of the Philippines, Manila

L 11 Epidemics and Emerging Infections 3
Objective
Identify the fundamentals of a hospital preparedness and response plan for epidemics.
Upon completion of this unit, you will be able to:

L 11 Epidemics and Emerging Infections 4
Biological Hazards
❑ “Terrorism” / Anthrax ❑ SARS ❑ Avian Flu ❑ Dengue ❑ MERSCoV ❑ Ebola
Vulnerability emerging to infectious diseases

L 11 Epidemics and Emerging Infections 5
Biological Hazards
Tartars used plague-infected
corpses in Kaffa, 1346.

L 11 Epidemics and Emerging Infections 6
Influenza Pandemic
Nurses work in the Red Cross rooms of Seattle, WA with “influenza masks” on their faces. December 1918 (Courtesy of the National Archives, 165-WW-269B-10)

L 11 Epidemics and Emerging Infections 7
Basic Dictum
Safety First!

L 11 Epidemics and Emerging Infections 8
Biological Event
❑ Bacterial agents ▪ Anthrax, Brucellosis, Yersinea pestis
(Plague) & Cholera , Salmonella ❑ Viruses
▪ Smallpox, Hemorrhagic Fever Virus ❑ Biological product
▪ Botulinum toxin, Endotoxins, Mycotoxin, SEB, ricin,

L 11 Epidemics and Emerging Infections 9
Smallpox – Bangladesh, 1976
A child stricken by smallpox is relatively cured but his health is still threatened by malnutrition and secondary infection. (Courtesy of the National Archives, 76-845)

L 11 Epidemics and Emerging Infections 10
Biological Event
❑ Infection borne through air, food and water
❑ Incubation period - delay from time of exposure until clinical symptoms arise
❑ Extensive exposure may occur before the primary event is appreciated.

L 11 Epidemics and Emerging Infections 11
Rare Diseases can be Overseen
Rare color photo of Baby with smallpox. National Archive film footage from Vietnam (RG-428-NPC-38594)

L 11 Epidemics and Emerging Infections 12
Biological Event
❑ Delivered with conventional explosives
❑ Emergency care, decontamination is necessary (outside the hospital)
❑ Personnel must be trained in patient decontamination

L 11 Epidemics and Emerging Infections 13
Decontamination Area❑ Storage for decontamination equipment
and supplies ❑ Decontamination area - cooled to reduce
the heat load on personnel caused by their protective equipment
❑ The decontamination site has 3 zones: ▪ Hot zone – incoming casualties ▪ Warm zone – decontamination area ▪ Cold zone – triage and transport

L 11 Epidemics and Emerging Infections 14
Contamination reduction (warm) zone
Support (cold) zone
Exclusion (hot) zone
wind
CORRIDOR
amp
Access control points
Crowd control line
Decontamination line
Hot line

L 11 Epidemics and Emerging Infections 15
Decontamination Area
❑ First responders and medical personnel SHOULD PROTECT THEMSELVES
❑ Personal Protective Equipment (PPE) ▪ Protect eyes, lungs and skin
L 11 Epidemics and Emerging Infections 16
Decontamination Area
Storage for decontamination equipment and supplies Decontamination area
❑ cooled to reduce the heat load on personnel caused by their protective equipment

L 11 Epidemics and Emerging Infections 17
Decontamination Area

L 11 Epidemics and Emerging Infections 18
Hot zone
Support zone
Decontamination zone
Patients
No special protective gear
hazmat teams with proper protective gear
gross contaminates removed here
remove victim’s contaminated clothing
wash & final rinse/soap & shampoo
wash & rinse
clean stretcher & blankets

L 11 Epidemics and Emerging Infections 19
Decontamination Area

L 11 Epidemics and Emerging Infections 20
Decontamination Area
❑ First responders (decontamination) protect themselves through PPE.
❑ Personal Protective Equipment (PPE) respiratory equipment
❑ Garments and barrier material
L 11 Epidemics and Emerging Infections 21
Decontamination Area
❑ Maximum protection is achieved through use of positive pressure respirators and total body encapsulation.
❑ Surgical mask and a pair of latex gloves provide minimum protection
L 11 Epidemics and Emerging Infections 22
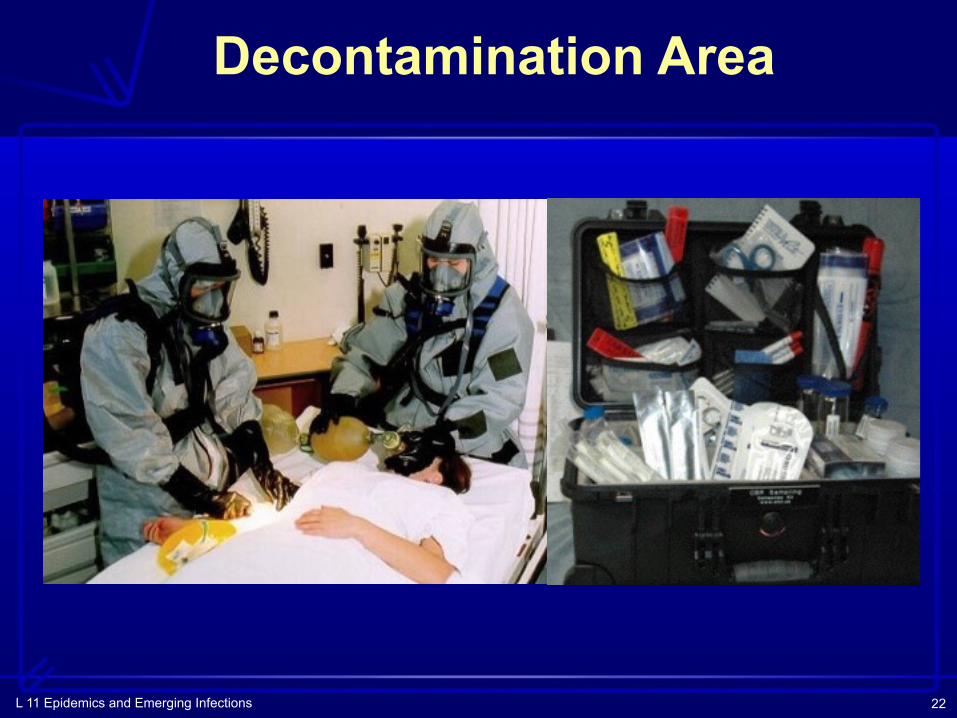
Decontamination Area

L 11 Epidemics and Emerging Infections 23
Personal Protective Equipment
Red Cross workers of Boston, MA removing bundles of masks for American Soldiers from a table where other women are busily engaged in making them. March 1919. (Courtesy of the National Archives, 165-WW-269B-37)

L 11 Epidemics and Emerging Infections 24
Medical Response
❑ Pandemic ▪ large number of
casualties with similar symptoms
▪ dissemination device ▪ receipt of a warning ▪ hospital may receive
untreated casualties directly from the site
Emergency Hospital at Brookline, MA to care for influenza cases.
October 1918

L 11 Epidemics and Emerging Infections 25
Medical Response
First responders and medical personnel SHOULD PROTECT THEMSELVES
September 11

L 11 Epidemics and Emerging Infections 26
Medical Response
Why is the level of Epidemic preparedness so critical?
❑ Because the consequences of not being prepared are so catastrophic
Smallpox Vaccine

L 11 Epidemics and Emerging Infections 27
Category A The public health systems and primary health-care providers must be prepared to address varied biological agents, including pathogens that are rarely seen. High-priority agents include organisms that pose a risk to national security because they –
❑ can be easily disseminated or transmitted person-to-person;
❑ cause high mortality, with potential for major public health impact;
❑ might cause public panic and social disruption; and
❑ require special action for public health preparedness.

L 11 Epidemics and Emerging Infections 28
Category A Agents Include:
❑ Variola major (Smallpox): ❑ Bacillus anthracis (Anthrax); ❑ Yersinia pestis (Plague); ❑ Clostridium botulinium toxin
(Botulism); ❑ Francisella tullarensis
(Tularemia);

L 11 Epidemics and Emerging Infections 29
Category A Agents Include:
❑ Filoviruses - Ebola Hemorrhagic Fever; - Marburg Hemorrhagic Fever; and
❑ Arenaviruses - Lassa (Lassa Fever)
- Junin (Argentine Hemorrhagic Fever) related viruses.
L 11 Epidemics and Emerging Infections 30
Category B
Second-highest priority agents: ❑ moderately easy to disseminate ❑ cause moderate morbidity and low
mortality ❑ require specific enhancements of CDC’s
diagnostic capacity and enhanced disease surveillance

L 11 Epidemics and Emerging Infections 31
Category B agents include:❑ Coxiella burnetti (Q fever) ❑ Brucella species (Brucellosis) ❑ Burkholderia mallei (Glanders) ❑ Alphaviruses
▪ Venezuelan encephalomyelitis ▪ Eastern and Western equine
encephalomyelitis ❑ Rich toxin from Ricinus communis (castor beans) ❑ Epsilon toxin of Clostridium perfringens ❑ Staphylococcus enterotoxin B
L 11 Epidemics and Emerging Infections 32
Category BA subset of List B agents include pathogens that are food or waterborne. These pathogens include, but are not limited to:
▪ Salmonella species ▪ Shigella dysenteriae ▪ Escherichia coli O157:H7 ▪ Vibrio cholerae ▪ Cryptosporidium parvum

L 11 Epidemics and Emerging Infections 33
Category C
Third-highest priority agents include emerging pathogens that could be engineered for mass dissemination in the future because of:
❑ availability ❑ ease of production and dissemination ❑ potential for high morbidity and mortality
due to major health impacts

L 11 Epidemics and Emerging Infections 34
Category C agents include:
❑ Nipah virus ❑ Hantaviruses ❑ Tickbone hemorrhagic fever viruses ❑ Tickbone encephalitis viruses ❑ Yellow fever ❑ Multi-drug resistant tuberculosis
L 11 Epidemics and Emerging Infections 35
Category C
Preparedness for List C agents requires ongoing research to improve disease detection, diagnosis, treatment and prevention. Linking bio-terrorism preparedness efforts with ongoing disease surveillance and outbreak response activities as defined in CDC’s emerging infectious disease strategy is imperative.

L 11 Epidemics and Emerging Infections 36
❑ Cholera epidemic, Europe 1830 - 1847 intensive infectious disease diplomacy multilateral cooperation; First International Sanitary Conference, Paris 1851
❑ 1948 WHO Constitution ❑ 1951 WHO adopted International Sanitary
Regulations ❑ International Health Regulations, 1969
History of the IHR

L 11 Epidemics and Emerging Infections 37
IHR (1969) to monitor and control six serious infectious diseases: Cholera, Plague, Yellow fever, Smallpox, Relapsing fever and Typhus
IHR (1969) - Cholera, Plague and Yellow fever remain of concern WHO must be informed
History of the IHR

L 11 Epidemics and Emerging Infections 38
1990's resurgence of epidemics Cholera - South America Plague - India Emergence of infectious agents Ebola (48th World Health Assembly, 1995 revision of IHR, May 2001) WHA 54.14, Global health security: epidemic alert and response
History of the IHR
L 11 Epidemics and Emerging Infections 39
May 2003 resolution WHA56.28 Revision of IHR IGWG sessions in Nov 2004 and Feb/May 2005 58th World Health Assembly adopted IHR (2005) 23 May 2005 resolution WHA58.3.
History of the IHR
L 11 Epidemics and Emerging Infections 40
International Health Regulations of 2005, Article 5-1 Surveillance
Declaration of Policies
• urges Member States to develop, strengthen and maintain as soon as possible, but no later than five years from entry into force of these regulations, and the capacity to detect, assess, notify and report events in accordance with these regulations.

L 11 Epidemics and Emerging Infections 41DOH – CHD, REGIONAL EPIDEMIOLOGY and SURVEILLANCE UNIT (RESU)
Priority Diseases/Syndromes And Conditions Targeted For Surveillance
Category I (Immediately Notifiable) 1. Acute Flaccid Paralysis 2. Adverse Event Following Immunization (AEFI) 3. Anthrax 4. Human Avian Influenza 5. Measles 6. Meningococcal Disease 7. Neonatal Tetanus 8. Paralytic Shellfish Poisoning 9. Rabies 1.Severe Acute Respiratory Syndrome (SARS)
Category II (Weekly Notifiable) 1. Acute Bloody Diarrhea 2. Acute Encephalitis Syndrome 3. Acute Hemorrhagic Fever Syndrome 4. Acute Viral Hepatitis 5. Bacterial Meningitis 6. Cholera 7. Dengue 8. Diphtheria 9. Influenza-like Illness 10. Leptospirosis 11. Malaria 12. Non-neonatal Tetanus 13. Pertussis •Typhoid and Paratyphoid Fever

L 11 Epidemics and Emerging Infections 42
Medical Response
First responders must take care that they don't become
victims themselves.

L 11 Epidemics and Emerging Infections 43
Medical Response
A 1995 NBC exercise in New York City determined the first 100 emergency responders to arrive on scene 'killed'
❑ not adequately prepared or trained to deal with this incident
Los Angeles exercise ❑ doctors admitting that 'victims' have
seriously contaminated hospitals

L 11 Epidemics and Emerging Infections 44
Why is the level of epidemic preparedness so critical?
Because the consequences of not being prepared are so
catastrophic!
L 10 Complex Emergencies 45
Terrorism
❑ ‘War Within Borders’ ❑ Asia - a nesting place for terrorism and
lead member of the globe in terrorism ❑ Afghanistan ➔ Japan ❑ Vulnerability of non-involved population ❑ Unclear end-point for termination of
further, recurrent acts

L 10 Complex Emergencies 46
Weapons of Mass Destruction (WMD)❑ In warfare for 2500 years ❑ Biological - Tartars used plague-infected
corpses in Kaffa in 1346. ❑ Modern warfare (1915) - Chlorine gas ❑ Nuclear bombs - Hiroshima and Nagasaki,
1945. ❑ Nerve and vesicant agents against Iran ❑ Cyanide against the Kurds

L 10 Complex Emergencies 47
Nuclear Agents❑ Nuclear detonation through
conventional explosives ❑ Activation of Radioactive material ❑ Dissemination through
▪ Food ▪ Water ▪ Direct environmental spread

L 10 Complex Emergencies 48
Injury Profile – Nuclear Agents❑ Thermal injury - burns ❑ Eye injuries - blindness due to blast
flash ❑ Ear injuries - deafness rupture of ear
drums ❑ Penetrating wounds/orthopedic
injuries/head injuries

L 10 Complex Emergencies 49
Radiation Sickness
❑ Irradiation injuries do not make the patient radioactive!
❑ Decontamination before transport
❑ Removal of all clothing ❑ Tepid bathing of skin surface

L 10 Complex Emergencies 50
Biological agents
❑ Infectious disease or toxin that can be used in bioterrorism or biological warfare
❑ Viruses, microorganisms (bacteria and fungi) and their associated toxins
❑ Can be delivered with conventional explosives, air, food and water

L 10 Complex Emergencies 51
❑ Incubation period: delay in time of exposure until clinical symptoms
❑ Some are rapidly fatal ❑ Others are severely incapacitating ❑ Extensive exposure may occur
before the primary event is revealed
Biological Agents

L 10 Complex Emergencies 52
Biological agents
❑ Bacteria - Anthrax, Brucellosis, Plague & Cholera
❑ Viruses - smallpox / hemorrhagic fever
❑ Biological products - Botulinum toxin, endotoxins, mycotoxin

L 10 Complex Emergencies 53
Anthrax
❑

L 10 Complex Emergencies 54
Plague
❑ Bubonic Plague – Enlarged Lymph nodes
❑“Black Death” – Peripheral
gangrene
L 10 Complex Emergencies 55
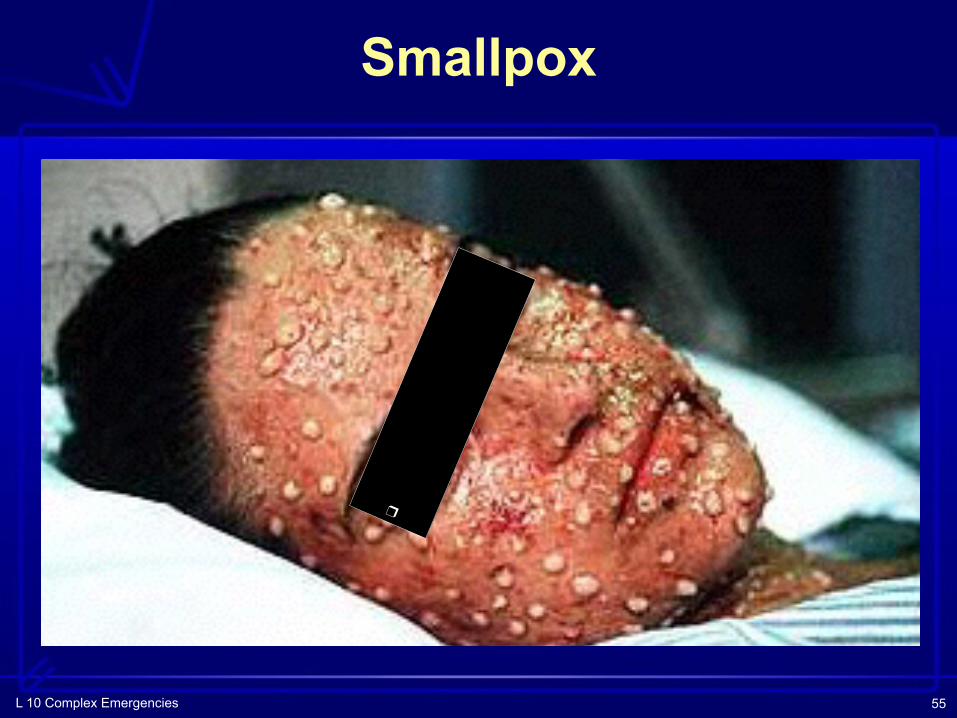
Smallpox
❑

L 10 Complex Emergencies 56
Chemical Agents
Chlorine gas dispersion during World War I

L 10 Complex Emergencies 57
❑ About 70 chemicals are documented in history as WMD which include:
Chlorine, Phosgene, Cyanide
and Vesicants (‘Nitrogen Mustard’)
❑ Exposure may not be revealed until chemical injuries are recognized
❑ On-site decontamination
Chemical Agents

L 10 Complex Emergencies 58
Nerve Gas (Sarin Gas Attack - Japan)
❑ Sarin - fluorinated phosphinate ❑ Similar to Insecticide - malathion ❑ Attacks the
nervous system

L 10 Complex Emergencies 59
NBC incident – Characteristics
❑ Mass casualties with similar symptoms ❑ Dissemination device ❑ Receipt of warning ❑ Hospital may receive untreated casualties
direct from the site ❑ Rescue personnel could become victims
due to unavailability of information
Fill in the Blank

L 10 Complex Emergencies 60
Hospital Preparedness for NBC Events
❑ Management system for mass NBC casualties
❑ HAZMAT suits and PPE for staff ❑ Education of staff and community
regarding local and regional risks ❑ Training in patient decontamination
Fill in the Blank

L 10 Complex Emergencies 61
Decontamination Protocols
❑ Patients could arrive at hospital prior to decontamination
❑ Risk to health care professionals who would subsequently require decontamination.
❑ Designated Decontamination areas in the Hospital
Fill in the Blank

L 10 Complex Emergencies 62
Review of Objectives As a result of this session, you should be able
to: ❑ Describe the characteristics and
challenges of Complex Disasters. ❑ Identify the salient features of NBC
incidents and the response required. ❑ Outline major health effects and hospital
preparedness for complex disasters.

L 11 Epidemics and Emerging Infections 63
Summary❑ Epidemics pose challenges for medical
personnel. ❑ Preparedness for an appropriate hospital
response activated is essential, while ensuring the safety of personnel.
❑ EMS may not provide the most effective and immediate medical response.
❑ Successful outcome of the medical care requires adequate preparedness.

L 11 Epidemics and Emerging Infections 64
Summary
❑ Planning, disciplined & coordinated behavior by personnel, mobilization ability, availability of medical resources, and communication are essential in effective care.
Continue…

L 11 Epidemics and Emerging Infections 65
Objectives
❑ Identify the fundamentals of a hospital preparedness and response plan for epidemics.
Upon completion of this unit you will be able to:

L 11 Epidemics and Emerging Infections 66
Exercise
❑ What resources does your hospital have which can be applied to a CBR incident?
❑ What training is required for EM personnel in order to mount a safe and effective hospital response to a CBR incident?
❑ With what other agencies should the hospital be conducting joint CBR exercises?

L 11 Epidemics and Emerging Infections 67
❑ With whom should the hospital coordinate regularly on CBR issues?
❑ Who should be represented on your hospital’s CBR functional preparedness committee?
Exercise
Continue…