rapid sequence intubation what every emergency physician must know
DESCRIPTION
Rapid Sequence Intubation What Every Emergency physician Must Know. Abdullah ALsakka EM Consultant KKUH. What do the following have in common?. 37 year old asthmatic man in extremis 22 year old overdose patient - barely arouses to pain 30 year old multiple trauma patient - PowerPoint PPT PresentationTRANSCRIPT
Rapid Sequence Intubation
What Every Emergency physician Must Know
Abdullah ALsakkaEM Consultant KKUH
What do the following have in common?
37 year old asthmatic man in extremis
22 year old overdose patient - barely arouses to pain
30 year old multiple trauma patient 67 year old man in cardiogenic shock 80 year old woman in refractory
pulmonary edema
Key Questions:Objectives
• What exactly is “RSI”?• Why use drugs?• Can I mitigate adverse effects?• What induction agent do I use?• What NMBA do I use?
Key Questions
• What exactly is “RSI”?• Why use drugs?• Can I mitigate adverse effects?• What induction agent do I use?• What NMBA do I use?
Rapid Sequence Intubation
Definition
The virtually simultaneous administration of a potent sedative agent and a
neuromuscular blocking agent to induce unconsciousness and motor paralysis for
tracheal intubation.
History
1979 first series of ED intubations – Taryle, 1979
1982 first series of intubations using succinylcholine in the ED – Thompson, 1982
History
1997 ACEP RSI policy statement:
“physicians performing RSI should possess training, knowledge, and experience in the techniques and pharmacologic agents used to perform
RSI”
“NMBA and appropriate sedative and induction agents should be immediately available in the ED and accessible to all physicians who perform RSI in the ED”
Reaffirmed, 2000
Rapid Sequence Intubation
Definition Incorporates:
• Patient has a full stomach• Preoxygenation• No interposed ventilation• Sellick’s maneuver
Rapid Sequence Intubation
Advantages of RSI
• Rapid control of the airway• Minimizes risk of aspiration• Highest success rates• Lowest complication rates• Optimal intubating conditions• Adaptable to patient condition
The Evidence
Prospective observational and retrospective studies National Emergency Airway Registry (NEAR)
Series of > 6000 ED intubations 26 teaching hospitals 88.1% adult and 81.1% pediatric intubations
performed by the EP
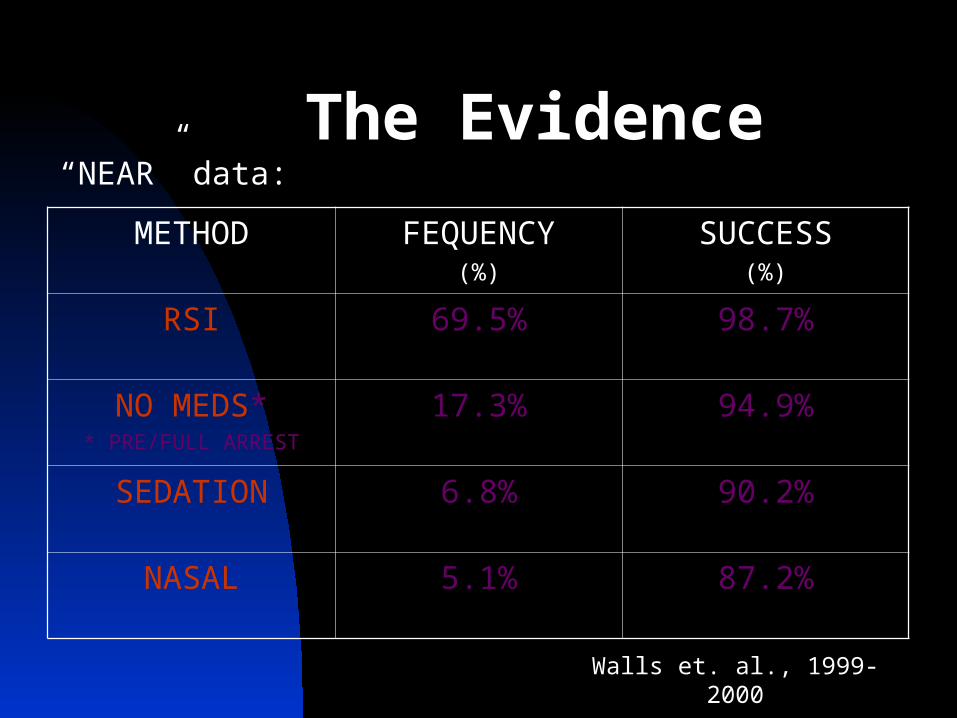
The Evidence
METHOD FEQUENCY(%)
SUCCESS(%)
RSI 69.5% 98.7%
NO MEDS** PRE/FULL ARREST
17.3% 94.9%
SEDATION 6.8% 90.2%
NASAL 5.1% 87.2%
“NEAR” data:
Walls et. al., 1999-2000
ABSTRACT
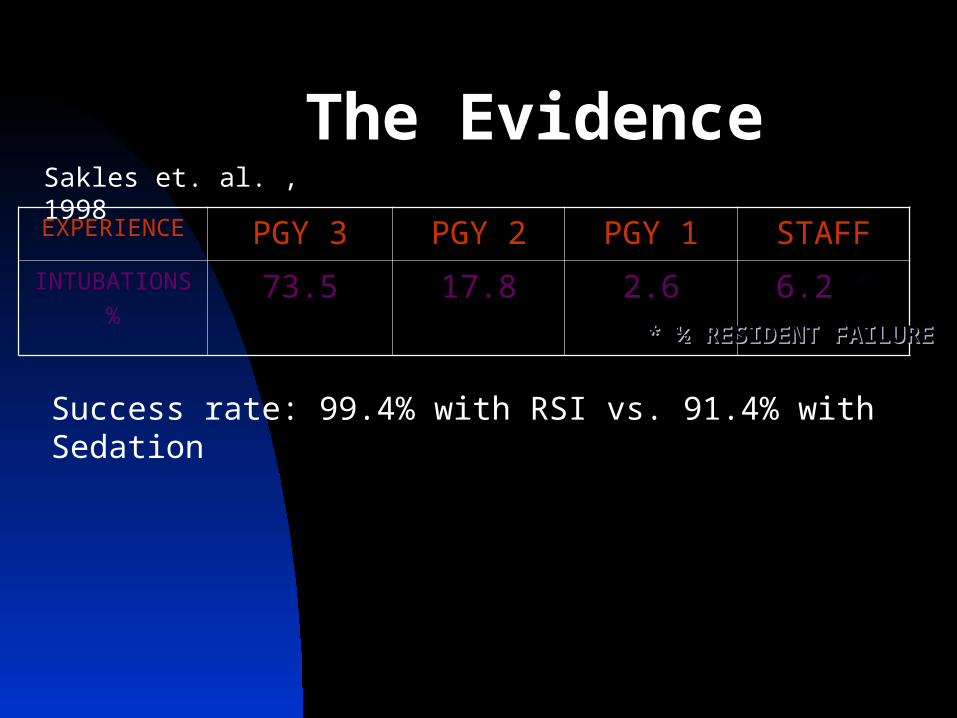
The Evidence
EXPERIENCE PGY 3 PGY 2 PGY 1 STAFFINTUBATIONS
%73.5 17.8 2.6 6.2 *
* ½ RESIDENT * ½ RESIDENT FAILUREFAILURE
Sakles et. al. , 1998
Success rate: 99.4% with RSI vs. 91.4% with Sedation
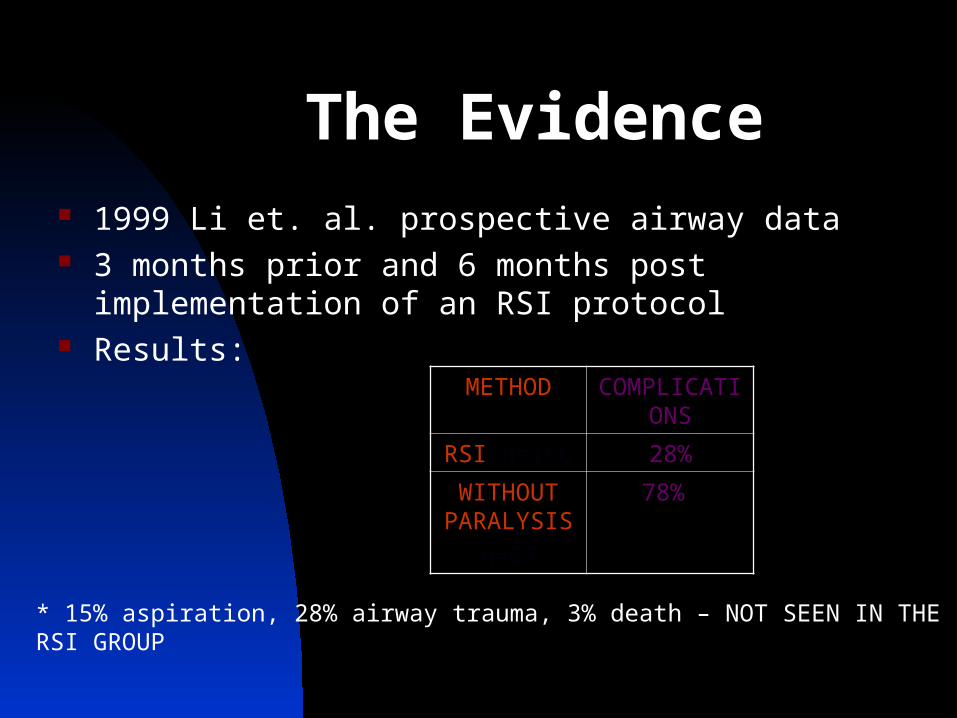
The Evidence 1999 Li et. al. prospective airway data 3 months prior and 6 months post implementation of an
RSI protocol Results:
METHOD COMPLICATIONS
RSI n=166 28%
WITHOUT PARALYSIS
n=67
78%*
* 15% aspiration, 28% airway trauma, 3% death – NOT SEEN IN THE RSI GROUP
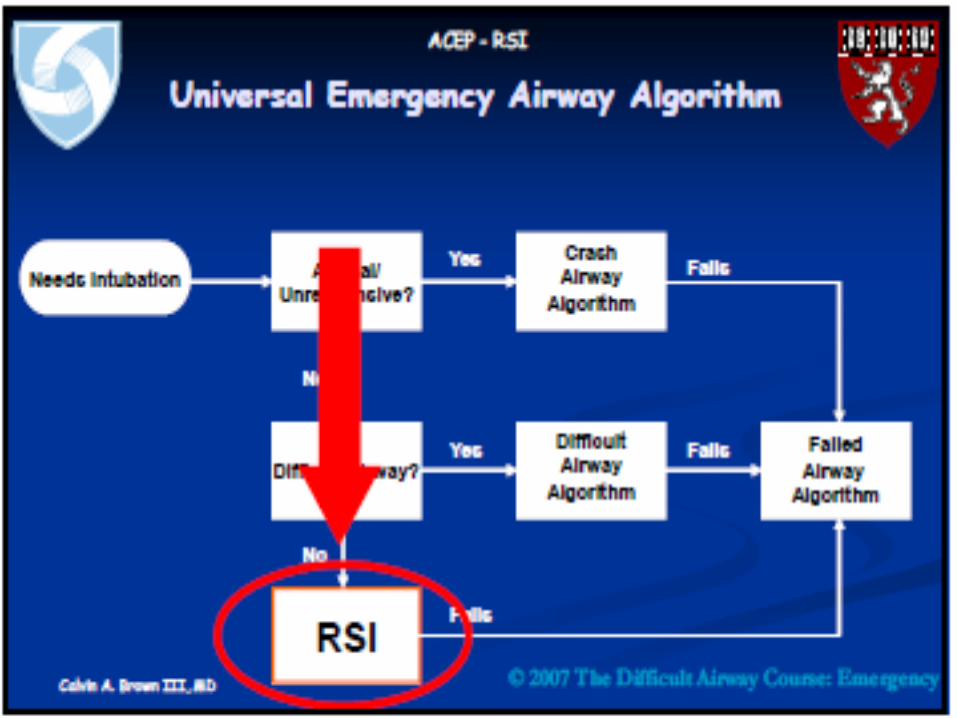
RSI
What are the contraindications to RSI?
RSI
The predicted difficult airway
Inexperience
Inadequate difficult airway tools and techniques
Rapid Sequence Intubation
The Seven Ps of RSI
PreparationPreoxygenationPretreatmentParalysis with inductionPositioning Placement with proofPost-Intubation Management
Rapid Sequence Intubation
The Sequence
Zero: the time of administration
of succinylcholine.
Zero - 10 minutes
Preparation• Assess airway difficulty (LEMON)• Plan approach• Assemble drugs and equipment• Establish access• Establish monitoring
Rapid Sequence Intubation
The Sequence
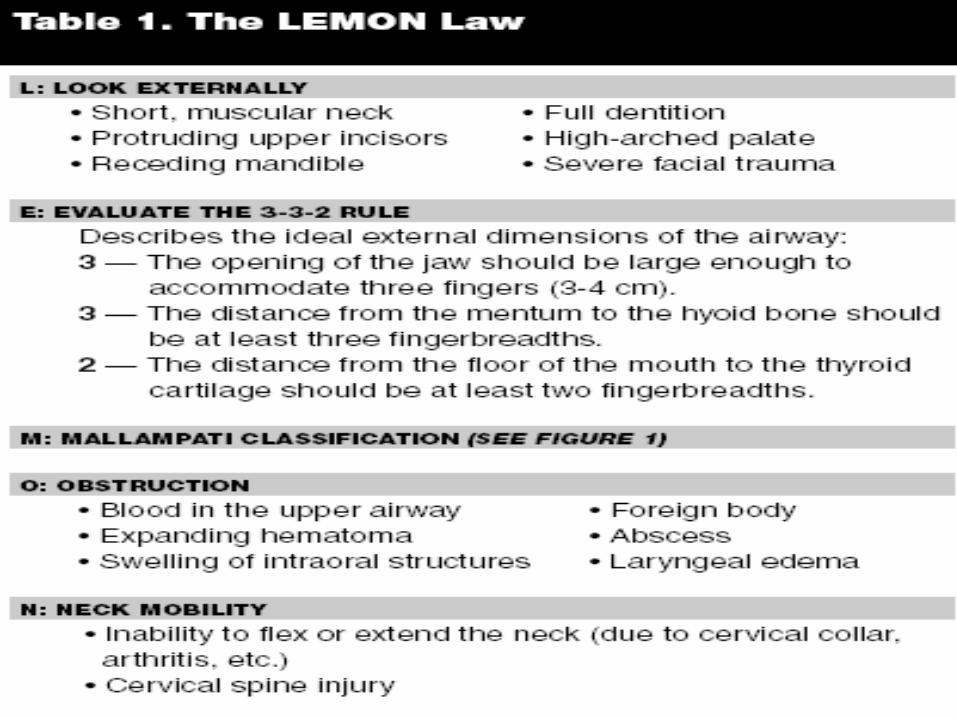
Rapid Sequence IntubationThe Difficult Airway Rule
L ook externallyE valuate 3-3-2M allampatiO bstruction?N eck mobility

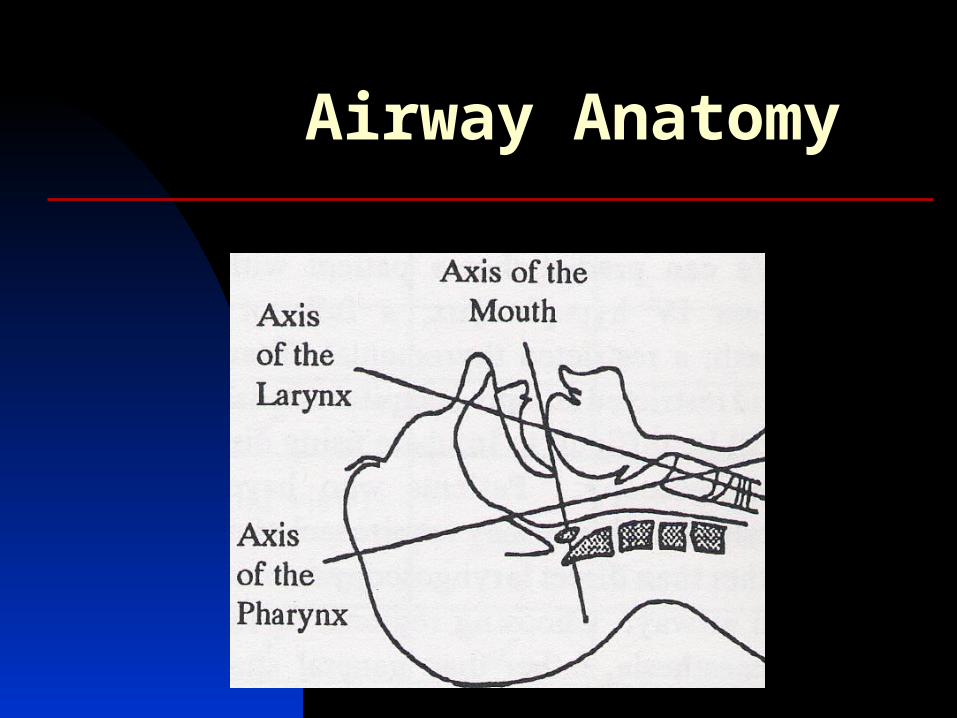
Airway Anatomy
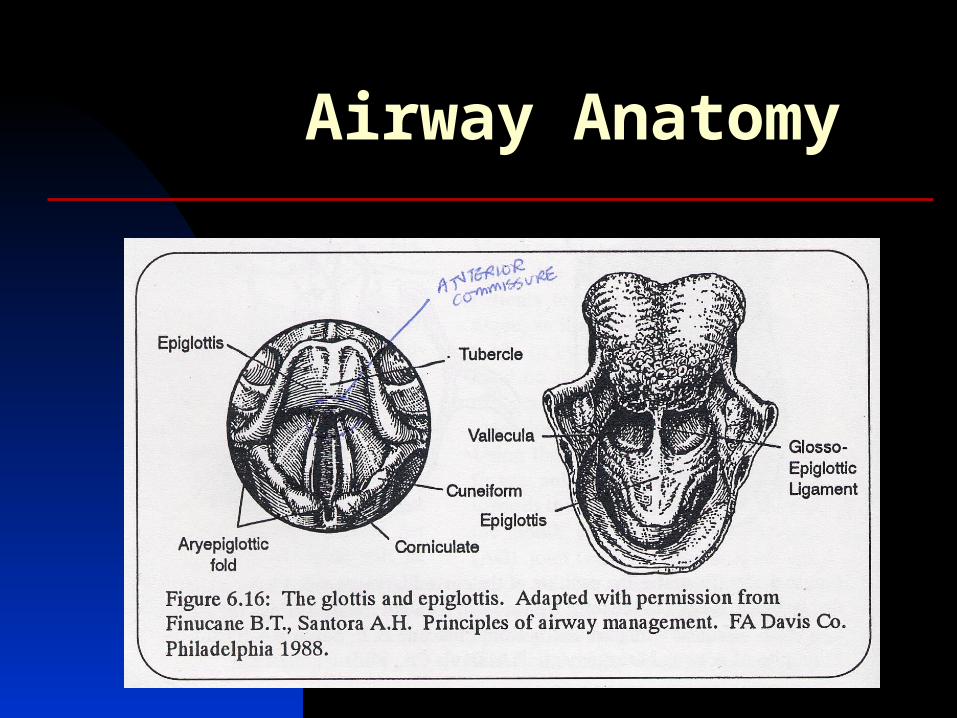
Airway Anatomy
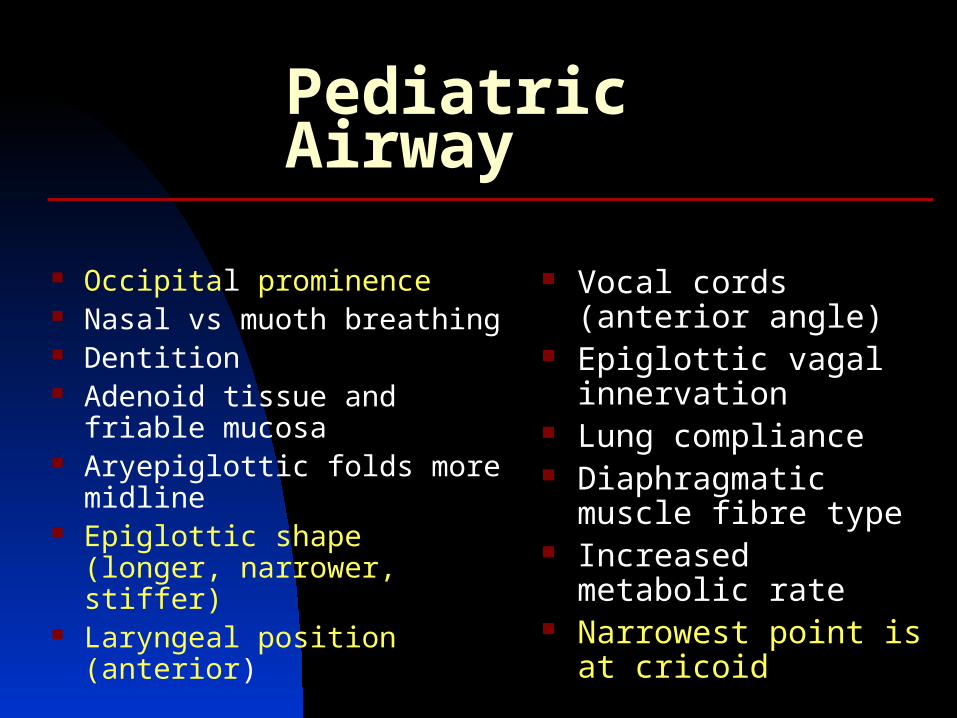
Pediatric Airway
Occipital prominence Nasal vs muoth breathing Dentition Adenoid tissue and friable
mucosa Aryepiglottic folds more
midline Epiglottic shape (longer,
narrower, stiffer) Laryngeal position (anterior)
Vocal cords (anterior angle)
Epiglottic vagal innervation
Lung compliance Diaphragmatic muscle
fibre type Increased metabolic rate Narrowest point is at
cricoid
Rapid Sequence IntubationThe Difficult Airway Rule
L ook externallyE valuate 3-3-2M allampatiO bstruction?N eck mobility
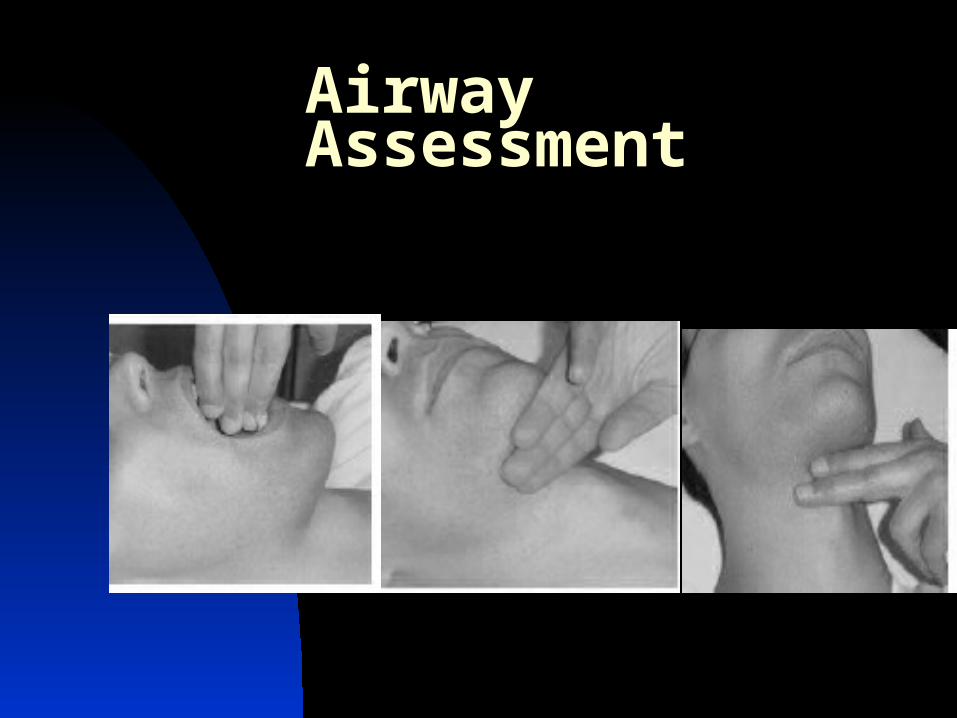
Airway Assessment
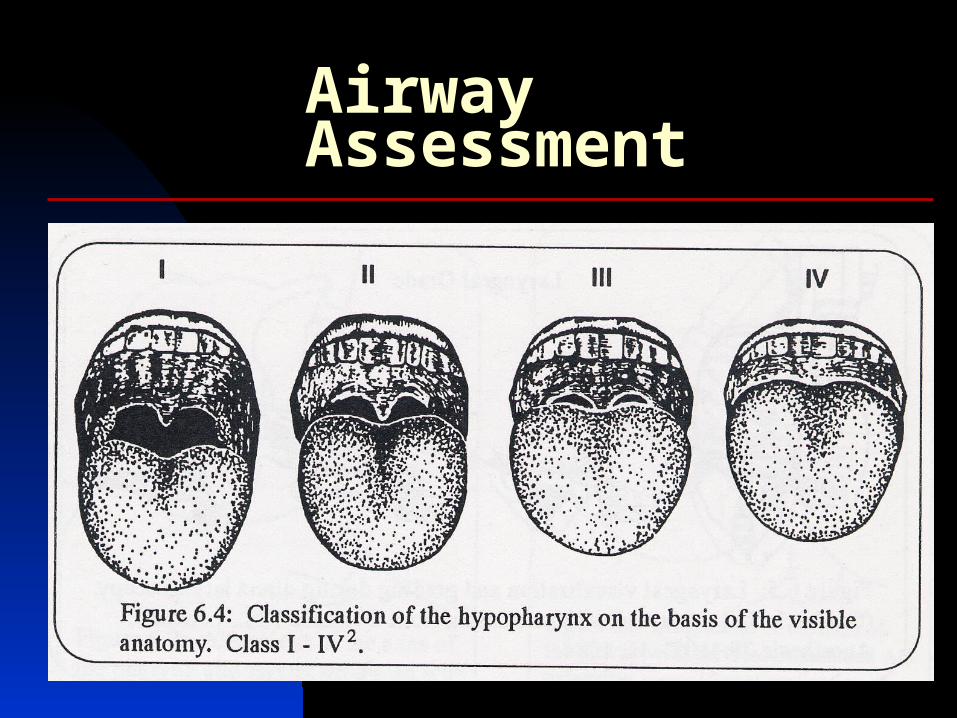
Airway Assessment
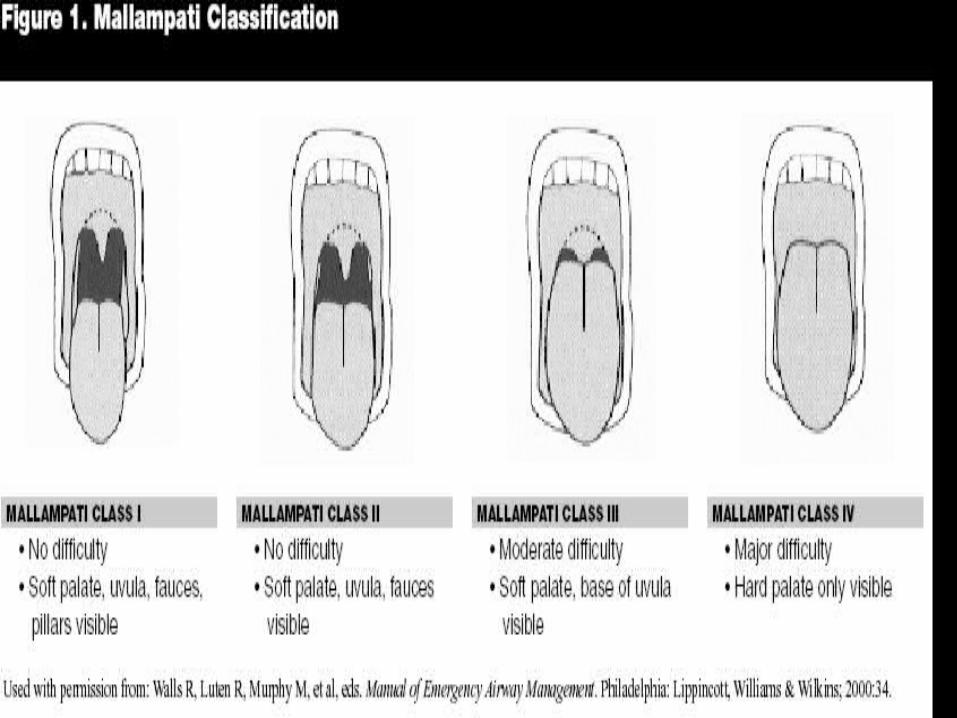
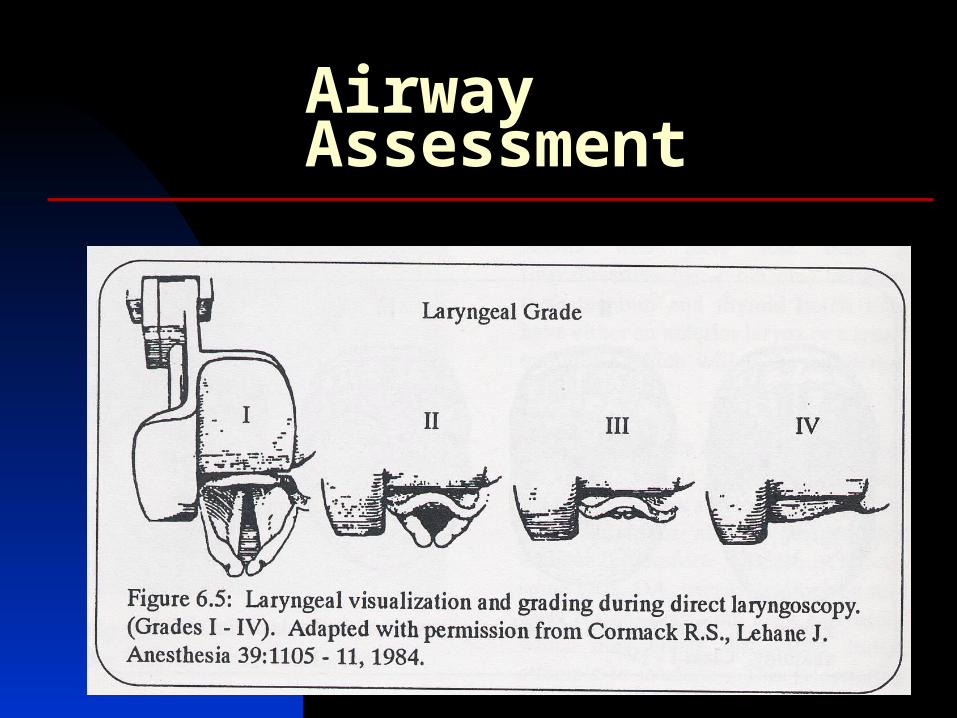
Airway Assessment

Zero - 5 minutes
Preoxygenation
• 100% oxygen for five minutes• 8 vital capacity breaths• Provides essential apnea time• Apnea time varies
Rapid Sequence Intubation
The Sequence
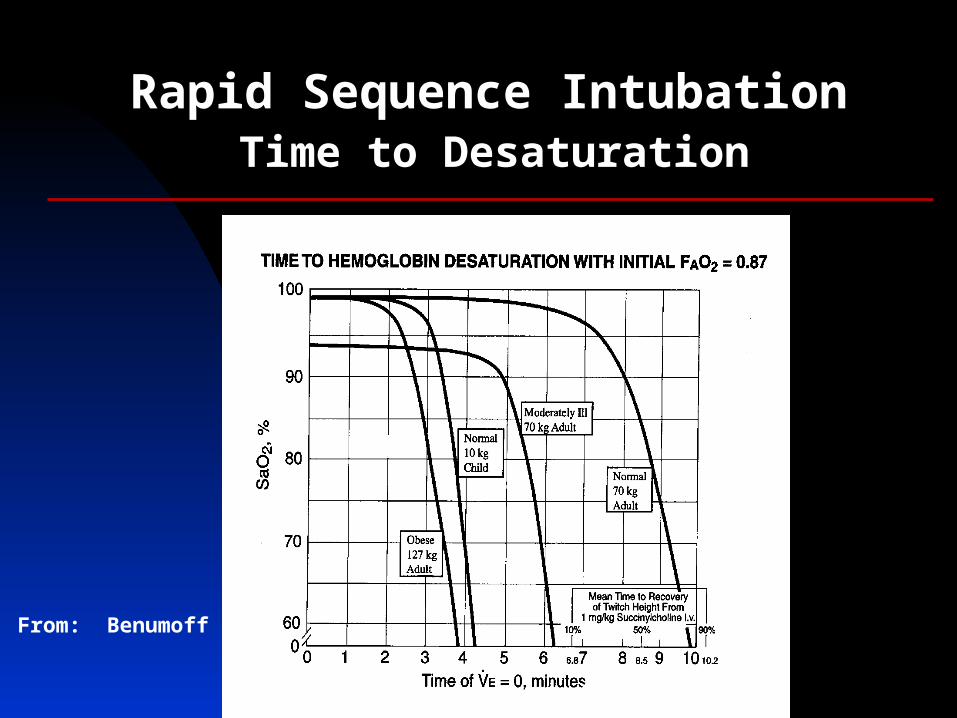
Rapid Sequence IntubationTime to Desaturation
From: Benumoff

Zero - 3 minutes
Pretreatment• Lidocaine• Opioid• Atropine• Defasciculation
“LOAD the patient before intubation.”
Rapid Sequence Intubation
The Sequence
Zero!!
Paralysis with induction
• Induction agent IV push • Neuromuscular blocking agent IV push
Rapid Sequence Intubation
The Sequence
Rapid Sequence Intubation
1. INDUCTION
2. PRESSURE
3. PARALYSIS
INTUBATION
Rapid Sequence Intubation
Zero + 30 seconds
Protection
• Sellick’s Maneuver• Position patient• Do not bag unless S O < 90%p 2
The Sequence
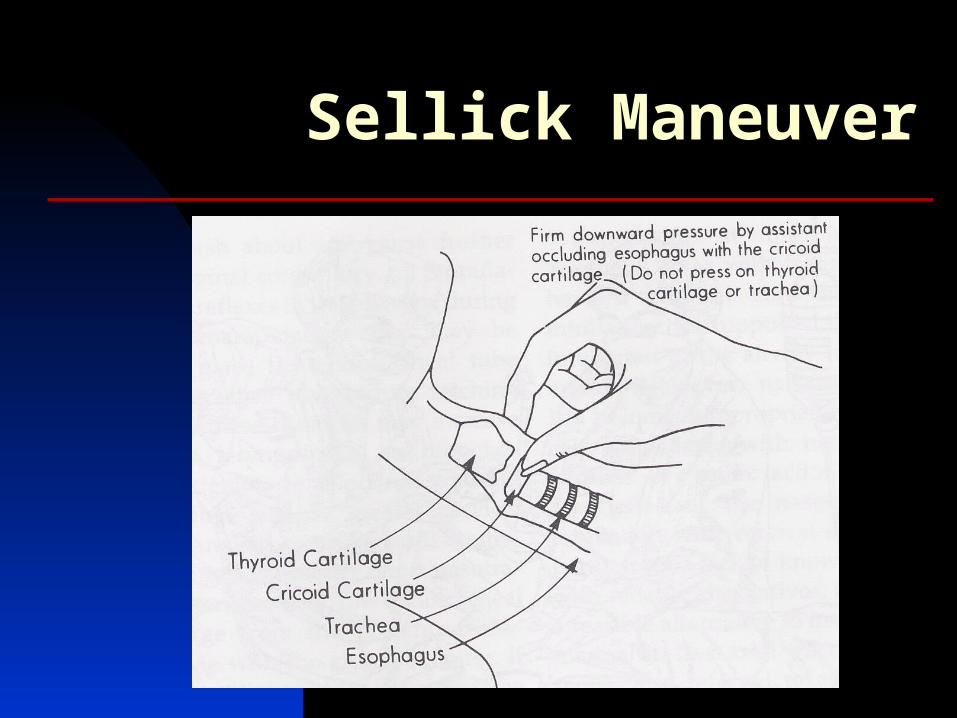
Sellick Maneuver

CRICOID PRESSURE IN EMERGENCY RAPID SEQUENCE INTUBATION
CONCLUSIONS: Although application of cricoid pressure has been described as the "linchpin of RSI" and has come to be a widely accepted practice, there is no clear evidence to suggest that it reduces the risk of aspiration during RSI.
Butler, J., Emerg Med J 22:815, November 2005
LARYNGEAL VIEW DURING LARYNGOSCOPY: A RANDOMIZED TRIAL COMPARING CRICOID PRESSURE, BACKWARD-UPWARD-RIGHTWARD PRESSURE, AND BIMANUAL LARYNGOSCOPY
CONCLUSIONS: bimanual laryngoscopy was more effective than cricoid pressure or the BURP maneuver in improving laryngoscopic visualization for intubation
Levitan, R.M., et al, Ann Emerg Med 27(6):548, June 2006
Zero + 45 seconds
Placement
• Check mandible for flaccidity• Intubate, remove stylet• Confirm tube placement - ET CO2
• Release Sellick’s maneuver
Rapid Sequence Intubation
The Sequence
‘BURP’ Technique
Blade (type, size, placement)
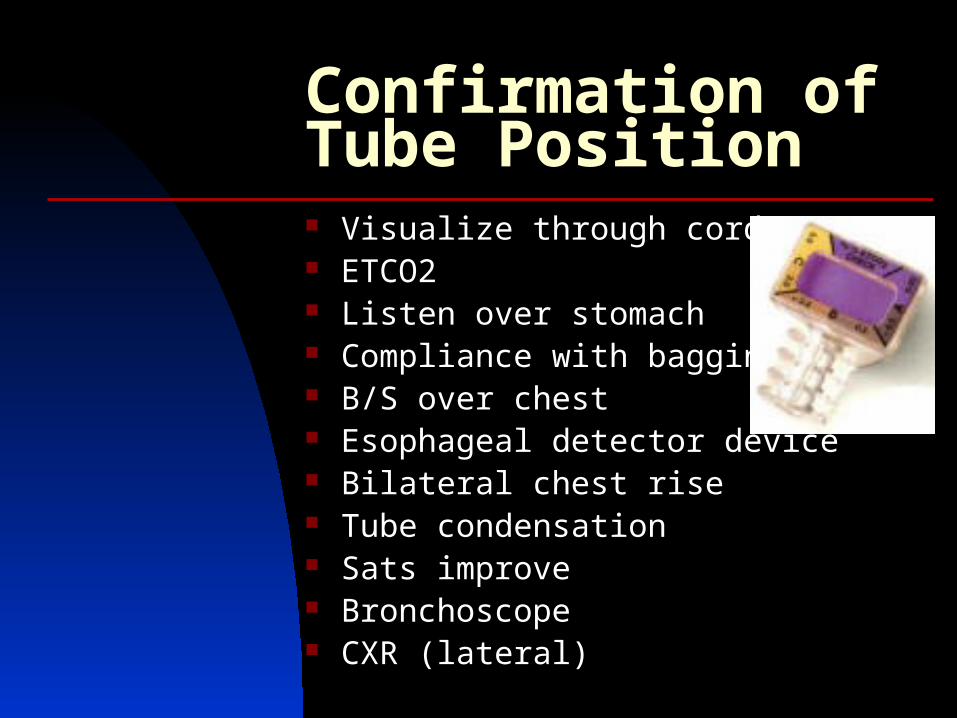
Confirmation of Tube Position Visualize through cords ETCO2 Listen over stomach Compliance with bagging B/S over chest Esophageal detector device Bilateral chest rise Tube condensation Sats improve Bronchoscope CXR (lateral)
Zero + 90 seconds
Post-intubation Management
• Secure tube• Chest x-ray• Long acting sedation/paralysis• Establish ventilator parameters
Rapid Sequence Intubation
The Sequence
Summary
The Seven Ps of RSI
PreparationPreoxygenationPretreatmentParalysis with inductionProtectionPlacementPost-Intubation Management
Rapid Sequence Intubation
• The first rescue from failed intubation is bagging
• The first rescue from failed bagging is better bagging
Rescue Maneuvers
Rapid Sequence Intubation
Failed Attempt
Key Questions
• What exactly is “RSI”?• Why use drugs?• Can I mitigate adverse effects?• What induction agent do I use?• What NMBA do I use?
Why use drugs?
• Blunt perception and recall• Make intubation easier• Mitigate adverse responses• Improve patient condition
Key Questions
• What exactly is “RSI”?• Why use drugs?• Can I mitigate adverse effects?• What induction agent do I use?• What NMBA do I use?
WHAT CAUSES THE RESPONSE?
• Laryngoscopy and intubation cause bronchospasm
ICP catecholamines
• Succinylcholine causes ICP
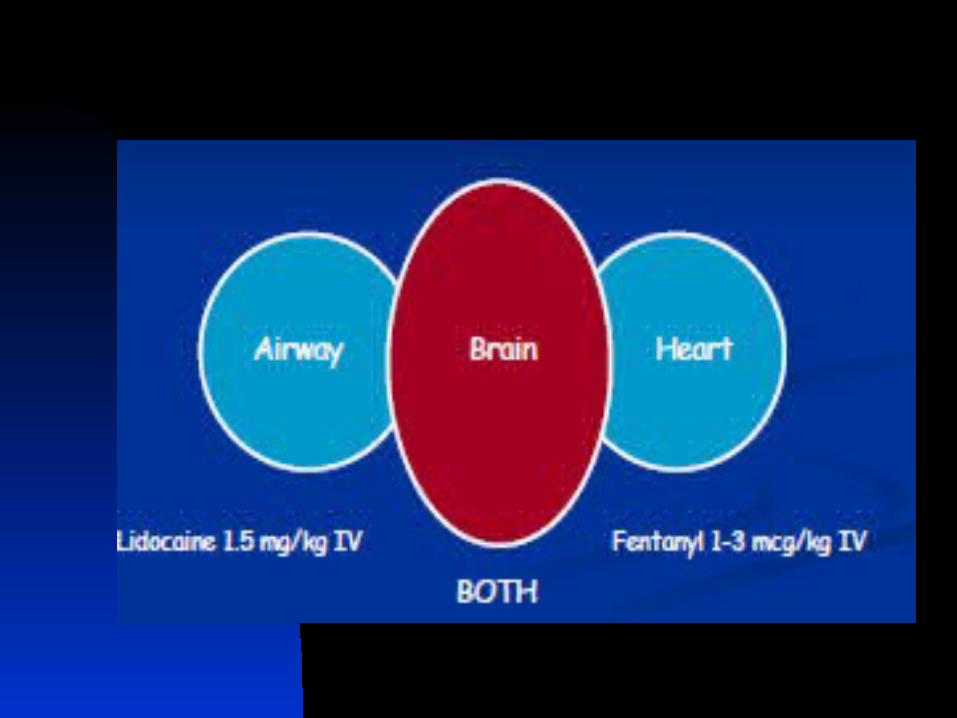
PATIENTS AT RISK
• Intracranial pathology “tight brain”• Cardiovascular disease “tight heart” “floppy heart”• Reactive airways disease “tight lungs”
• Pretreatment: L.O.A.D.
• Induction agents
ATTENUATING THE RESPONSE
L.O.A.D.• L idocaine• O pioid• A tropine no longer use• D efasciculation no
The Pretreatment drugs for RSIGive 3 minutes before SCh
LIDOCAINE
1.5 mg/kg
• Increased intracranial pressure• Bronchospasm
OPIOID
Fentanyl 3 g/kgMay give slowly over 3 minutes
• Cardiovascular disease• Intracranial hypertension
Caution if dependent on sympathetic drive
Atropine
•No longer recommended
DEFASCICULATION
•No longer recommended

Key Questions
• What exactly is “RSI”?• Why use drugs?• Can I mitigate adverse effects?• What induction agent do I use?• What NMBA do I use?
PHARMACOLOGIC INDUCTION
GOAL: INDUCTION OF UNCONSCIOUSNESS Doses dependent on:
Weight Hemodynamics Level of consciousness age
Etomidate Imidazole derivative ACTION
Sedative-hypnotic INDICATION
Hemodynamic instability Respiratory compromise increased ICP
DOSE 0.3 mg/kg iv
ADVERSE EFFECTS Adrenal suppression No analgesia property Pain on injection
Etomidate does cause adrenal insufficiency?
Not clear this affects overall survival
Barbiturates Sodium thiopental ACTION
GABAergic INDICATION
Increased ICP DOSE
3-5 mg/kg ADVERSE EFFECT
Negative inotrope and venodialtor (+) histamine release Apnea No analgesic property
Benzodiazepines Midazolam ACTION
GABAergic INDICATIONS
Cerebroprotective Amnesia Anxiolysis Muscle relaxation
DOSE 0.1 - 0.3 mg/kg (induction)
ADVERSE EFFECT Negative inotrope No analgesia property
Ketamine Phencyclidine derivative ACTION
Induces a cataleptic state INDICATION
Obstructive airway disease Hemodynamic instability Analgesia
DOSE 1-2 mg/kg
ADVERSE EFFECTS Myocardial depressant, induces tachycardia (via SNS) Unpleasant emergence
Ketamine in Head Injury Can you use ketamine in head injured patients?
• Critical review of literature
• Included 79 studies
• May improve cerebral perfusion
Neuroprotective
• No negative effects, possibly beneficial
Himmelseher S, et al. Anesth Analg 2005;101:524
Propofol Alkylphenol ACTION
Hypnotic, mechanism unknown (GABA) INDICATION
Increased ICP or IOP Amnesia Status epilepticus
DOSE 1-3 mg/kg
ADVERSE EFFECT Decreases cerebral perfusion myocardial and respiratory depression Venodilation Pain on injection No analgesic property
INDUCTION AGENTS HEALTHY, STABLE PATIENTS
• Etomidate 0.3 mg/kg• Midazolam 0.2-0.3 mg/kg• Ketamine 1.5 mg/kg• Propofol 1-3 mg/kg• Pentothal 3 mg/kg
“IV Push”
• Etomidate 0.15 mg/kg• Midazolam 0.1 mg/kg• Ketamine 1 mg/kg• Propofol 0.5 mg/kg• Pentothal 1.5 mg/kg
INDUCTION AGENTS COMPROMISED, UNSTABLE PATIENTS
INDUCTION AGENTS Special Circumstances
Reactive airways ketamineICP etomidate/pentothalHypotensive ketamine/etomidate
Operator preference

Key Questions
• What exactly is “RSI”?• Why use drugs?• Can I mitigate adverse effects?• What induction agent do I use?• What NMBA do I use?
NEUROMUSCULAR BLOCKING AGENTS
• Depolarizing - succinylcholine • Competitive (nondepolarizing)
• Aminosteroids•Rocuronium, vecuronium
• Benzylisoquinolines•Curare
•Benzylisoquinoliniums•Atracurium, mivacurium
SUCCINYLCHOLINE
• Rapid onset / brief duration• May ICP• Fatal hyperkalemia
• burns beyond day one• active neuromuscular disease• crush injuries• intra-abdominal sepsis
USE OF NONDEPOLARIZERS
• Pretreatment no more use
• Rapid sequence intubation rocuronium
• Maintaining paralysis for ventilation
What do the following have in common?
37 year old asthmatic man in extremis 22 year old overdose patient - barely
arouses to pain 30 year old multiple trauma patient 67 year old man in cardiogenic shock 80 year old woman in refractory
pulmonary edema
What do the following have in common?
All should be intubated with RSI in the absence of identified difficult airway attributes


Rapid Sequence Intubation
Questions ?
• Walls RM, et al: Manual of Emergency Airway Management, LWW, 2004