etomidate in pediatric rapid sequence intubation: gaba, gaba...
TRANSCRIPT
Etomidate in pediatric rapid sequence intubation: GABA, GABA doo or GABA, GABA don’t?
Ellen Robinson, Pharm.D. PGY-2 Emergency Medicine Pharmacy Resident
Department of Pharmacy, University Health System, San Antonio, TX Division of Pharmacotherapy, The University of Texas at Austin College of Pharmacy
Pharmacotherapy Education and Research Center, University of Texas Health Science Center at San Antonio
September 16, 2016
Learning Objectives:
1. Review steps and considerations for rapid sequence intubation (RSI)2. Explain anatomical and physiologic considerations for pediatric RSI3. Describe medications used in RSI4. Identify the controversial use of etomidate in the pediatric population5. Analyze pediatric safety and efficacy literature for etomidate in pediatric RSI

Robinson
2
Rapid Sequence Intubation
Rapid Sequence Intubation Review
• Airway compromise is the most common cause of mortality in acutely ill and injured children1
• RSI provides a method for emergent airway placement

Robinson
3
I. Purpose1-3 A. Airway management is a primary provider role in the
emergency department (ED)1 B. RSI is preferred method for emergent intubation in patients
with varying levels of consciousness and presumed to have a full stomach
C. Process designed to quickly secure an airway in patients requiring assisted ventilation3
D. With appropriate technique, RSI’s success rate is 98.5% II. Indications for RSI4-11
III. RSI Procedure Overview1-3 A. Streamlined process to ensure consistent placement of an emergent airway B. The “6 P’s”
•May result from primary pulmonary disease or other processes
•Poor/absent respiratory effort, poor color, altered mental status (AMS)
Inadequate oxygenation/ventilation
•Inability to produce audible breath sounds, AMS•Inspiratory, obstructive sounds with partial airway obstruction that fails to improve
Inability to maintain/protect airway
•Thermal inhalation injuries•Severe anaphylaxis or asthma exacerbations •Sepsis
Potential for clinical deterioration
•Combative or unstable coniditions requiring prolonged studies
•Allows for airway placement in less emergent situation
Prolonged diagnostic studies or patient transport
• Assess patient for potentially difficult airway • Ensure appropriate equipment is available at bedside • Connect patient to necessary monitors and gain intravenous access • Verify requested medications based on patient-specific factors • Tight-fitting non-rebreather oxygen mask for 3-5 minutes • Achieve optimal oxygen stores • Provides nitrogen wash-out • Reserve bag mask ventilation for patients not breathing spontaneously • Airway manipulation with laryngoscope and endotracheal tube can increase heart rate (HR), intracranial pressure (ICP), blood pressure (BP), and airway resistance
• Pre-treatment with atropine, lidocaine, muscle relaxants, and opiates may attenuate these reactions
Prepare
Preoxygenate

Robinson
4
IV. Physiologic responses to RSI1 A. Elicit cough and gag reflexes B. Tachycardia and hypertension C. Hypoxia D. Elevation in ICP and intraocular pressure E. Bradycardia
V. Unique considerations in the pediatric population12-39 A. Anatomy and physiology in infants and children vary compared to adults (See Appendix A
and B for detailed description of pediatric anatomical and physiologic considerations in RSI) 1. Larger tongues, tonsils, and adenoids 2. Shorter, narrower trachea 3. Prominent occiput, superior larynx, and floppy epiglottis 4. Increased chest wall compliance leads to respiratory fatigue and failure 5. Age-related respiratory rate 6. Preferential nasal breathing 7. Lower functional residual capacity 8. Higher oxygen metabolism 9. Increased respiratory fatigue
10. Higher vagal tone
VI. Ideal pharmacokinetic properties for RSI medications1,3
• Administer sedative prior to paralytic • Give neuromuscular blocker • Base drug selection on patient-specific characteristics
• Place endotracheal (ET) tube • Connect tube to ventilator • Check for appropriate placement (listen for gastric/ breath sounds, watch for
chest rise, check end-tidal CO2, obtain chest X-ray)
• Inflate cuff and secure ET tube • Establish waveform capnography monitoring • Provide continued pain and sedation therapy
Pre-treat
Paralytic
Place tube
Post-intubation care
RSI Medication Review

Robinson
5
VII. Pre-medications1-3 A. Administered to reduce anxiety and prevent negative physiologic responses to RSI B. Optimal timing is medication dependent C. Atropine
1. May be used for pediatric patients who experience bradycardia from ET tube placement or succinylcholine administration
2. American Heart Association recommendations for use in RSI a. All patients < 1 year b. Patients 1-5 years receiving succinylcholine c. Pediatric patients > 5 receiving subsequent doses of succinylcholine
Table 1: Atropine drug information Dose Onset Duration Adverse Events Clinical Pearls
0.02 mg/kg Max: 0.5 mg 1 minute 30-60 minutes
Dry mouth Tachycardia Hypertension Pupil dilation
Dries oral secretions but onset is not quick
enough to play a role in RSI
D. Lidocaine 1. May reduce adrenergic and physiologic responses to laryngoscopy and ET tube
placement 2. May reduce ICP so may be considered for patients with traumatic brain injury (TBI)
Table 2: Lidocaine drug information Dose Onset Duration Adverse Events Clinical Pearls
1.5 mg/kg Max: 100 mg
45-90 seconds 10-20 minutes Cardiac
arrhythmias Give 3 minutes prior to
RSI for full effect
VIII. Induction Agents1-3,40 A. Unless completely unconscious, sedate all patients prior to paralytic administration B. Many sedatives have been used for RSI in the pediatric population C. Administration of sedative agent several minutes prior to paralytic is typically preferred to
assure drug has taken effect 1. Exception: short-acting sedatives can be given immediately after to provide longer
sedation D. Barbiturates1-3
Rapid onset of action Short duration of action
Negligble hemodynamic
effectsMinmial side effect profile
Quickly reversible
Robinson
6
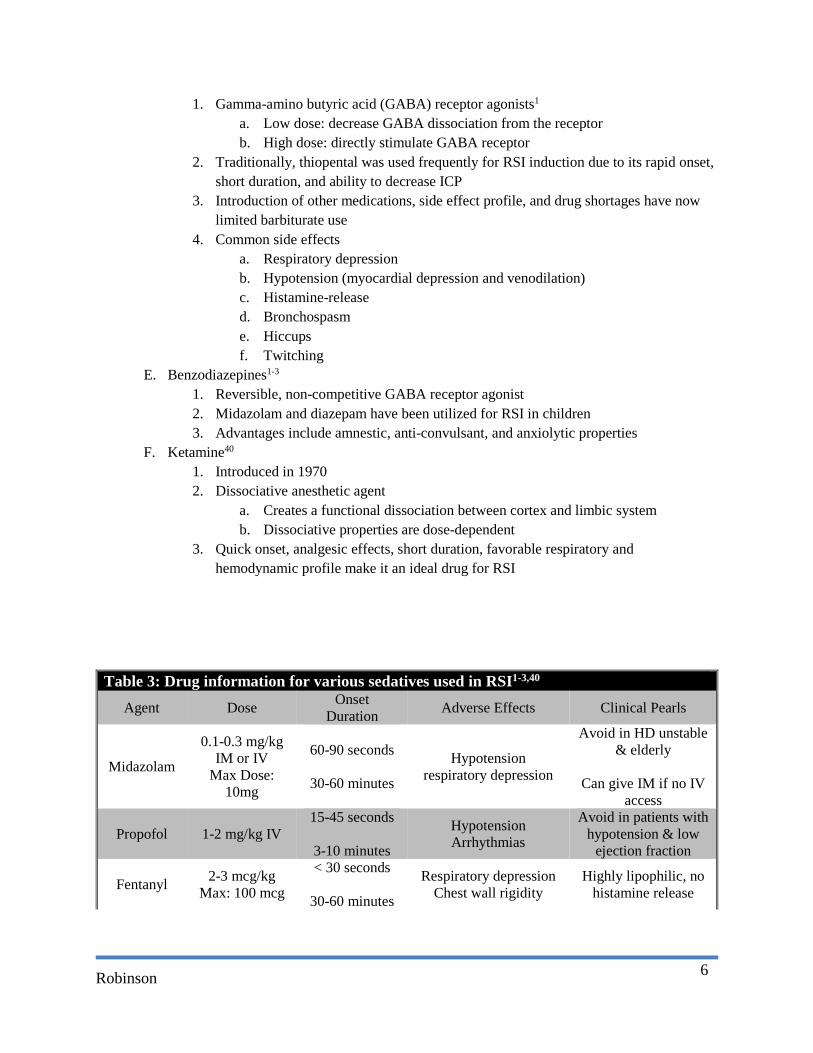
1. Gamma-amino butyric acid (GABA) receptor agonists1 a. Low dose: decrease GABA dissociation from the receptor b. High dose: directly stimulate GABA receptor
2. Traditionally, thiopental was used frequently for RSI induction due to its rapid onset, short duration, and ability to decrease ICP
3. Introduction of other medications, side effect profile, and drug shortages have now limited barbiturate use
4. Common side effects a. Respiratory depression b. Hypotension (myocardial depression and venodilation) c. Histamine-release d. Bronchospasm e. Hiccups f. Twitching
E. Benzodiazepines1-3 1. Reversible, non-competitive GABA receptor agonist 2. Midazolam and diazepam have been utilized for RSI in children 3. Advantages include amnestic, anti-convulsant, and anxiolytic properties
F. Ketamine40 1. Introduced in 1970 2. Dissociative anesthetic agent
a. Creates a functional dissociation between cortex and limbic system b. Dissociative properties are dose-dependent
3. Quick onset, analgesic effects, short duration, favorable respiratory and hemodynamic profile make it an ideal drug for RSI
Table 3: Drug information for various sedatives used in RSI1-3,40 Agent Dose Onset
Duration Adverse Effects Clinical Pearls
Midazolam
0.1-0.3 mg/kg IM or IV
Max Dose: 10mg
60-90 seconds
30-60 minutes
Hypotension respiratory depression
Avoid in HD unstable & elderly
Can give IM if no IV
access
Propofol 1-2 mg/kg IV 15-45 seconds
3-10 minutes
Hypotension Arrhythmias
Avoid in patients with hypotension & low
ejection fraction
Fentanyl 2-3 mcg/kg Max: 100 mcg
< 30 seconds
30-60 minutes
Respiratory depression Chest wall rigidity
Highly lipophilic, no histamine release
Robinson
7
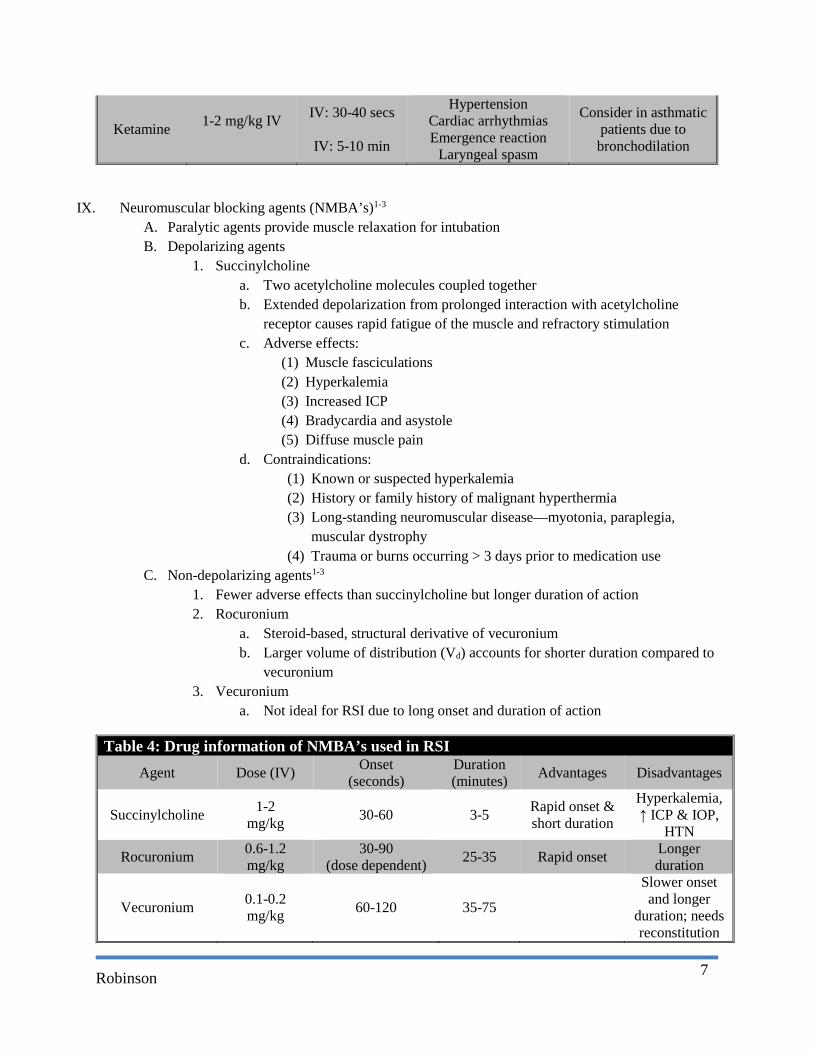
Ketamine 1-2 mg/kg IV
IV: 30-40 secs
IV: 5-10 min
Hypertension Cardiac arrhythmias Emergence reaction
Laryngeal spasm
Consider in asthmatic patients due to bronchodilation
IX. Neuromuscular blocking agents (NMBA’s)1-3 A. Paralytic agents provide muscle relaxation for intubation B. Depolarizing agents
1. Succinylcholine a. Two acetylcholine molecules coupled together b. Extended depolarization from prolonged interaction with acetylcholine
receptor causes rapid fatigue of the muscle and refractory stimulation c. Adverse effects:
(1) Muscle fasciculations (2) Hyperkalemia (3) Increased ICP (4) Bradycardia and asystole (5) Diffuse muscle pain
d. Contraindications: (1) Known or suspected hyperkalemia (2) History or family history of malignant hyperthermia (3) Long-standing neuromuscular disease—myotonia, paraplegia,
muscular dystrophy (4) Trauma or burns occurring > 3 days prior to medication use
C. Non-depolarizing agents1-3 1. Fewer adverse effects than succinylcholine but longer duration of action 2. Rocuronium
a. Steroid-based, structural derivative of vecuronium b. Larger volume of distribution (Vd) accounts for shorter duration compared to
vecuronium 3. Vecuronium
a. Not ideal for RSI due to long onset and duration of action
Table 4: Drug information of NMBA’s used in RSI Agent Dose (IV) Onset
(seconds) Duration (minutes) Advantages Disadvantages
Succinylcholine 1-2 mg/kg 30-60 3-5 Rapid onset &
short duration
Hyperkalemia, ↑ ICP & IOP,
HTN
Rocuronium 0.6-1.2 mg/kg
30-90 (dose dependent) 25-35 Rapid onset Longer
duration
Vecuronium 0.1-0.2 mg/kg 60-120 35-75
Slower onset and longer
duration; needs reconstitution
Robinson
8
IOP: intraocular pressure; HTN: hypertension
X. History of etomidate41-48 A. Past use of etomidate
1. 1972 a. Approved in Europe b. Used for endotracheal intubation and continuous sedation in mechanically
ventilated patients 2. 198342
a. Approved in United States b. Startling series of deaths in multi-trauma ICU patients raised concern and
prompted investigation c. Additional studies revealed adrenal suppression during continuous infusion d. Etomidate’s indication for continuous sedation was withdrawn
XI. Mechanism of action42,49 A. Carboxylated imidazole derivative B. Ultrashort-acting, non-barbiturate sedative agent C. Acts centrally through GABA receptor stimulation and depression of reticular activating
system XII. Adverse effect profile
A. Hemodynamically neutral 1. Decreased hypotension risk 2. Decreased cardiac event risk
B. Neuro-protective effects 1. Reduces ICP through a decrease in cerebral blood flow and O2 consumption
a. Bramwell et al.49 found single-dose etomidate use in pediatric patients with severe TBI resulted in significant ICP reduction
2. Maintains cerebral perfusion pressure 3. Can be utilized in trauma population with head injuries
C. Adrenocortical suppression40 1. 11-β hydroxylase enzyme inhibition reduces cortisol, aldosterone, and cortisone
production 2. Adrenal suppression duration, following one dose, varies between studies
a. Duthie et al.50 demonstrated decreased plasma cortisol levels 1 hour post etomidate induction but no difference at 24 hours
b. Absalom et al.51 & Donmez et al.52 reported decreased cortisol levels that continued at 24 hours
c. Vinclair et al.53 studied 40 patients and reported adrenal insufficiency in 80% at 12 hours, 9% at 48 hours, and 7% at 72 hours following one induction etomidate dose
Etomidate Review
Robinson
9
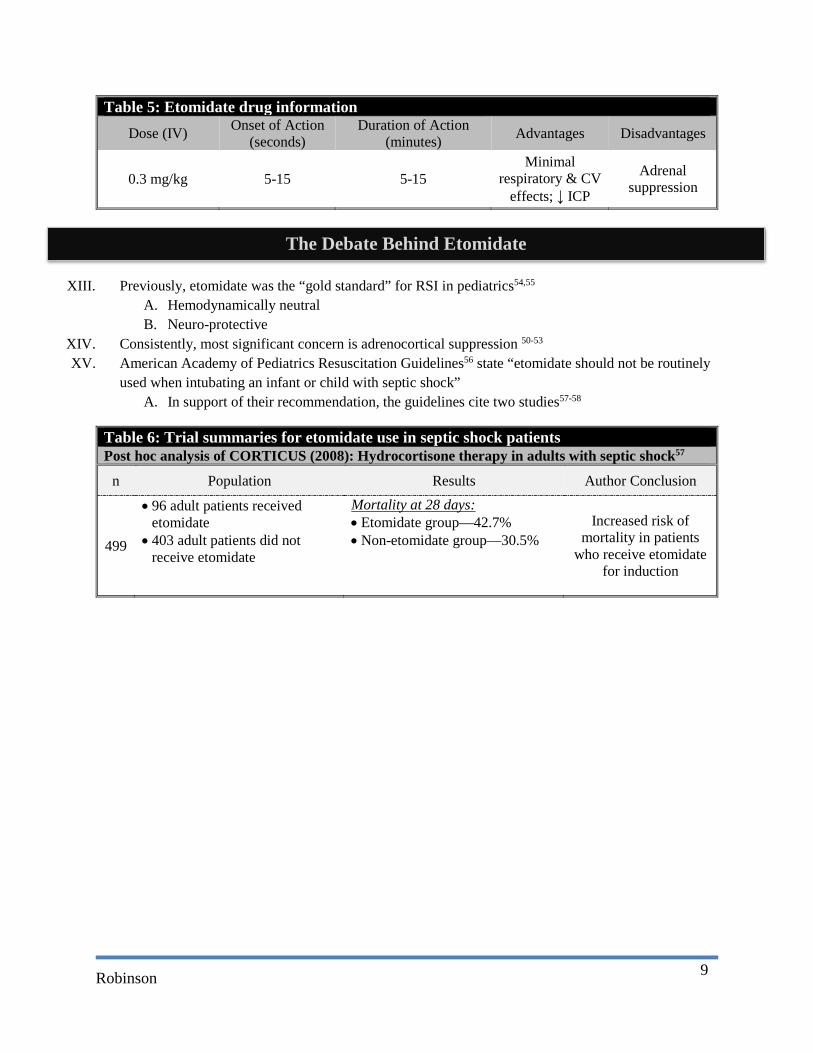
Table 5: Etomidate drug information Dose (IV) Onset of Action
(seconds) Duration of Action
(minutes) Advantages Disadvantages
0.3 mg/kg 5-15 5-15 Minimal
respiratory & CV effects; ↓ ICP
Adrenal suppression
XIII. Previously, etomidate was the “gold standard” for RSI in pediatrics54,55 A. Hemodynamically neutral B. Neuro-protective
XIV. Consistently, most significant concern is adrenocortical suppression 50-53 XV. American Academy of Pediatrics Resuscitation Guidelines56 state “etomidate should not be routinely
used when intubating an infant or child with septic shock” A. In support of their recommendation, the guidelines cite two studies57-58
Table 6: Trial summaries for etomidate use in septic shock patients Post hoc analysis of CORTICUS (2008): Hydrocortisone therapy in adults with septic shock57
n Population Results Author Conclusion
499
• 96 adult patients received etomidate
• 403 adult patients did not receive etomidate
Mortality at 28 days: • Etomidate group—42.7% • Non-etomidate group—30.5%
Increased risk of mortality in patients
who receive etomidate for induction
The Debate Behind Etomidate
Robinson
10
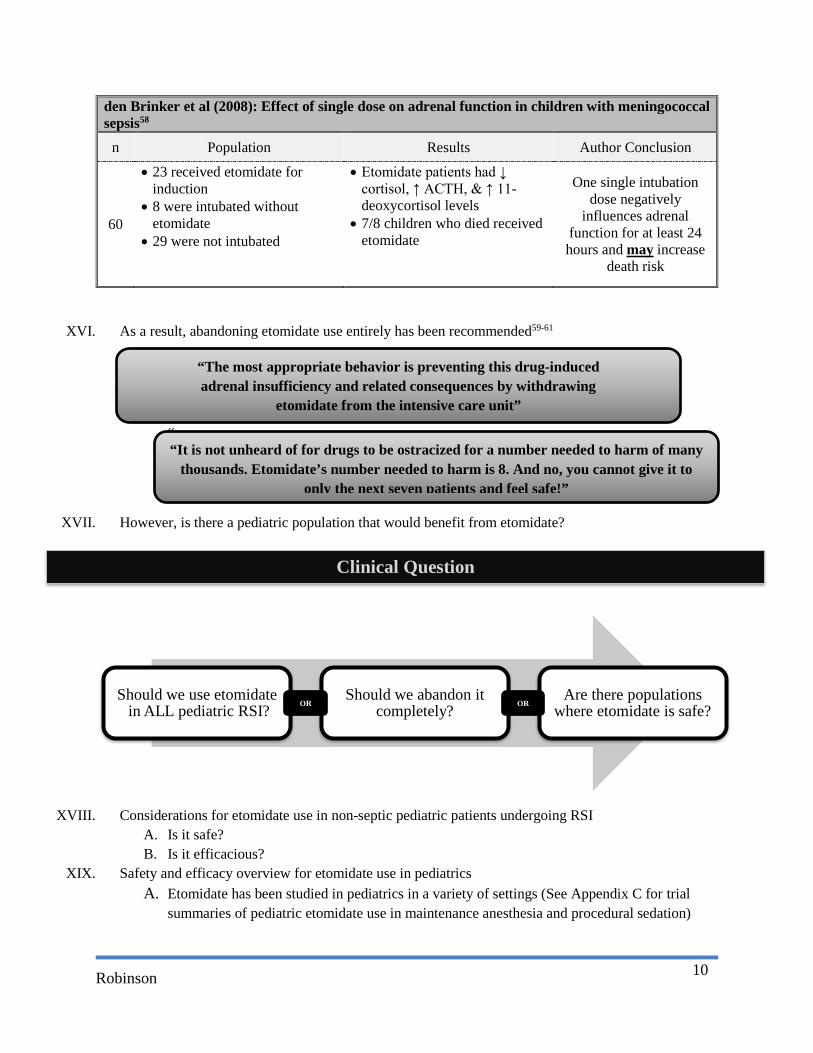
den Brinker et al (2008): Effect of single dose on adrenal function in children with meningococcal sepsis58
n Population Results Author Conclusion
60
• 23 received etomidate for induction
• 8 were intubated without etomidate
• 29 were not intubated
• Etomidate patients had ↓ cortisol, ↑ ACTH, & ↑ 11-deoxycortisol levels
• 7/8 children who died received etomidate
One single intubation dose negatively
influences adrenal function for at least 24 hours and may increase
death risk
XVI. As a result, abandoning etomidate use entirely has been recommended59-61
“
XVII. However, is there a pediatric population that would benefit from etomidate?
XVIII. Considerations for etomidate use in non-septic pediatric patients undergoing RSI A. Is it safe? B. Is it efficacious?
XIX. Safety and efficacy overview for etomidate use in pediatrics A. Etomidate has been studied in pediatrics in a variety of settings (See Appendix C for trial
summaries of pediatric etomidate use in maintenance anesthesia and procedural sedation)
Should we use etomidatein ALL pediatric RSI?
Should we abandon it completely?
Are there populations where etomidate is safe?
“The most appropriate behavior is preventing this drug-induced adrenal insufficiency and related consequences by withdrawing
etomidate from the intensive care unit”
“It is not unheard of for drugs to be ostracized for a number needed to harm of many thousands. Etomidate’s number needed to harm is 8. And no, you cannot give it to
only the next seven patients and feel safe!”
Clinical Question
OR OR
Robinson
11
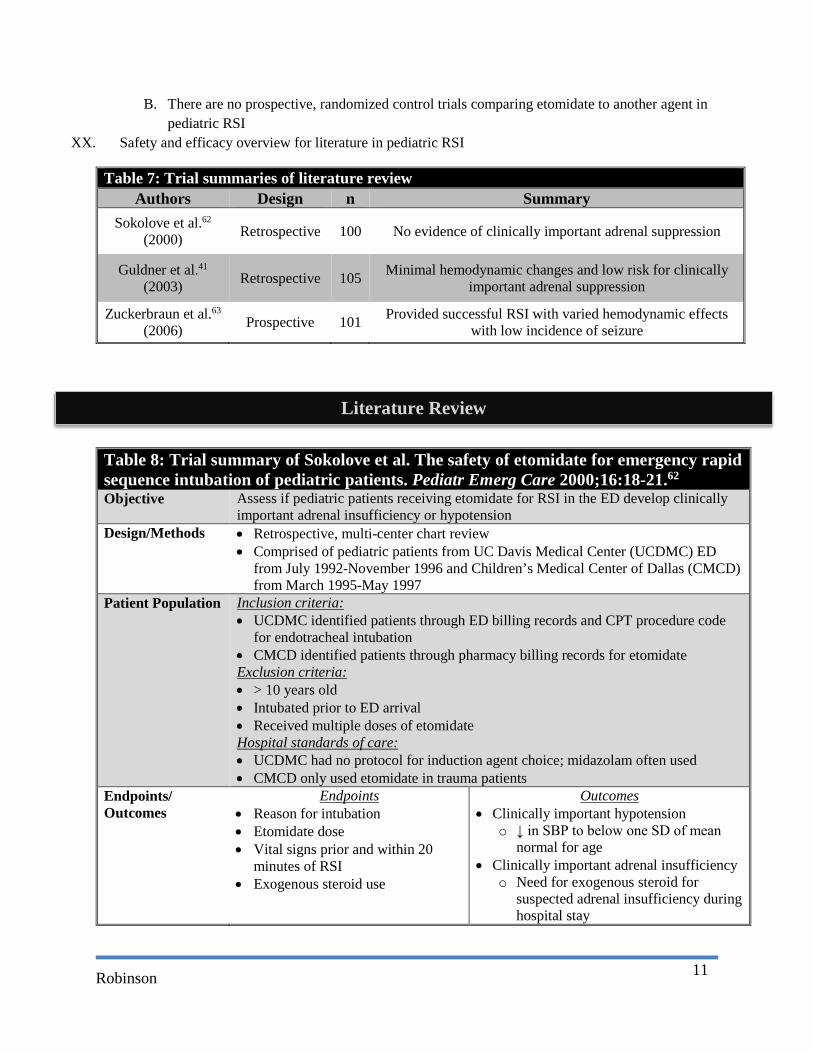
B. There are no prospective, randomized control trials comparing etomidate to another agent in pediatric RSI
XX. Safety and efficacy overview for literature in pediatric RSI
Table 7: Trial summaries of literature review Authors Design n Summary
Sokolove et al.62
(2000) Retrospective 100 No evidence of clinically important adrenal suppression
Guldner et al.41
(2003) Retrospective 105 Minimal hemodynamic changes and low risk for clinically important adrenal suppression
Zuckerbraun et al.63
(2006) Prospective 101 Provided successful RSI with varied hemodynamic effects with low incidence of seizure
Table 8: Trial summary of Sokolove et al. The safety of etomidate for emergency rapid sequence intubation of pediatric patients. Pediatr Emerg Care 2000;16:18-21.62 Objective Assess if pediatric patients receiving etomidate for RSI in the ED develop clinically
important adrenal insufficiency or hypotension Design/Methods • Retrospective, multi-center chart review
• Comprised of pediatric patients from UC Davis Medical Center (UCDMC) ED from July 1992-November 1996 and Children’s Medical Center of Dallas (CMCD) from March 1995-May 1997
Patient Population Inclusion criteria: • UCDMC identified patients through ED billing records and CPT procedure code
for endotracheal intubation • CMCD identified patients through pharmacy billing records for etomidate Exclusion criteria: • > 10 years old • Intubated prior to ED arrival • Received multiple doses of etomidate Hospital standards of care: • UCDMC had no protocol for induction agent choice; midazolam often used • CMCD only used etomidate in trauma patients
Endpoints/ Outcomes
Endpoints • Reason for intubation • Etomidate dose • Vital signs prior and within 20
minutes of RSI • Exogenous steroid use
Outcomes • Clinically important hypotension
o ↓ in SBP to below one SD of mean normal for age
• Clinically important adrenal insufficiency o Need for exogenous steroid for
suspected adrenal insufficiency during hospital stay
Literature Review

Robinson
12
Baseline Characteristics
• 100 patients (< 10 years) underwent RSI with etomidate o UCDMC [n]=56 o CMCD [n]=44
• 59% male • Mean age of 4.4 + 3.0 years (range 1 month-9.7 years)
Results • Intubation indication Trauma Status Epilepticus Pulmonary Other
72% 13% 10% 5% • Mean etomidate dose was 0.37 + 0.15 mg/kg (range 0.05-0.9 mg/kg) • BP measurements prior and within 20 minutes were recorded in 84 patients
o Mean change in BP was a decrease of 1 mmHg [95% CI -6 to +7 mmHg, p=0.83]
o Mean change as percentage of normal BP for age was a decrease of 1% [95% CI -7% to +6%, p=0.82]
o 4 patients exhibited decrease in BP to below one SD 1 due to blood loss, 1 had recurrent hypotension throughout
hospitalization, and 2 patients had transient hypotension • 14/100 patients (14%) received steroids during hospitalization but none were for
suspected adrenal insufficiency Author’s Conclusion
• One time etomidate doses do not result in clinically important adrenal suppression with a low incidence of clinically important hypotension
• Prospective comparison studies are needed to further evaluate etomidate safety in the pediatric population
Strengths • Pediatric population • Sufficient etomidate dose • Low missing data rate
Critique • Descriptive study (no comparator group) • Indirect adrenal function measure • Did not report intubation success
Take away • Trauma was primary indication for intubation • Hemodynamically neutral in pediatric population • No evidence of clinically significant adrenal insufficiency • Intubation success not addressed
Table 9: Trial summary of Guldner et al. Etomidate for rapid-sequence intubation in young children: Hemodynamic effects and adverse events. Acad Emerg Med 2003;10:134-39.41 Objective Evaluate frequency of immediate adverse effects (vomiting, seizures, myoclonus),
hemodynamic effects, and delayed adverse events (adrenal suppression and persistent seizures)
Design/Methods • Retrospective, single-center chart review • Included patients from a university tertiary care, level 1 trauma center, hospital ED
between July 1996-April 2001 Patient Population Inclusion criteria:
• Identified patients through pharmacy logs and hospital billing records
Robinson
13
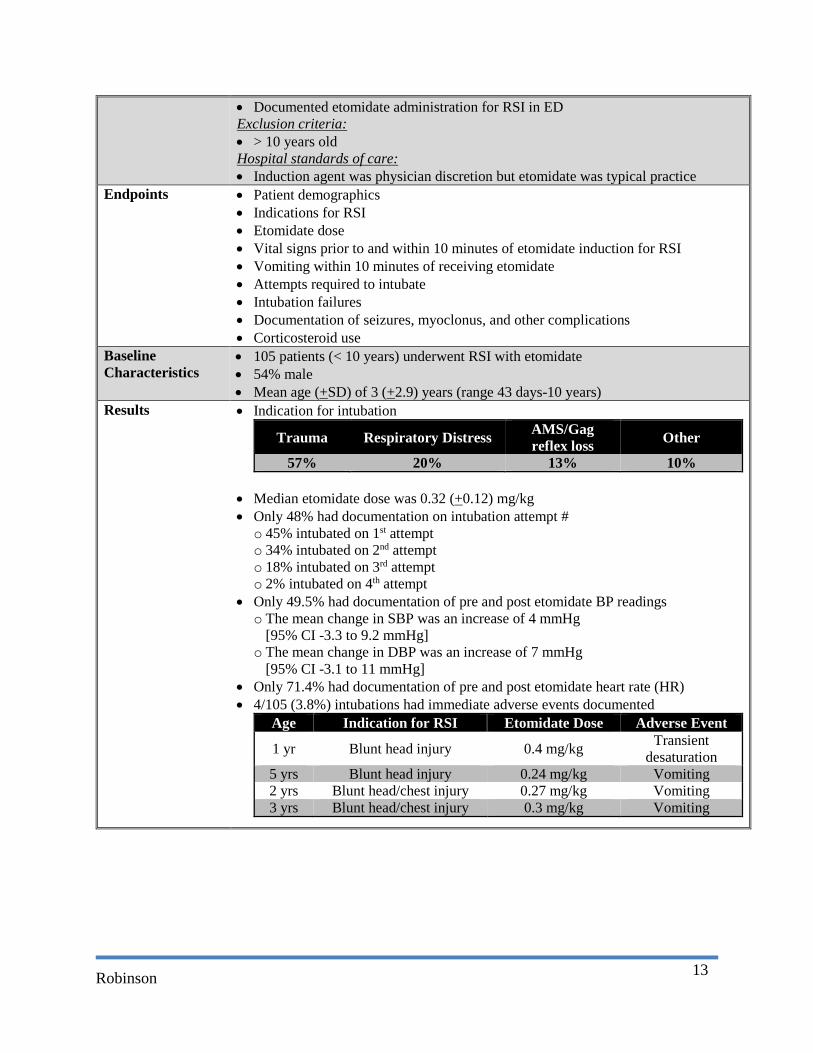
• Documented etomidate administration for RSI in ED Exclusion criteria: • > 10 years old Hospital standards of care: • Induction agent was physician discretion but etomidate was typical practice
Endpoints • Patient demographics • Indications for RSI • Etomidate dose • Vital signs prior to and within 10 minutes of etomidate induction for RSI • Vomiting within 10 minutes of receiving etomidate • Attempts required to intubate • Intubation failures • Documentation of seizures, myoclonus, and other complications • Corticosteroid use
Baseline Characteristics
• 105 patients (< 10 years) underwent RSI with etomidate • 54% male • Mean age (+SD) of 3 (+2.9) years (range 43 days-10 years)
Results • Indication for intubation
Trauma Respiratory Distress AMS/Gag reflex loss Other
57% 20% 13% 10% • Median etomidate dose was 0.32 (+0.12) mg/kg • Only 48% had documentation on intubation attempt # o 45% intubated on 1st attempt o 34% intubated on 2nd attempt o 18% intubated on 3rd attempt o 2% intubated on 4th attempt
• Only 49.5% had documentation of pre and post etomidate BP readings o The mean change in SBP was an increase of 4 mmHg
[95% CI -3.3 to 9.2 mmHg] o The mean change in DBP was an increase of 7 mmHg
[95% CI -3.1 to 11 mmHg] • Only 71.4% had documentation of pre and post etomidate heart rate (HR) • 4/105 (3.8%) intubations had immediate adverse events documented
Age Indication for RSI Etomidate Dose Adverse Event
1 yr Blunt head injury 0.4 mg/kg Transient desaturation
5 yrs Blunt head injury 0.24 mg/kg Vomiting 2 yrs Blunt head/chest injury 0.27 mg/kg Vomiting 3 yrs Blunt head/chest injury 0.3 mg/kg Vomiting
Robinson
14
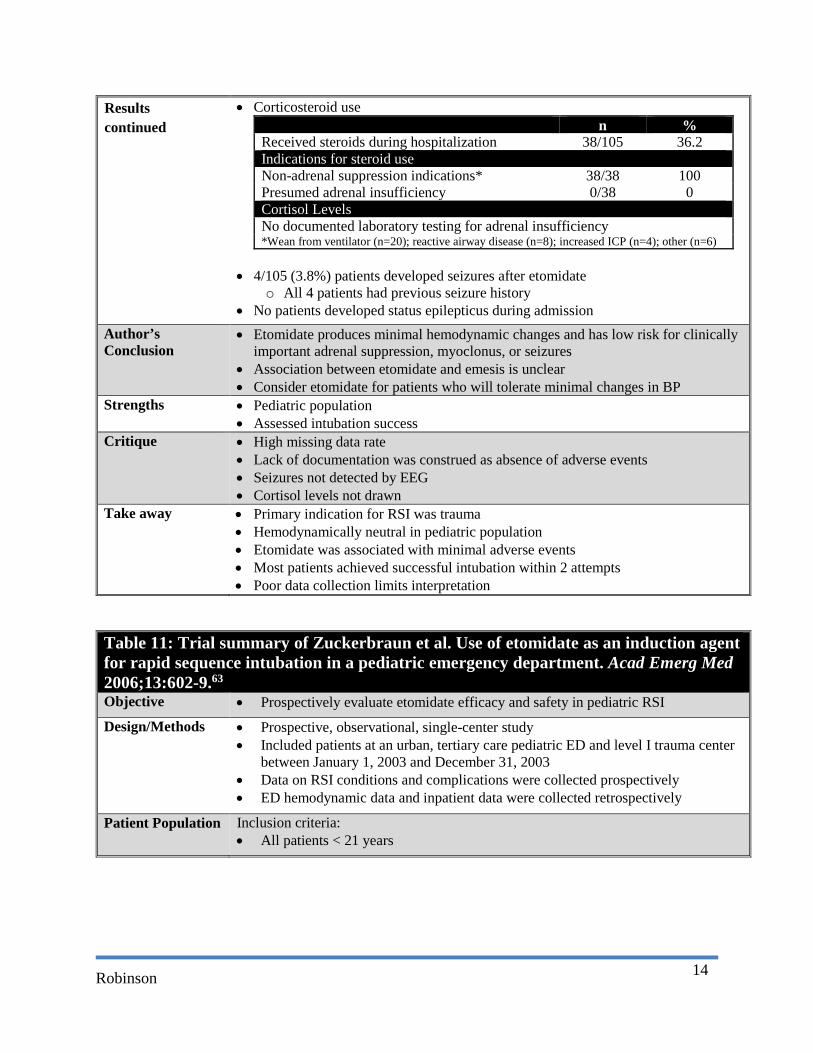
• Corticosteroid use n %
Received steroids during hospitalization 38/105 36.2 Indications for steroid use Non-adrenal suppression indications* 38/38 100 Presumed adrenal insufficiency 0/38 0 Cortisol Levels No documented laboratory testing for adrenal insufficiency *Wean from ventilator (n=20); reactive airway disease (n=8); increased ICP (n=4); other (n=6)
• 4/105 (3.8%) patients developed seizures after etomidate
o All 4 patients had previous seizure history • No patients developed status epilepticus during admission
Author’s Conclusion
• Etomidate produces minimal hemodynamic changes and has low risk for clinically important adrenal suppression, myoclonus, or seizures
• Association between etomidate and emesis is unclear • Consider etomidate for patients who will tolerate minimal changes in BP
Strengths • Pediatric population • Assessed intubation success
Critique • High missing data rate • Lack of documentation was construed as absence of adverse events • Seizures not detected by EEG • Cortisol levels not drawn
Take away • Primary indication for RSI was trauma • Hemodynamically neutral in pediatric population • Etomidate was associated with minimal adverse events • Most patients achieved successful intubation within 2 attempts • Poor data collection limits interpretation
Table 11: Trial summary of Zuckerbraun et al. Use of etomidate as an induction agent for rapid sequence intubation in a pediatric emergency department. Acad Emerg Med 2006;13:602-9.63
Objective • Prospectively evaluate etomidate efficacy and safety in pediatric RSI
Design/Methods • Prospective, observational, single-center study • Included patients at an urban, tertiary care pediatric ED and level I trauma center
between January 1, 2003 and December 31, 2003 • Data on RSI conditions and complications were collected prospectively • ED hemodynamic data and inpatient data were collected retrospectively
Patient Population Inclusion criteria: • All patients < 21 years
Results continued
Robinson
15
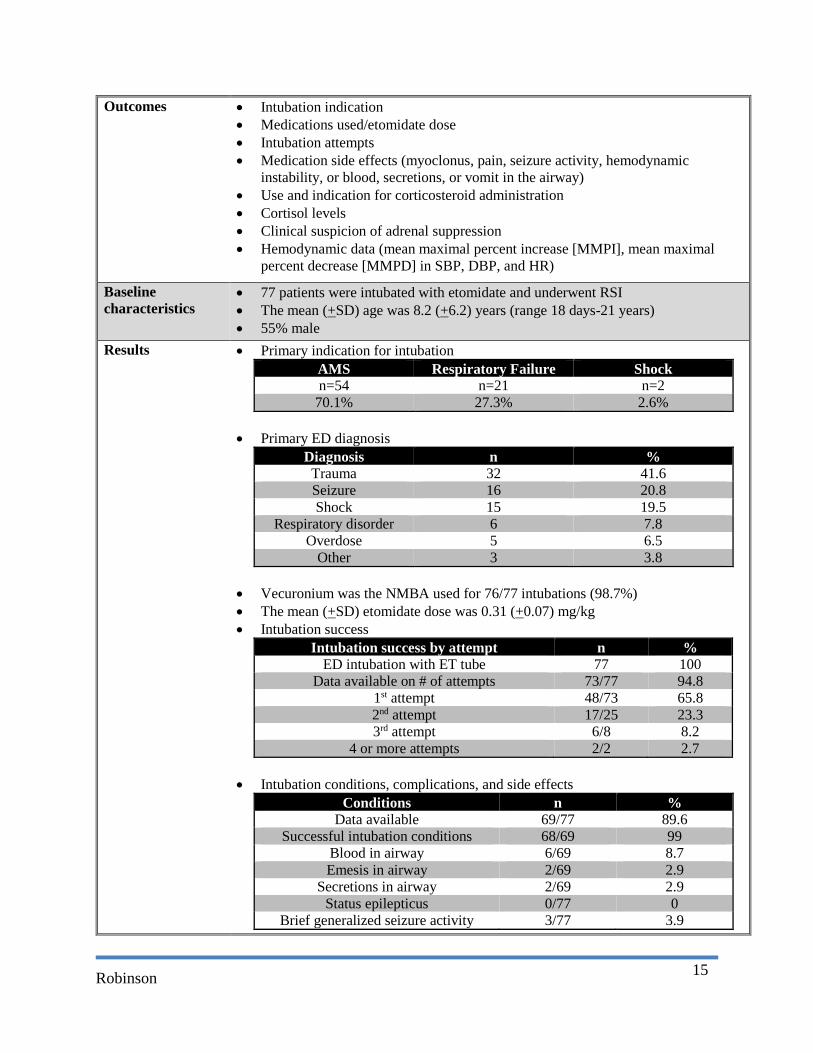
Outcomes • Intubation indication • Medications used/etomidate dose • Intubation attempts • Medication side effects (myoclonus, pain, seizure activity, hemodynamic
instability, or blood, secretions, or vomit in the airway) • Use and indication for corticosteroid administration • Cortisol levels • Clinical suspicion of adrenal suppression • Hemodynamic data (mean maximal percent increase [MMPI], mean maximal
percent decrease [MMPD] in SBP, DBP, and HR)
Baseline characteristics
• 77 patients were intubated with etomidate and underwent RSI • The mean (+SD) age was 8.2 (+6.2) years (range 18 days-21 years) • 55% male
Results • Primary indication for intubation AMS Respiratory Failure Shock n=54 n=21 n=2
70.1% 27.3% 2.6% • Primary ED diagnosis
Diagnosis n % Trauma 32 41.6 Seizure 16 20.8 Shock 15 19.5
Respiratory disorder 6 7.8 Overdose 5 6.5
Other 3 3.8 • Vecuronium was the NMBA used for 76/77 intubations (98.7%) • The mean (+SD) etomidate dose was 0.31 (+0.07) mg/kg • Intubation success
Intubation success by attempt n % ED intubation with ET tube 77 100
Data available on # of attempts 73/77 94.8 1st attempt 48/73 65.8 2nd attempt 17/25 23.3 3rd attempt 6/8 8.2
4 or more attempts 2/2 2.7 • Intubation conditions, complications, and side effects
Conditions n % Data available 69/77 89.6
Successful intubation conditions 68/69 99 Blood in airway 6/69 8.7 Emesis in airway 2/69 2.9
Secretions in airway 2/69 2.9 Status epilepticus 0/77 0
Brief generalized seizure activity 3/77 3.9

Robinson
16
• data n %
MMPD in SBP > 20% 12/69 17.4 SBP ↓ meeting PALS hypotension definition 7/12 10.1
PALS hypotension requiring intervention* 2/7 2.9 MMPI in SBP > 20% 26/69 38
MMPD in DBP > 20% 13/68 19 MMPI in DBP > 20% 32/68 47 MMPI in HR > 20% 30/73 41 MMPD in HR > 20% 14/73 19
*Hemorrhagic shock requiring blood; septic shock requiring fluids & vasopressors
• Hemodynamics in decompensated shock vs. non-shock at intubation
o Decompensated shock had lower MMPD in SBP compared to non-shock patients (2.5% vs. 11%)
o Decompensated shock had higher MMPI in SBP compared to non-shock patients (68.3% vs. 16.4%)
• Corticosteroid use n %
Received steroids during hospitalization 29/77 37.6 Indications for steroid use Non-adrenal suppression indications* 21/29 72.4 Presumed adrenal insufficiency 8/29 27.6 Cortisol Levels Normal random cortisol levels 1/8 12.5 Low random cortisol levels 7/8 87.5 *Stridor (n=9); asthma (n=4); baseline medication (n=4); other (n=4)
Author’s Conclusion
• Etomidate provided successful RSI conditions • Hypotension and seizures were uncommon and occurred in patients with
confounding diagnoses • Use with caution in patients with adrenal insufficiency
Strengths • Pediatric population • Assessed safety and efficacy of etomidate use • Low missing data rate
Critique • Descriptive study (no comparison group) • Cortisol level timing was inconsistent • Single-center study design • Shock etiology not reported
Take away • Primary indication for RSI was trauma • Etomidate use is likely safe in other populations • Difficult to draw conclusions on etomidate in septic shock patients based on
results in this trial
Conclusion & Recommendation
Results continued
Robinson
17
XXI. Summary A. The most common indication for RSI in our studies was trauma41.62.63 B. The recommendation to avoid etomidate use in septic shock pediatric patients is based on the
outcome in 23 pediatric patients56 C. Single dose etomidate safety has been shown in non-shock pediatric populations41,62-63,66-70
XXII. Unanswered questions A. Is etomidate safe in patients with septic shock? B. Should steroids be administered to patients at risk for adrenal insufficiency who receive
etomidate? XXIII. Future study and developments
A. Randomized controlled trial would improve strength of recommendation B. Carboetomidate may offer a hemodynamically neutral induction agent without adrenal
insufficiency65 1. Synthetic version of etomidate designed to avoid adrenal dysfunction 2. Studies indicate it provides adequate sedation with minimal inhibition of 11β-
hydroxylase 3. Not available on market
XXIV. Recommendations A. Consider etomidate in pediatric population in RSI for trauma
1. Trauma patients comprised largest population in pediatric safety and efficacy trials 2. Etomidate was hemodynamically neutral with low seizure and adrenal insufficiency
incidence B. Consider etomidate in pediatric medicine patients undergoing RSI
1. Medicine patients comprised reasonable portion of Guldner and Zuckerbraun studies 2. They displayed similar hemodynamic response if they did not present in shock 3. If unable to rule out septic shock from clinical presentation/story, select alternative
agent C. Select another induction agent for RSI in children with:
1. Septic shock a. Direct causal effect between etomidate and poor outcomes has not been
definitively proven b. However, it is wise to avoid adrenal suppression in patients unable to mount
their own physiological stress response 2. Risk for adrenal insufficiency
a. Chronic steroid use/abrupt withdrawal b. Genetic conditions (Congenital adrenal hyperplasia is most common) c. Infection (septic shock)
D. Administer 0.3 mg/kg IV for adequate sedation
Appendix A
Robinson
18
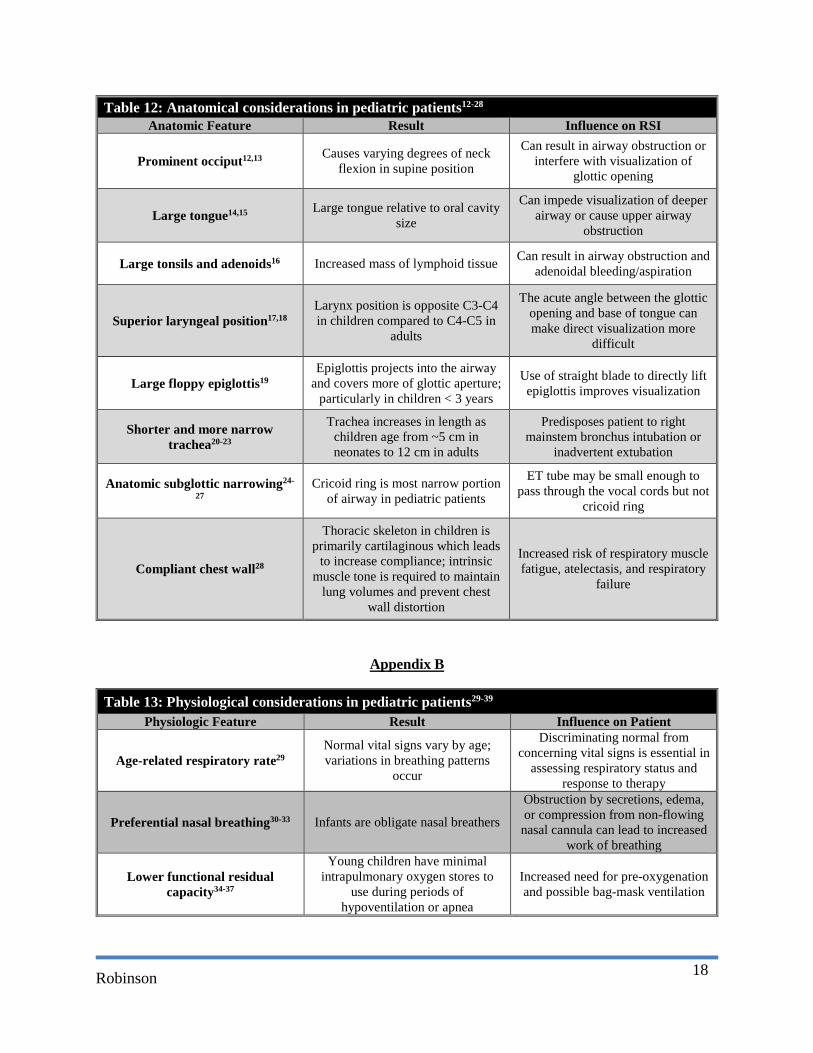
Table 12: Anatomical considerations in pediatric patients12-28
Anatomic Feature Result Influence on RSI
Prominent occiput12,13 Causes varying degrees of neck flexion in supine position
Can result in airway obstruction or interfere with visualization of
glottic opening
Large tongue14,15 Large tongue relative to oral cavity size
Can impede visualization of deeper airway or cause upper airway
obstruction
Large tonsils and adenoids16 Increased mass of lymphoid tissue Can result in airway obstruction and adenoidal bleeding/aspiration
Superior laryngeal position17,18 Larynx position is opposite C3-C4 in children compared to C4-C5 in
adults
The acute angle between the glottic opening and base of tongue can make direct visualization more
difficult
Large floppy epiglottis19 Epiglottis projects into the airway
and covers more of glottic aperture; particularly in children < 3 years
Use of straight blade to directly lift epiglottis improves visualization
Shorter and more narrow trachea20-23
Trachea increases in length as children age from ~5 cm in neonates to 12 cm in adults
Predisposes patient to right mainstem bronchus intubation or
inadvertent extubation
Anatomic subglottic narrowing24-
27 Cricoid ring is most narrow portion
of airway in pediatric patients
ET tube may be small enough to pass through the vocal cords but not
cricoid ring
Compliant chest wall28
Thoracic skeleton in children is primarily cartilaginous which leads
to increase compliance; intrinsic muscle tone is required to maintain
lung volumes and prevent chest wall distortion
Increased risk of respiratory muscle fatigue, atelectasis, and respiratory
failure
Appendix B
Table 13: Physiological considerations in pediatric patients29-39 Physiologic Feature Result Influence on Patient
Age-related respiratory rate29 Normal vital signs vary by age; variations in breathing patterns
occur
Discriminating normal from concerning vital signs is essential in
assessing respiratory status and response to therapy
Preferential nasal breathing30-33 Infants are obligate nasal breathers
Obstruction by secretions, edema, or compression from non-flowing
nasal cannula can lead to increased work of breathing
Lower functional residual capacity34-37
Young children have minimal intrapulmonary oxygen stores to
use during periods of hypoventilation or apnea
Increased need for pre-oxygenation and possible bag-mask ventilation
Robinson
19
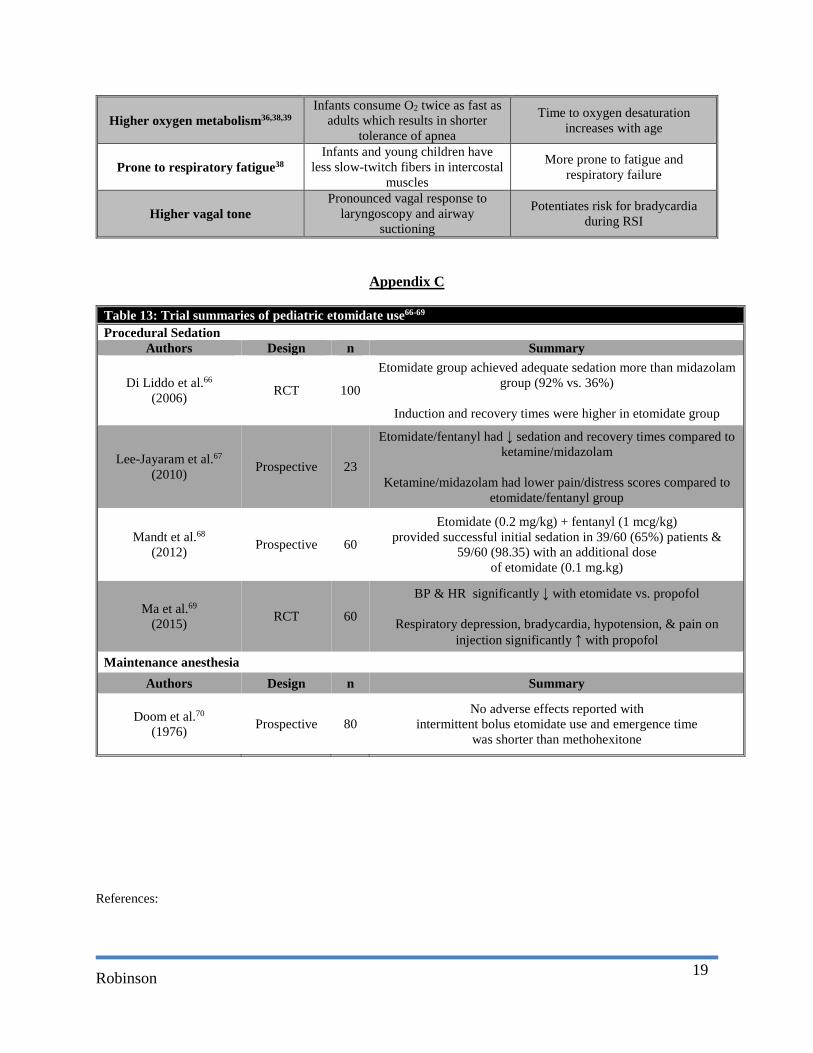
Higher oxygen metabolism36,38,39 Infants consume O2 twice as fast as
adults which results in shorter tolerance of apnea
Time to oxygen desaturation increases with age
Prone to respiratory fatigue38 Infants and young children have
less slow-twitch fibers in intercostal muscles
More prone to fatigue and respiratory failure
Higher vagal tone Pronounced vagal response to
laryngoscopy and airway suctioning
Potentiates risk for bradycardia during RSI
Appendix C
Table 13: Trial summaries of pediatric etomidate use66-69
Procedural Sedation Authors Design n Summary
Di Liddo et al.66
(2006) RCT 100
Etomidate group achieved adequate sedation more than midazolam group (92% vs. 36%)
Induction and recovery times were higher in etomidate group
Lee-Jayaram et al.67
(2010) Prospective 23
Etomidate/fentanyl had ↓ sedation and recovery times compared to ketamine/midazolam
Ketamine/midazolam had lower pain/distress scores compared to
etomidate/fentanyl group
Mandt et al.68
(2012) Prospective 60
Etomidate (0.2 mg/kg) + fentanyl (1 mcg/kg) provided successful initial sedation in 39/60 (65%) patients &
59/60 (98.35) with an additional dose of etomidate (0.1 mg.kg)
Ma et al.69
(2015) RCT 60
BP & HR significantly ↓ with etomidate vs. propofol
Respiratory depression, bradycardia, hypotension, & pain on injection significantly ↑ with propofol
Maintenance anesthesia Authors Design n Summary
Doom et al.70
(1976) Prospective 80 No adverse effects reported with
intermittent bolus etomidate use and emergence time was shorter than methohexitone
References:

Robinson
20
1. Gerardi MJ, Sacchetti AD, Cantor RM, et al. Rapid sequence intubation of the pediatric patient. Ann Emerg Med 1996; 28:55-74.
2. Mason MA, Weant KA, Baker SN. Rapid sequence intubation medication therapies: A review in light of recent drug shortages. Adv Emerg Nurs J 2013; 35(1):16-25.
3. Stollings JL, Diedrich DA, Oyen LJ, Brown DR. Rapid-sequence intubation: A review of the process and considerations when choosing medications. Ann Pharmacother 2014; 48(1):62-76.
4. Sagarin MJ, Chiang V, Sakles JC, et al. Rapid sequence intubation for pediatric emergency airway management. Pediatr Emerg Care 2002; 18:417-23.
5. Gentleman D, Dearden M, Midgley S, Maclean D. Guidelines for resuscitation and transfer of patients with serious head injury. BMJ 1993; 307:547-52.
6. Gabriel EJ, Ghajar J, Jagoda A, et al. Guidelines for prehospital management of traumatic brain injury. J Neurotrauma 2002; 19:111-74.
7. Adnet F, Baud F. Relation between Glasgow Coma Scale and aspiration pneumonia. Lancet 1996; 348:123-4.
8. Huxley EJ, Viroslav J, Gray WR, Pierce AK. Pharyngeal aspiration in normal adults and patients with depressed consciousness. Am J Med 1978; 64:564-8.
9. Broussard DL, Altschuler SM. Central integration of swallow and airway-protective reflexes. Am J Med 2000; 108 Suppl 4a:62S-67S.
10. Moulton C, Pennycook A, Makower R. Relation between Glasgow coma scale and the gag reflex. BMJ 1991; 303:1240-1.
11. Davies AE, Kidd D, Stone SP, MacMahon J. Pharyngeal sensation and gag reflex in healthy subjects. Lancet 1995; 345:487-8.
12. Todres ID. Pediatric airway control and ventilation. Ann Emerg Med 1993; 22:440-4. 13. Goetting MG. Mastering pediatric cardiopulmonary resuscitation. Pediatr Clin North Am 1994; 41:114-82. 14. Don GW, Kirjavainen T, Broome C, et al. Site and mechanics of spontaneous, sleep-associated obstructive
apnea in infants. J Appl Physiol 2000; 89:2453-62. 15. Eastwood PR, Szollosi I, Platt PR, Hillman DR. Collapsibility of the upper airway during anesthesia with
isoflurane. Anesthesiology 2002; 97:786-93. 16. Arens R, McDonough JM, Costarino AT, et al. Magnetic resonance imaging of the upper airway structure
of children with obstructive sleep apnea syndrome. Am J Respir Crit Care Med 2001; 164:698-703. 17. Westhorpe RN. The position of the larynx in children and its relationship to the ease of intubation. Anaesth
Intensive Care 1987; 15:384-8. 18. Schwartz DS, Keller MS. Maturational descent of the epiglottis. Arch Otolaryngol Head Neck Surg 1997;
123:627-8. 19. John SD, Swischuk LE. Stridor and upper airway obstruction in infants and children. Radiographics 1992;
12:625-43. 20. Fearon B, Whalen JS. Tracheal dimensions in the living infant (preliminary report). Ann Otol Rhinol
Laryngol 1967; 76:965-74. 21. Griscom NT, Wohl ME. Dimensions of the growing trachea related to age and gender. AJR Am J
Roentgenol 1986; 146:233-7. 22. Miller KA, Kimia A, Monuteaux MC, Nagler J. Factors Associated with Misplaced Endotracheal Tubes
During Intubation in Pediatric Patients. J Emerg Med 2016; 51:9-18. 23. Weiss M, Knirsch W, Kretschmar O, et al. Tracheal tube-tip displacement in children during head-neck
movement--a radiological assessment. Br J Anaesth 2006; 96:486-91. 24. Eckenhoff JE. Some anatomic considerations of the infant larynx influencing endotracheal anesthesia.
Anesthesiology 1951; 12:401-10. 25. Litman RS, Weissend EE, Shibata D, Westesson PL. Developmental changes of laryngeal dimensions in
unparalyzed, sedated children. Anesthesiology 2003; 98:41-5. 26. Dalal PG, Murray D, Messner AH, et al. Pediatric laryngeal dimensions: an age-based analysis. Anesth
Analg 2009; 108:1475-9. 27. Kleinman ME, Chameides L, Schexnayder SM, et al. Part 14: pediatric advanced life support: 2010
American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010; 122:S876-S908.

Robinson
21
28. Papastamelos C, Panitch HB, England SE, Allen JL. Developmental changes in chest wall compliance in infancy and early childhood. J Appl Physiol 1995; 78:179-84.
29. Kelly DH, Stellwagen LM, Kaitz E, Shannon DC. Apnea and periodic breathing in normal full-term infants during the first twelve months. Pediatr Pulmonol 1985; 1:215-9.
30. Swift PG, Emery JL. Clinical observations on response to nasal occlusion in infancy. Arch Dis Child 1973; 48:947-51.
31. Miller MJ, Martin RJ, Carlo WA, et al. Oral breathing in newborn infants. J Pediatr 1985; 107:465-9. 32. Rodenstein DO, Perlmutter N, Stănescu DC. Infants are not obligatory nasal breathers. Am Rev Respir Dis
1985; 131:343-7. 33. Stocks J, Godfrey S. Nasal resistance during infancy. Respir Physiol 1978; 34:233-46. 34. Gerhardt T, Reifenberg L, Hehre D, et al. Functional residual capacity in normal neonates and children up
to 5 years of age determined by a N2 washout method. Pediatr Res 1986; 20:668-71. 35. Stocks J, Quanjer PH. Reference values for residual volume, functional residual capacity and total lung
capacity. ATS Workshop on Lung Volume Measurements. Official Statement of The European Respiratory Society. Eur Respir J 1995; 8:492-506.
36. Patel R, Lenczyk M, Hannallah RS, McGill WA. Age and the onset of desaturation in apnoeic children. Can J Anaesth 1994; 41:771-4.
37. Rinderknecht AS, Mittiga MR, Meinzen-Derr J, et al. Factors associated with oxyhemoglobin desaturation during rapid sequence intubation in a pediatric emergency department: findings from multivariable analyses of video review data. Acad Emerg Med 2015; 22:431-40.
38. Keens TG, Bryan AC, Levison H, Ianuzzo CD. Developmental pattern of muscle fiber types in human ventilatory muscles. J Appl Physiol Respir Environ Exerc Physiol 1978; 44:909-13.
39. Sagarin MJ, Barton ED, Chng YM, et al. Airway management by US and Canadian emergency medicine residents: a multicenter analysis of more than 6,000 endotracheal intubation attempts. Ann Emerg Med 2005; 46:328-36.
40. Scherzer D, Leder M, Tobias JD. Pro-con debate: Etomidate or ketamine for rapid sequence intubation in pediatric patients. J Pediatr Pharmacol Ther 2012; 17(2):142-9.
41. Guldner G, Schultz J, Sexton P, Fortner C, Richmond M. Etomidate for rapid-sequence intubation in young children: Hemodynamic effects and adverse events. Acad Emerg Med 2003; 10:134-9.
42. Ching KY, Baun CR. Newer agents for rapid sequence intubatiob. Pediatr Emer Care 2009; 25:200-10. 43. Jackson W. Should we use etomidate as an induction agent for endotracheal intubation in patients with
septic shock? A critical appraisal. CHEST 2005; 127:1031-8. 44. Ledingham I, Watt I. Influence of sedation on mortality in critically ill multiple trauma patients [letter].
Lancet 1983; 1:1270. 45. Edbrooke DL, Newby DM Mather SJ et al. Safer sedation for ventilated patients: a new application for
etomidate. Anaesthesia 1982; 37:765-71. 46. Zed RJ, Mabasa VH, Slavik RS et al. Etomidate for rapid sequence intubation in the emergency
department: is adrenal suppression a concern? Can J Emerg Med 2006; 8:347-50. 47. Watt I, Ledingham, I et al. Mortality amongst multiple trauma patients admitted to an intensive therapy
unit. Anaesthesia 1984; 39:973-81. 48. de Jong H, Mallios C, Jansen C et al. Etomidate suppresses adrenal function by inhibition of 11-β
hydroxylation. J Clin Endocr Metab 1984; 60:1143-7. 49. Bramwell KJ, Haizlip J, Pribble C, VanderHeyden TC, Witte M. The effect of etomidate on intracranial
pressure and systemic blood pressure in pediatric patients with severe traumatic brain injury. Pediatr Emerg Care 22(2):90-3.
50. Duthie DJ, Fraser R, Nimmo WS. Effect of induction of anesthesia with etomidate on corticosteroid synthesis in man. Br J Anesth 1985; 57:156-9.
51. Absolam A, Pledger D, Kong A. Adrenocortical function in critically ill patients 24 h after a single dose of etomidate. Anesthesia 1999; 54:861-7.
52. Donmez A, Kaya H, Haberal A, Kutsal A, Arslan G. The effect of etomidate induction on plasma cortisol levels in children undergoing cardiac surgery. J Cardiothorac Vasc Anesth 1998; 12:182-5.
Robinson
22
53. Vinclair M, Broux C, Faure P, et al. Duration of adrenal inhibition following a single dose of etomidate in critically ill patients. Intensive Care Med 2008; 34:714-9.
54. Tobias JD. Etomidate in pediatric anesthesiology: Where are we now? Saudi J Anaesth 2015; 9(4):451-6. 55. Zelicof-Paul A, Smith-Lockridge A, Schnadower D, et al. Controversies in rapid sequence intubation in
children. Curr Opin Pediatr 2005; 17:355-62. 56. Janeczek M, Rice C, Aitchison R, Aithcison P, Wang E, Kharasch M. Pediatric resuscitation guidelines.
Disease-a-Month 2013; 59: 182-95. 57. Sprung CL, Annane D, Keh D, et al. Hydrocortisone therapy for patients with septic shock. New Engl J
Med 2008; 358(2): 111-24. 58. den Brinker M, Hokken-Koelega ACS, Hazelzet JA, De Jong FH, Hop WCJ, Joosten KFM. One single
dose of etomidate negatively influences adrenocortical performance for at least 24h in children with meningococcal sepsis. Intensive Care Med 2008; 34:163-8.
59. Annane D. ICU physicians should abandon the use of etomidate! Intensive Care Med 2005; 31:325-6. 60. Markovitz BP. The drug that would not die (though patients receiving it do). Pediatr Crit Care Med 2009;
10(3): 418-9. 61. Cotton BA, Guillamondegui OD, Fleming SB, et al. Increased risk of adrenal insufficiency following
etomidate exposure in critically injured patients. Arch Surg 2008; 143:62-7. 62. Sokolove PE, Price DD, Okada P. The safety of etomidate for emergency rapid sequence intubation of
pediatric patients. Pediatr Emerg Care 2000; 15(1):18-21. 63. Zuckerbraun NS, Pitetti RD, Herr SM, Roth KR, Gaines BA, King C. Use of etomidate as an induction
agent for rapid sequence intubation in a pediatric emergency department. Acad Emerg Med 2006; 13:602-9. 64. Sarkar M, Laussen PC, Zurakowski D, Shukla A, Kussman B, Odegard KC. Hemodynamic responses to
etomidate on induction of anesthesia in pediatric patients. Anesth Analg 2005; 101:645-50. 65. Cotton JF, Forman SA, Laha JK. Carboetimidate: A pyrrole analog of etomidate designed not to suppress
adrenocortical function. Anesthesiology 2010; 112:637-44. 66. Di Liddo L, D’Angelo A, Nguyen B, Bailey B, Amre D, Stanciu C. Etomidate versus midazolam for
procedural sedation in pediatric outpatients: a randomized controlled trial. Ann Emerg Med 2006: 48:433-40.
67. Lee-Jayaram JJ, Green A, Siembieda J, et al. Ketamine/midazolam versus etomidate/fentanyl: Procedural sedation for pediatric orthopedic reductions. Pediatr Emerg Care 2010; 26:408-12.
68. Mandt MJ, Roback MG, Bajaj L, Galinkin JL, Gao D, Wathen JE. Etomidate for short pediatric procedures in the emergency department. Pediatr Emerg Care 2012; 28:898-904.
69. Ma YH, Li YW, Ma L, Cao CH, Liu XD. Anesthesia for stem cell transplantation in autistic children: A prospective, randomized, double-blind comparison of propofol and etomidate following sevoflurane inhalation. Exp Ther Med 2015; 9:1035-9.
70. Doom A, Mundeleer P. Etomidate and tonsillectomy. Acta Anesthesiol Belg 1976; 27:181-6.