quality-based procedures - healthachieve 2014/health information... · quality-based procedures...
TRANSCRIPT
Quality-Based ProceduresCoding and Documentation
November 3, 2014
Michael StewartDirector, Quality-Based ProceduresMinistry of Health and Long-Term Care

Better quality and more affordable healthcare for future generations of Ontarians is both possible and achievable. A strong focus on these four pillars and the triple aim will inform our collective work.
2
Our Path Going Forward
Health System Funding Reform (HSFR) Goals and Objectives
Reflect needs of the community
Equitable allocation of health care dollars
Better quality care and improved outcomes
Moderate spending growth to sustainable level
Adopt/ learn from approaches used in other jurisdictions
Phased in over time at a managed pace
3

Global Funding
Move from the global provider-focused funding model to one that revolves around the person
Health System Funding Reform
Health Service Providers (e.g. Hospitals, CCACs)
4

Ontario’s Health System Funding Reform (HSFR) approach will draw from over 25 years of international Activity Based Funding experience
• Patient focused funding systems reimburse providers at an established rate, based upon quality care for standard patient groups
• Ontario is one of the last leading jurisdictions to move down this path
Pat
ient
Foc
used
Fun
ding
Ado
ptio
n Ti
mel
ine
5

HSFR has two funding components
• HBAM is a ‘made in Ontario' funding model that determines optimal amount of funding based on patient demographics, clinical data and financial data
• QBPs are clusters of patients with clinically related diagnoses/ treatments and functional needs identified by an evidence-based framework as providing opportunity for:
1. Aligning incentives to facilitate adoption of best clinical evidence-informed practices2. Appropriately reducing variation in costs and practice across the province while
improving outcomes3. Ensuring we are advancing right care, at the right place, at the right time
Note: At the culmination of HSFR, HSPs will account for approximately 70% of funding
HSFR
Health-Based Allocation Model
(HBAM)
Global Funding
(Non-HSFR)Quality-Based Procedures
(QBPs)
6
QBPs have been selected using an evidence-based framework…
7
The “Quality” in Quality-Based Procedures
• Best practices informed by clinical consensus and best available evidence
• Engage in clinical process improvement/ re-design and adopt best practices
• Best practice pricing to strengthen the linkage between quality and funding
• Develop indicators to evaluate and monitor actual practice
• Broaden scope of QBPs to strengthen the continuity of care
• Ensure every patient gets the right care, at the right place, at the right time
8
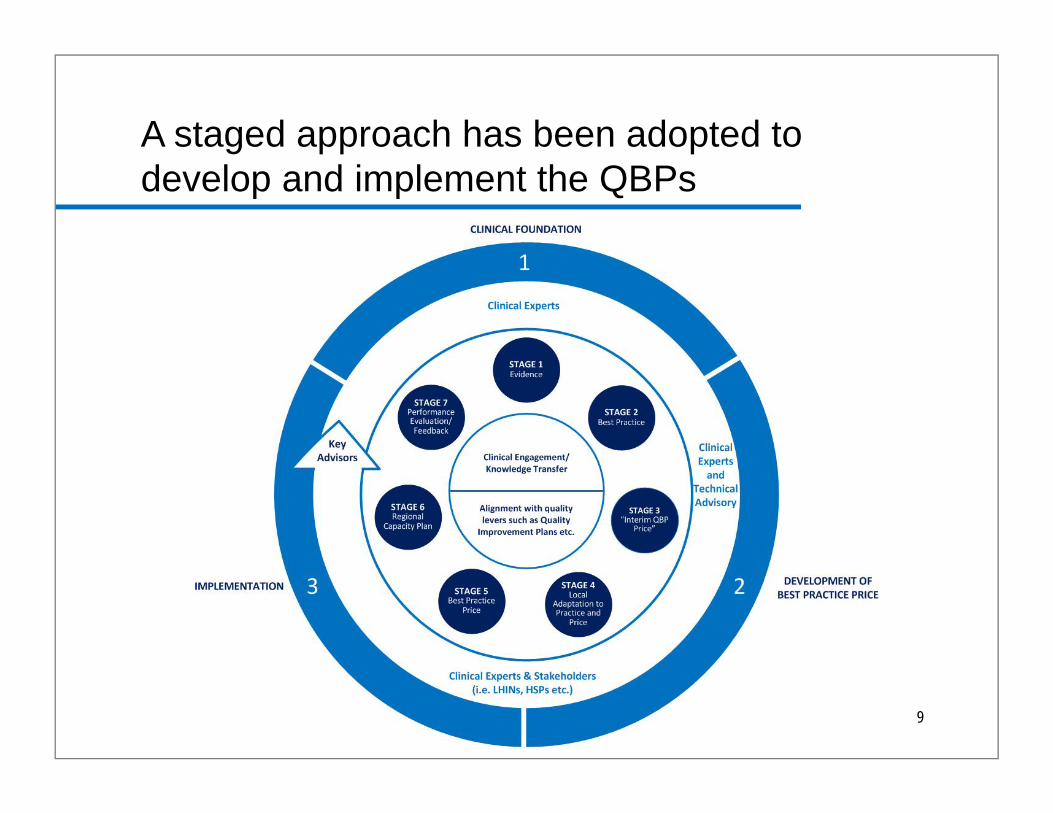
A staged approach has been adopted to develop and implement the QBPs
Agencies
9

Developing and implementing QBPs
Acute Inpatient• Entered Year 3 (FY 2014/15) of QBP implementation• To date, QBPs represent 13% of the total provincial budget
Transition from Acute Inpatient Admissions• Existing QBPs expanded to address transition from inpatient
admission/episode
Community• Concurrent work underway to define community-focused QBPs
Integrated Indicator Scorecard• Provide a starting point for monitoring and evaluating the impact of the
introduction of each QBP
10
Coding and data quality: raising the bar
Patient Assignment to all QBPs based on coded data • Funds to be paid for different QBPs will vary• Not all patients fit a QBP criteria• Funds for patients with the same diagnosis that are within or outside the QBP
criteria will differ • Capacity planning…it’s not just about volume reconciliation
It’s not the Ministry’s data: it’s the organization’s• Overt and transparent link between coded patient data and funding• Improved data quality benefits everyone• Documentation (physician and departmental) challenges need to be resolved,
need for issues to be escalated • Likely need new data elements; keeping abreast of standards even more
important
11
• Normal scapegoat for any performance results is coding
• Education sessions held by Medical Records departments for physicians and clinicians usually result in improved quality of charted data
• Main concern is getting physicians to consistently and accurately ensure highest quality of charted data
• Data review process
• Optimizing processes
Coding and data quality
12
• Demands for data in a shorter time
• Incomplete charts are an issue
• Inevitable changes to charts when all results and documentation becomes available
Timing and turnaround
13

• Complete, clear, and accurate documentation is the foundation for complete and accurate coding of all types of medical records
• Deficiencies in the documentation result from: o Failure of health care provider to record informationo Lack of detail or specificityo Conflicting or inconsistent informationo Illegible documents and/or o Missing documents
Deficiencies in documentation
14
• Depending on the QBP, in some instances, there may be a need to code new and/ or previously non-mandated codes. For example, in the case of Jaundice QBP, phototherapy has now been mandated for coding as of April 2014
• With the introduction of QBPs, it becomes even more imperative that there is full, complete and accurate documentation and coding of the patient care by the HSP
• Inaccuracies in coding will affect the HSPs, patient assignment to HIGs, and also weighted cases
154
With QBPs, how will clinical documentation change?

• HSFR is about standardized approaches to define best practices and funding best practice
• Each hospital should ensure the right patients are coded within a QBP, that way challenges to appropriate funding is based on actual patients and costs
• QBPs can be the catalyst for recognizing key coding processes (challenges) and improving clinical documentation
• Internal analysis should be undertaken to review patients included and excluded from QBPs in an organization. • Are there significant clinical differences? • Do these differences reflect the panel’s definitions?
HSFR and Coding
16
• To enable decision making, there will be an increased focus on ensuring the codes assigned in the patient record truly represent the case
• Ensuring the documentation in the record is accurate
• Conducting periodic internal audits of coding adequacy
• More involvement in organizational-wide QI initiatives for the relevant QBP (Currently low level of HIM involvement on internal QBP working groups)o Greater interdisciplinary collaborations to implement
strategies to improve documentation, coding practices, and staff development to optimize coding
• Reporting on patient-level cost data that brings together data on both utilization and cost per unit of service
What does this mean to you?
17

• Continued QBP coder education
• Educate clinical teams on documentation, coding process, internal standards; develop Tip and Tick sheets and identify when and how to use Order Sets and CPOE in the coding and abstracting process
• Facilitate and promote complete and accurate coding and abstractingo Physician documentationo Advocate query process especially for QBP patientso Incomplete chartso Ensure QA process to optimise coding for patient charts
• Increased coder participation with clinical teams and on QBP working groups/committees
Recommendations
18

• Ideally each panel should have at least one Health Information Analyst/Coder
• Panels include nurses, pharmacists, social workers, Physiotherapists, Occupational Therapists, Decision Support specialists, clinicians and administrators
• However, very few panels have HIM staff
• Looking to change process to include an additional step to have a group of HIM specialists review panel code-able inclusion/exclusion criteria
Involvement in expert panels
19
What role can you play?
Contact Our Helpline with Your Questions!
Please email or direct your enquiries related to HSFR to the
ministry’s health system funding Helpline:
or call 416-327-8379
21