ptpost-it d tiintroduction obtibservation of … d tiintroduction obtibservation of hlthhealth care...
TRANSCRIPT

P t i t d ti b ti f h lthPost-introduction observation of healthcare technologies after coverage
The Galician experience with percutaneous aortic valve replacement (TAVIs)
Leonor Varela LemaLeonor Varela LemaTeresa Queiro VerdesMarisa López GarcíaJeanette Puñal Riobóo
Bilbao. 26th June 2012
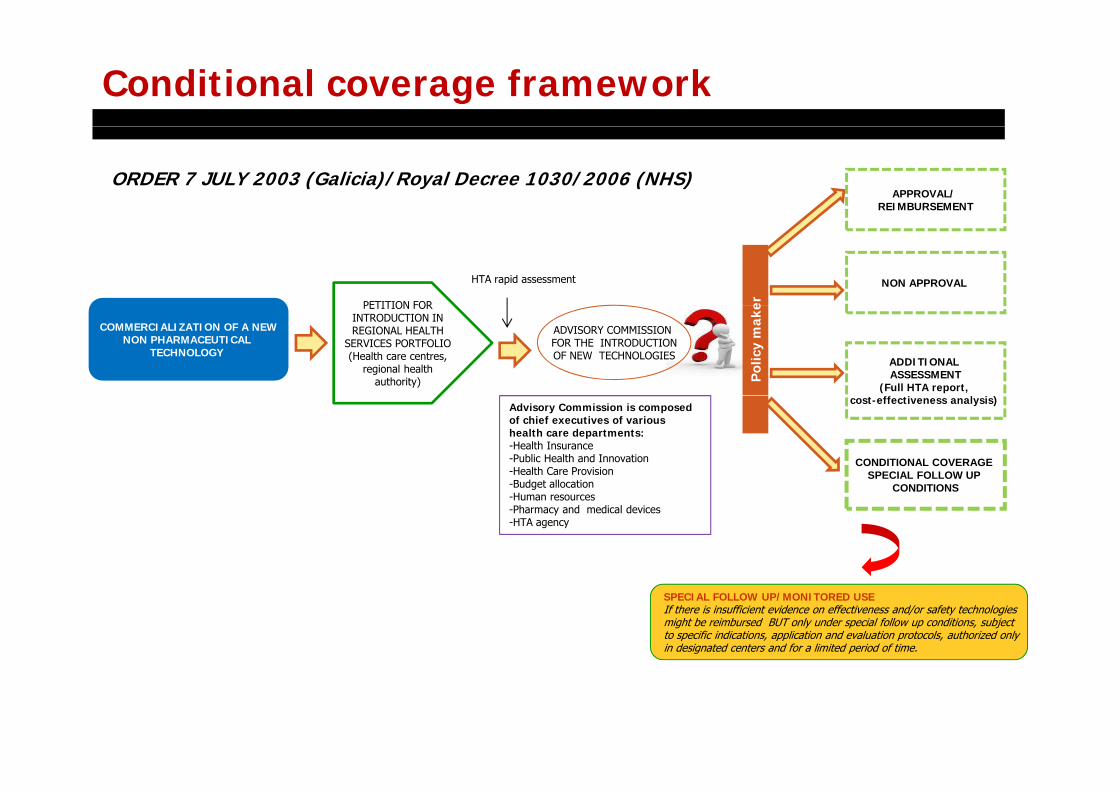
Conditional coverage framework
APPROVAL/ REIMBURSEMENT
ORDER 7 JULY 2003 (Galicia)/Royal Decree 1030/2006 (NHS)
NON APPROVAL HTA rapid assessment
PETITION FOR er
COMMERCIALIZATION OF A NEWNON PHARMACEUTICAL
TECHNOLOGY ADDITIONAL ASSESSMENT
(Full HTA report,
PETITION FOR INTRODUCTION IN REGIONAL HEALTH
SERVICES PORTFOLIO (Health care centres,
regional healthauthority) P
olic
ym
ake
ADVISORY COMMISSION FOR THE INTRODUCTIONOF NEW TECHNOLOGIES
cost-effectiveness analysis)
CONDITIONAL COVERAGE SPECIAL FOLLOW UP
CONDITIONS
Advisory Commission is composed of chief executives of various health care departments:-Health Insurance-Public Health and Innovation-Health Care Provision-Budget allocation CONDITIONSBudget allocation-Human resources-Pharmacy and medical devices-HTA agency
SPECIAL FOLLOW UP/MONITORED USEIf there is insufficient evidence on effectiveness and/or safety technologiesmight be reimbursed BUT only under special follow up conditions, subjectto specific indications, application and evaluation protocols, authorized onlyin designated centers and for a limited period of time.
Context
It can hamper the early introduction of technologies that are deemed to have an important
Concerns regarding the applicability of “special follow up” schemesIt can hamper the early introduction of technologies that are deemed to have an important impact on health.
In some cases the new technology has already diffused within the health system and patients who are candidates for the procedure can be discriminated from receiving it if they do not attendwho are candidates for the procedure can be discriminated from receiving it if they do not attend the authorized centers.
Research studies are frequently very demanding (too many variables, follow up visits, long follow up times) and clinicians allege that they have great difficulty in collaborating (lack of timefollow up times) and clinicians allege that they have great difficulty in collaborating (lack of time, important workload that difficults data collection, patient losses).
The process is very lengthy and medical procedures frequently evolve during the research process, to the point that indications might be obsolete or the trials findings might be of little relevanceto the point that indications might be obsolete or the trials findings might be of little relevance when results are available.
Does not provide useful information to resolve uncertainties regarding appropiate use in daily practice and best clinical managementpractice and best clinical management.
ReferenceVarela‐Lema Leonor, Atienza Merino Gerardo, López García Marisa, Vidal Martínez María, Gervas Triana Elena, Cerdá Mota Teresa. Demands and expectationsfor health technology assessment: qualitative analysis from the perspective of decision makers and clinicians. Gaceta Sanitaria 2011; 25(6):454‐460

Post-introduction observation conditional coverage scheme
onfor
the
NT
trod
uct
io
y Co
mis
sion
fod
uctio
n of
N
Reimbursement
Res
olu
tion
Brief report
Int
Advi
sory
Intr
o
Real life data
Post-introduction observation
There is sufficient evidence to establish that thetechnology is effective and safe but there are importantdoubts as to the applicability of the results when thetechnology is used in wider populations or importantuncertainty regarding the diffusion or application of thetechnology in real life practice (off label use, costdeviations).
Improving health caremanagementmanagement
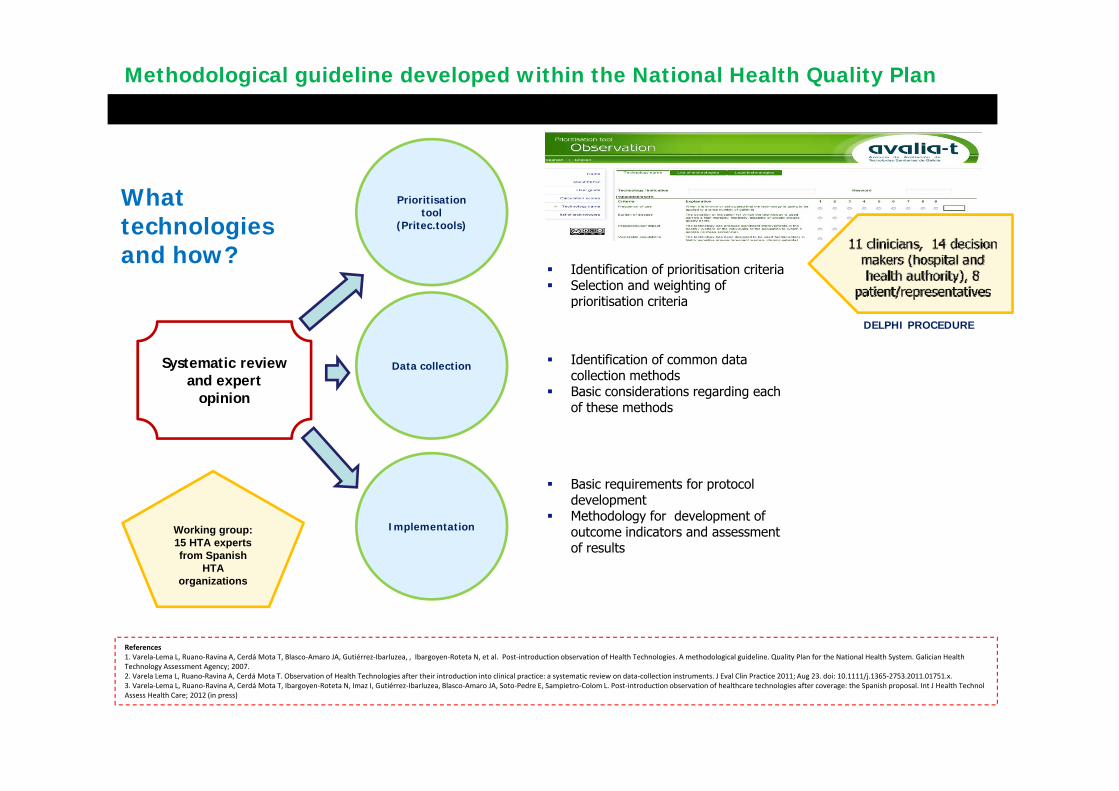
Methodological guideline developed within the National Health Quality Plan
What Prioritisationtool
technologies and how?
tool(Pritec.tools)
Identification of prioritisation criteriaSelection and weighting of prioritisation criteriaprioritisation criteria
Data collection
DELPHI PROCEDURE
Systematic reviewand expert
opinion
Identification of common data collection methodsBasic considerations regarding each
Basic requirements for protocol
opinion Basic considerations regarding eachof these methods
Implementation
Basic requirements for protocoldevelopmentMethodology for development of outcome indicators and assessmentof results
Working group: 15 HTA expertsfrom Spanish
HTA
References1. Varela‐Lema L, Ruano‐Ravina A, Cerdá Mota T, Blasco‐Amaro JA, Gutiérrez‐Ibarluzea, , Ibargoyen‐Roteta N, et al. Post‐introduction observation of Health Technologies. A methodological guideline. Quality Plan for the National Health System. Galician Health T h l A t A 2007
organizations
Technology Assessment Agency; 2007.2. Varela Lema L, Ruano‐Ravina A, Cerdá Mota T. Observation of Health Technologies after their introduction into clinical practice: a systematic review on data‐collection instruments. J Eval Clin Practice 2011; Aug 23. doi: 10.1111/j.1365‐2753.2011.01751.x. 3. Varela‐Lema L, Ruano‐Ravina A, Cerdá Mota T, Ibargoyen‐Roteta N, Imaz I, Gutiérrez‐Ibarluzea, Blasco‐Amaro JA, Soto‐Pedre E, Sampietro‐Colom L. Post‐introduction observation of healthcare technologies after coverage: the Spanish proposal. Int J Health Technol Assess Health Care; 2012 (in press)

Main considerations derived from the guideline
Only key data should be collected (MINIMUM DATA SET)
The different stakeholders should be implicated from the beginning and should be involved in theestablishement of data requirements, data collection methods, follow up schedule and outcomeindicators that are considered feasible, clinically meaningfull and relevant to the health caresystemy
Data recorded should be as far as possible, final result variables and be part of data recordedroutinelly in medical records or considered relevant for decision making
The study should not increase the number of procedures or tests performed to the patient
Whenever possible, follow up contacts should be in agreement with routine check ups
The follow up should be as short as possible, even though sufficient for obtaining an adequatenumber of patients in each study subgroup
Data collection instruments should be context specific. The incorporation of outcome variables into theelectronic clinical records is the recommended option but not always feasible.

Post-introduction observation of transcatheter aortic valve implantation
Patient recruiment
D t ll ti
IMPLEMENTATIONPLANNINGPRIORITISATION
Data collection
Information exchange
HTA based follow up protocolSystematic review
Representatives from health authority
Opinion of clinicians from authorized centres
All 3 authorized centres
Approval of TAVI (transapical and transfemoral) for treatment of
1st meeting: consensus on outcome variables, subgroups, follow up schedule, data collection instruments , information exchange, information rights,
Proposal for post-introductionObservation of TAVI from health authority
for treatment of non operable or high risk patients with severe aortic stenosis (> 75 years old)
Creation data base
Protocol development
o a o g ,confidentiality
2º meeting: Discussion of results and recommendations
Data analysis
Technical report
avalia tavalia-t

Data collectionData collection: pre-intervention, post-intervention, 1, 6 and 12 monthsExcel questionnaire form to be completed on the computer or manuallyE-mail or ordinary mail
INTERVENTION
FOLLOW UP
Patient´s selection criteria
Adverse events
Description of procedure
Valve hemodynamics and NYHA functional class
Success of the intervention
Hospital complications
Hospital readmissions
F ll l d d hFollow up losses and death causes
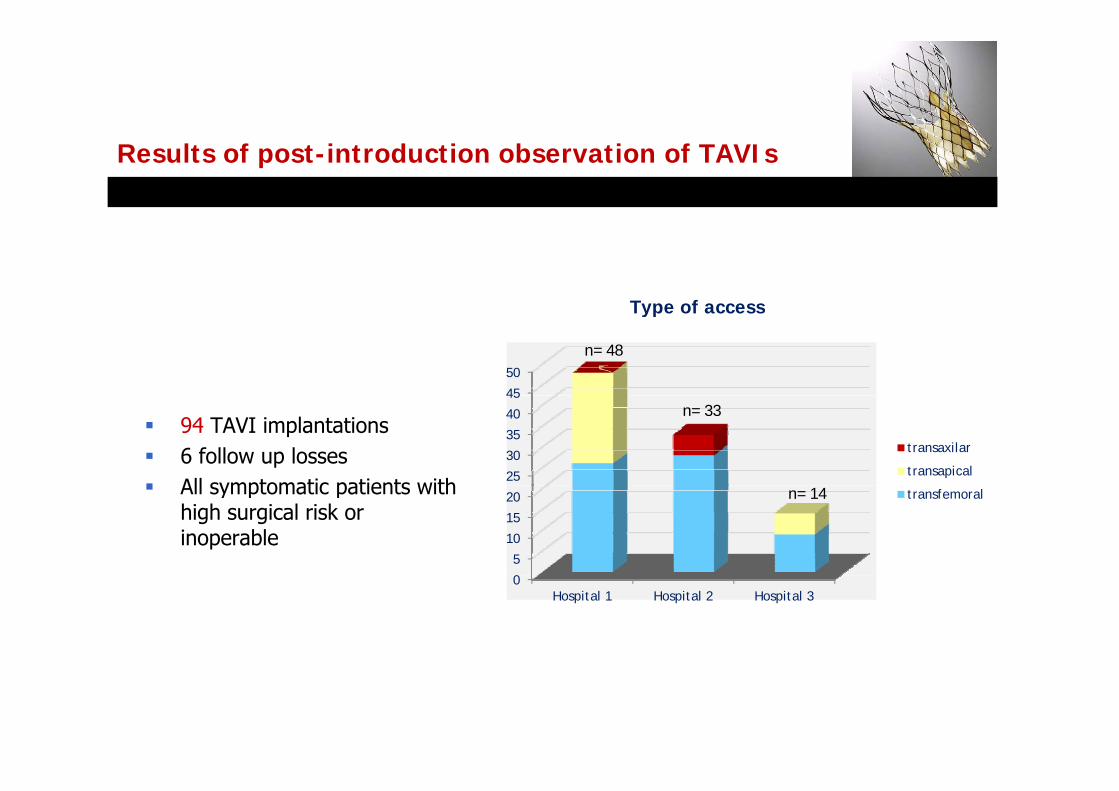
Vía de accesoResults of post-introduction observation of TAVIs
Type of accessType of access
45
50
n= 48
94 TAVI implantations6 follow up lossesAll symptomatic patients with
25
30
35
40
45
transaxilar
transapical
n= 33
All symptomatic patients withhigh surgical risk orinoperable
0
5
10
15
20 transfemoraln= 14
0Hospital 1 Hospital 2 Hospital 3
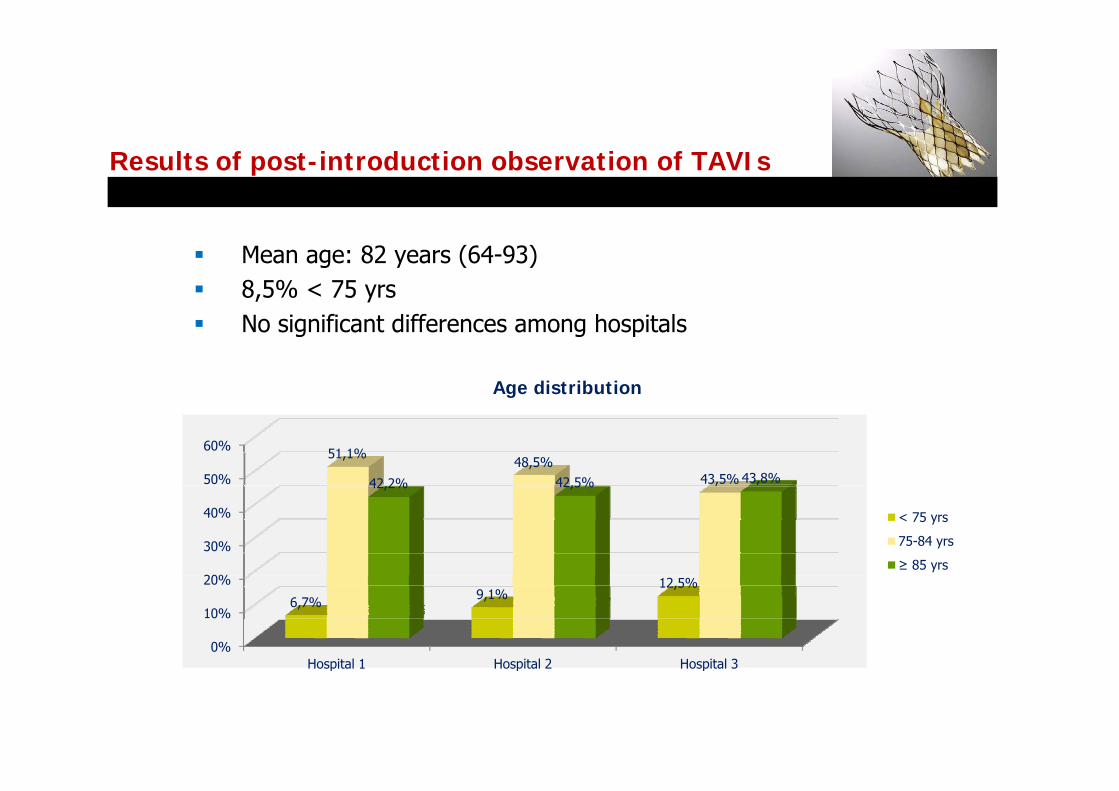
Results of post-introduction observation of TAVIs
Mean age: 82 years (64-93)8,5% < 75 yrsNo significant differences among hospitals
Age distribution
50%
60% 51,1%48,5%
43,5%42 2% 42,5% 43,8%
g
20%
30%
40%
,42,2% 42,5%
< 75 yrs
75-84 yrs
≥ 85 yrs
0%
10%
20%
Hospital 1 Hospital 2 Hospital 3
6,7% 9,1%12,5%
Hospital 1 Hospital 2 Hospital 3

Results of post-introduction observation of TAVIs
Logistic EuroScore: 15,1% (2,9-73,2)
EuroScore distribution
50%
60%
70%60,0%
36 4%
45,5%50,0%
EuroScore< 10%
20%
30%
40%
18% 18%
25%
36,4%
25,0%22,2%
EuroScore< 10%
EuroScore 10-20%
EuroScore > 20%
0%
10%
Hospital 1 Hospital 2 Hospital 3

Results of post-introduction observation of TAVIs
Distribution of adverse events
Correct implantation: 96,8% 35%
40%
45% 42,4%43,9%
37,7%
p ,Hospital mortality: 7,4%Acumulated 1 year survival: 81,7%Complications: 40,4 %
20%
25%
30%
22%18,8%
25,1%
Hospital 1
Hospital 2
All patients improved NYHA functional class
5%
10%
15%
20% 16%
4%2%
9%
3%
Hospital 3
0%
5%
Vascular complications
Cardiac Complications
Renal failure Others complications
2%3%0%
Proposal derived from the stakeholder meeting
Update of systematic review and creation of a multidisciplinar group for therevision of selection criteria for TAVI authorization
Policy makers
Representatives from authorized centres
Creation of a multidisciplinary Hospital Commission within each authorizedhospital to consensuate TAVI implantation
Cardiologists and cardiac surgeonsCardiologists and cardiac surgeons
Analise implantation variability not attributed to geographical differences(accessibility problems, overuse, underuse?)

Main limitations
Delay in the forwarding of data (various contacts and active collection in 1 centre)
Different follow up visits and data recording times
Not all patients underwent transthoracic echocardiography before or after the intervention and so it was impossible to assess valve hemodynamics, paravalvular leaks or severity of aortic stenosis
The majority of centres only took into account disnea to establish symptomatology
Insufficient number of patients to determine if there are deviations in adverse events (n s) or if there are differences between different subgroups (type of access type of(n.s) or if there are differences between different subgroups (type of access, type of valve, hospital, etc)
Insufficient patients to detect cost deviations
Reticence of clinicians to be evaluated by external organizations
Ongoing strategies to improve applicabilityOngoing strategies to improve applicability
Definition and standardization of result variables to homogeneizeDefinition and standardization of result variables to homogeneizedata recording
Development of a web application to promote visibility and use ofDevelopment of a web application to promote visibility and use of the tool in collaborative projects in order to increase power todetect deviations in effectiveness/safety and allow for subgroupanalysisy
NEAR FUTURE!!! Incorporate result variables in electronic clinicalrecords and develop linkage mechanism to import data
