preventing and reducing adverse drug events in care coordination communities: cycle 1 results anne...
TRANSCRIPT
Preventing and Reducing Adverse Drug Events in
Care Coordination Communities:Cycle 1 Results
Anne Myrka, RPh, MATIPROJuly 30, 2015
Objectives
Describe IPROs CMS 11th Scope of Work Priorities and Goals
IPRO Drug Safety work overview
Describe the Preventing and Reducing Adverse Drug Events (PARADE) initiative: Objectives and Strategy
Provide Cycle 1 (January – June) results
Highlight facility specific interventions and experiences – guest speakers
Next Steps, Q & A
2

Thank You!!!
3

Coordination of Care Task Goals
Promote Effective Communication and Coordination of Care
Reduce hospital readmission rates in the Medicare program by 20% by 2019 Reduce hospital admissions rates in the Medicare program by 20% by 2019
Increase community tenure, as evidenced by increased number of nights spent at home, for Medicare beneficiaries by 10% by 2019
Reduce the prevalence of adverse drug events (ADEs) that contribute to significant patient harm, emergency department visits, observation stays, hospital admissions or readmissions occurring as a result of the care transitions process
● Anticoagulants
● Hypoglycemic Agents
● Opioids
4

IPRO Drug Safety overview
NYS Anticoagulation Coalition Appropriate DOAC use – included in utilization reports
Effective EHR utilization – manuscript published
Peri-procedural utilization of all anticoagulants – MAP tool (app under development)
Pain Management Task Force Reducing opioid-related adverse drug events (ADEs)
Hypoglycemia agent Task Force Reducing hypoglycemia-related ADEs
5
What is IPRO’s PARADE Initiative?
6
PARADE Initiative – 2014 Pilot study and results Evidence-based system improvements were applied
to Anticoagulation Discharge Communication and Med Rec on Admission according to site-specific baseline results
Significant improvement in communication of requisite anticoagulation-related elements to subsequent provider upon transfer/discharge:
All facilities (16%, 95% CI 11.6%-20.3%)
Hospitals (8%, 95% CI 1.2%-15.2%)
SNFs (19%, 95% CI 12.7%- 25.8%)
Significant improvement in completion of medication reconciliation processes upon admission in SNFs (21.2%, 95% CI 9.6%- 31.9%)
7

PARADE Initiative
QIOs are directed by CMS in the 11th Statement of Work (11SoW- 2015-2019) to:
Establish relationships and collaborations in the community to coordinate provider communication and medication management across care settings with a patient centered focus
Help providers utilize new or existing evidence-based tools and practices to improve the care of those prescribed high risk medications, specifically anticoagulants, diabetic agents and opioids
Use health information technology to screen for and prevent ADEs in Medicare beneficiaries
8
PARADE Objectives and Strategy
9
PARADE Objectives
To identify patients at risk of experiencing ADEs due to high risk medication use following hospital discharge
To identify hospital readmissions and emergency department visits associated with high risk drug exposure
To evaluate the post-discharge medication use system across care settings and identify opportunities for system improvements
To facilitate the implementation and serial evaluation of evidence-based intervention strategies
10
PARADE Strategy Process measures – All facilities/healthcare providers
Small, low-impact audits of medication reconciliation processes and high risk drug discharge communication (5-10 charts, retrospective)
Serial evaluation to guide improvements
Goal: measureable improvement in adherence to audit criteria
Interventions
Evidence based interventions according to site-specific results
Outcome measures – Hospitals only
Readmissions due to ADEs using data from electronic health record data (hospital) and claims data (IPRO)
Serial evaluation to identify improvements
Goal: Demonstrate measureable improvement over 5 year scope of work
11
PARADE Strategy Based on 6 month improvement cycles
Cross setting work will be achieved within each care transition coalition Medication Management Committee monthly meetings
Eligible facilities: hospitals, skilled nursing facilities (SNF), rehabilitation facilities, home healthcare services/agencies (HHA), residential facilities, adult homes, pharmacies (hospital, community, SNF vendors, etc.)
Participating individuals are administrators, physicians, nurses, pharmacists (including SNF consultant pharmacists), quality improvement professionals, discharge planners, HHA hospital liaisons, etc.
Cycle 1 was January 6, 2015 – June 30, 2015 All facilities focused on Medication Reconciliation and Anticoagulation
Discharge Communication
12
PARADE Strategy
Cycle 2 is September 2015 – February 2016 Continue to work on ADE hospital readmission measure,
high risk drug discharge communication and med rec improvement processes (expanding to discharge)
Expand to medication management of hypoglycemics, opioids, other (e.g. antibiotics)
IPRO is currently convening subject matter experts to provide guidance on best practices for management across care settings during transitions
Subsequent Cycle work will focus on continued evidence based improvements, sustainability and applicable cross-setting emerging measures
13

PARADE Process Measures: Audit Methods
14

PARADE Process Measures: Audit Methods
Medication Reconciliation on Admission Audit Medication Discrepancy Tool
Anticoagulation Discharge Communication Audit Anticoagulation Information Discovery Tool
15
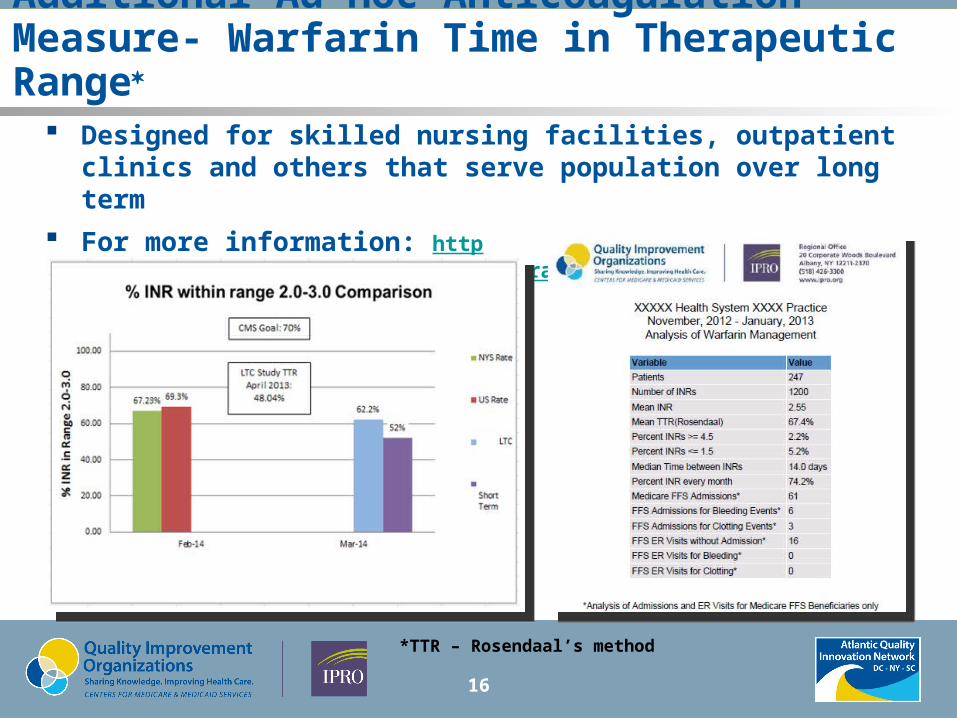
Additional Ad Hoc Anticoagulation Measure- Warfarin Time in Therapeutic Range
Designed for skilled nursing facilities, outpatient clinics and others that serve population over long term
For more information: http://qio.ipro.org/drug-safety/collaborative-partners/analytic-services
16
*TTR – Rosendaal’s method
Cycle 1 Results
17

18
Anticoagulation Discharge Communication

19
Medication Reconciliation
20
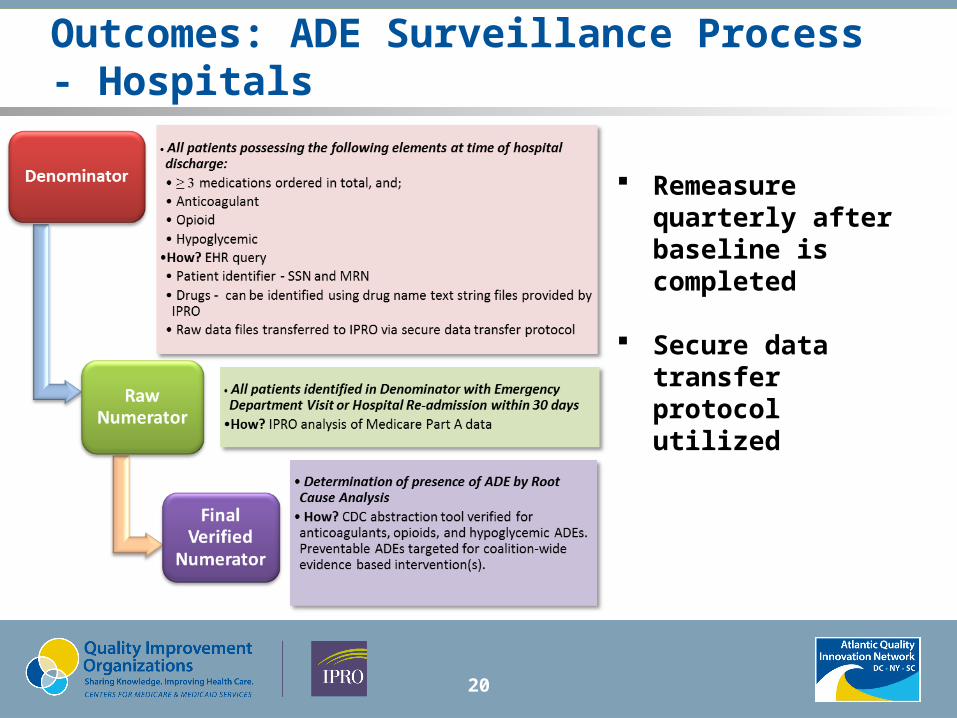
Outcomes: ADE Surveillance Process - Hospitals
Remeasure quarterly after baseline is completed
Secure data transfer protocol utilized
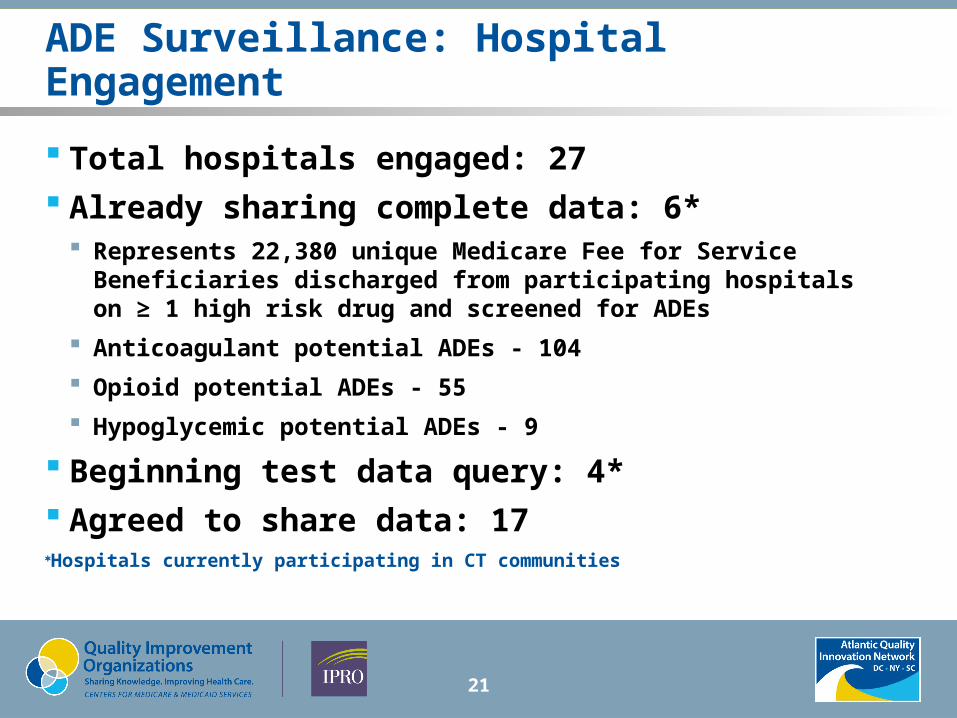
ADE Surveillance: Hospital Engagement
Total hospitals engaged: 27 Already sharing complete data: 6*
Represents 22,380 unique Medicare Fee for Service Beneficiaries discharged from participating hospitals on ≥ 1 high risk drug and screened for ADEs
Anticoagulant potential ADEs - 104
Opioid potential ADEs - 55
Hypoglycemic potential ADEs - 9
Beginning test data query: 4* Agreed to share data: 17Hospitals currently participating in CT communities
21

PARADE Interventions
22

Medication Reconciliation Improvement Tools
23
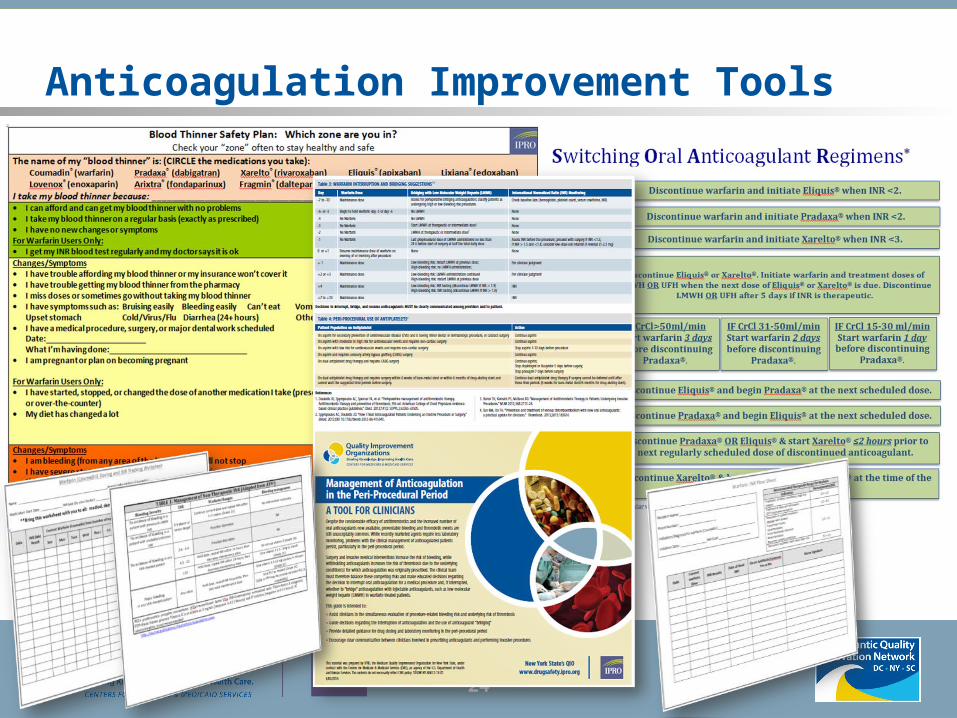
Anticoagulation Improvement Tools
24
Facility Specific Interventions
25
HealthAlliance of the Hudson Valley, Kingston, NY Medication Reconciliation Risk Reduction Strategies
Identified ASU staff were provided additional training on how to
enter home medications in the EMR to generate a “clean” medication reconciliation. No free texting!
Orthopedics -aggressive education with Medical Staff on steps to complete medication reconciliation utilizing the EMR. Informatics staff assisted MD with 1:1 concurrent training
Set up touch points with MD to address any concerns identified with use of medication reconciliation process
Sole use of the EMR for medication reconciliation. No more paper!
26

HealthAlliance of the Hudson Valley, Kingston, NY Medication Reconciliation Risk Reduction Strategies
Identified continued: The Emergency Department created dedicated resource
called “Clinical Data Specialist”
This position is staffed with an a Pharmacy Tech or LPN. They are required to enter into the hospital EMR all of the “Home Medications” for all patients admitted.
Two sources must be utilized to reconcile the list of home medications
The patient’s list
Call pharmacy
Calling the patient’s MD
Reviewing the list from the ER EMR
27
HealthAlliance of the Hudson Valley, Kingston, NY
Medication Reconciliation Opportunities for Improvement:
CHF patient post discharge phone calls identified need for clearer patient instructions on home medication resumption or discontinuation. Not always evident in the medical record.
Pharmacy medical record application does not allow pharmacist to view MD reason for stopping/discontinuing medications.
28
HealthAlliance of the Hudson Valley, Kingston, NY
Blood Thinner Adverse Events – Risk Reduction Strategies Identified:
Orthopedics physicians managing post operative course of blood thinner or conferring with patient’s cardiologist.
Orthopedics - plan to pilot a sequential compression biomechanical device (SCBD) replacing the use of utilizing blood thinner medications
29
HealthAlliance of the Hudson Valley, Kingston, NY
Blood Thinner Adverse Events – Opportunities for Improvement:
Multiple places in EMR where information regarding high risk blood thinner medication may be documented.
Auditing difficult due to inconsistent documentation. Sub-group identified location of possible documentation – evaluating possibility of creating a blood thinner tab in EMR for centralized documentation.
Information needed for transition of care not summarized.
30
HealthAlliance of the Hudson Valley, Kingston, NY Medication Reconciliation – High Risk Medication –
Discharge Process Audit Audit 35 charts utilizing IPRO medication reconciliation
discharge tool to obtain baseline.
Audits to be completed no later than July 31, 2015
Charts to be audited by discharge location: ● 5 - SNF, Rehab, Acute Care
● 5 – ED
● 5 – Orthopedics
● 5 – General – Home
● 5 – Endo
● 5 – Hypoglycemic agents
● 5 – CHF
31

Albany Memorial Hospital, Albany, NY
32
Anticoagulant-related high priority elements highlighted for hospitalists in real time during discharge summary dictation – facilitated by case management at time of discharge
Kaizen done regarding standardization of discharge practices● Patient teach back
● Identifying high risk patients
● ED med rec by pharmacist
● Contact PCP on admit
● Identify caregiver/family by day 2
● Rapid summaries for high risk drugs
Evergreen Commons, East Greenbush, NY
Initiated the Blood Thinner Safety Plan Complete med list printed from Omniview indicating
drug, dosage and time of next dose due Most recent fall risk assessment faxed to community
PCP Resident PT/INR flow sheet faxed to community PCP Medication Reconciliation – home meds Developed a discharge check list
33
Home Healthcare
Dominican Sisters Family Health Services Multiple PDSAs and PARADE huddles weekly
Business Development Managers and Liaison Champions
Standardized New Electronic Referral which includes mandatory fields to capture Anticoagulant high priority elements
Collaboration with hospital readmission teams
Access to hospital electronic medical record attained
Nurse education
Cross-setting pilot of Blood Thinner Safety Plan - planning for next cycle.
34

Home Healthcare
VNA of the Hudson Valley
Evidence Based Patient Education Protocols and Materials – including BTSP, INR Worksheet, RN Pt. Teaching Plan Checklist, Guidelines for Lovenox Administration/Precautions; Patient self-test re: learning achieved
Guidelines for Home Health Intake Coordinators – Baseline transfer information
Anticoagulation information to be sent to PCP upon discharge from homecare; Transfer summaries to reflect status of anticoagulation therapy
Nurse education
35

Home Healthcare VNS Westchester – Putnam Branch
Implementing intake template revision to capture salient anticoagulation information for use by Home Health Intake Coordinators and Liaisons
Piloting Blood Thinner Safety Plan and Warfarin Dose and INR flow sheet
Developing Discharge Summary Form for patients on AC therapy to be sent to the PCP or other provider upon discharge from home care services: to include diagnosis requiring need for AC therapy, flow sheet account of past INR readings, corresponding AC medication changes, s/s bleeding, related teaching, etc.
Working with local hospital readmission task force for access to patient portal and other options to obtain most current accurate discharge medication and other pertinent data related to AC therapy: last 3 INR’s, reason for AC therapy, identification of patients new to AC therapy, therapeutic level, etc.
Working with Director of Pharmacy at local hospital for identification of patients on AC therapy at risk for complications and in need of home care follow-up.
Developing process for standardized, mandatory clinician education on the assessment and pharmacology aspects of the anticoagulated patient.
36

Next Steps Webinar: PARADE Cycle 2 Launch
Wednesday, September 9, 2015 2:00pm – 3:00pm This webinar will serve as an introduction to IPRO’s Preventing
and Reducing Adverse Drug Events (PARADE) initiative for new communities and provide information for those communities entering PARADE Cycle 2.
Click or Copy and Paste this URL to your web browser: https://qualitynet.webex.com
Password: IPRO
Dial in number is 866-209-5917. The access code is NO CODE NEEDED.
37

38
Questions / Feedback
For more informationAnne MyrkaPharmacist – Drug Safety(518) [email protected]
IPRO CORPORATE HEADQUARTERS
1979 Marcus AvenueLake Success, NY 11042-1002
IPRO REGIONAL OFFICE
20 Corporate Woods BoulevardAlbany, NY 12211-2370
www.atlanticquality.org
This material was prepared by the Atlantic Quality Innovation Network/IPRO, the Medicare Quality Innovation Network Quality Improvement Organization for New York State, South Carolina, and the District of Columbia, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents do not necessarily reflect CMS policy. 11SOW-AQINNY-TskC.3-15-25
IPRO Care Transitions Web Site:http://qio.ipro.org/care-transitions/overview
IPRO Drug Safety Web Site:http://qio.ipro.org/drug-safety/overview
Sara ButterfieldSenior Director – Care Coordination(518) [email protected]
Darren TrillerSenior Director – Drug Safety(518) [email protected]