presentación de powerpoint -...
TRANSCRIPT

Colangiocarcinoma
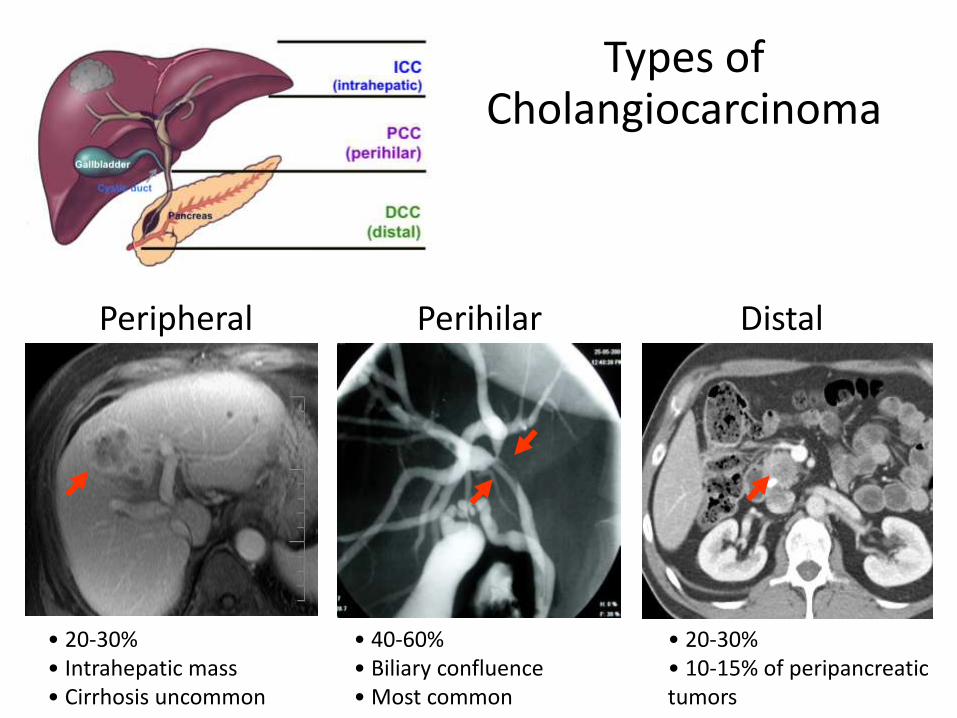
Types of Cholangiocarcinoma
Peripheral
• 20-30% • Intrahepatic mass • Cirrhosis uncommon
Perihilar
• 40-60% • Biliary confluence • Most common
Distal
• 20-30% • 10-15% of peripancreatic tumors

Epidemiology of Cholangiocarcinoma

Epidemiology of ICC
• Second most frequent primary liver tumor
• Increasing incidence and mortality worldwide
Changes in age standardized mortality rate
Khan SA, et al. Lancet 2005;366>1313

Etiology Cholangiocarcinoma
• Primary sclerosing cholangitis • Mainly associated with pCC.
• Hepatobiliary flukes (40% ICC) • Clonorchis sinensis and Opistorchis viverrini (OR up to 27)
• Biliary tract cysts • Choledochal cystic disease types I and IV (OR: 10 to 37)
• Hepatholithiasis • OR: 6 to 50
• Hepatotoxins • Nitrosamines

Etiology of ICC
81,8
8
3,6
2,6
1,6
1
10
100
Biliary Dis Cirrhosis DM HCV Smoking
Re
lati
ve R
isk
Chaiiteerakij D et al. Hepatology 2013; 57:648
• Cirrhosis • Of any nature.
• Chronic viral hepatitis • HBV and HCV.
• Obesity
• Diabetes • Conflicting results.
• Alcohol
• Smoking

Genetic variation and risk of cancer
A
Single nucleotide polymorphism (SNP)
G
* *
Normal Individuals Cancer Patients
RISK FACTORS
GENETIC DIFFERENCES

Etiology of ICC
• Several genetic polymorphisms have been identified
Bridgewater J, et al. J Hepatol 2014;60:1268
DNA preservation Toxin clearance Inflammation

Gene regulation Cyclin
CDK
p53 cell proliferation
Oncogenes y Cáncer
PI3K
AKT
RAS
RAF
MEK
GSK3b
APC
G Protein
Adenylate cyclase
JAK
mTOR MEKK MAPK MKK
b-Catenin PKA
STAT
myc ERK JNK
fos jun b-Catenin
CREB
STAT
RTK RTK
Survival Factors (e.g. IGF1)
Chemokines, Hormones (e.g. Interleukins, serotonin)
Growth Factors (e.g. TGF, EGF, HGF)
WNT
Cytokines (e.g. IFN)

Mecanismos de activación de oncogenes
Normal gene
Normal protein

Mecanismos de activación de oncogenes
gene mutation
gene deletion
novel regulatory sequences
hyperactive growth-stimulating protein in normal amount
gene amplification
normal growth-stimulating protein in excess
chromosome rearrangements
fusion transcripts
normal growth-stimulating protein in excess
hyperactive growth-stimulating protein in normal amount or excess

Cambios en la metilación y cáncer

Pathogenesis of ICC
Sia D, et al. Oncogene 2013;32:4861

Molecular Classification of ICC
Sia D, et al. Gastroenterology 2013; 144:829

Clinical Presentation of ICC
• Patients with early stage are usually asymptomatic.
• At more advanced stages, they may have non-specific symptoms
• weight loss, malaise, abdominal discomfort, night sweats, fever, or a palpable mass.
• Jaundice due to biliary tract obstruction is infrequent.
• CCA should be considered in patients with underlying disease (hepatolithiasis or PSC) with worsening performance status or unexplained loss of weight.
• Changes in liver function tests are non-specific, mainly with increased APh and GGT
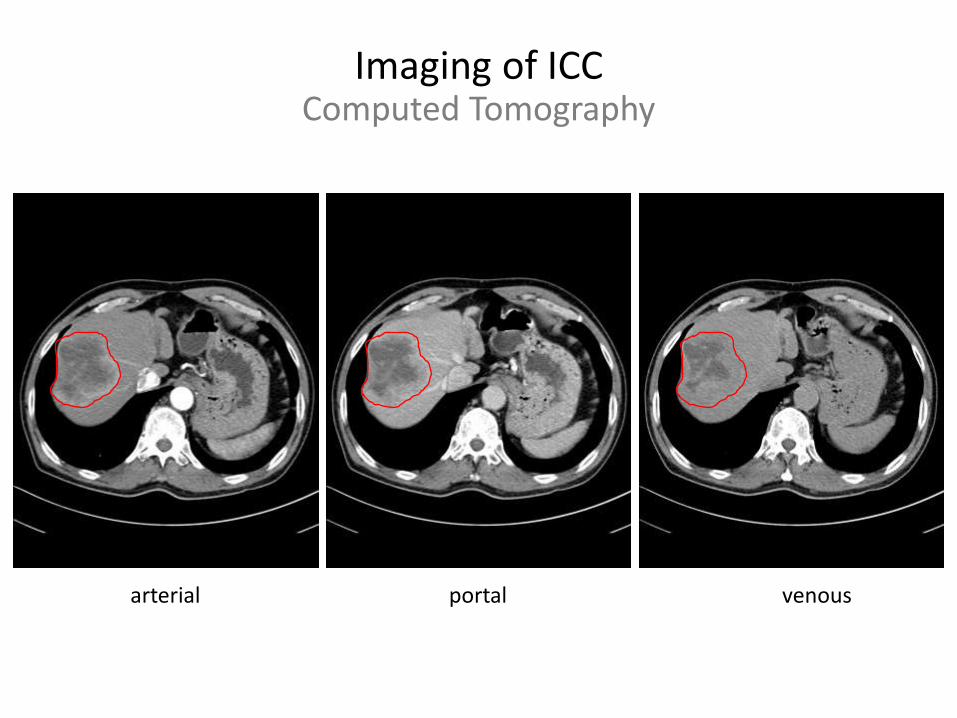
Imaging of ICC Computed Tomography
arterial portal venous

Imaging of ICC Magnetic Resonance
arterial portal venous
T1 T2

Imaging of ICC
arterial portal venous

Imaging of ICC
arterial portal venous
T1 T2 DWI

Imaging of ICC
25 patients with ICC on cirrosis. Median diameter 25 mm.
Rimola J, et al. Hepatology 2009;50:791

Tumor Markers
• CA 19-9 has significant overlap with benign diseases.
• Sensitivity is 62%
• Specificity is 63%
• CA 19-9 has some prognostic power:
• Preoperative values > 100 U/ml are associated with worse RFS.
• Bile duct obstruction may affect CA 19-9 levels (it should be reassessed after biliary intervention or drainage).

Pathological Diagnosis
• Typically an adenocarcinoma with tubular and/or papillary structures and a variable fibrous stroma.
• Similar to metastatic adenocarcinoma especially those of foregut origin (lung, pancreas, esophagus, and stomach).
• The expression of CK7 and CK20 may be helpful to establish a biliary origin.
• Differentiation from mixed HCC tumors may require evaluation of specific markers of hepatocellular or progenitor cell features
• Hep-Par-1, GPC3, HSP70, GS, EpCAM, and CK19.
• Pathological diagnosis is • required for definitive diagnosis, particularly those with cirrhosis and small
hepatic mass lesions.
• recommended for all patients who will be undergoing systemic chemotherapy or radiation therapy, or enrolling in a therapeutic clinical trial.

Colangiocarcinoma Intrahepático
Estadio I Estadio II Estadio III Estadio IV
Tumor único Multiple Invasión vascular (IV)
Perforación peritoneo visceral, Invasión hepática local
Invasión periductal, N1M1

Colangiocarcinoma Intrahepático
Estadio I Estadio II Estadio III Estadio IV
Tumor único Multiple Invasión vascular (IV)
Perforación peritoneo visceral, Invasión hepática local
Invasión periductal, N1M1
Resecable (30-40 %) No resecable (60-70 %)
Enfermedad sólo intrahepática
Enfermedad extrahepática
Resección curativa
Resección no curativa
Terapia Locorregional
Terapia Sistémica
Observación Ensayos Clínicos
Supervivencia a 5 años R0: 40 % Supervivencia a 5 años N1 e IV: 20 %
RF/TACE: mediana supervivencia 15 meses Quimioterapia: mediana supervivencia 12 meses
Bridgewater J, et al. J Hepatol 2014;60:1268

Liver Transplantation
• ICC has been considered a contraindication to LT based on very poor outcomes in historical series
• However, “very early” tumors may have much better outcomes
• A retrospective cohort multicenter study in 16
Spanish transplant centers.
• 29 patients found to have an iCCA on
pathology examination AND cirrhosis of
etiologies other than PSC.
• Indication for LT: HCC, or liver dysfunction with
pre-transplant identification of a liver nodule;
incidental tumors also included.
Sapisochin G, et al. Am J Transplant 2014; 14: 660

Liver Resection
Spolverato G, et al. JAMA Surg. 2015;150:538
• The main determinants of resectability are • extrahepatic disease
• tumor number and location
• involvement of portal vein and bile ducts
• Resectability rates are 20-40%
• Portal vein embolization may allow surgical rescue.
• Prolonged survival is infrequent, even in good surgical candidates.
535 resected patients (1990-2013)

Liver Resection
Spolverato G, et al. JAMA Surg. 2015;150:538
• Multicenter, international, retrospective study
• 584 patients who underwent resection of ICC (1990-2013)
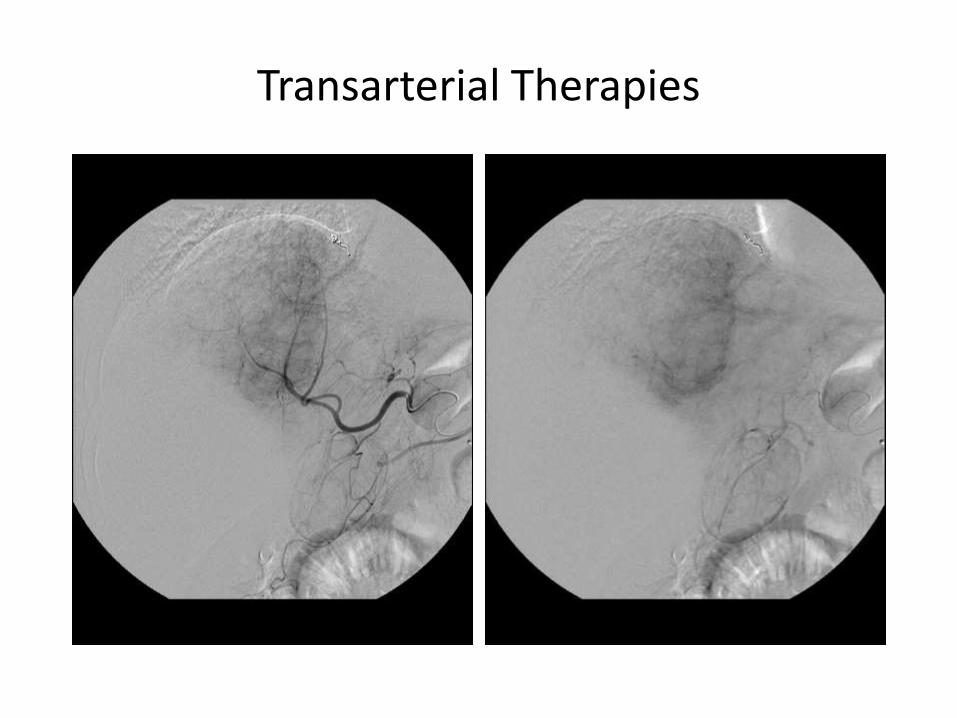
Transarterial Therapies

TACE for ICC

TACE for ICC
Variable Burger Herber Schiffman Park
No. of patients 17 15 24 72
Drugs CDDP- DOX-MMC MMC DEBIRI CDDP
ECOG > 0 53% 26% 35%
Multifocal 29% 53% 87% 57%
• Chemo 35% 26% 80% 0
• Resection 6% 29% 0
Tumor Response 47%* 6% 25% 23%
Median survival from RE 23 21.1 17.5 12.2 * EASL criteria

Radioembolization for ICC
Before Y90 MAA-PET/CT
Y90-PET/CT 3-months post-Y90

Radioembolization for ICC
Variable Ibrahim Saxena Hoffman Rafi Mouli
No. of patients 24 25 33 19 46
ECOG > 0 58% 40% 49% 95% 48%
Multifocal 54% 70% 68% 35%
Burden < 25% 83% 40% 75% 78%
• Chemo 29% 72% 79% 100% 35%
• Resection 40% 36% 11%
Tumor Response 27% 24% 36% 11% 25%
Survival since RE 14.9 9.3 22 11.5

Systemic Chemotherapy
Valle J, et al. N Engl J Med 2010;362:1273.

Systemic Chemotherapy
• Cisplatin (25 mg/m2) + Gemcitabine (1000 mg/m2) days 1 and 8 every 3 weeks is currently the standard of practice
• There is currently no targeted therapy which is applicable in CAA.
• There is no evidence which supports a second line chemotherapy
Valle J, et al. N Engl J Med 2010;362:1273.
Okusaka T, et al. Br J Cancer 2010;103:469. Eckel and Schmid. Br J Cancer 2007;96:896.

Schweitzer and Vogel. Best Practice & Research Clinical Gastroenterology 2015, 29:345.
Targeted Agents Under Investigation