premature infant maturity at discharge & subsequent healthcare costs” or: is it time to send...
TRANSCRIPT

Premature Infant Maturity at Discharge & Subsequent Healthcare Costs”
or: Is it Time to Send that Baby Home Yet?
Jeffrey H. Silber, M.D., Ph.D.Professor, Departments of Pediatrics,
Anesthesiology and Critical Care The University of Pennsylvania School of Medicine
Professor of Health Care SystemsThe Wharton School
Director, Center for Outcomes ResearchThe Children’s Hospital of Philadelphia

Acknowledgments• Center for Outcomes Research, CHOP and PENN Med
and Wharton– Jeffrey H. Silber, MD, PhD– Scott A. Lorch, MD, MSCE– Paul R. Rosenbaum, PhD– Barbara Medoff-Cooper, PhD, RN– Susan Bakewell-Sachs, PhD, RN– Andrea M. Millman, BA– Lanyu Mi, MS– Orit Even-Shoshan, MS
• Division of Research, Northern California Kaiser Permanente Medical Care Program– Gabriel J. Escobar, MD– Marla Gardner, BA
• FUNDING: Maternal and Child Health Bureau R40-MC-00236

Introduction
• Premature Births contribute a major portion to total inpatient pediatric costs
• The decision as to when to discharge a premature infant is complex, and like many other decisions in healthcare, not always uniform
• While guidelines exist through the AAP, there is considerable variation in practice

Goals of Study
• To determine whether keeping a premie baby a few days longer in the NICU solely to increase maturity may lead to subsequent cost savings after discharge
• To determine whether such cost savings after discharge could outweigh the greater inpatient costs associated with longer stays initially


Why is Attila Relevant?
• We wanted a point in time in the infant stay when even “Attila” would not send the baby home—we thought 31 weeks PMA would be reasonable.
• Starting at the Attila point, we recorded the daily physiologic variables needed to make a decision to discharge– Feeding, weight gain, off IVs– Temperature Stability (out of incubator)– Cardio-Respiratory Stability (No A’s and B’s while off
oxygen and stimulants)

Study Population
• Babies born a one of five NICUs in the Northern California Kaiser-Permanente System
• Born between 1998-2002• GA 34 weeks or less• Without congenital anomalies• No VP shunts, no major cardiac surgery patients• Of 2,144 electronically screened and randomly
selected (after all babies less than 28 weeks were included), 1474 met study criteria, 30 charts were missing and 42 had incomplete records. Hence 1402 were included in the study (with 265 babies less than 28 weeks).

Study Design: Matching
• Divide the 1402 study babies into two groups through nonbipartate multivariate matching
• 702 Early babies• 702 Late babies (matched to the Early
baby on the day the Early baby went home, but who went home on average 3 days later than their Early baby matched pair)
Matching Variables
• We matched on variables relevant for determining when a baby should go home as obtained from chart review:– The infant’s medical history (BW, GA and History
variables such as NEC, IVH, BPD)– The infants maturity leading up to discharge
• Exponentially smoothed history of days since a skill was mastered. For example, days out of incubator, days off gavage feeding, days off methylxanthines
• Propensity Score for discharge based on a time-dependent Cox model
– Maternal Characteristics: Age, number of children, income

Defining Costs
• Costs were based on resource consumption furnished from KPMCP (Kaiser-Permanente Medical Care Program) for both inpatient and outpatient expenditures
• Costs were based on the health care system perspective
• A death was assigned an infinite cost

Early
Late
“Initial” Post Early Discharge Cost through day i
Early baby discharged at day 0
Late baby discharged at day i
“Subsequent” Costs from day i to day 180
“Total” Cost (Early or Late Baby)
“Initial” day 0 through i Pre-Discharge Late Costs
“Subsequent” Costs from day i to day 180
i days
“Post-Discharge” Costs for Late Baby: from day i to day 180+i
“Post Discharge” Cost for Early Baby
“First” Cost for Late Baby = i days

Defining Clinical Outcomes
• We constructed a continuous metric for POST DISCHARGE outcomes based on a “Coherence” score [Rosenbaum, Biometrics 1994 ]
• Each patient is compared to the other 1401 patients in the data set to rank order their outcomes
• Death > (ICU days & Hospitalized Days) > ED visits > Sick Visits
• Score + 1 if you are unambiguously worse than someone else, -1 if better and 0 if ambiguous

Results
• Quality of the matches
• Patterns of Discharge by NICU and day of week
• Cost Results
• Outcome Results
• Sensitivity Analysis

(1) (2) (3) (4) (5) (6)
Late Baby
at Early Late Baby at DIFFAV DIFFAV
Early Baby Baby Late Baby (3)-(2) (4)-(2)
Variable Name Discharge Discharge Discharge (SD) (SD)
PMA (days) 247.4 247.4 250.9 0 0.29e
Gest age at
birth (wks) 31.1 31.1 31.2 0.03 0.03
Male Sex 0.51 0.52 0.52 0.01 0.01
Weight (birth) 1669 1686 1686 0.03 0.03
SNAP-II 20 to 59 0.15 0.13 0.13 -0.05 -0.05
SNAP-II 10 to19 0.18 0.20 0.20 0.04 0.04
SNAP-II 0 to 9 0.67 0.67 0.67 0.01 0.01ap<0.05; bp<0.01; cp<0.005; dp<0.001; ep<0.0001
Matching Results for 701 Early and 701 Matched Late Babies

(1) (2) (3) (4) (5) (6) Late Baby at Early Late Baby at DIFFAV DIFFAV Early Baby Baby Late Baby (3)-(2) (4)-(2)Variable Name Discharge Discharge Discharge (SD) (SD)
Propensity to discharge 0.67 0.64 1.33 -0.03 0.75e
Apnea score 0.04 0.05 0.03 0.08 -0.16Brady score 0.06 0.07 0.04 0.09 -0.15Methyl score 0.04 0.03 0.02 -0.08 -0.17Oxygen score 0.11 0.11 0.07 0.01 -0.15a
Gavage score 0.22 0.23 0.10 0.01 -0.65e
Incubator score 0.15 0.15 0.08 0.01 -0.34e
Combined score 0.62 0.63 0.34 0.02 -0.70e
ap<0.05; bp<0.01; cp<0.005; dp<0.001; ep<0.0001
Matching Results for 701 Early and 701 Matched Late Babies

(1) (2) (3) (4) (5) (6) Late Baby at Early Late Baby at DIFFAV DIFFAV Early Baby Baby Late Baby (3)-(2) (4)-(2)Variable Name Discharge Discharge Discharge (SD) (SD)
Weight on day specified 2153 2148 2231 -0.01 0.22e
Weight < 1700 0.02 0.03 0.01 0.06 -0.091700 < W < 1800 0.06 0.06 0.02 -0.03 -0.17e
Weight > 1800 0.92 0.91 0.97 -0.01 0.19e
BPD 0.09 0.11 0.11 0.06 0.06NEC 0.01 0.01 0.01 -0.04 -0.04ROP > 2 0.06 0.06 0.06 -0.01 -0.01IVH > 3 0.02 0.01 0.01 -0.05 -0.05ap<0.05; bp<0.01; cp<0.005; dp<0.001; ep<0.0001
Matching Results for 701 Early and 701 Matched Late Babies

(1) (2) (3) (4) (5) (6) Late Baby at Early Late Baby at DIFFAV DIFFAV Early Baby Baby Late Baby (3)-(2) (4)-(2)Variable Name Discharge Discharge Discharge (SD) (SD)Maternal Age 29.9 30.3 30.3 0.08 0.08Single 0.24 0.24 0.24 0 0Other Child = 0 0.40 0.37 0.37 -0.07 -0.07Other Child = 1 0.34 0.37 0.37 0.07 0.07Other Child > 2 0.26 0.26 0.26 0.01 0.01Income x K ($) 59.5 59.5 59.5 0 0White Race 0.47 0.48 0.48 0.02 0.02Black 0.10 0.09 0.09 -0.02 -0.02Asian 0.20 0.23 0.23 0.08 0.08Hispanic 0.22 0.18 0.18 -0.09 -0.09
Matching Results for 701 Early and 701 Matched Late Babies

Patterns of Discharge
• NICU Early discharge rate ranged from 35% to 65% (P < 0.0001)
• Discharge varied by day of the week (P<0.001)– Sat & Sun: Observed vs Exp 358:401– Fri & Mon: Observed vs Exp 445:401
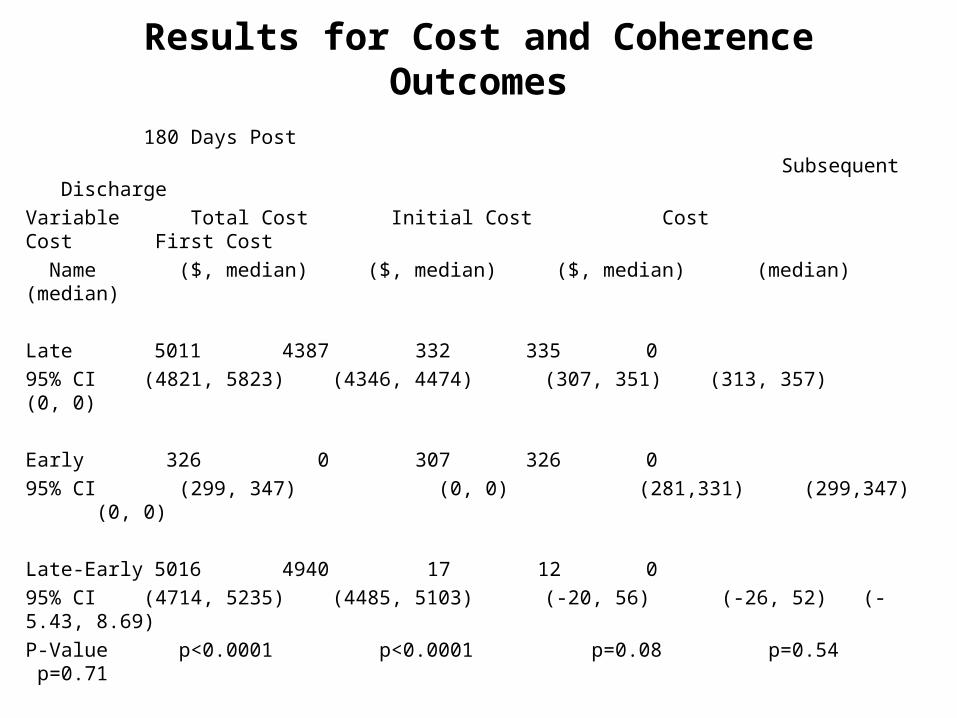
Results for Cost and Coherence Outcomes
180 Days Post
Subsequent Discharge
Variable Total Cost Initial Cost Cost Cost First Cost
Name ($, median) ($, median) ($, median) (median) (median)
Late 5011 4387 332 335 0
95% CI (4821, 5823) (4346, 4474) (307, 351) (313, 357) (0, 0)
Early 326 0 307 326 0
95% CI (299, 347) (0, 0) (281,331) (299,347) (0, 0)
Late-Early 5016 4940 17 12 0
95% CI (4714, 5235) (4485, 5103) (-20, 56) (-26, 52) (-5.43, 8.69)
P-Value p<0.0001 p<0.0001 p=0.08 p=0.54 p=0.71




Clinical Coherence Outcomes
Post Discharge First
Variable Coherence Coherence
Name ($, median) ($, median)
Late 2.6 -27.6
95% CI (-11.3, 13.1) (-27.7, -27.7)
Early 2.6 -27.6
95% CI (-11.3, 2.6) (-27.7, -27.7)
Late-Early 4.2 0
95% CI (-2.1, 11.0) (0, 0)
P-Value p=0.21 p=0.96



Sensitivity Analysis: Null Hypothesis states there is a difference
Odds Ratio*
Reject |$500|
Reject |$1000|
Reject |$2500|
1 <0.00001 <0.00001 <0.00001
2 0.002 <0.00001 <0.00001
3 0.90 0.14 <0.00001
5 1 1 0.002
* An unobserved variable that produces the odds of being discharged late

Summary
• Initial costs are higher for Late babies because they are still in the NICU while the Early are already discharged
• Subsequent costs are very similar• Post-discharge Costs (180 days) are
identical• Our results are very insensitive to an
unobserved variable highly associated with Late discharge and costs

Conclusions
• Holding babies solely to increase maturity (once the baby has achieved the usual milestones needed for discharge) will not save money or improve clinical outcomes

The End

Statistical Tests• For individual outcomes, we report medians and 95%
nonparametric confidence intervals for the median• For tests comparing outcomes in matched pairs, we
used Wilcoxon’s signed rank test, the associated confidence interval and the associated Hodges-Lehmann point estimate (Hollander and Wolfe 1999).
• In measuring balance on covariates at baseline, we used two standard informal measures:– DIFFAVE (Rosenbaum and Rubin 1985; Silber et al. 2001),
defined to be the difference in covariate means divided by the standard deviation
– For testing balance of a covariate before and after matching, we used Wilcoxon’s rank sum test (which compares the balance obtained by matching on covariates to the balance expected in a completely randomized experiment).